47
PEDIATRIC TRAVEL MEDICINE Dr Suchitra Rao Assistant Professor Pediatric Infectious Diseases Children's Hospital Colorado September 25, 2014
| Date post: | 22-Dec-2015 |
| Category: |
Documents |
| Upload: | curtis-summers |
| View: | 213 times |
| Download: | 0 times |

PEDIATRIC TRAVEL MEDICINE
Dr Suchitra Rao
Assistant Professor
Pediatric Infectious Diseases
Children's Hospital Colorado
September 25, 2014

Travel medicine and children- unique perspectives• Travel medicine in children- unique set of challenges • More travel to destinations placing them at risk of
• malaria, diarrhea, enteric fevers, dengue fever, dermatoses
• Proportion of children VFR has increased• Immunizations may not be effective or not studied in
younger children/ infants
• Analysis of post-travel data from large multicenter study:• Children were less likely to receive pre-travel advice• More likely to require inpatient care than adults

Objectives• Discuss routine pediatric vaccines pertinent to travel• Discuss travel vaccines specific to pediatric population• Prevention and management of traveler’s diarrhea• Malaria prophylaxis- pediatric considerations• Tips on travelling with children, management of travel-
related conditions

ROUTINE CHILDHOOD VACCINES MODIFIED FOR TRAVEL

Case 1 • A family of 4 are travelling to Nepal, including two children
aged 18 months and 6 years of age. Children’s vaccines are up to date. The mother is wondering whether her youngest needs any additional vaccines.

VACCINE MINIMUM AGE FOR FIRST DOSE
MINIMUM TIME TO SECOND DOSE (WEEKS)
MINIMUM TIME TO THIRD DOSE (WEEKS)
MINIMUM TIME TO FOURTH DOSE (WEEKS)
MMR 6 MONTHSa 4 - -
HEPATITIS B BIRTH 4 8b -
DTP/DTaP 6 WEEKS 4 4 6 MO
HIB 6 WEEKS 4 4 8c
IPV 6 WEEKS 4 4 6 MOd
MCV 6 WEEKS 8 e e
MPS4 2 YEARS 5 YR e e
PCV 4 WEEKS 4 4 8
VARICELLA 12 MONTHS 4
ROTAVIRUS 4 WEEKSf 4 4
HEPATITIS A 12 MONTHS 6 MO
Accelerated vaccine schedule

a Children traveling abroad may be vaccinated as early as 6 months of age. Before departure, children aged 6–11 months should receive the first dose of MMR vaccine. This will not count towards their series and they will still require 2 doses after 12 months of age.b The third dose should be given at least 4 months after the first dose and at a minimum of 6 months of age.c If third dose is given after 4 years, the fourth dose is not required.dRecommended at 6–18 months of age.e Minimum 6 weeks for HiB-MenCY, 9 months for Menactra (MCV4-D), 2 years for Menveo (MCV4-CRM).f this differes from the package insert but is validated by data held by the manufacturer
DTaP, diphtheria-tetanus-acellular pertussis; DTP, diphtheria-tetanus-pertussis; Hib, Haemophilus influenzae type b; IPV, inactivated polio vaccine; MCV, meningococcal conjugate vaccine; MMR, measles, mumps, rubella; MPS4, meningococcal polysaccharide.
The fineprint!

VACCINE MINIMUM AGE FOR FIRST DOSE
MINIMUM TIME TO SECOND DOSE (WEEKS)
MINIMUM TIME TO THIRD DOSE (WEEKS)
MINIMUM TIME TO FOURTH DOSE (WEEKS)
MMR 6 MONTHSa 4 - -
HEPATITIS B BIRTH 4 8b -
DTP/DTaP 6 WEEKS 4 4 6 MO
HIB 6 WEEKS 4 4 8c
IPV 6 WEEKS 4 4 6 MOd
MCV 6 WEEKS 8 e e
MPS4 2 YEARS 5 YR e e
PCV 4 WEEKS 4 4 8
VARICELLA 12 MONTHS 4
ROTAVIRUS 4 WEEKSf 4 4
HEPATITIS A 12 MONTHS 6 MO
Accelerated vaccine schedule


MMR• Children as young as 6 months of age traveling outside
the US are recommended to receive the vaccine• Any doses given prior to 12 months don’t count toward an
adequate two dose series (maternal antibodies)• Still require another dose at 12-15 months, and a second
dose at 4-6 months• Second dose protects individuals who did not respond the
first time• If accelerated schedule is required, two doses must be
separated by a minimum of 4 weeks

Case 2 • 8 yo male born in Togo is returning with his family for a
vacation in December. They last travelled 4 years ago, and he received MCV4 at that time. Does he require further doses?

Meningococcal vaccine• MCV4 for
• 9-23 months of age (need two doses 8 weeks apart)• 2-55 years (1 dose)
• Give at least 10 days before international travel• MPSV4 for
• 2 years and older
• Protects for 3 years, so boosters needed for ongoing exposure

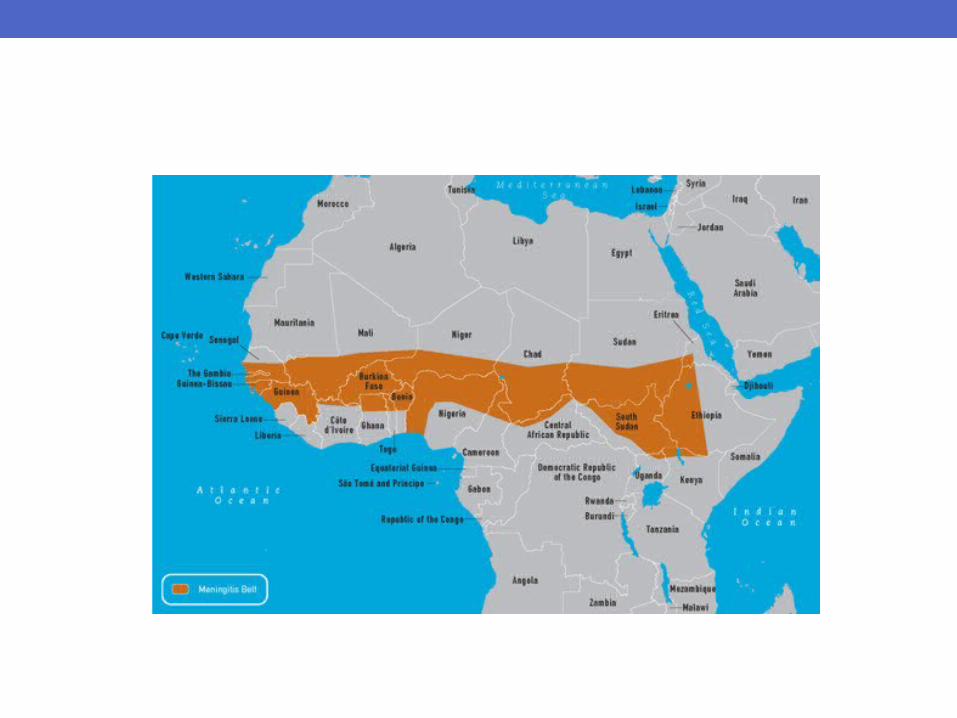
• Hib-MenCY-TT• Approved for children aged 6 weeks to 18 months • But since it doesn’t contain A or W, shouldn’t be used as a travel vaccine since most disease outside of US is type A
• Previously vaccinated infant who has received this vaccine should receive MCV4.

• If vaccinated previously and are living in or returning to Africa’s meningitis belt may need to be revaccinated.
• If previously vaccinated at 9 months - 6 years , should receive an additional dose of conjugate vaccine 3 years after their previous meningococcal vaccine and every 5 years thereafter, if at continued risk.
TRAVEL VACCINES

Case 3
• The parents of a 6 month old bring their baby in for a pre-travel visit. They will be traveling to Thailand, Vietnam and Indonesia for 6 months. They want to know if there are any travel-specific vaccines that he may need.

Japanese Encephalitis Vaccine
• Highest risk during hot summer months• JE vaccine now licensed down to 2 months of age- Ixiaro
• 0.25 mL Given at 0, 28 days for 2 months to 2 years• 0.5 mL given for 3 years to 16 years• Safety data for children – recent open label trial in the Philippines, low rates of adverse events

Typhoid vaccine
• Recommended for long-term travelers to an endemic area, those traveling off standard tourist routes, immunocompromised travelers, those of south Indian ancestry, and patients with cholelithiasis.
• Capsular polysaccharide – ViCPS- minimum age is 2 years
• Oral Vaccine Ty21 – licensed for children over the age of 6 years

Case 2 • 8 yo male born in Togo is returning with his family for a
vacation in December. What other vaccines should be considered in this child?

• Recommended minimum age 9 months of age, • Not to less than 6 months of age, due to increased risk of encephalitis (0.5–4 per 1000 vaccinees)
• Decision to immunize 6–8 months of age must balance infant’s risk for exposure with risk for vaccine-associated encephalitis.
Yellow Fever Vaccine

Rabies Vaccine• Children are at high risk • Smaller, more likely to come into contact with animals and
be bitten• Rabies is endemic among domestic animals (dogs) in
most developing countries• Consider immunization if living in rural regions for more
than 3 months • Obtain from wholesaler for pre-exposure prophylaxis
• 3 doses: days 0, 7, 21 OR 28
• Can obtain for post-exposure prophylaxis

MALARIA AND BUG BITE PREVENTION

Bug bite preventionFor skin• DEET - safe for infants and children over the age of 2 months
– (~ 30% DEET recommended) • Should not be applied to children’s hands, mouth, or near
the eyes; wash off upon returning indoors• Picaridin – considered safe for use in children by the
American Academy of Pediatrics (use minimum of 20%)• Lacks the safety profile of DEET, especially for children
• Oil of lemon eucalyptus or PMD- not on infants under 3 yrs • IR 3535 – good DEET alternative, deemed safe for use in
children but need more safety data
For clothing• Permethrin- for considered non-toxic but further studies are
needed to establish its safety profile in children

Additional reminders• Mosquito nets -can be used over beds, cribs, playpens,
car seats, and strollers• Avoid areas near standing water – birdbaths and
flowerpots, for example – where insects breed• Air conditioning and fans help• Avoid products that combine insect repellents and
sunscreens

Malaria prophylaxis• Pediatric considerations:• Age, child’s ability to swallow tablets, frequency of dosing,
access to a compounding pharmacy for adequate dispensing of medication
• Once weekly mefloquine preferable, approved for children of any age
• Atovaquone/proguanil - pediatric dosing available, only in tablet formulation. Approved in most countries for children > 5 kg
• Doxycycline - in children 8 years or older due to the risk of teeth staining

Malarone (once a day, start 1 day before travel, continue for 7 days after travel)• 5-8 kg (unlabeled dosing): Atovaquone/proguanil 31.25
mg/12.5 mg (Boggild, 2007)= ½ pediatric tablet• 9-10 kg (unlabeled dosing): Atovaquone/proguanil 46.8
mg/18.75 mg (Boggild, 2007) = ¾ pediatric tablet• 11-20 kg: Atovaquone/proguanil 62.5 mg/25 mg= 1
pediatric tablet• 21-30 kg: Atovaquone/proguanil 125 mg/50 mg = 2
pediatric tablets• 31-40 kg: Atovaquone/proguanil 187.5 mg/75 mg = 3
pediatric tablets• >40 kg: Atovaquone/proguanil 250 mg/100 mg = 1 adult
tablet

• Mefloquine (once a week, start 1 week before travel, continue for 4 weeks after travel)
Dose forms: 228 mg base (250 mg salt) tabletDose: (adult) 250 mg (salt) weekly Pediatric < 9kg: 4.6 mg/kg/base (5 mg/kg salt) weekly19-30 kg: ½ tablet weekly30-45 kg: ¾ tablet weekly45 kg: 1 tablet weekly
• Chloroquine (once a week, start 1 week before travel, continue for 4 weeks after travel)
tablet: 500 mg = 300 mg base ; Administer 5 mg base/kg/week
• Doxycycline (once a day, start 1 day before travel, continue for 4 weeks after travel)
Suspension= 50mg/5mL, tablet/capsule: 50 mg, 100 mgDose: 2.2 mg/kg/day

TRAVELER’S DIARRHEA IN CHILDREN

Diarrhea – prevention and treatment• Children are at highest risk – usually have more severe and
prolonged illness than adults• <2 yrs- high risk of dehydration• Enterotoxigenic Escherichia coli (ETEC) is the most
common cause - up to one-third of cases. • Prevention – pediatric specific
• Using alcohol-containing hand sanitizers as an alternative to soap and water when access is limited during travel.
• Milk that is pasteurized or boiled is considered safe provided that it is stored at the appropriate temperature.
• It may be necessary to bring powdered milk to mix it with safe drinking water if the quality of milk is questionable.
• Meticulous cleanliness of bottles used for formula feeding should be ensured.

Diarrhea- treatment• Mild symptoms – hydration, no diet restriction; ORT• Can give parents instructions on how to make ORT• The breast-fed infant should continue to breast feed, in
addition to receiving oral rehydration therapy• ORT- small amounts frequently – can use syringe
• ¼ teaspoon (1.25 cc) salt
• ¼ teaspoon (1.25 cc) bicarbonate of sodaa
• 2 tablespoons (30 cc) sugar
• 1 L of wateraIf bicarbonate of soda is
not available, substitute an additional ¼ teaspoon (1.25 cc) of salt.

Diarrhea- treatment• Avoid – loperamide• Avoid - bismuth subsalicylate • For children with signs and symptoms of bacterial
gastroenteritis, such as fever or blood in the stool, empiric azithromycin (10 mg/kg orally once a day for 3 days)
• Ciprofloxacin is currently not recommended for treatment of traveler’s diarrhea in children

Diarrhea- treatment• Trimethoprim–sulfamethoxazole (TMP–SMX) no longer
recommended because of increasing antibiotic resistance. • Rifaximin- for patients 12 years of age and older at a
treatment dose of 200 mg three times a day for 3 days.• Prophylaxis not routinely recommended

TRAVELLING WITH CHILDREN



Tips for parents on travel with children- plan for the worst, hope for the best
• Travel with children and infants is much more enjoyable when:• the number of journeys in a single trip is limited• travel time is kept relatively short• travel delays are anticipated.
• Planning for delays:• bring new or favorite toys or games for distraction• carrying extra food and drink• changes of clothing• fever medications

WHAT IS THE MOST COMMON CAUSE OF MORBIDITY AND MORTALITY IN TRAVELING CHILDREN?

Trauma• Rent larger, safer vehicles• Use car seats whenever possible • In many developing countries, car seats are not available,
so caretakers may need to travel with their own• Taxis often do not have seatbelts, so it may be necessary
to request taxis with seatbelts by calling in advance

Motion sickness:• Children <5 may present with gait abnormalities as well as
other more common symptoms• Tips on avoiding motion sickness:
• eating a light meal at least 3 hours before travel• avoiding dairy products and foods high in calories, protein, and
sodium before travel• sitting in the middle of the back
seat or in the front seat• focusing on a stable object or the
horizon• avoiding reading/visual stimuli• eye closure, fresh air• limiting excessive head movement

• Pharmacological interventions• diphenhydramine is recommended in children less than 12 years of
age- 0.5 to 1 mg/kg • scopolamine is acceptable for children older than 12 years of age• not evidence-based
• Ear pain: • More of an issue in infants and
toddlers• chewing, swallowing, nursing,
and bottle feeding during take-off
and landing
Other travel related problems• Altitude Sickness:
• Can be subtle in children - unexplained fussiness or change in appetite and sleep patterns
• mild symptoms - rest and hydration, or analgesics such as ibuprofen or acetaminophen
• Usually resolves much faster in children compared with adults• Acetazolamide – not been studied for AMS but is safe in this age
group, used for both prophylaxis and treatment. • 5 mg/kg/day (125 mg maximum) divided twice daily, starting 1 day
before ascent, and continued for 2 days at high altitude.

Take home points• MMR in children < 6 months of age• Meningococcal vaccine• Yellow fever, typhoid, JE vaccine• Traveler’s Diarrhea- avoid bismuth and loperamide,
azithromycin for TD treatment• Malaria prophylaxis- mefloquine preferred, better
tolerated, can give malarone down to 5kg

QUESTIONS ?Suchitra Rao
TEAM (Travel, Expedition, Altitude Medicine) Clinic
University of Colorado
Children’s Hospital Colorado

Protozoan diarrhea• Consider if diarrhea is severe, persists beyond 7 days• Ask to seek medical attention if interfering with ADL,
decreased urine output, other sx of dehydration• Can obtain stool O&P (may need up to 3 specimens)• Acute diarrhea- no therapy needed• If prolonged symptoms, consider carefully chosen empiric
therapy • Tinidazole for children > 3 years of age single dose• Unpleasant tasting, not available as liquid suspension• Nitazoxanide for children > 1 year of age – twice daily for
3 days• Excellent safety profile, strawberry flavored suspension

Hepatitis A
• Usually anicteric and mild in young children• But could be the source of infection for their parents and
adult relatives• Routine vaccination in children 12 months of age and
older, second dose months later• Infants younger than 12 months can receive
immunoglobulin at least 7 days prior to travel



![Gupto Dhoner Gujob - Suchitra Bhattacharya [Amarboi.com]](https://static.documents.pub/doc/80x56/55cf9c0c550346d033a85e8e/gupto-dhoner-gujob-suchitra-bhattacharya-amarboicom.jpg)













