20
Pediatric HIV Care & Treatment in Uganda A Five-Day Training Course For Health Professionals
| Date post: | 24-Dec-2015 |
| Category: |
Documents |
| Upload: | shanon-may |
| View: | 229 times |
| Download: | 1 times |

Pediatric HIV Care & Treatmentin Uganda
A Five-Day Training CourseFor Health Professionals
Module I: Introduction to Paediatric HIV Care & Treatment in Uganda
Key questions:• Why is there a need for Paediatric HIV care and
treatment? (WHY ARE WE HERE?)• What difference can Paediatric HIV care and
treatment make?
• Why is Paediatric HIV care for children and infants so challenging?
• How is Uganda currently addressing Paediatric HIV Care & Treatment?
• How can you be part of the solution?

Global & National HIV Estimate for adults and children, 2009
Global Uganda
People Living with HIV 33.3 million 1 million
Children living with HIV 2.5 million (7.5%) 146,000 (14.6%)
Total New Infections 2.6 million 132,500
New Infections in Children 370,000 (14%) 25,000 (18.8%)
Death due to HIV 1.8 million 70,000
Deaths due to HIV children 260,000 ??
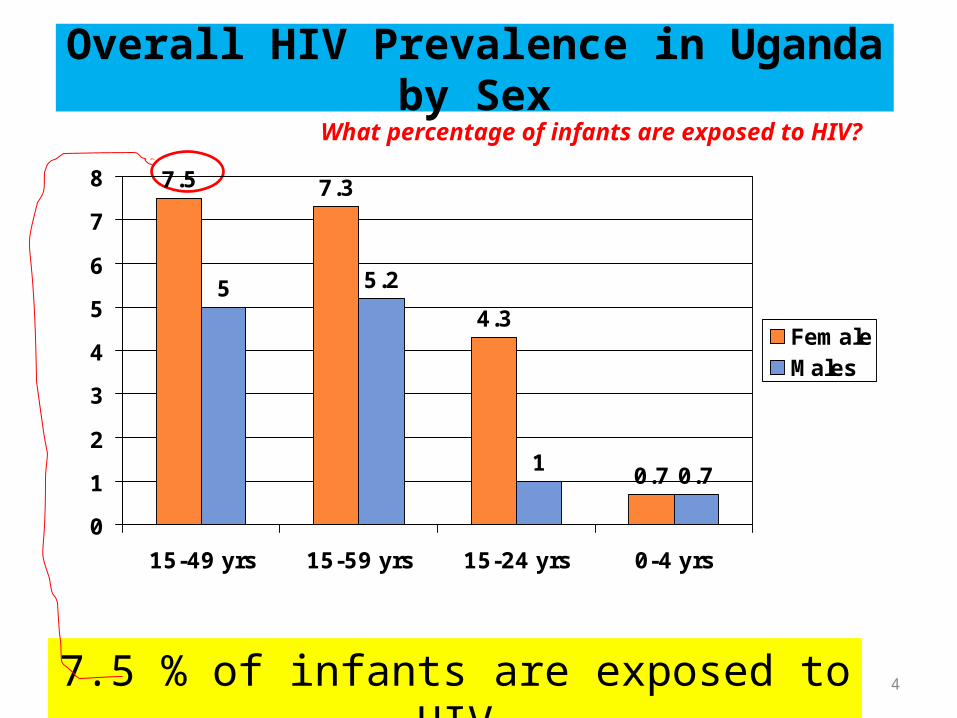
Overall HIV Prevalence in Uganda by Sex
7.5 7.3
4.3
0.7
5 5.2
10.7
0
1
2
3
4
5
6
7
8
15-49 yrs 15-59 yrs 15-24 yrs 0-4 yrs
FemaleMales
47.5 % of infants are exposed to HIV
What percentage of infants are exposed to HIV?

What key factors contribute to the high HIV
prevalence in children in Uganda?
• High prevalence of HIV infection in women of child bearing age
• Low coverage of PMTCT interventions
• Stigma
• Lack of male partner involvement
• Multiple and concurrent sexual partners
• Intergeneration sexual issues

Modes Of HIV Transmission To Children
Vertical transmission Refers to mother-to-child transmission of HIV (MTCT);
contributes 95% of infected infants
• In an untreated breastfeeding population the total transmission rate is 30 - 45%
How or when does MTCT occur?During pregnancy 5-10%
During labor & delivery 10-15%
Through breast feeding 5-20%
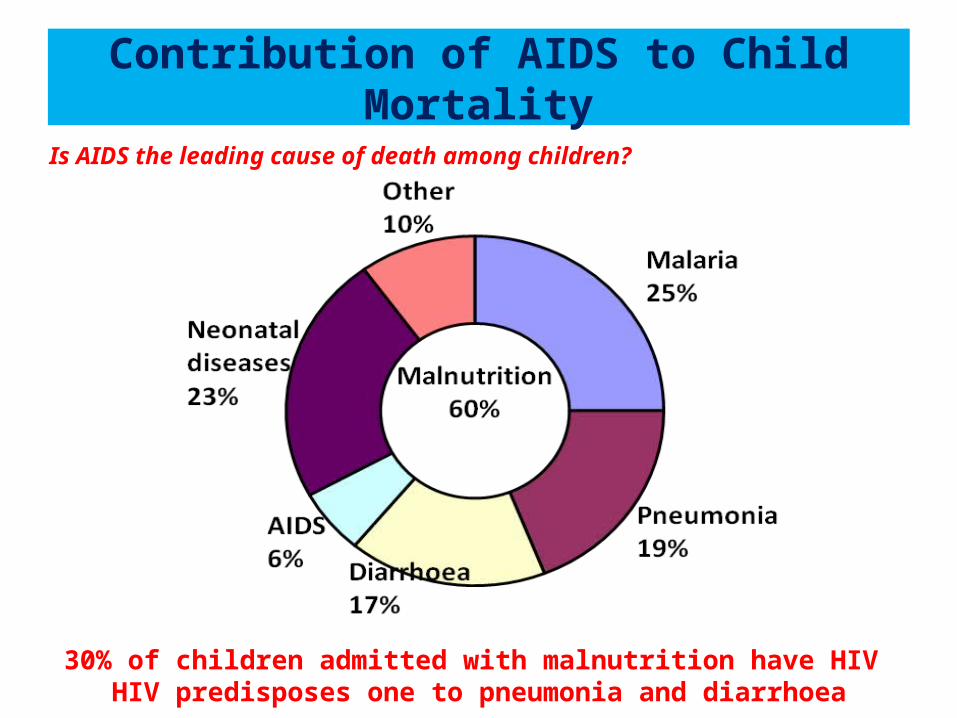
Contribution of AIDS to Child Mortality
30% of children admitted with malnutrition have HIV HIV predisposes one to pneumonia and diarrhoea
Is AIDS the leading cause of death among children?

What main activities are included in Paediatric HIV Prevention, Care & Treatment program?
• Maximize Interventions for prevention of Mother to child transmission
• Increase availability of EID services
• Proactively identify and link to care HIV exposed and HIV infected infants and children.
• Ensure quality care , treatment, follow up of HIV exposed / infected infants and children
• Increase availability of and access to Paedaitric ART
• Promote family centered care model.

Strategic Framework for Prevention of HIV Infection in Infants and Young Children
Prevention of unintended
pregnancies in HIV infected
women
Provision of care and support for HIV-infected women, their children, and their families
Prevention of mother-to-child
HIV transmission
Primary Prevention
Of HIV

10
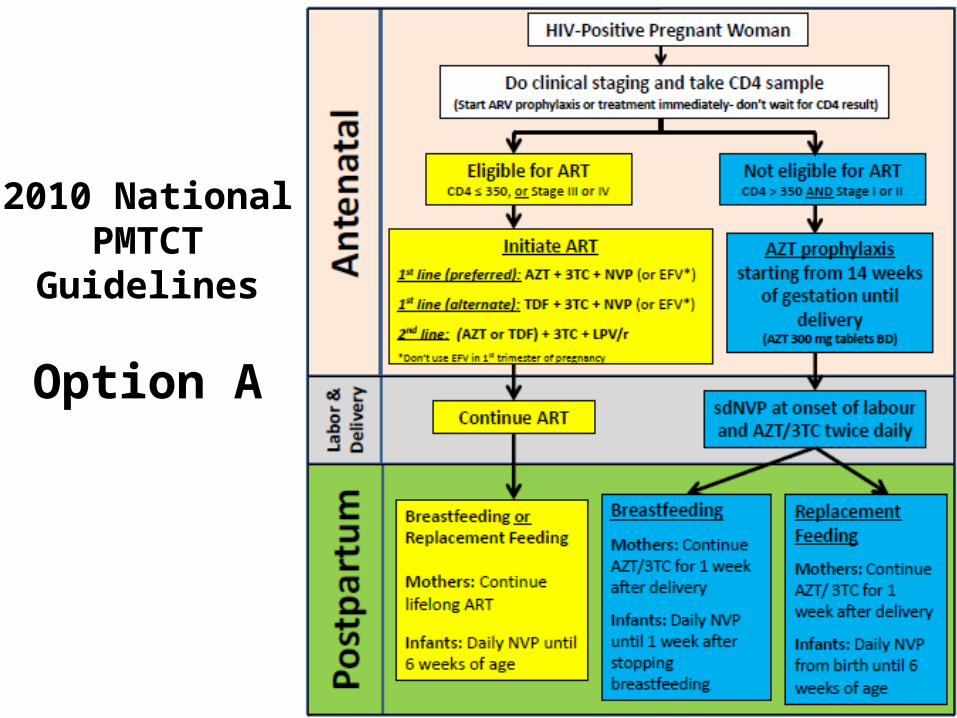
Revised PMTCT guidelines -Option A
MotherIf CD4 >350 or stage 1,2• Ante partum AZT (from 14 weeks)• sdNVP + AZT/3TC at delivery• AZT/3TC for 7 days postpartum
If CD4 ≤350 or stage 3 or 4: Lifelong ART
Infant• If breastfeeding: daily NVP from birth until one wk after breastfeeding has
stopped• If not breastfeeding or mother on ART: NVP for 6 wks
Uganda has adopted Option Awith plan to transition to Option B when sufficient resources are available
11
2010 National PMTCT Guidelines
Option A
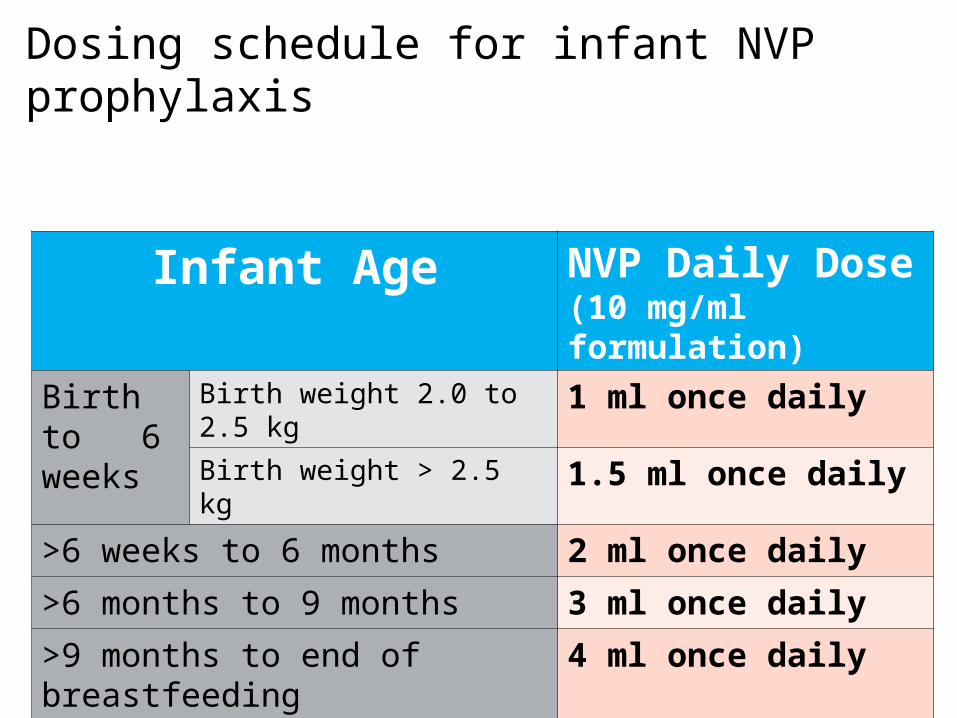
Dosing schedule for infant NVP prophylaxis
12
Infant Age NVP Daily Dose (10 mg/ml formulation)
Birth to 6 weeks
Birth weight 2.0 to 2.5 kg 1 ml once dailyBirth weight > 2.5 kg 1.5 ml once daily
>6 weeks to 6 months 2 ml once daily
>6 months to 9 months 3 ml once daily
>9 months to end of breastfeeding 4 ml once daily
What difference can Paediatric HIV care & treatment make?

14
Provide care for exposed and infected infants
Newell et al. Lancet 2004: vol 364: 1236-43
Without ART, 50% of HIV-positive infants will die by age 2

15
Provide care for exposed and infected infants
Newell et al. Lancet 2004: vol 364: 1236-43
Typical age at initiation of ART
Without ART, 50% of HIV-positive infants will die by age 2

16
Provide care for exposed and infected infants
Newell et al. Lancet 2004: vol 364: 1236-43
Typical age at initiation of ART
Without ART, 50% of HIV-positive infants will die by age 2
Why is it so challenging to care and treat HIV exposed children and infants in our country?
What are the challenges you experience?What are the main barriers you face?Activity: Pair workDiscuss with your partner, and then in your Guides, list the main BARRIERS or CHALLENGES you experience in your working areas/clinics in caring for and treating HIV exposed / infected children.

What did we learn about the challenges and barriers we face in implementing effective Paediatric HIV care?
• There are certainly many challenges, but thereare also several actions you can take to help mitigate some of these barriers!
• This training is designed to provide you with knowledge and skills to help you take appropriate actions and better serve HIVexposed and infected children and their families.

You are part of the solution!We hope you will become front-line pediatric
HIV care and treatment providers.This training will help you:• Gain the necessary skills, knowledge, and tools to
effectively treat and care for HIV infected children/infants.
• Gain the confidence, knowledge and skills to communicate with caretakers of HIV exposed or infected children/infants.
• Become equipped with the tools and skills to improve your systems to effectively integrate pediatric HIV services into your clinics.

The Government is also part of the solution
Ugandan Government is committed to: • To virtually eliminate Paediatric HIV/AIDS by 2015
• Scale up care & treatment for HIV Infected children to all sites providing ARV’s by 2012
Level of effort:• Strengthen the PMTCT-EID program & scale up to 20% of HCIII• Train and mentor• Ensure availability of commodities• Strengthen lab capacity for EID to improve turn around time• Ensure availability of ARV’s
















