35
Pediatric Trauma Bartholomew J Tortella MTS, MD, MBA, FACS, FCCM 1
| Date post: | 27-Dec-2015 |
| Category: |
Documents |
| Upload: | gwen-kelley |
| View: | 221 times |
| Download: | 0 times |

Pediatric Trauma
Bartholomew J TortellaMTS, MD, MBA, FACS, FCCM
1

Outline
• Background• Trauma scores• Principles and Approach• ABC’s• Specific injuries– Head, C-Spine, Chest, Abdominal, Burns
• Abuse
2

Background• Leading cause of death > 1 yr• 50% of all childhood deaths• < 5 yr highest risk; boys > girls• 1.5M injures / 250k hospitalizations / 100k
permanent disabilities• 85% Blunt / 15% penetrating • Ped trauma ctr.– St. Christopher’s Hospital for Children– Children’s Hospital of Philadelphia
3

Special Pediatric Considetions
• Smaller body size (larger force transfer/area)• Increased body surface area• Less subcutaneous fat• Head disproportionately large / C-spine• Bones have physes• Resp = leading cause of arrest• BP changes VERY late
4

Airway
• Respiratory #1 cause of arrest• Twice O2 demands
• ET tube size: Age/4 + 4• Uncuffed ET tube
5

Anatomical airway issues in kids
• Big tongue, soft tissue obstruction• Anterior larynx• Big epiglottis straight blade (Miller / Wisconsin)• Short trachea• narrowest at subglottis (uncuffed tube)• Big occiput forces airway shut when on back board
6

Rapid Sequence Intubation
• Pre-treat atropine 0.02 mg/kg all < 6yr• Induction: Etomidate 0.3 mg/kg
• Paralytic: Succinylcholine 1.5 mg/kg• Post intubation• Morphine (0.05mg/kg)• Midazolam • Vecuronium (0.3 mg/kg)
7
Breathing
• Signs of distress: retractions, tracheal tug, nasal flaring
• Infants: Diaphragm 1° muscle resp & easily fatigued
• Thoracic structures mobile shift• Rib Fx uncommon so beware the Tension PTx
without rib fractures
8

Circulation
• Hypotension LATE sign: kids compensate well– 25% loss of blood volume– Minimum acceptable BP: 70 + (2 x age)
• Shock: HR, RR, mottled, cool, pulses, altered LOC, cap refill < 2 sec, narrow Pulse pressure
• Note: scalp laceration can cause shock
9

Circulation
• IV’s: antecubital / femoral• Attempts >90 sec: intraosseous• Fluids– Ringer’s Lactate 20mL/kg x 2– pRBC 10mL/kg– FFP / Platelets
• No role for MAST: mortality• Surgery for continued instablility
10

Disability Pediatric Glasgow Coma Scale1 2 3 4 5 6
Eyes Does not open eyes
Opens eyes in response to painful stimuli
Opens eyes in response to speech
Opens eyes spontaneously
Verbal No verbal response
Inconsolable agitated
Inconsistent inconsolable Moaning
Cries but consolable
Inapp’prate interactions
Smiles, orients to sounds, follows objects, interacts
Motor No motor response
Extension to pain (decerebrate response)
Abnormal flexion to pain for an infant (decorticate response)
Infant withdraws from pain
Infant withdraws from touch
Infant moves spontaneously or purposefully
11
Exposure
• Thorough exam then COVER• Trauma X:– Multiple bruises in different stages of healing– Usual fractures (torque)– Cigarette / cigar burns– Changing / unrealistic history
• Legal duty to report (criminal liability for physician)
12

Secondary Survery
• Head to toe examination• History from EMS / Care giver / Patient
13

Laboratories & Intervenions
• Blood Bank Sample• PT / PTT (coagulopathy = higher mortality)• Others– Hemogram– Lytes
• Orogastric tube• Foley catheter
14
Imaging
• FAST• Chest X-Ray• Obvious fractures• CT Scan
15

Head Injury
• Leading cause of death in peds trauma (80%)• 90 % “minor”• Falls > MVC > MPC > bicycle > assault• Few require surgery: 0.5 -1.5%• 4-6% with normal exam have ICH on CT
16

Head Injury: Anatomic differences
Protective• Fontanelles• Open sutures• Plasticity
Susceptible• Big head torque• Soft cranium injury w/o
fracture• Less myelin more shearing
forces• Prone to reactive hyperemia
17
Head Injury: Types of injury
• Contusions, DAI, SAH, parenchymal• Subdural: common, poor outcome, <1 yr• Epidural: uncommon, <4 yr, subtle
presentation, minor trauma
18

Skull Fracture
• 20 x risk ICH• Linear > depressed > basilar• X-rays not sensitive nor specific• 90% linear have overlying hematoma• “Growing skull”:diastatic dural tear meninges
herniate, prevents closure: NSx F/U
19
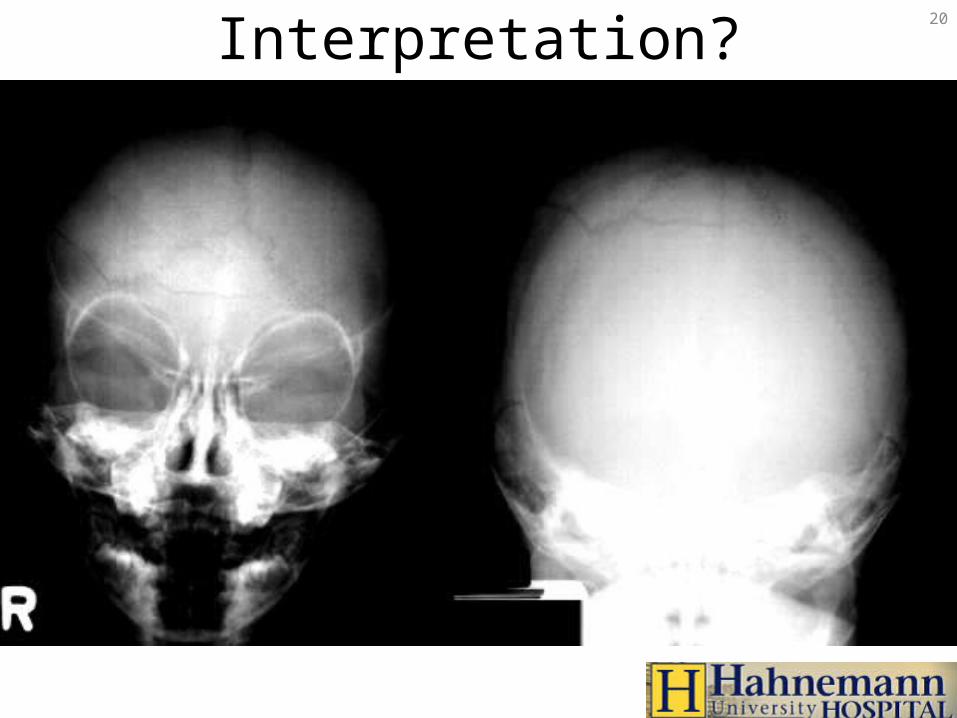
Interpretation? 20

Growing Skull Fracture21

C-Spine Injuries
• Less common in kids BUT higher mortality• <8 yr: 2/3 above C3
22
C-Spine• Less common in kids BUT higher mortality• <8 yr: 2/3 above C3• Big head, less muscles torque, fulcrum C2-3• Cartilage & lax ligaments injury w/o fracture• Pseudosubluxation
C2-3, C3-4: 3-4 mm or 50% vertebral body width• Prevertebral space: C2=7mm, C3=5mm, C6=14mm• Predental space 4-5 mm• Watch out for ncomplete ossification, multiple centres
23
SCIWORA
• 16-50% SCI!!• < 9 years• Transient neuro symptoms (parasthesias)• Recur up to 4 days later• bottom line: – CT/MRI if abn neck/neuro exam, distracting
injuries, alt. LOC, high risk mech DESPITE normal 3-views
24

Chest Trauma
• 2ND leading cause pediatric trauma death• Compliant chest wall rib fracture uncommon– Significant injuries w/o external signs– If fracture present, severe injury
• Treat non-operatively• PTx: 15% require more than chest tube• Pulmonary contusion most common, aortic
injury rare
25
Chest Trauma
• Traumatic asphyxia– Sudden compression elastic chest wall against closed glottis
intrathoracic pressureobstruction of SVC/IVC capillary extravasation
– Petechiae face, neck ,chest– Periorbital edema– Retinal hemorrhages– Resp distress / hemoptysis, pulmonary/cardiac contusions,
liver injuries, pneumothorax
• Treat: chest tube prn, ventilate, PEEP, elevate head
26

Abdominal Trauma: Anatomic issues
• Larger solid organs, less musculature, compact torso, elastic ribcage, liver & spleen anterior– Potential internal injury– Most solid organ – Spleen>liver>kidney>pancreas>intestine
• Bladder intra-abdominal (10% GU injury)
27

Abdominal Trauma: Assessment
• Clinical findings unreliable• Shoulder tip pain, flank / lap ecchymosis• Feassess, reassess, reassess • Mechanism classics: handlebars, lap belt
28

Abdominal Imaging: CT
• FAST not as reliable as adults• Stable pt only• ID’s injuries, retroperitoneum• Insensitive for hollow viscous (25% sens),
pancreas (85% sens)
29
Abdominal Trauma: Management
• Spleen and liver:– 90% Non-operative: admit, observe, Hct– Fatal hemorrhage with liver injuries
• Pancreas:– Observation– Drain
• Hematuria:– gross or >20 RBC + unstable OR– >10 RBC + stable CT cysto
30

Child Abuse: Clues
History• story injuries• history changing• injury development• delay seeking help• inappropriate level of
concern
Physical Exam• multiple old and new
bruises• posterior rib #, sternum
#, spiral # < 3• immersion burns,
cigarette
31

Child Abuse
• 1 million confirmed cases / year (US)• high index of suspicion• RF: poverty, single parent, substance abuse,
<2 yr, disability, low birth wt• cutaneuos injuries most common• death 2° head & abd trauma• interview child & parent separately
32

Child Abuse: Head Injury
• blunt, acceleration/decceleration • 31% missed, 28% re-injured• fractures:– bilateral, cross sutures, diastatic, non-parietal
• IC injuires:– SAH, subdural, ICH, edema
• CT if suspect
33

Child Abuse: Management
• DOCUMENT• full P/E (rectal, genital)• photograph• B/W: CBC, PT/PTT, LFTs, lipase, U/A• skeletal survey• CT head, abd prn• Child Protection
34

Bottom Lines
• NOT just little adults BUT resuscitation remains the same
• Severely injured do better at trauma centre• Metabolic requirements differ• Multisystem injury is RULE• Occult injuries are common• Head injuries: high mortality, assoc injuries• be aware of potential abuse
35

















