Page 1
444 | The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019
CLINICAL RESEARCH
Periodontal considerations for
adhesive ceramic dental restorations:
key points to avoid gingival problems
Maristela Lobo, DDS, MsC, PhD
Professor of Advanced Program in Implant and Esthetic Dentistry, SENAC University,
Sao Paulo, Brazil
Oswaldo Scopin de Andrade, DDS, MSc, PhD
Director of Advanced Program in Implant and Esthetic Dentistry, SENAC University,
Sao Paulo, Brazil
João Malta Barbosa, DDS, MSc
Prosthodontist, Department of Oral Rehabilitation, Implantology Institute, Lisbon, Portugal
Volunteer Researcher, Department of Biomaterials and Biomimetics,
New York University College of Dentistry, New York, NY, USA
Ronaldo Hirata, DDS, MsC, PhD
Assistant Professor of Biomaterials, New York University College of Dentistry, New York, NY, USA
Correspondence to: Dr Maristela Maia Lobo
Rua Ministro Gabriel de Resende Passos, 500, Cj 1010, Moema São Paulo SP, Brazil;
Tel: +55 11 5051-3534/+55 11 9 9447-7436; Email: [email protected]
Page 2
LOBO ET AL
445The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019 | 445The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019 |
Abstract
The stability and health of the periodontal tissues
should be a common goal for all dental care providers
with regard to natural or restored teeth as well as im-
plant-supported restorations or any other type of
prosthesis. The objective of this study was to address
the key aspects to be respected when executing ad-
hesive oral rehabilitations involving ceramic restora-
tions, regardless of their thickness, and to reinforce
the importance of each step to ensure the success
and longevity of the treatment from a periodontal
standpoint. This article reviews the fundamentals of
the periodontics that relate directly or indirectly to ad-
hesive ceramic dental restorations, and also addresses
their clinical relevance.
(Int J Esthet Dent 2019;14:444–457)
Page 3
CLINICAL RESEARCH
446 | The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019
Introduction
A healthy periodontium should be the ulti-
mate goal for all professionals involved with
comprehensive oral rehabilitations because
the health and stability of the periodon-
tal-restorative transition is key to treatment
success.1 Unfortunately, frequent adhesive
rehabilitation failures occur because this
clear goal for prosthetic rehabilitations is
not sufficiently respected. These failures oc-
cur as recurrent gingivitis, localized or gen-
eralized, or as irreversible periodontal at-
tachment loss through gingival recession
and/or periodontal pocket formation that,
in extreme cases, may ultimately lead to
tooth loss.2,3 The recurrence of these clinic-
al scenarios may indicate that there has not
been enough commitment to periodontal
health by some dental professionals. It
therefore seems pertinent to reinforce the
importance of the commitment to health,
function, and esthetics, in that order. These
goals are fundamental to obtain the desired
longevity and stability for any provided treat-
ment.
The term ‘contact lenses’ has been in-
creasingly used worldwide by the dental
community as a marketing term to describe
thin porcelain veneers that aim to improve
smile esthetics without dental preparation
(no-prep veneers). However, clinical reality
has shown that only very few and highly
specific situations make it possible to avoid
the need for dental preparation while pro-
viding the space required for the restorative
material. In most clinical situations, the
need for a ceramic restoration is highly
subjective, and the request for such a treat-
ment by a patient may be comparable with
the desire to acquire a fashion/trendy item.
When a patient demands a treatment that
conflicts with the clinician’s recommenda-
tion, the clinician should educate the pa-
tient and explain the indications and contra-
indications of such a treatment so that a
fully informed decision can be taken. De-
spite this ideal approach, unfortunately
some clinicians seem more interested in
performing the treatment regardless of its
clinical indications, which leads to an in-
crease in overtreatments. As a conse-
quence, the rate of retreatments of recently
performed adhesive esthetic rehabilitations
due to periodontal compromises is also on
the rise. With that, the patient enters, often
at an early age, the so called ‘restorative cy-
cle,’ which sooner or later culminates in
tooth loss.4
Most failures occur from what can only
be seen as a lack of knowledge of the inter-
action between restorative dentistry and
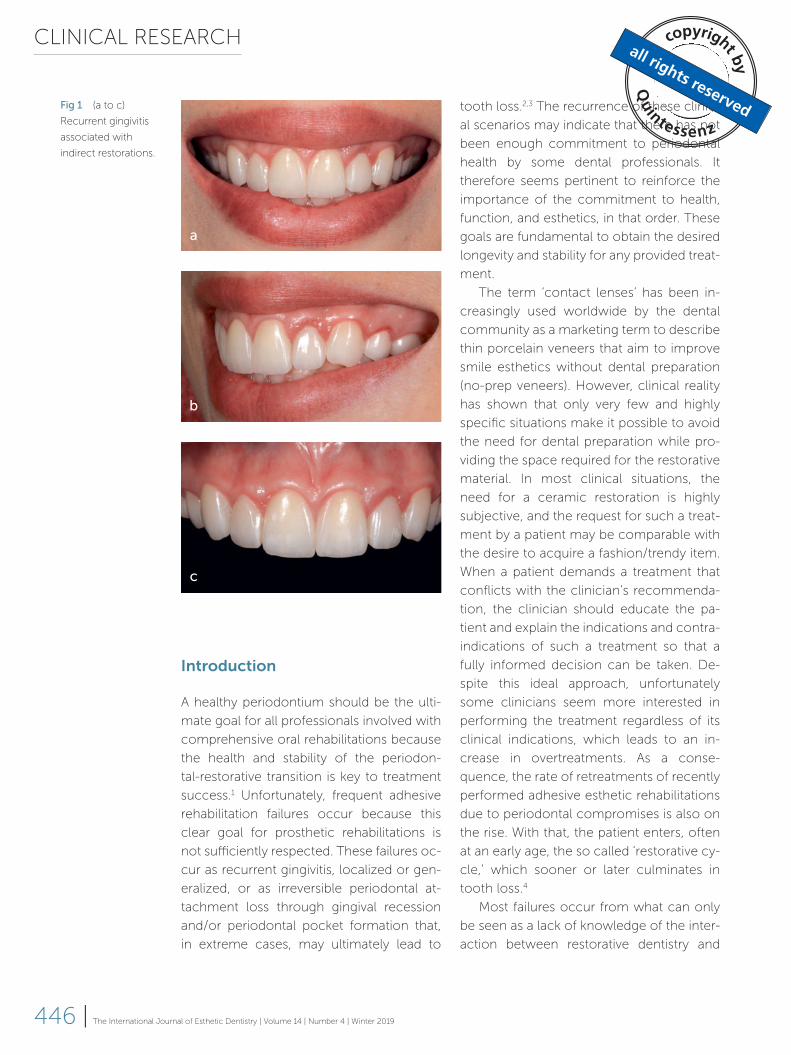
Fig 1 (a to c)
Recurrent gingivitis
associated with
indirect restorations.
a
b
c
Page 4
LOBO ET AL
447The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019 |
periodontics, sometimes combined with a
poor or careless technical execution (Figs 1
and 2). An important factor that seems to
potentiate these negative outcomes is the
presence of a thin/festooned periodontal
biotype, described to present an increased
risk of gingival margin instability and conse-
quent esthetic compromise.5 Patients with
delicate biotypes are more prone to devel-
oping gingival margin recession as a result
of a temporary or prolonged periodontal
aggression, often seen in adhesive rehabili-
tations with ‘contact lenses.’ Therefore, it is
important to recall patients presenting deli-
cate biotypes that require extra care when
managing soft tissues for restorative pur-
poses (ie, it can be stated that periodontal
tissues require clinical respect).
Periodontal clinical respect means to:
1. Preserve the biological space, avoiding
the direct contact of the restorative ma-
terials with the junctional epithelium (JE)
and/or the connective tissue (CT) attach-
ment.6,7
2. Optimize the emergence profile and the
cervical contour of the restoration by
avoiding overlapping or misadaptations
that may promote plaque accumulation
and/or affect the ideal food trajectory.8
3. Avoid excessive manipulation of the gin-
gival margin with retraction cords, he-
mostatic agents, clamps, impression ma-
terials, and inadequate instrumentation.9
4. Strive for excellent marginal adaptation,
with or without tooth preparation.
5. Avoid the contact of impregnated mater-
ials during cementation (retraction cords
and an excess of adhesive cement).
6. Ensure adequate sealing and adaptation
of the restoration in relation to the dental
substrate, avoiding misadaptations, voids,
and/or spaces susceptible to subsequent
plaque accumulation.10
The objective of this article is to address
the key factors or ‘rules’ to be respected
during the execution of adhesive ceramic
restorations, regardless of their thickness,
and to reinforce the importance of each
step to ensure the success and longevity of
the treatment from a periodontal stand-
point.
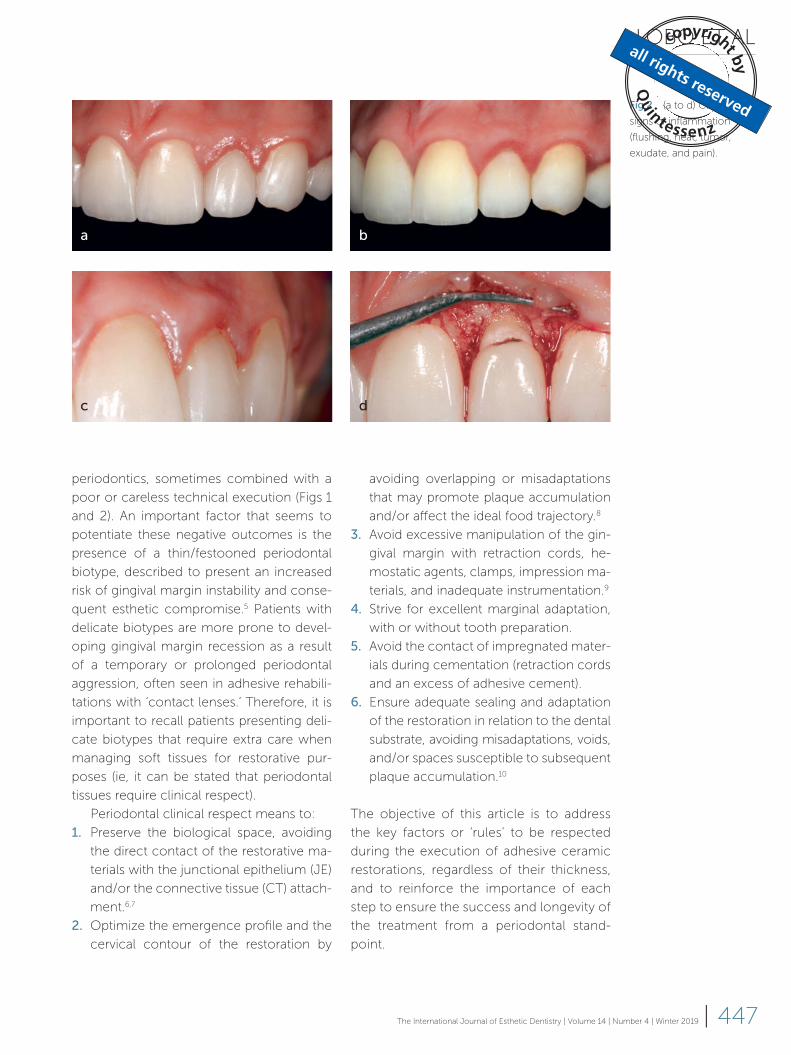
Fig 2 (a to d) Classic
signs of inflammation
(flushing, heat, tumor,
exudate, and pain).
a
c
b
d
Page 5
CLINICAL RESEARCH
448 | The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019
Rule 1: The biological equilibrium of prosthetic/periodontal transi-tion determines the success and longevity of the treatment
For the majority of mammals, teeth are ar-
ticulated organs. This imposes an anatomi-
cal challenge to the organism’s defense
system: one third of the tooth is exposed in
the oral cavity, in contact with the saliva
and diverse microorganisms, and the re-
maining two thirds are inserted within the
bony structure of the alveolar process.
Therefore, an efficient and reliable bio-
logical seal is essential to maintain a bio-
logical and ecological balance between
the external and internal environments so
as to prevent microorganisms from pene-
trating the systemic blood stream. This seal
exists through the combined functions of
the JE (epithelial seal) and the CT insertion
(connective seal), which in combination
form the so-called biological space11-13
(Fig 3).
The first line of periodontal defense
consists of the oral epithelium (OE), partic-
ularly the inserted gingiva. This epithelial
layer is stratified and keratinized as well as
impermeable and resistant to mechanical,
chemical, and bacterial aggressors.14 It is
considered to be part of the protective
periodontium as it plays a role in protecting
the more internal organic layer – the CT –
from coming into contact with external
agents. Like other epithelial tissues, the
periodontal epithelium exhibits little inter-
stitial space, with its constituting cells very
close to each other and with few to no
blood vessels. Therefore, the nutrition of
this outer layer is provided by the underly-
ing CT through the basal layer of the epi-
thelium. Often, with the goal of increasing
the area of nutrition, the epithelium can
project crests toward the inner CT that can
increase in number and size in the pres-
ence of inflammatory processes.15
Due to the dual environment (external
and internal) in which a tooth exists, the OE
invaginates toward the tooth surface to
form a sulcus. This sulcular epithelium (SE)
is less keratinized and has characteristics
similar to those of the OE, with a superficial
layer of keratin. This characteristic allows it
to seal the internal and external environ-
ments and therefore represents the primary
line of periodontal protection.16 On average,
it is 0.7 mm long in the vestibular surface
and 1.0 mm long in the interproximal sur-
face of the anterior teeth11 (Fig 3). It is clini-
cally important to recall that the SE can
only be evaluated histologically (eg, it is not
possible to perform a probing evaluation).
Fig 3 (a to c) A
biological seal is
provided by the
combined functions
of the junctional
epithelium and the
connective tissue
insertion, which in
combination form
the biological space.a
b
c
Connective sealing
Epithelial sealingGingival sealing
Page 6
LOBO ET AL
449The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019 |
However, it can be assumed that, as this is a
transition tissue, it will present much vari-
ability among different individuals and
should be considered the anatomical and
histological limit for the intracrevicular level
of a restorative margin preparation.
A second epithelial layer – the JE – lies
underneath the SE and presents distinct his-
tological characteristics compared with the
OE and the gingival epithelium. The JE is
not keratinized and is therefore permeable,
allowing for fluid exchange between the in-
ternal and external environments. The JE
only presents two layers of cells – the exter-
nal lamina (EL) and the internal basal lamina
(IBL) – with only the former providing tissue
stability and sealing by adhering weakly to
the surface of the enamel through hemides-
mosomes.16 It is through the JE that the hu-
moral and cellular defenses come into con-
tact with external agents, as in cases of
tissue inflammation. Additionally, the JE is
responsible for the secretion of the gingival
crevicular fluid.
In cases of lesioning (common during
periodontal probing and/or procedures such
as prophylaxis and the insertion of a retrac-
tion cord for impression, amongst others),
the JE is able to regenerate quickly (in 48 h)
unlike the other epithelial tissues.17
The following are some critical clinical
aspects regarding the JE:
1. Being a permeable tissue, no restorative
material or debris resulting from clinical
procedures should remain in contact
with the JE due to the risk of inducing
transient or permanent gingival inflam-
mation.
2. The conventional periodontal probing
performed with a Williams or North
Caro lina millimeter probe should be per-
formed with a slight digital pressure,
since the depth of the clinical sulcus dif-
fers from that of the gingival sulcus that
often encompasses a small or medium
portion of the JE. Thus, this clinical mea-
surement should not be used to define
how far the probe can penetrate into the
gingival sulcus under pressure, since this
action will likely invade the JE.
3. The restorative materials currently avail-
able for restorative adhesive dentistry are
biotolerable but not biocompatible. This
means that they should not remain in
contact with the JE because an anti-
gen-antibody reaction may occur.6,7 Ideal-
ly, these materials should be bioactive,
stimulating cellular proliferation and ad-
hesion, which is similar to what happens
in oral and orthopedic implantology18
with materials such as titanium and zirco-
nia as well as polymers such as polyether-
etherketone (PEEK).19 Even implant-sup-
ported restorations, being transmucosal
in nature, have been considered by some
authors to invade the biological space.20
From the approximate level of the cemento-
enamel junction (CEJ), the JE gives way api-
cally to a CT insertion. The CT forms a union
through connective fibers with the root ce-
mentum. This connection is real, since the
tooth end of these fibers is mineralized and
anchors in the cement surface (the Sharpey’s
fibers). From this mineralized origin they di-
rect toward the CT of the gingival margin,
being part of its structure. From a sealing
perspective, an important function of the
CT is to prevent apical migration of the JE,
keeping the level of the gingival margin in
position.15
Rule 2: The excellence of the clinical execution is more determi-nant than the selected restorative material
Several factors should be observed to
achieve periodontal health in the vicinity of
a dental restoration, regardless of its extent
and the material used. The primary factor
relates to the vertical location of the tooth
Page 7
CLINICAL RESEARCH
450 | The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019
preparation limit. In this respect, two ele-
ments should be considered: first, ensuring
an appropriate distance for an adequate re-
storative emergence profile; and second,
aiming whenever possible for a supragin-
gival (SupG) or equigingival (EqG) restorative
limit. However, if a subgingival (SubG) limit is
unavoidable, the preparation limit should re-
main in contact with the SE (an imperme-
able tissue), penetrating a maximum of
0.5 mm on the vestibular surface and
1.0 mm on the interproximal surfaces in re-
lation to the free gingival margin.21
In addition to the vertical level of the
preparation limit (SupG, EqG or SubG), the
overall excellence of the tooth preparation
and the adequate adaptation of the overlay-
ing restoration (temporary or permanent) is
paramount to achieving periodontal health.
An inadequate dental preparation may re-
sult in excessive restoration contouring, an
inadequate emergence profile, an incorrect
occlusal design, and ultimately in functional
and esthetic failure.
It is important to recall that the purpose
of any dental preparation is to provide space
for the restorative material. In rare excep-
tions, a tooth may present a deficient coro-
nal volume and therefore require no prepara-
tion (Fig 4a). However, even in the case of a
tooth with such characteristics, it is import-
ant to plan for the position of the cervical
and interproximal restorative limits of the
future restoration. It is also important to plan
for its emergence profile in such a way that
a predictable adaptation in the restoration is
achieved, avoiding possible periodontal
damage. This cervical and interproximal de-
marcation should be smooth, with an aver-
age depth of 0.2 to 0.4 mm to avoid cervical
dentin exposure (Fig 4b).
According to Richter and Ueno,22 the
definition and excellence of the preparation
limit may be even more important than its
vertical level in relation to the free gingival
margin. Preferably, dental preparations
should not be positioned within the gingival
sulcus,21 ideally being 0.2 to 0.5 mm above
the gingival margin, especially when the
color of the substrate is favorable (Fig 4c).
SupG preparations have various advantages
as they are more accessible during the exe-
cution of several clinical procedures, includ-
ing easier access and visualization during
preparation, facilitated impression or scan-
ning as well as for oral hygiene procedures
and long-term maintenance.21,23
Despite all the previous considerations,
SubG preparations are justified in certain sit-
uations:
1. Substrate discoloration (Fig 5).
2. Replacement of restorations that already
Fig 4 (a) The
purpose of any
dental preparation is
to provide space for
the restorative
material. A tooth may
present a deficient
coronal volume and
therefore not require
preparation. (b) It is
important to position
the cervical and
interproximal
demarcation with an
average depth of 0.2
to 0.4 mm to avoid
cervical dentin
exposure and ensure
an adequate
emergence profile.
(c) Dental prepara-
tions should ideally
be positioned 0.2 to
0.5 mm above the
gingival margin, espe-
cially when the color
of the substrate is
favorable.
a
b
c
Page 8
LOBO ET AL
451The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019 |
Fig 5 (a to g)
Subgingival prepara-
tions are justified in
situations of substrate
discoloration that
require total
coverage of the
tooth by the
restoration. Figure (e)
shows that some-
times it is important
to restore the
discolored substrate
with direct opaque
composite resin prior
to cementation.
a
c
e
b
d
f
g
Page 9
CLINICAL RESEARCH
452 | The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019
present with SubG preparations or res-
torations (Fig 6).
3. For SubG caries.
4. For diastemas that require a suitable
proximal emergence profile to optimize
the position of the interdental papilla
(Fig 7).
In the above cases, there is a justifiable need
to extend the preparation within the sulcus.
However, the position of the JE must be fully
respected, and direct contact of the restora-
tive material should be limited to the SE,
which is keratinized and impermeable. Since
the SE is a tissue with unique characteristics
Fig 6 (a to e)
Subgingival prepara-
tions are also justified
to replace restor-
ations that already
present with
subgingival prepara-
tions or restorations.
a b
c d
e
Page 10
LOBO ET AL
453The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019 |
that are clinically indefinable, parameters
such as probing should not be used in the
decision-making process regarding how
much a particular sulcus can be penetrated
in relation to the free gingival margin. It is im-
portant to consider that in the vast majority
of individuals, the gingival sulcus (or SE) has a
perennial distance, being a transitional epi-
thelium between the OE and the JE.11
From an evidenced-based dentistry (EBD)
standpoint, some of the previously men-
tioned clinical considerations regarding the
relational dental preparation limit and the
periodontal tissues have already gained con-
sensus with the scientific community, these
being:
1. The JE is part of the biological space and
is permeable. Therefore, any restorative
material that contacts its surface will
have an almost direct contact with the
underlying CT and will generate varying
levels of inflammation.24
2. The restorative materials available for
dental restorations are only biotolerable,
not biocompatible or bioactive.25 All re-
storative materials (direct or indirect,
temporary or final) can generate anti-
gen-antibody reactions and should not
come into direct contact with the JE,
with the exception of titanium, zirconia,
and PEEK.6,19
3. The vast majority of patients present with
thin/festooned periodontal biotypes,
which increases the risk of periodontal
harm, gingival margin stability, and a re-
sultant esthetic compromise.5 Depend-
ing on the periodontal biotype, different
clinical and histological responses may
arise from a biological space violation:
periodontal pocket formation, gingival
recession, and/or apical migration of the
dentogingival complex.26
In summary, it is important to define clinic-
al strategies, not only regarding the preser-
vation of hard dental tissues but also in
terms of respecting the periodontal in-
volvement. These clinical strategies should
translate into sufficient invasiveness, ade-
quate instrumentation, EBD clinical proto-
cols, and the employment of premium ma-
terials. Well-adjusted provisional and/or
final restorations directly affect the final re-
storative outcome as well as the health of
the adjacent tissues. An in-depth know-
ledge of the histoanatomy of the periodon-
tal tissues and an awareness of how certain
prosthetic procedures can impact perio-
dontal health are prerequisites for any clin-
ician involved in adhesive restorative den-
tistry.
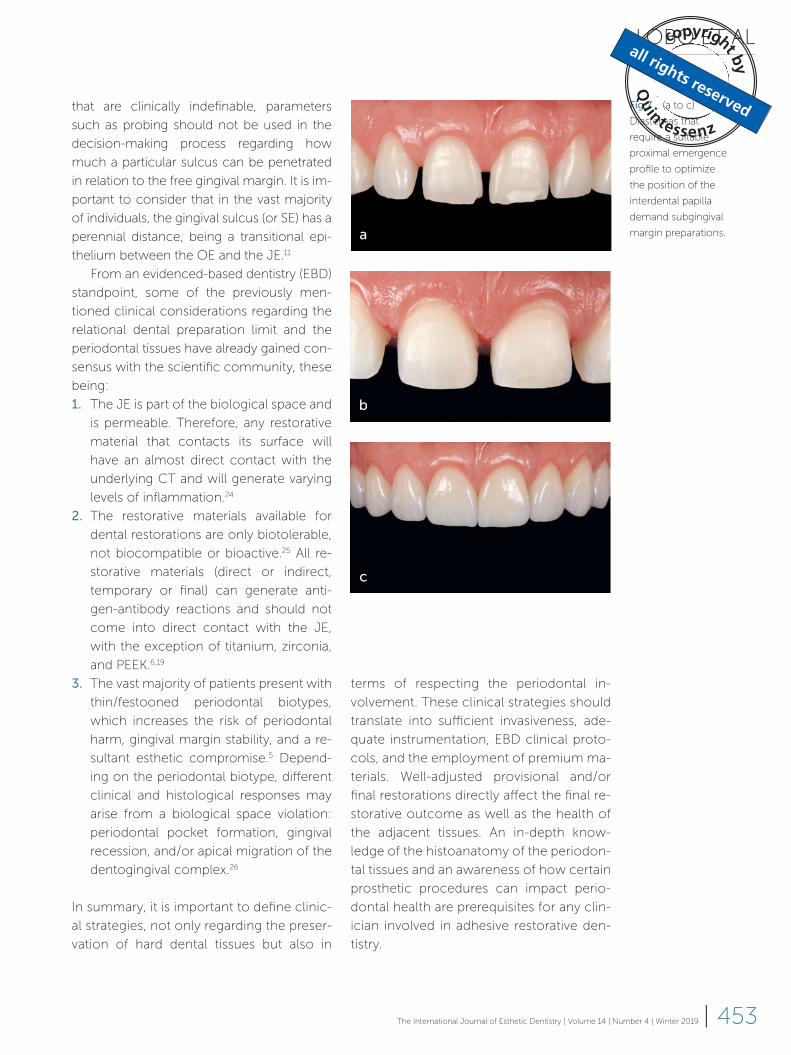
Fig 7 (a to c)
Diastemas that
require a suitable
proximal emergence
profile to optimize
the position of the
interdental papilla
demand subgingival
margin preparations.a
b
c
Page 11
CLINICAL RESEARCH
454 | The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019
Rule 3: The periodontal biotype is fundamental to define the vestibu-lar convexity of the restoration
The periodontal biotype is a factor of para-
mount importance for the esthetic risk as-
sessment in restorative dentistry and its ob-
servance is fundamental to selecting the
adequate treatment sequence and proto-
cols, including preparation, impression pro-
cedures, temporization, and cementation.
The periodontal biotype is directly related to
the convexity of the vestibular surface of
natural teeth, which plays an important role
in directing bolus trajectory during mastica-
tion and promoting proper stimulation and
toning of the gingival margins.27
When the periodontium is thin/fes-
tooned, the teeth usually present a more
pronoun ced vestibular convexity, located
between the middle and cervical thirds of
the crown, which seems to alleviate the di-
rect impact of food on the periodontium.
Clinicians should be careful not to cause
overcontouring in cases of no-prep as this
could lead to periodontal damage (Fig 8).
The flat and thick periodontium is typically
more mechanically resistant and is generally
associated with teeth that have a flatter ves-
tibular surface. This biotype is less sensitive
to dental procedures and may allow for cer-
tain clinical indelicacies without resulting in
permanent periodontal damage.28 On the
other hand, this biotype appears more
prone to developing periodontal pockets in
the presence of inflammation, which may
mask the evolution of irreversible tissue
loss.15
Rule 4: A respectful transition between the periodontium and restoration increases the consis-tency of the clinical results
The tooth-restoration-periodontium inter-
face should be optimized, with the aim of
achieving harmony between tissues that are
very different from an anatomical and bio-
logical standpoint. The position, preparation
limit, emergence profile in combination
with the vestibular contour of the ceramic
restoration, and establishment of an “area of
adhesive continuity” (AAC)29 allow for an ad-
equate perio-restorative integration, facili-
tating plaque control in the cervical region
(Fig 9). The AAC, forming a hybrid interface
of different structures that have been bond-
ed together, results from the correct adap-
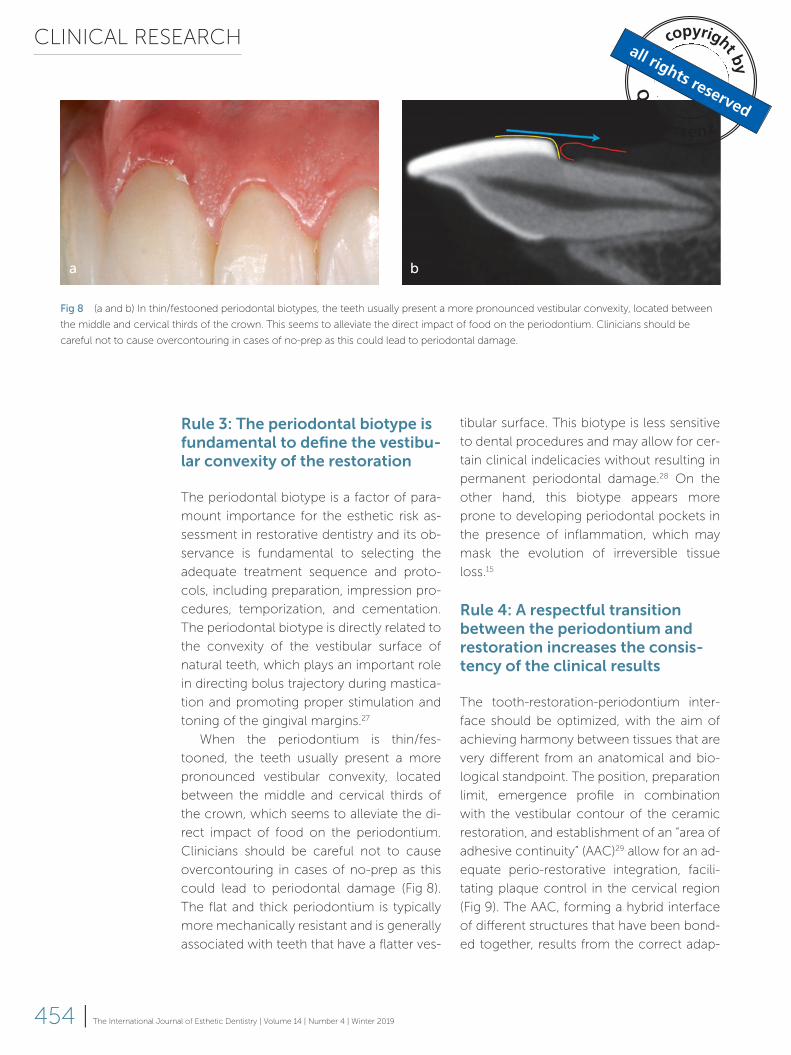
Fig 8 (a and b) In thin/festooned periodontal biotypes, the teeth usually present a more pronounced vestibular convexity, located between
the middle and cervical thirds of the crown. This seems to alleviate the direct impact of food on the periodontium. Clinicians should be
careful not to cause overcontouring in cases of no-prep as this could lead to periodontal damage.
a b
Page 12
LOBO ET AL
455The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019 |
tation between them, so that there are no
discrepancies that promote plaque accu-
mulation.
Not only the clinician but also the dental
technician/ceramist must be knowledge-
able about the biological implications of the
indirect restoration being produced in order
to ensure an adequate finishing and adapta-
tion of the restoration margin as well as an
appropriate emergence profile. The dental
technician must observe the position of the
soft tissues and respect the biological space
in no-prep cases, participating together with
the clinician in the material selection pro-
cess for each particular situation.
Finally, care during the bonding of ce-
ramic dental restorations is fundamental to
attaining a successful perio-restorative in-
terface connection. Attention should be
paid to the choice of the composite resin
cement viscosity and the adhesive protocol,
which must be respected and followed me-
ticulously. The use of gingival retraction
cords should be restricted to cases where
complete hemostasis is not attainable in the
JE, allowing for the passage of crevicular
fluid from the internal to the external envi-
ronment. In these cases, a thinner retraction
cord (No. 000), impregnated with an alumi-
num-based hemostatic solution (to avoid
subsequent spotting) should be selected
and positioned at the level of the JE (ie, it
should not be apparent). Retraction cords
should also be used in cases of SubG prep-
arations, since mechanical separation is re-
quired. The shorter the time the retraction
cord is kept in position, the better for the
health of the periodontium. On the other
hand, there is no need to use gingival re-
traction cords in the case of a SupG prepara-
tion with healthy periodontal tissues.
While absolute isolation (with rubber
dam) is fundamental to control humidity, it
may be deleterious to the gingival margin
during cementation.30 Alternatively, this
control could be achieved with relative iso-
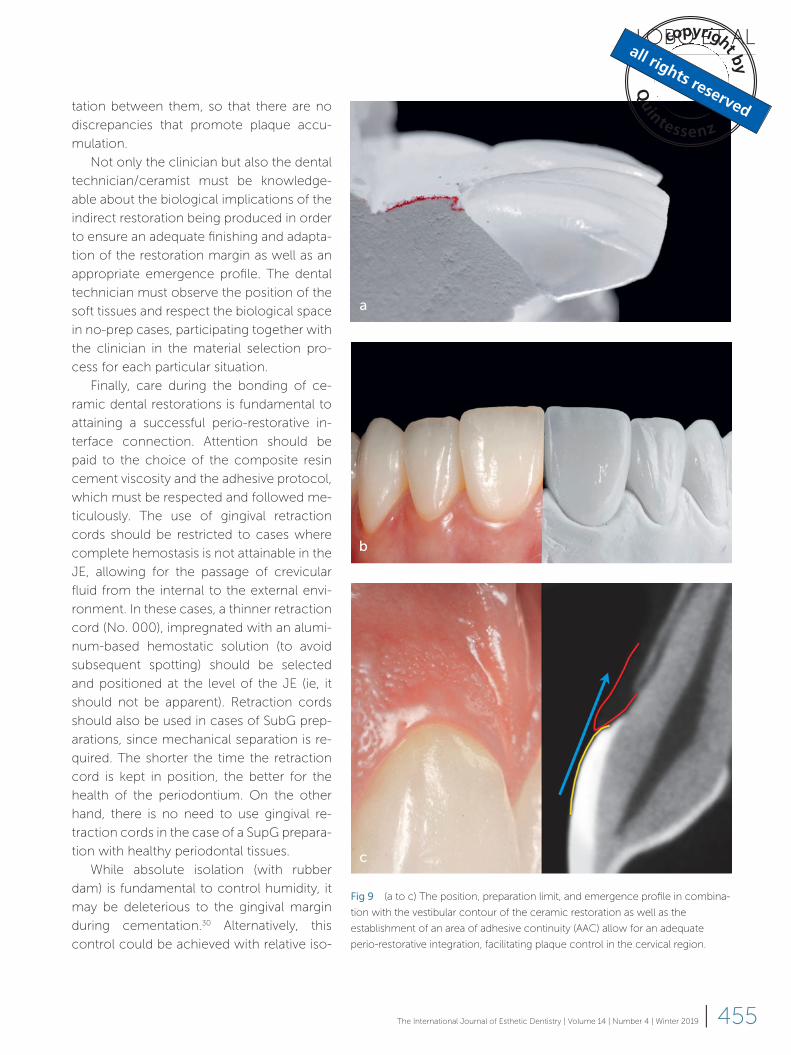
Fig 9 (a to c) The position, preparation limit, and emergence profile in combina-
tion with the vestibular contour of the ceramic restoration as well as the
establishment of an area of adhesive continuity (AAC) allow for an adequate
perio-restorative integration, facilitating plaque control in the cervical region.
a
b
c
Page 13
CLINICAL RESEARCH
456 | The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019
lation through the use of saliva absorbents
and lip retractors or by utilizing modified ab-
solute isolation.
Another important aspect is the sealing
of the restoration and the flow of the ce-
ment. During this procedure, the clinician
should be careful to prevent the formation
of voids that occur when air is trapped be-
tween the restoration and the tooth surface.
Once the restoration is fully seated, the ex-
cessive cement should be carefully re-
moved using appropriate instrumentation,
brushes, and floss, ideally under magnifica-
tion. Light curing only the central area of the
restoration through the use of collimating
tips on the photopolymerization device fa-
cilitates the complete removal of the resin
cement. This helps to ensure that there is
no excess material before the final polymer-
ization of the resin cement at the AAC.
In cases of multiple restorations, the gin-
gival retraction cords (if indicated) should be
removed only after complete photopoly-
merization of all the elements. After this has
been completed, marginal finishing should
take place, for which No. 12 and/or No. 12D
scalpel blades, prophylactic strips, dental
floss, and in some cases rubber cups with
fine polishing pastes may be used.
A follow-up appointment should be
scheduled to assure that the periodontium
in the vicinity of the new restoration pres-
ents a healthy appearance, with no signs of
inflammation, pain, heat, redness, tumor,
and/or exudate.
Final considerations
Many factors can be related to the perio-
dontal success of an adhesive dental reha-
bilitation. Although techniques and mater-
ials will change and evolve over the years
and new tools will emerge, the biology will
not change. The clinician and dental techni-
cian/ceramist are obliged to keep abreast of
the latest developments and constantly ex-
pand their knowledge of the biological be-
havior of the periodontal and dental tissues
in relation to the techniques and materials
used for oral rehabilitation, so that by res-
pecting these tissues the success and long-
evity of the restoration may be fully achieved.
The stability and health of the periodontal
tissues should be a common goal for all
dental care providers with regard to natural
or restored teeth as well as implant-support-
ed restorations or any other type of pros-
thesis.
Page 14
LOBO ET AL
457The International Journal of Esthetic Dentistry | Volume 14 | Number 4 | Winter 2019 |
References
1. Gracis S, Fradeani M, Celletti R, Bracchetti
G. Biological integration of aesthetic res-
torations: factors influencing appearance
and long-term success. Periodontol 2000
2001;27: 29–44.
2. Newcomb GM. The relationship between
the location of subgingival crown margins
and gingival inflammation. J Periodontol
1974;45: 151–154.
3. Schroeder HE, Listgarten MA. The gingival
tissues: the architecture of periodontal pro-
tection. Periodontol 2000 1997;13: 91–120.
4. Cohen LC, Dahlen G, Escobar A, Fejer-
skov O, Johnson NW, Manji F. Dentistry in
crisis: time to change. La Cascada Declara-
tion. Aust Dent J 2017;62: 258–260.
5. Fischer KR, Künzlberger A, Donos N, Fickl
S, Friedmann A. Gingival biotype revisited
– novel classification and assessment tool.
Clin Oral Investig 2018;22: 443–448.
6. Messer RL, Lockwood PE, Wataha JC,
Lewis JB, Norris S, Bouillaguet S. In vitro cy-
totoxicity of traditional versus contemporary
dental ceramics. J Prosthet Dent 2003;90:
452–458.
7. Raffaelli L, Rossi Iommetti P, Piccioni E, et
al. Growth, viability, adhesion potential, and
fibronectin expression in fibroblasts cultured
on zirconia or feldspathic ceramics in vitro.
J Biomed Mater Res A 2008;86: 959–968.
8. Padbury A Jr, Eber R, Wang HL. Interac-
tions between the gingiva and the margin
of restorations. J Clin Periodontol 2003;30:
379–385.
9. Lang NP, Kiel RA, Anderhalden K. Clinical
and microbiological effects of subgingival
restorations with overhanging or clinically
perfect margins. J Clin Periodontol 1983;10:
563–578.
10. Dragoo MR, Williams GB. Periodontal
tissue reactions to restorative procedures.
Int J Periodontics Restorative Dent 1981;1:
8–23.
11. Gargiulo AW, Wentz FM, Orban B. Di-
mension and relations of the dentogingival
junction in humans. J Periodontol 1961;32:
261–267.
12. Stern IB. Current concepts of the
dentogingival junction: the epithelial and
connective tissue attachments to the tooth.
J Periodontol 1981;52: 465–476.
13. Nevins M, Skurow HM. The intracrevic-
ular restorative margin, the biologic width,
and the maintenance of the gingival margin.
Int J Periodontol Restorative Dent 1984;4:
30–49.
14. Lange D, Schroeder HE. Cytochemistry
and ultrastructure of gingival sulcus cells.
Helv Odontol Acta 1971;15(suppl 6): 65–86.
15. Pöllänen MT, Laine MA, Ihalin R, Uitto VJ.
Host-bacteria crosstalk at the dentogingival
junction [epub ahead of print 26 July 2012].
Int J Dent 2012;2012:821383.
16. Nakamura M. Histological and immu-
nological characteristics of the junctional
epithelium. Jpn Dent Sci Rev 2018;54:
59–65.
17. Kinumatsu T, Hashimoto S, Muramatsu
T, et al. Involvement of laminin and integrins
in adhesion and migration of junctional
epithelium cells. J Periodontal Res 2009;44:
13–20.
18. Rompen E, Domken O, Degidi M,
Pontes AE, Piattelli A. The effect of material
characteristics, of surface topography and
of implant components and connections
on soft tissue integration: a literature review.
Clin Oral Implants Res 2006;17(suppl 2):
55–67.
19. Schwitalla A, Müller WD. PEEK dental
implants: a review of the literature. J Oral
Implantol 2013;39: 743–749.
20. Schupbach P, Glauser R. The defense
architecture of the human periimplant mu-
cosa: a histological study. J Prosthet Dent
2007;97(6 suppl): S15–S25.
21. Schätzle M, Land NP, Anerud A, Boysen
H, Bürgin W, Löe H. The influence of
margins of restorations of the periodontal
tissues over 26 years. J Clin Periodontol
2001;28: 57–64.
22. Richter WA, Ueno H. Relationship of
crown margin placement to gingival inflam-
mation. J Prosthet Dent 1973;30: 156–161.
23. Christensen GJ. Marginal fit of gold inlay
castings. J Prosthet Dent 1966;16: 297–305.
24. Ten Cate AR. The role of epithelium in
the development, structure and function
of the tissues of tooth support. Oral Dis
1996;2: 55–62.
25. Werner S, Huck O, Frisch B, et al. The
effect of microstructured surfaces and lami-
nin-derived peptide coatings on soft tissue
interactions with titanium dental implants.
Biomaterials 2009;30: 2291–2301.
26. Maynard JG Jr, Wilson RD. Physiologic
dimensions of the periodontium significant
to the restorative dentist. J Periodontol
1979;50: 170–174.
27. Kao RT, Pasquinelli K. Thick vs. thin gin-
gival tissue: a key determinant in tissue re-
sponse to disease and restorative treatment.
J Calif Dent Assoc 2002;30: 521–526.
28. Block MS. Management of the facial gin-
gival margin. Dent Clin North Am 2011;55:
663–671.
29. Scopin de Andrade OS, Borges GA, Ky-
rillos M, Moreira M, Calicchio L, Correr-So-
brinho L. The Area of Adhesive Continuity:
A New Concept for Bonded Ceramic Res-
torations. Quintessence Dental Technology
2013;36: 9–26.
30. Daudt E, Lopes GC, Vieira LC. Does
operatory field isolation influence the per-
formance of direct adhesive restorations?
J Adhes Dent 2013;15: 27–32.