A feasibility and open pilot two-arm randomised controlled trial comparing Pressure Garment Therapy with No Pressure Garment Therapy for the prevention of abnormal Scarring after burn injury PEGASUS Trial Protocol Version 2.0, 1 st October 2014 Sponsor: University Hospitals Birmingham NHS Foundation Trust Chief investigator: Mr Naiem Moiemen Coordinating Centre: Birmingham Clinical Trials unit Funder: NIHR Health Technology Assessment Programme ISRCTN: 34483199 REC Ref. No.: 14/WM/0160
Transcript
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 1
A feasibility and open pilot two-arm randomised controlled trial comparing Pressure Garment Therapy with No Pressure Garment Therapy for the prevention of abnormal Scarring after burn injury
PEGASUS Trial Protocol
Version 2.0, 1st October 2014
Sponsor: University Hospitals Birmingham NHS Foundation Trust
Chief investigator: Mr Naiem Moiemen
Coordinating Centre: Birmingham Clinical Trials unit
Funder: NIHR Health Technology Assessment Programme
ISRCTN: 34483199
REC Ref. No.: 14/WM/0160
TRIAL COMMITTEES AND CONTACT DETAILS
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 2
Trial Management Group
Chief Investigator Mr Naiem Moiemen
University Hospitals Birmingham NHS Foundation Trust, Queen Elizabeth Hospital Email: [email protected]
Co-Investigator/applicant Professor Jon Deeks
Director of Birmingham Clinical Trials Unit Email: [email protected]
Co-Investigators/applicants Professor Melanie Calvert Dr Jonathan Mathers Dr Emma Frew Dr Philip Kinghorn Dr Laura Jones
Independent Members Dr Annemarie Nelson Dr Jamie Kirkham
Marie Curie Palliative Care Research Centre, Cardiff Email: [email protected] Institute of Translational Medicine, University of Liverpool Email: [email protected]
On behalf of the Trial Management Group Mr Naiem Moiemen Professor Jon Deeks Dr Vikram Sharma Miss Sarah Reavenall Mr David Udale
University Hospital Birmingham NHS Foundation Trust, Queen Elizabeth Hospital Email: [email protected] Director of Birmingham Clinical Trials Unit, University of Birmingham Email: [email protected] University of Oxford, Clinical Genetics Research Group, Email: [email protected]) The Welsh Centre for Burns and Plastic Surgery, Email: [email protected] PPI Representative Email: [email protected]
PEGASUS RCT Office For general protocol queries relating to the RCT and supply of RCT materials:
Birmingham Clinical Trials Unit (BCTU), School of Health & Population Sciences, Public Health Building, University of Birmingham, Edgbaston,
The Chief Investigator and Sponsor have discussed this protocol and agree to abide by this
protocol and to conduct the trial in compliance with EU Good clinical Practice (GCP), the UK Data
Protection Act (1998), the Trust Information Governance Policy (or local equivalent) and the
Research Governance Framework (2005 2nd Edition; as amended).
Chief Investigator Mr Naiem Moiemen
Signature Date
Sponsor Representative
Dr Chris Counsell
Signature Date
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 6
Principal Investigator Signature Page
Principal Investigator:
I have read and agree to the protocol, as described in this document. I agree to adhere to the protocol as outlined and agree that any suggested changes to the protocol must be approved by the Trial Steering Committee prior to seeking approval from the Main Research Ethics Committee (MREC).
I am aware of my responsibilities as an investigator under the guidelines of Good clinical Practice (GCP), the declaration of Helsinki and the trial protocol and I agree to conduct the trial according to these guidelines and to appropriately direct and assist the staff under me control, who will be involved in the trial.
Principal investigator Print Name:
Signature Date
Name of Institution Print Name:
Signature Date
The Principal Investigator should sign this page and return a copy to the Pegasus Trial Office
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 7
TABLE OF CONTENTS
Principal Investigators in Participating Centres ........................................................ 4
4 PHASE 1 – QUALITATIVE RESEARCH AND PRELIMINARY SURVEYS .................. 18
4.1. Survey and Telephone Interviews with Burns Consultants and Occupational Therapists .................................................................................................................... 18
4.2. Qualitative Research with Patients and Carers ................................................. 18
4.3. Patient & Public Input .......................................................................................... 19
5 PHASE 2 – PILOT TRIAL ............................................................................................. 19
5.1. Health Technologies and Outcome Assessment .............................................. 19
5.2. Health Technologies being Assessed ................................................................ 19
5.3. Qualitative Research Pilot Trial Process Evaluation ........................................ 20
5.4. Screening and Consent of Potential Participants ............................................. 20
5.5. Inclusion and Exclusion Criteria ........................................................................ 21
5.6. Approaching Potential Participants for Consent .............................................. 21
This protocol describes the PEGASUS trial only. The trial will be conducted in accordance with the protocol, Good
Clinical Practice (GCP) and applicable regulatory requirements. Every care has been taken in the drafting of this protocol, but future amendments may be necessary, which will receive the required approvals prior to implementation.
Abbreviations
AE Adverse event
ASR Annual Safety Report
BCTU Birmingham Clinical Trials Unit
CI Chief Investigator
CRF Case Report Form
DMC Data Management Committee
GCP Good Clinical Practice
GP General Practitioner
HCP Health Care Professional
ISF Investigator Site File
ISRCTN International Standard Randomised Controlled Trial Number
MRC Medical Research Council
MREC Multi centre Research Ethics Committee
NHS National Health Service
NIHR National Institute for Health Research
OT
P1
P2
PI
PIL
Occupational Therapist
Phase 1
Phase 2
Principal Investigator
Patient Information Leaflet
PPI Patient and Public Involvement
PGT Pressure Garment Therapy
POSAS
PRO
Patient and Observer Scar Assessment Scale Patient Reported Outcomes
QoL Quality of Life
RCT Randomised Controlled Trial
ROM Range of Movement
RN Research Nurse
SAE Serious Adverse Event
SOP Standard Operating Procedure
TBSA Total Body Surface Area
TMG Trial Management Group
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 10
TSC Trial Steering Committee
VSS Vancouver Scar Scale
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 11
1 Trial Summary
Title A feasibility and open pilot two-arm Randomised controlled trial comparing Pressure Garment Therapy with No Pressure Garment Therapy for the
prevention of abnormal scarring after burn injury
Acronym PEGASUS
Type of trial The study has two overlapping Phases, P1 and P2:
The overarching aim of the project is to define the design and assess the feasibility of a full-scale randomised controlled trial of the effectiveness and cost-effectiveness of pressure garments. The aim is addressed through two interlinked Phases (P1 and P2) of feasibility work.
P1: Qualitative Research Preliminary Surveys: Web-based survey and telephone interviews with burns consultants and occupational therapists designed to explore initial opinions on willingness to randomise and identify perceived barriers to participation in a Randomised Controlled Trial. In addition, in-depth interviews and focus groups with adults, children, carers and clinicians will be used to explore patient centred outcomes and willingness to randomise. Resource use and health economic measures will also be assessed.
For participants and parents/carers of participants who are already undergoing PGT or have had previously had PGT:
In Adults (16 years and over): 8-10 completed interviews will be conducted per site (24-30 total across three sites).
Parents/carers (children aged 1-8 years): 6-8 completed interviews per site (12-16 total across two sites)
Children and young people (aged 9-15 years): There will be two discussion groups (of up to six children in each) per site: 1 x 9-11 year olds, 1 x 12-15 year olds (four discussion groups in total across two sites; two in each age group)
Results from the P1 surveys and qualitative research will be reviewed and discussed with the research team and at the burns patient and carer stakeholder panel. These discussions will help to inform the P2 trial’s patient reported outcomes, clinical and health economic measures collected during the randomised trial.
P2 Randomised Controlled Trial:
A feasibility and open pilot two-arm Randomised Controlled Trial (RCT) comparing PGT with no-PGT; the trial will assess willingness to randomise and pilot trial processes, outcomes and health economic assessments across 7 UK centres.
Adults, young persons and children can be recruited and screened for the randomised controlled trial when their burns are 90% healed, and can be randomised and commence intervention when the burns have fully healed.
Qualitative Research Pilot Trial Process Evaluation:
Participants and parents/carers of participants who are recruited to the pilot trial OR declined to participate in the trial; non-participant viewpoints, participant viewpoints, trial site staff viewpoints will be included.
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 12
Outcome measures P1 will identify outcome measures for P2. These may include:
A validated measure of scar appearance (selected from existing tools such as the Vancouver Scar Scale (VSS) and Patient Observer Scar Assessment Scale (POSAS)
Other patient centred outcomes which may include: objective measurements of scar firmness/pliability, colour and thickness, elasticity (assessed using a Cutometer), pain, itch and sensation
Pruritus
Active and passive range of movement (assessed by goniometry)
Psychological evaluations;
Return to work
Adverse events
Assessment of compliance with scar management therapy.
Measuring Quality of Life using the EQ-5D-5L, CHU-9D or PedsQL questionnaire
Trial design Open pilot 2-arm feasibility Randomised Controlled Trial
Patients who will be considered eligible for inclusion include:
Adults and Children with burn injuries > 1 % Total Body Surface Area
Those treated with split thickness skin grafts or conservatively managed burn wounds or donor sites which have taken > 2 weeks to heal
Those with potential for hypertrophic scarring
Those considered suitable for treatment with Pressure Garment Therapy
Exclusion criteria:
Potential participants will not be considered eligible for the pilot trial if they:
Cannot read, write or understand English. Since the outcomes identified from P1 may not have data collection tools in translatable versions for the future RCT, patient’s understanding of English is essential.
Have pre-existing skin conditions affecting wound healing
Have a history of keloid scarring
Have a prior allergy to Lycra or any other component of PGT
Are not, in the investigator’s opinion, suitable to participate in the trial due to clinically relevant past medical history or other pertinent factors.
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 13
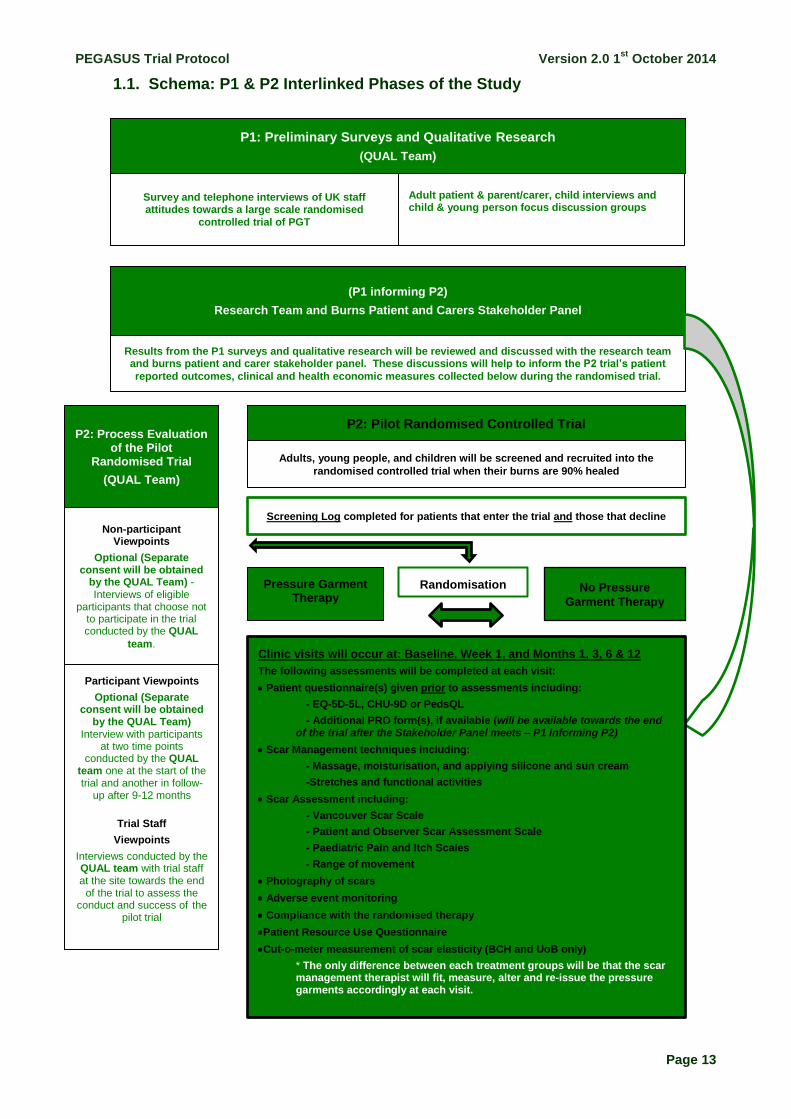
1.1. Schema: P1 & P2 Interlinked Phases of the Study
P2: Process Evaluation of the Pilot
Randomised Trial
(QUAL Team)
Survey and telephone interviews of UK staff attitudes towards a large scale randomised
controlled trial of PGT
Adult patient & parent/carer, child interviews and child & young person focus discussion groups
(P1 informing P2)
Research Team and Burns Patient and Carers Stakeholder Panel
Results from the P1 surveys and qualitative research will be reviewed and discussed with the research team and burns patient and carer stakeholder panel. These discussions will help to inform the P2 trial’s patient
reported outcomes, clinical and health economic measures collected below during the randomised trial.
Adults, young people, and children will be screened and recruited into the
randomised controlled trial when their burns are 90% healed
Randomisation Pressure Garment Therapy
No Pressure
Garment Therapy
P1: Preliminary Surveys and Qualitative Research
(QUAL Team)
P2: Pilot Randomised Controlled Trial
Screening Log completed for patients that enter the trial and those that decline
Non-participant Viewpoints
Optional (Separate consent will be obtained
by the QUAL Team) - Interviews of eligible
participants that choose not to participate in the trial conducted by the QUAL
team. Clinic visits will occur at: Baseline, Week 1, and Months 1, 3, 6 & 12
The following assessments will be completed at each visit:
Patient questionnaire(s) given prior to assessments including:
- EQ-5D-5L, CHU-9D or PedsQL
- Additional PRO form(s), if available (will be available towards the end of the trial after the Stakeholder Panel meets – P1 informing P2)
Scar Management techniques including:
- Massage, moisturisation, and applying silicone and sun cream
-Stretches and functional activities
Scar Assessment including:
- Vancouver Scar Scale
- Patient and Observer Scar Assessment Scale
- Paediatric Pain and Itch Scales
- Range of movement
Photography of scars
Adverse event monitoring
Compliance with the randomised therapy
Patient Resource Use Questionnaire
Cut-o-meter measurement of scar elasticity (BCH and UoB only)
* The only difference between each treatment groups will be that the scar management therapist will fit, measure, alter and re-issue the pressure garments accordingly at each visit.
Participant Viewpoints
Optional (Separate consent will be obtained
by the QUAL Team) Interview with participants
at two time points conducted by the QUAL
team one at the start of the trial and another in follow-
up after 9-12 months
Trial Staff
Viewpoints
Interviews conducted by the QUAL team with trial staff at the site towards the end
of the trial to assess the conduct and success of the
pilot trial
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 14
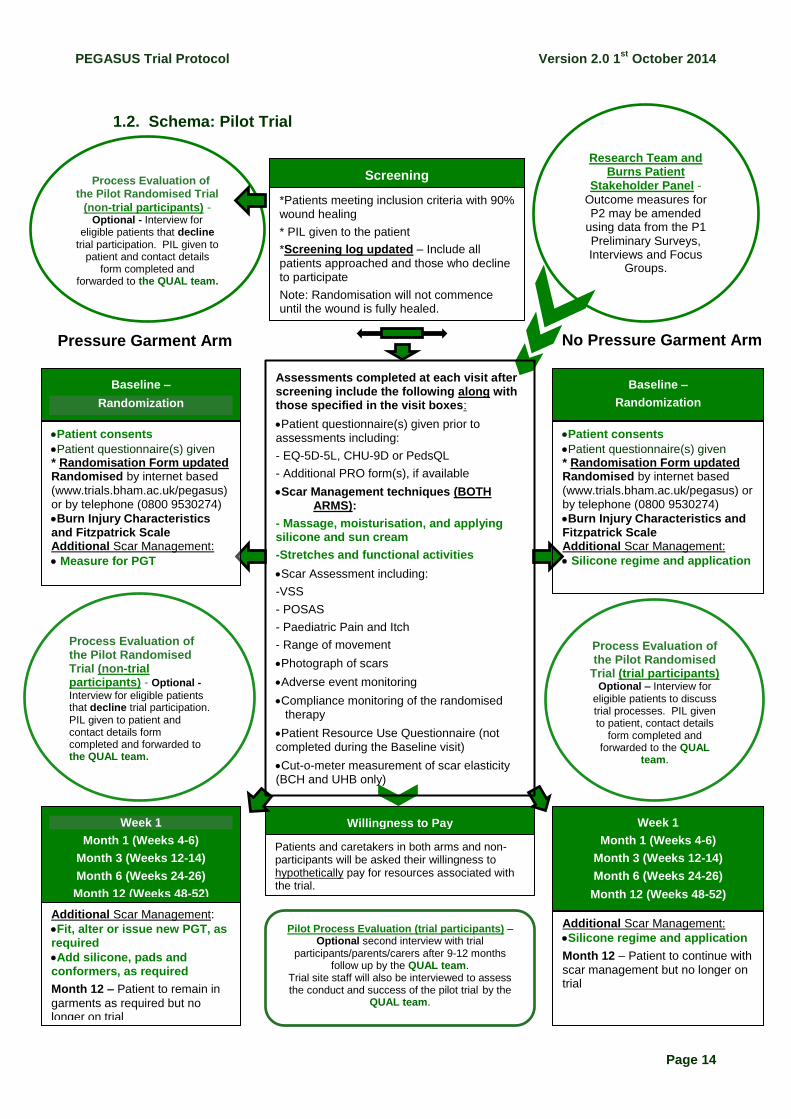
1.2. Schema: Pilot Trial
Week 1
Week 1
Week 1
Week 1
Week 1
Week 1
Week 1
Week 1 Week 1
Screening
Pressure Garment Arm No Pressure Garment Arm
*Patients meeting inclusion criteria with 90% wound healing
* PIL given to the patient
*Screening log updated – Include all
patients approached and those who decline to participate
Note: Randomisation will not commence until the wound is fully healed.
Baseline –
Randomization
Week 1
Month 1 (Weeks 4-6)
Month 3 (Weeks 12-14)
Month 6 (Weeks 24-26)
Month 12 (Weeks 48-52)
Week 1
Month 1 (Weeks 4-6)
Month 3 (Weeks 12-14)
Month 6 (Weeks 24-26)
Month 12 (Weeks 48-52)
Willingness to Pay
Patients and caretakers in both arms and non-participants will be asked their willingness to hypothetically pay for resources associated with the trial.
:
TProcess Evaluation of the Pilot Randomised Trial
(non-trial participants) - Optional - Interview for
eligible patients that decline trial participation. PIL given to
patient and contact details form completed and
forwarded to the QUAL team.
Research Team and Burns Patient
Stakeholder Panel -
Outcome measures for P2 may be amended
using data from the P1
Preliminary Surveys, Interviews and Focus
Groups.
Process Evaluation of the Pilot Randomised Trial (non-trial participants) - Optional -
Interview for eligible patients that decline trial participation. PIL given to patient and contact details form completed and forwarded to the QUAL team.
Assessments completed at each visit after screening include the following along with those specified in the visit boxes:
Patient questionnaire(s) given prior to assessments including:
- EQ-5D-5L, CHU-9D or PedsQL
- Additional PRO form(s), if available
Scar Management techniques (BOTH ARMS):
- Massage, moisturisation, and applying silicone and sun cream
-Stretches and functional activities
Scar Assessment including:
-VSS
- POSAS
- Paediatric Pain and Itch
- Range of movement
Photograph of scars
Adverse event monitoring
Compliance monitoring of the randomised therapy
Patient Resource Use Questionnaire (not completed during the Baseline visit)
Cut-o-meter measurement of scar elasticity (BCH and UHB only)
Additional Scar Management:
Silicone regime and application
Month 12 – Patient to continue with
scar management but no longer on trial
Baseline –
Randomization
Patient consents
Patient questionnaire(s) given * Randomisation Form updated Randomised by internet based
(www.trials.bham.ac.uk/pegasus) or by telephone (0800 9530274)
Burn Injury Characteristics and Fitzpatrick Scale Additional Scar Management:
Silicone regime and application
Patient consents
Patient questionnaire(s) given * Randomisation Form updated Randomised by internet based
(www.trials.bham.ac.uk/pegasus) or by telephone (0800 9530274)
Burn Injury Characteristics and Fitzpatrick Scale Additional Scar Management:
Measure for PGT
Additional Scar Management:
Fit, alter or issue new PGT, as required
Add silicone, pads and conformers, as required
Month 12 – Patient to remain in
garments as required but no longer on trial
Pilot Process Evaluation (trial participants) – Optional second interview with trial
participants/parents/carers after 9-12 months follow up by the QUAL team.
Trial site staff will also be interviewed to assess the conduct and success of the pilot trial by the
QUAL team.
Process Evaluation of the Pilot Randomised
Trial (trial participants) Optional – Interview for
eligible patients to discuss trial processes. PIL given to patient, contact details
form completed and forwarded to the QUAL
team.
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 15
2 Background
Clinical Context
Approximately 130,000 people with burn injuries visit Emergency Departments each year and approximately 10,000 are admitted to hospital. Of these, approximately 500 (5%) are admitted to hospital with a severe burn, requiring fluid resuscitation. A severe burn is considered in paediatrics as ≥10% Total Body Surface Area (TBSA) and in adult’s ≥15% TBSA. The majority of these cases will be referred and treated in a specialist Burns Centre. At the Queen Elizabeth Hospital Burns Centre, 1252 patients were admitted with varying degrees of burn severity from January 2011 to January 2014. The majority of patients (75%) present with a small burn ≤5% TBSA.
A burn injury can have a variety of aetiologies such as thermal (flash, contact, scald, radiation), electrical (low voltage, high voltage) and chemical (acid, alkali). The severity of a burn is dependent on the size and anatomical site of the injury, the depth of the burn, the age of the patient, the presence of an inhalation injury and other significant co-morbidities. All of these factors will influence morbidity and mortality.
The most common complication following burns, reported in up to 70% of patients, is hypertrophic (abnormal) scarring2-4. These develop within one to three months following burn injury. Age, ethnic group, genetic factors and burn type and depth have been implicated to affect burn healing. The main documented non-surgical approach to their prevention and treatment is pressure garment therapy (PGT) 1, 5-8. PGT involves the wearing of tight, Lycra-based garments, in direct contact with skin from when the burn wounds have healed (i.e. the skin surface intact and can tolerate pressure) until scarring has matured (characteristics of the scar approach those of the patient’s normal skin or a plateau in progress). Garments are recommended to be worn for 23 hours a day, over an average of 12 to 18 months, as scars mature at different rates in different patients. PGT is recommended if spontaneous healing takes longer than 14 days or the wound is skin grafted. As soon as the wounds are healed and can tolerate pressure, PGT is applied.
Two other important treatment modalities, however, are silicone applied to the burn (in the form of gels, sprays or sheets), and intra-lesional corticosteroid injections. These have been used independently, in conjunction with each other, and with PGT. Their exact mode of action is currently unknown. Other less studied modalities include lasers, cryotherapy, and radiotherapy2. PGT for hypertrophic burn scars was first popularised at the Shriners Galveston Burn Hospital, USA in the 1970’s5, 9. PGT has since been used as a primary measure to prevent the development of abnormal scarring, based on this and other historical experience. Garments exist in different forms and sizes and can become uncomfortable, sweaty, itchy and difficult to wear, which may lead to problems with compliance. A study of pressure garment adherence in adults has reported PGT dropout rates between 30% and 59% due to such accompanying side-effects10. The burden can also be on parents and carers. PGT is costly to the NHS in terms of i) garments (which are produced by different commercial companies, or manufactured in-house, and require regular resizing), and ii) resources (occupational therapists’/physiotherapists’ time utilised in patient/scar/garment assessment). The use of PGT has recently been questioned given a paucity of RCTs6. The only available meta-analysis in the literature of these few studies suggested that PGT only seems to reduce scar height, which is of questionable clinical importance1. Currently, there are no national or international trials that are registered.
PGT became the standard of care for patients with burns scarring based on a case series in the 1970’s9. At that time, delayed surgery was the usual practice, with wound closure being achieved well after six weeks post-injury. It has since been shown that wound closure after three weeks is associated with worse scarring11. Therefore, current surgical burns management constitutes early burn excision, aiming to achieve wound closure within two to
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 16
three weeks post-injury. PGT is still routinely prescribed based on historical practice1,5-7. With earlier surgery, it could be expected that the incidence of hypertrophic scarring, and hence the requirement for PGT, would have diminished.
PGT can be ineffective in certain areas as adequate pressure cannot be delivered (e.g. sternum, abdomen and buttocks)12. It is well documented that treatment with PGT can be complicated by physical symptoms such as pain, itching, overheating, blistering, ulceration and rashes. These can become extremely uncomfortable for patients over time. In addition PGT has been shown to present psychological complaints such as emotional distress, shame and embarrassment to wear unsightly/untrendy garments which may also impact on adherence or compliance. This may also contribute to social challenges in terms of reintegration and return to work13-15. On the other hand, PGT may improve the appearance of scarring, in particular scar height1. PGT provides the opportunity to the patient to have regular contact with and assessment by the scar therapy team which can be supportive and reassuring. This is important for patients who also require psychological support during their intensive multidisciplinary rehabilitation.
PGT is costly as it involves regular re-measuring/refitting by the physiotherapist or occupational therapist. Over the PGT period (12-24 months), patients require on average eight garments, including new garments for children as they grow, in addition to replacements and a requirement for spares. Such resizing and provision of new pressure garments can also be costly in terms of staffing time. Furthermore, PGT may represent a significant financial cost to patients and carers in terms of regular visits to the hospital for assessment (whereby the hospital may be a considerable distance away given the nature of specialised burns services being located in tertiary centres).
Although PGT is now the standard of care, the evidence of the benefits of PGT in the literature is weak and considering the cost to the patients in terms of discomfort and sometimes complications, a feasibility study of PGT is now required.
3 Study Design
The overarching aim of the project is to define the design and assess the feasibility of a full-scale open trial of the effectiveness and cost-effectiveness of pressure garments. The aim is addressed through two interlinked Phases (P1 and P2) of feasibility work.
3.1. Study Components
P1 will include survey and qualitative research approaches; work with clinicians, patients and parents/carers of child patients) will explore perspectives regarding a trial of PGT including barriers and facilitators to randomisation, and identify patient centred outcomes including patient reported outcomes (PROs) for use in P2.
P2 is afeasibility and open pilot two-arm randomised controlled trial, with a 12-month follow-up period. During an estimated 9 month recruiting period 88 participants will be recruited. Participants will be randomised to compare PGT with massage, moisturisation and silicone and no-PGT with massage, moisturisation and silicone in seven specialist burns units in the UK. In addition, a qualitative process evaluation will explore through interviews the perspectives and experience of patients, carers and clinicians participating in the pilot trial as well as patients who decline to participate. Resource use and health economic measures will also be assessed, including a willingness to pay exercise.
3.2. Objectives
There are a number of interrelated objectives for Phases 1 and 2:
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 17
P1 Objectives:
1. to understand clinicians’ and therapists’ willingness to randomise children and adults between PGT and no-PGT and identify perceived facilitators and barriers to participation in an RCT
2. to assess patient (adult and children) and parent/carer experience of PGT and assess willingness to be randomised between the two arms of the trial; either PGT or no-PGT and to identify and select patient centred outcomes
3. to identify appropriate methods for evaluating outcomes and resource use (including the selection of valid, reliable questionnaires and time points for assessment).
P2 Objectives:
4. to assess recruitment rates and willingness to randomise between PGT and no-PGT in multiple sites
5. to assess compliance with the randomised allocation, either PGT (with massage, moisturisation and silicone) or no-PGT (with massage, moisturisation, and silicone)
6. to test processes for achieving blinded assessment of outcomes 7. to assess processes for PRO data collection and levels of missing data 8. to assess participant, parent/carer and clinician perspectives on trial participation and
processes 9. to assess the use of economic measures that will inform the design of a cost-utility
analysis and cost-benefit analysis in a definitive trial.
3.3. Outcome Measures
As information on valid outcome measures from P1 of this project emerges, refinement of the outcome measures will be made as required for P2.
1. Existing outcomes considered for inclusion in P2 that will also be assessed in P1 are: validated measures of global scar appearance (Vancouver Scar Scale and Patient Observer Scar Assessment Scale); objective measurements of scar firmness/pliability, colour, thickness, elasticity (assessed using Cutometer); pain, itch, and sensation; range of movement (assessed by established methods); pruritus; psychological evaluations; return to work; and adverse events (ulceration/wound breakdown, contractures/significant loss of joint range of movement, interference with growth, intra-lesion steroid injection for aggressive hypertrophic scars, surgical intervention/scar revision).
2. Outcome measures for each of the important patient centred outcomes identified in P1 will be considered for P2. Outcomes will be assessed using validated instruments (ideally for the population under study - if not further validation work may be required), with an appropriate recall period, that are deemed acceptable by the stakeholder panel.
3. The ability to assess compliance with PGT or no-PGT at each visit will be assessed.
4. Scars will be recorded by photograph at each visit. Blinded assessment of the scar photographs will be undertaken by a panel using the photographs. The success of this blinding (it may be possible to identify indentations created by wearing pressure garments) will be assessed by comparing assessors’ estimates of group allocation with actual allocations.
5. The feasibility and acceptability of measuring QoL using the EQ-5D-5L for adults, and the CHU-9D and the PedsQL for children will be assessed during the trial.
6. We will also explore the feasibility of valuing broader sets of outcomes (including process attributes likely to be relevant to patients wearing pressure garments) through willingness to pay (WTP). Willingness to pay questions will be administered face to face to patients in both arms and we will explore: the acceptability of the method; difficulties encountered and the success of various options to enhance understanding and engagement.
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 18
7. The economic evaluation will primarily adopt an NHS perspective and will include direct treatment costs and consultation and follow-up costs. Much of the resource use data will be recorded by centre staff during the follow-up appointments (Week 1; Month 1 (weeks 4-6); Month 3 (weeks 12-14); Month 6 (weeks 24-26) and Month 12 (weeks 48-52)however the Month 12 appointment can be completed earlier if the participant’s last scar management appointment falls before this window or the trial ends). Recruitment is for 9 months. The 12 month appointment will only be completed if this date is before September 2015. Additional information will be collected using a questionnaire, self-completed by the participant and/or parent, during the follow-up appointments. The scope of the self-reported questionnaire will include some societal costs, such as time off work. The resource use questionnaires will be adapted from existing questionnaires listed on the DIRRUM website and through consultation with the study team and PPI representatives.
3.4. Setting
The trial will be carried out in seven specialist burns units in the UK. Some centres specialise in treating either adults or children, whereas others treat both.
3.5. Treatment Duration
The interventional phase of the trial will last up to 12 months. The estimated total trial duration is 24 months, participants enrolled during the later stages of the trial may not complete the full 12 months of trial visits, however the participant will continue their treatment following standard of care.
4 Phase 1 – Qualitative Research and Preliminary Surveys
4.1. Survey and Telephone Interviews with Burns Consultants and Occupational Therapists
All burns consultants, registrars, scar therapists, and senior nurses will be invited to participate in a short online (equivalent to a max 2 sides A4) survey in order to understand current attitudes toward the use of PGT in burns scar management, and in particular likely willingness to randomise and participate in a pragmatic RCT of PGT. The survey will also gather data relating to perceived facilitators and barriers to participation in an RCT through fixed response and free text questions. Respondents will be asked to indicate their willingness to participate in a supplementary telephone interview in order to provide a more in-depth understanding of the clinical perspectives described by the survey data. Telephone interviews will explore and explain current attitudes toward an RCT, variation in these, and amenability to change. A purposive sample of clinicians and scar therapists (n≈20) indicating willingness to participate during the online survey will be selected for a telephone interview. Sampling will be based, for example, on stated willingness to participate in a pragmatic RCT (e.g. willing, unwilling, undecided), associated clinical equipoise, burns unit and clinical experience (e.g. work with adults and children), and other relevant factors identified via the survey.
The findings from the survey and telephone interviews will be discussed at two focus groups including clinical staff at two of the burns centres participating in Phase 2 (pilot trial). These will provide data triangulation and allow opportunity to discuss strategies that might be used to overcome any barriers to a full scale RCT of PGT with moisturisation, massage and silicone vs no PGT with moisturisation, massage and silicone.
4.2. Qualitative Research with Patients and Carers
A maximum variation sample (n≈24-30) of adult patients will take part in face-to-face in-depth interviews. In order to reflect the broad range of adult patients that might be included in a trial of PGT , this purposive sample will include patients according to age, sex, type and
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 19
severity of burn injury (e.g. scald, flame), ethnicity and skin colour, and time since injury and completion of PGT. Interviews with parents and carers of paediatric burns patients (n≈12-16) will also be conducted. Children aged from 9-15 years will be recruited to taking part in four age-defined discussion groups (two each with 9-11 year olds and 12-15 year olds) across two burn centres. Patients will be identified and recruited via clinical networks, including support groups for patients and carers (For example, ‘Enzo’s Friends’ is a support group run by Birmingham Children’s Hospital for children, young people and their families following a burn injury).
Interviews and discussion groups will explore patients’ experience of burn injury and PGT treatment; perspectives on a clinical trial of PGT, patient-centred outcome preferences and appropriate time-points for assessment. The findings will be considered by the research team and by a burns patient stakeholder panel in order to identify suitable PRO, clinical and health economic measures to feed into the Phase 2 Pilot trial, and that align with perspectives explored in this qualitative research with patients and carers, and the survey and interview work with clinicians.
4.3. Patient & Public Input
Design and conduct of qualitative work with burns patients will be undertaken in collaboration with our burns stakeholder panel constituted of adult burns patients and parents / carers of paediatric patients. For example, the design of discussion groups with children may be assisted by members of the panel, and a local children’s play therapist. We will explore the possibility of stakeholders actively guiding and managing these sessions in conjunction with the research team.
5 Phase 2 – Pilot Trial
Large, Simple Trial: Minimal Extra Workload
In order to obtain the potentially large number of participants necessary for the reliable evaluation of PGT, the trial will need the participation of several specialist burns centres. To make this practicable, trial procedures will be kept simple, with minimal extra workload placed on participating clinicians, beyond standard care. This will be achieved by simple inclusion criteria, the use of standard local treatment regimens, and routine follow-up of participants (visits or tests to be performed as part of standard care), minimising documentation and using largely participant-based evaluation of outcome.
Following standard of practice consideration of scar management starts before the wound has healed. We will recruit participants to the trial when they have 90% healing, and will randomise and commence interventions when the participant has fully healed.
5.1. Health Technologies and Outcome Assessment
Following standard practice, consideration of scar management starts before the wound has healed. We will recruit participants to the trial when they have 90% healing, and will randomise and commence interventions when the participant has fully healed.
5.2. Health Technologies being Assessed
Participants in both arms of the trial will receive standard education concerning scar management techniques from their clinical team. Standard education involves demonstration of massage techniques, recommendation to undertake massage 3-4 times per day with moisturiser, stretching and other exercises, sun cream advice and a discussion concerning returning to normal functioning. In order to mirror both the PGT arm and the no-PGT arms of the trial will be issued with silicone products including gels, sprays or sheets. The PGT arm will be issued with silicone at Month 1 and the no-PGT arm will be issued with silicone at Week 1, or when appropriate.
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 20
Participants in the PGT with massage, moisturisation and silicone arm will receive pressure garments. These are tight, Lycra-based garments, worn in direct contact with skin from when the burn wounds have healed (i.e. the skin surface intact and can tolerate pressure) until scarring has matured Garments are recommended to be worn for 23 hours a day, over an average of 12 -18 months, as scars mature at different rates in different participants. Some hospitals purchase garments commercially, others manufacture their own. Each centre in the trial will use their standard supply route. Participants randomised to PGT will be measured for their garments after randomisation, and will return to clinic for garment fitting one week later, where any alterations are made. To avoid interruption of the application of the pressure garment for the recommended 23 hours a day, a second garment will be supplied. The fit and wear of the garments will be checked throughout the trial at the routine clinic visits, and garments replaced as required.
The PGT arm of the trial will reflect current clinical practice; the no-PGT arm differs solely through the absence of pressure garments. All participants will attend routine follow-up scheduled appointments, with additional appointments allowed (for issues such as vulnerable adults and children) in line with standard management practice in each centre. These appointments will be given to the participants as part of the standard care pathway and not as part of the trial appointments.The PGT arm of the trial will reflect current clinical practice; the no-PGT arm differs solely through the removal of pressure garments. All participants will attend routine follow-up scheduled appointments, with additional appointments allowed (for issues such as vulnerable adults and children) in line with standard management practice in each centre. These appointments will be given to the participants as part of the standard care pathway and not as part of the trial appointments.
5.3. Qualitative Research Pilot Trial Process Evaluation
In-depth interviews with key stakeholders (patients, carers, clinicians) will provide perspectives on trial participation and processes. Patients and / or carers of patients across three of the units participating allocated to either PGT (n≈4) or no-PGT (n≈4) will be interviewed at two time points (1) following allocation and (2) after 9-12 months trial participation.
Interviews (n≈20) with key trial staff in each of the units participating (burns consultants, therapists, research nurses) will be conducted 12 months after commencement of the pilot trial to provide understanding of clinical perspectives on patient recruitment and consent; accrual; integration of trial processes in clinical contexts; acceptability of allocation to treatment; compliance, and measurement of outcomes.
5.4. Screening and Consent of Potential Participants
Participants who potentially fulfil the inclusion criteria for this trial must have their eligibility confirmed by medically qualified personnel with access to, and an understanding of, the potential participant’s medical history. If eligibility has been assessed and documented by medically qualified personnel, then the process of obtaining informed consent may be delegated as appropriate. Participants can be screened for potential recruitment when 90% wound healing has occurred (visual assessment by therapist). Once their burns have fully healed, potential participants will have their eligibility confirmed via the inclusion/exclusion criteria, be consented and randomised to either the PGT arm with massage, moisturisation or silicone or no-PGT arm with massage, moisturisation and silicone. A Screening Log will be completed for all potential participants approached to join the trial; including those who declined participation.
This study will include optional consent to allow linkage to patient data available in NHS routine clinical datasets, including primary care data (e.g. Clinical Practice Research
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 21
Datalink; CPRD, The Health Improvement Network; THIN, QResearch), secondary care data (Hospital Episode Statistics; HES) and mortality data from the Office of National Statistics (ONS) through The Health and Social Care Information Centre and other central UK NHS bodies. The consent will also allow access to other new central UK NHS databases that will appear in the future. This will allow us to double check the main outcomes against routine data sources, and extend the follow-up of patients in the trial and collect long-term outcome and health resource usage data without needing further contact with the study participants. This is important as it will link a trial of treatments that may become a clinical standard of care to long-term outcomes that are routinely collected in clinical data but which will not be collected during the follow-up period of the trial.
5.5. Inclusion and Exclusion Criteria
Inclusion Criteria:
Potential participants who will be considered eligible for inclusion include:
Adults and Children with burn injuries > 1 % Total Body Surface Area
Those treated with split thickness skin grafts or conservatively managed burn wounds or donor sites which have taken > 2 weeks to heal
Those with potential for hypertrophic scarring
Those considered suitable for Scar Management Therapy
Exclusion Criteria:
Potential participants will not be considered eligible for the pilot trial if they:
Cannot read, write or understand English. Since the outcomes identified from P1 may not have data collection tools in translatable versions for the future RCT, patient’s understanding of English is essential.
Have pre-existing skin conditions affecting wound healing
Have a history of keloid scarring
Have a known allergy to Lycra or any other component of pressure garments
Are not, in the investigator’s opinion, suitable to participate in the trial due to clinically relevant past medical history or other pertinent factors.
5.6. Approaching Potential Participants for Consent
Eligibility must be assessed and confirmed prior to obtaining consent. The process of obtaining informed consent may be delegated to a suitably trained member of the local research team who is documented on the PEGASUS Delegation and Signature Log. The person obtaining informed consent will provide the potential participant with the REC approved Patient Information Leaflet (PIL) on NHS Trust headed paper. Adequate time will be given for consideration by the potential participant, and where appropriate their parent or carer before taking part. It will be explained to the potential participant or their parent/carer that there is no obligation for them to enter the trial, and that they can withdraw from the interview, discussion group, or the trial at any time, without having to give a reason. A copy of the signed informed consent form will be given to the participant or their parent/carer. The original signed form will be retained at the study site in the ISF and a copy placed in the medical notes. A copy will also be sent to the PEGASUS Trial Office. With the participant’s prior consent, their GP will also be informed using a standard letter (trial participants).
Informed consent will be obtained before any interview, discussion group, or trial-related procedures are undertaken.
The participants enrolled in this research (interviews, discussion groups, or trial) will fall into two groups: 1. Adult participants with mental capacity
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 22
2. Children (aged <16 yrs.)
Adult participants with mental capacity (MCA 2005)
For those participants who present with capacity they will be provided with the PIL; this will give them an outline of the research (interview or trial). If the participant, following a discussion with the research team, agrees to participate in the research (interview or trial), they will be asked to sign a consent form.
Children (aged <16 yrs.)
PILs have been written for different age groups to allow for different levels of communication skills and understanding. The participant will be issued with the relevant PIL and the parents or legal guardians with a more detailed information leaflet, explaining the full details of the discussion groups or trial. Parental consent will be given for each participant under the age of sixteen. Participants will be asked to also give assent to participate if they are considered able, dependent on their age and level of understanding.
5.7. Withdrawal
Participants may withdraw from the interview, discussion group or trial at any time if they choose not to continue or the responsible clinician(s) feel(s) that continued participation is inappropriate.
There are three different types of withdrawal:
The participant would like to withdraw from the randomised treatment allocation, but is willing to be followed-up according to the trial protocol (i.e. has agreed that follow-up data can be collected)
The participant does not want to complete the QoL and economic forms but has agreed to be followed-up according to standard practice (i.e. has agreed that follow-up data can be collected at standard clinic visits)
The participant is not willing to be followed up for trial purposes at any further visits (i.e. has agreed that any data collected prior to the withdrawal of consent can be used in the trial final analysis)
The participant does not wish to participate in the interview or discussion group.
The participant does not wish to participate in the interview(s) or discussion group(s) but has agreed to be continue in the trial.
The participant does not wish to participate in the interview(s) or discussion group(s) and does not want to participant in any further study activities.
If initiated by a healthcare professional the reason(s) for withdrawal will be recorded on the case report forms (CRFs); otherwise, a simple statement reflecting participant preference will suffice. Participants who withdraw from trial treatment but continue with on-going follow-up and data collection will be followed-up in accordance with the protocol.
Informing the Patient’s GP
The patient's GP will only be notified about their participation in the Phase 2 pilot RCT. A letter will be sent to the GP with the participant’s consent. The participant’s GP will not be informed about participation in the Phase 1 qualitative research.
6 Randomisation
After all eligibility criteria have been confirmed and informed consent has been obtained, the participant can be randomised into the PEGASUS trial.
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 23
The Birmingham Clinical Trials Unit (BCTU) will provide a third-party web-based randomisation service with a telephone option as back-up. Once eligibility criteria have been confirmed, consent has been obtained; and baseline QoL questionnaires have been completed participants will be randomised online via a secure internet facility in a 1:1 ratio.
Telephone and online randomisation
Participants can be randomised into PEGASUS via a secure 24/7 internet-based randomisation service (https://www.trials.bham.ac.uk/pegasus) or by telephone (number 0800 9530274).
Telephone randomisation is available Monday - Friday, 09:00-17:00. Online randomisation is available 24 hours a day, 7 days a week, apart from short periods of scheduled maintenance and occasional network problems. For the secure internet randomisation, each site and each researcher will be provided with a unique log-in username and password.
Randomisation Forms will be provided to investigators and should be completed and used to collate the necessary information prior to randomisation.
The inclusion and exclusion criteria included on the Randomisation Form must be answered before a Trial Number can be given.
Once a Trial Number has been allocated, a confirmatory e-mail will be sent to the local PI and the named RN or scar management therapist. With the participant’s permission, the GP should be notified using the standard Letter to GP provided for this purpose.
Back-up randomisation
If the internet-based randomisation service is unavailable for an extended period of time, a back-up paper randomisation service will be available from BCTU. In this instance, investigators should ring the BCTU randomisation service (0800 9530274). The randomisation list will be produced using a random length block design.
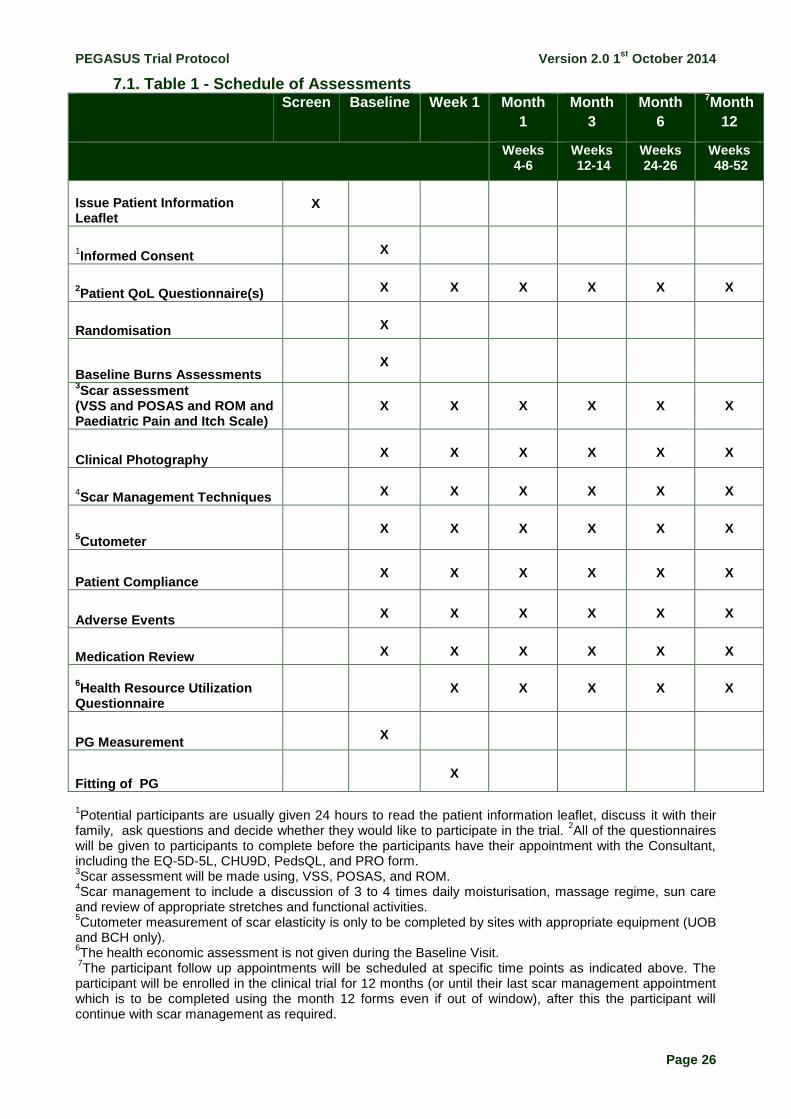
7 Study Procedures and Schedule of Assessments
QoL Questionnaire(s)
The participant (or carer/guardian) is to complete the QoL questionnaire(s) prior to completing any visit procedures. During the Baseline visit the participant will complete the QoL questionnaire after consent but prior to randomisation.
Four QoL questionnaires are available a PedsQL, a CHU-9D (child version), a CHU-9D (parent version) and EQ-5D-5L which are to be completed by the participant and/or parent/guardian depending on the participants age (See Table 3 Preference Based Questionnaires for further details).
Additional PRO form(s) may become available later in the trial after the Stakeholder Panel meets; P1 informing P2, these should be completed along with the QoL Questionnaire prior to any visit procedure being completed.
Baseline Burns Assessments
The burn injury assessment will be captured during the baseline assessment including:
1. Burn Injury Characteristics
The aetiology of the burn will be specified such as thermal (flash, contact, scald, radiation), electrical (low voltage or high voltage) or chemical (acid or alkali). The TBSA percent will be recorded.
2. Fitzpatrick Scale
The Fitzpatrick scale defining a numerical classification of skin colour will be completed.
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 24
3. Medical History
A history enquiring into any significant co-morbidities will be collected in the following categories: Neurological, Psychiatric/behavioural, Musculoskeletal, Dermatologic, and Endocrinologic.
Scar Assessment
To be completed throughout the trial by a scar management therapist on the same scars (maximum of 3 scars) that were initially suitable for PGT. The scar assessment will include three components:
1. Vancouver Scar Scale
The burn scar index will be completed documenting change in scar appearance. The same scars will be assessed throughout the trial. Any additional scars that may require a VSS assessment should be assessed following local practice and documented in the medical notes but these additional scar assessments will not be recorded in the CRFs for trial purposes.
2. POSAS
The POSAS consists of two parts: a Patient Scale and an Observer Scale. Each part contains six items that are scored numerically. The POSAS should be completed by the scar therapist and patient for each of the same scars throughout the trial.
3. Range of Movement
The range of movement of joints affected by the burn injury will be assessed by goniometry. The scar management therapist will complete goniometry for the range of movement of the hand, lower quadrant, and upper limb. Only the goniometry of joints affected by the scars being followed in the trial will be documented in the CRF. The same goniometry assessments should be completed at each visit for the affected joints of scars being followed throughout the trial.
Clinical Photography
The scar(s) being assessed at each trial visit will have a photograph taken (either with the digital camera provided by the PEGASUS trial or using medical illustration). Each of the photographs will be taken and stored securely according to standard local practice for review later by the blinded assessor(s).
Cutometer
The Cutometer assessment of elasticity will be undertaken at two sites, UHB and BCH only (see trial manual for more details).
Scar Management Techniques
The participant will be advised on scar management techniques including daily moisturisation, massage and sun care advice as per standard clinical protocol/guidelines. Additionally, appropriate stretches and functional activities to be undertaken between visits will be discussed with the participant.
For the PGT arm, the scar therapist will measure and fit the participant for pressure garments and re-issue pressure garments and add silicone, pads or conformers throughout the trial following standard local practice.
Compliance
Compliance with the randomised scar management therapy will be assessed by a few simple questions from the scar therapist during each visit for both the PGT and no-PGT arm. Any required re-education on the importance of the scar management therapy should be
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 25
discussed with the participant and documented in the medical notes according to local practice.
Adverse Events
The review of adverse events occurring since the previous visit will be recorded in the medical notes as part of routine clinical care and may also be entered onto the trial follow-up CRFs, as appropriate (see section 9).
Medication Review
Use of trial related medications will be recorded on the CRFs for the following categories:
Antihistamines
Analgesics
Mild Opioid-Analgesics
Opioids
Anti-convulsants (for pain management)
Patient Health Resource Use Questionnaire
The participant will be given the Patient Health Resource Use Questionnaire to complete at each visit (except the Baseline Visit); it can be given at any time during the visit. The form will capture many aspects of costs incurred by the participant including loss of work, fees for prescription costs and over-the-counter medication and transportation costs.
(VSS and POSAS and ROM and Paediatric Pain and Itch Scale)
X
X
X
X
X
X
Clinical Photography
X
X
X
X
X
X
4Scar Management Techniques
X
X
X
X
X
X
5Cutometer
X
X
X
X
X
X
Patient Compliance
X
X
X
X
X
X
Adverse Events
X
X
X
X
X
X
Medication Review
X
X
X
X
X
X
6Health Resource Utilization
Questionnaire
X
X
X
X
X
PG Measurement
X
Fitting of PG
X
1Potential participants are usually given 24 hours to read the patient information leaflet, discuss it with their
family, ask questions and decide whether they would like to participate in the trial. 2All of the questionnaires
will be given to participants to complete before the participants have their appointment with the Consultant, including the EQ-5D-5L, CHU9D, PedsQL, and PRO form. 3Scar assessment will be made using, VSS, POSAS, and ROM.
4Scar management to include a discussion of 3 to 4 times daily moisturisation, massage regime, sun care
and review of appropriate stretches and functional activities. 5Cutometer measurement of scar elasticity is only to be completed by sites with appropriate equipment (UOB
and BCH only). 6The health economic assessment is not given during the Baseline Visit.
7The participant follow up appointments will be scheduled at specific time points as indicated above. The
participant will be enrolled in the clinical trial for 12 months (or until their last scar management appointment which is to be completed using the month 12 forms even if out of window), after this the participant will continue with scar management as required.
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 27
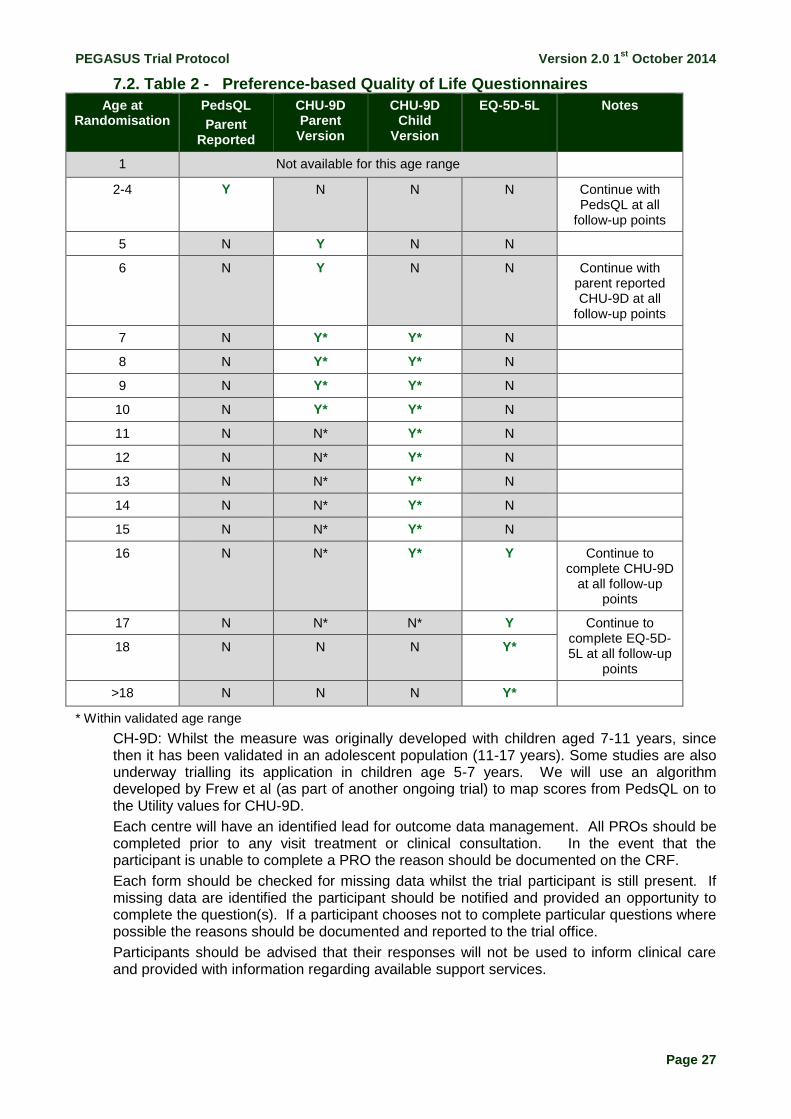
7.2. Table 2 - Preference-based Quality of Life Questionnaires
Age at Randomisation
PedsQL
Parent Reported
CHU-9D Parent
Version
CHU-9D Child
Version
EQ-5D-5L Notes
1 Not available for this age range
2-4 Y N N N Continue with PedsQL at all
follow-up points
5 N Y N N
6 N Y N N Continue with parent reported CHU-9D at all
follow-up points
7 N Y* Y* N
8 N Y* Y* N
9 N Y* Y* N
10 N Y* Y* N
11 N N* Y* N
12 N N* Y* N
13 N N* Y* N
14 N N* Y* N
15 N N* Y* N
16 N N* Y* Y Continue to complete CHU-9D
at all follow-up points
17 N N* N* Y Continue to complete EQ-5D-5L at all follow-up
points
18 N N N Y*
>18 N N N Y*
* Within validated age range
CH-9D: Whilst the measure was originally developed with children aged 7-11 years, since then it has been validated in an adolescent population (11-17 years). Some studies are also underway trialling its application in children age 5-7 years. We will use an algorithm developed by Frew et al (as part of another ongoing trial) to map scores from PedsQL on to the Utility values for CHU-9D.
Each centre will have an identified lead for outcome data management. All PROs should be completed prior to any visit treatment or clinical consultation. In the event that the participant is unable to complete a PRO the reason should be documented on the CRF.
Each form should be checked for missing data whilst the trial participant is still present. If missing data are identified the participant should be notified and provided an opportunity to complete the question(s). If a participant chooses not to complete particular questions where possible the reasons should be documented and reported to the trial office.
Participants should be advised that their responses will not be used to inform clinical care and provided with information regarding available support services.
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 28
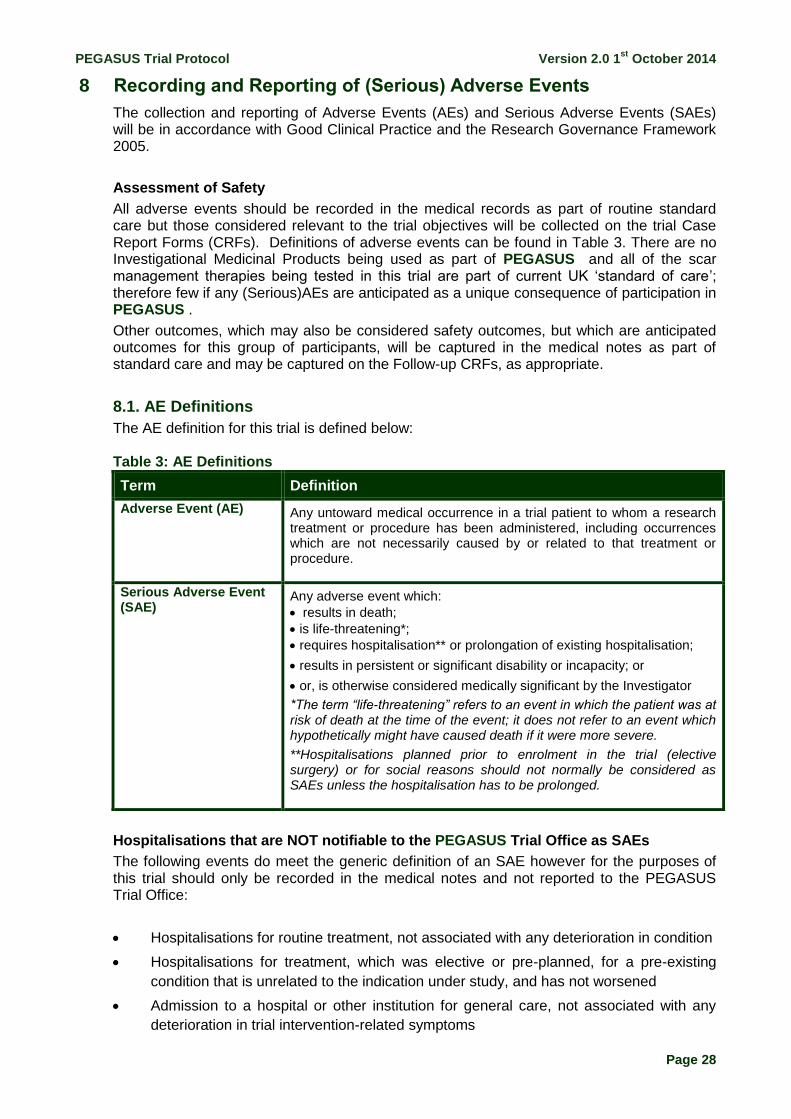
8 Recording and Reporting of (Serious) Adverse Events
The collection and reporting of Adverse Events (AEs) and Serious Adverse Events (SAEs) will be in accordance with Good Clinical Practice and the Research Governance Framework 2005.
Assessment of Safety
All adverse events should be recorded in the medical records as part of routine standard care but those considered relevant to the trial objectives will be collected on the trial Case Report Forms (CRFs). Definitions of adverse events can be found in Table 3. There are no Investigational Medicinal Products being used as part of PEGASUS and all of the scar management therapies being tested in this trial are part of current UK ‘standard of care’; therefore few if any (Serious)AEs are anticipated as a unique consequence of participation in PEGASUS .
Other outcomes, which may also be considered safety outcomes, but which are anticipated outcomes for this group of participants, will be captured in the medical notes as part of standard care and may be captured on the Follow-up CRFs, as appropriate.
8.1. AE Definitions
The AE definition for this trial is defined below:
Term Definition
Adverse Event (AE) Any untoward medical occurrence in a trial patient to whom a research treatment or procedure has been administered, including occurrences which are not necessarily caused by or related to that treatment or procedure.
Serious Adverse Event (SAE)
Any adverse event which:
results in death;
is life-threatening*;
requires hospitalisation** or prolongation of existing hospitalisation;
results in persistent or significant disability or incapacity; or
or, is otherwise considered medically significant by the Investigator
*The term “life-threatening” refers to an event in which the patient was at risk of death at the time of the event; it does not refer to an event which hypothetically might have caused death if it were more severe.
**Hospitalisations planned prior to enrolment in the trial (elective surgery) or for social reasons should not normally be considered as SAEs unless the hospitalisation has to be prolonged.
Hospitalisations that are NOT notifiable to the PEGASUS Trial Office as SAEs
The following events do meet the generic definition of an SAE however for the purposes of this trial should only be recorded in the medical notes and not reported to the PEGASUS Trial Office:
Hospitalisations for routine treatment, not associated with any deterioration in condition
Hospitalisations for treatment, which was elective or pre-planned, for a pre-existing
condition that is unrelated to the indication under study, and has not worsened
Admission to a hospital or other institution for general care, not associated with any
deterioration in trial intervention-related symptoms
Table 3: AE Definitions
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 29
Treatment on an emergency, outpatient basis for an event not fulfilling any of the
definitions of serious given above and not resulting in hospital admission.
8.2. Recording and Assessment of Adverse Events and Serious Adverse Events
Most of the (S)AEs occurring in PEGASUS will be ‘expected’ in the sense that they are recognised and accepted complications/consequences of a burn injury. All (S)AEs will therefore continue to be recorded in the medical records according to local practice as part of routine clinical care.
From randomisation through to the completion of the trial intervention follow-up period those relevant to trial participation (and detailed below) will also be recorded on the relevant CRFs and forwarded to the PEGASUS Trial Office.
AEs to be Notified on the Follow-up CRFs
Adverse events of relevance to this trial are listed below:
Wound break down
Infection
Skin rash
Itch
Blisters
Allergic reaction to component of pressure garment fabric
Ulceration
Contractures (Significant loss of ROM)
Interference with growth
Intra-lesion steroid injection for aggressive hypertrophic scars
Surgical intervention as a complication of the burn injury
Scar revision
“Expected” SAEs to be Notified on an SAE Form
If any of the above events progress to meet the criteria of being of being defined as ‘serious’, as detailed in Table 3 above, these should then be reported on an SAE Form. ‘Expected’ SAEs will not require expedited notification to the PEGASUS Trial Office.
“Unxpected” SAEs to be Notified on an SAE Form in an Expedited Timeframe
For any SAEs not encompassed in the definition of “expected” (above), an SAE Form should be completed and faxed to the PEGASUS Trial Office within 24 hours of the site becoming aware of the event. An assessment of relatedness and expectedness to the trial intervention will be performed, based on all available information at the time.
SAE Forms requiring expedited notification should be faxed to the PEGASUS Trial Office on
0121 415 9135.
Note: Death from any cause should be reported on an SAE Form and returned to the PEGASUS Trial Office.
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 30
8.3. Notification Timeframes and Procedures
All SAEs require notification on an SAE Form (as detailed above) to the PEGASUS Trial Office, but only those SAEs which have not been defined as expected have to be so within 24 hours of a site becoming aware of the event; these will immediately be referred to the CI or delegated deputy. All SAEs will be followed up until the final outcome is determined (even if that continues after the end of the planned follow-up period).
Site Investigators should also report any SAEs as required by their own institutional policies.The PI at each site will be required to respond to any related queries raised by the PEGASUS Trial Office as soon as possible.
8.4. Expedited reporting to the Research Ethics Committee
SAEs categorised as both suspected to be related to trial participation and unexpected will be subject to expedited reporting to the REC. The CI (or delegated deputy) will undertake urgent review of all such SAEs and may request further information immediately from the clinical team at site. The CI will not overrule the causality, expectedness or seriousness assessment given by the site PI but may add additional comment on these. Related and Unexpected SAEs will be notified to the REC by the PEGASUS Trial Office within 15 days after the Trial Office has been notified. The PEGASUS Trial Office (on behalf of the CI) will inform all PIs of relevant information about SAEs that could adversely affect the safety of participants.
In addition, at regular time points, the Trial Steering Committee will be provided with details of all SAEs.
8.5. Annual Progress Reports
An annual progress report will be submitted to the REC within 30 days of the anniversary date on which the favourable opinion was given, and annually until the trial is declared ended.
8.6. Reporting Urgent Safety Measures
If any urgent safety measures are taken, the CI / BCTU shall immediately, and in any event no later than three days from the date the measures are taken, give written notice to the REC of the measures taken and the circumstances giving rise to those measures.
8.7. Notification of Serious Breaches of GCP and/or the Protocol
A “serious breach” is a breach which is likely to effect to a significant degree:
a) the safety or physical or mental integrity of the patients of the trial; or
b) the scientific value of the trial.
The BCTU on behalf of the Sponsors shall notify the MREC in writing of any serious breach of:
c) the conditions and principles of GCP in connection with the trial; or
d) the protocol relating to the trial, as amended from time to time, within 7 days of
becoming aware of that breach.
The Sponsor will be notified immediately of any case where the above definition applies during the trial conduct phase.
9 Data Management and Quality Assurance
9.1. Confidentiality
All data will be handled in accordance with the UK Data Protection Act 1998.
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 31
The CRFs will not bear the participant’s full name. The participant’s initials, date of birth and trial number, will be used for identification.
9.2. Data Collection
All outcome assessments will be completed as far as possible at clinically indicated, hospital visits. Outcomes will be assessed at Baseline, Week 1, and Months 1, 3, 6 and 12 as outlined in Tables 1 and 2. The 12 Month visit assessments will be completed at the participant’s last visit ideally at 12 months but the forms may be completed prior if the participant’s treatment schedule requires it.
The CRFs will comprise, but will not necessarily be limited to, the following forms (Table 4):
Table 4: Form Table
Form Name Schedule for Submission
Screening Log Weekly
Randomisation Form Collected at randomisation
Basline As soon as possible after each visit
Follow Up (Week 1, Month(s) 1, 3, 6 & 12) As soon as possible after each visit
Serious Adverse Event (SAE) Form Faxed within 24hrs of research staff site becoming aware of event
Health Resource Utilization Questionnaire As soon as possible after each visit
Outcomes will be collected by delegated PEGASUS trial staff and entered either onto paper CRFs or directly into the online trial database via http://www.bctu.bham.ac.uk/pegasus. Authorised staff at participating sites will require an individual secure login username and password to access this online data entry system. The PEGASUS Trial Signature & Delegation Log will identify all of those personnel with the responsibility of data collection. It will be the responsibility of the investigator to ensure the accuracy of all data entered in the CRFs.
9.3. Data Handling and Analysis
If data are being collected on paper CRFs, these must be completed, signed/dated and returned to the PEGASUS Trial Office by the PI or an authorised member of the site research team (as delegated on the PEGASUS Trial Signature & Delegation Log) within the timeframe listed in the table above. Entries on paper CRFs should be made in ballpoint pen, in black ink, and must be legible. Any errors should be crossed out with a single stroke, the correction inserted and the change initialled and dated. If it is not obvious why a change has been made, an explanation should be written next to the change. Data reported on each CRF should be consistent with the related source data or the discrepancies should be explained. If information is not known, this must be clearly indicated on the CRF. All sections should be completed; all missing and ambiguous data will be queried. In all cases it remains the responsibility of the PI to ensure that the CRF has been completed correctly and that the data are accurate.
CRFs may be amended by the PEGASUS Trial Office, as appropriate, throughout the duration of the trial. Whilst this will not constitute a protocol amendment, new versions of the CRFs must be implemented by participating sites immediately on receipt.
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 32
10 Archiving
Archiving will be authorised by the BCTU on behalf of the Sponsor following submission of the end of trial report. PIs are responsible for the secure archiving of essential trial documents (for their site) as per their NHS Trust policy. All essential documents will be archived for a minimum of 5 years after completion of trial. Destruction of essential documents will require authorisation from the BCTU on behalf of the Sponsor.
11 Statistical Considerations
As this is a feasibility study, no single primary outcome is specified a priori. Instead, this study will involve the identification and/or design of valid primary outcome measures through the Phase 1 work. Once appropriate measures are identified, the characteristics of their distributions (e.g. means and standard deviations) will be used to inform sample size estimates for the full trial. The primary outcomes will not be analysed using hypothesis testing as this study is not formally powered to address these questions16.
A list of parameters to be analysed will be developed through the Phase 1 work. The data analysis plan will be reviewed and approved by the Trial Steering Committee (TSC). Any amendments to the original plan will be approved, recorded and justified in any final report. Analysis of results will be performed by the trial statistician and will be based on treatment code only. The correspondence between actual treatment arm and the assigned code will be revealed only on completion of all analyses.
The trial will conform to CONSORT recommendations17. Analysis will be on an intention-to-treat basis. Statistics will be analysed using SAS (SAS Institute Inc., Cary, NC, USA) and R (R Foundation for Statistical Computing, Vienna, Austria).
11.1. Statistical Analysis
The intervention arm (no-PGT) will be compared against the control (PGT) for all primary analyses. The analysis will be by intention-to-treat. Data will be gathered on all subjects randomised, irrespective of compliance with the treatment protocol. If there are a substantial number of protocol violations, a separate per-protocol (secondary) analysis will be conducted.
Summary statistics will be provided for baseline data and outcome data. The distributions of continuous variables will be examined and tested for normality using Shapiro-Wilk tests. If normally distributed, summaries will consist of means and standard deviations. If not normally distributed, summaries will consist of medians and inter-quartile ranges. Categorical data will be summarised by proportions or percentages. Data will also be summarised on the numbers of participants recruited and of those participants lost to follow-up. The progression of participants through the trial will be summarised using a CONSORT diagram17.
For dichotomous outcomes, analysis results will be calculated as Risk Ratios (RR) with corresponding 95% confidence intervals. For continuous outcomes, the mean differences or ratios will be used as appropriate. For the main outcomes, 95% confidence intervals around the point estimates of treatment effects will be reported, but no formal hypothesis testing will be performed.
Any imbalance between treatment and control arms will be addressed by the use of linear or logistic regression as appropriate. Potential multivariable analyses will be considered, but will most likely be limited by the relatively small projected sample size.
Missing data will be adjusted for by the use of multiple imputation.
11.1.1 Handling Missing Data
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 33
11.2. Sub-group Analysis
Subgroup analyses will be performed to compare outcomes, following the Phase 1 work, between children and adults, patients with different types of burn, patients with different severity of burn (%TBSA) and the body regions affected by the burn.
12 Analysis of Survey and Qualitative Data
12.1. Analysis of Interview and Focus Group Data
Interviews and focus groups will be recorded with the consent of patients and transcribed clean for analysis. Analysis will be conducted within the qualitative research team (Mathers, Jones, and Wright) and in conjunction with the PPI burns stakeholder panel, with reference to recordings, transcripts and field notes taken at the time of data collection. A thematic analysis of content will be informed by the Framework analytical approach. Following initial familiarisation with the interview and focus group data, development of thematic frameworks and data coding will proceed in an iterative manner. A priori analytical questions will include; what are current perspectives on PGT amongst the clinical community?; what are clinical attitudes toward a trial of PGT?; are there barriers to the conduct of a pilot and /or pragmatic RCT of PGT, and are these amenable to change?; what are patient and carer perspectives on important outcomes related to burns treatment, scar management and PGT use?; and will patients participate in a trial of PGT? Thematic charts / grids will be used to aid interrogation of patterning within the qualitative data. Analysis and discussion within the qualitative team and in partnership with the stakeholder PPI panel will provide multiple perspectives on the data during the development of this thematic analysis. Data collection and analysis will run concurrently so that emergent analytical themes can inform further data collection, and particularly comparative analytical questioning amongst the clinical community and with reference to patient and carer perspectives.
12.2. Analysis of Survey Data
The online survey data will be analysed using simple descriptive statistics for fixed categorical responses and simple directed content analysis approaches for free text data.
12.3. Qualitative Data protection and Handling
Data will be collected and retained in accordance with the Data Protection Act 1998. Interview and focus group audio recordings will be held securely on encrypted and password protected computers and networks. Recordings will be transcribed by professional transcription services that have existing data confidentiality agreements with the University of Birmingham, and appropriate data security arrangements. Data will be marked with a unique study ID. All personal identifiers will be removed from hard copy interview transcripts. All qualitative data will only be accessed by the members of the research team.
13 Direct Access to Source Data
The investigator(s)/institution(s) will permit trial-related monitoring, audits and REC review, providing direct access to source data/documents. Trial participants will be informed of this during the informed consent discussion and will consent to provide access to their medical notes.
14 Ethics
The Sponsor will ensure that the trial protocol, PIL, consent forms, GP letter and submitted supporting documents have been approved by the REC, prior to any potential participant recruitment. The protocol, and all substantial amendments, will be documented and submitted for ethical approval prior to implementation.
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 34
Before a site can enrol potential participants into the trial, the PI or designee must apply for and be granted NHS permission from their Trust (R&D). It is the responsibility of the PI (or designee) at each site to ensure that all subsequent amendments gain the necessary approval. This does not affect the individual clinician’s responsibility to take immediate action if thought necessary to protect the health and interest of individual participants. Within 90 days after the end of the trial, the CI/Sponsor will ensure that the REC is notified that the trial has finished. If the trial is terminated prematurely, those reports will be made within 15 days after the end of the trial. The CI will supply the Sponsor with a summary report of the clinical trial, which will then be submitted to the REC within one year after the end of the trial.
15 Monitoring Requirement for the Trial
Monitoring of PEGASUS will ensure compliance with GCP. A risk proportionate approach to the initiation, management and monitoring of PEGASUS will be adopted and outlined in the trial-specific risk assessment.
16 Oversight Committees
Trial Management Group (TMG)
The TMG will comprise the CI, other lead investigators (clinical and non-clinical) and members of the BCTU. The TMG will be responsible for the day-to-day running and management of PEGASUS. It will convene at least once a month, and more frequently when required.
Trial Steering Committee (TSC)
An independent TSC will provide overall supervision for PEGASUS and advice to the CI. The ultimate decision regarding the feasibility of the trial lies with the TSC. Further details of TSC functioning are presented in the TSC Charter.
17 Finance
This project was funded by the National Health Research’s Health Technology Assessment Programme (project number 12/145/04)
18 Indemnity
This is a clinician-initiated study. ABPI guidelines for participants compensation by the pharmaceutical industry will not apply. As this clinical trial is being carried out in a hospital setting, NHS Trust and Non-Trust Hospitals have a duty of care to participants treated, whether or not the participant is taking part in a clinical trial. Compensation is only available via NHS indemnity in the event of clinical negligence being proven.
Participants who sustain injury and wish to make a claim for compensation should do so in writing in the first instance to the Chief Investigator, who will pass the claim to the Sponsor’s Insurers, via the Sponsor’s office.
Hospitals selected to participate in this trial shall provide clinical negligence insurance cover for harm caused by their employees and a copy of the relevant insurance policy or summary should be provided to University of Birmingham, upon request.
19 Dissemination and Publication
Regular newsletters will keep collaborators informed of trial progress, and regular meetings will be held to report progress of the trial and to address any problems encountered in the conduct of the study.
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 35
The CI will coordinate dissemination of data from PEGASUS. The results of the analysis will be published in the name of the PEGASUS Collaborative Group in a peer reviewed journal (provided that this does not conflict with the journal’s policy). All contributors to the trial will be listed, with their contribution identified. Trial participants, if requested, will be sent a summary of the final results of the trial, which will contain a reference to the full paper. Statement of Compliance
The trial will be conducted in compliance with the approved protocol, the principles of Good
Clinical Practice (GCP), the UK Data Protection Act and the National Health Service (NHS) Research Governance Framework for Health and Social Care (RGF).
PEGASUS Trial Protocol Version 2.0 1st
October 2014
Page 36
20 References
1. Anzarut A, Olson J, Singh P et al. The effectiveness of pressure garment therapy for the prevention of abnormal scarring after burn injury: a metaanalysis. J Plast Reconstr Aesthet Surg 2009;62:77–84. 2. Bloemen MCT, van der Veer WM, Ulrich MMW, et al. Prevention and curative management of hypertrophic scar formation. Burns 2009;35:463-475. 3. McDonald WS, Deitch EA. Hypertrophic skin grafts in burned patients: a prospective analysis of variables. J Trauma 1987;27:147e50. 4. Bombaro KM, Engrav LH, Carrougher GJ. What is the prevalence of hypertrophic scarring following burns? Burns 2003;29:299–302. 5. Linares HA, Larson DL, Willis-Galstaun BA. Historical notes on the use of pressure in the treatment of hypertrophic scars or keloids. Burns 1993;19:17–21. 6. Engrav LH, Heimbach DM, Rivara FP, et al. 12-Year within-wound study of the effectiveness of custom pressure garment therapy. Burns 2010;36:975-983. 7. Parks DH. History of pressure garments. In: Engrav LH, editor. Houston;2009 8. Ward RS. Pressure therapy for the control of hypertrophic scar formation after burn injury. A history and review. J Burn Care Rehabil 1991;12:257-262. 9. Larson DL, Abston S, Evans EB, Dobrkovsky M, Linares HA. Techniques for decreasing scar formation and contractures in the burned patient. J Trauma 1971;11:807–23 10. Ripper S, Renneberg B, Landmann C, et al. Adherence to pressure garment therapy in adult burn patients. Burns 2009;35:657-664 11. Deitch EA, Wheelahan TM, Rose MP, et al. Hypertrophic burn scars: analysis of variables. J Trauma 1983;23:895–898 12. Macintyre L, Gilmartin S, Rae M. The Impact of Design Variables and Aftercare Regime on the Long-Term Performance of Pressure Garments. J Burn Care Res 2007;28:725–733 13. Macintyre L, Baird M. Pressure garments for use in the treatment of hypertrophic scars—a review of the problems associated with their use. Burns 2006; 32:10–15 14. Stoddard FJ, Ronfeldt H, Kagan J, et al. Young burned children: the course of acute stress and physiological and behavioral responses. Am J Psychiatry 2006;163:1084-90 15. Johnson J, Greenspan B, Gorga D, et al. Compliance with pressure garment use in burn rehabilitation. J Burn Care Rehabil 1994;15:180-188
16. Lancaster, G. A., Dodd, S. and Williamson, P. R. (2004), Design and analysis of pilot studies: recommendations for good practice. Journal of Evaluation in Clinical Practice, 10: 307–312.
17. Schulz, K.F., Altman, D.G., Moher, D. and Group, C. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. International Journal Of Surgery. 2011; 9(8): 672-7.