87
Pediatric Stroke and Vascular Service CME Course. September 7 th , 2017 ERIC GRABOWSKI FERDINANDO BUONANNO PATRICIA L. MUSOLINO MASSACHUSETTS GENERAL HOSPITAL HARVARD MEDICAL SCHOOL

PediatricStrokeandVascularServiceCMECourse.September7th,2017ERICGRABOWSKIFERDINANDO BUONANNO
PATRICIAL. MUSOLINOMASSACHUSETTS GENERAL HOSP ITAL HARVARD MEDICAL SCHOOL

Drs.Grabowski,Buonanno andMusolinohavenofinancialdisclosures

PediatricStrokeandVascularService

PediatricStrokeTeamatMGHRapid,coordinatedresponsetothemanagementofpediatricstrokecases.
Long-termfollow-upcareforthesepatients.
Resourcesforfamiliesandpatients§www.massgeneral.org/children/services/treatmentprograms.aspx?id=1628

WhyaPediatricStrokeServiceisImportanttoPediatriciansIncreasedrecognitionofafrequentlyunsuspected,orevenmisdiagnosed,conditioninpediatrics.
Efficacyofanti-thrombotictherapyintheolderchild.
Majorroleforthrombophiliaintheolderchild,vs. atherosclerosis,diabetes,hypotension,andlipidsinolderpatients.
Amultidisciplinaryteamapproachprovidestheneededexpertiseandtoolstodiagnoseandmanagepediatricstrokeeffectively.
Apediatricstrokespecialistcanappreciatethedistinctnessofstrokeinthenewborn,vs. theolderchild,vs. thechildwithsicklecelldisease.

AcutePediatricStroke-statisticsPrevalence:11-24/100,000(comparabletostrokeincidenceinyoungadults)
Incidence:3/100,000/yr,vs. 65/100,000/yr inadults
AtMGH,consistentwiththeabove,25pediatricand800+adultstrokeswereevaluatedandmanagedin2016.

InternationalPediatricStrokeStudyCenters60Centers,5151ChildrenEnrolled(9/2016)

CerebrovasculardiseaseinchildrendiffersfromthatinadultsMoredifficulttodiagnoseRiskfactorsaredifferentLesserdegreesofresidualdysfunctioninsomeRehabilitationpotentialandchallengesaredifferentMultidisciplinarycareisalwaysneeded

DifferentStrokeManifestationsAdultsandolderchildren
§ acutefocaldeficitinarterialterritory
Neonates§ Seizures;apnea;autonomicinstability§ Hypotonia;abnormalreflexes§ Lethargy;encephalopathy§ Earlyhandedness(<18mos);developmentaldelay(CP)§ None(untilage2-3months,orserendipitousfindinguponCNSimaginginlaterlife)

CategoriesofRiskFactorsPlasma-phasebasedriskfactors
Structuralfactors
Familyhistoryandhereditaryconditions
Co-morbidconditions(andtriggers)
Maternal,LaborandDelivery,forperinatalstroke
Sickle-celldisease

ImpactofThrombophiliaonAISorCSVTinChildrenEvaluationofallstudiesofpediatricstrokeand/orCSVTfrom1970to2009(185publications)
22ofthesesatisfiedcriteriaforinclusioninameta-analysistoestimateoddsratiosandconfidenceintervals
1526childrenwithAIS,238withCSVTvs.2799Controls
MGHwasoneof28centersworldwidewhichcontributedtothestudy
Kenet etal,2010

Riskfactor Pts/controls OddsratioProteinCdef 844/1207 11.0(5.1-23.6)
APA/LA 930/1194 7.0(3.7-13.1)
Lipoprotein(a) 616/578 6.5(4.5-9.6)
FVG1691A1014/2581 3.7(2.8-4.9)
FIIG20210A1059/2278 2.6(1.7-4.1)
MTHFRTT 777/1715 1.6(1.2-2.1)
≥2genetictraits701/1265 18.8(6.5-54.1)
ImpactofThrombophiliaonAISorCSVTinChildren
Kenet etal,2010

ImpactofThrombophiliaonthrombo-embolisminChildren(moregenerally)
Evaluationofallstudiesofpediatricthrombo-embolismfrom1970to2007(50publications)
35ofthesesatisfiedcriteriaforinclusioninameta-analysistoestimateoddsratiosandconfidenceintervals
2653childrenwiththrombo-embolicevents(PE,DVT,AIS,CSVT)vs.1979controls
MGHwasoneof23centersworldwidewhichcontributedtothestudy
Youngetal,2008
PediatricStroke-NeonatalandInfantPerinataldepression
§ HIE,ECMO,Sepsis,meningitis§ CongenitalHeartDisease
Dehydration,hypernatremia
Coagulopathy§ Prothrombotic (DIC,APLA,polycythemia)§ Bleedingdiatheses(vW disease,hemophilia,NAIT,severeliverdisease)
Metabolic(organicacidemias,mitochondrialdisorders)
Maternal(pre-eclampsia,diabetes,PROM,cocaine)
Placental(chorioammionitis,abruption,thrombosis)

PerinatalStrokeandPlacenta
CourtesyofNeuroplacentology StudyGroup
PediatricStroke-OlderChild(1-13y.o.)Congenitalheartdisease,mitralvalveprolapse,ECMO
PFOwithrighttoleftshunt
Coagulopathy
Infectious§ rheumaticheartdisease,endocarditis,meningitis,mastoiditis
Canceranditstreatment(lymphoreticular,ProML,ALL,gliomas,s/pXRT,chemo)
Autoimmunediseases(esp.SLE,PAN,Takayasu)
Metabolic(MELAS,Kearns-Sayre,Fabry’s,homocystinuria)
Vasculopathies(HHT,Ehlers-Danlos,NF,Down’s,moya-moya)

Pediatricstroke-AdolescenceSameasforages1-13,plus:§FMD§Dissections§Trauma(EDH,SDH,SAH,IPH,IVH)§OCPs,pregnancy§Cocaine,otherdrugs

Stroke- DiagnosticworkupDiagnosticevaluation§ HeadUS(maymisssuperficialandischemiclesions)§ CTheadtoruleouthemorrhageifthrombolytictherapyisbeingconsidered§ RapidMRI,MRAandMRVtoestablishtypeofstrokeandvesselanatomy§ CTAtoidentifydissectionsandprimaryvascularanomalies
MetabolicandHematologicalEvaluation
Geneticsasindicated

CARASIL-Cerebralautosomalrecessivearteriopathy withleukoencephalopathyandstroke(HTRA)
CADASIL-Cerebralautosomaldominant
arteriopathy withleukoencephalopathyand
stroke(NOTCH3)Loeys-DietzSyndrome(TGFBR1-TGFBR2-SMAD3-TGFB2)Hereditaryangiopathy withnephropathy,aneurysmsandmusclecramps(COL4A1,COL4A2)Marfans Syndrome(FBN1)
MonogeneticVascularDiseasesaremorefrequentinpediatricstroke
Fabry disease(GLA)Rendu-Osler-WeberSyndrome(HHT-ENG)Hereditaryendotheliopathy withretinopathy,nephropathyandstroke(TREX1)
Arteriopathy (ACTA2)Arteriopathy (MYLK)
Aicardi–Goutieressyndrome(SAMHD1)
ADA2(CECR1)MoyaMoya(RNF213)

Stroke- AcuteManagementClinicaldiagnosis,acutestabilization
§ (e.g.O2;BP;controlseizures),andtriage
Diagnosticimaging
Studiesforthrombophilia
Anticoagulation/Clottingfactorreplacement
Follow-up

CorrectionofHypoxemia.Treatanemia
Euthermia,Euglycemia
HypothermiashouldnotbeusedoutsideclinicaltrialorconcomitantHIE
Normotension.Treatdehydration
MonitorandcontrolICPtokeepadequateCPP
ContinuousEEGmonitoring§ Intheabsenceofclinicalorelectrographicseizures,NOAEDsisindicated
Stroke- AcuteManagement

Case 1: Arterial Ischemic Stroke in a neonate

Initialpresentationandimaging:MRI3.3Kgboybornat403/7gestation
Uncomplicatedvaginaldelivery
Apgars:6and9
EveningofDOL1:tonicclonicactivityLlimbs,oralsmacking,Leyeblinking

FurtherworkupEchocardiogram:§diffusethickening,shaggyandirregular,ofseptalleafletoftricuspidvalve,c/wvegetationorthrombus
§ rightatrialdilatation
Basicmetabolic,cultures,hypercoag studiesallnegative

Managementandfollow-upimagingTreatedwithphosphenytoin andphenobarbital;LMWH
DGwasanticoagulatedinviewofthickeningoftheseptalleafletofhistricuspidvalve,combinedwithapatentforamenovale.
Hedidnothaveanyplasma-phasebasedriskfactors
Follow-upFLAIRsequenceatage7months

ArterialIschemicStrokeinNewbornsUsuallyduetoperinatal/maternalfactors,anddonotrequireanticoagulation.Butanechocardiogramshouldbeperformedtoexcludethrombusinaventricleoronavalve,aswellasright-to-leftshunting.
Asmanyas30%,however,maybeassociatedwithaplasma-phasebasedriskfactor.Studiesareunderwaytoconfirmthatthissubgroupdoesneedanticoagulationinordertopreventrecurrence.

ArterialIschemicStrokeinNewbornsRecurrentthromboemboliceventsarenotcommon:3.3%of215neonateswithAIS.Thisreflectsthedominanceofperinatalandmaternalfactors.
However,perinatalthromboticevents,nonetheless,areassociatedwiththepresenceofplasmaphaseriskfactorsinthesettingofunderlyingsystemicdisease
Infact,prothrombotic riskfactorsareactuallyveryfrequent:127/215,or61%ofneonatesintheKurnik study,and15/50,or30%ofperinatalAIS’satMGH
Kurnik etal,Stroke34:2887-93,2003;Grabowski,BuonannoandMusolino,Blood2010

Prothrombotic riskfactorsarefrequentandimportantTheidentificationofsuchriskfactorsisthusveryimportant:§ Closureforparentsasking“Whyourchild?”§ Maypredictincreasedriskofthromboembolisminlaterlife:canthen
mitigaterisks§ MaypredictsignificantrecurrenceriskinCSVT
Kenet etal,Blood106:1629,2006; Nowak-Gottl etal,2009;Youngetal,2010Grabowski,BuonannoandMusolino,2010
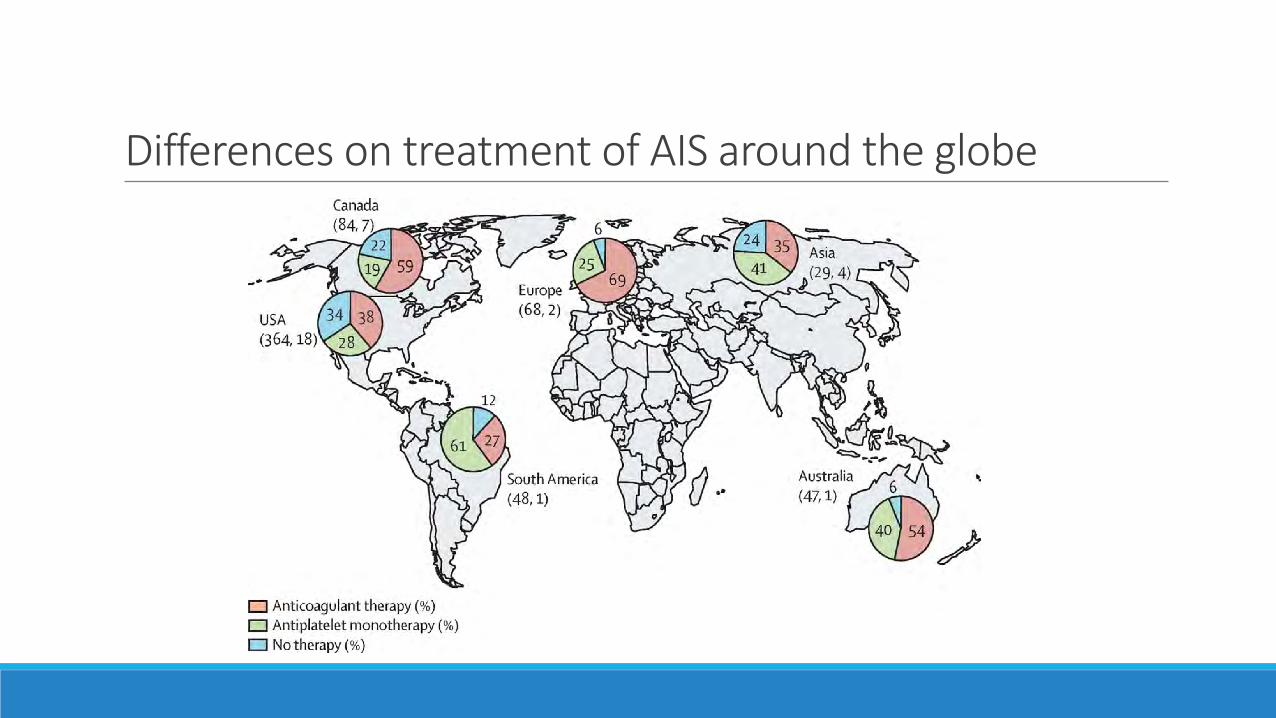
DifferencesontreatmentofAISaroundtheglobe
AnticoagulationGuidelinesAlthoughnewbornswithstrokeusuallydonotrequireanticoagulanttherapy,thistherapyshouldbeusedinthefollowingsituations:
§ Presenceofathrombusinaheartchamberand/oronaheartvalve,and/orinthemajorarterialtree(e.g.,aorticarch),especiallyinthepresenceofaPFO,VSD,orASD.
§ CSVTorcorticalvenousthrombosiswithvenousinfarctionorriskofterritorytobelostwithvenousinfarction.
§ Radiologically-confirmedprogressionofstroke,orstrokerecurrence(bothrare).

Neonatalstroke-prognosisSurvival
§ 60-80%afterhemorrhage,§ 85-95%afterischemicinfarct
Neurologicresiduain75%§ Paresis,focaldisorders(hemianopsia,language,etc.),movementdisorder§ Behavioralandcognitivedeficitsarenotinfrequent(11%behavioral,21%language,69%reductionof≥1IQindexmeasure.
Seizuresremitinmostofchildren.However,between38%and46%ofneonateswithAISwilldevelopepilepsy.
§ Riskfactorsfordevelopmentofepilepsyincludedseizureatpresentationandinfantilespasms

Case 2: Sino-venous thrombosis in a child
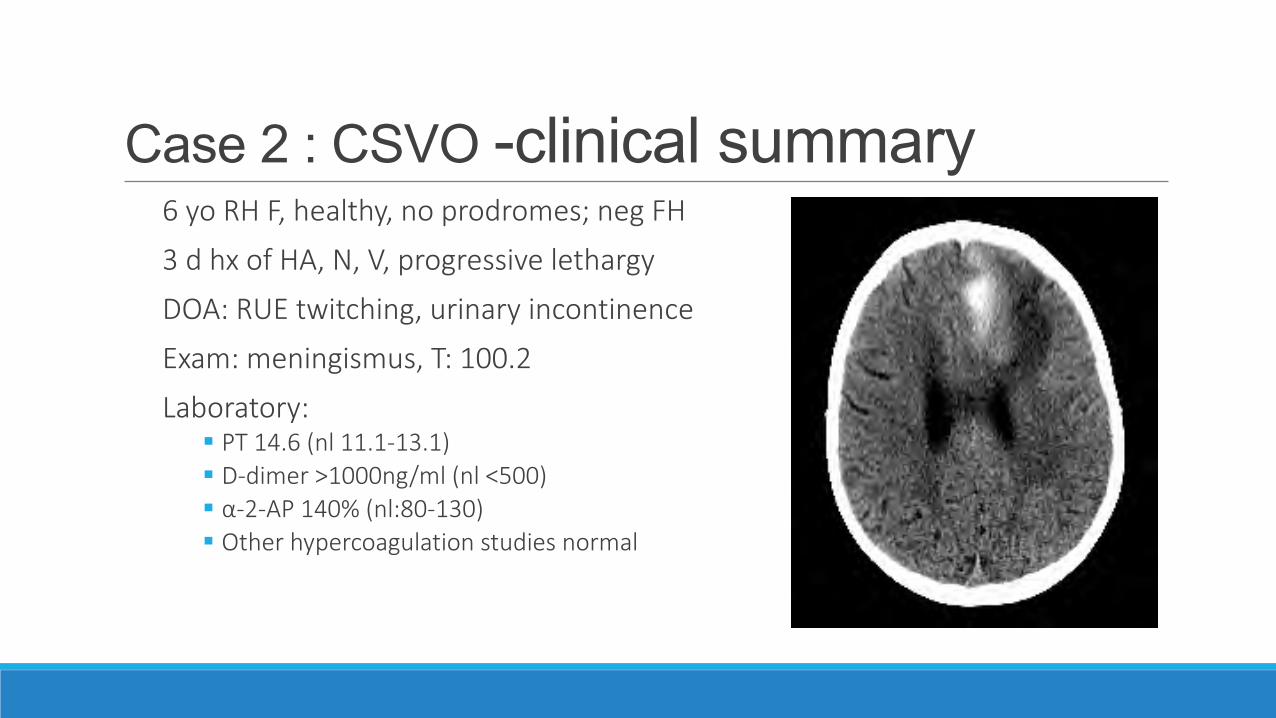
Case 2 : CSVO -clinical summary6yo RHF,healthy,noprodromes;negFH
3dhx ofHA,N,V,progressivelethargy
DOA:RUEtwitching,urinaryincontinence
Exam:meningismus,T:100.2
Laboratory:§ PT14.6(nl 11.1-13.1)§ D-dimer>1000ng/ml(nl <500)§ α-2-AP140%(nl:80-130)§ Otherhypercoagulationstudiesnormal

InitialMRV
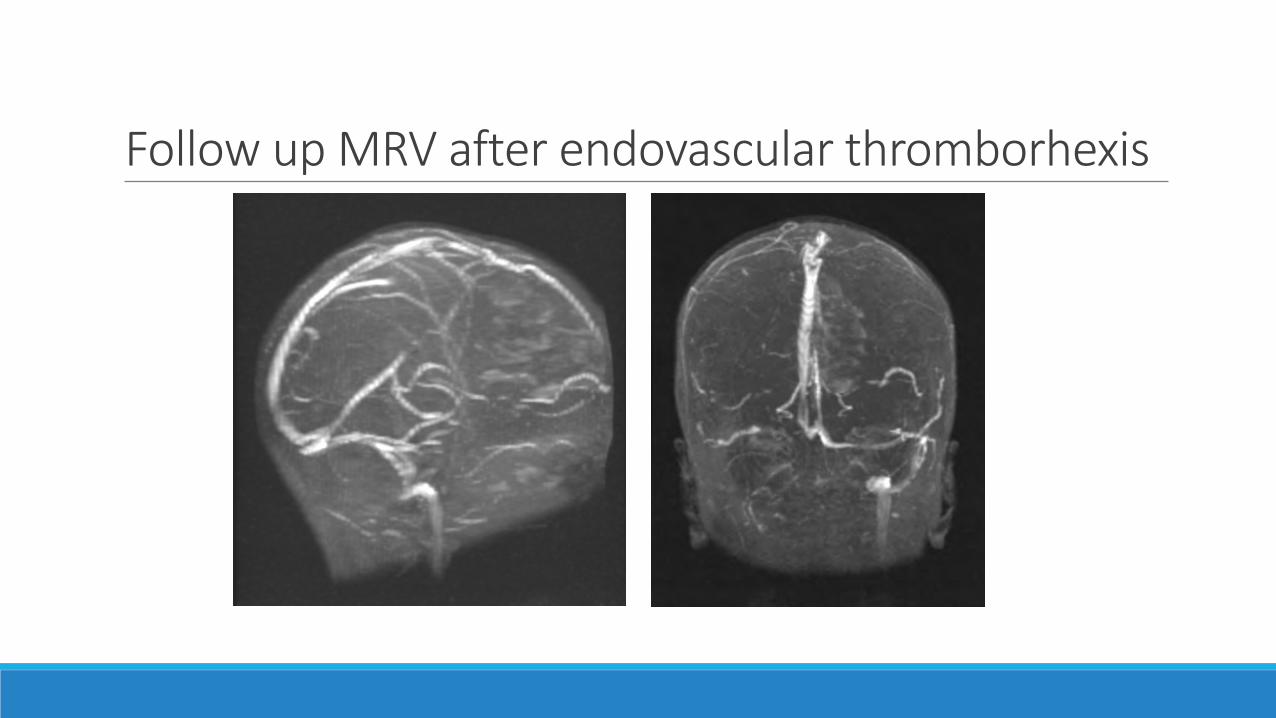
FollowupMRVafterendovascularthromborhexis

Case 3: Sino-venous thrombosis in a neonate

Initialpresentationandimaging:CThead
§Fulltermboy
§Vacuumassisteddelivery
§BW3.72Kg(25th %ile);headcircumf.36.5cm(10th)
§Intubatedatdeliveryb/orespiratorydistress

NeonatalCSVT:CTV-sag§CTVenogram
§PartialcompressionposteriorthirdSSS
§MRIandMRV,whenavailable,mayreplaceCTandCTV
SinusThrombosisinNeonatesThereisa15-20%incidenceofprogression,basedonexperienceatMGHPediatricsandDenverChildren’sHospital.
Riskfactorsinclude:§ involvementofadominanttransversesinusand/orthetorcula;presenceofaseizure
§ intracranialhemorrhageinatermNBintheabsenceoftrauma,§ vacuumextraction,§ orableedingdiathesis,§ positivefamilyhistoryforahypercoagulabilitydisorder

AnticoagulationinneonatesandchildrenwithCSVTAsymptomaticchild(noneurologicchanges,noheadandneckedema):§ Thereisnoconsensusatthistimeconcerningtheuseof
anticoagulanttherapy.§ Intheabsenceofintracranialhemorrhage,wepreferto
anticoagulate (optimallywithlowMWheparin)inviewofasignificantincidenceofprogressiontoheadandneckedema.
Symptomaticchild (noneurologicchanges,noheadandneckedema):§Consensusexiststousestandardunfractionatedheparin,butthereisnodatatosupportornotsupporttheearlyuseoffull-doseanticoagulanttherapy,especiallyinthesettingofapre-existingintracranialhemorrhage.
AnticoagulationinneonatesandchildrenwithCSVT

HeparinDosingLowmolecularweightheparin(enoxaparin)◦ Age>1yr 1mg/KgbidSC◦ Age3mo -1year 1.2mg/KgbidSC◦ Newborn– 3months 1.5mg/KgbidSC
Unfractionatedheparin(newbornto3months)◦ Standarddose 28U/Kg/hr◦ Lowdose 10U/Kg/hr

CSVT- longtermoutcomesDevelopmentaldelay 28-58%
Learningdisabilities ~5%
Cerebralpalsy 6-28%
Epilepsy 6-20%

Case 4: Arterial ischemic stroke in a 14 y.o. with Down’s syndrome
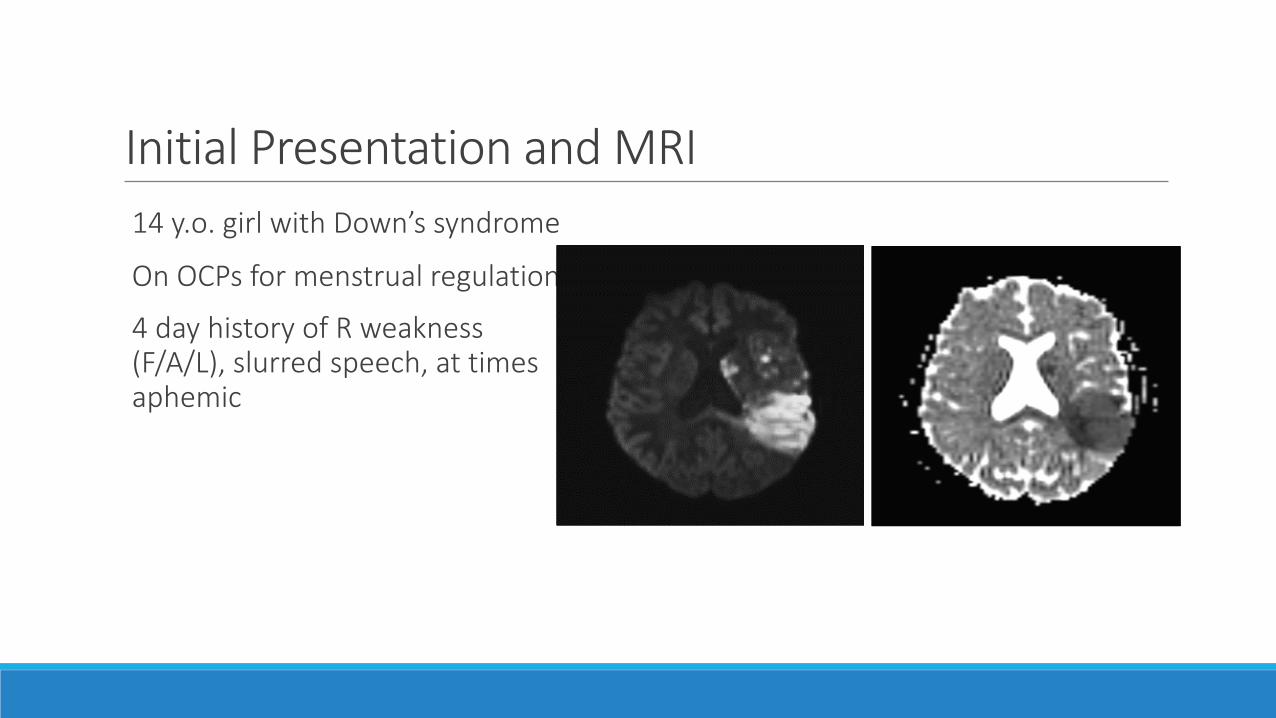
InitialPresentationandMRI14y.o.girlwithDown’ssyndrome
OnOCPsformenstrualregulation
4dayhistoryofRweakness(F/A/L),slurredspeech,attimesaphemic
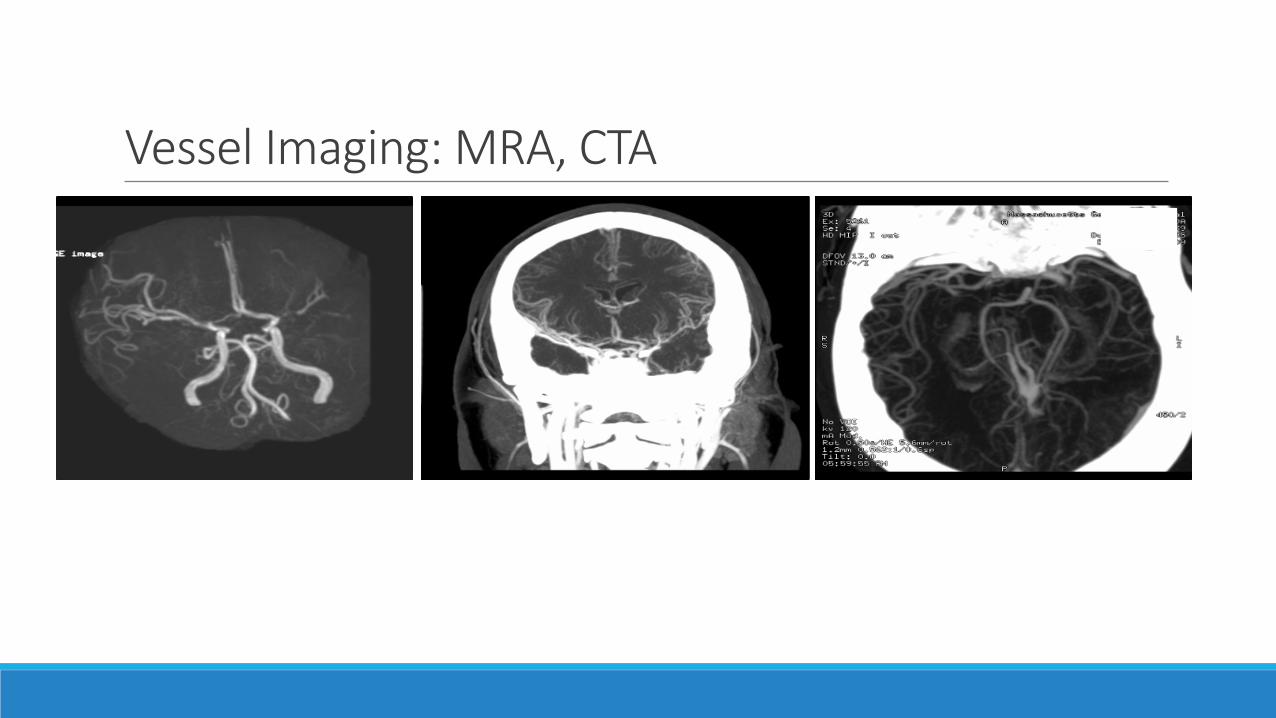
VesselImaging:MRA,CTA

Conventionalcatheterangiogram
Disordersassociatedwithmoya-moya pattern§Sicklecelldisease
§Post-XRT(usuallyofopticglioma,craniopharyngioma,hypothalamicorbasalgangliaglioma)
§Neurofirbomatosis (NF-1)
§Tuberoussclerosis
§Down’ssyndrome
§Sturge-Webersyndrome
§TB,pyogenicmeningitis,leptospirosis
§Marfan’s;pseudoxanthomaelasticum;connectivetissuedisorders;FMD
§Aorticcoarctation
§Apert’s syndrome;Fanconi’s anemia
§Polyarteritis nodosa
§Glycogenstoragedisorders

Moya-MoyaBimodaldistribution<10,or>30y.o.§Youngerpatients->ischemicinfarcts§Olderpatients->hemorrhages(incl.‘rysmal)
Notassociatedwithspecificstroketype§RecurrentTIAs,esp.afterhyperventilation§TIAsaccruinginfarcts§ Infarctfromoutset

RiskFactors§LeftMCA:M1stenosis,withriskoffuturemoya-moya changesintrisomy21
§ElevatedLipoprotein(a):24mg/dL (nl <3)
§Familyhistory:mothersufferedanacuteMIinher50s

ApoaproteinboundtoLDLKringle andproteasedomainshomologoustoplasminogen
HeterogeneityofLp(a)[180-650kDa]duetonumberofKringle 4repeatsinApoa
Lipoprotein(a)
6.5- fold increased risk

Lipoprotein(a)Alowdensitylipoproteinwithahighdegreeofsequenceidentitywithplasminogen
Elevationsconfera6.5-foldincreasedriskofstrokeandCSVT(Kenet etal.,Stroke 2010) and3.2-foldofthromboembolisminchildhood(vonDepka etal,Blood,2002)
Antifibrinolytic(thereforepro-thrombotic)viacompetitionwithplasminogenforbindingsitesonaspecificendothelialcellreceptor
Bindsandinactivatestissuefactorpathwayinhibitor
Carriescholesteroltothevesselwall
Lipoprotein(a)inDown’sSyndromeItisunknownwhetherlipoprotein(a)iselevatedinTrisomy21§However,thereissomeevidencethatlipidsandlipoproteinsaregenerallyelevatedinthisgeneticcondition
PediatricstroketreatmentModifystrokeriskfactorsandtreatunderlyingconditions§SCD,CCAD,hypercoag states,moya-moya,Fabry’s,etc§Fesupplementation
Properdiet;exercise;tobaccoanddrugavoidance
AlternativestoOCPs◦ Norethindrone◦ Norgestrel (MirenaIUD)

t-PAforPediatricAcuteIschemicStroke?Norandomizedcontrolledtrials.
Importanttoestablishtimeofonset,whichcanbedifficultintheyoungchild
Requirementoftimelyimaging
Riskofcatheter-associatedthrombosisduringintra-arterialadministration(issues:useofheparin,catheterasforeignsurface,contrastmediumhyperosmolality)

ThrombolysisinPediatricStroke(TIPS)Five-yearmulti-centerinternationaltrial§ Safetyanddose-findingstudyofintravenous(IV)tPA inchildrenwithacuteAIS§ Determinethemaximalsafedoseofintravenous(IV)tPA§ Threedoses(0.75.0.9,1.0mg/kg)forchildrenage2-17years§Within4.5hoursfromonsetofacuteAIS.
Terminatedbecauseoflackofpatientaccrual,
Butdidleadto“consensus”dosesoft-PAtouseforthoseuncommoncasesinwhicht-PAisindicated

Amlie-Lefond C, et al. 2009 Lancet Neurology 2009
IPSScaseseriesoftPA use2003-2007(n=18)§ NostandardizedpediatrictPA guidelines,sotreatment‘realworld’§ basedonindividualcentres’ protocol/practicee.g.adulttPA protocol§ N=18children(9intra-arterial-tPA,9intravenous-tPA),16/18Ant.Circ.§ 2.2%ofchildrenwithAIS(vs.Janjua healthrecordlinkagestudy:1.6%)§ Treatmentfrequently‘offprotocol’e.g.IVMean3.3hrs post-onset
Outcome at Discharge IA or IV tPAN=18
No tPAN=656
Neurologically Normal 11% (2) 21%Neurological Deficit 78% (14) 74%Death 11% (2*) 3%Post-tPA ICH 22% (4) (all asymptomatic) NAOther Femoral A. thrombosis
+ foot amputation
*1 brain herniation, 1 brainstem infarct
IPSSOfflabel-compassionateuseoftPA
AspirinTherapyLow-dosecanbeaseffectiveas“full”dose,ifabsorbedproperly
Theremayalsobean“optimal”dosewhichblocksplateletthromboxanewhilepreservingatleastsomeendothelialcellprostacyclinproduction(i.e.,20to40mgQDinanadult)
Facedwithaspirin“failure,”onemayswitchtoclopidogrel

AspirinResistanceMaybeacauseofrecurrentischemicvasculareventsinpatients
takingaspirin.
Actuallyreferstomanydifferentphenomena:§ inabilityofaspirintoprotectpatientsfromvascularevents
(clinical);§ inabilityofaspirintoaffectanyoneofseveralmeasuresof
platelet(biochemical)§ inabilityofGItracttoabsorbASA
PlateletThrombi

Platelet-FibrinThrombusFormationInFlowingWholeBloodE.F.Grabowski2015
Platelets:greenFibrin:red
Case 5: Stroke in a child with Sickle Cell Disease
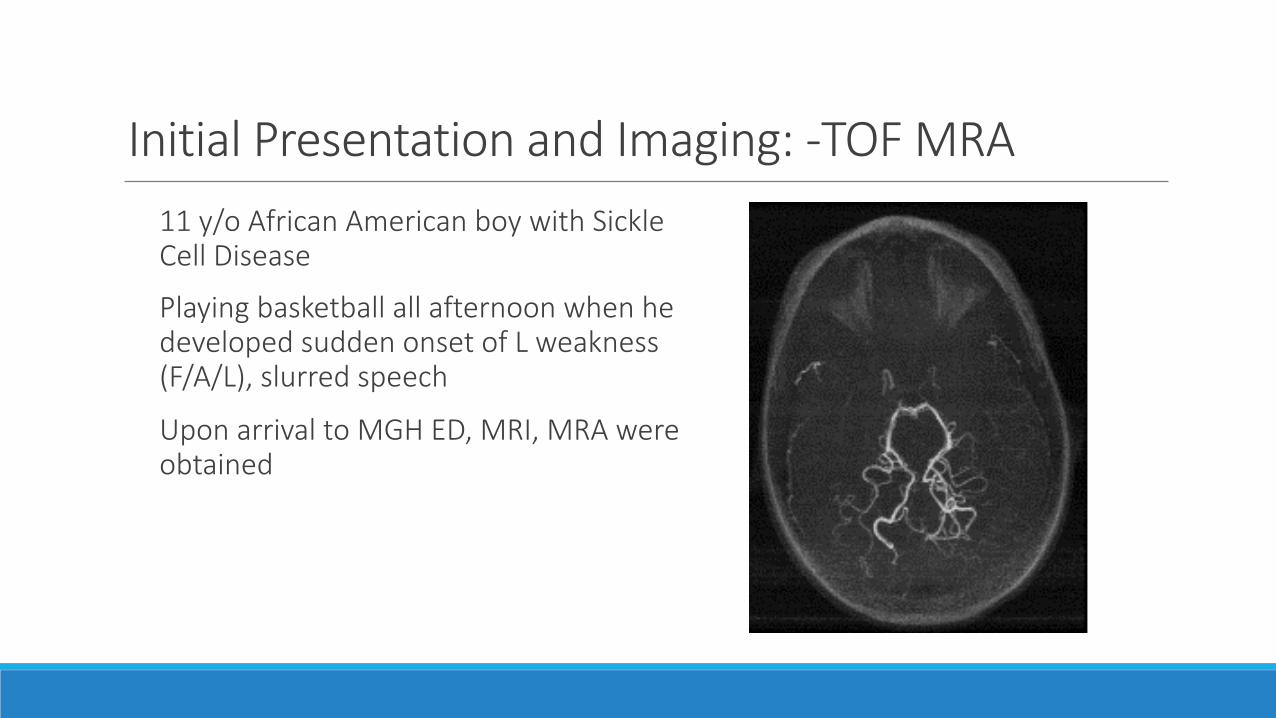
InitialPresentationandImaging:-TOFMRA11y/oAfricanAmericanboywithSickleCellDisease
PlayingbasketballallafternoonwhenhedevelopedsuddenonsetofLweakness(F/A/L),slurredspeech
UponarrivaltoMGHED,MRI,MRAwereobtained

Sicklecell- acuteandchronicinfarctions

SickleCellDiseaseAffects0.16%ofBlacks
25%havecerebrovasculardiseaseonneuroimaging,withorwithoutsymptoms§Cerebralinfarction 75%§ ICH20%§ SAH1-2%§Cerebralsino-venousocclusion§ FatembolismfromHbS-relatedboneinfarcts
q

RelativeIncidenceofSSStrokevs.AISinPediatrics§ArterialIschemicStroke
~0.05%byage18yrs (1/2000)
§HemoglobinSSStroke
16%byage18yrs (1/6)inSSdisease

SickleCellDisease:InfarctionIn70-80%,strokeoccursinunder-15y.o.
In60%,recurrent,usuallywithin3years
Occursinpatientswith§morefrequentcrises,andattimeofcrisis§ cardiomegaly§ concurrentinfection
andisaccompaniedby§ seizuresand§ alteredmentalstatus(but“cerebral,”oranalgesicdruguse?)

SickleErythrocytesandCerebralArteryOcclusion

SickleCellDisease:StrokeManagementO2andassure/establishairway
Controlofseizureactivity
Redcellpheresis toHgbS <30%
AvoidHct of>30owingtohyper-viscosityandconsequentimpairedO2delivery:SSRBCsareinherentlylessdeformableandgiverisetonearlythesameviscosityasAAblood,eventhoughSSHCTisnormallyonly20-24.
Anticoagulationiscontroversial;underinvestigation,butnotcurrentstandardofcare

StrokePreventioninSickleCellDisease(STOP)- TCDIfnormalPSV(<170cm/sec):annualscreening(orsemiannualif2-10y.o.)IfPSV>200cm/sec,repeatstudyinonemonth,andrepeatin3-6monthsStrokePreventionTrialinSickleCellAnemia(STOP):chronictransfusiontoHgbS <30%inchildrenwithpersistentlyabnormalTCDresultsOutcome:Incidenceofstrokedecreasedby90%

HydroxyureatrialsinSickleCellDiseaseSWITCH
90%secondarystrokeprevention
Stoppedbecauseofsafetyandfutilityconcerns§ Wareetal,StrokewithTransfusionsChangingtoHydroxyureaClinicalTrial(SWITCH).Blood2012;119:32925;§ Alvarezetal,AmJHematol,2013;88(11):932
TWITCH(TCDWithTransfusionsSwitchingtoHydroxyurea)
100%primarystrokepreventioninchildrenwithelevatedTCDvelocities
Inmaintenance,hydroxyureaequivalenttotransfusiontherapy§ Wareetal.HydroxyureaversuschronictransfusionformaintenanceoftranscranialDopplerflowvelocitiesinchildrenwithsicklecellanemia- TCDwithtransfusionschangingtohydroxyurea(TWITCH):amulticenter,open-label,phase3,non-inferioritytrial.Lancet2016;387:661

NovelNeuroprotectantsinAcuteIschemicStroke3K3A-APC§ GeneticallyengineeredactivatedproteinC,usedincombinationwitht-PA§ Clinicaltrialforsafety(Rhapsody,May2015-May2017)
Pre-Implantationfactor(PIF)§ Promotesembryotrophic andneuroprotectivedecidual genes
PlacentaleXpanded (PLX)cells§ ProtectPC12cells- anestablishedmodelofvariousnervecellsincludingdopaminergicneurons- fromdeathafteroxygenandglucosedeprivation

Case 6: Compelling risk factors for stroke
Primary Stroke Prevention

Nostroke,butcompellingriskfactorsina13y.o.boyDiagnosis:At-high-risk-for-Stroke
FH:mothersufferedanischemicstrokeatage42;hadmigraines,ANAof1:21,000,andfoundtohaveproteinSdeficiency.
Patienthad:§Migraines§ ANAof1:1280§ ProteinSof41%§ Lipoprotein(a)of65mg/dl(normal<30mg/dl)§ PFOwithright-to-leftshunting.

ManagementWarfarinand81mgASAx8months,untilPFOclosure
81mgASAsubsequently
Niaspantocorrecttheelevatedlipoprotein(a)§ Interestingly,hisheadachesdisappearedafterPFOclosure.

ConclusionsMortalityduetountreatedpediatricstrokeisapproximately9-10%
Thereissignificantneurologicalandneurocognitivemorbidityinthesurvivors,includingseizures,hemiparesis,andneurocognitiveissues
Neonatesoverallhaveabetterprognosisthanolderchildren

ConclusionsNeonateswithearlypresentationhavebetterprognosisthanthosewithdelayedpresentation,especiallyintermsofmotordeficits
ThosewithAIStendtohavemoredeficitsthanthosewithCVST
Thereisasignificantcorrelationbetweenthepresenceofmotordeficitsandbothepilepsyandneurocognitivedeficits

ConclusionsPost-strokeevaluationmustinclude:§Physicaltherapy§Occupationaltherapy§Speechandlanguagepathology§Neuropsychologicalevaluation§Vocationaltraining§Psychology/socialwork§Psychiatry(ifindicated)

SummaryStrokeinchildhood,whilenotcommon,isalso
a)notrare,and
b)frequentlyunsuspectedatpresentation.
Thecausesandpatternsofpediatricstrokediffermarkedlyfromthoseofadultstroke.
Acoordinatedmulti-disciplinarypediatricstroketeamisnecessarytoprovideeffectiveandtimelyevaluationandmanagement.

TeamMembersatMGHNeurology:P.Musolino,K.Krishnamoorthy,andF.Buonanno
PediatricHematology/Oncology:E.Grabowski
PediatricNeuroradiology:P.Caruso
Neurosurgery:W.ButlerandC.Duhaime
CoagulationLab:E.VanCott
Neuropsychology:A.Morgan
PediatricPMR:D.Nimec,S.Quinn
Follow-upClinic:E.Grabowski,F.Buonanno,P.Musolino

ThefullteamatMGHwww.massgeneral.org/children/services/treatmentprograms.aspx?id=1628

HowtoreachusForACUTE cerebro-vascularreferrals:§ call617-726-2000§ andpage21333,the“pediatricneurologyresidentoncall.”
§ thispersonthenactivatesthepediatricstroketeam
ForOUTPATIENT evaluationsandfollow-up:§ call617-726-2737

Thankyou….
Thankyou...questions?

NeurogenesisduringEmbryoniclifeà SVZ
Arias-Carrión InternationalArchivesofMedicine2008NatureNeuroscience14,1382–1389(2011)

PostnatalNeurogenesisà PerivascularNiche
AdaptedfromZacchigna etal.NeuralStemCells- NewPerspectivesbyLucaBonfanti.Chapter8.2013

ACUTESTROKEin2-18yearoldpatientPediNeuro FellowConsultPaged
Likely IschemicStroke LSW <6hs
PediNeuro FellowactivatesPediStrokeGroupPage
Examine patient and obtain history (if at home page Adult Acute Stroke Fellow and ask to start evaluation)
PICUResourceNurse•NotifyPICUfellow•Preparebedforpossibleadmission•AlertsRapidResponseTeam
EDorFloorRN•CheckFSBS•Place18-20gaIVsx2•SendLabs;Heme,Chem-7,Coags•PrepareptforCTorrapidMRI- CheckBP- O2tokeepSpO2>94%•WeightptorestimateusingBroselow traumatapeStrictNPO•AvoidplacingNGT/foley•VSq15”
EDPharmacist•Respondtopt’sbedside•CommunicatewithCRConcallnurse(pager)•Reviewptweight• CalculatestPA dosagewithTIPStrialpharmacist•DispensetPA fromTIPStrialtoMD•Dispenseothermeds(D50W,labetolol,nicardipine)
PediNeuro andPICUFellow•Gatherparent/guardiancontactinfo•PerformsPediatricNIHSS•VerifiesLSWandcontraindications•AssuresCT/CTA/MRIandlabordersareplacedbyEDresident•ReviewsMRIsafetyquestionswithparent/guardian•UpdatesPedi-StrokeandConsultAttending
EDResident•Orderslabs,MRIbrainpediatricstrokeprotocolandCT/CTAheadandneckstrokeprotocol•Helpscoordinatesedation(ifneeded)withpediatricanesthesia
CRCNurse•AssistsEDnurseandTIPStrialpharmacist•Startsexamsandblooddrawsperprotocol•FacilitatestransitiontoPICUnurse
PediStrokeAttending•DeterminesImagingprotocolneeded•PerformsPediatricNIHSS•DetermineseligibilityforRxinterventions
Discusswithparentstherapeuticoptionsandrisks
NosignificantchangesfrominitialNIHSSManageSBPandDBPtokeep<90%ile
IfCT/MRIokPediStrokeAttendingconsideranticoagulation,IVtPA orendovascularRx
TransportpttoEDCT/MRIscanner

















