58
Pediatric Assessment & Care Management RN Residency Core Curriculum
| Date post: | 30-Dec-2015 |
| Category: |
Documents |
| Upload: | ira-hooper |
| View: | 39 times |
| Download: | 1 times |
Pediatric Assessment&
Care Management
RN Residency Core Curriculum
• Understand charting by exception and documentation at CCHMC.
• Understand the daily RN responsibilities.• Identify safety standards here at CCHMC.• Review case studies pertinent to pediatric
nursing care.
• Understand policies and procedures related to assessment and how to locate them.
• Describe the components of the pediatric health and physical assessment.
• Identify age appropriate exam techniques.
• Past Medical History• History of Present Illness• Family History• Social and Environmental History• Review of systems (Physical Assessment)
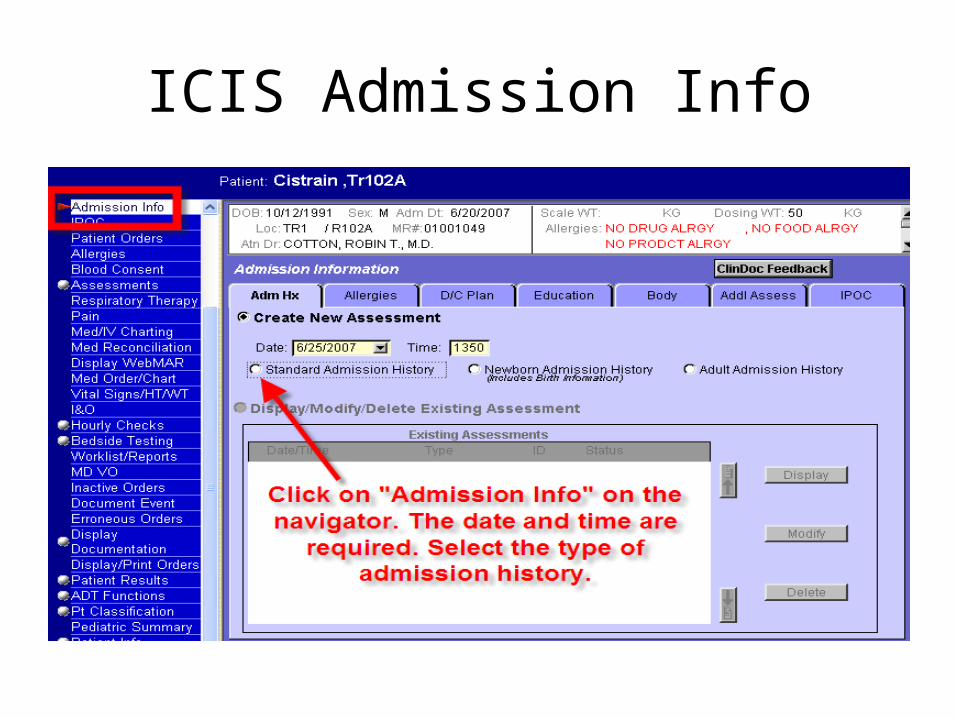
ICIS Admission Info
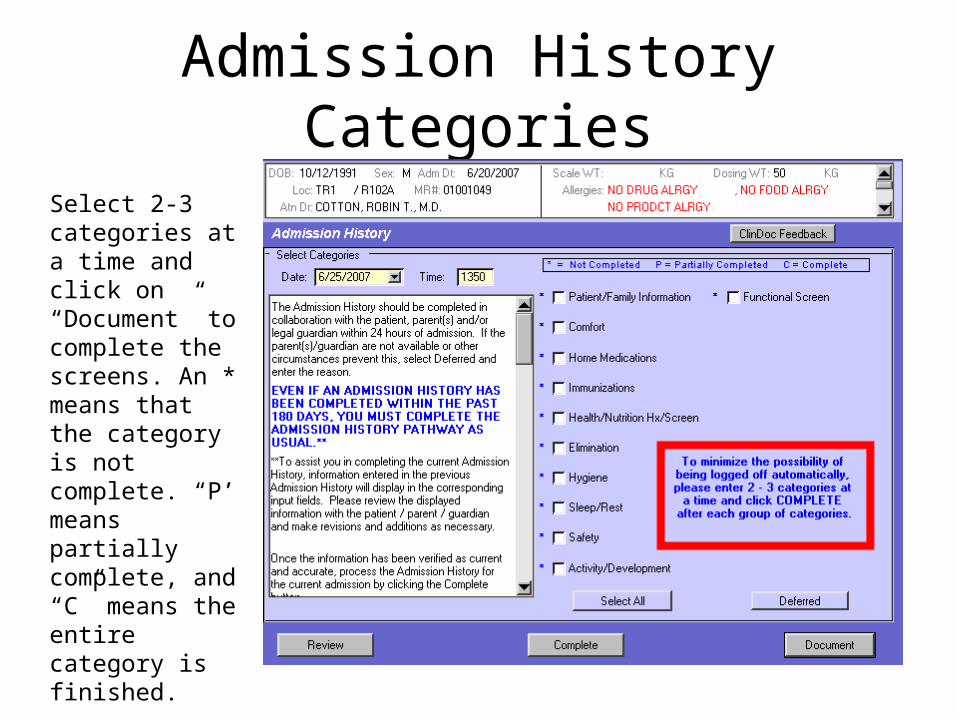
Admission History Categories
Select 2-3 categories at a time and click on “Document” to complete the screens. An * means that the category is not complete. “P’ means partially complete, and “C” means the entire category is finished.
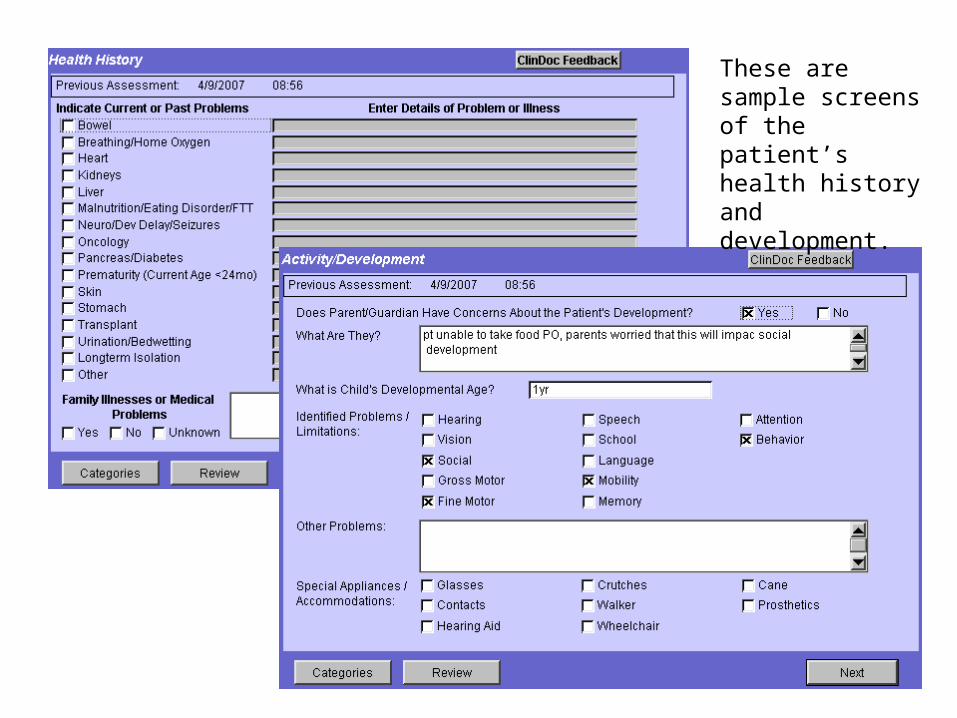
These are sample screens of the patient’s health history and development.

Past Medical History
• Perinatal history• Birth History• Hospitalizations• Previous Illnesses• Allergies
• Current Medications• Immunizations• Nutrition• Growth and
Development
• Signs
• Symptoms
• Onset
• What makes it better/worse?
Components of Pediatric Physical Assessment
• General Appearance
• Laboratory Values
• Vital Signs
• Physical Assessment


• Neurological• Respiratory• Cardiac • GI• GU• HEENT• Skin
Also include:
• PAIN• ACCESS
• Chart body assessment findings in ICIS according to policy VI-101
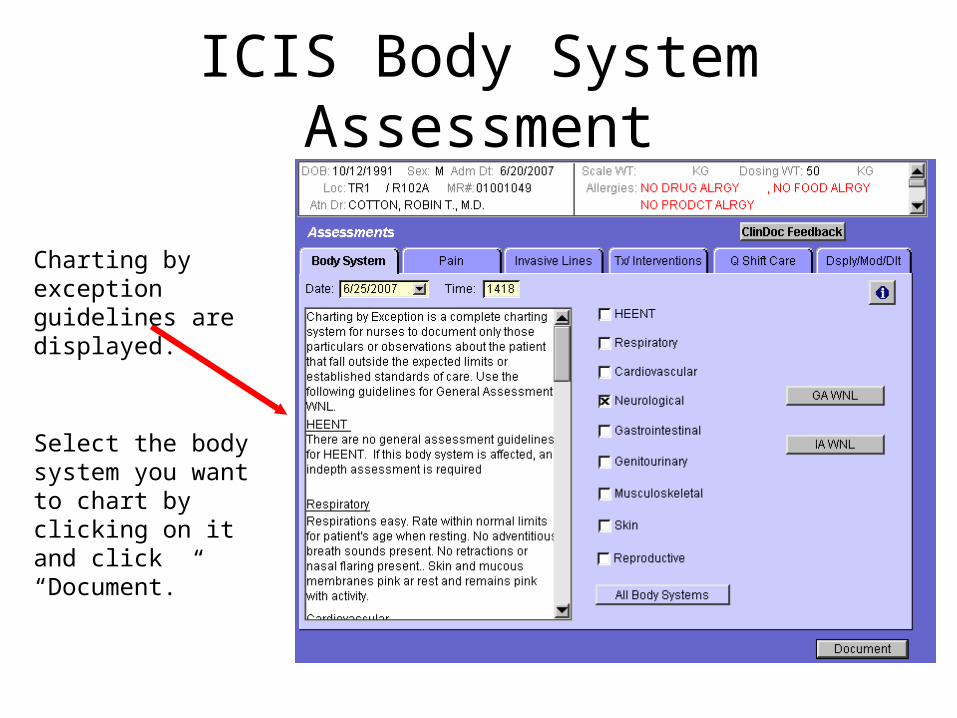
ICIS Body System Assessment
Charting by exception guidelines are displayed.
Select the body system you want to chart by clicking on it and click “Document.”
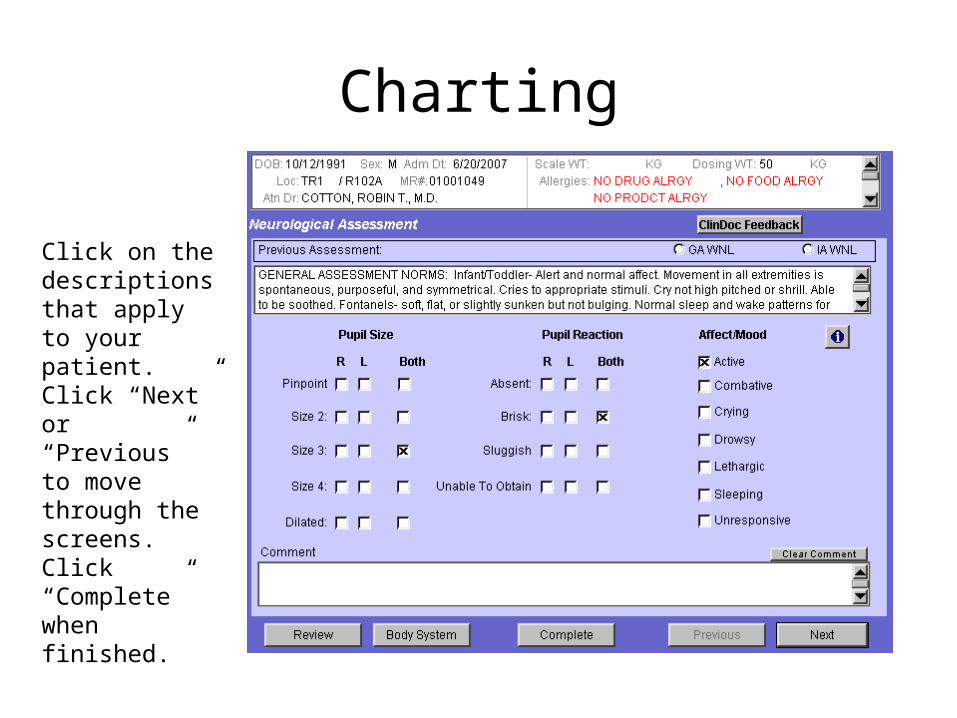
Charting
Click on the descriptions that apply to your patient. Click “Next” or “Previous” to move through the screens. Click “Complete” when finished.
General Appearance
• Physical Appearance
• Facial expression
• Posture, position and types of movement
• Activity
• Pain
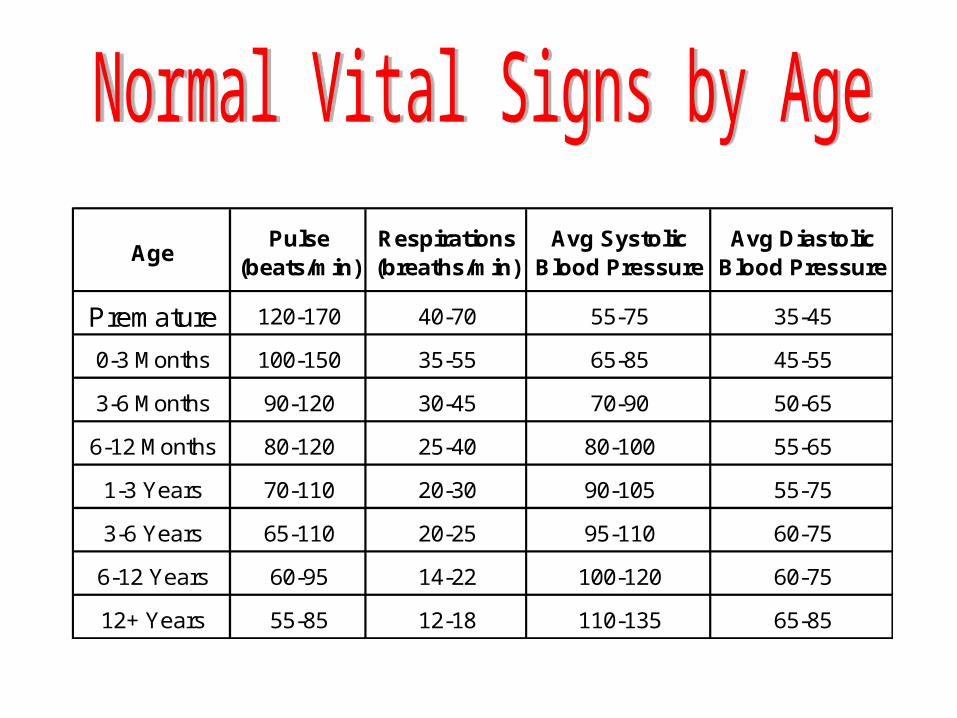
AgePulse
(beats/min)Respirations (breaths/min)
Avg Systolic Blood Pressure
Avg Diastolic Blood Pressure
Premature 120-170 40-70 55-75 35-45
0-3 Months 100-150 35-55 65-85 45-55
3-6 Months 90-120 30-45 70-90 50-65
6-12 Months 80-120 25-40 80-100 55-65
1-3 Years 70-110 20-30 90-105 55-75
3-6 Years 65-110 20-25 95-110 60-75
6-12 Years 60-95 14-22 100-120 60-75
12+ Years 55-85 12-18 110-135 65-85
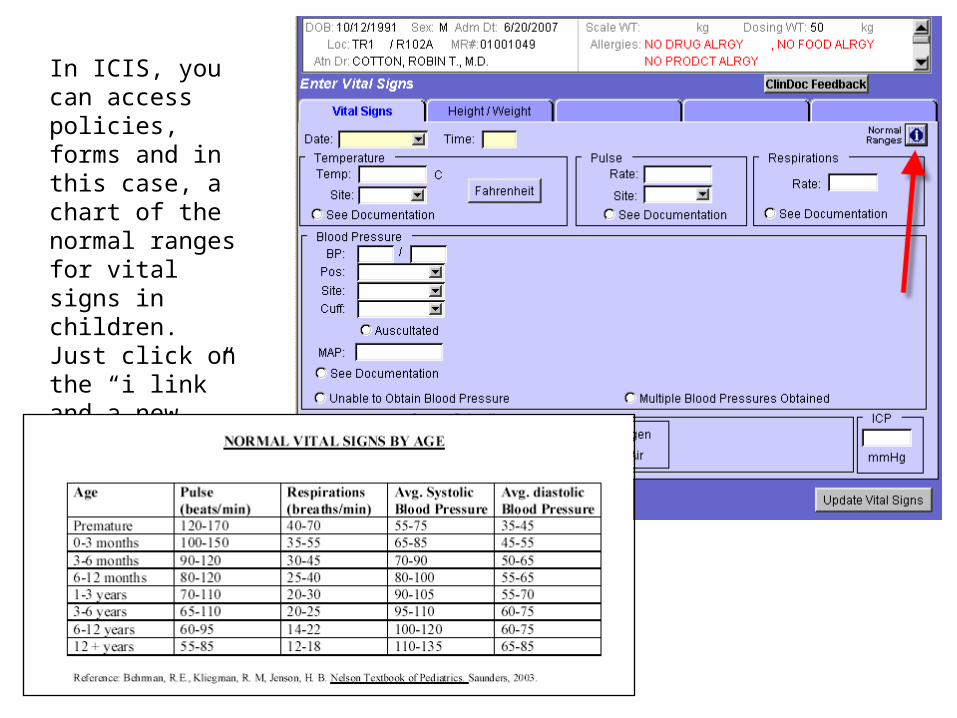
In ICIS, you can access policies, forms and in this case, a chart of the normal ranges for vital signs in children. Just click on the “i link” and a new window will open with information.
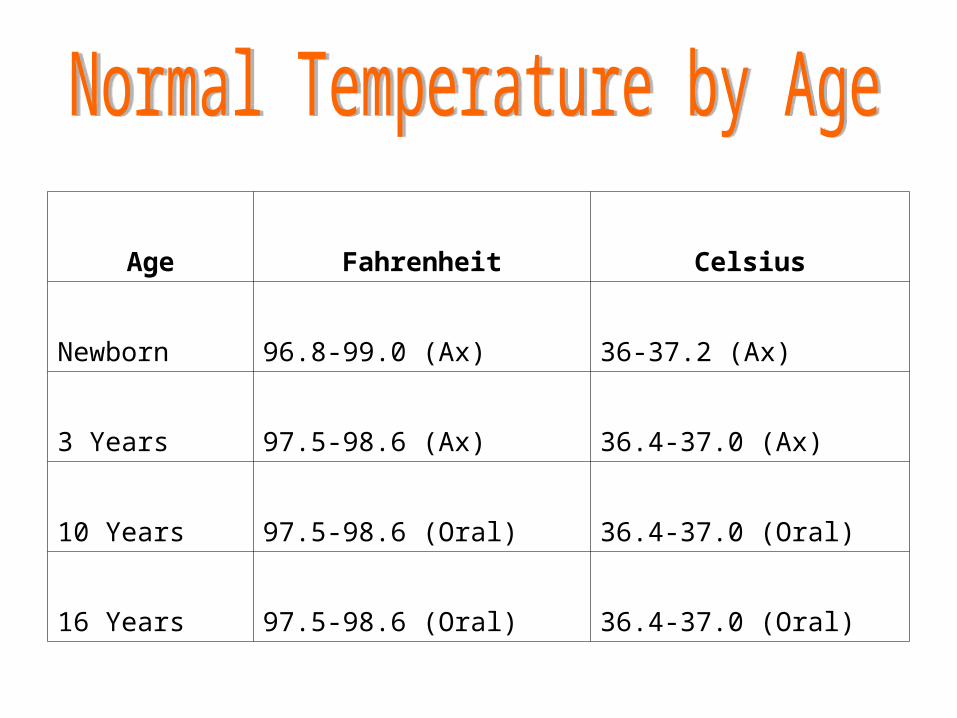
Age Fahrenheit Celsius
Newborn 96.8-99.0 (Ax) 36-37.2 (Ax)
3 Years 97.5-98.6 (Ax) 36.4-37.0 (Ax)
10 Years 97.5-98.6 (Oral) 36.4-37.0 (Oral)
16 Years 97.5-98.6 (Oral) 36.4-37.0 (Oral)
Where to start.

• Receive report from off-going RN• Organize yourself.• Ensure you have your
equipment.• Tell the parent what you are
going to do.• Enlist the parent(s) help.• Wash your hands.• Physical Exam should be flexible
– Allow for play and exploration• Least invasive to the most
intrusive– Inspect, “look”– Auscultate, “listen”– Palpate/percussion, “feel”.
• Neurological• Respiratory• Cardiac • GI• GU• HEENT• Skin/Musculoskeletal
• Fontanels, suture lines• Look for asymmetry• Distended neck veins• Swollen glands• Eyes (PEARL, Tracking,
Size)• Ears• Nose (Nasal Flaring =
respiratory difficulty)• Nasal membranes• Mouth (Mucus
membranes)
• Level of Consciousness (LOC)• Fontanels• Head Circumference• Pupillary Response• MAE• Pain
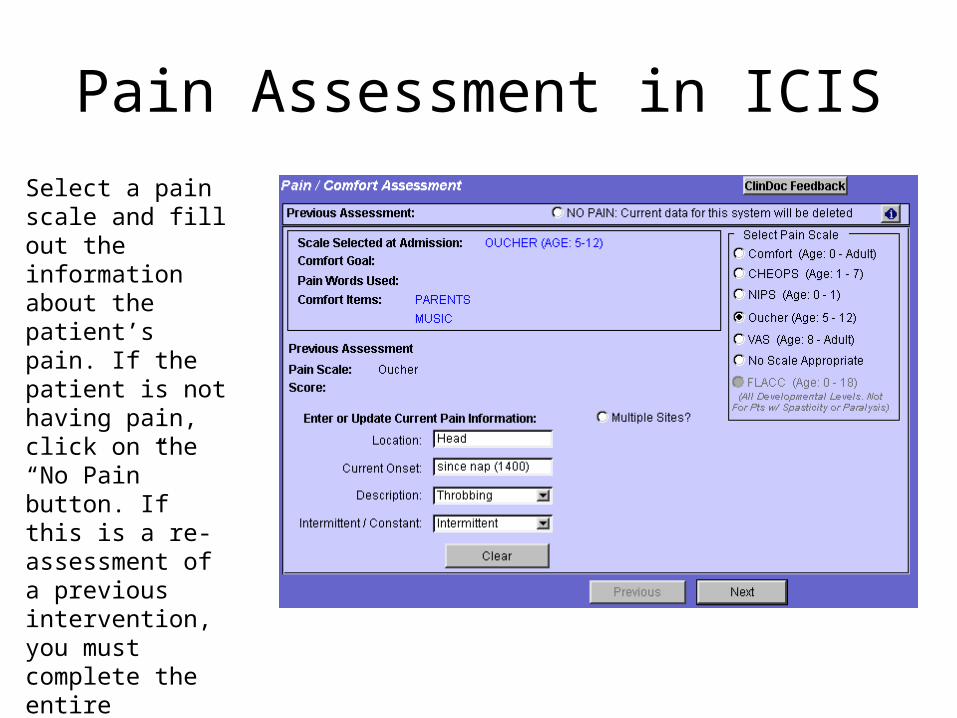
Pain Assessment in ICIS
Select a pain scale and fill out the information about the patient’s pain. If the patient is not having pain, click on the “No Pain” button. If this is a re-assessment of a previous intervention, you must complete the entire assessment and may not click on “No Pain.”
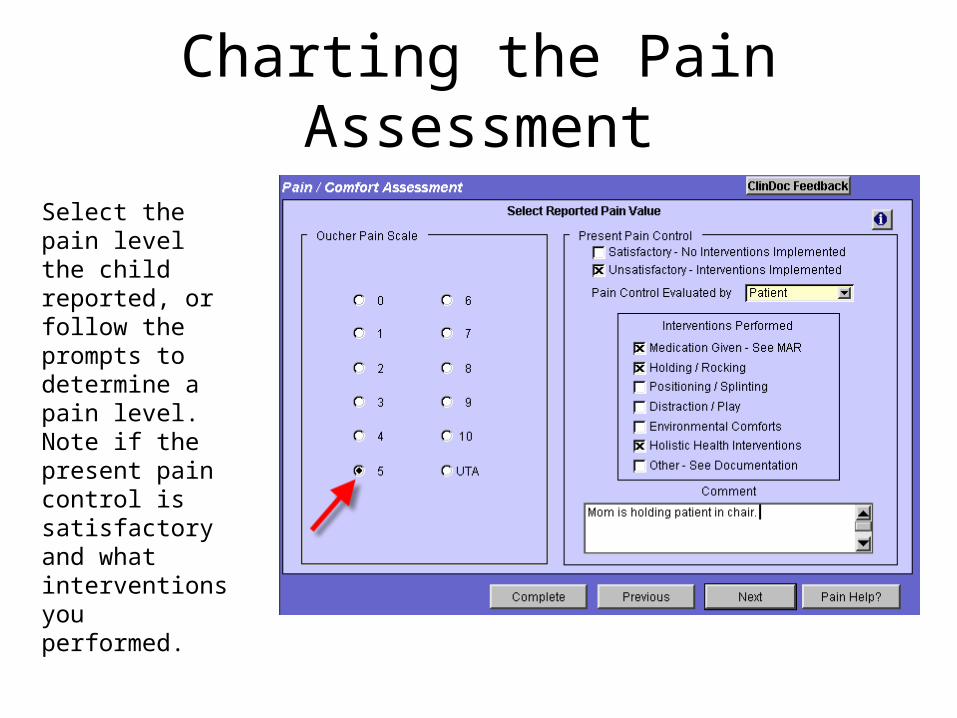
Charting the Pain Assessment
Select the pain level the child reported, or follow the prompts to determine a pain level. Note if the present pain control is satisfactory and what interventions you performed.
• Respiratory Rate• Work of Breathing• Color• Air Movement• O2 Saturations• O2 Requirements• What do they
sound like?
• Airway Differences– Smaller upper and lower
airways
– Infants obligate nose breathers
– Tongue is larger in proportion to mouth
– Less compensatory reserve than adults
– Infants rely primarily on diaphragm for breathing
• Heart rate/rhythm: WNL for age (use apical)
• Murmur: Present or not.• Palpable pulses: Radial,
brachial, femoral, pedal.• Capillary refill: < 3 seconds• Skin color: noncyanotic, warm
& dry• Urine output: WNL• Blood pressure: WNL for age• Edema• Access (PIV, PICC, CVC)
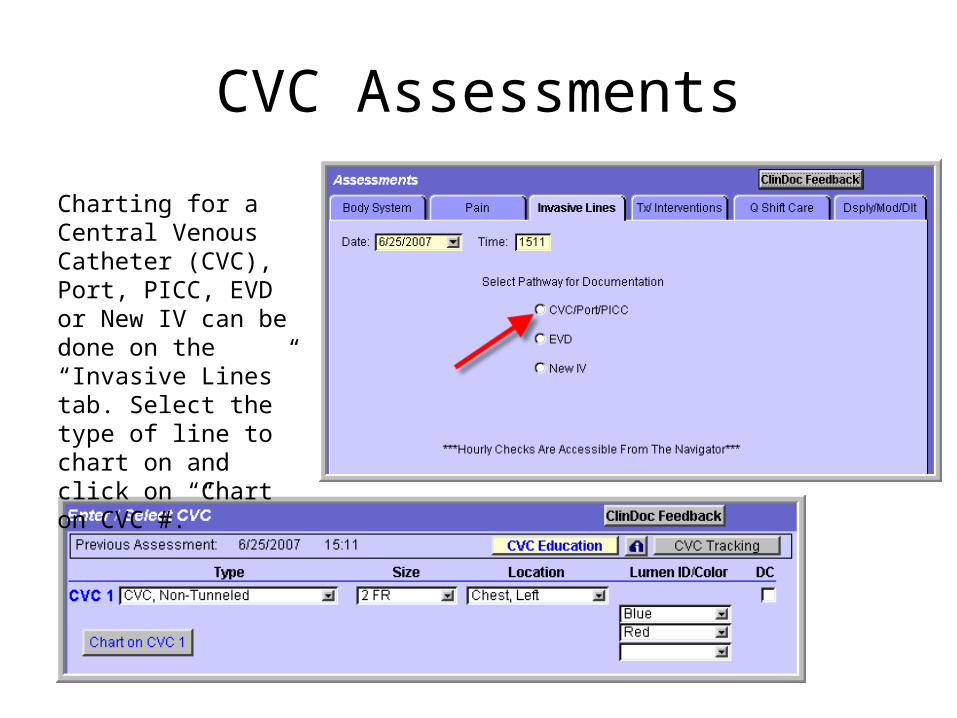
CVC Assessments
Charting for a Central Venous Catheter (CVC), Port, PICC, EVD or New IV can be done on the “Invasive Lines” tab. Select the type of line to chart on and click on “Chart on CVC #.”
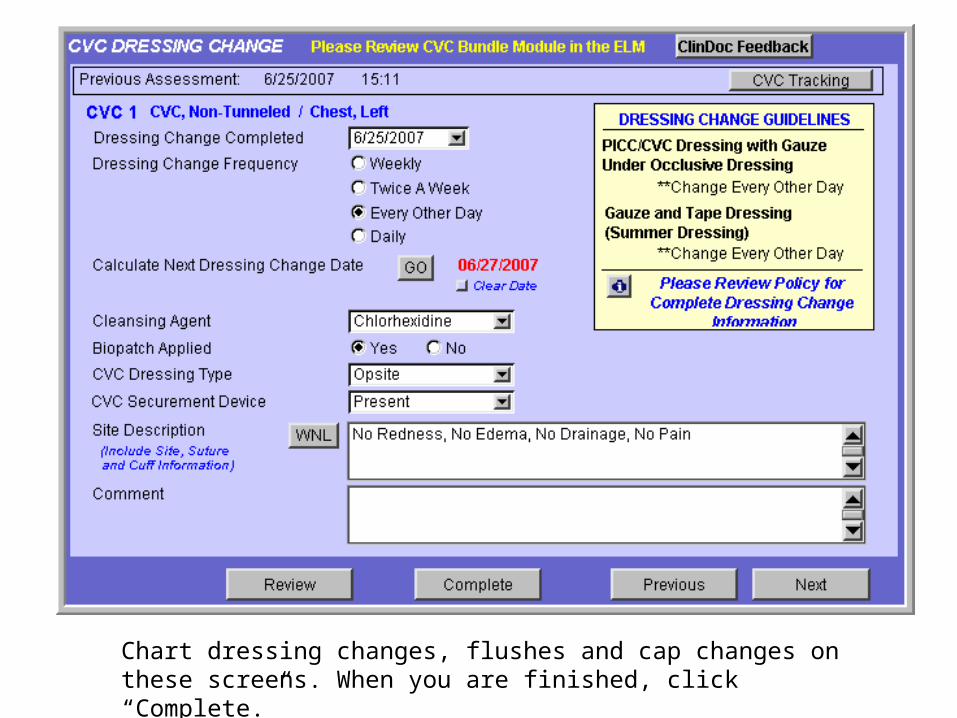
Chart dressing changes, flushes and cap changes on these screens. When you are finished, click “Complete.”
• Feeding and Swallowing
• Abdomen
• Intestinal Motility
• Stool
• Diet
• Tubes
• Urine output

• Motor Movement/gait• Muscle strength• Devices/casts
• Temperature• Color• Moisture• Turgor• Lesions, Rashes, scars
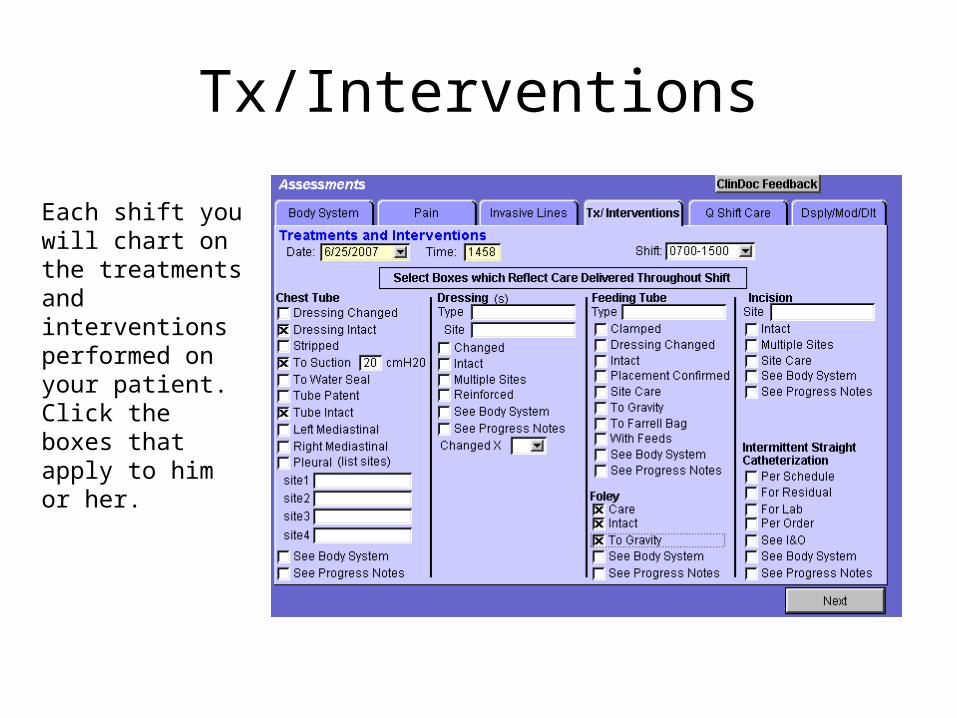
Tx/Interventions
Each shift you will chart on the treatments and interventions performed on your patient. Click the boxes that apply to him or her.
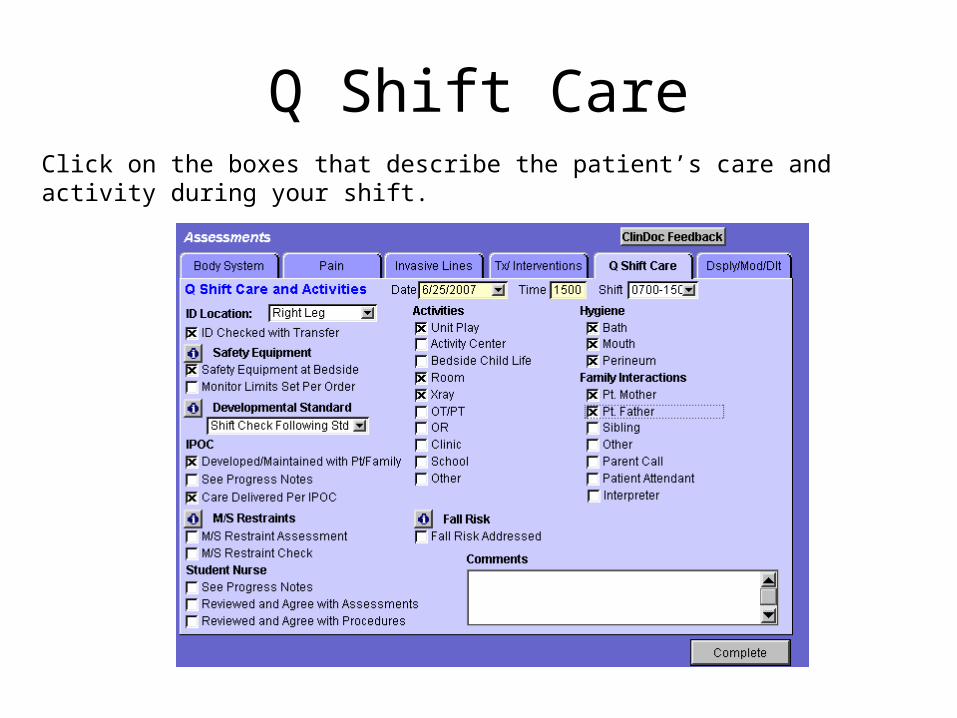
Q Shift CareClick on the boxes that describe the patient’s care and activity during your shift.
Preparation• Completely undress• Leave diaper on male infant• Pacify with bottle• Avoid abrupt movements• Enlist parent’s help
Positioning• Before sits alone: supine or prone• After sits alone: sit in parents lap
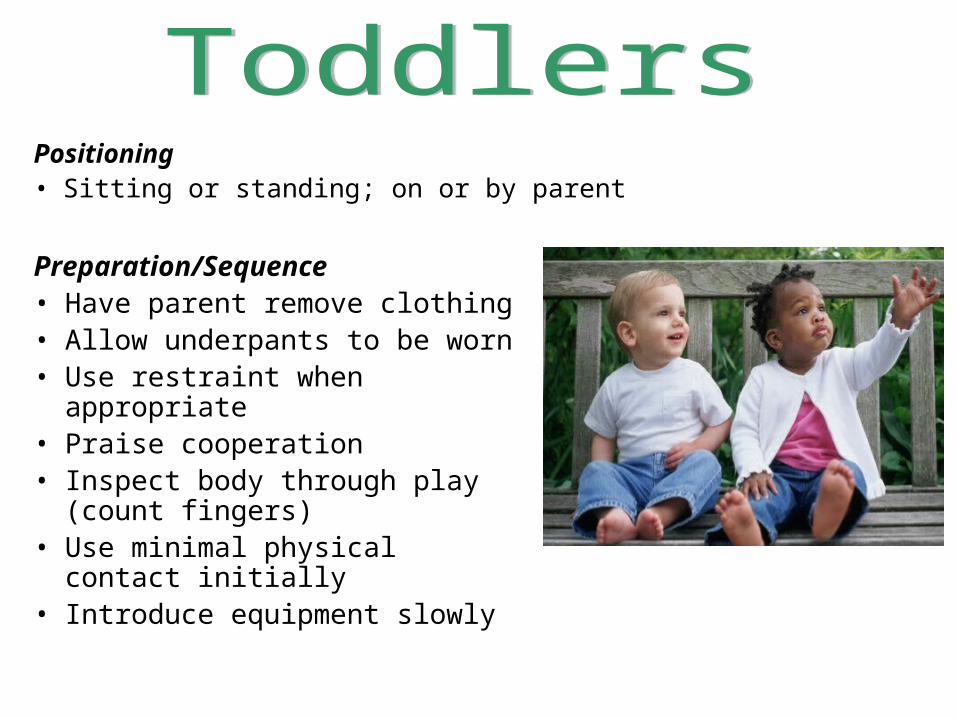
Preparation/Sequence• Have parent remove clothing• Allow underpants to be worn• Use restraint when appropriate• Praise cooperation• Inspect body through play
(count fingers)• Use minimal physical contact
initially• Introduce equipment slowly
Positioning• Sitting or standing; on or by parent
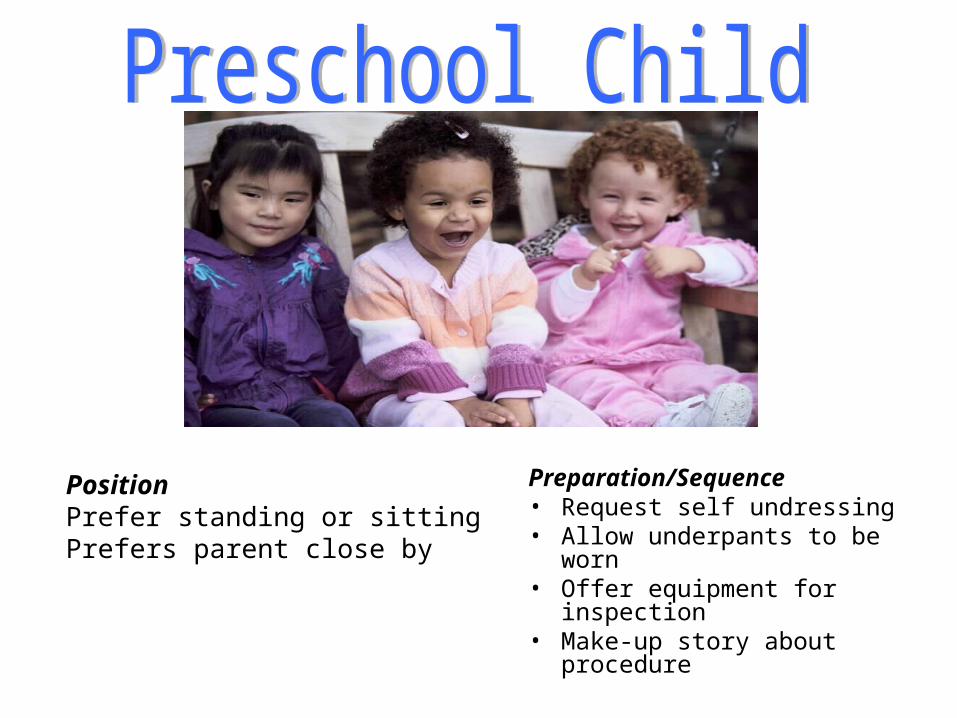
Preparation/Sequence• Request self undressing• Allow underpants to be worn• Offer equipment for
inspection• Make-up story about
procedure
PositionPrefer standing or sittingPrefers parent close by
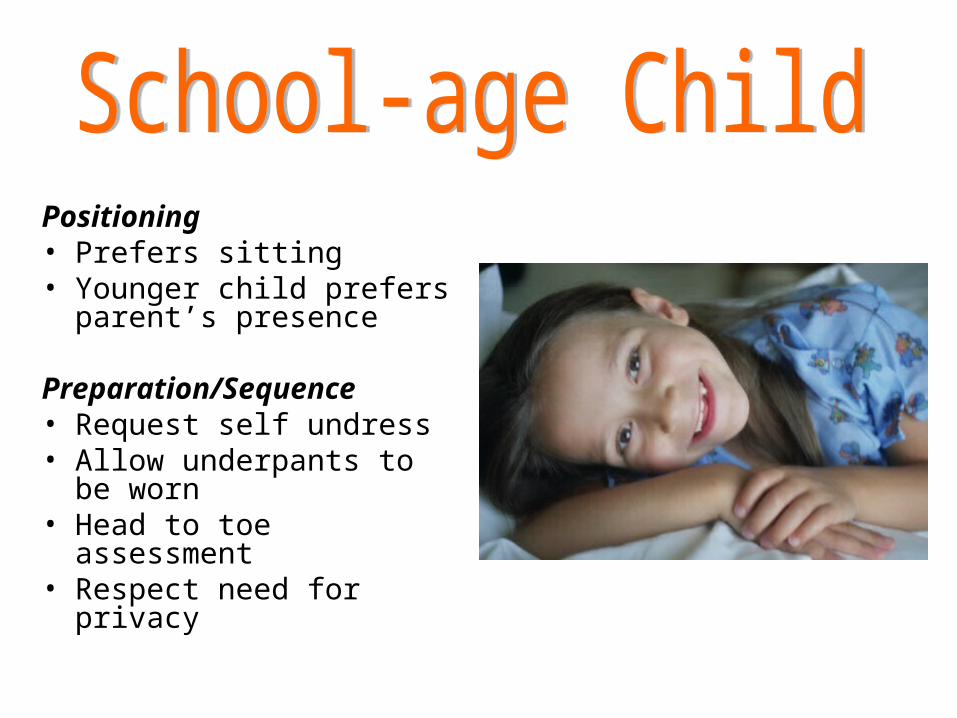
Positioning• Prefers sitting• Younger child prefers
parent’s presence
Preparation/Sequence• Request self undress• Allow underpants to be
worn• Head to toe assessment• Respect need for privacy
Getting Report• Basics – Name, age, weight, allergies
• Hx – Previous medical (surgeries, significant hospitalizations)
• Dx – Why are they here?
• Head to Toe
> Neurological > HEENT
> Respiratory > Access
> Cardiac > Pain
> GI/GU
> Skin
• Receive report.• Check orders – Shift check.• Review chart and update report notes as needed.• Initial brief check of patients.• Check all IV rates and fluids.• Complete assessment of patients within first 2
hours of your shift.• Verify your patient medications are available for
shift.
• Update the family/caregiver as needed.• Provide Discharge teaching and document any
teaching or education performed. • Coordinate ancillary services as needed
– Social Work– Case Management– Child Life– Chaplain
• Coordinate any off unit tests and arrange for transport.
• Provide Team Leader/Charge Nurse with updates on your patients as needed.
• Chart I & O’s at 0559, 1359 & 2159 and clear/zero pumps.
• Restock bedside supplies for on-coming nurse.
• Order medications/fluids for on-coming nurse.

• Armbands• Infection control• Medication 5 rights• Call light access• Side rails• Needle safety
• Emergency code blue• Monitors on with
alarms set • Fire alarm and
extinguishers• Abduction prevention
plan
Case #1:6 Month Old with URI
• 6 month old boy admitted for URI has been coughing and breathing fast during your shift. He has refused his 3pm bottle feed and is irritable and fussy. His respiratory rate is currently 60 bs/min., a pulse of 140/min., temp. 99.8F and has a normal blood pressure. You observe nasal flaring, intercostal and supraclavicular retractions and occasional grunting.
Case #2:2 Year Old with URI
• A 2 year old girl with URI. The report that you receive is satisfactory.
• You find her unresponsive and hypertonic with arched trunk and extended arms and legs that are jerking rhythmically. Her eyes are open, but her gaze is directed upward. She is bubbling saliva around her lips as well as circumoral cyanosis. This episode lasted 90 seconds.
Case #3:The Child with Diarrhea
• A 3 year old girl suffering from diarrhea for 2 days at home.
• Diarrhea continues during hospitalization for one day.
• Weight: 13.7 kg (you note that this is a slight decrease from the admit weight).
Case # 4:6 yr old w/ trach
• 6 year old developmental delay with a tracheostomy.
• Admitted with pneumonia that is responding well to antibiotics.
• Report is normal and routine care.
Case #5:The 7 Month Old with R/O
Infection
• 7 month old admitted with r/o infection during the night. One-day history of fever, vomiting and questionable abdominal pain.
• Suspect UTI, urine sent for urinalysis and urine culture.
• Antibiotics have been started as ordered• Report is normal.• The infant is irritable but fully awake & alert.
Policies and Procedures
• IV-105 Documentation Guidelines for Charting by Exception
• VI-101 Assessment Standards
• VI-400 General Standards of Care for the Short Stay patient
• V-348 Adult Patient