40
PENDRED SYNDROME Dr.Yassin M Alsaleh
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | yassin-alsaleh |
| View: | 209 times |
| Download: | 0 times |

PENDRED SYNDROMEDr.Yassin M Alsaleh


• 10 year old boy case of chronic osteomylitis, deafness, found to have goitre .
• Lab: showed euthyrodsim.
• Biopsy: showed follicular carcinoma.
• gene for SLC26A4 : negative.
Case scenario

• Pendred syndrome is an autosomalrecessive disorder characterized by congenital sensorineural deafness, goitre, and impaired iodide organification.
Introduction

History
• In 1896 Vaughan Pendredfirst described Pendredsyndrome as a combination of congenital deafness and goiter.
• Although this disease was described more than a hundred years ago.
• it remains unknown to most physicians in clinical practice, and its diagnosis is certainly often missed.
Introduction
• estimated incidence : 7.5 to 10 in 100,000 .
• This disorder may account to approximately 10% of the cases of hereditary deafness.
• Most common cause of syndromicdeafness
Epidemiology

Genetics
• Pendred syndrome is inherited as an autosomal recessive trait .
• in many families consanguinity is present.
• The phenotype of Pendred patients, can vary within and between families

• Pendred syndrome is caused by mutations in the SLC26A4 gene (PDS gene) .
• The gene is located at chromosome 7 .
• Gene encodes a protein (pendrin) that functions as a chloride, iodide transporter
• Up to now , more than 100 different mutations in the PDS gene have been discovered
Genetics
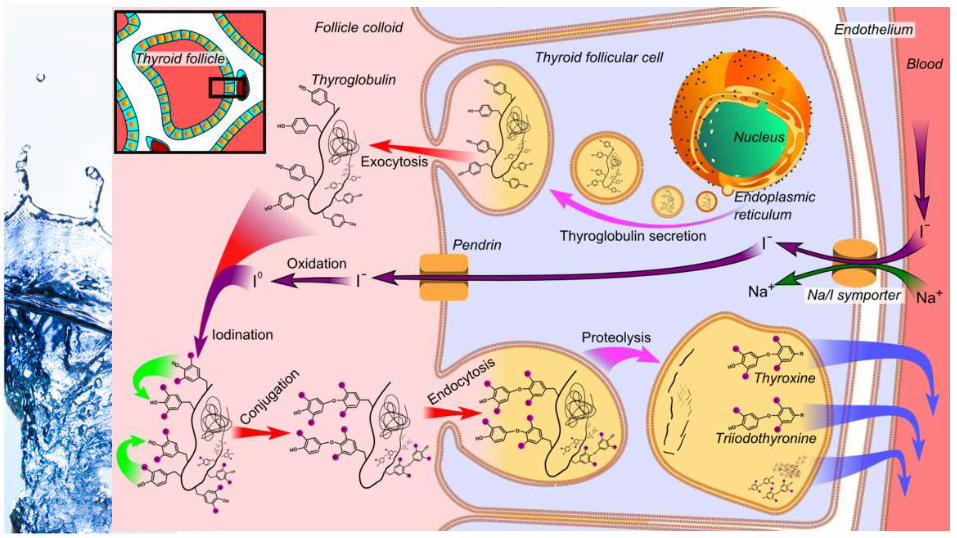


• In the absence of the transporter, iodine is taken up normally by the thyrocyte, but is not efficiently bound to thyroglobulin in the colloid.
• gene is expressed in the thyroid gland, the inner ear, and the kidney.
• Mutations in the SLC26A4 cause not only classical PS but also an autosomal recessive form of isolated deafness without thyroid disease.
Genetics

• The mechanisms involved in goiter formation in PS are not completely understood
• It may include :• transient increases in serum TSH in
response to low thyroid hormone synthesis due to less efficient organification of iodide
• increased iodide retention in thyrocytes.
Pathophysiology (goitre)

• increased deiodinase activities in goiters of PS patients and the resulting increased intrathyroidalconversion of T4 into T3
Pathophysiology (euthyroidism)

• hearing impairment is the leading manifestation .
• Always bilateral.• although one ear may be more
severely affected than the other .• The hearing impairment is of the
sensorineural type and is usually severe.
presentation

• It is usually already present at birth
• typically comes to medical attention through the absence or marked delay of language development (prelingually deaf).
presentation

• the other characteristic feature of Pendred syndrome is thyroid involvement, with goiter and hypothyroidism.
• A defect of thyroid hormone synthesis impairs the transport of iodide from thyroid cells into the colloid.
presentation
• the thyroid abnormality is of highly variable severity,
• it may be absent when the hearing impairment is first diagnosed.
presentation

presentation
• most Pendred patients develop a goiter during adolescence or adulthood.
• Although neonates with Pendredsyndrome rarely have goitre.
• approximately 75% of affected persons will eventually develop a multinodular or diffuse goiter
• Patients are usually euthyroid.

• Sometimes the goiter is large enough to cause tracheal compression.
presentation

diagnosis
hearing impairment
euthyroid or hypothyroid
goiter
Organificationdefect
• The conclusive evidence of Pendredsyndrome:
• Disease-producing mutations in both alleles of the SLC26A4/PDS gene in a person with hearing impairment and thyroid pathology (goiter and/or hypothyroidism)
Diagnostic criteria for Pendred syndrome

LAB
• thyroid-stimulating hormone (TSH). H,N.
• free thyroxine (fT4).N,L.
• the serum thyroglobulin .H,N.
Imaging
• computed tomography (CT) or magnetic resonance tomography (MRT) :
• reveals an enlarged vestibular aqueduct (EVA) in 85% to 100% of cases .
• Mondini deformity in Approximately 20%.

• They have a type of cochlear malformation known as a Mondinidefect (cochlea).
• A Mondini malformation is characterized by 1.5 coils instead of 2.5 coils.
Imaging
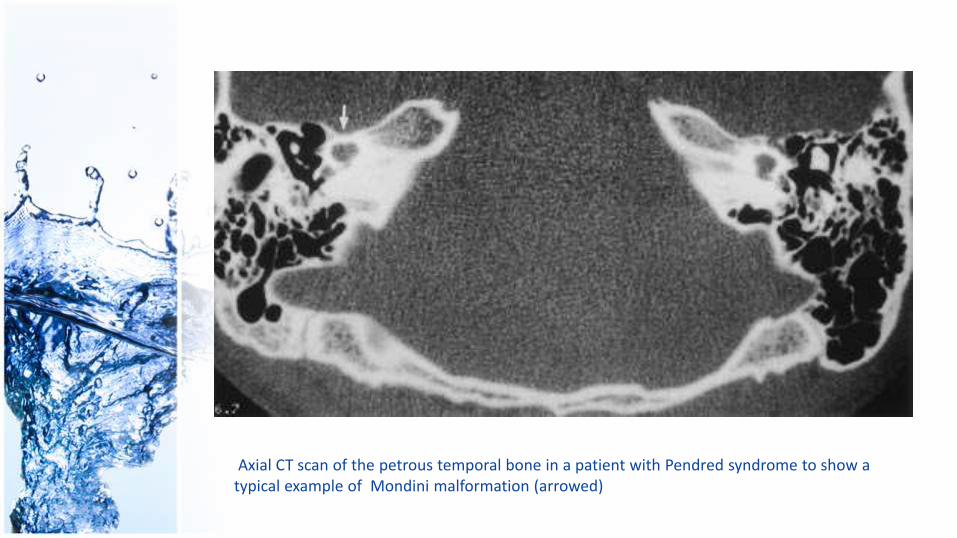
Axial CT scan of the petrous temporal bone in a patient with Pendred syndrome to show a typical example of Mondini malformation (arrowed)

• thyroid ultrasonography :
• thyroid volume .
• any cysts .
• inflammatory or malignant diseases of the thyroid gland.
• Annually US.
Imaging

• test is no more criteria for the diagnosis.
• In Pendred syndrome, as in other defects of thyroid hormone synthesis, the test is typically positive.
• is neither 100% specific nor 100% sensitive.
• This test, therefore, is increasingly being replaced by molecular genetic analysis
perchlorate discharge test
• Perchlorate inhibits NIS function (sodium iodine symporter) eliminating the iodine gradient which is required for maintaining the iodine in the gland.
• This will results in a partial discharge of radiolabelled iodide from the thyroid.
• indicating an impaired organification.
perchlorate discharge test

perchlorate discharge test• In this test, radioactive iodide (I123) is given
orally .• One hour later, perchlorate 600 mg
intravenously is administered.• diffusion of inorganified iodine from the
thyroid gland is measured as a drop in thyroid counting rate.
• An abnormal result is defined as a release of >20% of the radioactive iodide taken up by the thyroid gland.
• there are rare, usually sporadic cases of Pendred syndrome in which no mutations are found.
• This implies that other genetic causes of Pendred syndrome may be implicated.
Molecular diagnosis

Differential
• It has been recently demonstrated that some families with features of PDS do not have the inner ear malformations and mutations in the PDS gene.
• This condition has been named as “pseudo-Pendred syndrome” (pseudo-PDS), and has been hypothesized to
• be of autoimmune origin.

• Although patients with TPO defect do not usually have deafness, some cases with both TPO defect and hearing loss, have been reported
Differential

Malignant potintial• Patient with Dyshormonogenetic
goiters may undergo malignant transformation probably due to prolonged stimulation by thyrotropin.
• In Pendred syndrome, the incidence of thyroid cancer is estimated to be about 1%.
• The most common histology of the thyroid cancers arising from dyshormonogenetic goiters in patients with Pendred syndrome is follicular carcinomas .
• follicular variant of papillary thyroid carcinoma also reported.
• This is why the thyroid gland should be periodically followed up with US.
Malignant potintial

treatment• optimal treatment of patients with Pendred
syndrome requires collaboration of :• Pediatricians. • Endocrinologists.• Geneticists.• phoniatrists/pediatric audiologists. • ENT specialists.• and neuroradiologists.
Take home message
• regular follow-up by using thyroid imaging is advicable in patients with Pendred syndrome.















![Annals of Clinical Case Reports Short Communication · Pendred syndrome is the syndrome that should not be forgotten in differential diagnosis of hypothyroidism [1]. If there is hearing](https://static.documents.pub/doc/80x56/60ba76ce3f3f2c466e248320/annals-of-clinical-case-reports-short-pendred-syndrome-is-the-syndrome-that-should.jpg)


