IMPROVING CARE TRANSITIONS IN NORTHWEST DENVER Risa Hayes, CPC Program Manager, CFMC Integrating Care for Populations and Communities ARC Learning Session February 23, 2012 This material was prepared by CFMC (PM-4010-058 CO 2012), the Medicare Quality Improvement Organization for Colorado under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy.
Transcript
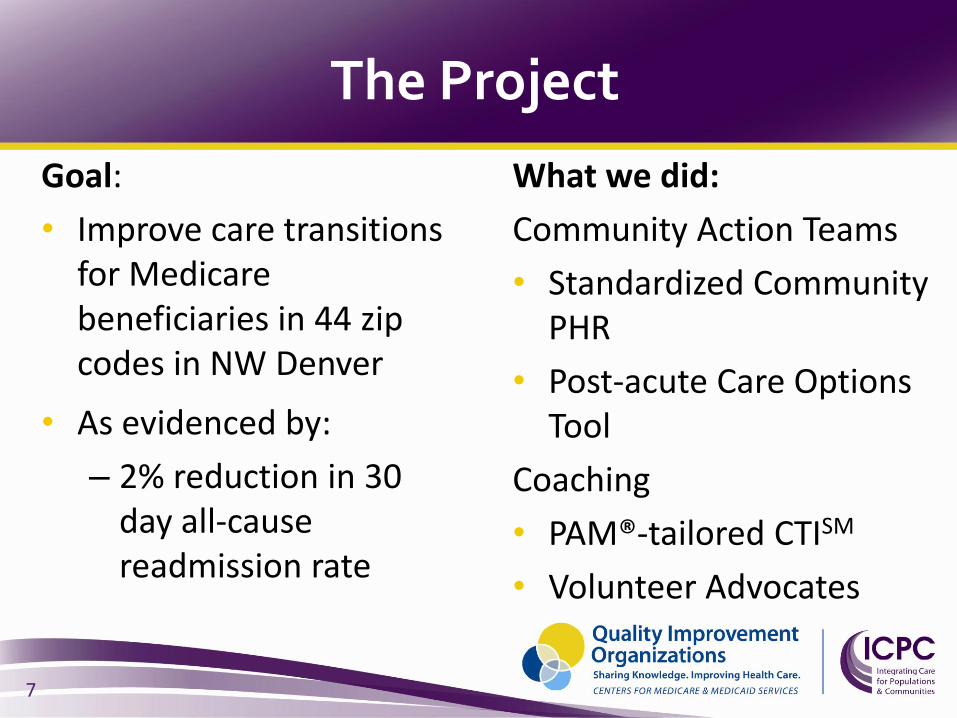
IMPROVING CARE TRANSITIONS IN NORTHWEST DENVER
Risa Hayes, CPC
Program Manager, CFMC
Integrating Care for Populations and Communities
ARC Learning Session
February 23, 2012
This material was prepared by CFMC (PM-4010-058 CO 2012), the Medicare Quality Improvement Organization for Colorado under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human
Services. The contents presented do not necessarily reflect CMS policy.
( )
Our Equation
Readmissions
and
Admissions
( ) 2
3
So What is a “Community”?
• The Medicare population that you serve and share with your partners and competitors
• Specified set of zip codes, in which the people you serve live
4
Who is the Community?
• Acute Care Hospitals
• LTACs
• SNFs
• Home Health Agencies
• Non-medical Home Care companies
• Senior Resource Centers
• Physician Offices
• Patient Advocates
• Hospice providers
• Palliative Care providers
• Medical Society
• Mental Health
• AAA
• QIO
• Hospitalists
• Physician management group
5
Why are people readmitted?
No community infrastructure for achieving common goals
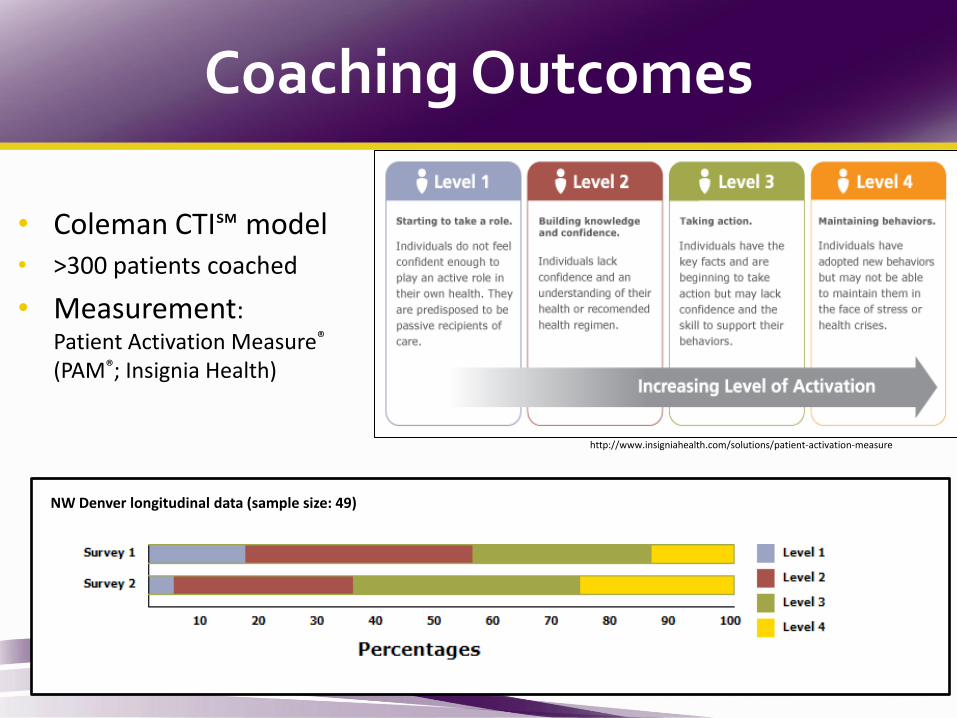
PAM questions assess three core domains – belief in self-impact, knowledge/skills, and confidence - that drive health behavior and outcomes
17
Sample Questions: #1: “When all is said and done, I am the person who is responsible for taking care of my health.” #12: “I am confident I can figure out solutions when new problems arise with my health”
The PAM is scored on a 100 point continuum. Most patients score between 35 and 80
PAM-13: Measuring Patient Activation
17
Does Activation Matter?
18
Inspiration
“I feel that I must tell someone about
how greatly I benefited from and
appreciate the services of the nurse
who follows up on patients
discharged from your hospital.
She comforted me and helped make
several forceful phone calls, and
soon all was well. What a great help!
What a relief! Thanks.”
Mr. H: A Patient Story
19
SeniorMetrix
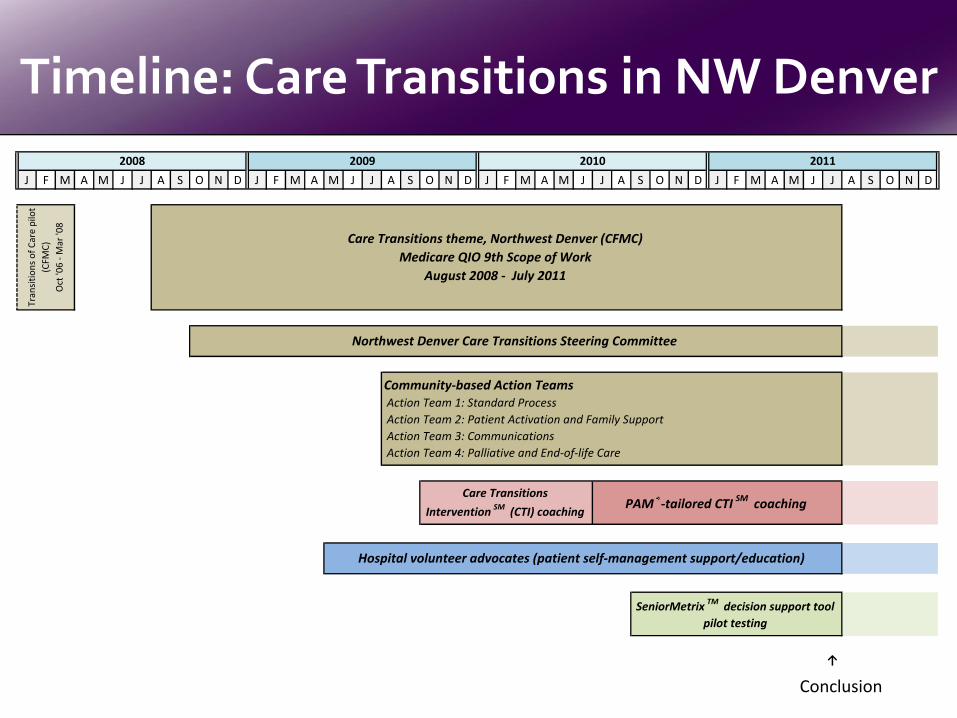
Care Transitions theme, Northwest Denver (CFMC)
Medicare QIO 9th Scope of Work
August 2008 - July 2011
Northwest Denver Care Transitions Steering Committee
Community-based Action Teams Action Team 1: Standard Process
Action Team 2: Patient Activation and Family Support