23
Percutaneous mitral valve repair using the MitraClip® device (e- valve) Angela Hoye, Rajesh Nair, Farqad Alamgir Castle Hill Hospital, Hull Post-script
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| Upload: | anthony-blake |
| View: | 214 times |
| Download: | 0 times |

Percutaneous mitral valve repair using the MitraClip® device (e-
valve)
Angela Hoye, Rajesh Nair, Farqad AlamgirCastle Hill Hospital, Hull
Post-script

No conflict of interest in relation to this presentation

Introduction: MR• Mitral regurgitation occurs due to:
• valvular degeneration (50%)
• rheumatic disease (20%)
• ischaemia (17%)
• Where possible, surgical mortality is lower following MV repair rather than replacement
However, after MV repair surgery, published data show a rate of recurrence of grade 3 or 4 MR of 17-20% at 5 yrs

Anatomy

The Alfieri technique• The surgical “edge-to-edge” technique
was first described in early 1990`s (Alfieri)
• Over 1,500 pts reported in the literature
• Safe, effective, durable
• No occurrence of mitral stenosis
• Facilitates proper leaflet coaptation
• Degenerative - anchor flail / prolapsing leaflets
• Functional - Coapt tethered leaflets to reduce time and force required to close valve
• Creates tissue bridge
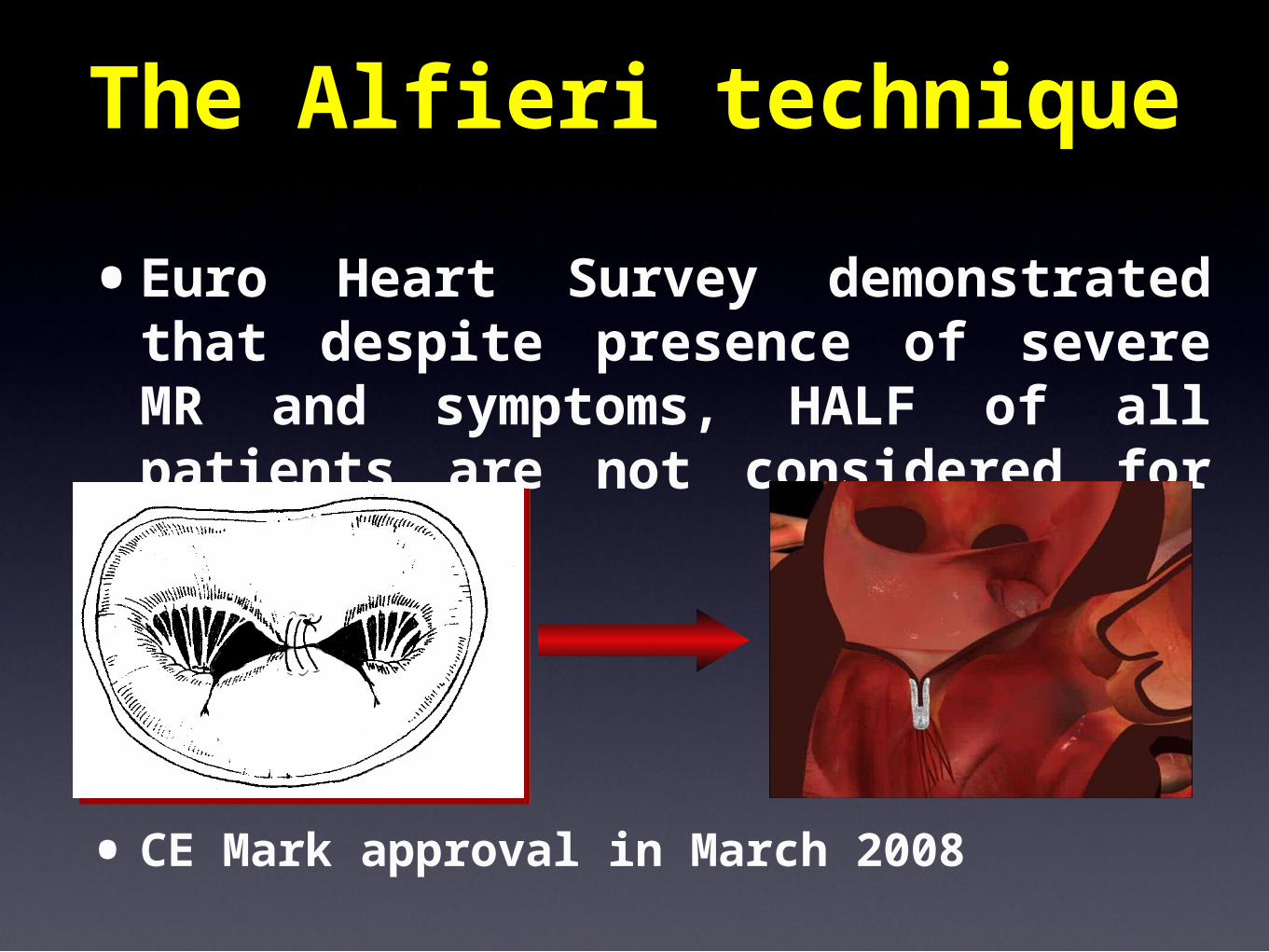
The Alfieri technique
•Euro Heart Survey demonstrated that despite presence of severe MR and symptoms, HALF of all patients are not considered for surgery
•CE Mark approval in March 2008

MitraClip® procedure overview
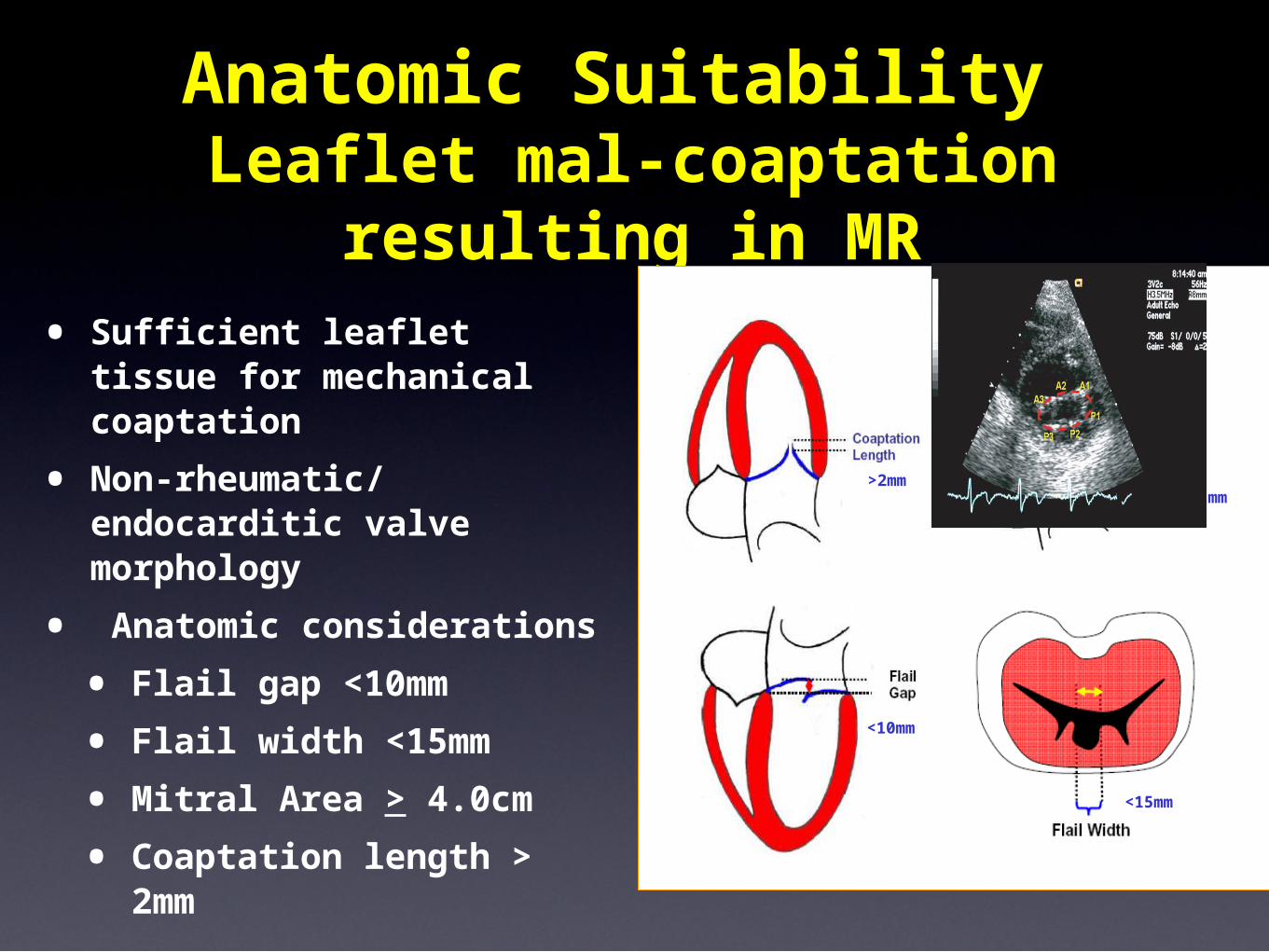
Anatomic Suitability Leaflet mal-coaptation resulting
in MR• Sufficient leaflet tissue
for mechanical coaptation
• Non-rheumatic/endocarditic valve morphology
• Anatomic considerations
• Flail gap <10mm
• Flail width <15mm
• Mitral Area > 4.0cm
• Coaptation length > 2mm
>2mm>11mm
<10mm
<15mm

Enrollment Population n
EVEREST I
Feasibility (completed)Registry patients 55
EVEREST II
Randomized n=279
Roll-in
Randomized Clip
Randomized Surgery
60
187
92
EVEREST II High Risk Registry 78
• 47 sites
Studies

Data: EVEREST•Age 18 years or older
•Moderate to severe (3+) or severe (4+) MR
• Symptomatic
• Asymptomatic with LVEF < 60% or LVESD > 40mm*
•MR originates from A2-P2 mal-coaptation
•Candidate for mitral valve surgery
•Key exclusions:
• EF < 25% or LVESD > 55 mm
• Renal insufficiency
• Endocarditis, rheumatic heart disease
*ACC/AHA Guidelines, Circ. 114;450,2006

One or more Clips implanted in 90% of cases
Results
•EVEREST I + roll-in phase of EVEREST II
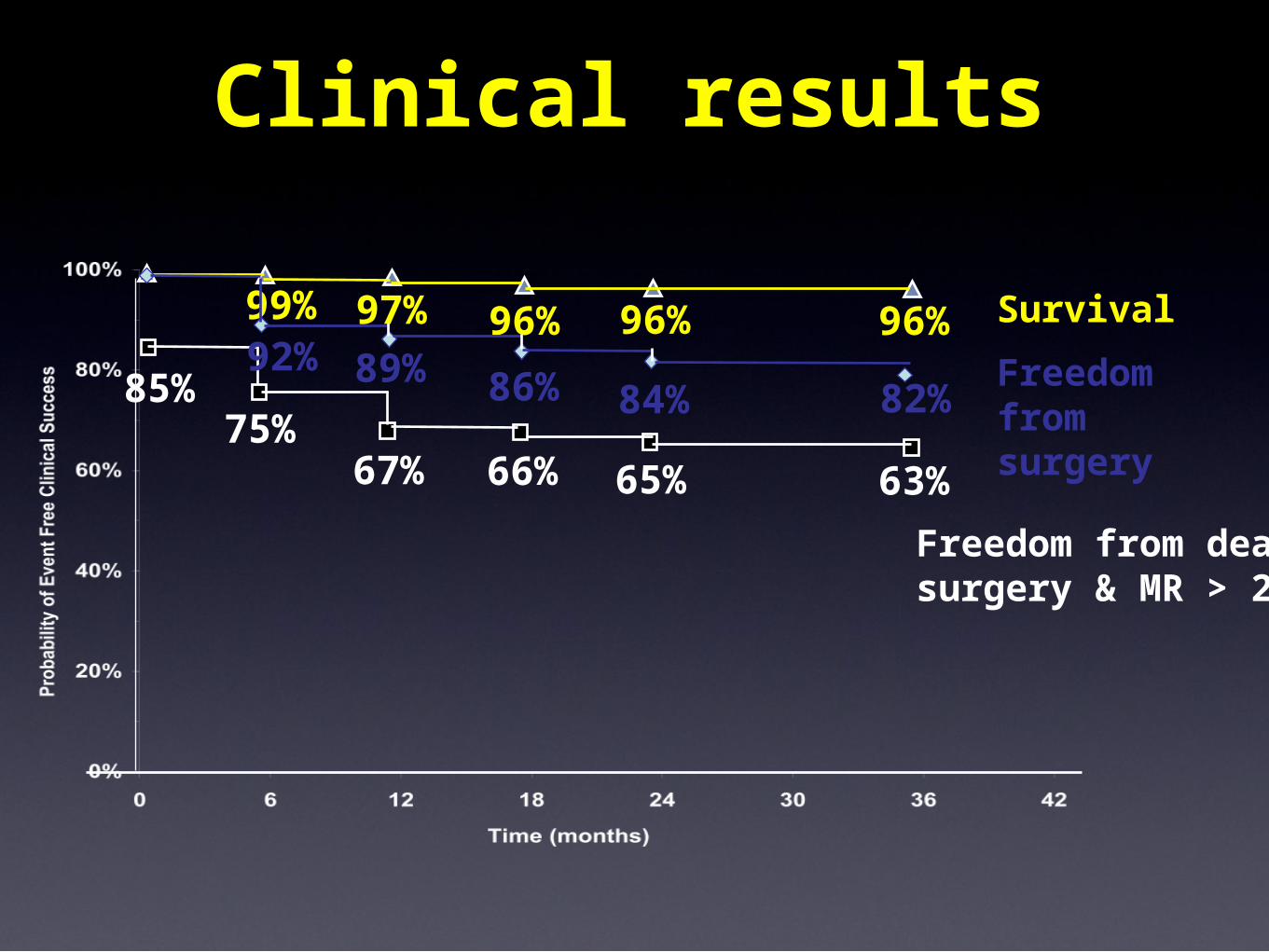
Clinical results
Survival
Freedom from surgery
Freedom from death, surgery & MR > 2+
99% 97% 96% 96% 96%
85%75%
67% 66% 65% 63%
84% 82%92% 89% 86%

Reverse LV remodelling•LV Dysfunction Population (EF <
55% or LVIDs > 4.5cm)

Our experience•All potential patients were discussed
at MDT
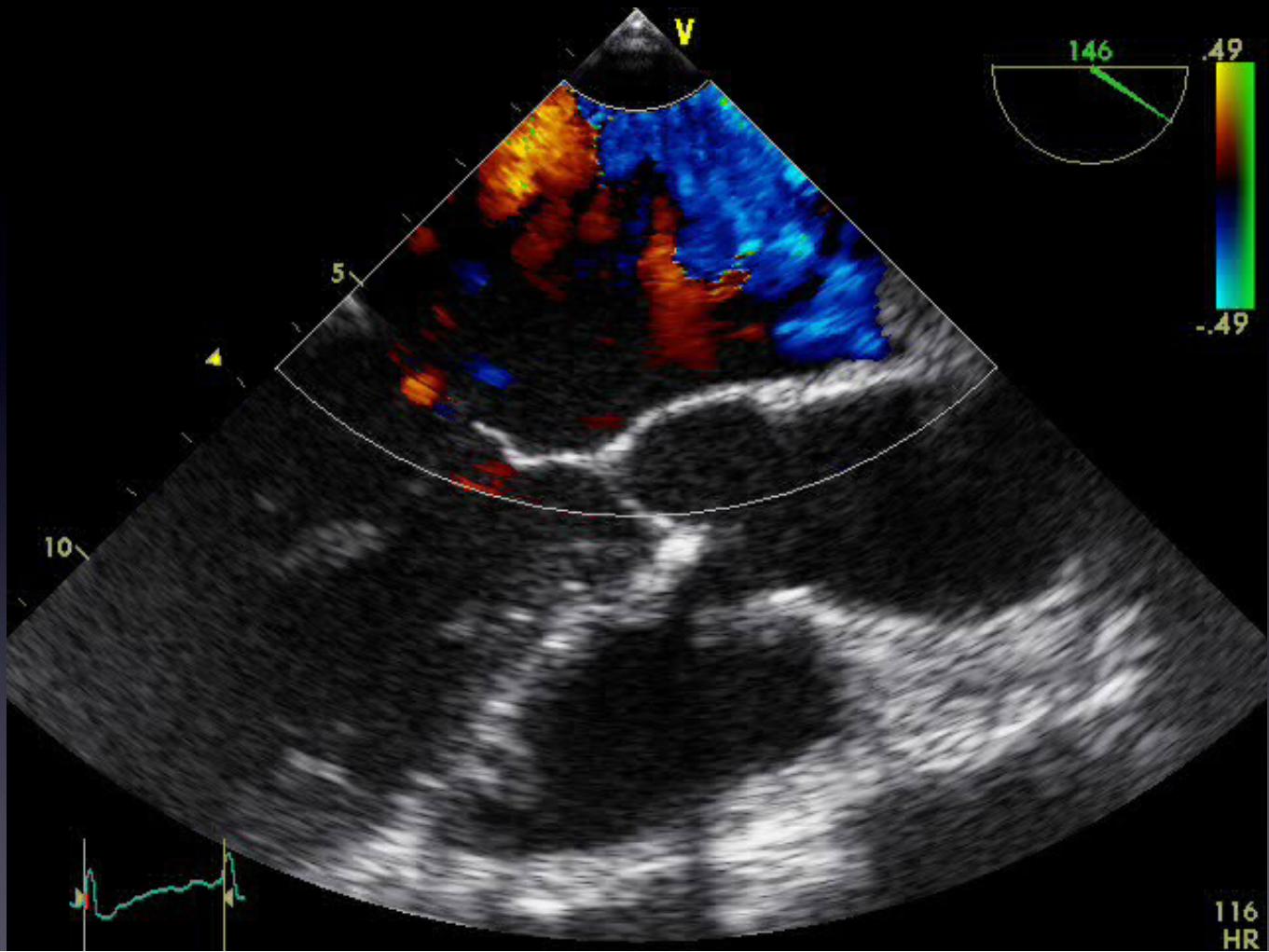
•Pre-procedural TTE and TOE to determine suitability
•Teamwork is vital• Interventional cardiologist
• Cardiac anaesthetist
• ECHO specialist
• Lab staff – specialist training given to nursing staff
• All procedures performed with support from physicians from the company
Our experience
•Successfully treated 3 patients, all with degenerative MR
• 2 pts with a single clip, 1 with 2 clips
•No procedural MACE
•At 1 month, all patients report a marked improvement in symptoms / exercise capacity


AmplatzGuide

QuickTime™ and a decompressor
are needed to see this picture.




Conclusions• Preliminary results of percutaneous
mitral valve repair with the MitraClip® demonstrate that it is safe and feasible
• Steep learning curve and it is essential to understand MV anatomy and TOE images
• Definite place for this technology in a subset of patients with MR and suitable anatomy
• All potential candidates should be evaluated by a multidisciplinary team
• Patient selection is paramount

















