35
Peer to Peer: Why and How to be Restraint Free October 10, 2007 Session AE-4 8:00 – 9:00 AM Room ___ – Convention Center
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | magdalen-gibbs |
| View: | 213 times |
| Download: | 1 times |
Peer to Peer: Why and How to be Restraint Free
October 10, 2007 Session AE-4 8:00 – 9:00 AM
Room ___ – Convention Center

Moderator: Gloria Bean, RN TMF Health Quality Institute, Austin, Texas
Speakers: Michelle Madkins, Director of Nursing
Greenville Health and Rehabilitation Center, Greenville, Texas Pam Quinn, RN, Director of Nursing
Orchard View Manor, East Providence, Rhode Island
Objectives
Discuss the QIO’s statewide work and lessons learned to reduce restraint use.
Recognize specific strategies used by providers to reduce restraint use, as well as the impact on other restraint outcome measures.
Learn how providers have specifically implemented quality improvement methodologies to reduce restraint use.
National/State QIO Efforts
Build partnerships
Provide evidence based protocols
Educate
Consult

Results Over TimePhysical Restraints in Texas and the Nation
Prepared by TMF Health Quality Institute
Data source: Quality Measure Data from Nursing Home Compare
0
5
10
15
20
25
2002
Q2
2002
Q3
2002
Q4
2003
Q1
2003
Q2
2003
Q3
2003
Q4
2004
Q1
2004
Q2
2004
Q3
2004
Q4
2005
Q1
2005
Q2
2005
Q3
2005
Q4
2006
Q1
2006
Q2
2006
Q3
2006
Q4
2007
Q1
Ave
rag
e R
estr
ain
t S
core
(%
)
Nation
Texas
7sow ipg
8sow ipg

Biggest Barriers To Being Restraint Free
“Restraints keep residents safe”
AND
“Without restraints residents will fall and fracture”

FDA SAFETY ALERT
The FDA estimates there may be at least 100 deaths or injuries annually associated with the use of restraints, many deaths occurring when the patient is trying to get out of the restraint or while attempting purposeful behavior such as going to the bathroom.
July 15, 1992

Texas trends for restraints, fractures, and fallsQuality Indicator Data, Oct. 1998 - March 2007
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
20.0%
Me
an
pro
po
rtio
n o
f p
op
ula
tio
n
Restraints
Falls
Fractures
QIO Efforts began*
Texas Trends for Restraints
Michelle Madkins, Director of NursingGreenville Health and Rehabilitation Center
Greenville, Texas
How to Be Restraint Free
The problem
Mindset that residents were safe in restraints
Didn’t know restraints were a problem
Had concerns about chemical restraints
Had 12 restraints or 13% when we started working with the QIO in 2003

Our approach
Goals
Elimination
Removal
Orders

Our most difficult case
History of broken hip
Doctor/family refusal
Resident cried in restraints
Quality of Life issue, staff faced a dilemma

Our solution
Enlisted help
Educated the family
Pursued alternatives

One of our discoveries
Bed and wheelchair alarms can be restraints.

The process we used for handling bed/chair alarms
Determine why the resident is getting up
Staff members walk residents until they are tired
For residents that can’t walk, staff check to see if they are wet or uncomfortable (assessment)

* 0% since Q4 2005
*

How we stay restraint-free
Educate new staff
Problem-solve
Keep restraints out of the building
If a physician orders a restraint, staff are required to call me

Pam Quinn, RN, Director of NursingOrchard View Manor, East Providence, Rhode Island
ORCHARD VIEW MANORPresents
Maintaining a Restraint-Free Environment
Enthusiasm is Key
YOUR STAFF WILL NOT BELIEVE IT UNLESS YOU DO!!
Decide, as a facility that no restraint is necessary.
1. Reduced restraints equal
2. Reduced incontinence
3. Reduced wounds
4. Reduced depression
5. Reduced behaviors
6. Reduced ADL decline

DATA SHOULD BE DERIVED FROM MDS QUERY – DECIDE
THAT EVEN ONE IS TOO MANY.Include:
1. Physical restraints
2. Bed against the wall
3. GERI chairs with trays
4. LAP buddies
5. Even some interventions can be restraints, if they prevent rising.
LTGDecide to have zero tolerance within six (6)
months.
STGTo evaluate each resident – one per unit, per week for reduction.

(START WITH THE “EASY’ ONES)HAVE A SOLID PLAN
Be a cheerleader:
1. Form your focus group.
2. Meet weekly for twenty (20) minutes.
3. Stay positive with a “can do” attitude.
4. If you don’t care, they wont.
5. Get families involved.
CELEBRATE SUCCESS!
1. Lots of positive feedback to staff and residents.
2. Post the data.
3. Advertise yourself as a “restraint-free” facility.

A GREAT FALLS PROGRAM IS ESSENTIAL
1. Become an expert at intervention.
2. Begin a Restorative Program with weight training.
3. Vitamin D prevents falls! New study.
4. Use the “Thirty-Nine (39) alternatives”.
5. Review every fall every day with front line staff and the resident.

HOW DID WE SUSTAIN IT?
1. By the time we were done, it was part of our culture.
2. Referring Agencies are notified.
3. Families are re-educated.
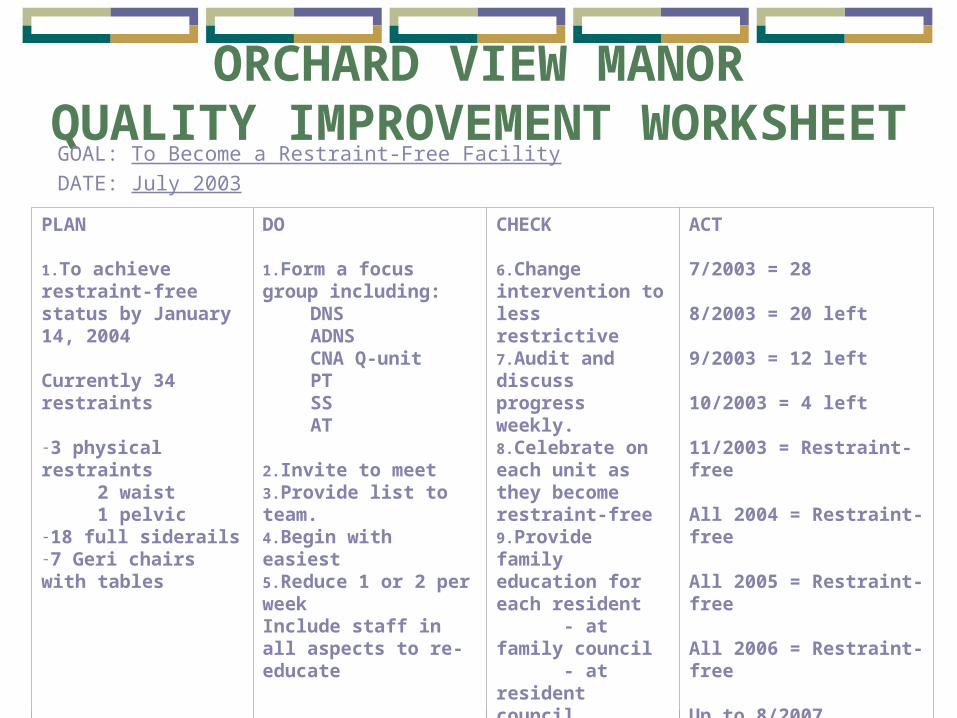
ORCHARD VIEW MANORQUALITY IMPROVEMENT WORKSHEET
GOAL: To Become a Restraint-Free Facility
DATE: July 2003
PLAN
1.To achieve restraint-free status by January 14, 2004
Currently 34 restraints
-3 physical restraints 2 waist 1 pelvic-18 full siderails-7 Geri chairs with tables
DO
1.Form a focus group including:
DNSADNSCNA Q-unitPTSSAT
2.Invite to meet3.Provide list to team.4.Begin with easiest 5.Reduce 1 or 2 per weekInclude staff in all aspects to re-educate
CHECK
6.Change intervention to less restrictive7.Audit and discuss progress weekly.8.Celebrate on each unit as they become restraint-free9.Provide family education for each resident - at family council - at resident council
ACT
7/2003 = 28
8/2003 = 20 left
9/2003 = 12 left
10/2003 = 4 left
11/2003 = Restraint-free
All 2004 = Restraint-free
All 2005 = Restraint-free
All 2006 = Restraint-free
Up to 8/2007

TIPS FOR SUCCESSFULLY AFFECTING A CHANGE
(NO MATTER HOW BIG OR HOW SMALL) 1. Form a focus group to discuss the pros & cons.
2. Keep your meeting to 20 minutes or less.
3. Let everyone have a say-there are no wrong opinions.
4. Write down the steps needed to achieve the goal or complete the project.
5. Assign tasks.
6. EDUCATE ALL WHO WILL BE AFFECTED.
7. Institute the change.
8. Audit the process for success or failure.
9. Re-assemble the focus group and revise the plan, if needed.
10. Celebrate success.

FALLS AVOIDANCE INTERVENTIONS
The following list is for alternatives to try to reduce falls:
1. PT
2. OT
3. RNA
4. Ambulation program
5. B&B program
6. Increase activities
7. Slip grip in chair
8. Slip strips on floor
9. Slipper socks
10.½ side rails for support
11.Medical work-up
12.Bladder scan

FALLS AVOIDANCE INTERVENTIONS
(CONTINUED 2)13. Monitoring of bowel status
14. Q15min checks
15. Keep in plain view of staff when OOB
16. Psych to reduce meds
17. Orthostatic signs
18. Low bed with mattress beside it
19. Caution tape @ door to room
20. Stop signs
21. Anti-tippers for the w/c
22. Extra snacks
23. Reminder ribbons for the wheelchair
24. Written instructions to the resident

FALLS AVOIDANCE INTERVENTIONS
(CONTINUED 3)25. Afternoon naps
26. Pain management
27. Encourage family to visit
28. Soothing music
29. Quiet areas on the unit
30. Take the resident outdoors
31. One-on-one
32. Avoid sleeping pills
33. Decrease caffeine intake
34. Decrease fluids after supper
35. Exercise programs
36. Raised toilet seat
37. Safe-hips

Questions?

In Summary:
10 Keys to Success
1. Make sure Administration is on board2. Educate everyone3. Create a multidisciplinary team4. Start with a small number of the easiest
residents to reduce first5. Identify medical and care issues that led to
restraint use for each individual

10 Keys to Success Cont.
6. Use comprehensive assessment to determine residents capabilities and needs
7. Review all falls daily8. Trial least restrictive interventions first9. Use increased intervals of Restraint Free time
with more difficult cases10.Document, Communicate and Celebrate
Any additional questions for our speakers?
Thank you for your attendance and participation!