92
F. Borghi PERCORSO DELLA CHIRURGIA COLO-RETTALE
| Date post: | 16-Feb-2019 |
| Category: |
Documents |
| Upload: | trinhtuyen |
| View: | 216 times |
| Download: | 0 times |

F. Borghi
PERCORSO DELLA CHIRURGIA
COLO-RETTALE

2010: PROCESSO DI ACCREDITAMENTO REGIONALE DEI TUMORI
COLO-RETTALI.
BACKGROUND
F. Borghi
2009: REVISIONE LETTERATURA PER STESURA PDTA

F. Borghi
BACKGROUND:
PIEMONTE - VOLUME TM COLON
F. Borghi
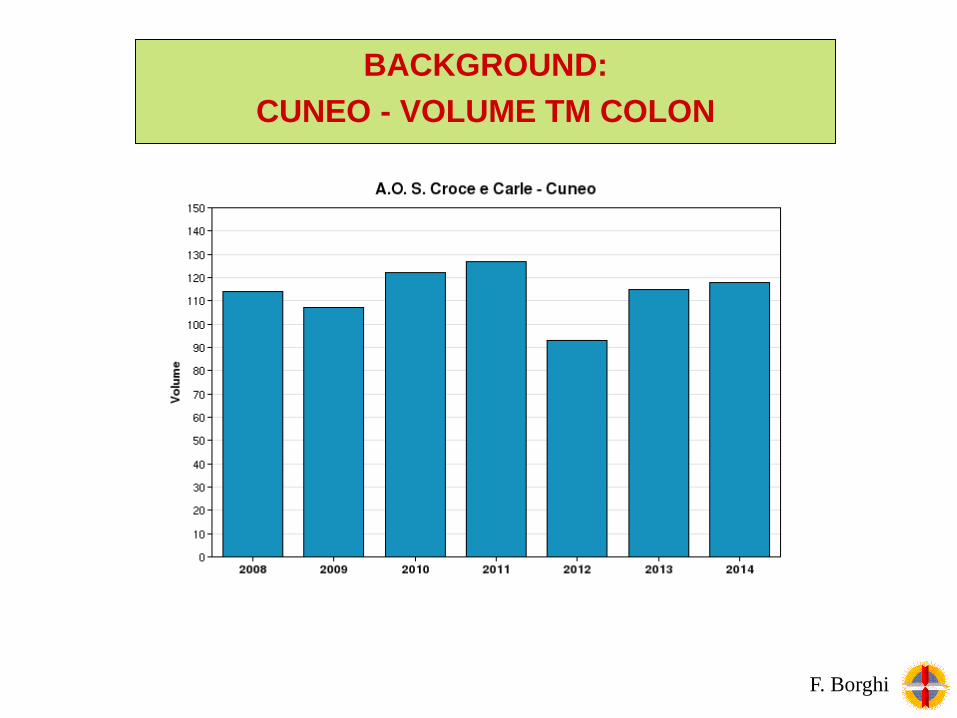
BACKGROUND:
CUNEO - VOLUME TM COLON

F. Borghi
BACKGROUND:
PIEMONTE - VOLUME TM COLON LAPARO

F. Borghi
BACKGROUND:
CUNEO - VOLUME TM COLON LAPARO

F. Borghi
BACKGROUND:
ITALIA - DEGENZA POST-OP COLON LAPARO

F. Borghi
VARIABILITA’ PER REGIONE
DEGENZA POST-OP COLON IN LAPAROSCOPIA

F. Borghi
BACKGROUND:
PIEMONTE - DEGENZA POST-OP COLON LAPARO

In 1999, Kehlet published the first important paper reporting median LOS of
2 days following colonic resections, using Fast Track protocol.
Kehlet H, Mogensen T. Hospital stay of 2 days after open sigmoidectomy with a multimodal
rehabilitation programme. Br J Surg 1999;86:227–30.
BACKGROUND:
LITERATURE DATA
F. Borghi
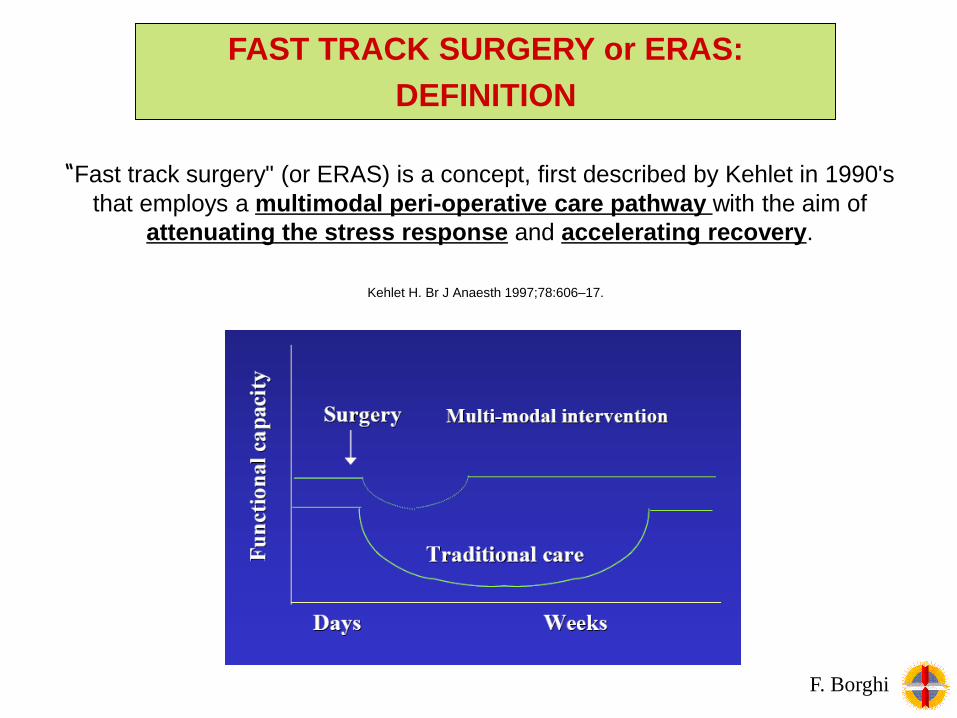
Kehlet H. Br J Anaesth 1997;78:606–17.
“Fast track surgery" (or ERAS) is a concept, first described by Kehlet in 1990's
that employs a multimodal peri-operative care pathway with the aim of
attenuating the stress response and accelerating recovery.
F. Borghi
FAST TRACK SURGERY or ERAS:
DEFINITION

ELEMENTS INFLUENCING
POST-OPERATIVE RECOVERY
F. Borghi

In 2001 the Enhanced Recovery After Surgery Study Group was
created to develop the Kehlet protocol and to create international surgical
units use the same peri-operative protocol.
Enhanced Recovery After Surgery: The Future of Improving Surgical Care
Varadhan KK et al. Crit Care Clin 26 (2010) 527–547
BACKGROUND:
ERAS STUDY GROUP
F. Borghi

An evidence-based consensus protocol for perioperative care in patients
undergoing colonic surgery was drafted by the ERAS Group in 2005
Fearon et al. Clinical Nutrition (2005) 24, 466–477
BACKGROUND:
WHY FAST-TRACK?
F. Borghi

Gustaffson et al. World J Surg 2013 DOI 10.1007/s00268-012-1772-0
F. Borghi
BACKGROUND:
WHY FAST-TRACK?

The consensus protocol was updated in 2009
F. Borghi
BACKGROUND:
WHY FAST-TRACK?
Lsaan K et al. Arch Surg. 2009;144(10):961-969
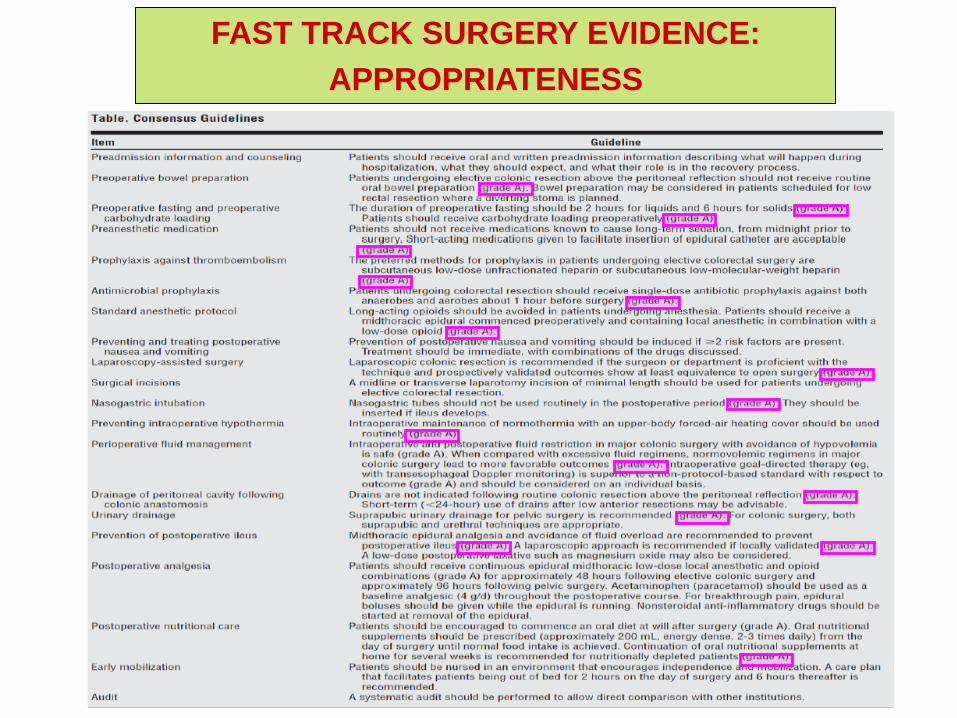
FAST TRACK SURGERY EVIDENCE:
APPROPRIATENESS

Author Year Trial Pt ( FT vs TRAD) LOS Mortality Morbidity
Anderson 2003 RCT 25 (14 vs 11)
3 vs 7
p=0.002 0 vs 9% p=n.s.
28.5% vs
45,5% p=n.s.
Delaney 2003 RCT 64 (31 vs 33)5,2 vs 5,8
p=0.12*/
22% vs 30%
p=n.s.
Gatt 2005 RCT 39 (19 vs 20)5 vs 7.5
p=0.0270 vs 5.3% p=n.s.
25,3 vs 55,7
p=0.076
Khoo 2007 RCT 70 (35 vs 35)5 vs 7
p<0.0010 vs 5.7% p=n.s. 26% vs 46%
Ionescu 2009 RCT 96 (48 vs 48)6,4 vs 9,1
p=0.001/
12,5 vs 22,9
p=n.s.
Serclova 2009 RCT 103 (51 vs 52)7 vs 10
p<0.001/
21,6 vs 48,1
p=0.003
Muller 2009 RCT 156 (76 vs 75)5 vs 9
p<0.0001
1.3% vs 1.3%
p=n.s.
17% vs 37%
p=0.006
FAST TRACK SURGERY EVIDENCE:
APPROPRIATENESS
F. Borghi

Author Year Trial Pt (FT vs TRAD) Lap/Open LOS Morbidity % Mortality %
Bradshaw 1998 CCT 72 (36 vs 36) Open 4,9 vs 6 8,3% vs 11,4% /
Stephen 2003 CCT 138 (86 vs 52) Open 3,7 vs 6,6* 12% vs 25% /
Raue 2004 CCT 52 (23 vs 29) Lap 4 vs 7* 17,4% vs 24,7% 0 vs 0
Basse 2004 CCT 260 (130 vs 130) Open 2 vs 8* 25.4% vs 55.4%* 4.6% vs 3%
Jakobsen 2004 CCT 40 (20 vs 20) Open 2 vs 8* / /
Jakobsen 2006 CCT 160 (80 vs 80) Open 4,2 vs 8,3 / /
Polle 2007 CCT 107 (55 vs 52) Open/Lap CR 4 vs 6* 27.3% vs 30.8% 0 vs 0
Wichmann 2007 CCT 40 (20 vs 20) Open 6,7 vs 9,7 / /
Kariv 2007 CCT 194 (97 vs 97) Open / / 0 vs 0
Hill 2008 CCT 100 (50 vs 50) Lap/Open 4 vs 6,5 54 vs 66 0 vs 4
Zargar 2008 CCT 52 (26 vs 26) Open 4 vs 6.5* 54% vs 66% 0 vs 4%
Maessen 2008 CCT 173 (121 vs 52) Open colon 2vs1 delay* Wound infect FT /
Nygren 2009 CCT 168 (99 vs 69) Open CR 2 vs 5* 18% vs 37%* 0
Teeuwen 2009 CCT 183 (61 vs 122) Open CR 6 vs 9* 14.8% vs 33.6%* 0 vs 1.6%
Walter 2010 CCT 600 (200 vs 400) Lap/Open 6 vs 9* p<0.001 n.s.
FAST TRACK SURGERY EVIDENCE:
APPROPRIATENESS

Author Year RCT (pts) CCT (pts) LOS Morbidity Readmission
Wind 2006 3 (64 vs 64) 3 (191 vs 195)−1·56 (−2·61,
−0·50) p=0.004
0·54 (0·42,
0·69) p<0.001
1·17 (0·73,
1·86) p=0.52
Gouvas 2009 4 (99 vs 101) 7 (447 vs 416)-2.46 (-3.43,-
1.48) p<0.00001
0.56 (0.45,
0.69) p<0.00001
1.37 (0.97,
1.92) p=0.07
Eskicioglu 2009 4 (198) / /0.61 (0.42,
0.88) p=0.009
0.67 (0.20,
2.19) p=0.50
Walter 2009 2 (33 vs 31)* 2 (153 vs 159)-3.64 (-4.98, -
2.29) p<0.0001
0.63 (0.39,
1.02) p=0.06*
/
Varadhan 2010 6 (226 vs 226) /-2.51(-3.54, -
1.47) p<0.00001
0.53 (0.41,
0.69) p<0.00001
0.80 (0.32,
1.98) p=0.62
FAST TRACK SURGERY EVIDENCE:
APPROPRIATENESS
F. Borghi
Metanalysis 2006-2010

Primary analyses ERAS versus conventional, outcome: Major Complications.
Primary analyses ERAS versus conventional, outcome: All complications
FAST TRACK SURGERY EVIDENCE:
APPROPRIATENESS
F. Borghi

La creazione di percorsi clinici costituisce la soluzione ideale per
standardizzare il trattamento pre, intra e post-operatorio dei pazienti e per
ridurre i costi (diretti e indiretti).
King PM, et al. Colorectal Dis 2006; 8(6):506–513
FAST TRACK SURGERY EVIDENCE:
COSTS
F. Borghi

Lemanu et al.. Colorectal Dis
2013
FAST TRACK SURGERY EVIDENCE:
COSTS
F. Borghi

A recent systematic review to assess cost effectiveness of enhanced recovery
after surgery programmes in colorectal surgery shows that FT is cost
effective (deficiencies regarding the reporting of data).
Lemanu et al. A systematic review to assess cost effectiveness of enhanced recovery after surgery
programmes in colorectal surgery. Colorectal Dis 2013
FAST TRACK SURGERY EVIDENCE:
COSTS
F. Borghi

Khan S et al. Colorectal Disease 2010 ; 12: 1175–1182
There is no evidence that ERAS adversely affect QoL or patient
satisfaction. Certain aspects of such as pain and fatigue may improve with
ERAS. Further research is required.
FAST TRACK SURGERY EVIDENCE:
QoL
F. Borghi

We have enough evidence to conclude that the FT methodology
concept provides major benefits to colonic surgery.
The issue is no longer whether Fast-Track colonic surgery is
better than standard care, but how to improve the approach and
its implementation.
Kehlet. Nat. Rev. Gastroenterol. Hepatol (2011). 8, 539–540
FAST-TRACK SURGERY:
From WHY to HOW
F. Borghi

Kehlet. Nat. Rev. Gastroenterol. Hepatol (2011). 8, 539–540
Despite some examples of FT program implemented outside expert
centres, there is a real gap between evidence based medicine and daily
practice: “the knowing-doing gap’’.
FAST-TRACK SURGERY:
From WHY to HOW
F. Borghi

Surgery 2010; 147:219-26
The first Italian trial in FT program.
FAST-TRACK SURGERY:
From WHY to HOW
F. Borghi

Surgeons, nurses, anesthesiologists motivation
(multidisciplinary team)
Preconceptions (patients and
clinicians)
Complexity of the program
Different resourses in different centres
Changement in the organization
FAST-TRACK SURGERY:
OBSTACLES
F. Borghi

FAST-TRACK SURGERY:
PERCHE’ AUDIT?
- Letteratura specifica convincente
- Outcomes lavori scientifici di centri accreditati difformi
- Prevedibile miglioramento qualità assistenza
- Messa in discussione abitudini consolidate
- Modello clinico e manageriale
-Racchiude appropriatezza, efficacia, efficienza e qualità tecnica
F. Borghi
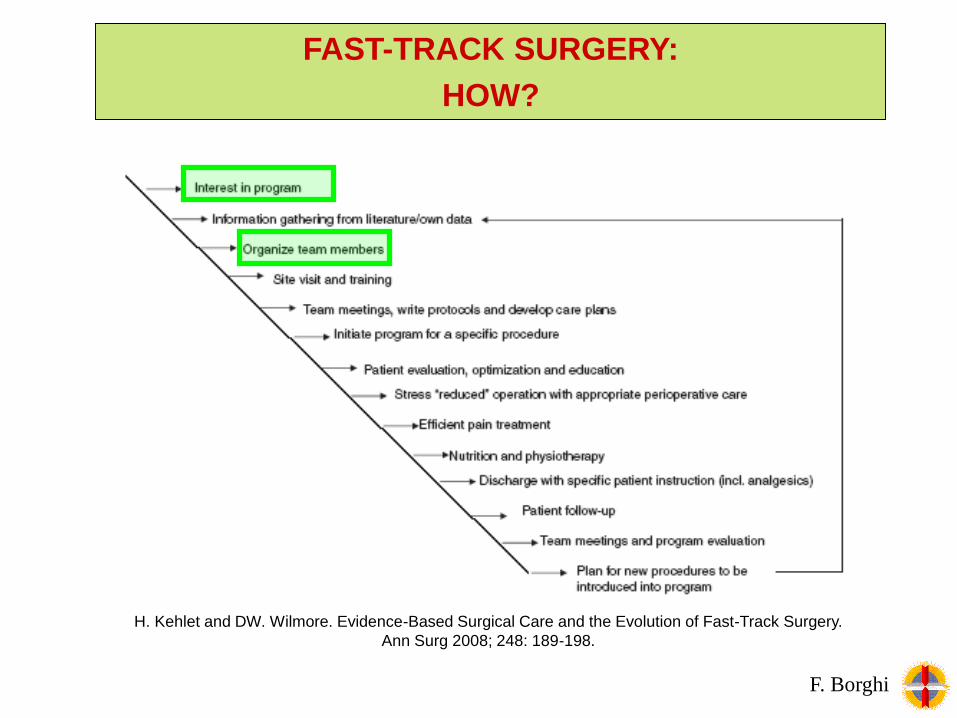
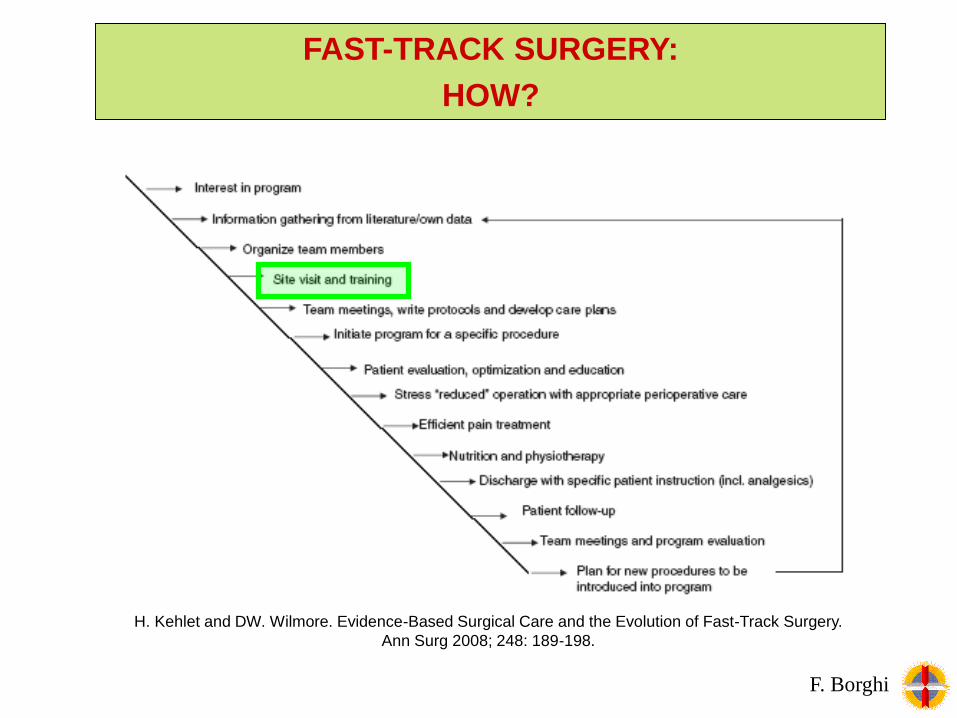
H. Kehlet and DW. Wilmore. Evidence-Based Surgical Care and the Evolution of Fast-Track Surgery.
Ann Surg 2008; 248: 189-198.
F. Borghi
FAST-TRACK SURGERY:
HOW?

Dietician
General
Practitioner
Nurse
Anesthesiologist
Surgeon
Physiotherapist
Patient
FAST-TRACK SURGERY:
HOW?
F. Borghi
Direzione sanitaria
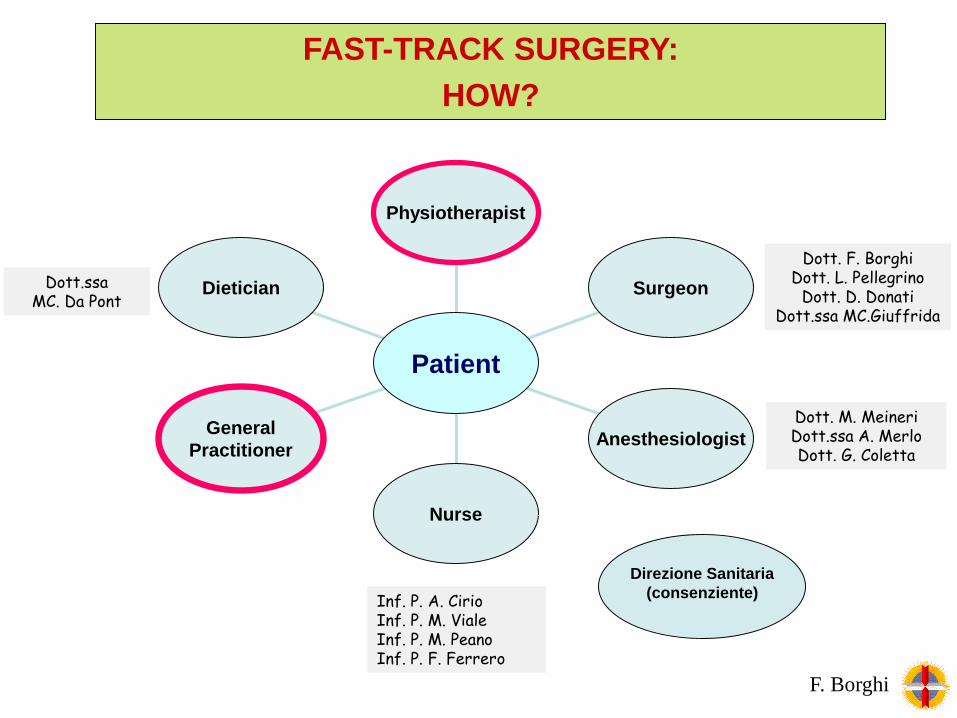
Dott. F. BorghiDott. L. Pellegrino
Dott. D. DonatiDott.ssa MC.Giuffrida
Dott. M. MeineriDott.ssa A. MerloDott. G. Coletta
Inf. P. A. CirioInf. P. M. VialeInf. P. M. PeanoInf. P. F. Ferrero
Dott.ssa MC. Da Pont
Dietician
General
Practitioner
Nurse
Anesthesiologist
Surgeon
Physiotherapist
Patient
FAST-TRACK SURGERY:
HOW?
F. Borghi
Direzione Sanitaria
(consenziente)
H. Kehlet and DW. Wilmore. Evidence-Based Surgical Care and the Evolution of Fast-Track Surgery.
Ann Surg 2008; 248: 189-198.
F. Borghi
FAST-TRACK SURGERY:
HOW?

St. Luc’s University Hospital Brussels – Belgium
Department of Abdominal Surgery and Transplantation
Colorectal Surgery Unit (Prof. Alex Kartheuser)
ASO S. Croce e Carle Cuneo - Italy
Dipartimento chirurgico
SC Chirurgia Generale (Direttore: Dr. F. Borghi)
FAST TRACK SURGERY or ERAS:
VISITING CENTER WITH EXPERIENCE
F. Borghi

FAST TRACK SURGERY or ERAS:
WRITING PROTOCOL
F. Borghi

... FOR ANESTHESIA AND ANALGESIA

... FOR NURSING
F. Borghi
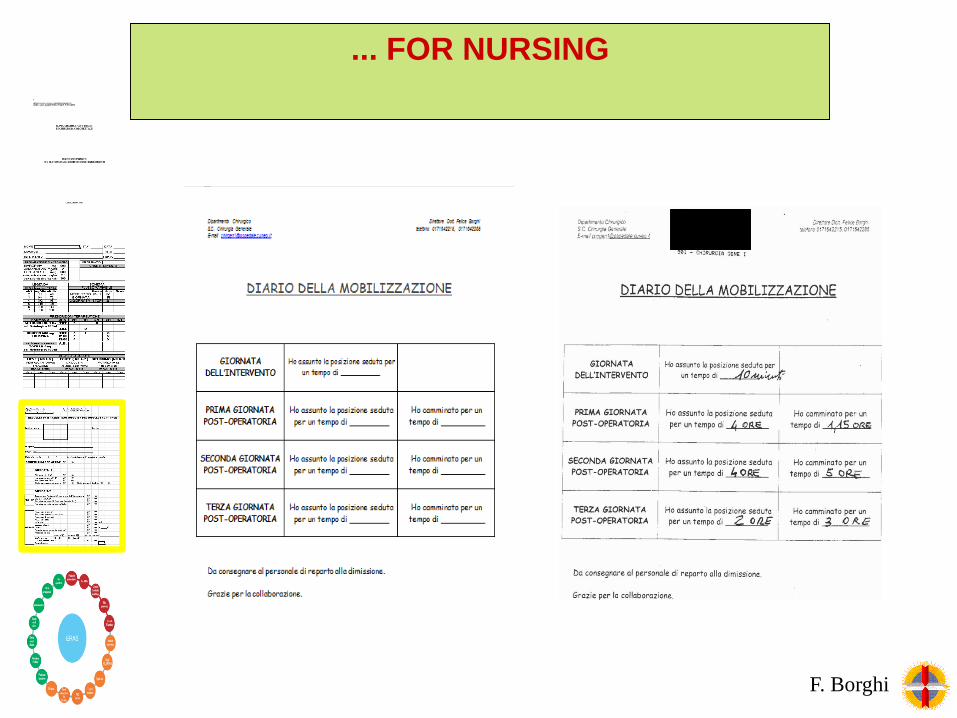
... FOR NURSING
F. Borghi

... INCLUDING THE ITEMS
F. Borghi
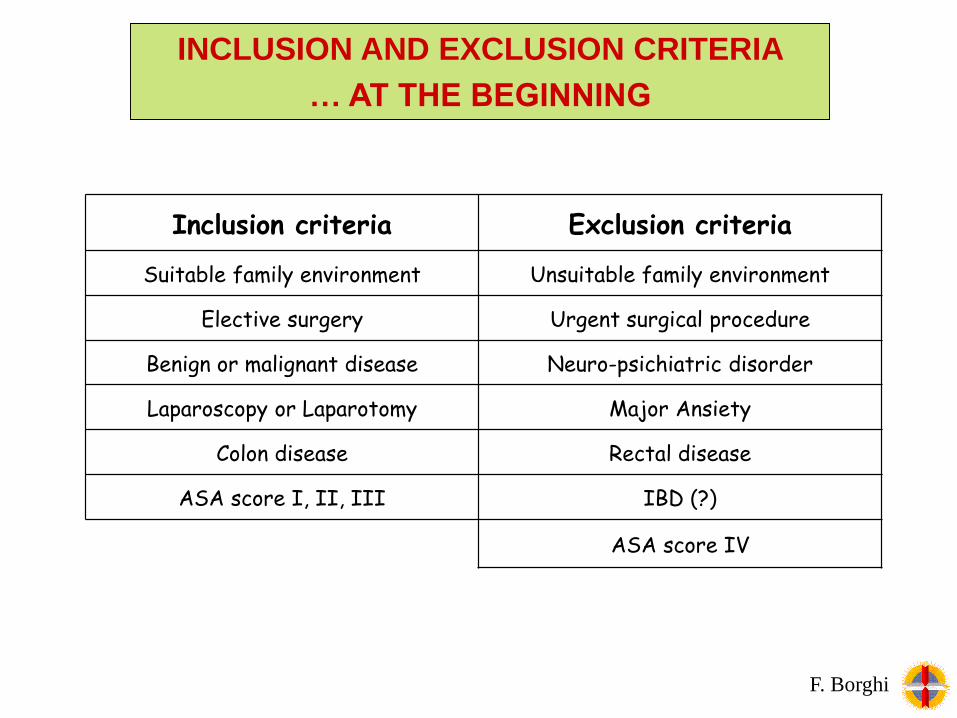
Inclusion criteria Exclusion criteria
Suitable family environment Unsuitable family environment
Elective surgery Urgent surgical procedure
Benign or malignant disease Neuro-psichiatric disorder
Laparoscopy or Laparotomy Major Ansiety
Colon disease Rectal disease
ASA score I, II, III IBD (?)
ASA score IV
INCLUSION AND EXCLUSION CRITERIA
… AT THE BEGINNING
F. Borghi

1. Pain control with oral pain killers
2. Resuming of oral feeding
3. Recovery of intestinal function (gas)
4. Willing of the patient to come back home
DISCHARGE CRITERIA
…AT THE BEGINNING
F. Borghi

FAST TRACK SURGERY or ERAS:
DATA COLLECTION
F. Borghi

Intervento
DimissioneContatto telefonico
Visita pre-operatoria
J0 J3 J4-J20 -J1
Ricovero
Posiz.CPD
CHO
No MBP
Chirurgo, Anestesista,
Infermiere e Dietologo
J2 J7 J30
Visita ambulatoriale
Pre-ospedaliera Fase ospedaliera Fase Post-ospedaliera
J1
Rimozione CPD
CHO
Stop ev
Ripresa alimentazione
Mobilizzazione
Rimozione CV
Deambulazione
J5
Visita dal MMG
J6
MMG
Restrizione ev
O2 terapia
Stop O2 terapia
Emocr elettr creat
CoagulEsami preoperatori
Esame istologico
Incremento alimentazione
FAST TRACK SURGERY or ERAS:
CARE PLAIN
F. Borghi

Visita pre-operatoria
-J20
Chirurgo, Anestesista,
Infermiere e Dietologo
Pre-ospedaliera
Esami preoperatori
- Inclusion in FT program and program
explication
- Brochure
FAST TRACK SURGERY or ERAS:
PRE-HOSPITAL CARE PLAIN
F. Borghi

Visita pre-operatoria
-J20
Chirurgo, Anestesista,
Infermiere e Dietologo
Pre-ospedaliera
Esami preoperatori
- Inclusion in FT program and program
explication
- Brochure
- Optimization of pre-operative status
- PONV
- Explication of analgesia (epidural
analgesia)
FAST TRACK SURGERY or ERAS:
PRE-HOSPITAL CARE PLAIN
F. Borghi

Visita pre-operatoria
-J20
Chirurgo, Anestesista,
Infermiere e Dietologo
Pre-ospedaliera
Esami preoperatori
- Inclusion in FT program and program
explication
- Brochure
- Optimization of pre-operative status
- PONV
- Explication of analgesia (epidural
analgesia)
- Counselling in case of stoma creation
(rectal surgery with TME)
- Diet and maltodestrin (3h before
surgery)
- LMWH
- In case of >10% weight loss
FAST TRACK SURGERY or ERAS:
PRE-HOSPITAL CARE PLAIN
F. Borghi
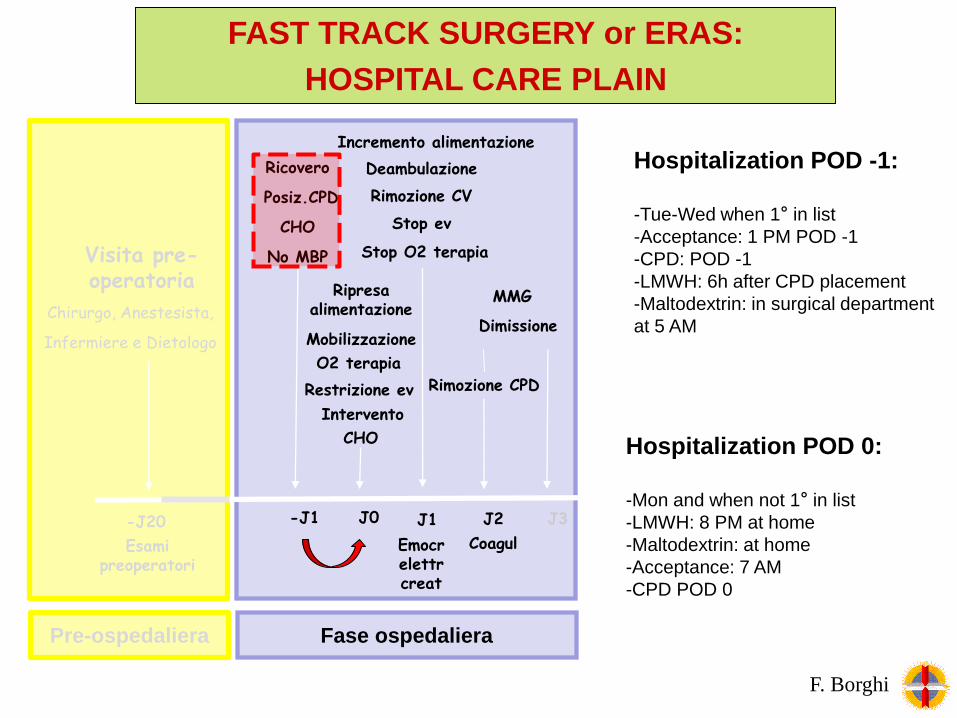
Intervento
Dimissione
Visita pre-operatoria
J0 J3-J20 -J1
Ricovero
Posiz.CPD
CHO
No MBP
Chirurgo, Anestesista,
Infermiere e Dietologo
J2
Pre-ospedaliera Fase ospedaliera
J1
Rimozione CPD
CHO
Stop ev
Ripresa alimentazione
Mobilizzazione
Rimozione CV
Deambulazione
MMG
Restrizione ev
O2 terapia
Stop O2 terapia
Emocr elettr creat
CoagulEsami preoperatori
Incremento alimentazione
Hospitalization POD 0:
-Mon and when not 1° in list
-LMWH: 8 PM at home
-Maltodextrin: at home
-Acceptance: 7 AM
-CPD POD 0
Hospitalization POD -1:
-Tue-Wed when 1° in list
-Acceptance: 1 PM POD -1
-CPD: POD -1
-LMWH: 6h after CPD placement
-Maltodextrin: in surgical department
at 5 AM
FAST TRACK SURGERY or ERAS:
HOSPITAL CARE PLAIN
F. Borghi

Intervento
Dimissione
Contatto telefonico chirurgo o infermiera
Visita pre-operatoria
J0 J3 J4-J20 -J1
Ricovero
Posiz.CPD
CHO
No MBP
Chirurgo, Anestesista,
Infermiere e Dietologo
J2 J7 J30
Visita ambulatoriale
Pre-ospedaliera Fase ospedaliera Fase Post-ospedaliera
J1
Rimozione CPD
CHO
Stop ev
Ripresa alimentazione
Mobilizzazione
Rimozione CV
Deambulazione
J5
Visita dal MMG
J6
MMG
Restrizione ev
O2 terapia
Stop O2 terapia
Emocr elettr creat
CoagulEsami preoperatori
Esame istologico
Incremento alimentazione
FAST TRACK SURGERY or ERAS:
POST- HOSPITAL CARE PLAIN
F. Borghi

FAST-TRACK SURGERY:
HOW?

FAST-TRACK SURGERY:
HOW?
F. Borghi

F. Borghi

Post-HospitalPre-Hospital Intra-Hospital
FAST-TRACK SURGERY:
AUDIT
F. Borghi

Feroci F et al. Int J Colorectal Dis Sept. 2012
Improved adherence to the standardized multimodal ERAS protocol is
significantly associated with improved clinical outcomes, indicating a dose-
response relationship.
Gustafsson UO et al. Arch Surg 2011 May;146(5):571-577.
Stein SL. Semin Colon Rectal Surg 2010; 21:180-183
F. Borghi
FAST-TRACK SURGERY:
AUDIT FOR COMPLIANCE

Passive elements (delivered to the patient without their direct contribution)
Active elements (the participation of the patient is required)
Preadmission counselling Carbohydrate loading
Avoidance of MBP (except TME cases) Urinary catheter removed day1 or 3TME
Avoidance of long acting sedative GI stimulation (laxatives)
Thoracic epidural Oral analgesia alone day 3
PONV prophylaxis IV fluids discontinued on day 1
Laparoscopic surgery Solid food taken on day 1
Avoidance of NG tube «Mobilization»
Intra-operative patient warming
Intra-operative fluid guidance
Avoidance of abdominal drains (colon)
Compliance with the passive elements (93,5%) is higher than active elements
(53,6%). Poor compliance with active elements is associated with major
morbidity and may be a surrogate marker of early complications.
Cthorn et al. Int J Colorectal Dis 2016 DOI 10.1007/s00384-016-
2588-4F. Borghi
FAST-TRACK SURGERY:
AUDIT FOR COMPLIANCE

Avoiding overload of ev fluids and oral intake of calories on the day of operation
are predictors of improved 5-year survival. A third independent predictor for
improved long-term survival is low C-reactive protein levels
Gustafsson et al World J Surg 2016 DOI 10.1007/s00268-016-3460-y
FAST-TRACK SURGERY:
AUDIT FOR COMPLIANCE
F. Borghi

• Personal collection data
• Multicentric collection data
• Literature analysis / congress/
referral centre
• Protocol modifications
AUDIT…
F. Borghi

• Personal collection data
• Multicentric collection data
• Literature analysis / congress/
referral centre
• Protocol modifications
AUDIT…
F. Borghi

N° pazienti
(tot 150)
Dindo-Clavien 3a 2 (1,3%)
Posizionamento di drenaggio radiologico (%) 2 (1,3%)
Dindo-Clavien 3b 8 (5.3%)
Deiscenze anastomotiche (%) 3 (2%)
Lesioni coliche iatrogene (%) 2 (1,3%)
Peritoniti post-operatorie (%) 3 (2%)
Dindo-Clavien 4 1 (0,7%)
ARDS (%) 1 (0,7%)
Mortalità (Dindo-Clavien 5) 0%
FAST TRACK SURGERY or ERAS:
PRELIMINARY DATA
F. Borghi

L-Group
(64 pts)
R-Group
(41 pts)
Dindo-Clavien 1-2 16
(25,0%)6 (14,6%)
Dindo Clavien 3a 0 2 (4,9%)
Dindo Clavien 3b 1 (1,6%) 3 (7,3%)
Dindo Clavien 4-5 0 0
L-Group: emicolectomia sinistra LAPR-Group: emicolectomia destra lap
Posters presentation at the 1° ERAS Congress, Cannes, October 2012
FAST TRACK SURGERY or ERAS:
PRELIMINARY DATA
F. Borghi

N° pazienti
(tot 150)
Degenza post-operatoria mediana (giorni) 3 giorni [range, 2-35]
Degenza post-operatoria media ± DS (giorni) 4.4 ± 3.5 giorni
Degenza post operatoria mediana LAP 3 giorni [range, 2-18]
Degenza post operatoria mediana OPEN 4,5 giorni [range, 3-35]
Degenza post operatoria mediana CPD 3 giorni [range, 2-35]
Degenza post operatoria mediana non CPD 4 giorni [range, 3-14]
FAST TRACK SURGERY or ERAS:
PRELIMINARY DATA
F. Borghi

FAST TRACK SURGERY or ERAS:
PRELIMINARY DATA
F. Borghi
3%
49%
27%
21%
DPO 2 giorni
DPO 3 gg
DPO 4 gg
DPO > 4 gg
79% dei pazienti dimessi entro la IV giornata post-operatoria

N° patients
(tot 150)
Pazienti dimessi entro le 72h po 85 (56,7%)
Pazienti dimessi dopo le 72h po 65 (43,3%)
Complicanze intra-ospedaliere 34 (22,7%)
Complicanze maggiori 10 (6,7%)
Complicanze minori/osservazione clinica 24 (16%)
Ritardo nella riabilitazione 15 (10%)
Problemi nell’applicazione del protocollo 16 (10,7%)
1° poster prize at the 12° International meeting on coloproctology, Turin, March 2012
FAST TRACK SURGERY or ERAS:
PRELIMINARY DATA
F. Borghi
• Personal collection data
• Multicentric collection data???
• Literature analysis / congress /
referral centre (>50 visiting surgeons)
• Protocol modifications
AUDIT…
F. Borghi

Author Year Pts RCT (FT vs no FT) Pts CCT (FT vs no FT)
Wind 2006 3 (64 vs 64) 3 (191 vs 195)
Gouvas 2009 4 (99 vs 101) 7 (447 vs 416)
Eskicioglu 2009 4 (198) /
Walter 2009 2 (33 vs 31) 2 (153 vs 159)
Varadhan 2010 6 (226 vs 226) /
Spanjersberg 2011 4 (119 vs 118) /
Adamina 2011 6 (226 vs 226) /
Lv 2012 7 (419 vs 433) /
Lemanu 2013 (costs) 2 5
Zhuang 2013 13 (1910) /
Greco 2013 16 (1181 vs 1195) /
Shao 2014 13 (9+4*) (1962) /
Li 2014 6 (323 vs 332) /
Zhao 2014 5 (696 vs 621) 5
Wang 2014 24 (2093 vs 1272) /
Spanjerberg 2015 3 (520 pts) 5 (422 pts)
Implementation of FT program in colorectal surgery:
reduction in LOS, post operative morbidity and cost.
F. Borghi
FAST TRACK SURGERY EVOLVING DATA:
META-ANALYSIS

ERAS pathway significantly reduced overall morbidity (15.1 % in the ERAS
group vs 24.6 % in the control group)
Greco M et al. World J Surg 2013 DOI 10.1007/s00268-013-2416-8
F. Borghi
FAST TRACK SURGERY or ERAS:
OVERALL COMPLICATIONS
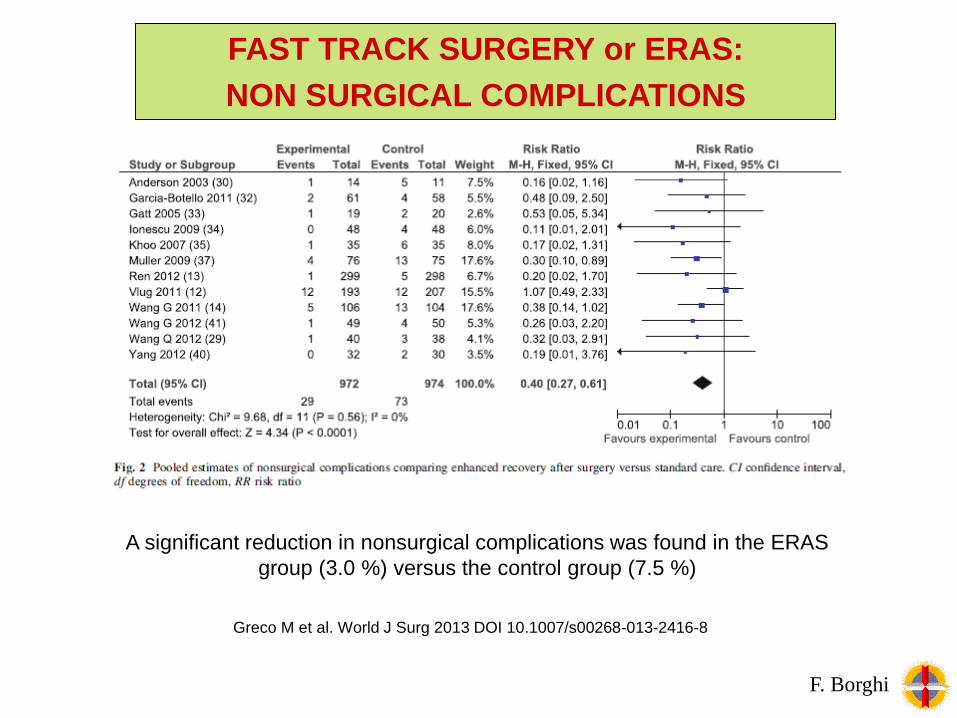
A significant reduction in nonsurgical complications was found in the ERAS
group (3.0 %) versus the control group (7.5 %)
Greco M et al. World J Surg 2013 DOI 10.1007/s00268-013-2416-8
F. Borghi
FAST TRACK SURGERY or ERAS:
NON SURGICAL COMPLICATIONS

Greco M et al. World J Surg 2013 DOI 10.1007/s00268-013-2416-8
F. Borghi
FAST TRACK SURGERY or ERAS:
POST-OPERATIVE STAY
In metanalysis mean LOS is 5.8 days in the ERAS group and 8.0 days in the
control group (p<0.001).

FAST TRACK SURGERY EVIDENCE:
EVOLVING APPROPRIATENESS
World J Surg. 2013 Feb;37(2) F. Borghi

• Personal collection data
• Multicentric collection data
• Literature analysis / congress
• Protocol modifications
AUDIT…
F. Borghi

Inclusion criteria Exclusion criteria
Elective surgery Urgent surgical procedure
Benign or malignant disease
Laparoscopy or Laparotomy
IBD
Colonic disease
Rectal disease (PME and TME)
ASA score I, II, III, IV
EVOLVING… INCLUSION AND EXCLUSION
CRITERIA
F. Borghi

1. Pain control with oral pain killers
2. Resuming of oral feeding
3. Recovery of intestinal function (gas)
4. Willing of the patient to come back home
4. Stoma management and correct output (in TME)
EVOLVING… DISCHARGE CRITERIA
F. Borghi

Item Colon Rectum
Preoperative CounselingYes (surgeon,
anesthesiologist)Yes (idem + nurse)
Preoperative Optimisation Yes Yes
MBP No Yes
CHO and no fasting Yes Yes
Preanaesthesia No long-acting sedation No long-acting sedation
Hospitalization J0 (J-1) J0 (J-1)
Analgesia Peridural Peridural
PONV Yes Yes
Nasogastric tube No No
Anaesthesia management Blended Blended
Laparoscopic approach Laparoscopic/Open Robotic/Open
Resection-site drainage No Yes
Immediate postoperative diet Yes Yes
Removal of urinary catheter J1 J2 (3)

656 pazienti
Patients (M:F) 383/273
Age (mean) 68,6 [25-91 anni]
BMI (Kg/m^2) 25.3 ± 4.7 Kg/m2
Benign disease (%) 47 (7,5%)
Cancer or polyp (%) 607 (92,5%)
FAST TRACK SURGERY or ERAS:
PERSONAL EXPERIENCE (2010 – 03/2016)
F. Borghi

FAST TRACK SURGERY or ERAS:
PATIENTS DATA
F. Borghi

FAST TRACK SURGERY or ERAS:
ASA SCORE
F. Borghi

110 RAR + PME72 RAR + TME
FAST TRACK SURGERY or ERAS:
SURGICAL PROCEDURE
F. Borghi

656 patients
MIS procedures (lap + rob) 439 (67%)
Laparotomic procedures 217 (33%)
Conversion rate (%) 28 (4,3%)
Median operative time (min) 194
FAST TRACK SURGERY or ERAS:
OPERATIVE DATA
F. Borghi

656 patients
Peridural catheter positioning (%) 584 (89%)
Problems related to PDA (%) 6.4%
PDA displacement 4,5%
Ipothension related to PDA 1,9%
PDA removing (median) II day
FAST TRACK SURGERY or ERAS:
PERIDURAL
F. Borghi

J0 J1 J2 J3
Posizione seduta (min) 14 258 278 397
Deambulazione (min) ---- 178 168 289
Totale (min) 14 436 446 686
Data recorded for 60 patients
FAST TRACK SURGERY or ERAS:
PATIENT MOBILIZATION
F. Borghi

656 patients
Minor complications (Dindo-Clavien 1-2) 216 (32,9%)
Major complications (Dindo-Clavien 3-4) 35 (5,3%)
Mortality (Dindo-Clavien 5) (30 days) 1 (0,1%)
Post-operative complications in literature: 4 – 47%
(bias: different classification of complications)
FAST TRACK SURGERY or ERAS:
COMPLICATIONS
F. Borghi

4,3% re-intervention
FAST TRACK SURGERY or ERAS:
COMPLICATIONS
F. Borghi

In LAFA Trial the median POS in lap+FT group was 5 (4–7) days;
open+FT 6 (4.5–10) days.
656 patients
Median post operative stay (days) 4 days [range, 2-35]
Mean post-operative stay ±DS (days) 5,6 ± 4,1 days
Median post-operative stay in LAP 4 days [range, 2-18]
p<0,05Median post-operative stay in OPEN 7 days [range, 3-35]
FAST TRACK SURGERY or ERAS:
LOS
F. Borghi

65% patients are discharged within V post-operative day
FAST TRACK SURGERY or ERAS:
LOS
F. Borghi

INTERA CASISTICA (316 CASI)
PRIMI 100 CASI SELEZIONATI
3 days
4 days
> 4 days
4 days
> 4 days
3 days
Median LOS 4 days Median LOS 3 days
4 days
> 4 days
3 days
FAST TRACK SURGERY or ERAS:
LOS
F. Borghi

FAST TRACK SURGERY or ERAS:
VARIATION IN INCLUSION CRITERIA
F. Borghi

656 patients
Median post operative stay (days) 4 days [range, 2-35]
Median post-operative stay in colon 4 days
Median post-operative stay in RAR 5 days
Median post-operative stay in RAR + TME 6 days
K. Anderin et al. / EJSO 41 (2015) 724e730
The presence of diverting stoma in patients undergoing RAR within an ERAS
setting is associated with a delayed postoperative recovery .
FAST TRACK SURGERY or ERAS:
VARIATION IN INCLUSION CRITERIA
F. Borghi

Re-admission in FT program in literature: 0 – 25%.
656 patients
Patients without re-admission 639 (97,4%)
Re-admissions (30 days) (%) 17 (2,6%)
Re-intervention after discharge 1 (0,1%)
FAST TRACK SURGERY or ERAS:
RE-ADMISSION
F. Borghi

Fonte: www.agenas.it
From 2010 the
FT protocol was
implemented in
our department
ASO SANTA CROCE CUNEO
DEGENZA POST-OP COLON IN LAPAROSCOPIA
F. Borghi

BACKGROUND:
WHY FAST-TRACK?
F. Borghi

F. Borghi

F. Borghi

















