106
Ed Mulligan, PT, DPT, OCS, SCS, ATC Advanced Physical Therapy Practice: Clinical Orthopedic Residency Education Series 2014 Pediatric Orthopedic Management

Ed Mulligan, PT, DPT, OCS, SCS, ATC
Advanced Physical Therapy Practice: Clinical Orthopedic Residency
Education Series 2014
Pediatric Orthopedic Management

Children and Adolescents
Child = 2 years to puberty Adolescent = onset of puberty to cessation of growth,
epiphyseal closure, and attainment of adult stature– Adolescent Growth Spurt
Girls 10‐11 Boys 12‐13
– Epiphyseal Fusion Girls 15 Boys 17

Determining Musculoskeletal (vs. chronological) AgeTanner Stages of Physiologic Maturity
STAGE MALE FEMALE
I No pubic hair No breast development
II Minimal pubic hair Breast budsMinimal pubic hair
III Pubic hair over penisVoice changes
Enlargement of breastPubic hair on monsAxillary hair
IV Adult pubic hairAxillary hair
Areola enlargementAdult pubic hair
V Adult Adult
GIRLS BOYS

Determining Musculoskeletal (vs. chronological) Age
Greulich/Pyle Atlas
Greulich/Pyle Atlas– X‐ray of left hand– Available as iPad app

Anatomical and Physiological Differences in Pediatric Patient
Structure/System Pediatric Adult
Skeletal Sites of primary and secondary growth centers
Greater vascularity and porosityStronger periosteumHigher levels of circulating hormones
Fully ossified and closed growth centers
Less likely to completely remodel from a fracture
Soft Tissue Greater tissue pliabilityPredominance of type III collagenLess force productionLoss of flexibility and coordination during growth spurts
Greater tissue stiffnessPredominance of type I collagenGreater muscular force production
Metabolic Greater energy expenditure during activityPoor thermoregulation, longer to acclimatize to heat
Great mechanical efficiencyEfficient temperature regulation
What you see … What I seeWhat you see … What I see
Adolescent Injuries
Participation in athletics is high– 55% participation (59% male vs. 41% female) according
to 2011 survey of National Federation of State High School Associations– Texas has the most (10% of U.S. population)
Overuse injuries accounted for 10% of injuries in 1980, now 50% Traumatic injury rate relatively unchanged
– 6% will sustain traumatic sports injuries that require medical care in 1980; 7% more recently
Injury rate increases as age increases– 3% injury rate in elementary school, 7% in junior high, and 11% in high
school

Injury Source
40% in unorganized sports 38% in physical education class 15% in organized school sport 7% in community sponsored sports
Highest injury rates occurred in football, gym games, and speed augmented sports (roller and skate boards)

Musculoskeletal Risk Factors
Structural qualities are different in children as comparedto adults, therefore healing responses also differ

Immature Musculoskeletal System
The weak link is the growth plate (epiphyses) and the area of tendon attachment (apophysis)
The growth plate is vulnerable to abnormal mechanical pressures/forces and alterations in the timing, direction, and magnitude of the force

Unique Adolescent Risk Factors
Pliable bones Articular cartilage is soft and has
decreased resistance to repetitive loading
Ligaments 2‐3 x stronger than centers of bone growth
At greater risk for apophyseal avulsion and tendon inflammation rather than muscular strain or tendonitis

Rapid Growth
Bone elongation is faster than muscle elongation resulting in inflexibility
Muscle imbalance predisposes to sprains, strains, and overuse injuries
Differential growth rate of bone and soft tissue during periods of growth creates imbalances that can lead to injury
Somatotype
• Inconclusive evidence linking body type to incidence of injury
• Some studies suggest that heavier or obese athletes tend to be injured more often

Adolescent Flexibility
Some investigators believe flexibility has on effect on risk of injury – others do not
“abstract” ideal along the continuum of flexibility
Joint hyperlaxity (especially knee and shoulder) have been implicated as risk factors
“Tight” adolescents are at higher risk for apophyseal and soft tissue injuries

Adolescent Strength
Researchers do agree that increased muscle strength is important in averting injury
Weak Neck ‐ cervical spine and soft tissue injuries Weak Rotator Cuff ‐ shoulder subluxation and tendinitis Weak Trunk ‐ low back and hamstring injuries Weak Quads ‐meniscal and patellofemoral injuries Weak Lower Leg ‐ ankle sprains, “shin splints”, and Achilles injuries

Resistance Training in Children/Adolescents
Safe and effective if age appropriate guidelines followed– Most injury occurs with improper techniques, excessive
weight/resistance, and lack of adult supervision
Strength changes and muscular hypertrophy will not be distinguishable until post‐puberty
During preadolescence strength changes are related to neurological mechanisms– Increased motor unit activation– Motor unit coordination/recruitment– Intrinsic adaptations
Weight Training General Guidelines
Teach proper technique with minimal loads or resistance Supervision/instruction from qualified fitness
or medical professional Provide exercise variety of all major muscle
groups Particular attention to the core muscles
(hips/trunk)
Consider Periodization– systematically varied over time
Weight Training General Guidelines
No ideal combination of sets/reps/frequency– 2‐3 x wk, nonconsecutive days– 2‐3 sets of 10‐15 reps
Intensity– Training intensity of 75% of 1 RM
or 6‐7 on perceived exertions scale Velocity – moderate General Design
– Incorporate balance and coordination– Emphasize functional movement and multi‐
directional exercise
Unique Considerations in Pediatric Orthopedic Examination
Growth status (height/weight change) Parental involvement Intellectual Capacity, Level of Attention, Fear level, etc Child activity level and interests Posture/Postural Habits Different expectations regarding strength/flexibility
Functional assessment whenever possible
Congenital Orthopedic Issues
Congenital Orthopedic Problems
Developmental Dysplasia of Hip Legg‐Calves‐Perthes Disease Slipped Capital Femoral Epiphysis Tibial Varum (Blount’s Disease) Talipes Equinovarus (Club Foot) Metatarsus Adductus Scoliosis Torticollis Start with Normal Physiologic Development
Normal Physiologic Pediatric Development
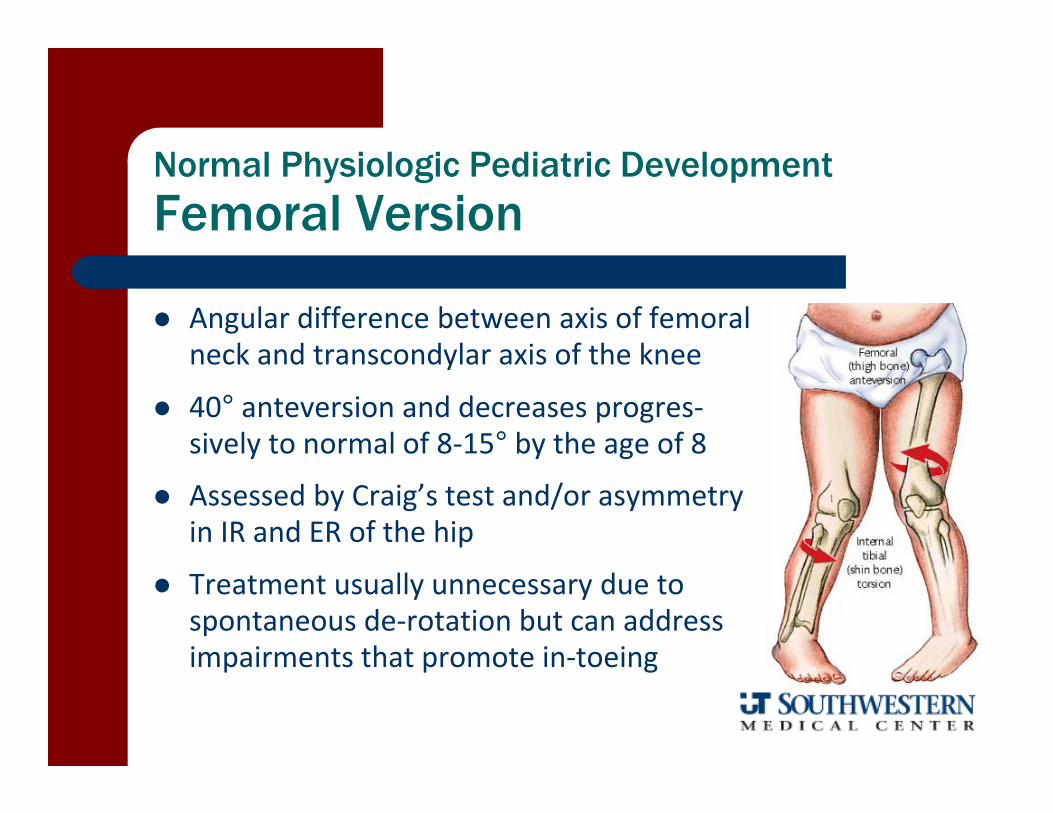
Femoral Version
Angular difference between axis of femoral neck and transcondylar axis of the knee
40° anteversion and decreases progres‐sively to normal of 8‐15° by the age of 8
Assessed by Craig’s test and/or asymmetry in IR and ER of the hip
Treatment usually unnecessary due to spontaneous de‐rotation but can address impairments that promote in‐toeing

Angular difference between transmalleolar axis and the transcondylar axis of the knee
External tibial torsion increases from about 5° at birth to 15‐20° at skeletal maturity
Assessment: — Evaluate amount of posterior displacement of
lateral malleolus compared to medial malleolus with the knee flexed to 90°
Osteotomies generally only considered when deformity is + 3 S.D. — > 10° internal torsion or > 35° external torsion
Normal Physiologic Pediatric Development
Tibial Torsion

Natural Development of Coronal Plane Knee Alignment
Bowlegs: up to age 1½‐2 yrs and straightening by 2½ years Knock‐Knees: up to 4 yrs and straightening by 6 years
When to be concerned:– Delayed motor milestones– Marked unilateral asymmetry– Persistence of normal variation
beyond age when usually resolved– Red Flags: difficult birth, prematurity

Developmental Dysplasia of Hip (DDH)
Hip anomalies with predisposition to instability and dislocation
Incidence– 1 per 100 – subluxation – 1 per 100 – dislocation– 6:1 female‐to‐male ratio
Etiology– Multifactorial– small intrauterine space, breech delivery, hormone laxity

DDH
Additional Risk Factors– White and Navajo Indian– First Born– Female– Breech delivery
Requires post‐birth US screening
Complications if untreated– Pain– Waddling gait with decreased agility– Early onset hip OA

DDH Signs/Symptoms
Clinical Examination– Newborn
5‐10° asymmetry or limitation of hip ROM Asymmetric thigh or gluteal folds
– Older children exhibit trendelenberg or waddling gait Unequal femoral length
Special Tests

DDH Special Tests
New Borns Ortolani Test
– From FLEX/ADD ABDUCT hip– + test = clunk
Barlow Test– From FLEX/ABD ADDUCT hip with post glide– + test = dislocation/clunk
3 months or older Galeazzi’s Test
– One knee lower than the other
Barlow Maneuver Ortolani Maneuver
DDH Treatment
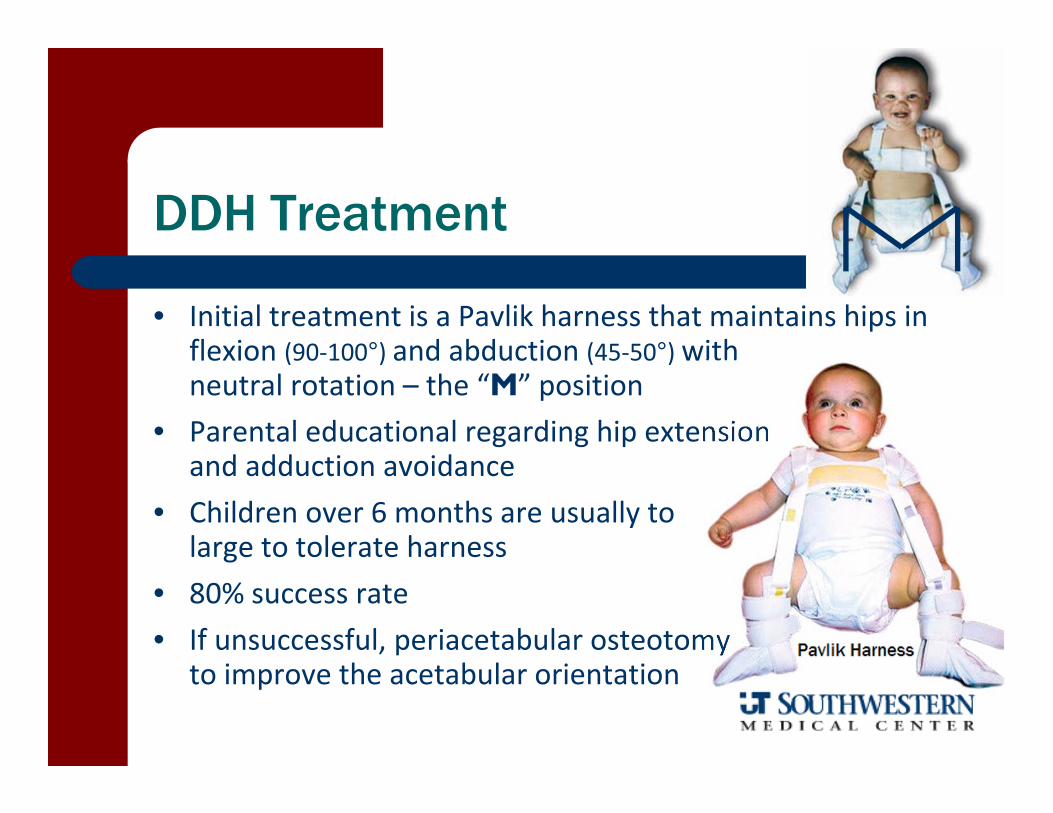
• Initial treatment is a Pavlik harness that maintains hips in flexion (90‐100°) and abduction (45‐50°) with neutral rotation – the “M” position
• Parental educational regarding hip extension and adduction avoidance
• Children over 6 months are usually to large to tolerate harness
• 80% success rate• If unsuccessful, periacetabular osteotomy
to improve the acetabular orientation

Legg Calves Perthes - coxa plana
Axial non-enhanced CT scan through the hip clearly shows the loss of structural integrity of the right femoral head.
avascular necrosis resulting in a flattening of the femoral head
LCP Disease
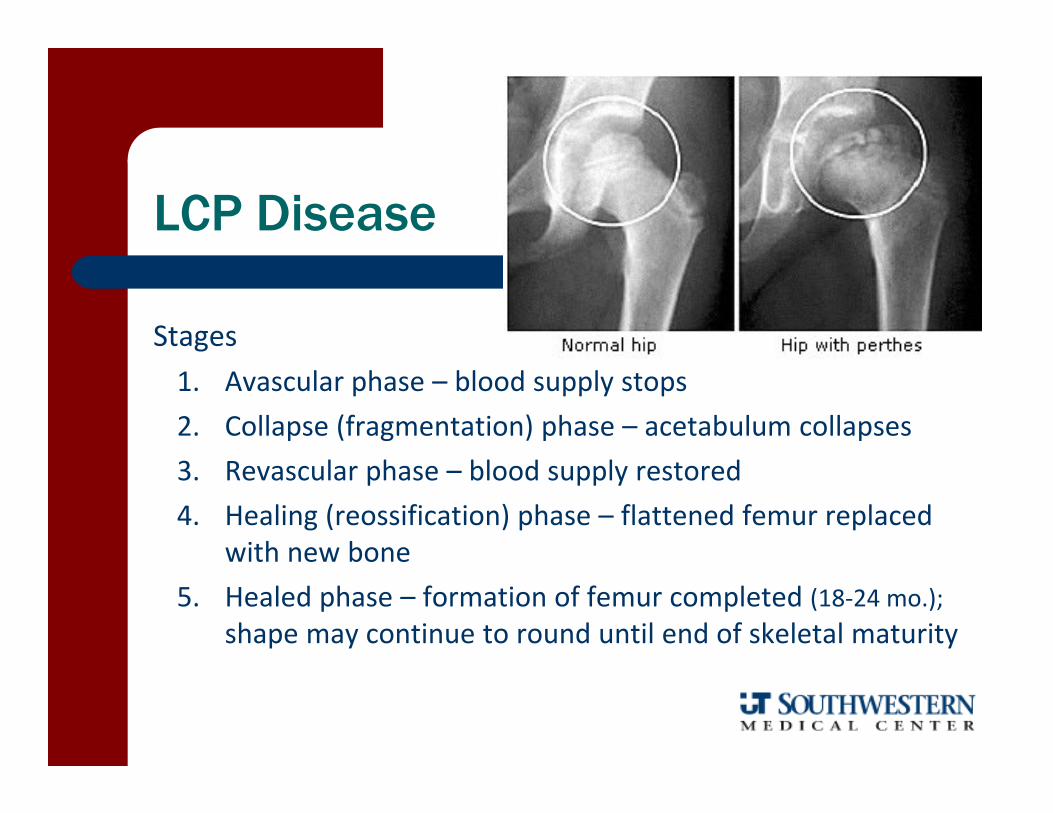
Stages1. Avascular phase – blood supply stops2. Collapse (fragmentation) phase – acetabulum collapses3. Revascular phase – blood supply restored4. Healing (reossification) phase – flattened femur replaced
with new bone5. Healed phase – formation of femur completed (18‐24 mo.);
shape may continue to round until end of skeletal maturity
• Prevalence: 1:1200 kids (males > females)
• Self limiting disease with spontaneous healing as necrotic bone is replaced by new bone formation over 1‐4 years
• Can have residual effects from incon‐gruency and persistent hip abductor weakness
Legg-Calves-Perthes Disease

Signs and Symptoms:– Usually a gradual onset in boys (4:1) between the age of 4‐8– More typical in small for age, hyperactive kids– Mild limp (trendelenburg) following activity with vague hip and groin
pain; symptoms usually relieved by rest– Limitations in Abduction and Internal Rotation
Management:– Rest (reduced activity), crutches prn, maintain ROM (especially
abduction), NSAIDs, – Surgery indicated if over 8 (femoral or pelvic osteotomy)
Legg-Calves-Perthes Disease

Slipped Capital Femoral Epiphysis (SCFE)
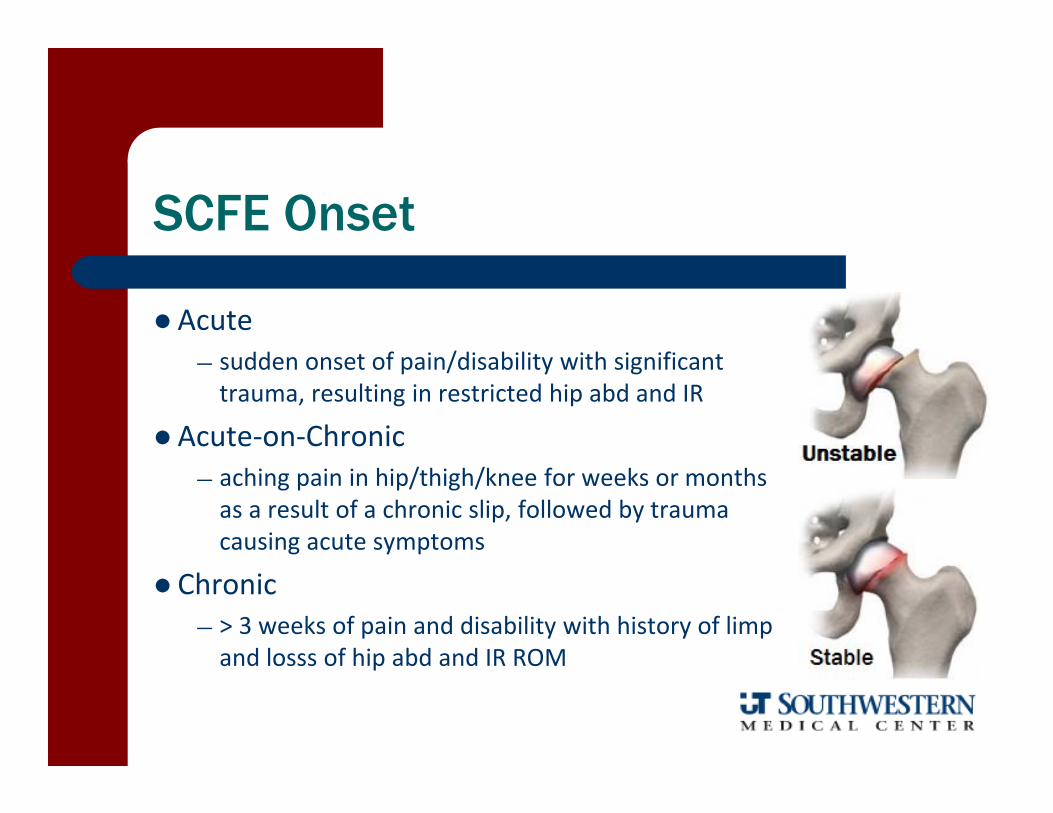
Femoral head slips in a posteromedial direction on the femoral neck
Acute: sudden onset of pain/disabilityChronic: > 3 week onset of pain/disabilityAcute‐on‐Chronic:
SCFE Onset
Acute — sudden onset of pain/disability with significant trauma, resulting in restricted hip abd and IR
Acute‐on‐Chronic — aching pain in hip/thigh/knee for weeks or months as a result of a chronic slip, followed by trauma causing acute symptoms
Chronic — > 3 weeks of pain and disability with history of limp and losss of hip abd and IR ROM
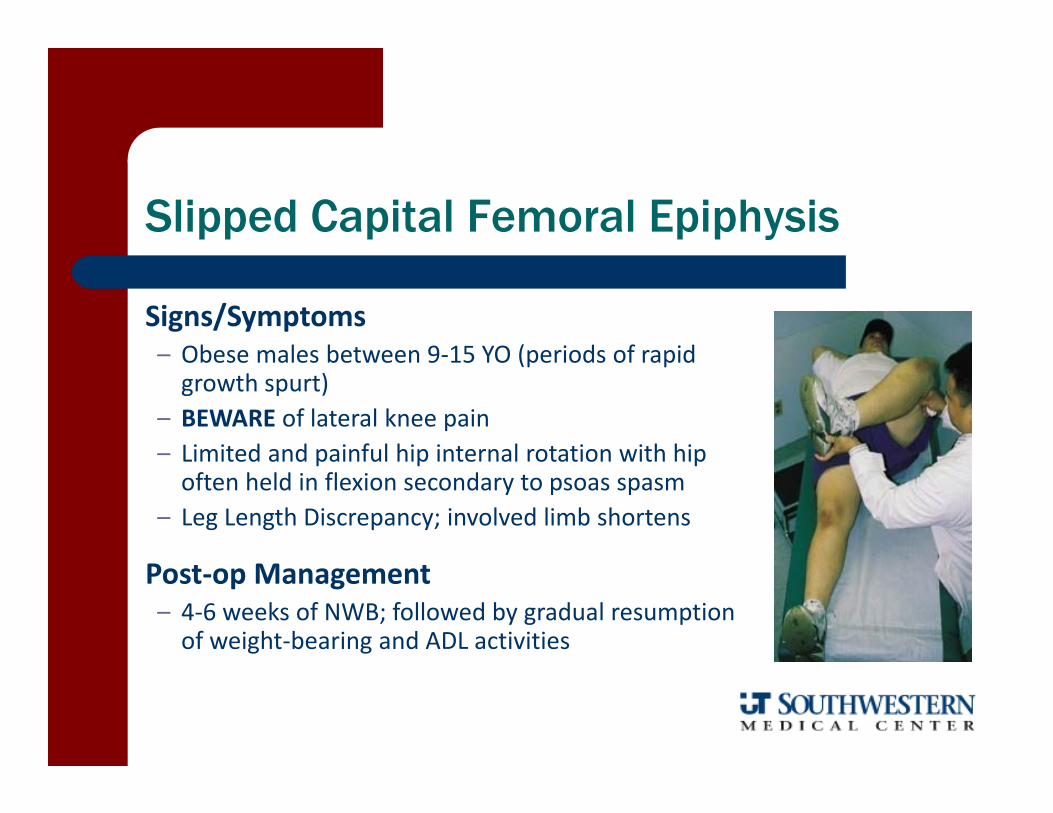
Signs/Symptoms– Obese males between 9‐15 YO (periods of rapid growth spurt)
– BEWARE of lateral knee pain– Limited and painful hip internal rotation with hip often held in flexion secondary to psoas spasm
– Leg Length Discrepancy; involved limb shortens
Post‐op Management– 4‐6 weeks of NWB; followed by gradual resumption of weight‐bearing and ADL activities
Slipped Capital Femoral Epiphysis

SCFE has more limitation in flexion SCFE symptoms are usually more severe Evidence of slippage evident on radiograph
Clinical Evidence of Slippage Stable
– vague knee/hip pain;– antalgic limp with toe out gait
Unstable– hip flexion accompanied by ext. rotation– unable to walk without crutches
Differentiation of SCFE and LCP
Tibia Vara (Blount’s Disease)
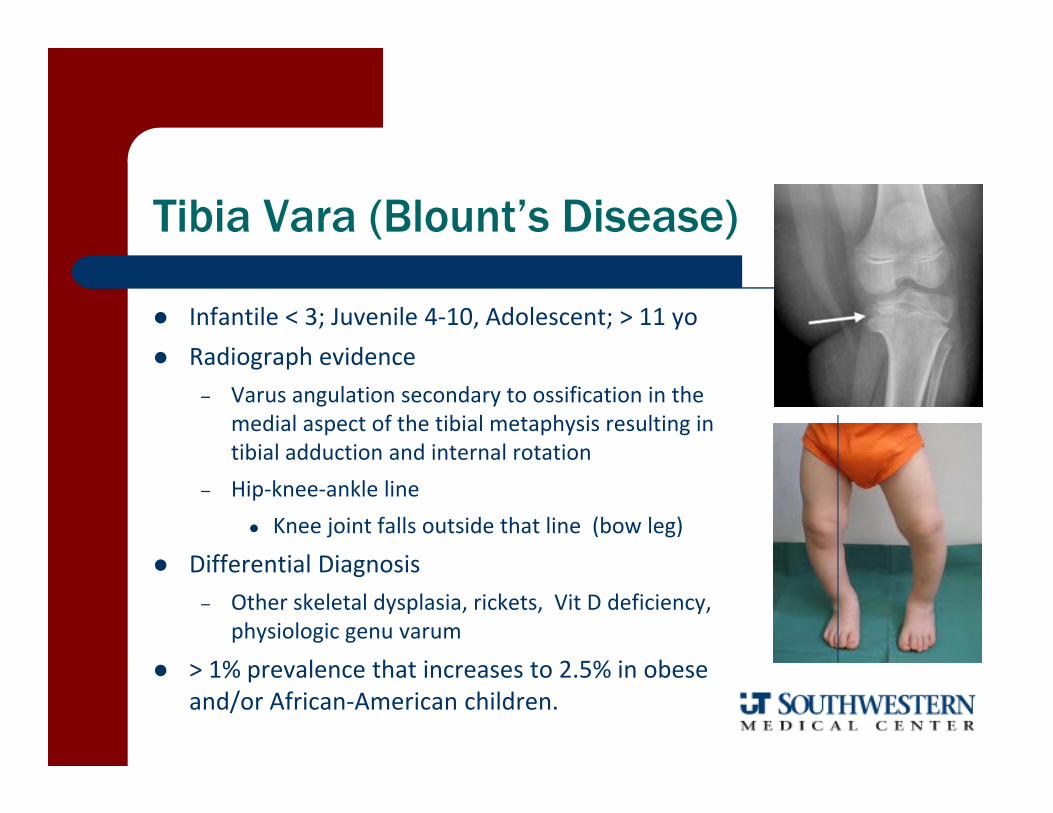
Infantile < 3; Juvenile 4‐10, Adolescent; > 11 yo Radiograph evidence
– Varus angulation secondary to ossification in the medial aspect of the tibial metaphysis resulting in tibial adduction and internal rotation
– Hip‐knee‐ankle line Knee joint falls outside that line (bow leg)
Differential Diagnosis– Other skeletal dysplasia, rickets, Vit D deficiency,
physiologic genu varum
> 1% prevalence that increases to 2.5% in obese and/or African‐American children.

Blount’s Disease Management
Bracing for infantile onset Surgery may be necessary for
failed bracing, delayed diagnosis, or marked deformity (> 13°)
Surgical Choices– Guided growth (hardware on
health side to allow injured side to catch up)
– Tibial Osteotomy
Talipes Equinovarus (Club Foot)
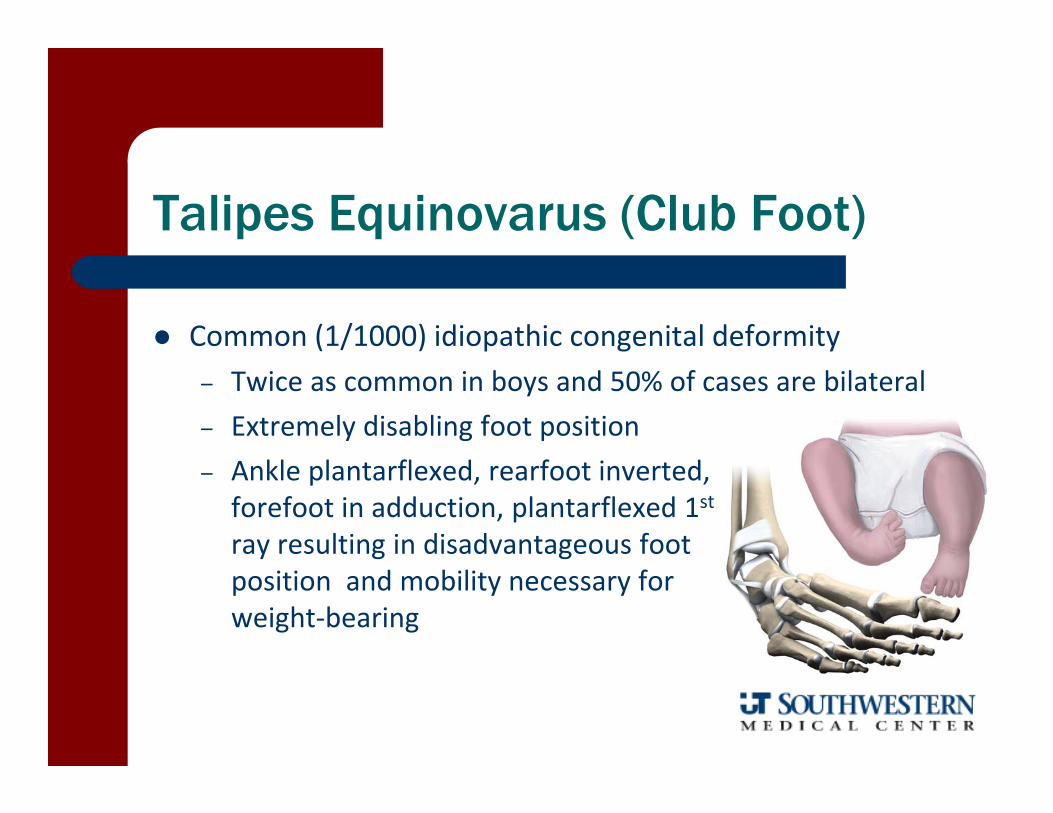
Common (1/1000) idiopathic congenital deformity – Twice as common in boys and 50% of cases are bilateral– Extremely disabling foot position– Ankle plantarflexed, rearfoot inverted, forefoot in adduction, plantarflexed 1stray resulting in disadvantageous foot position and mobility necessary for weight‐bearing
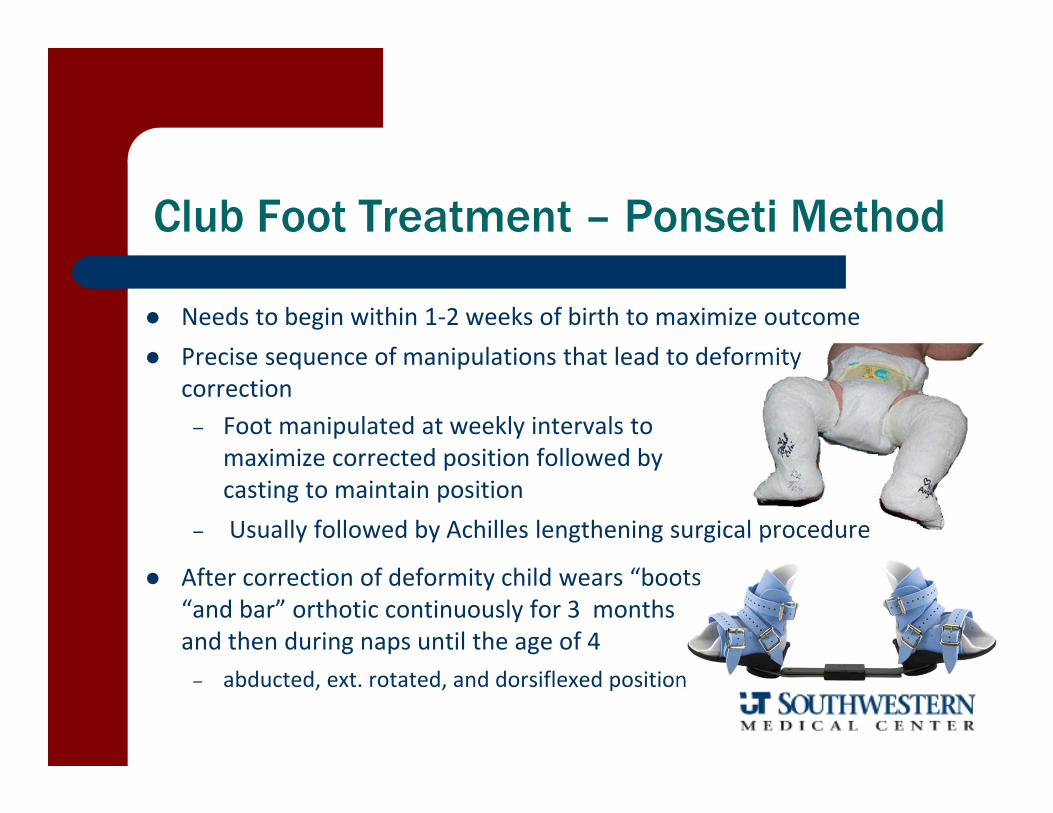
Club Foot Treatment – Ponseti Method
Needs to begin within 1‐2 weeks of birth to maximize outcome Precise sequence of manipulations that lead to deformity
correction– Foot manipulated at weekly intervals to
maximize corrected position followed by casting to maintain position
– Usually followed by Achilles lengthening surgical procedure
After correction of deformity child wears “boots “and bar” orthotic continuously for 3 months and then during naps until the age of 4– abducted, ext. rotated, and dorsiflexed position

Metatarsus Adductus
Forefoot curved medially with rearfoot in slight valgus position
Treatment– Mild (or flexible) – stretching, cast‐immobilization, and shoe
therapy (straight and/or reverse last)
– Severe (or structural) – manipulation; serial casting, and/or surgical correction
Surgical Correction includes rearfoot realignment, tendoachilles lengthening, and medial cuneiform opening/cuboid closing osteotomy

Scoliosis
3‐D deformity with > 10° deviation in coronal plane Idiopathic prevalence 1‐3% Three Types
– Congenital ‐ abnormally formed vertebrae– Syndromic – neuromuscular disorder– Idiopathic – unknown cause; most common variety with onset > 10 years old
Structural – Fixed, rotary component with trunk flexion– Named for location and direction – “C” or “S” curves
Non‐structural– Corrects with lateral bending and curve (postural scoliosis) not present in
forward bending
Right Thoracic
Left Lumbar

Adam’s Forward Bend Test
Scoliosis screening – assessment of rib prominence
Presence of LLD
Pelvis/Waist line obliquity
Shoulder/Scapular obliquity

Cobb Angle – Standing Radiograph

Scoliosis
Cobb Angle• < 25° ‐monitor• 25‐40° nonsurgical treatment• > 40° consider surgical intervention
Curve Progression• Healthy child unlikely to progress if curve is < 30° at maturity
• > 50° progresses even after growth is finished

Scoliosis Treatment
Goals:– Maintain (or halt) curvature progression– Address weakness and flexibility impairments
strengthen convex, stretch concave– Pain Management
Systematic review:– Effectiveness of bracing is controversial– Exercise therapy can retard curve progression
and offer improvement in impairments
Exercise Approaches
Schroth Method – intense in‐house multi‐discipline program consisting of active strengthening, auto‐
correction exercise, therapist facilitation, bracing, ADL counseling, and behavioral therapy
DoboMed – active 3‐D auto‐correction exercise in ‐CKC, rib mobilization and respiration training
Side Shift Program – self lateral shifts and tilt exercise combined with hitch exercise (lifting and holding
the limb on the convex side)
SEAS Program (Lyon Method) – auto‐elongation exercises with emphasis on deep spinal stabilization training,
behavioral modification, and family involvement
Fusco C, et al, Exercise Systematic Review, Physiother Theor Prac, 2011
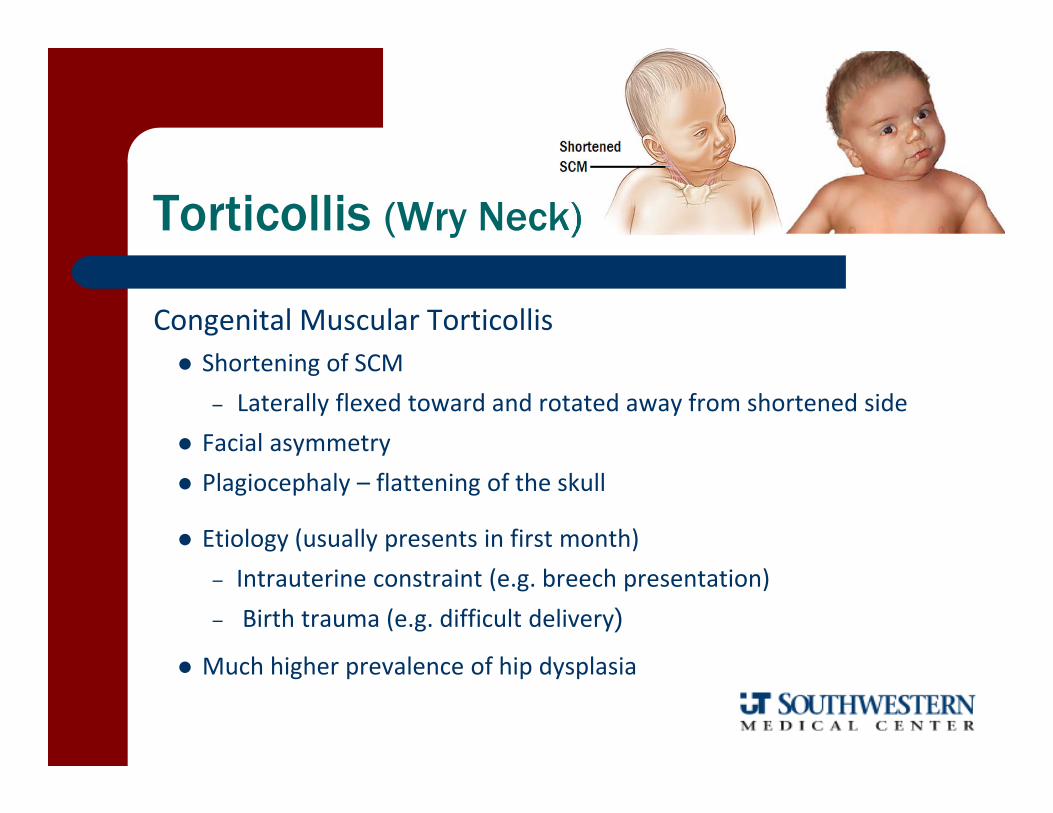
Torticollis (Wry Neck)
Congenital Muscular Torticollis Shortening of SCM
– Laterally flexed toward and rotated away from shortened side Facial asymmetry Plagiocephaly – flattening of the skull
Etiology (usually presents in first month)– Intrauterine constraint (e.g. breech presentation)– Birth trauma (e.g. difficult delivery)
Much higher prevalence of hip dysplasia
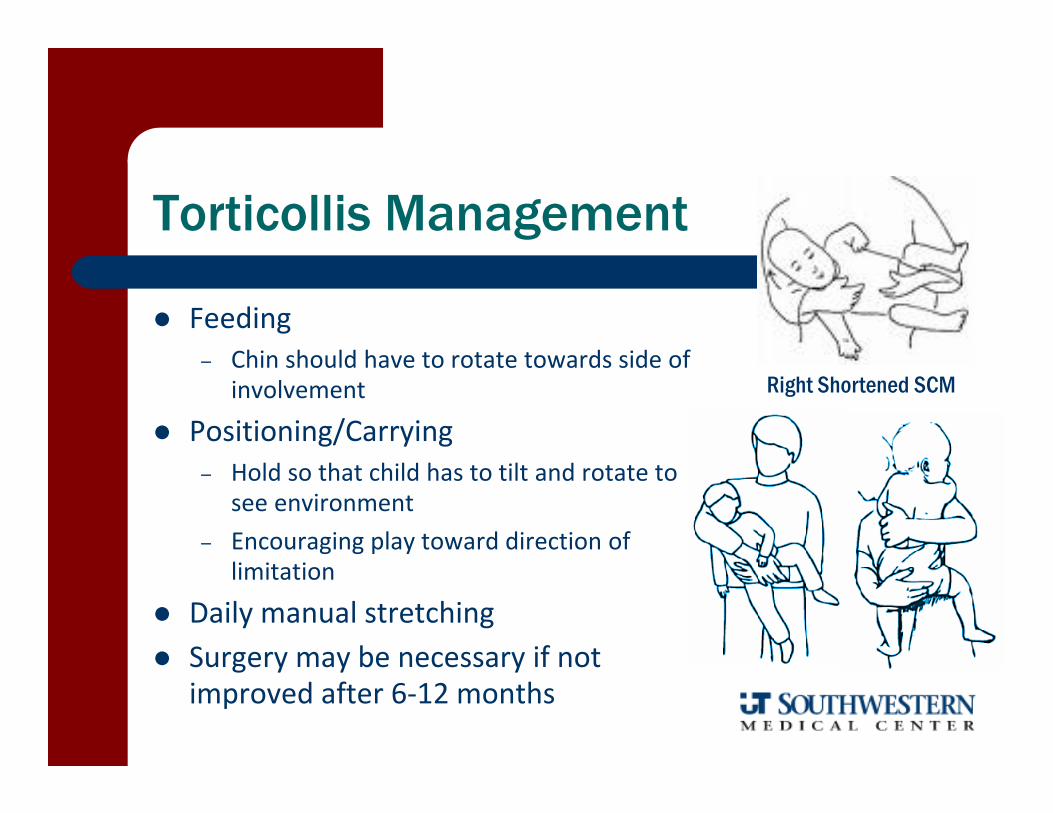
Torticollis Management
Feeding– Chin should have to rotate towards side of
involvement
Positioning/Carrying– Hold so that child has to tilt and rotate to
see environment– Encouraging play toward direction of
limitation
Daily manual stretching Surgery may be necessary if not
improved after 6‐12 months
Right Shortened SCM

Overuse Injuries
Pathogenesis– Natural process of healing is unable to keep up with breakdown of tissue
– If stress repeats before rebuilding and recovery – inflammatory response may occur
– Tissue progressively weakens and may fail

Factors Contributing to Overuse Injury
Factors contributing to overuse
Injuries
Condition of the Athlete Inadequate
Rest Poor Technique
Inappropriate Training
Previous Injury
Equipment
Playing Surface
Adult Peer Pressure
Maturity Level
Self-Esteem
Body Morphology
Muscle Imbalances
Anatomic Alignment
Inflexibility
Menstrual Status
Instability-Laxity
Growth Plate Status

Apophyseal Injury
Musculotendinous units pulling on developing insertional areas– Cause traction injury with bony change
Therapy typically starts after 2‐4 wks rest– Flexibility (pain free range)– Strengthening
Progression from concentric to eccentric – Slow, careful progression to prevent avulsion

Sites for Hip Apophysitis

Iliac Apophysitis
Mechanism of Injury– gradual onset of apophyseal in‐flammation at the ossification center of the growth plate 2ary to repetitive contractions by the oblique abdominals, gluteus medius, TFL, and hamstrings
– particularly common in adolescent runners, soccer players, or jumpers
ASIS
Lesser Trochanter
Ischial Tuberosity
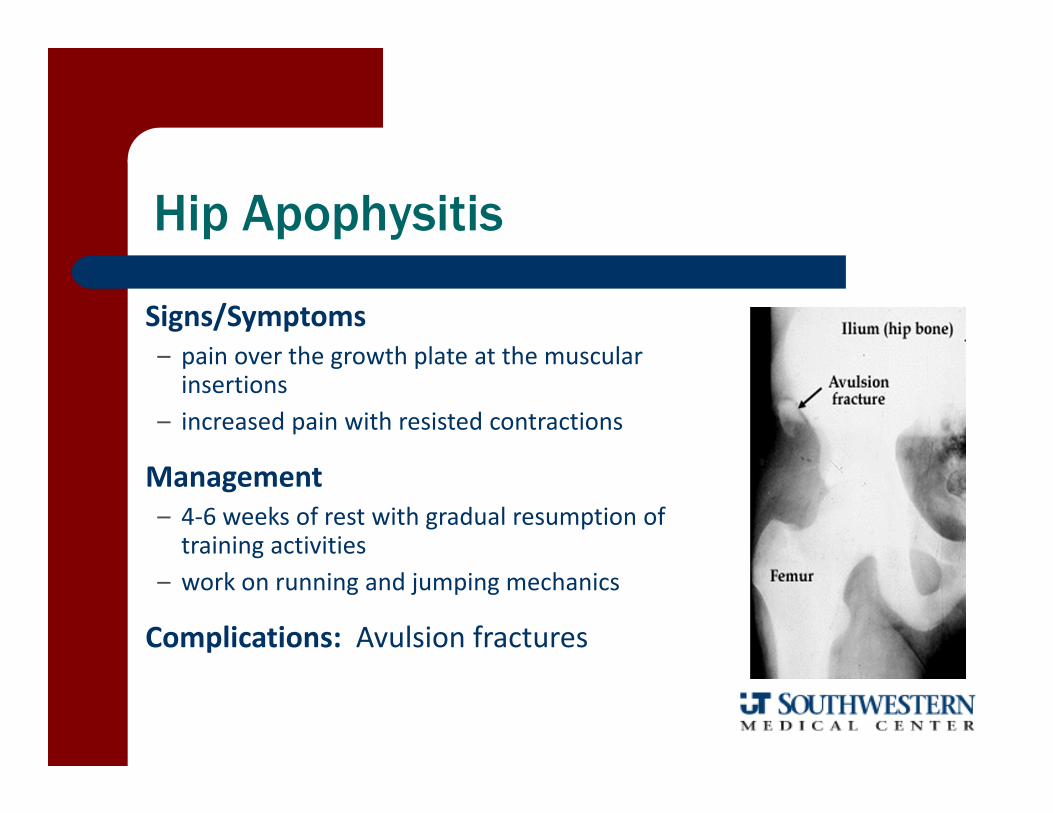
Signs/Symptoms– pain over the growth plate at the muscular insertions
– increased pain with resisted contractions
Management – 4‐6 weeks of rest with gradual resumption of training activities
– work on running and jumping mechanics
Complications: Avulsion fractures
Hip Apophysitis
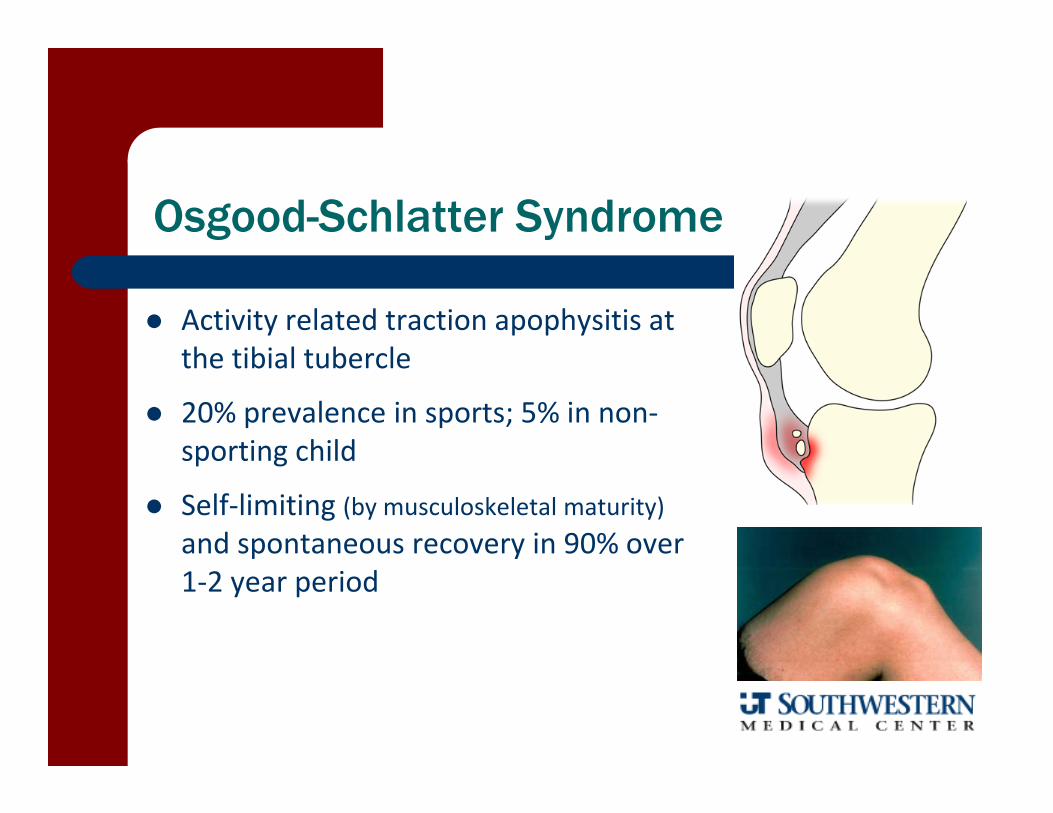
Osgood-Schlatter Syndrome
Activity related traction apophysitis at the tibial tubercle
20% prevalence in sports; 5% in non‐sporting child
Self‐limiting (by musculoskeletal maturity)and spontaneous recovery in 90% over 1‐2 year period
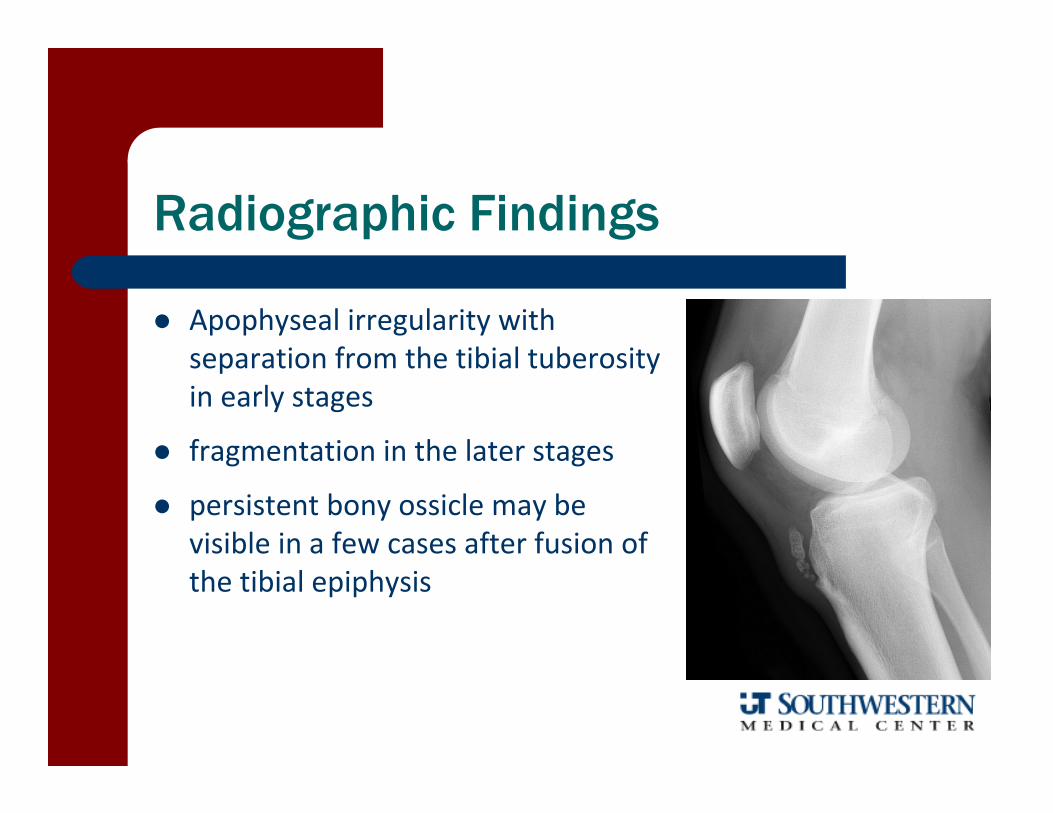
Radiographic Findings
Apophyseal irregularity with separation from the tibial tuberosity in early stages
fragmentation in the later stages
persistent bony ossicle may be visible in a few cases after fusion of the tibial epiphysis

Differential Diagnosis
Sinding – Larsen – Johansson Syndrome– traction apophysitis at inferior pole of patella
Hoffa Syndrome– fat pad syndrome
Tibial Tubercle Avulsion Fracture– Violent, forceful quad contraction (single event)
OS Signs/Symptoms
Pain/swelling at patellar tendon insertion Limited and painful quad activation Painful kneeling
Athletically active with increased plyometric load

Osgood-Schlatter Syndrome
Subacute Care– Quadricep and Hamstring stretching– Bubble pad with infrapatellar strap during activity– Quad isometrics and SLRs
Acute Care– Ice massage to tibial tubercle– Aspirin prn– Selective rest from irritating activities
avoid total immobilization minimize running/jumping activities
Sinding-Larsen-Johansson
Inferior pole of patella– Differentiate from OS via palpation
Similar presentation to Osgood‐Schlatter– Pain specific to inferior pole
Most common in 10‐12 y.o. males
Managed similar to OS

Sever’s Disease (Calcaneal Apophysitis)
tight Achilles tendon (particularly in the rapidly growing athlete) pulls on the calcaneal epiphyseal attachment producing a disruption of circulation and possible fragmentation of the calcaneus
common with cleated shoe wear or rapid alterations in the heel height of the athletic shoe– Ground reaction forces dissipated through
less surface area (contact area directly under cleated area more concentrated)

Sever’s Disease
SIGNS/SYMPTOMS– young athlete (8‐11yo)– pain on the posterior heel at the insertion
of the achilles tendon and positive heel squeeze test
– aggravated by activity and relieved by rest– Self‐limiting condition ends at skeletal
maturity when the growth plate closes
TREATMENT – judicious rest and the insertion of bilateral
heel lifts to alleviate injurious stresses– gastroc/Soleus stretching
Little League ElbowMedial Epicondyle Apophysitis
Traction apophysitis of medial epicondyle in adolescents from valgus overload
Graded according to severity of symptoms and degree of displace‐ment or avulsion
Throwing faults– Open up to soon (arm behind body)
– Excessive ER
Examination
Position(s) played, number of throws/week, and pitch type Palpation for area of tenderness Special Tests
– Valgus Stress Test at 30°– Moving Valgus Test– Milking Sign– Valgus Extension Overload
Elbow Flexor/Pronator Strength Axioscapular/Scapulohumeral Strength

Management
Minimum 4‐6 weeks rest Icing Flexor/Pronator Training Throwing biomechanics analysis Parental/Coach Education:
– For the average pitcher age 8 to 13 years, mastering the fastball and change‐up pitches alone will allow a thrower to remain highly competitive

What do you see?
Classic radiographic signs are physeal widening on standard AP X‐rays, lateral fragmentation or calcification, sclerosis, demineralization, and cystic changeAnton C, Pediatr Radiol, 2010
Would it help to know this is 13 year-old boy who plays baseball
Widening of the proximal humeral physis on the right while normal physis on the left

Little League Shoulder Proximal Humeral Epiphysiolysis
epiphysiolysis is thought to resemble that of a stress fracture or Salter–Harris type‐I injury (growth plate separation)

Most common in high performance pitchers from ages 11‐16
Caused by large rotational torque and poor throwing mechanics
Palpation tenderness at proximal/lateral humerus that is aggravated by throwing
GIRD is usually present (GHL IR ROM Deficit)
Little League Shoulder Proximal Humeral Epiphysiolysis

Little League Shoulder
Rehab– Provide early rest (6‐12 wks duration)– Scapular stabilization training– Progress to isotonic RC strengthening– Implement proprioceptive techniques– Must complete pain‐free interval throwing program prior to
return 90% are asymptomatic after 3 months of rest
Carson WG, Am J Sports Med, 1998

What is the critical intervention strategy?

Protect the Young Throwing Athlete
Watch and respond to signs of fatigue 4 months/year off Adhere to pitch count limits and days rest
recommendations (nexttwoslides) Avoid pitching on multiple teams with overlapping seasons Avoid using radar guns Learn good throwing mechanics emphasizing fast balls and
change‐ups A pitcher should not also be a catcher for his team If a pitcher complains of pain – get an evaluation from a
sports medicine physician Inspire fun and encourage multiple‐sport
participation

Daily Limits on Number of Pitches
Age 2006 USA Baseball Guidelines 2010 Little League Baseball Regulations
17‐18 NA 105/day
15‐16 NA
13‐14 75/game 95/day
11‐12 75/game 85/day
9‐10 50/game 75/day
7‐8 NA 50/day

Guidelines for Pitch Volume and Rest
Age 2006 USA Baseball Guidelines 2010 Little League Baseball Regulations
13‐14 125/wk ‐ 1000/season ‐ 3000/yr
11‐12 100/wk ‐ 1000/season ‐ 3000/yr
9‐10 75/wk ‐ 1000/season ‐ 2000/yr
All ages21‐35 pitches 1 day rest36‐50 pitches 2 days rest51‐65 pitches 3 days/rest66+ pitches 4 days/rest
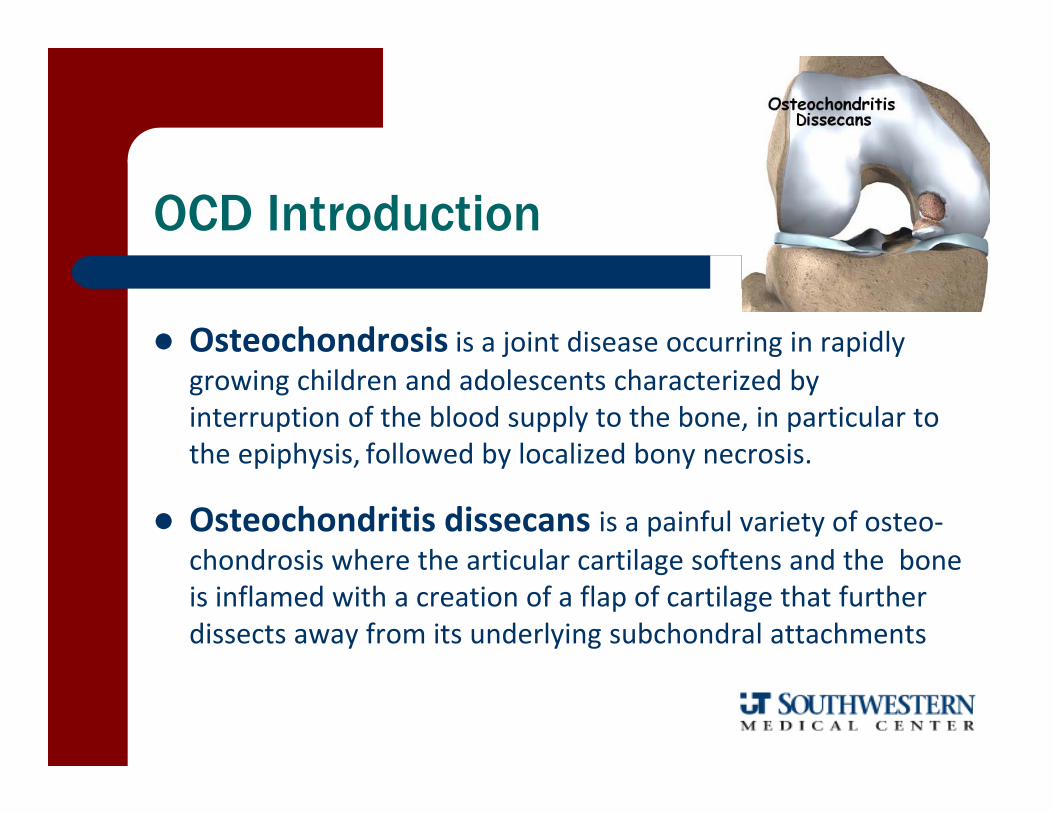
OCD Introduction
Osteochondrosis is a joint disease occurring in rapidly growing children and adolescents characterized by interruption of the blood supply to the bone, in particular to the epiphysis, followed by localized bony necrosis.
Osteochondritis dissecans is a painful variety of osteo‐chondrosis where the articular cartilage softens and the bone is inflamed with a creation of a flap of cartilage that further dissects away from its underlying subchondral attachments

OCD
Location1. Knee: most commonly affected;
intercondylar region of MFC2. Elbow: capitellum of baseball pitchers3. Talus: athletic teenagers, especially males
Signs/Symptoms– Joint effusion, pain– Knee pathology: antalgic gait or “locking”
due to loose body

Knee OCD
Wilson’s Test– IR leg and extend knee from full flex, repeat with ER– (+) when IR is painful and ER is not
Treatment– Non‐displaced, mild/moderate cases
Short period of immobilization; quad strengthening, and gradual return to activity
– Loose fragments/skeletally mature adolescent Fragment < 5 mm: simple excision Fragment > 5mm: internal fixation
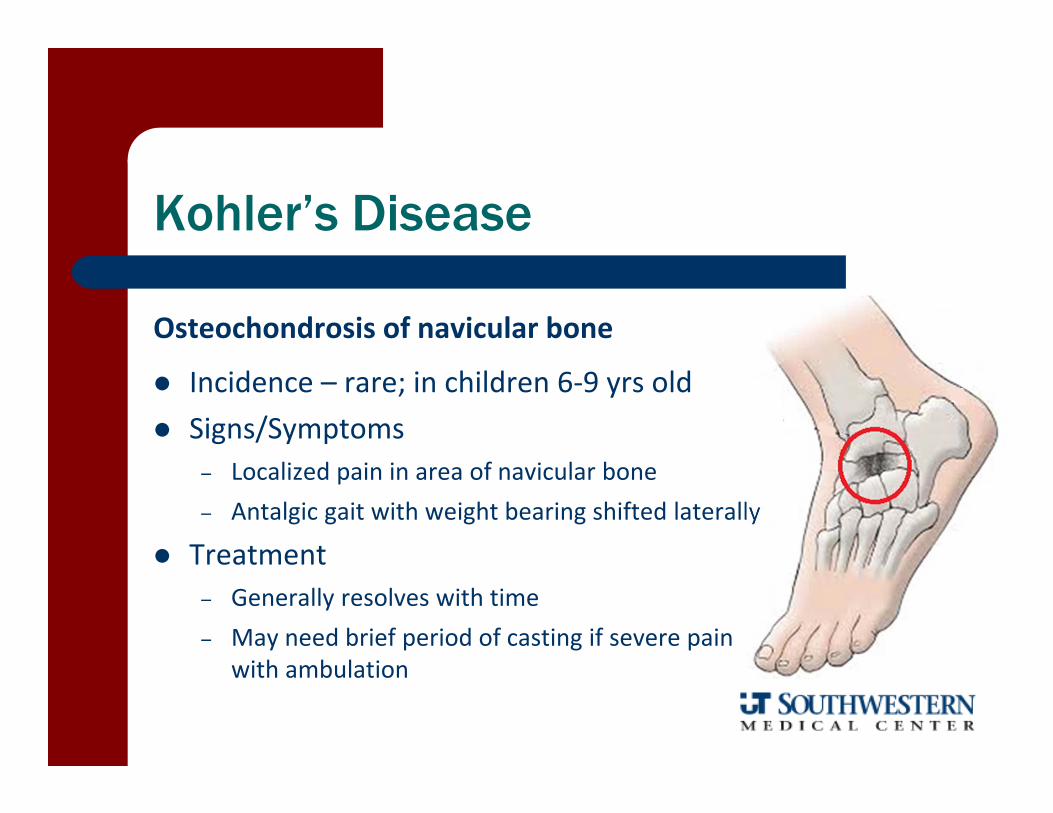
Kohler’s Disease
Osteochondrosis of navicular bone
Incidence – rare; in children 6‐9 yrs old Signs/Symptoms
– Localized pain in area of navicular bone– Antalgic gait with weight bearing shifted laterally
Treatment– Generally resolves with time– May need brief period of casting if severe pain
with ambulation
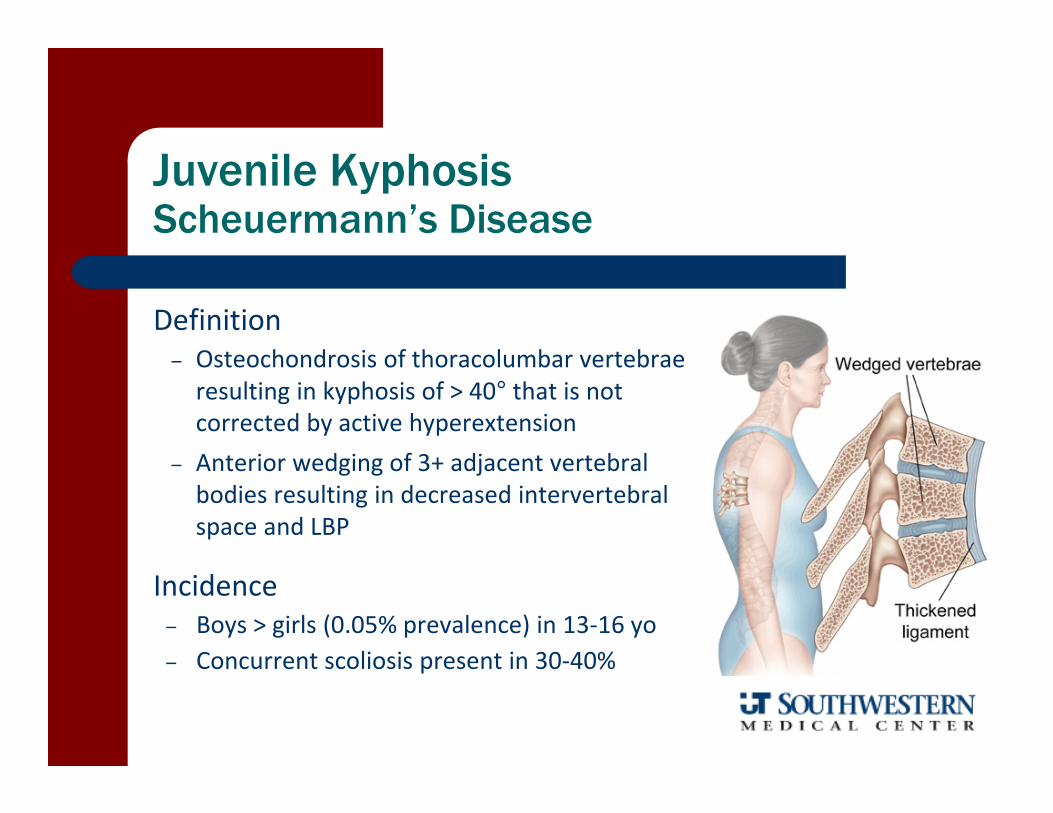
Juvenile KyphosisScheuermann’s Disease
Definition– Osteochondrosis of thoracolumbar vertebrae resulting in kyphosis of > 40° that is not corrected by active hyperextension
– Anterior wedging of 3+ adjacent vertebral bodies resulting in decreased intervertebral space and LBP
Incidence– Boys > girls (0.05% prevalence) in 13‐16 yo– Concurrent scoliosis present in 30‐40%
Juvenile KyphosisScheuermann’s Disease Treatment
Trunk extensor strengthening
Thoracolumbar passive trunk extension stretching
Core training of deep postural muscles and gluteals
LE stretching (hamstrings)
Orthotic bracing and/or surgery in more severe cases

Broken Bones
Pediatric Fractures are Unique
Immature Bone
– Thick fibrous periosteum is strong and not easily torn at time of injury
Ligaments are often stronger than growth plates
– Physeal (growth plate) fracture is more common than ligament sprains or joint dislocations

Pediatric Fractures are Unique
Fractures heal more rapidly (than in adults)
– Ex: adult femoral shaft fracture takes 5 mo. to heal while it takes 3 wks in newborn
– Non‐union fractures are rare in children
– Significant remodeling can occur at fracture site allowing some malunion deformities to correct spontaneously
– Complications include osteomyelitis or growth disruption

Saltar-Harris Fracture Scale
Type Description
I Follows course along physis
II Runs along physis and through metaphysis
III Runs along physis and through epiphysis
IV Travels through metaphysis and epiphysis, transecting physis
V Crush fracture

Salter-Harris Physeal Fracture Mnemonic
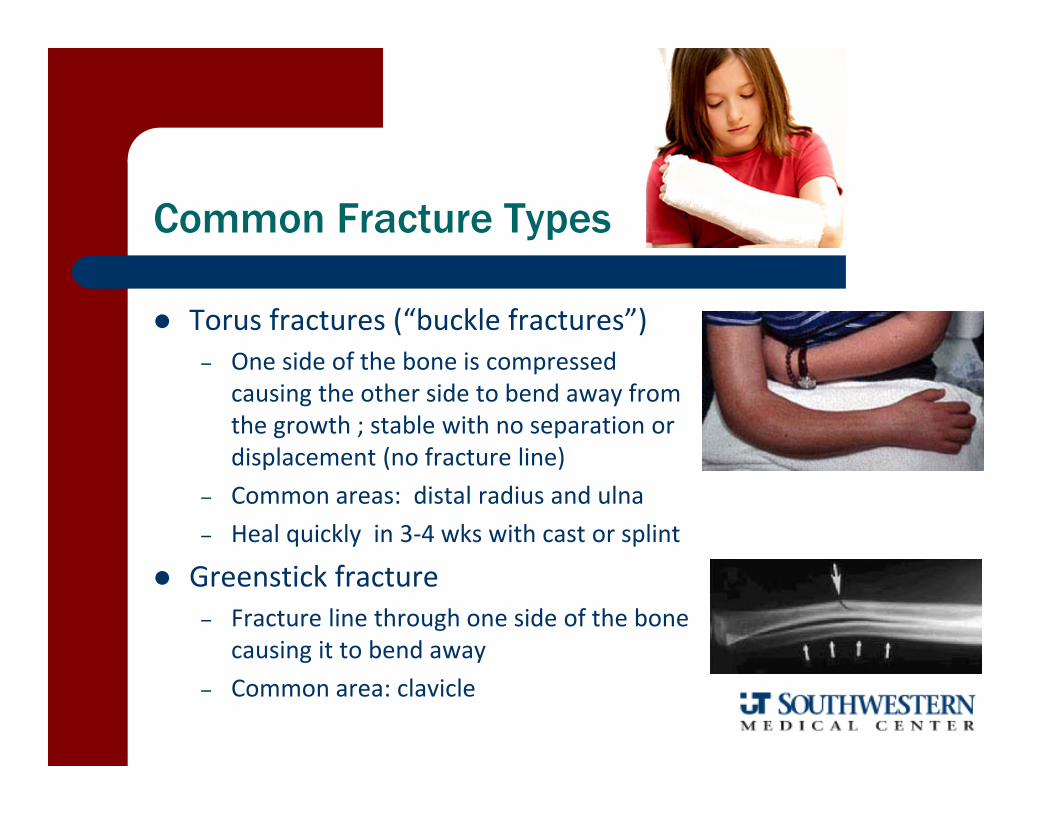
Common Fracture Types
Torus fractures (“buckle fractures”)– One side of the bone is compressed
causing the other side to bend away from the growth ; stable with no separation or displacement (no fracture line)
– Common areas: distal radius and ulna– Heal quickly in 3‐4 wks with cast or splint
Greenstick fracture– Fracture line through one side of the bone
causing it to bend away– Common area: clavicle
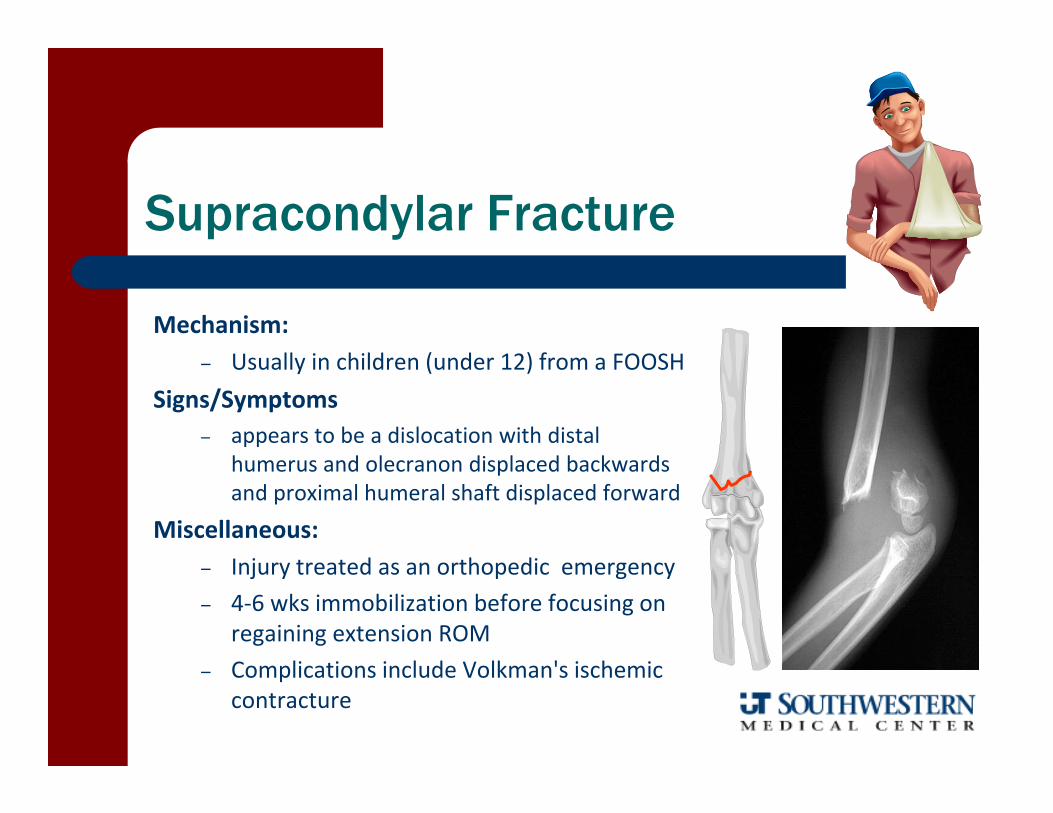
Supracondylar Fracture
Mechanism:– Usually in children (under 12) from a FOOSH
Signs/Symptoms– appears to be a dislocation with distal
humerus and olecranon displaced backwards and proximal humeral shaft displaced forward
Miscellaneous: – Injury treated as an orthopedic emergency– 4‐6 wks immobilization before focusing on
regaining extension ROM– Complications include Volkman's ischemic
contracture
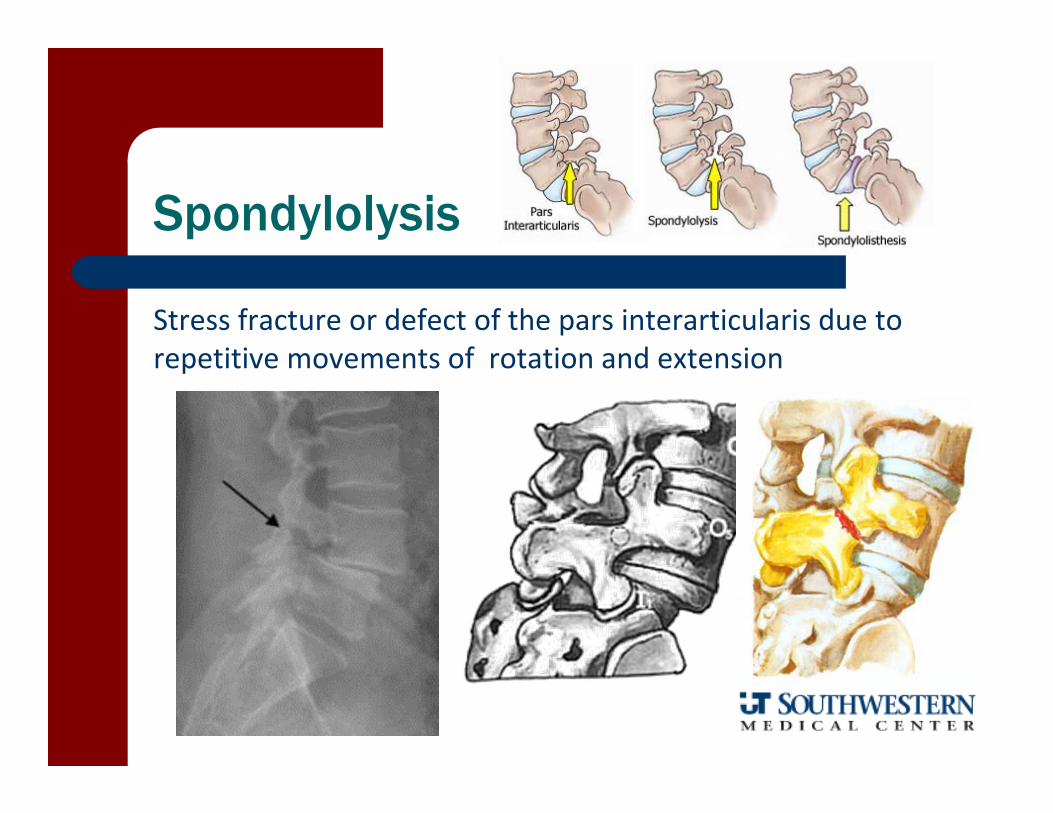
Spondylolysis
Stress fracture or defect of the pars interarticularis due torepetitive movements of rotation and extension

Spondylolisthesis
Forward slip of vertebrae
– Grade I 25% slippage
– Grade II 25‐50% slippage
– Grade III 50‐75% slippage
– Grade IV > 75% slippage

Spondy Signs/Symptoms
Insidious onset of unilateral low back pain
Pain with active movement testing – extension— Accentuated with hyperextension and ipsilateral
rotation in single limb stance
Hyperlordotic posture with possible step off sign– Tight hamstrings– Short torso with flat buttocks– Rib cage appears low and iliac crests high– Vertical sacrum; lacking full hip extension

Athletic Populations at Risk for Spondy
Activities that require or have emphasis on repetitive lumbar hyperextension Gymnasts (43% elite; 63% Olympic) Football Offensive Lineman Divers Pole Vaulters Weight Lifters Wrestlers Dancers High Jumpers Swimmers (butterfly)

Spondy Treatment Principles
• In absence of neurologic symptoms, Grade I & II respond well to conservative interventions
• Restriction from aggravating activities• Non‐rotational hyperextension or axial loading
movements
• Thoracolumbosacral bracing to limit or prevent lumbar extension (physician preference)
• Anti‐lordotic postural training: • Core/Abdominal strengthening • Hamstring /Hip Flexor stretching
Spondy Prognosis
Bony Union— 29% patients with bilateral spondy healed completely— 100% patients with unilateral healed completely (Sys et al, Eur Spine J, 2001)
Return to full activity at about 4 months
If resolution of symptoms does not occur, surgery indicated — usually wait 9‐12 months before recommendation for surgery
III and IV may require surgery (particularly if athlete is still growing)— posterior lateral fusion(most common)— decompressive laminectomies (more severe slips)— 82% post op were able to return to sport (Debnath et al, JBJS, 2003)
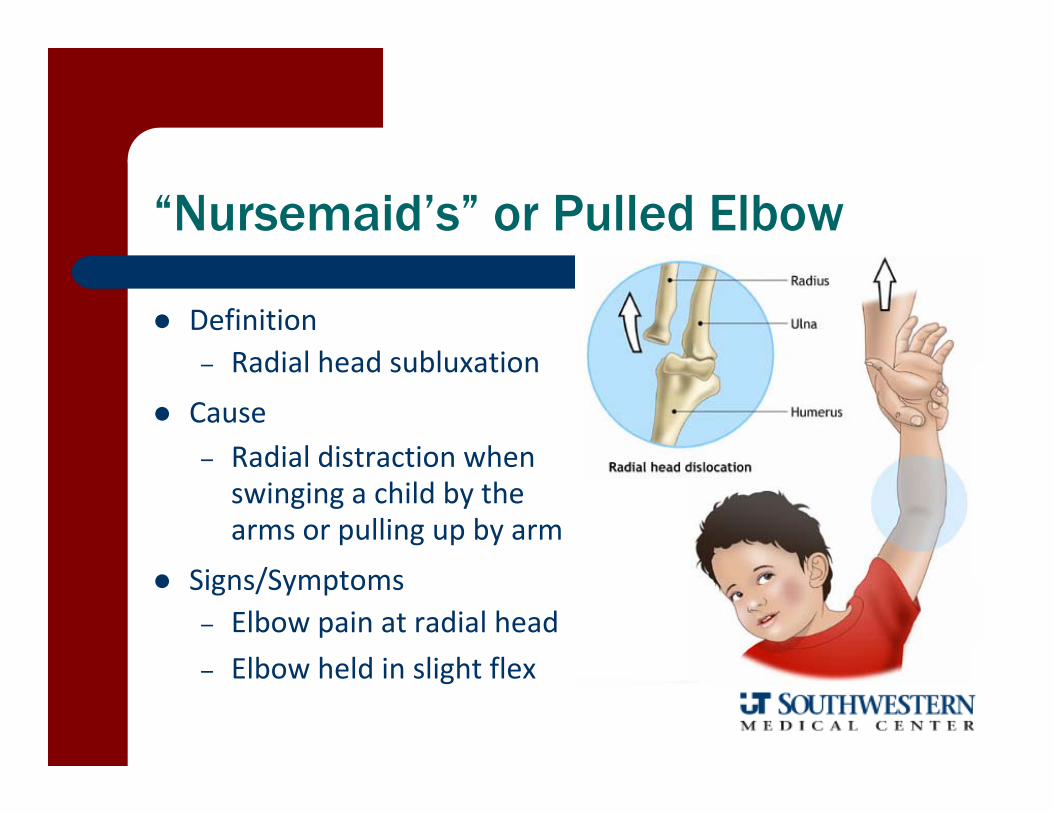
“Nursemaid’s” or Pulled Elbow
Definition– Radial head subluxation
Cause– Radial distraction when swinging a child by the arms or pulling up by arm
Signs/Symptoms– Elbow pain at radial head– Elbow held in slight flex
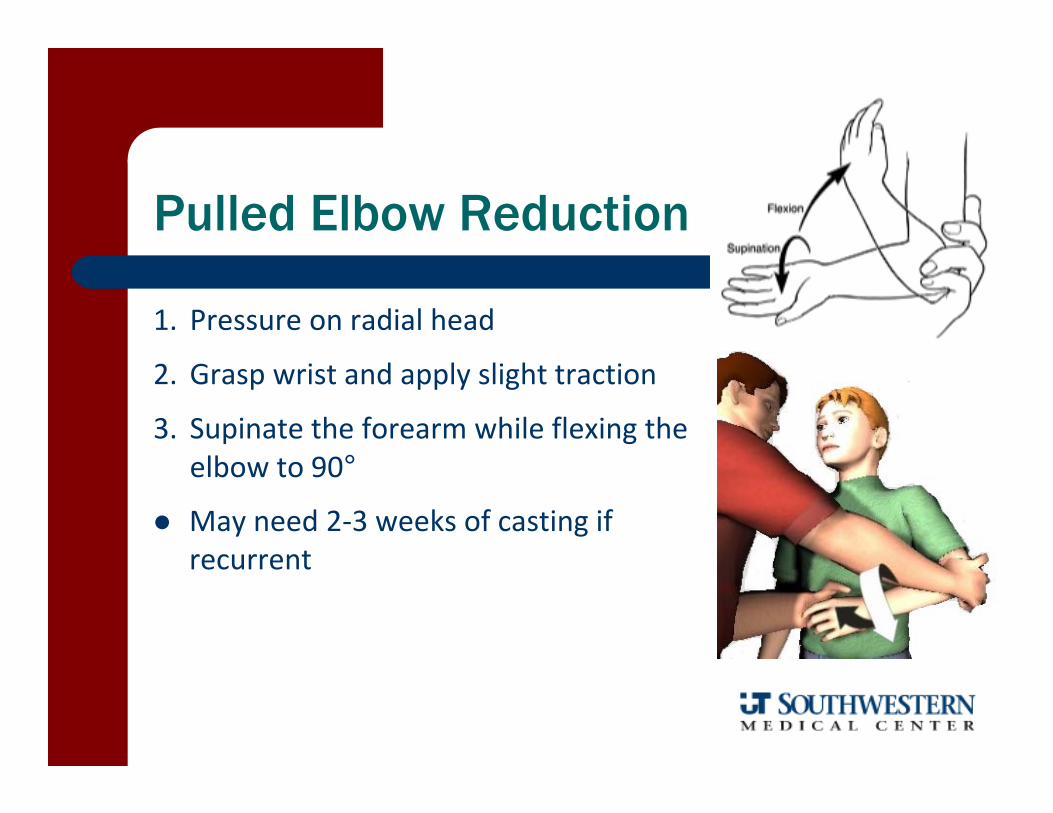
1. Pressure on radial head
2. Grasp wrist and apply slight traction
3. Supinate the forearm while flexing the elbow to 90°
May need 2‐3 weeks of casting if recurrent
Pulled Elbow Reduction

Adolescent ACL Injuries
The risk of surgical management to prevent further joint deterioration in the young athlete probably outweighs the concern for growth plate arrest from drilling the surgical tunnels for graft passage
Additionally, we have good retrospective data that indicates that bracing and activity modification have a poor likelihood of allowing returning to pre‐injury activity levels
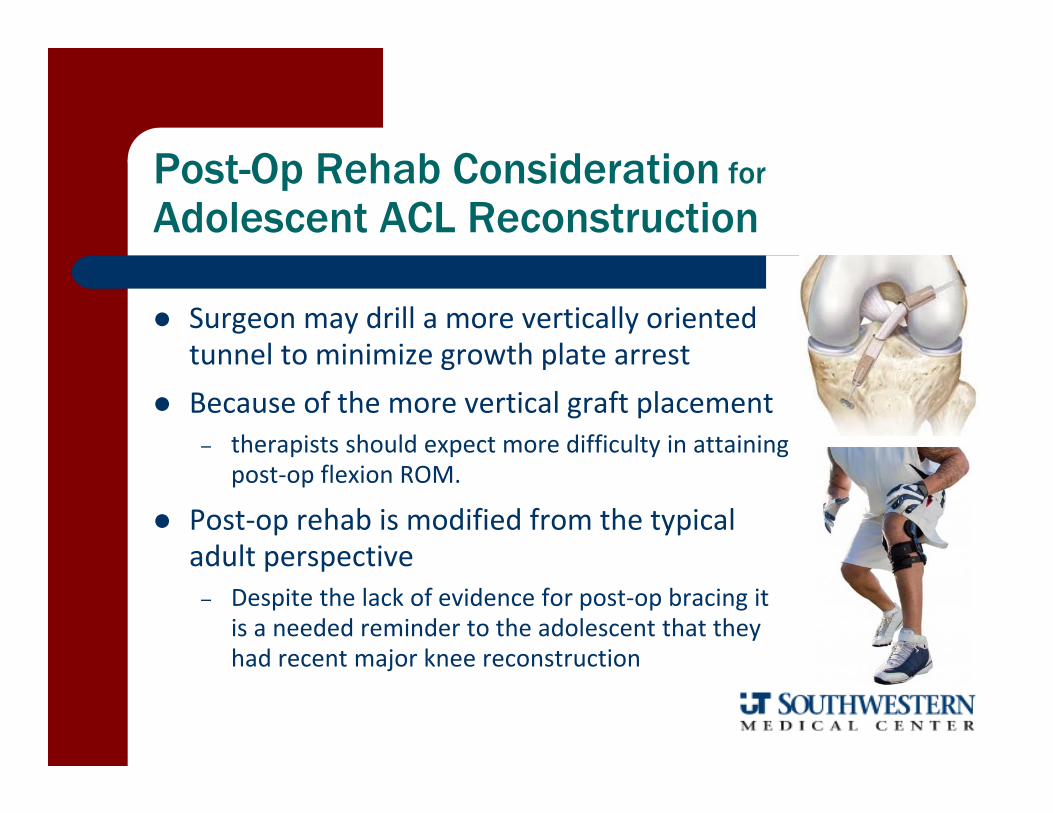
Post-Op Rehab Consideration for
Adolescent ACL Reconstruction
Surgeon may drill a more vertically oriented tunnel to minimize growth plate arrest
Because of the more vertical graft placement– therapists should expect more difficulty in attaining
post‐op flexion ROM.
Post‐op rehab is modified from the typical adult perspective – Despite the lack of evidence for post‐op bracing it
is a needed reminder to the adolescent that they had recent major knee reconstruction
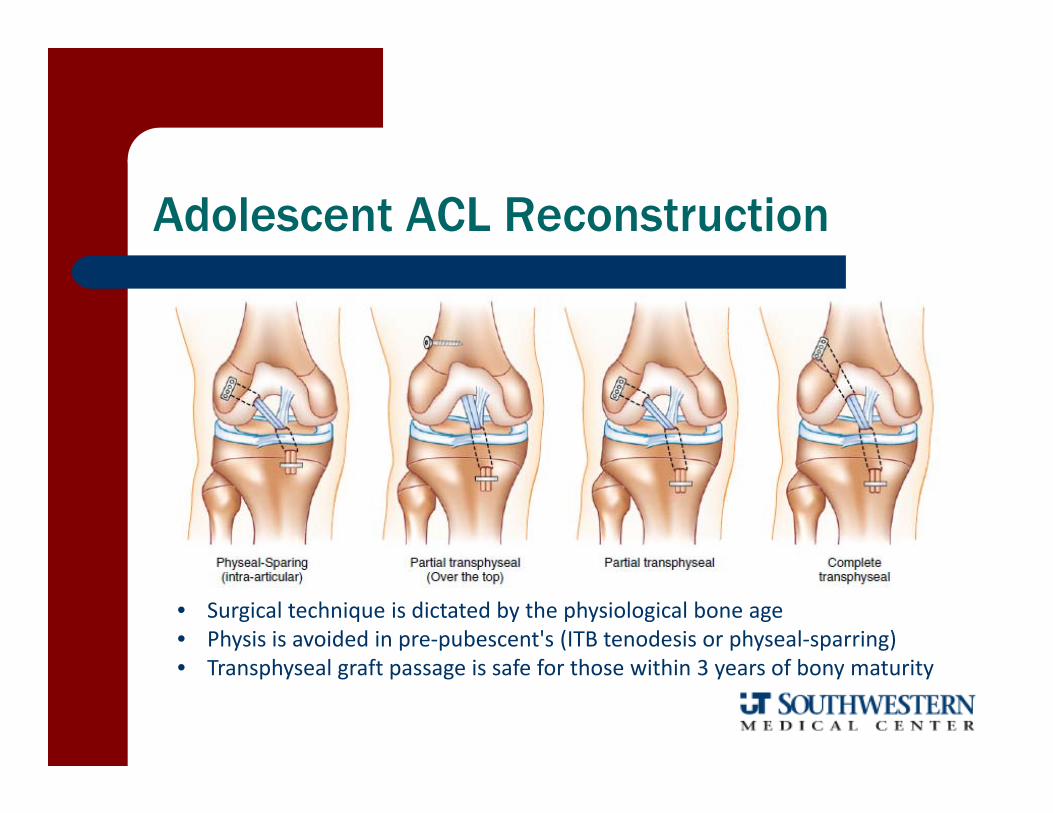
Adolescent ACL Reconstruction
• Surgical technique is dictated by the physiological bone age • Physis is avoided in pre‐pubescent's (ITB tenodesis or physeal‐sparring) • Transphyseal graft passage is safe for those within 3 years of bony maturity
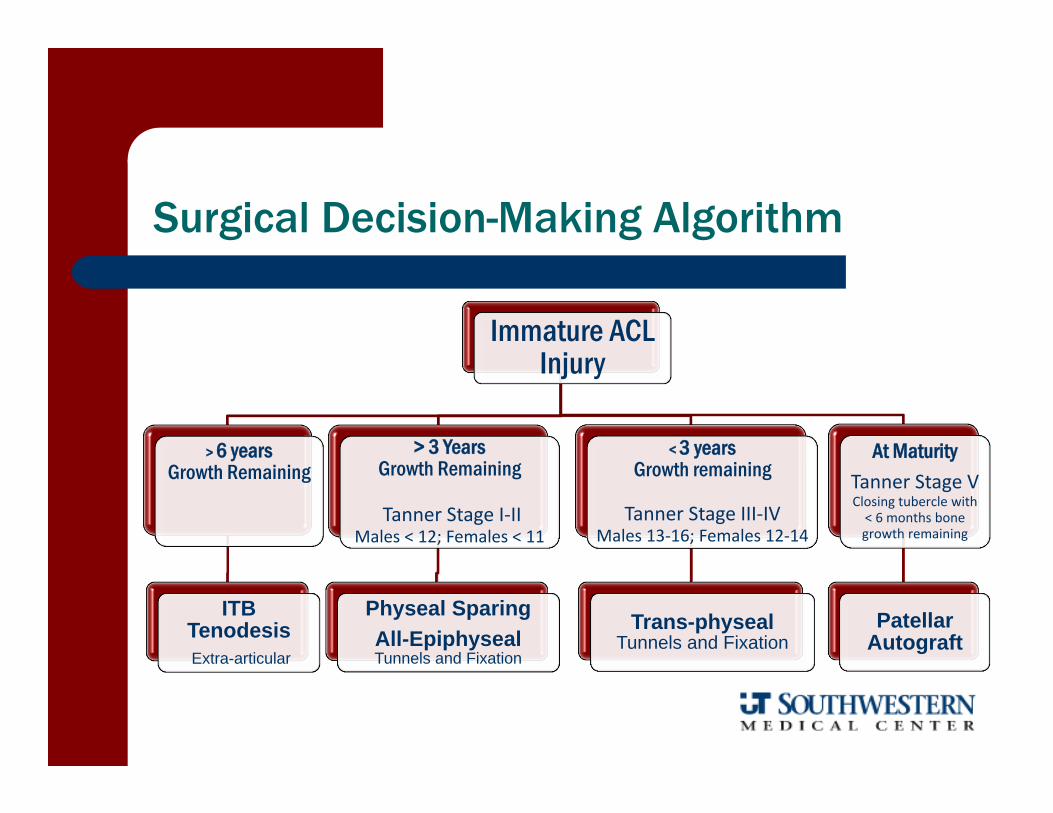
Immature ACL Injury
> 6 years Growth Remaining
ITB TenodesisExtra-articular
> 3 Years Growth Remaining
Tanner Stage I‐IIMales < 12; Females < 11
Physeal SparingAll-EpiphysealTunnels and Fixation
< 3 years Growth remaining
Tanner Stage III‐IVMales 13‐16; Females 12‐14
Trans-physealTunnels and Fixation
At MaturityTanner Stage VClosing tubercle with < 6 months bone growth remaining
Patellar Autograft
Surgical Decision-Making Algorithm
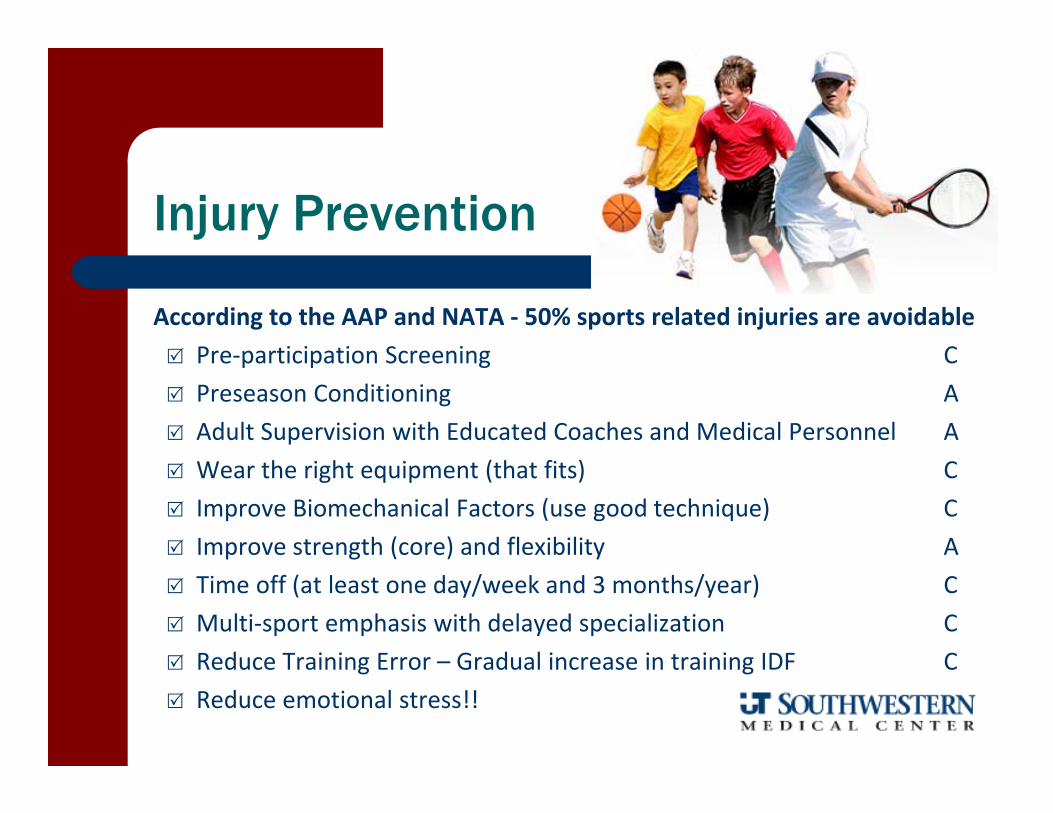
Injury Prevention
According to the AAP and NATA ‐ 50% sports related injuries are avoidable Pre‐participation Screening C Preseason Conditioning A Adult Supervision with Educated Coaches and Medical Personnel A Wear the right equipment (that fits) C Improve Biomechanical Factors (use good technique) C Improve strength (core) and flexibility A Time off (at least one day/week and 3 months/year) C Multi‐sport emphasis with delayed specialization C Reduce Training Error – Gradual increase in training IDF C Reduce emotional stress!!
Excellent Resource
Journal of Athletic Training 2011;46(2):206‐220

The Right Focus
Not — did you win?— did you play well?— did you do your best? ….
but
Did you have fun!

Why youth sports are “good”
You learn how to compete You learn how accept criticism You learn how be a teammate You learn how to be healthy You learn how to win …
and you learn how to lose

www.stopsportsinjuries.com
The Sports Trauma andOveruse Prevention sports Injuries campaign was initiated by the AOSSM in early 2007
Excellent resources for coaches, parents, athletes and health care providers


















