Page 1
REVIEW
Peri- and post-menopausal incidental adnexal masses and the risk ofsporadic ovarian malignancy: new insights and clinical management
FAUSTINO R. PEREZ-LOPEZ1, PETER CHEDRAUI2, & JUAN M. TROYANO-LUQUE3
1Department of Obstetrics and Gynaecology, Facultad de Medicina, Universidad de Zaragoza, Hospital Clınico de Zaragoza,
Zaragoza 50009, Spain, 2Academic and Research Department, Hospital Gineco-Obstetrico Enrique C. Sotomayor, Guayaquil,
Ecuador, and 3Department of Obstetrics and Gynaecology, Facultad de Medicina, Universidad de La Laguna,
Hospital Universitario de Canarias, Tenerife 38071, Spain
(Received 11 January 2010; accepted 15 April 2010)
AbstractAdnexal masses are common among peri- and post-menopausal women. Although ovarian cancer is a significant cause ofmortality in menopausal women, large population-based studies demonstrate that the majority of adnexal masses are benign.Despite this, the appearance of an adnexal mass is a concern for the patient and an insight exercise for physicians. In mostcases, an adnexal enlargement is an incidental finding, generally corresponding to a benign cyst and easily diagnosed byconventional ultrasound. Exceptionally an ovarian tumour may be malignant and should be treated as early as possible.When conventional ultrasound renders complex morphology other diagnostic tools must be used such as: colour Dopplerand functional tumour vessel properties, serum CA 125 levels, nuclear magnetic resonance imaging and in some caseslaparoscopy. Several new tumour markers are being studied for clinical application, although there are presently no clearrecommendations. Adnexal masses with benign morphological and functional properties must be periodically monitored asan alternative to surgery since malignant transformation is exceptional.
Keywords: Menopause, adnexal mass, ovarian cancer, ultrasound scan, Doppler, CA 125, incidental ovarian cyst
Introduction
Ovarian cancer is the most lethal disease of the female
reproductive tract. Risk for ovarian malignancy in-
creases with age, and decreases with pregnancy.
Lifetime risk is about 1.6%, while women with affected
first-degree relatives have a 5% risk, those with a
mutated BRCA1 or BRCA2 gene or hereditary non-
polyposis colorectal cancer (Lynch syndrome) have a
25–60% risk depending on the specific mutation
[1–3]. Contrary to this, most ovarian cysts are never
noticed and resolve without women ever knowing so.
Prevalence of ovarian and paraovarian cysts is high in
both peri- and post-menopausal women, and while
most cases are benign [4–6], other incidental adnexal
masses are infrequent [7,8]. Hormonal changes taking
place around the menopause may predispose the
development of these benign ovarian cysts [9,10].
Proposal for ovarian cancer screening have failed or
have not been cost-effective; therefore, aside from
clinical trials, screening is not currently recom-
mended in the general populations [11–13]. Routine
ultrasound in pre- and post-menopausal women
allows diagnosing many ovarian cysts that are devoid
of any significant clinical symptom. An incidental
ovarian finding produces concern in many women
and should be differentiated from ovarian cancer.
When a cyst causes symptoms, pain is by far the most
common one. This pain may be due to cyst rupture,
rapid growth and stretching, intracyst bleeding and/or
torsion around its blood supply. The most common
type of ovarian cyst is the follicular caused by a follicle
growth. Other types include the haemorrhagic or
endometrioid. Dermoid cysts are infrequent around
the menopause [14]. Ovarian cancer is a silent killer,
especially affecting women above 50 years; although
presentation is often vague and non-specific, symp-
toms are definitely present. Therefore, a proper
clinical examination and appropriate tests should be
carried out upon onset in peri- and post-menopausal
Correspondence: Faustino R. Perez-Lopez, Facultad de Medicina, Department of Obstetrics and Gynaecology, Universidad de Zaragoza, Hospital Clınico de
Zaragoza, Zaragoza 50009, Spain. Tel: þ34-976-76-1734. Fax: þ34-976-76-1735. E-mail: [email protected]
Gynecological Endocrinology, September 2010; 26(9): 631–643
ISSN 0951-3590 print/ISSN 1473-0766 online ª 2010 Informa UK Ltd.
DOI: 10.3109/09513590.2010.487611
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
BSC
O o
n 09
/06/
10Fo
r pe
rson
al u
se o
nly.
Page 2
women. This study will update and assess the
available evidence concerning the management of
incidental adnexal masses around the menopause in
otherwise healthy women. Since women with heredi-
tary ovarian cancer risk may also have breast and colon
cancer risks and receive especial clinical recommen-
dations [15–17], hereditary cancer will not be
addressed.
Structure of the human menopausal ovary:
focussing on epithelial neoplastic capability
Ovarian plasticity has been postulated to facilitate
neoplastic transformation, tumour heterogeneity and
the complex pattern of its clinical course [18]. The
most common ovarian cancer is the epithelial with
three sub-types: mucinous, serous and endometrioid.
Germ cell and sex-cord stromal tumours are less
frequent types. Epithelial types of cancers derive
from the ovarian surface epithelium and its inclusion
cysts. Borderline ovarian tumours also arise from the
ovarian epithelium and show histological features
that are intermediate between benign and malignant
tumours. The surface epithelium is embryologically
formed from the invagination of the coelomic
mesothelium over the gonadal ridges [19], which
can migrate into the ovarian stroma to create
inclusion cysts. However, cysts can also develop
from periovarian and peritubal adhesions [20]. The
exposure of an inclusion cyst to the ovarian environ-
ment may cause phenotypic changes to the epithe-
lium commonly found in these cysts [21,22].
Metaplastic epithelium may also initiate neoplastic
changes which may be, under certain circumstances,
the pathway for developing an epithelial carcinoma
[23–25]. Characteristics of the epithelium surface of
early and advanced ovarian cancer have been
classified according to gene expression in attempt
to find the causes for cancer progression [26–31].
Despite this, no reasonable explanation for the
carcinogenesis process has been elucidated. Serous
borderline tumours are a separate category and in
most cases probably do not progress to authentic
carcinomas [32].
Assessment of the risk of developing ovarian
carcinoma has been performed by comparing the
histological ovarian features of women with high and
low risk. Ovaries removed from women with in-
creased risk of developing ovarian cancer contained
atypical features such as: surface epithelial pseudoes-
tratification, surface papillomatosis, deep epithelium
cortical surface invagination, multiple papillar pro-
jections with small cysts, epithelial inclusion cysts,
cortical stromal hyperplasia and hyperthecosis, in-
creased follicular activity, corpus luteum hyperplasia
or hiliar cell hyperplasia [33–35]. An early disruption
of the ovarian hormonal balance may exist in women
with pre-disposition to ovarian cancer that favours
the expression of certain genes and tumour growth
[36–38]. However, there are no clear ovarian
carcinoma precursors [20,32]. Risk factors for
sporadic ovarian cancer include age and a family
history of the disease, while increasing parity, oral
contraceptive (OC) use, oophorectomy, and breast-
feeding have protective effects. Modifiable risk
factors for epithelial ovarian cancer include lifestyle
ones such as, high body mass index, central obesity,
cigarette smoking, alcohol consumption, recreational
activities and post-menopausal hormone treatment
(HT) [39–49].
In young women, the ovarian surface epithelium is
a single layer of mesothelial cells that covers the
surface of the ovary, which is cyclically submitted to
conspicuous changes due to the ovulatory rupture
and repair process. This continuous process pro-
duces biochemical changes to date unknown that
may favour carcinogenic transformation. There is a
large number of biochemical candidates that may
initiate genetic alterations and progression, including
steroids, cytokines, prostaglandins, caspases, apop-
totic regulators and growth factors [50–52]. The
reduction of the number of ovulations due to
multiparity or OC use have protective effects against
epithelial ovarian cancer risk through the annulations
of repetitive rupture-reparation process in the cell
surface ovarian epithelium. Experimental (in-vitro
animal studies), epidemiological and clinical evi-
dence have shown that normal ovaries and many
ovarian tumours are influenced by endocrine factors
are hormone dependent or may be submitted to HT.
However, the relationships between ovarian hormone
function and carcinogenesis are still not clear. The
presence of oestrogen (ER) and androgen receptors
have been documented in a great number of primary
ovarian cancers (63% and 69%, respectively), while
progesterone receptors are reported in half of
tumours and glucocorticoid receptors in up to 88%
of ovarian cancers [53–56].
Oestrogen acts on the ovary by the two ER, a and bwhich are present in the ovary, although ER-bmRNA is the most abundant. Specific roles for each
ER at the ovarian level have yet to be established.
However, a reduction of ER-b has been suggested to
be associated to severity and prognosis of ovarian
cancer. The importance of ER signals in the ovarian
function has been postulated in the oestrogen
depleted aromatase knockout mouse. Although it
remains to be determined what genes are regulated
by ER-b in the human ovary [57]. Gene expression
profile (24 genes) differs in ovarian cancer cell lines
with different ER-a and ER-b populations, by adding
oestradiol or genistein. It seems that in-vitro oestro-
gens play a role in ovarian carcinogenesis in
association with unidentified cofactors [58]. Mole-
cular factors involved in epithelial ovarian cancer
have been studied by microarray techniques to
632 F. R. Perez-Lopez et al.
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
BSC
O o
n 09
/06/
10Fo
r pe
rson
al u
se o
nly.
Page 3
identify gene expression profiles that participate in
cell signalling, proteinase secretion, cell adhesion and
proliferation, extracellular matrix formation and
apoptosis [59,60]. Clinicopathological correlates
have tried to determine malignant disease develop-
ment, growth, infiltration and progression. However,
the mechanisms underlying gene alterations and the
specific role of involved proteins remain to be
elucidated.
HT use has been related to ovarian cancer risk in
post-menopausal women [61–63]. A meta-analysis of
8 cohort and 19 observational studies examined the
relation between menopausal HT and ovarian
cancer, estimating the risks for less than 5 years,
6–10 and more than 10 years use as 1.02, 1.13 and
1.21, respectively [64]. A more recent systematic
review examined a total of 14 publications, including
case–control, cohort and randomised studies con-
cerning the use of oestrogen-alone (ET) or oestrogen
associated to progestin treatment (EPT) and the risk
of ovarian cancer. The use of ET and EPT for 5 years
significantly increased this risk (RR: 1.22 and 1.10,
respectively) [63]. It seems that progestin addition
may slightly reduce cancer risk related to ET. The
Danish National Cancer Registry provides interest-
ing information regarding HT and ovarian cancer
incidence in a total of 909,946 of women. During a
follow up of 8 years, there were 3068 incident ovarian
cancers, of which 2681 were epithelial ones. Among
current HT users ovarian cancer incidences were
1.38 and 1.44 for epithelial ovarian cancers. In-
creased ovarian cancer risk was independent of
treatment duration, formulations, progestin used
and route of administration. It seems that cancer
risk disappears more than 2–4 years after HT
discontinuation. Incidence rates in current and never
HT users were respectively 0.52 and 0.40 per 1000
years [62].
New aspects regarding carcinogenesis are emer-
ging, including the importance of tumour origin and
distribution. Thus, it has been postulated that some
serous tumours may originate in the fimbria or
peritoneoum where p53 tumour suppressor gene
mutations have been found [65].
Clinical symptoms of the asymptomatic killer
It is assumed that early ovarian cancer diagnosis
results in better survival and also assumed that stages
I and II progress to stage III and IV. However,
neither of the two assumptions has been clearly
demonstrated. Early stages of ovarian cancers have
an insidious onset and cause no or non-specific
symptoms. Most women with ovarian cancer have
one or several symptoms, including abdominal pain
or discomfort, bloating, back pain, urinary urgency,
pelvic pain, abnormal genital bleeding and abdom-
inal mass or unjustified weight loss [66–69]. Because
of the lack of early symptoms or non-specific nature
of these, about two-thirds of patients with ovarian
cancer present in FIGO stages III and IV, having
tumour dissemination in the abdominal cavity, with
or without varying degrees of pleural effusion.
Pavlik et al. [70] have reported the value of clinical
symptoms as compared to ultrasound for the early
detection of ovarian cancer malignancy. Hence, in a
selected group of women, clinical symptoms were
correlated with ultrasound vaginal findings, being
respectively sensitivity 73% versus 20%. Clinical
symptoms have higher specificity (91%) in benign
tumours than in malignant ones (74%). In this
regard, studied tumours that are negative by both
symptom and ultrasound assessment are likely to be
benign, and by adding to symptoms information
ultrasound malignancy assessment increases sensi-
tivity only 3.3%.
Ultrasound features of incidental adnexal
masses
The diagnosis of an adnexal mass is usually
established by ultrasound. Prevalence of adnexal
masses is influenced by the number of scanned
women, the inclusion criteria used in each study, and
may increase with some endocrine treatments
[71,72] Simple cysts are more common than
previously thought (2.5–14%) and are frequently
diagnosed incidentally [4,8,73–75]. In many cases,
bidimensional (2D) ultrasound examination is suffi-
cient to give a clear diagnosis of benign or malignant
ovarian lesions. However, in clinical practice there
are many overlapping situations. Thus, some malig-
nancies are detected as simple cyst without a
complex morphological image, and contrarily some
very complex images may correspond to benign
pathological findings.
Three-dimensional (3D) sonography is currently a
major development in ultrasound imaging with a
significantly higher sensitivity, specificity and accu-
racy as compared to 2D ultrasound [76]. 3D
ultrasound characterises an entire soft tissue volume
by storing multiple 2D images. Computer software
then rapidly creates a tridimensional image. Despite
the fact that 3D ultrasound is gaining clinical
acceptance it seems, however, that in routine practice
it will not replace conventional 2D ultrasound.
Indeed those who support 3D ultrasound vascular
assessment for the differential diagnosis of an adnexal
mass consider this procedure still under research
[74,76]. To improve results, colour Doppler assess-
ment of intratumoural blood flow has been proposed.
It is based upon assigning red colour to flow directing
toward the transducer and blue colour for flow
directing away. Colour Doppler flow imaging is very
useful in the detection of uterine adnexal malignan-
cies because of the frequent neovascularisation found
Menopause and ovarian cancer 633
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
BSC
O o
n 09
/06/
10Fo
r pe
rson
al u
se o
nly.
Page 4
in these cases [7–9,77,78]. However, considerable
overlapping exists between benign and malignant
adnexal masses in terms of resistance (RI) and
pulsatility (PI) indices. Therefore, colour Doppler
RI measurements cannot be used alone for the
detection of malignant ovarian tumours. Further-
more, results from ultrasound explorations are highly
dependent on individual operator dedication and
technical expertises [79]. The use of power Doppler
3D implies new haemodynamic indices, such as the
flow index, vascularisation index and the flow
vascularisation index, which replace the traditional
RI and PI. This allows performing flow volumetric
calculations. Vascular tridimensionality may be
assessed and the mean vascular density calculated
for any tumoural area calculated. In this sense, the
most recent technology constitutes the virtual organ
computer-aided analysis that allows to automatically
obtaining angiographic volumes of spherical or
regular structures, as well as of irregular ones.
Ultrasonographic morphological features of incidental
adnexal masses
The morphological characteristics found at ultra-
sound may suggest the type of lesion. Complex
intracystic ovarian masses, including solid and
parietal irregularities, are associated with ovarian
carcinoma, suggesting these findings as significant
markers of malignancy [4]. Sonographic character-
istics of an incidental early ovarian cancer include
multilocular or multiple cysts, irregular thick septa or
walls, poor-defined borders, papillar growths, solid
elements and echogenic components [77,80,81].
Transvaginal sonography has relatively low positive
predictive value for ovarian cancer, in some studies
with a 10% value in post-menopausal women
[81,82]. The presence of a purely solid tumour is
highly suspicious of metastatic cancer rather than a
primary ovarian cancer [78]. The presence of ascites
is suggestive of malignancy but may be related to
other causes. Careful examination of the abdominal
cavity should be performed to detect the extent of
the disease.
Paraovarian (peritoneal inclusion close to the
ovary) and paratubal cysts constitute up to 10% of
all adnexal masses [83], being more frequent in
young women than in menopausal ones. Upon
ultrasound examination they may be separately
identified from ovaries (76%) as thin walled,
anechoic and unilocular cysts. Most usually in these
cases ovaries are normal [84]. However, sometimes
they display solid nodular areas within the cyst,
septations, thick or irregular walls [85,86].
Sonographical features of incidentally detected
small ovarian dermoids are better detected by means
of transvaginal ultrasound. They generally appear as
a solid homogeneous or heterogeneous hyperechoic
image, sometimes with a full fluid area and a
hyperechoic focus in its wall, an inconstant mixed
pattern with solid and liquid areas or calcifications
and a frequent posterior or lateral acoustic shadow-
ing [87]. Ultrasonographic morphology has a high
accuracy and specificity in differentiating dermoid
cysts from other adnexal masses [88].
Ovarian cystadenofibromas are infrequent epithe-
lial tumours that include fibrous stroma as the
dominant element and usually appear during the
fourth and fifth decade of life. Although in many
cases they are simple cysts, sometimes they may have
solid and liquid components, therefore simulating
upon ultrasound assessment as malignant neoplasms
[89]. Ovarian Brenner tumours may also be often
incidentally found in women in their 60s, being in 2–
5% of cases malignant [90]. During ultrasound
assessment, these tumours are in two-third of cases
solid, multilocular and partially cystic epithelial
nests; sometimes affecting both ovaries, and asso-
ciated to other benign ovarian neoplasms [91].
Borderline ovarian tumours show similar ultra-
sonographic morphological findings as malignant
lesions (89%), including intracystic papillae, diffuse
internal echogenicity, intracystic septs, heteroge-
neous images and a solid pattern [92]. However,
neither papillae nor other sonographic features
are sensitive ultrasound markers for borderline
tumours [93].
Vascular Doppler assessment of ovarian tumours
Tumour angiogenesis is an essential part of tumour
growth and development. Angiogenesis in early small
tumours may be studied with Doppler ultrasound by
measuring resistive indices that show the down-
stream impedance to blood flow within a vessel.
Doppler ultrasound findings include: a dominant
cyst mass, solid papillar projections and vascularisa-
tion. The latter is present in almost half of cases
appearing with a typical peripheral pattern and
vessels of high blood impedance [72,77–79]. In
some cases, malignant tumours display low potential
for inducing an angiogenic response or vessels are so
small and fail in being detected by color and pulsed
Doppler. Specificity for cancer diagnosis may reach
97% and the positive predictive value 91% [94,95].
Nevertheless, overlaps in terms of findings between
malignant and benign cases have been long recog-
nised. Medeiros et al. [96] carried out a systematic
review to estimate the accuracy of colour Doppler
sonography in the diagnosis of ovarian tumours.
Diagnosis was confirmed by paraffin-embedded
pathology study. The pooled sensitivity was 0.87
(95% CI: 0.84–0.90) and the specificity was 0.92
(95% CI: 0.87–0.90). Receiver operating character-
istic curves demonstrated that colour Doppler is a
valid tool prior to surgery in predicting the diagnosis
634 F. R. Perez-Lopez et al.
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
BSC
O o
n 09
/06/
10Fo
r pe
rson
al u
se o
nly.
Page 5
of ovarian tumours. Colour Doppler imaging for
borderline ovarian tumours have lower PI and RI
compared to benign lesions [92].
3D ultrasound in combination with power Dop-
pler provides better morphologic visualisation of
complex ovarian masses (the tumour per se or its
vascularisation), significantly improving preoperative
diagnostic accuracy of suspected ovarian lesions. A
significant problem with power Doppler is that
information regarding speed and flow direction is
lacking, and the technique is highly dependent on
operator expertise. To define an ovarian malignancy
the presence of at least two of the following findings
have been proposed: irregular branching, vessel
diameter changes, microaneurysms and vascular
lakes [79].
Paraovarian, paratubal or peritoneal pseudocysts
may be diagnosed by 2D and 3D ultrasound. In one
retrospective study, pathological paraovarian cyst
findings were assessed preoperatively with 2D
sonography and power Doppler evaluation. In 30%
of cases there were papillary projections within the
cyst, and in a quarter of these cases the papillae had
blood vessels. Malignancy risk is low in cases without
papillar growths; however, when wall proliferations
are found this may correspond to borderline ovarian
tumours [86].
Assessing the Doppler flow characteristics of
dermoid cysts has been intended to differentiate
benign ovarian cystic teratoma from malignant cases.
Thus, intratumoural blood flow is more frequent in
malignant teratomas compared to benign ones.
Malignant teratomas usually have RI less than 0.4
and PI less than 0.6, while peak systolic velocity
values are similar in benign and malignant teratomas
[97]. Ovarian struma ovarii represent 5% of cases of
ovarian dermoid cysts, and most women are pre-
menopausal with a mean lesion diameter of 5 cm and
normal CA 125 values. Although blood flow signals
may be present and low resistance to flow may be
more common in struma ovarii, it is difficult to
distinguish between struma ovarii and dermoid cysts
on the basis of their sonographic appearance [98].
Figure 1 presents the general morphological
characteristics of incidental adnexal masses found
at ultrasound. Finally, a need to emphasise that there
are ovarian cancers that – very early in its develop-
ment – produce peritoneal dissemination without
significant ovarian growth, and therefore, a normal
ovarian ultrasound exploration is not synonymous of
absence of malignant disease. Van Nagell et al. [99]
have clearly established this possibility in their long
term ultrasound follow up of the Kentucky cohort.
Tumour markers
Elevation alone of serum tumour markers are not diag-
nostic, only suggestive of malignancy or related
lesions, and some markers are so non-specific that
their increase may be associated to benign conditions.
Ovarian tumour markers should ideally be specific for
each one, indicating what type of cancer is present, or
predicting treatment outcome. However, markers
may be non-specifically produced in high levels by
different cells – ovarian or extraovarian – which suffer
various alterations in their biochemical machinery.
Unfortunately, a unique and ideal tumour marker is
currently not available. Genomic advances may
improve ovarian cancer detection in the near future
when used with diagnostic imaging.
CA 125, tumour-associated trypsin inhibitor, afoetoprotein and chorionic gonadotrophin
Initial optimism for markers such as CA 125, CA
19.9, CA 72-4, CASA, CYFRA and others to be
Figure 1. General morphologic characteristics of incidental adnexal masses in peri- and post-menopausal women according to ultrasound
findings.
Menopause and ovarian cancer 635
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
BSC
O o
n 09
/06/
10Fo
r pe
rson
al u
se o
nly.
Page 6
used in combination with ultrasound, has been
confronted because of their non-specific nature in
detecting ovarian malignant lesions and borderline
tumours [100–103]. Serum CA 125 is the only
validated marker for ovarian cancer, and it is useful
for follow up purposes and evaluating treatment
response or disease recurrence. However, it is not a
diagnostic or prognostic marker [104]. The utility of
serum CA125 in the identification of early stages of
epithelial ovarian cancer is shadowed by the fact that
not all cancers display elevated levels [105], and
since isolated CA125 values lack adequate sensitivity
or specificity [106]. CA 125 screening for the general
population is impaired by the low cancer incidence
and the high rates of false positive [107]. Several
benign gynaecological conditions, such as first
trimester pregnancy, pelvic inflammatory disease,
uterine fibroids, ovarian cysts, pelvic adhesions and
endometriosis may be associated to elevated CA 125
levels [108,109]. These conditions are exceptional in
post-menopausal women. Therefore, CA 125 may
regain some application in this population for the
detection of ovarian malignancies. In addition, serial
CA 125 determinations at 3–4 week intervals may
detect increases associated to malignant growth.
Contrarily benign adnexal masses should not associ-
ate to abrupt marker increases but rather stable or
diminishing values.
The natural history of ovarian cancer development
in relation to changes in serum CA 125 level has been
studied in the Shizuoka Cohort Study on Ovarian
Cancer Screening. In this study, CA 125 measure-
ment was performed to 396 women with ovarian
cancer 4.1 years (mean) before confirming diagnosis.
The change of CA125 level before the diagnosis of
ovarian cancer could be clearly separated into two
groups according to the length of the following
intervals: 47% (107/228) of patients with non-serous-
type ovarian cancers develop secondarily from slightly
elevated CA125 level (355CA1255 65 U/ml), with
a mean interval of 3.8 years. On the other hand, 75%
(126/168) of patients with serous-type ovarian cancer
seem to develop suddenly from a normal CA125 level
(CA1255 35 U/ml), with a mean interval of 1.4 years
(p¼ 0.011) [110]. In a small number of cases,
ultrasonographic abnormalities associated to normal
CA 125 values result in cancer found at surgery [111].
Therefore, depending on the tumour type CA 125
elevation may present a different behaviour and
elevation velocity, or even with low values a cancer
may be present. These possibilities should be care-
fully considered when evaluating incidental ovarian
masses.
Tumour-associated trypsin inhibitor (TATI) has
been considered as a potential polypeptide tumour
marker for mucinous ovarian carcinomas, colorectal
cancer and other tumours [112,113]. In mucinous
ovarian tumours, TATI has an 89% specificity and
an 86% positive predictive value for malignancy.
However, less than half of ovarian cancers – even at
advanced stages7 express tissue trypsinogen-1 and 2
and TATI, although TATI tissue expression is an
adverse prognostic factor, independent of cancer
clinical stage and histological tumour type [114]. In
patients with epithelial ovarian carcinoma, using a
cut-off of 21 ng/ml TATI had a 63% sensitivity and
72% specificity, as compared – respectively – to 80%
and 82% for CA 125 at a cut-off value of 35 U/ml.
When measurement of both markers were combined
(TATI4 21 ng/ml or CA 1254 35 U/ml) specificity
was 65% [115]. It seems that despite its limitations,
CA 125 is the single marker of choice for suspicious
epithelial ovarian malignancy. TATI measurement
may be helpful as an additional marker in combina-
tion with CA 125 when mucinous carcinomas are
suspected.
Human a foetoprotein (AFP) and chorionic
gonadotrophin are the main tumour markers for
germ cell tumours, including ovarian and extragona-
dal germ cell tumours as well as malignant teratomas
of any location. In females, germ cell tumours
represent a third of ovarian tumours, but only 1–
3% are malignant tumours [116]. These tumours are
infrequent in menopausal women. In recent years
several messenger RNA AFP isoforms have been
described, opening new insights for the development
of specific diagnostic possibilities for the cited
ovarian tumours [117].
New tumour markers
In recent years concerns have been reported
regarding the validation of new biomarkers and
risks. Inhibin may complement CA 125 in the
assessment of malignant ovarian cancers; although
there is limited information since studies have been
confined to advanced cases [118,119]. Inhibin is
elevated in post-menopausal women with granulose
cell tumour and in mucinous epithelial cancers, and
less frequently in epithelial serous and endome-
trioid ovarian carcinoma subtypes [118,120,121].
In peri-menopausal women, inhibin measurements
are of less value for ovarian cancer detection
because it may be elevated in relation to the
menstrual cycle. Serum anti-mullerian hormone
levels have been studied for the diagnosis and
follow-up of granulose cell tumours [119]. This
serum hormone is a more specific parameter than
inhibin for granulose cell cancers, since inhibin may
also increase in some mucinous epithelial ovarian
tumours [122].
Human epididymis protein 4 (HE4) is a protease
overexpressed by patients with epithelial ovarian
cancers and found elevated in circulating blood
[123]. Serum HE4 measurements allow to dif-
ferentiate epithelial ovarian cancers from benign
636 F. R. Perez-Lopez et al.
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
BSC
O o
n 09
/06/
10Fo
r pe
rson
al u
se o
nly.
Page 7
pathology, including endometriosis [124,125]. Ser-
um HE4 levels have equal sensitivities as CA 125 for
ovarian malignancy detection [126]. However, it
seems that HE4 sensitivity increase when combined
with CA 125 or other marker [127–129]. There is a
group of ovarian cancer cases that do not express Ca
125 nor HE4, and perhaps combining both markers
could be complementary by improving sensitivity for
detecting epithelial cancers [130,131].
Mesothelin is a glycoprotein expressed by normal
mesothelial cells, and overexpressed in different types
tumours including ovarian carcinomas. It is also a
potential target for cancer immunotherapy [132].
Women with diagnosed ovarian cancer show a cor-
relation between high mesothelin levels and che-
moresistance and poor survival [133]. It has been
postulated that the interaction between mesothelin
and CA 125 may be involved in the peritoneal disse-
mination, although the available information is limi-
ted [134]. There are at least three mesothelins, and by
means of flow cytometry the most frequent molecule
in ovarian cancer cells is mesothelin 1 [135].
Decoy receptor 3 (DcR3) or DD-C248 is a
protein member of the tumour necrosis receptor
family that prevents apoptosis via direct binding of
Fas-ligand. Elevated DcR3 tumour tissue and/or
serum levels have been reported in gastrointestinal
and ovarian cancers. In advance ovarian cancers
with ascites, DcR3 has been associated with
negative outcomes [136,137]. B7-H4 or protein
DD-O110 is expressed in activated T-cells and is
involved in cell mediated immunity [138]. This
protein has been demonstrated in ovarian and
breast cancer cells using immunohistochemical
techniques [139]. Patients with ovarian cancer
show elevated serum levels as compared to those
with benign gynaecological disease or healthy
women. The value of B7-H4 measurements seems
to rely as a complement to CA 125 determination
in the detection of early stage ovarian cancer [140].
Spondin 2 or protein DD-P108 has been demon-
strated in prostate and ovarian cancers [136,141].
New diagnostic markers have not yet been
validated for clinical use [142–144]. The utility of
combining several biomarkers is currently under
study. Recent results point out to the fact that a
panel of different markers may inform about ovarian
cancer existence before symptoms appear [145]. It
seems that CA 125, HE4 and mesothelin began to
slightly increase some 3 years before diagnosis;
however, detectable elevations only were present
within the final year before diagnosis. Nosov et al.
[146] have reported that a serum panel including Ca
125, apolipoprotein A-1, transthyretin and transfer-
rin are useful for the detection of early-stage cancer
(I–II), being the highest sensitivity for the endome-
trioid subtype. However, as authors concluded
prospective clinical studies are needed.
Optimism of these results should be carefully
considered to prevent massive testing which later
might demonstrate to be cost ineffective, stressful
and useless, as occurred in the past. In fact,
Anderson et al. [145] insist in the low discriminatory
power of their used markers. Although these studies
are scientifically encouraging, they are difficult to
extrapolate to the early diagnosis and clinical
management of ovarian cancer of any individual
subject due to the low prevalence of the disease,
tumour heterogeneity and the psychosomatic impli-
cations of implementing a screening programme with
non-standardised tests.
Proteomic technology
Proteomic technology may allow studying new
biomarkers for the early diagnosis of malignant
and pre-malignant stages. These targets may
theoretically be the first step in the development
of new diagnostic and therapeutical tools. Tu-
mour tissue, plasma and ascitis samples have
been studied to delineate the signals involved in
ovarian cancer [147–151]. However, attempts to
link genetics, molecular characterisation of the
system and clinical measures has not yet been
successful [152–155]. There is a need for further
developments in serum proteomic analysis to
develop more specific screening methods for
ovarian cancer and to differentiate from benign
lesions.
Magnetic resonance imaging
Although sonography is the primary imaging
approach for the diagnosis of adnexal masses,
magnetic resonance imaging (MRI) provides
additional information on the composition of
soft-tissue masses [156–158]. Normal ovaries and
dysfunctional cysts have been detailed by MRI at
different ages [159]. MRI has a 90–98% overall
accuracy for differentiating benign from malignant
adnexal tumours. Simple and complex cysts may be
clearly identified by MRI with a high degree of
precision [160–163]. Benign solid lesions may
include fat, haemorrhage or fibrous components.
Thus, mature teratomas possessed high fat content
and contained derivatives of all three germ layers,
although with predominance of ectodermal compo-
nents [164]. Ovarian fibromas and cystadenofibro-
mas have a dense fibrous tissue [165,166]. Using
MRI, paraovarian and paratubal cysts located near
the ipsilateral round ligament and the uterus may be
separately defined from the ovary [167]. Although
preoperative MRI is not free of misinterpretations
when correlating adnexal mass images with patholo-
gical findings, malignancy diagnosis is often not
[168,169].
Menopause and ovarian cancer 637
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
BSC
O o
n 09
/06/
10Fo
r pe
rson
al u
se o
nly.
Page 8
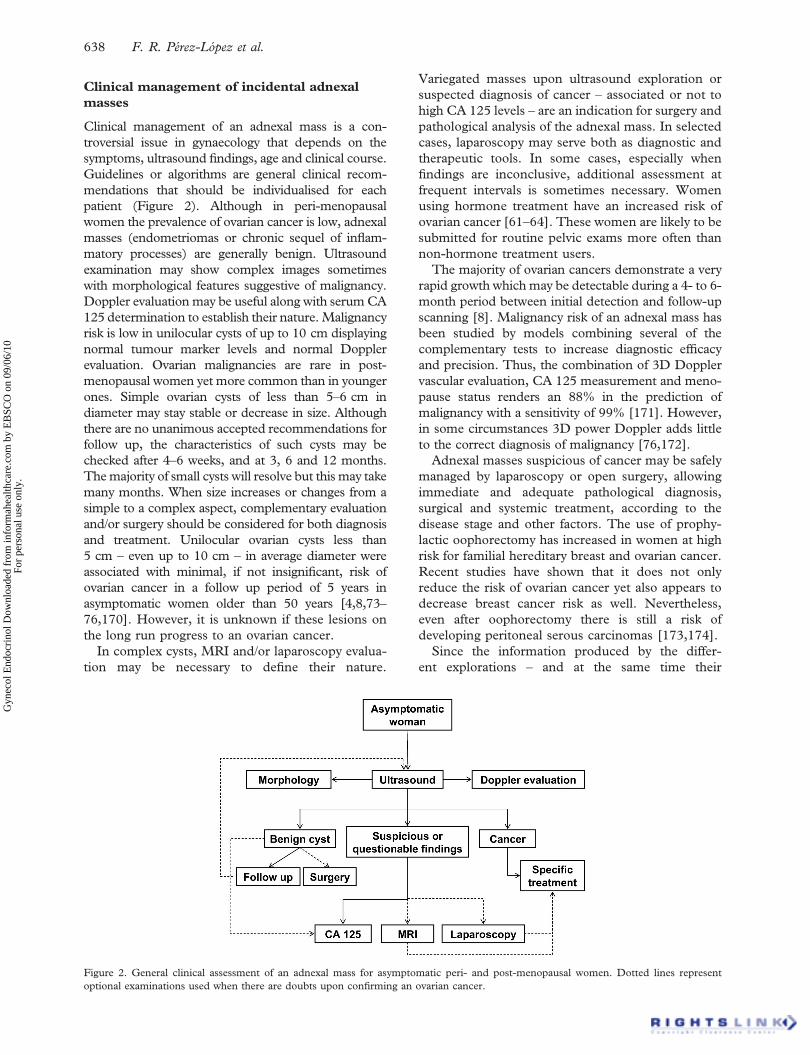
Clinical management of incidental adnexal
masses
Clinical management of an adnexal mass is a con-
troversial issue in gynaecology that depends on the
symptoms, ultrasound findings, age and clinical course.
Guidelines or algorithms are general clinical recom-
mendations that should be individualised for each
patient (Figure 2). Although in peri-menopausal
women the prevalence of ovarian cancer is low, adnexal
masses (endometriomas or chronic sequel of inflam-
matory processes) are generally benign. Ultrasound
examination may show complex images sometimes
with morphological features suggestive of malignancy.
Doppler evaluation may be useful along with serum CA
125 determination to establish their nature. Malignancy
risk is low in unilocular cysts of up to 10 cm displaying
normal tumour marker levels and normal Doppler
evaluation. Ovarian malignancies are rare in post-
menopausal women yet more common than in younger
ones. Simple ovarian cysts of less than 5–6 cm in
diameter may stay stable or decrease in size. Although
there are no unanimous accepted recommendations for
follow up, the characteristics of such cysts may be
checked after 4–6 weeks, and at 3, 6 and 12 months.
The majority of small cysts will resolve but this may take
many months. When size increases or changes from a
simple to a complex aspect, complementary evaluation
and/or surgery should be considered for both diagnosis
and treatment. Unilocular ovarian cysts less than
5 cm – even up to 10 cm – in average diameter were
associated with minimal, if not insignificant, risk of
ovarian cancer in a follow up period of 5 years in
asymptomatic women older than 50 years [4,8,73–
76,170]. However, it is unknown if these lesions on
the long run progress to an ovarian cancer.
In complex cysts, MRI and/or laparoscopy evalua-
tion may be necessary to define their nature.
Variegated masses upon ultrasound exploration or
suspected diagnosis of cancer – associated or not to
high CA 125 levels – are an indication for surgery and
pathological analysis of the adnexal mass. In selected
cases, laparoscopy may serve both as diagnostic and
therapeutic tools. In some cases, especially when
findings are inconclusive, additional assessment at
frequent intervals is sometimes necessary. Women
using hormone treatment have an increased risk of
ovarian cancer [61–64]. These women are likely to be
submitted for routine pelvic exams more often than
non-hormone treatment users.
The majority of ovarian cancers demonstrate a very
rapid growth which may be detectable during a 4- to 6-
month period between initial detection and follow-up
scanning [8]. Malignancy risk of an adnexal mass has
been studied by models combining several of the
complementary tests to increase diagnostic efficacy
and precision. Thus, the combination of 3D Doppler
vascular evaluation, CA 125 measurement and meno-
pause status renders an 88% in the prediction of
malignancy with a sensitivity of 99% [171]. However,
in some circumstances 3D power Doppler adds little
to the correct diagnosis of malignancy [76,172].
Adnexal masses suspicious of cancer may be safely
managed by laparoscopy or open surgery, allowing
immediate and adequate pathological diagnosis,
surgical and systemic treatment, according to the
disease stage and other factors. The use of prophy-
lactic oophorectomy has increased in women at high
risk for familial hereditary breast and ovarian cancer.
Recent studies have shown that it does not only
reduce the risk of ovarian cancer yet also appears to
decrease breast cancer risk as well. Nevertheless,
even after oophorectomy there is still a risk of
developing peritoneal serous carcinomas [173,174].
Since the information produced by the differ-
ent explorations – and at the same time their
Figure 2. General clinical assessment of an adnexal mass for asymptomatic peri- and post-menopausal women. Dotted lines represent
optional examinations used when there are doubts upon confirming an ovarian cancer.
638 F. R. Perez-Lopez et al.
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
BSC
O o
n 09
/06/
10Fo
r pe
rson
al u
se o
nly.
Page 9
limitations – patients should know the advantages and
risk of a conservative management in complex cysts.
Surgery and pathologic study will give assurance in
those cases which are not clear or present overlapping
benign and malignant features. As in many medical
aspects clinical management of adnexal masses
should be guided by evidence. Furthermore, clinical
management should consider full diagnostic and
therapeutic opportunities provided by available tools,
not by biased selection of a technique or procedure.
Acknowledgements
This study was partially supported by the B/017543/
08 AECID (Agencia Espanola de Cooperacion
Internacional para el Desarrollo) grant.
References
1. Young RC. Gynecologic malignancies. In: Fauci AS,
Harrison TR, Kasper DL, Braunwald E, Isselbacher KJ,
editors. Harrison’s principles of internal medicine. 16th ed.
New York: McGraw Hill; 2005. pp. 553–558.
2. Walsh CS, Blum A, Walts A, Alsabeh R, Tran H, Koeffler
HP, Karlan BY. Lynch syndrome among gynecologic
oncology patients meeting Bethesda guidelines for screening.
Gynecol Oncol, 2010;116:516–521.
3. South SA, Vance H, Farrell C, DiCioccio RA, Fahey C, Piver
MS, Rodabaugh KJ. Consideration of hereditary nonpoly-
posis colorectal cancer in BRCA mutation-negative familial
ovarian cancers. Cancer 2009;115:324–333.
4. Bailey CL, Ueland FR, Land GL, DePriest PD, Gallion HH,
Kryscio RJ, van Nagell JR Jr. The malignant potential of
small cystic ovarian tumors in women over 50 years of age.
Gynecol Oncol 1998;69:3–7.
5. Christensen JT, Boldsen JL, Westergaard JG. Functional
ovarian cysts in premenopausal and gynecologically healthy
women. Contraception 2002;66:153–157.
6. Dorum A, Blom GP, Ekerhovd E, Granberg S. Prevalence and
histologic diagnosis of adnexal cysts in postmenopausal women:
an autopsy study. Am J Obstet Gynecol 2005;192:48–54.
7. Drake J. Diagnosis and management of the adnexal
mass. Am Fam Physician 1998;57:2471–2476, 2479–2480.
8. McDonald J, Modesitt SC. The incidental postmeno-
pausal adnexal mass. Clin Obstet Gynecol 2006;49:506–516.
9. Vuento MH, Pirhonen JP, Makinen JI, Laippala PJ,
Gronroos M, Salmi TA. Evaluation of ovarian findings in
asymptomatic postmenopausal women with color Doppler
ultrasound. Cancer 1995;76:1214–1218.
10. Healy DL, Bell R, Robertson DM, Jobling T, Oehler MK,
Edwards A, Shekleton P, Oldham J, Piessens S, Teoh M,
et al. Ovarian status in healthy postmenopausal women.
Menopause 2008;15:1109–1114.
11. U.S. Preventive Services Task Force. Screening for ovarian
cancer: recommendation statement. Am Fam Physician
2005;71:759–762.
12. Menon U, Gentry-Maharaj A, Hallett R, Ryan A, Burnell M,
Sharma A, Lewis S, Davies S, Philpott S, Lopes A, et al.
Sensitivity and specificity of multimodal and ultrasound
screening for ovarian cancer, and stage distribution of
detected cancers: results of the prevalence screen of the UK
Collaborative Trial of Ovarian Cancer Screening (UKC-
TOCS). Lancet Oncol 2009;10:327–340.
13. Clarke-Pearson DL. Clinical practice. Screening for ovarian
cancer. N Engl J Med 2009;361:170–177.
14. Comerci JT Jr, Licciardi F, Bergh PA, Gregori C, Breen JL.
Mature cystic teratoma: a clinicopathologic evaluation of 517
cases and review of the literature. Obstet Gynecol 1994;84:
22–28.
15. Finch A, Beiner M, Lubinski J, Lynch HT, Moller P, Rosen
B, Murphy J, Ghadirian P, Friedman E, Foulkes WD, et al.
Hereditary Ovarian Cancer Clinical Study Group. Salpingo-
oophorectomy and the risk of ovarian, fallopian tube, and
peritoneal cancers in women with a BRCA1 or BRCA2
Mutation. JAMA 2006;296:185–192.
16. Rosenthal A, Jacobs I. Familial ovarian cancer screening.
Best Pract Res Clin Obstet Gynaecol 2006;20:321–
338.
17. van der Velde NM, Mourits MJ, Arts HJ, de Vries J, Leegte
BK, Dijkhuis G, Oosterwijk JC, de Bock GH. Time to stop
ovarian cancer screening in BRCA1/2 mutation carriers? Int J
Cancer 2009;124:919–923.
18. Berry NB, Bapat SA. Ovarian cancer plasticity and epige-
nomics in the acquisition of a stem-like phenotype. J Ovarian
Res 2008;1:8.
19. Cochard LR, Netter FH. The urogenital system. In: Netter’s
atlas of human embryology, Teterboro, NJ: Icon Learning
Systems; 2002. Chapter 7, pp 157–183.
20. Scully RE. Pathology of ovarian cancer precursors. J Cell
Biochem 1995;23 (Suppl):208–218.
21. Brown PO, Palmer C. The preclinical natural history of
serous ovarian cancer: defining the target for early detection.
PLoS Med 2009;6:e1000114.
22. Thomassen M, Jochumsen KM, Mogensen O, Tan Q, Kruse
TA. Gene expression meta-analysis identifies chromosomal
regions involved in ovarian cancer survival. Genes Chromo-
somes Cancer 2009;48:711–724.
23. Bendoraite A, Knouf EC, Garg KS, Parkin RK, Kroh EM,
O’Briant KC, Ventura AP, Godwin AK, Karlan BY,
Drescher CW, et al. Regulation of miR-200 family micro-
RNAs and ZEB transcription factors in ovarian cancer:
evidence supporting a mesothelial-to-epithelial transition.
Gynecol Oncol 2010;116:117–125.
24. Fischer D, Thome M, Becker S, Cordes T, Diedrich K,
Friedrich M, Thill M. Expression of 25-hydroxyvitamin D3–
24-hydroxylase in benign and malignant ovarian cell lines
and tissue. Anticancer Res 2009;29:3635–3639.
25. Karihtala P, Soini Y, Vaskivuo L, Bloigu R, Puistola U. DNA
adduct 8-hydroxydeoxyguanosine, a novel putative marker of
prognostic significance in ovarian carcinoma. Int J Gynecol
Cancer 2009;19:1047–1051.
26. Wang K, Gan L, Jeffery E, Gayle M, Gown AM, Skelly M,
Nelson PS, Ng WV, Schummer M, Hood L, et al. Montoring
gene expression profile changes in ovarian carcinomas using
cDNA microarray. Gene 1999;229:101–108.
27. Ono K, Tanaka T, Tsunoda T, Fujita M, Miwa N, Tanaka
T, Tsunoda T, Yang KC, Nakamura Y, Furukawa Y.
Identification by cDNA microarray of genes involved in
ovarian carcinogenesis. Cancer Res 2000;60:5007–5011.
28. Ross DT, Scherf U, Eisen MB, Perou CM, Rees C,
Spellman P, Iyer V, Jeffrey SS, Van de Rijn M, Waltham
M, et al. Systematic variation in gene expression patterns
in human cancer cell lines. Nat Genet 2000;24:227–
235.
29. Shridhar V, Lee J, Pandita A, Iturria S, Avula R, Staub J,
Morrissey M, Calhoun E, Sen A, Kalli K, et al. Genetic
analysis of early- versus late-stage ovarian tumors. Cancer
Res 2001;61:5895–5904.
30. Ahluwalia A, Hurteau JA, Bigsby RM, Nephew KP. DNA
methylation in ovarian cancer. II. Expression of DNA
methyltransferases in ovarian cancer cell lines and normal
ovarian epithelial cells. Gynecol Oncol 2001;82:299–304.
31. Feeley KM, Wells M. Precursor lesions of ovarian epithelial
malignancy. Histopathology 2001;38:87–95.
Menopause and ovarian cancer 639
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
BSC
O o
n 09
/06/
10Fo
r pe
rson
al u
se o
nly.
Page 10
32. Hoskins WJ. Histologic changes in the ovaries of cancer-
prone women: an indication of premalignant change? J Natl
Cancer Inst 1996;88:1790–1791.
33. Salazar H, Godwin AK, Daly MB, Laub PB, Hogan WM,
Rosenblum N, Boente MP, Lynch HT, Hamilton TC.
Microscopic benign and invasive malignant neoplasms and a
cancer-prone phenotype in prophylactic oophorectomies. J
Natl Cancer Inst 1996;88:1810–1820.
34. Werness BA, Afify AM, Bielat KL, Eltabbakh GH, Piver MS,
Paterson JM. Altered surface and cyst epithelium of ovaries
removed prophylactically from women with a family history
of ovarian cancer. Hum Pathol 1999;30:151–157.
35. Piek JM, Verheijen RH, Menko FH, Jongsma AP, Weegen-
aar J, Gille JJ, Pals G, Kenemans P, van Diest PJ. Expression
of differentiation and proliferation related proteins in
epithelium of prophylactically removed ovaries from women
with a hereditary female adnexal cancer predisposition.
Histopathology 2003;43:26–32.
36. Parrott JA, Doraiswamy V, Kim G, Mosher R, Skinner MK.
Expression and actions of both the follicle stimulating
hormone receptor and the luteinizing hormone receptor in
normal ovarian surface epithelium and ovarian cancer. Mol
Cell Endocrinol 2001;172:213–222.
37. Leung PC, Choi JH. Endocrine signaling in ovarian surface
epithelium and cancer. Hum Reprod Update 2007;13:143–162.
38. Laviolette LA, Garson K, Macdonald EA, Senterman MK,
Courville K, Crane CA, Vanderhyden BC. 17{beta}-
estradiol accelerates tumor onset and decreases survival in a
transgenic mouse model of ovarian cancer. Endocrinology,
2010;151:928–938.
39. Bagnardi V, Blangiardo M, La Vecchia C, Corrao G. Alcohol
consumption and the risk of cancer: a meta-analysis. Alcohol
Res Health 2001;25:263–270.
40. Soegaard M, Jensen A, Høgdall E, Christensen L, Høgdall
C, Blaakaer J, Kjaer SK. Different risk factor profiles for
mucinous and nonmucinous ovarian cancer: results from the
Danish MALOVA study. Cancer Epidemiol Biomarkers Prev
2007;16:1160–1166.
41. Jordan SJ, Whiteman DC, Purdie DM, Green AC, Webb
PM. Does smoking increase risk of ovarian cancer? A
systematic review. Gynecol Oncol 2006;103:1122–1129.
42. Jordan SJ, Siskind V, C Green A, Whiteman DC, Webb PM.
Breastfeeding and risk of epithelial ovarian cancer. Cancer
Causes Control, 2010;21:109–116.
43. Collaborative Group on Epidemiological Studies of Ovarian
Cancer; Beral V, Doll R, Hermon C, Peto R, Reeves G.
Ovarian cancer and oral contraceptives: collaborative reana-
lysis of data from 45 epidemiological studies including
23,257 women with ovarian cancer and 87,303 controls.
Lancet 2008;371:303–314.
44. Delort L, Kwiatkowski F, Chalabi N, Satih S, Bignon YJ,
Bernard-Gallon DJ. Central adiposity as a major risk factor of
ovarian cancer. Anticancer Res 2009;29:5229–5234.
45. Lahmann PH, Cust AE, Friedenreich CM, Schulz M,
Lukanova A, Kaaks R, Lundin E, Tjønneland A, Halkjær J,
Severinsen MT, et al. Anthropometric measures and epithelial
ovarian cancer risk in the European Prospective Investigation
into Cancer and Nutrition. Int J Cancer, 2010;126:2404–2415.
46. Gates MA, Rosner BA, Hecht JL, Tworoger SS. Risk factors
for epithelial ovarian cancer by histologic subtype. Am J
Epidemiol 2010;171:45–53.
47. Rossing MA, Cushing-Haugen KL, Wicklund KG, Doherty
JA, Weiss NS. Recreational physical activity and risk of
epithelial ovarian cancer. Cancer Causes Control, 2010;21:
485–491.
48. Toriola AT, Surcel HM, Agborsangaya C, Grankvist K,
Tuohimaa P, Toniolo P, Lukanova A, Pukkala E, Lehtinen
M. Serum 25-hydroxyvitamin D and the risk of ovarian
cancer. Eur J Cancer, 2010;46:364–369.
49. Kotsopoulos J, Baer HJ, Tworoger SS. Anthropometric
measures and risk of epithelial ovarian cancer: results from
the nurses’ health study. Obesity (Silver Spring), in press.
50. Amsterdam A, Sasson R. The anti-inflammatory action of
glucocorticoids is mediated by cell type specific regulation of
apoptosis. Mol Cell Endocrinol 2002;189:1–9.
51. Nilsson EE, Skinner MK. Role of transforming growth factor
beta in ovarian surface epithelium biology and ovarian
cancer. Reprod Biomed Online 2002;5:254–258.
52. Wong AS, Leung PC. Role of endocrine and growth factors
on the ovarian surface epithelium. J Obstet Gynaecol Res
2007;33:3–16.
53. Galli MC, De Giovanni C, Nicoletti G, Grilli S, Nanni P,
Prodi G, Gola G, Rocchetta R, Orlandi C. The occurrence of
multiple steroid hormone receptors in disease free and
neoplastic human ovary. Cancer 1981;47:1297–1302.
54. Slotman BJ, Rao BR. Ovarian cancer (review): etiology,
diagnosis, prognosis, surgery, radiotherapy, chemotherapy
and endocrine therapy. Anticancer Res 1988;8:417–434.
55. Perez-Lopez FR, Campo C, Ibanez F, Blasco C. Receptores
de estrogenos y de progesterona en ovarios sanos y
tumorales. Acta Ginecologica (Madrid) 1992;49:115–122.
56. Chien J, Fan JB, Bell DA, April C, Klotzle B, Ota T, Lingle
WL, Gonzalez Bosquet J, Shridhar V, Hartmann LC.
Analysis of gene expression in stage I serous tumors identifies
critical pathways altered in ovarian cancer. Gynecol Oncol
2009;114:3–11.
57. Drummond A, Fuller P. The importance of ER{beta}
signalling in ovarian function. J Endocrinol, 2010;205:15–23.
58. Parker LP, Taylor DD, Kesterson S, Gercel-Taylor C. Gene
expression profiling in response to estradiol and genistein in
ovarian cancer cells. Cancer Genomics Proteomics
2009;6:189–194.
59. Yoshida S, Furukawa N, Haruta S, Tanase Y, Kanayama S,
Noguchi T, Sakata M, Yamada Y, Oi H, Kobayashi H.
Expression profiles of genes involved in poor prognosis of
epithelial ovarian carcinoma: a review. Int J Gynecol Cancer
2009;19:992–997.
60. Boyer A, Goff AK, Boerboom D. WNT signaling in ovarian
follicle biology and tumorigenesis. Trends Endocrinol
Metab, in press.
61. Beral V, Bull D, Green J, Reeves G; Million Women Study
Collaborators,. Ovarian cancer and hormone replacement
therapy in the Million Women Study. Lancet 2007;369:
1703–1710.
62. Mørch LS, Løkkegaard E, Andreasen AH, Kruger-Kjaer S,
Lidegaard O. Hormone therapy and ovarian cancer. JAMA
2009;302:298–305.
63. Pearce CL, Chung K, Pike MC, Wu AH. Increased ovarian
cancer risk associated with menopausal estrogen therapy is
reduced by adding a progestin. Cancer 2009;115:531–539.
64. Zhou B, Sun Q, Cong R, Gu H, Tang N, Yang L, Wang B.
Hormone replacement therapy and ovarian cancer risk: a
meta-analysis. Gynecol Oncol. 2008;108:641–651.
65. Crum CP, Drapkin R, Kindelberger D, Medeiros F, Miron A,
Lee Y. Lessons from BRCA: the tubal fimbria emerges as an
origin for pelvic serous cancer. Clin Med Res 2007;5:35–44.
66. Goff BA, Mandel L, Muntz HG, Melancon CH. Ovarian
carcinoma diagnosis. Cancer 2000;89:2068–2075.
67. Goff BA, Mandel LS, Melancon CH, Muntz HG. Frequency
of symptoms of ovarian cancer in women presenting to
primary care clinics. JAMA 2004;291:2705–2712.
68. Bankhead CR, Kehoe ST, Austoker J. Symptoms associated
with diagnosis of ovarian cancer: a systematic review. BJOG
2005;112:857–865.
69. Ryerson AB, Eheman C, Burton J, McCall N, Blackman D,
Subramanian S, Richardson LC. Symptoms, diagnoses, and
time to key diagnostic procedures among older U.S. women
with ovarian cancer. Obstet Gynecol 2007;109:1053–1061.
640 F. R. Perez-Lopez et al.
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
BSC
O o
n 09
/06/
10Fo
r pe
rson
al u
se o
nly.
Page 11
70. Pavlik EJ, Saunders BA, Doran S, McHugh KW, Ueland FR,
Desimone CP, Depriest PD, Ware RA, Kryscio RJ, van
Nagell JR Jr. The search for meaning-Symptoms and
transvaginal sonography screening for ovarian cancer: pre-
dicting malignancy. Cancer 2009;115:3689–3698.
71. Kazandi M, Sendag F, Akercan F, Terek MC, Ozsaran A,
Dikmen Y. Ovarian cysts in postmenopausal tamoxifen-
treated breast cancer patients with endometrial thickening
detected by transvaginal sonography. Eur J Gynaecol Oncol
2002;23:257–260.
72. Cohen I, Potlog-Nahari C, Shapira J, Yigael D, Tepper R.
Simple ovarian cysts in postmenopausal patients with breast
carcinoma treated with tamoxifen: long-term follow-up.
Radiology 2003;227:844–848.
73. Hata K, Hata T, Kitao M. Intratumoral peak systolic velocity
as a new possible predictor for detection of adnexal
malignancy. Am J Obstet Gynecol 1995;172:1496–1500.
74. Oyelese Y, Kueck AS, Barter JF, Zalud I. Asymptomatic
postmenopausal simple ovarian cyst. Obstet Gynecol Surv
2002;57:803–809.
75. Alcazar JL, Galan MJ, Ceamanos C, Garcıa-Manero M.
Transvaginal gray scale and color Doppler sonography in
primary ovarian cancer and metastatic tumors to the ovary. J
Ultrasound Med 2003;22:243–247.
76. Alcazar JL. Ecografıa y angiografıa power Doppler tridimen-
sional en el diagnostico diferencial de las masas anexiales:
Estado actual. Rev Chil Ultrasonog 2008;11:4–9.
77. Wolf I, Gosink BB, Feldesman MR, Lin MC, Stuenkel CA,
Braly PS, Pretorius DH. Prevalence of simple adnexal cysts
in postmenopausal women. Radiology 1991;180: 65–71.
78. Modessit SC, Pavlik EJ, Ueland FR, DePriest PD, Kryscio
RJ, van Nagell JR. Risk of malignancy in unilocular ovarian
cystic tumors less than 10 centimeters in diameter. Obstet
Gynecol 2003;102:594–599.
79. Castillo G, Alcazar JL, Jurado M. Natural history of
sonographically detected simple unilocular adnexal cysts in
asymptomatic postmenopausal women. Gynecol Oncol
2004;92:965–969.
80. Valentin L, Ameye J, Testa A, Lecuru F, Bernard JP,
Paladini D, Van Huffel S, Timmerman D. Ultrasound
characteristics of different types of adnexal malignancies.
Gynecol Oncol 2006;102:41–48.
81. van Nagell JR Jr, DePriest PD, Ueland FR, DeSimone CP,
Cooper AL, McDonald JM, Pavlik EJ, Kryscio RJ. Ovarian
cancer screening with annual transvaginal sonography:
findings of 25,000 women screened. Cancer 2007;109:
1887–1896.
82. van Nagell JR, DePriest PD, Puls LE, Donaldson ES,
Gallion HH, Pavlik EJ, Powell DE, Kryscio RJ. Ovarian
cancer screening in asymptomatic postmenopausal women
by transvaginal sonography. Cancer 1991;68:458–462.
83. Barloon TJ, Brown BP, Abu-Yousef MM, Warnock NG.
Paraovarian and paratubal cysts: preoperative diagnosis using
transabdominal and transvaginal sonography. J Clin Ultra-
sound 1996;24:117–122.
84. Kim JS, Woo SK, Suh SJ, Morettin LB. Sonographic
diagnosis of paraovarian cysts: value of detecting a separate
ipsilateral ovary. AJR Am J Roentgenol 1995;164:1441–1444.
85. Korbin CD, Brown DL, Welch WR. Paraovarian cystade-
nomas and cystadenofibromas: sonographic characteristics in
14 cases. Radiology 1998;208:459–462.
86. Savelli L, Ghi T, De Iaco P, Ceccaroni M, Venturoli S,
Cacciatore B. Paraovarian/paratubal cysts: comparison of trans-
vaginal sonographic and pathological findings to establish diag-
nostic criteria. Ultrasound Obstet Gynecol 2006;28:330–334.
87. Serafini G, Quadri PG, Gandolfo NG, Gandolfo N,
Martinoli C, Derchi LE. Sonographic features of incidentally
detected, small, nonpalpable ovarian dermoids. J Clin
Ultrasound 1999;27:369–373.
88. Ekici E, Soysal M, Kara S, Dogan M, Gokmen O. The
efficiency of ultrasonography in the diagnosis of dermoid
cysts. Zentralbl Gynakol 1996;118:136–141.
89. Alcazar JL, Errasti T, Mınguez JA, Galan MJ, Garcıa-
Manero M, Ceamanos C. Sonographic features of ovarian
cystadenofibromas: spectrum of findings. J Ultrasound Med
2001;20:915–919.
90. Yamamoto R, Fujita M, Kuwabara M, Sogame M, Ebina Y,
Sakuragi N, Kato H, Fujimoto S. Malignant Brenner tumors
of the ovary and tumor markers: case reports. Jpn J Clin
Oncol 1999;29:308–313.
91. Green GE, Mortele KJ, Glickman JN, Benson CB. Brenner
tumors of the ovary: sonographic and computed tomographic
imaging features. J Ultrasound Med 2006;25:1245–1251.
92. Pascual MA, Tresserra F, Grases PJ, Labastida R, Dexeus S.
Borderline cystic tumors of the ovary: gray-scale and color
Doppler sonographic findings. J Clin Ultrasound 2002;30:
76–82.
93. Exacoustos C, Romanini ME, Rinaldo D, Amoroso C,
Szabolcs B, Zupi E, Arduini D. Preoperative sonographic
features of borderline ovarian tumors. Ultrasound Obstet
Gynecol 2005;25:50–59.
94. Alcazar JL, Ruiz-Perez ML, Errasti T. Transvaginal color
Doppler sonography in adnexal masses: which parameter
performs best? Ultrasound Obstet Gynecol 1996;8:114–119.
95. Buy JN, Ghossain MA, Hugol D, Hassen K, Sciot C, Truc
JB, Poitout P, Vadrot D. Characterization of adnexal masses:
combination of color Doppler and conventional sonography
compared with spectral Doppler analysis alone and conven-
tional sonography alone. AJR Am J Roentgenol 1996;
166:385–393.
96. Medeiros LR, Rosa DD, da Rosa MI, Bozzetti MC.
Accuracy of ultrasonography with color Doppler in ovarian
tumor: a systematic quantitative review. Int J Gynecol Cancer
2009;19:1214–1220.
97. Emoto M, Obama H, Horiuchi S, Miyakawa T, Kawar-
abayashi T. Transvaginal color Doppler ultrasonic character-
ization of benign and malignant ovarian cystic teratomas and
comparison with serum squamous cell carcinoma antigen.
Cancer 2000;88:2298–2304.
98. Zalel Y, Seidman DS, Oren M, Achiron R, Gotlieb W,
Mashiach S, Goldenberg M. Sonographic and clinical char-
acteristics of struma ovarii. J Ultrasound Med 2000;19:857–861.
99. van Nagell JR Jr, DePriest PD, Ueland FR, DeSimone CP,
Cooper AL, McDonald JM, Pavlik EJ, Kryscio RJ. Ovarian
cancer screening with annual transvaginal sonography: findings
of 25,000 women screened. Cancer 2007;109:1887–1896.
100. Hasholzner U, Baumgartner L, Stieber P, Meier W,
Hofmann K, Fateh-Moghadam A. Significance of the tumour
markers CA 125 II, CA 72-4, CASA and CYFRA 21-1 in
ovarian carcinoma. Anticancer Res 1994;14:2743–2746.
101. Schutter EM, Davelaar EM, van Kamp GJ, Verstraeten RA,
Kenemans P, Verheijen RH. The differential diagnostic
potential of a panel of tumor markers (CA 125, CA 15-3, and
CA 72-4 antigens) in patients with a pelvic mass. Am J
Obstet Gynecol 2002;187:385–392.
102. Ayhan A, Guven S, Guven ES, Kucukali T. Is there a
correlation between tumor marker panel and tumor size and
histopathology in well staged patients with borderline ovarian
tumors? Acta Obstet Gynecol Scand 2007;86:484–490.
103. Tsao KC, Hong JH, Wu TL, Chang PY, Sun CF, Wu JT.
Elevation of CA 19-9 and chromogranin A, in addition to CA
125, are detectable in benign tumors in leiomyomas and
endometriosis. J Clin Lab Anal 2007;21:193–196.
104. Meyer T, Rustin GJ. Role of tumour markers in monitoring
epithelial ovarian cancer. Br J Cancer 2000;82:1535–1538.
105. Chu CS, Rubin SC. Screening for ovarian cancer in the
general population. Best Pract Res Clin Obstet Gynecol
2006;20:307–320.
Menopause and ovarian cancer 641
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
BSC
O o
n 09
/06/
10Fo
r pe
rson
al u
se o
nly.
Page 12
106. Bast RC Jr. Status of tumor markers in ovarian cancer
screening. J Clin Oncol 2003;21(10 Suppl):200s–205s.
107. Jacobs IJ, Skates S, Davies AP, Woolas RP, Jeyerajah A,
Weidemann P, Sibley K, Oram DH. Risk of diagnosis of
ovarian cancer after raised serum CA 125 concentration: a
prospective cohort study. BMJ 1996;313:1355–1358.
108. Seow K-M, Lin Y-H, Hsieh B-C, Huang LW, Pan HS,
Chang JZ, Chen HJ, Hwang JL. Transvaginal three-dimen-
sional ultrasonography combined with serum CA125 level
for the diagnosis of pelvic adhesions before laparoscopic
surgery. J Am Assoc Gynecol Laparosc 2003;10:320–326.
109. Sevinc A, Camci C, Turk HM, Buyukberber S. How to
interpret serum CA125 levels in patients with serosal
involvement? A clinical dilemma. Oncol Rev 2003;65:1–6.
110. Kobayashi H, Ooi H, Yamada Y, Sakata M, Kawaguchi R,
Kanayama S, Sumimoto K, Terao T. Serum CA125 level
before the development of ovarian cancer. International J
Gynecol Obstet 2007;99:95–99.
111. Kobayashi H, Yamada Y, Sado T, Sakata M, Yoshida S,
Kawaguchi R, Kanayama S, Shigetomi H, Haruta S, Tsuji Y,
et al. Prevalence of ovarian cancer among women with a
CA125 level of 35 U/ml or less. Gynecol Obstet Invest
2008;65:133–138.
112. Mogensen O, Mogensen B, Jakobsen A. Tumour-associated
trypsin inhibitor (TATI) and cancer antigen 125 (CA 125)
in mucinous ovarian tumours. Br J Cancer 1990;61:327–
329.
113. Solakidi S, Tiniakos DG, Petraki K, Stathopoulos GP,
Markaki I, Androulakis G, Sekeris CE. Co-expression of
trypsin and tumour-associated trypsin inhibitor (TATI) in
colorectal adenocarcinomas. Histol Histopathol 2003;18:
1181–1188.
114. Paju A, Vartiainen J, Haglund C, Itkonen O, von Bogus-
lawski K, Leminen A, Wahlstrom T, Stenman UH. Expres-
sion of trypsinogen-1, trypsinogen-2, and tumor-associated
trypsin inhibitor in ovarian cancer: prognostic study on tissue
and serum. Clin Cancer Res 2004;10:4761–4768.
115. Peters-Engl C, Medl M, Ogris E, Leodolter S. Tumor-
associated trypsin inhibitor (TATI) and cancer antigen 125
(CA125) in patients with epithelial ovarian cancer. Antic-
ancer Res 1995;15:2727–2730.
116. Roth LM, Talerman A. Recent advances in the pathology
and classification of ovarian germ cell tumors. Int J Gynecol
Pathol 2006;25:305–320.
117. Tagaya H, Fukasawa H, Shoda T, Hoshi K, Hirata S. Novel
alpha-fetoprotein-V messenger RNA isoforms in humans.
Reprod Sci 2009;16:794–801.
118. Robertson DA, Pruysers E, Jobling T. Inhibin as a diagnostic
marker for ovarian cancer. Cancer Lett 2007;249:14–17.
119. Geerts I, Vergote I, Neven P, Billen J. The role of inhibins B
and antimullerian hormone for diagnosis and follow-up of
granulosa cell tumors. Int J Gynecol Cancer 2009;19:847–
855.
120. Healy DL, Burger HG, Mamers P, Jobling T, Bangah M,
Quinn M, Grant P, Day AJ, Rome R, Campbell JJ. Elevated
serum inhibin concentrations in postmenopausal women with
ovarian tumours, New Eng J Med 1993;329:1539–1542.
121. Lappohn RE, Burger HG, Bouma J, Bangah M, Krans M, de
Bruijn HWA. Inhibin as a marker for granulose cell tumours.
New Engl J Med 1989;321:790–793.
122. Geerts I, Vergote I, Neven P, Billen J. The role of inhibins B
and antimullerian hormone for diagnosis and follow-up of
granulosa cell tumors. Int J Gynecol Cancer 2009;19:847–
855.
123. Drapkin R, von Horsten HH, Lin Y, Mok SC, Crum CP,
Welch WR, Hecht JL. Human epididymis protein 4 (HE4) is
a secreted glycoprotein that is overexpressed by serous and
endometrioid ovarian carcinomas. Cancer Res 2005;65:
2162–2169.
124. Hellstrom I, Hellstrom KE. SMRP and HE4 as biomarkers for
ovarian carcinoma when used alone and in combination with
CA125 and/or each other. Adv Exp Med Biol 2008;622:15–21.
125. Huhtinen K, Suvitie P, Hiissa J, Junnila J, Huvila J, Kujari H,
Setala M, Harkki P, Jalkanen J, Fraser J, et al. Serum HE4
concentration differentiates malignant ovarian tumours from
ovarian endometriotic cysts. Br J Cancer 2009;100:1315–1319.
126. Shah CA, Lowe KA, Paley P, Wallace E, Anderson GL,
McIntosh MW, Andersen MR, Scholler N, Bergan LA,
Thorpe JD, et al. Influence of ovarian cancer risk status on
the diagnostic performance of the serum biomarkers me-
sothelin, HE4, and CA125. Cancer Epidemiol Biomark Prev
2009;18:1365–1372.
127. Lowe KA, Shah C, Wallace E, Anderson G, Paley P,
McIntosh M, Andersen MR, Scholler N, Bergan L, Thorpe
J, et al. Effects of personal characteristics on serum CA125,
mesothelin, and HE4 levels in healthy postmenopausal
women at high-risk for ovarian cancer. Cancer Epidemiol
Biomarkers Prev 2008;17:2480–2487.
128. Moore RG, Brown AK, Miller MC, Skates S, Allard WJ,
Verch T, Steinhoff M, Messerlian G, DiSilvestro P, Granai
CO, et al. The use of multiple novel tumor biomarkers for
the detection of ovarian carcinoma in patients with a pelvic
mass. Gynecol Oncol 2008;108:402–408.
129. Andersen MR, Goff BA, Lowe KA, Scholler N, Bergan L,
Dresher CW, Paley P, Urban N. Combining a symptoms
index with CA 125 to improve detection of ovarian cancer.
Cancer 2008;113:484–489.
130. Rosen DG, Wang L, Atkinson JN, Yu Y, Lu KH, Diamandis
EP, Hellstrom I, Mok SC, Liu J, Bast RC Jr. Potential
markers that complement expression of CA125 in epithelial
ovarian cancer. Gynecol Oncol 2005;99:267–277.
131. Moore RG, Brown AK, Miller MC, Skates S, Allard WJ,
Verch T, Steinhoff M, Messerlian G, DiSilvestro P, Granai
CO, et al. The use of multiple novel tumor biomarkers for
the detection of ovarian carcinoma in patients with a pelvic
mass. Gynecol Oncol 2007;108:402–408.
132. Feng Y, Xiao X, Zhu Z, Streaker E, Ho M, Pastan I,
Dimitrov DS. A novel human monoclonal antibody that
binds with high affinity to mesothelin-expressing cells and
kills them by antibody-dependent cell-mediated cytotoxicity.
Mol Cancer Ther, in press.
133. Cheng WF, Huang CY, Chang MC, Hu YH, Chiang YC,
Chen YL, Hsieh CY, Chen CA. High mesothelin correlates
with chemoresistance and poor survival in epithelial ovarian
carcinoma. Br J Cancer 2009;100:1144–1153.
134. Gubbels JA, Belisle J, Onda M, Rancourt C, Migneault M,
Ho M, Bera TK, Connor J, Sathyanarayana BK, Lee B, et al.
Mesothelin-MUC16 binding is a high affinity, N-glycan
dependent interaction that facilitates peritoneal metastasis of
ovarian tumors. Mol Cancer 2006;5:50.
135. Hellstrom I, Raycraft J, Kanan S, Sardesai NY, Verch T,
Yang Y, Hellstrom KE. Mesothelin variant 1 is released from
tumor cells as a diagnostic marker. Cancer Epidemiol
Biomarkers Prev 2006;15:1014–1020.
136. Simon I, Liu Y, Krall KL, Urban N, Wolfert RL, Kim NW,
McIntosh MW. Evaluation of the novel serum markers B7-
H4, Spondin 2, and DcR3 for diagnosis and early detection
of ovarian cancer. Gynecol Oncol 2007;106:112–118.
137. Connor JP, Felder M. Ascites from epithelial ovarian cancer
contain high levels of functional decoy receptor 3 (DcR3)
and is associated with platinum resistance. Gynecol Oncol
2008;111:330–335.
138. Collins M, Ling V, Carreno BM. The B7 family of immune-
regulatory ligands. Genome Biol 2005;6:223.1–223.7.
139. Tringler B, Liu W, Corral L, Torkko KC, Enomoto T,
Davidson S, Lucia MS, Heinz DE, Papkoff J, Shroyer KR.
B7-H4 over-expression in ovarian cancer. Gynecol Oncol
2006;100:44–52.
642 F. R. Perez-Lopez et al.
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
BSC
O o
n 09
/06/
10Fo
r pe
rson
al u
se o
nly.
Page 13
140. Simon I, Zhou S, Corral L, Diamandis EP, Sarno MJ,
Wolfert RL, Kim NW. B7-H4 is a novel membrane-bound
protein and a candidate serum and tissue biomarker for
ovarian cancer. Cancer Res 2006;66:1570–1575.
141. Parry R, Schneider D, Hudson D, Parkes D, Xuan JA,
Newton A, Toy P, Lin R, Harkins R, Alicke B, et al.
Identification of a novel prostate tumor target, mindin/RG-1,
for antibody-based radiotherapy of prostate cancer. Cancer
Res 2005;65:8397–8405.
142. Kong F, Nicole White C, Xiao X, Feng Y, Xu C, He D,
Zhang Z, Yu Y. Using proteomic approaches to identify new
biomarkers for detection and monitoring of ovarian cancer.
Gynecol Oncol 2006;100:247–253.
143. Coates RJ, Kolor K, Stewart SL, Richardson LC. Diagnostic
markers for ovarian cancer screening: not ready for routine
clinical use. Clin Cancer Res 2008;14:7575–7576.
144. Visintin I, Feng Z, Longton G, Ward DC, Alvero AB, Lai Y,
Tenthorey J, Leiser A, Flores-Saaib R, Yu H, et al.
Diagnostic markers for early detection of ovarian cancer.
Clin Cancer Res 2008;14:1062–1072.
145. Anderson GL, McIntosh M, Wu L, Barnett M, Goodman G,
Thorpe JD, Bergan L, Thornquist MD, Scholler N, Kim N,
et al. Assessing lead time of selected ovarian cancer
biomarkers: a nested case-control study. J Natl Cancer Inst
2010;102:26–38.
146. Nosov V, Su F, Amneus M, Birrer M, Robins T, Kotlerman
J, Reddy S, Farias-Eisner R. Validation of serum biomarkers
for detection of early-stage ovarian cancer. Am J Obstet
Gynecol 2009;200:639.e1–639e.5.
147. Wong AS, Kim SO, Leung PC, Auersperg N, Pelech SL.
Profiling of protein kinases in the neoplastic transformation
of human ovarian surface epithelium. Gynecol Oncol
2001;82:305–311.
148. Wulfkuhle JD, Aquino JA, Calvert VS, Fishman DA, Coukos
G, Liotta LA, Petricoin EF III. Signal pathway profiling of
ovarian cancer from human tissue specimens using reverse-
phase protein microarrays. Proteomics 2003;3:2085–2090.
149. Mor G, Visintin I, Lai Y, Zhao H, Schwartz P, Rutherford T,
Yue L, Bray-Ward P, Ward DC. Serum protein markers for
early detection of ovarian cancer. PNAS 2005;102:7677–7782.
150. Wang J, Zhang X, Ge X, Guo H, Xiong G, Zhu Y.
Proteomic studies of early-stage and advanced ovarian cancer
patients. Gynecol Oncol 2008;111:111–119.
151. Cadron I, Van Gorp T, Timmerman D, Amant F, Waelkens
E, Vergote I. Application of proteomics in ovarian cancer:
which sample should be used? Gynecol Oncol 2009;
115:497–503.
152. Palmer C, Duan X, Hawley S, Scholler N, Thorpe JD,
Sahota RA, Wong MQ, Wray A, Bergan LA, Drescher CW,
et al. Systematic evaluation of candidate blood markers for
detecting ovarian cancer. PLoS One 2008;3:e2633.
153. Khalil I, Brewer MA, Neyarapally T, Runowicz CD. The
potential of biologic network models in understanding the
etiopathogenesis of ovarian cancer. Gynecol Oncol, in press.
154. Gunawardana CG, Kuk C, Smith CR, Batruch I, Soosaipillai
A, Diamandis EP. Comprehensive analysis of conditioned
media from ovarian cancer cell lines identifies novel
candidate markers of epithelial ovarian cancer. J Proteome
Res 2009;8:4705–4713.
155. Tinelli A, Vergara D, Martignago R, Leo G, Pisano M,
Malvasi A. An outlook on ovarian cancer and borderline
ovarian tumors: focus on genomic and proteomic findings.
Curr Genomics 2009;10:240–249.
156. Outwater EK, Dunton CJ. Imaging of the ovary and adnexa:
clinical issues and applications of MR imaging. Radiol-
ogy1995;194:1–18.
157. Jeong YY, Outwater EK, Kang HK. Imaging evaluation of
ovarian masses. RadioGraphics 2000;20:1445–1470.
158. Huber S, Medl M, Baumann L, Czembirek H. Value of
ultrasound and magnetic resonance imaging in the pre-
operative evaluation of suspected ovarian masses. Anticancer
Res 2002;22:2501–2507.
159. Outwater EK, Mitchell DG. Normal ovaries and functional
cysts: MR appearance. Radiology 1996;198:397–402.
160. Hricak H, Chen M, Coakley FV, Kinkel K, Yu KK, Sica G,
Bacchetti P, Powell CB. Complex adnexal masses: detection
and characterization with MR imaging –multivariate analysis.
Radiology 2000;214:39–46.
161. Sohaib SAA, Sahdev A, Van Trappen P, Jacobs IJ, Reznek
RH. Characterization of adnexal lesions on MR imaging.
AJR 2003;180:1297–1304.
162. Temma-Asano K, Kimura T, Tsutsui T, Nobunaga T,
Samejima Y, Mitsuda N, Kameda T, Ohta Y, Yamamoto T,
Saji F, et al. MR imaging evaluation of postmenopausal
adnexal masses: correlation with final pathologic diagnosis.
Maturitas 2006;53:27–31.
163. Guerra A, Cunha TM, Felix A. Magnetic resonance
evaluation of adnexal masses. Acta Radiol 2008;49:700–
709.
164. Saini A, Dina R, McIndoe GA, Soutter WP, Gishen P,
deSouza NM. Characterization of adnexal masses with MRI.
AJR Am J Roentgenol 2005;184:1004–1009.
165. Outwater EK, Siegelman ES, Talerman A, Dunton C.
Ovarian fibromas and cystadenofibromas: MRI features of
the fibrous component. J Magn Reson Imaging 1997;7:465–
471.
166. Cho SM, Byun JY, Rha SE, Jung SE, Park GS, Kim BK,
Kim B, Cho KS, Jung NY, Kim SH, et al. CT and MRI
findings of cystadenofibromas of the ovary. Eur Radiol
2004;14:798–804.
167. Kishimoto K, Ito K, Awaya H, Matsunaga N, Outwater EK,
Siegelman ES. Paraovarian cyst: MR imaging features.
Abdom Imaging 2002;27:685–689.
168. Asch E, Levine D, Pedrosa I, Hecht JL, Kruskal J. Patterns of
misinterpretation of adnexal masses on CT and MR in an
academic radiology department. Acad Radiol 2009;16:969–
980.
169. Asch E, Levine D, Kim Y, Hecht JL. Histologic, surgical,
and imaging correlations of adnexal masses. J Ultrasound
Med 2008;27:327–342.
170. Valentin L, Akrawi D. The natural history of adnexal cysts
incidentally detected at transvaginal ultrasound examination
in postmenopausal women. Ultrasound Obstet Gynecol
2002;20:174–180.
171. Mansour GM, El-Lamie IK, El-Sayed HM, Ibrahim AM,
Laban M, Abou-Louz SK, Abd Allah MY, El-Mahallawi
MN, El-Lamie KI, Gad-Allah M. Adnexal mass vascularity
assessed by 3-dimensional power Doppler: does it add to the
risk of malignancy index in prediction of ovarian malignancy?
Four hundred-case study. Int J Gynecol Cancer 2009;19:
867–872.
172. Jokubkiene L, Sladkevicius P, Valentin L. Does three-
dimensional power Doppler ultrasound help in discrimina-
tion between benign and malignant ovarian masses? Ultra-
sound Obstet Gynecol 2007;29:215–225.
173. Kauff ND, Satagopan JM, Robson ME, Scheuer L, Hensley
M, Hudis CA, Ellis NA, Boyd J, Borgen PI, Barakat RR,
et al. Risk-reducing salpingo-oophorectomy in women with a
BRCA1 or BRCA2 mutation. New Eng J Med 2002;346:
1609–1615.
174. Rebbeck TR, Lynch HT, Neuhausen SL, Narod SA, Van’t
Veer L, Garber JE, Evans G, Isaacs C, Daly MB, Matloff E,
et al. Prevention and observation of Surgical End Points
Study Group. Prophylactic oophorectomy in carriers of
BRCA1 or BRCA2 mutation. New Eng J Med 2002;306:
1616–1622.
Menopause and ovarian cancer 643
Gyn
ecol
End
ocri
nol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
BSC
O o
n 09
/06/
10Fo
r pe
rson
al u
se o
nly.