43
Perioperative Care of Patients with Cardiac Rhythm Management Devices Jonathan Dubsky, M.D. Staff Anesthesiologist Southwest Division OAG September 13, 2012
| Date post: | 01-Jan-2016 |
| Category: |
Documents |
| Upload: | alan-young |
| View: | 221 times |
| Download: | 3 times |

Perioperative Care of Patients with Cardiac Rhythm Management Devices
Jonathan Dubsky, M.D. Staff Anesthesiologist
Southwest Division OAG September 13, 2012

1. To learn a brief history and basic knowledge of Cardiovascular Implantable Electronic Devices
2. To understand preoperative evaluation and preparation necessary for patients with these devices
3. Intraoperative management of these patients and devices including procedure specific considerations and problems that can occur
4. Necessary postoperative evaluation and management
5. To provide example CME/MOCA type exam questions concerning these patients and devices
Objectives:

Pacemakers 101
1st implantable pacemaker placed in Sweden in 1958.It lasted 3 hours before failing and was replaced. (The replacement lasted 2 days.) The patient, Arne Larrson ended up having 26 pacemakers placed and replaced over the course of his lifetime, though he outlived both the inventor and surgeon who performed his first procedure.

1st implantable pacemaker: circa 1958
Arne Larrson (1915-2001) 1st implantable pacemaker recipient
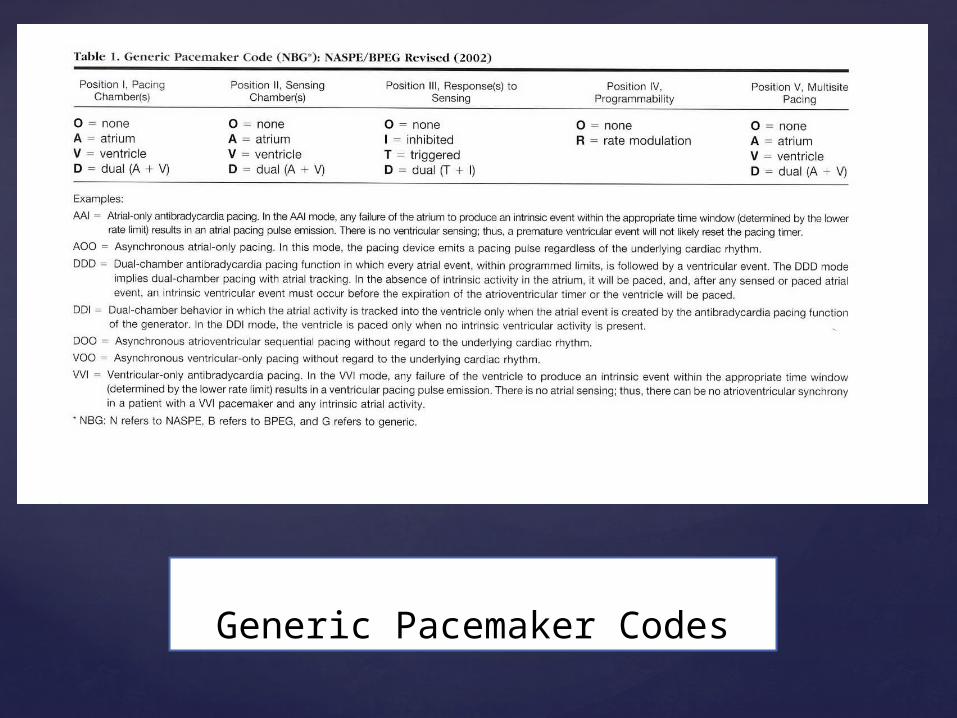
PacemakersGeneric Pacemaker Code
Generic Pacemaker Codes
First implantable defibrillator placed in 1980 at Johns Hopkins
To date, two defibrillators have been placed in dogs with life-threatening arryhthmias
A Brief (Very Brief) History of Implantable Defibrillators

Table 2 Generic Defibrillator Code

Famous people with implantable defibrillators

In 2011, the American Society of Anesthesiologists (ASA) and The Heart Rhythm Society (HRS) came out with an expert consensus on the management of patients with Cardiovascular Implantable Electronic Devices (CIEDs)This was published in Heart Rhythm 2011; 8: 1114-1152The full article and recommendations are available in this journal or on the websites of the ASA or the HRSThis presentation is based on these recommendations

-The writing committee consisted of eight cardiac electrophysiologists, four anesthesiologists(including one from CCF), one CT surgeon, and one allied health professional.-The consensus is based on literature review, input from a reference group, as well as the authors personal experience treating patients.-The literature reviewed consisted of case reports and case series(small numbers). There were no randomized, controlled studies even to be reviewed.- Not everyone had to be in agreement (85% or greater)
How do they come up with an expert consensus and what does this mean?
Back in the olden days……

In the past, it was just generally accepted that placing a magnet over the defibrillator or pacemaker would be a one size fits all solution. Until recently, this was even recommended on one of the web sites of a manufacturer of CIEDs.That’s no longer necessarily the case, so……

EMI (electromagnetic interference) Patients are exposed to many sources of EMI in the perioperative period, and EMI is well documented to cause malfunction of CIEDs. But how this affects management depends on many things including - strength, duration and type of interference - patient’s dependence on, indication for CIED and intrinsic rate and rhythm - built-in protective engineering of current devices
Before we can come up with a plan to manage these patients, we need to understand what type of problems can occur with CIEDs in the perioperative period

So… What is the most common source of EMI and CIED interaction in the operating room?????

Monopolar electrosurgery

Bipolar vs. monopolar electrosurgery
Bipolar – current flows between limbs of forceps - only used for coagulation not dissection - does not cause EMI unless applied directly to the CIED
Monopolar – current flows from pen through patient’s body to return surface electrode. Most common form of EMI and CIED interation in operating room

1. Inhibition of pacing function due to oversensing (most common)2. Inappropriate ICD therapy/shocks (can cause sustained ventricular arrhythmias though likely will do nothing more than cause skeletal muscle contraction with shock if not using muscle paralysis)3. Triggering unnecessary antitachyarrhythmia therapy4. Device reset (infrequent)5. Pulse generator damage(uncommon as long as electrosurgery current kept greater than 6 inches from generator)6. Damage to the lead-myocardial interface(unlikely)
The last two are extremely unlikely unless energy applied directly to the generator or leads
What types of problems can monopolar electrosurgery/EMI cause to CIEDs?
Risks of oversensing and other complications determined by site of electrosurgery application, duration of electrosurgery, and positioning of the return electrode
RECOMMENDATIONSKeep electrosurgery current path as far away as possible from generatorLimit electrosurgery usage to short bursts (4 to 5 seconds) if possibleDuring surgeries close to generator (head, neck, shoulder, carotid etc.) use bipolar electrosurgery if possibleStrategic positioning of return electrode so current path avoids CIED
Risk mitigation

For surgery below the umbilicus in patients with upper chest implanted generators, oversensing problems are unlikely. Surgeries above the umbilicus pose more of a risk
RECOMMENDATIONSFor procedures below the umbilicus, the consensus group feels that it is generally best to make a pacemaker asynchronous only if significant inhibition is observed (even if the patient is pacemaker dependent)
For procedures below the umbilicus, the patient with ICD can have no intervention or application of a magnet depending on comfort level of anesthesia provider. Magnet application suspends arrhythmia detection
If nothing is done, a magnet should still be immediately available. If ICD is deactivated, continuous monitoring for arrhythmia should be performed and cardioversion/defibrillation equipment available
Risk mitigation continued
Cardioversion- problems rarely observed with external cardioversion. Use ant/post positioning of electrodes and >8cm from ant lead to CIED. Occasionally CIED reset observed with internal/direct cardioversion in OHS
RF ablation- can cause same problems as monopolar electrosurgery and may be more problematic due to prolonged exposure of current
Diagnostic radiation- generally does not cause problems
Therapeutic radiation- is type of EMI most likely to cause device reset. Discuss with radiation oncologist shielding possibilities. Calculation can be done to figure amount of radiation that will by absorbed by device. If this exceeds manufacturers recommended amount, CIED may need to be moved to different location.
Special situations

ECT- Hemodynamically significant inhibitionof pacing is unlikely due to stimulus being so brief. Extreme sinus tachycardia that followsseizure may be problematic though.
TURP- place return electrode on thigh or buttock
GI procedures- same precautions as monopolar electrosurgery if electrosurgery to be used
Tissue expanders- use expanders without magnets in patients with CIEDs
TENS and Spinal Cord Stimulators – In general TENS not recommended in pacemaker dependent patients. There are specific recommendations available if felt treatment necessary and these recommendations also apply to SCS
Lithotripsy – risk to CIED is low. Recommend continuous monitoring, terminate procedure is arrhythmias occur, magnet if inhibition occurs, interrogation if complications occur
Special situations continued
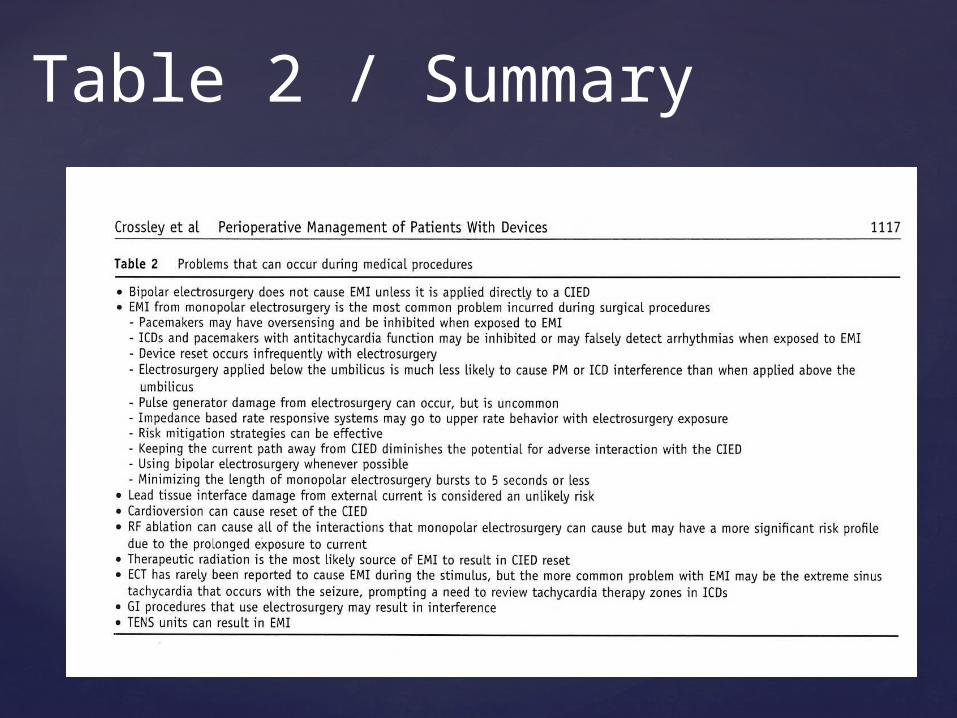
Table 2 / Summary
Many larger institutions have 24 hour access to a member of a CIED team(cardiologist, electrophysiologist, device nurses, staff etc.)
The procedure team should advise the CIED team about the anticipated surgical intervention and the CIED team should make recommendations ( a prescription) for management of the device perioperatively.
***** The consensus group feels that it is inappropriate to have industry employed allied health professionals develop the prescription/plan ******
Preoperative evaluation of a patient with a CIED
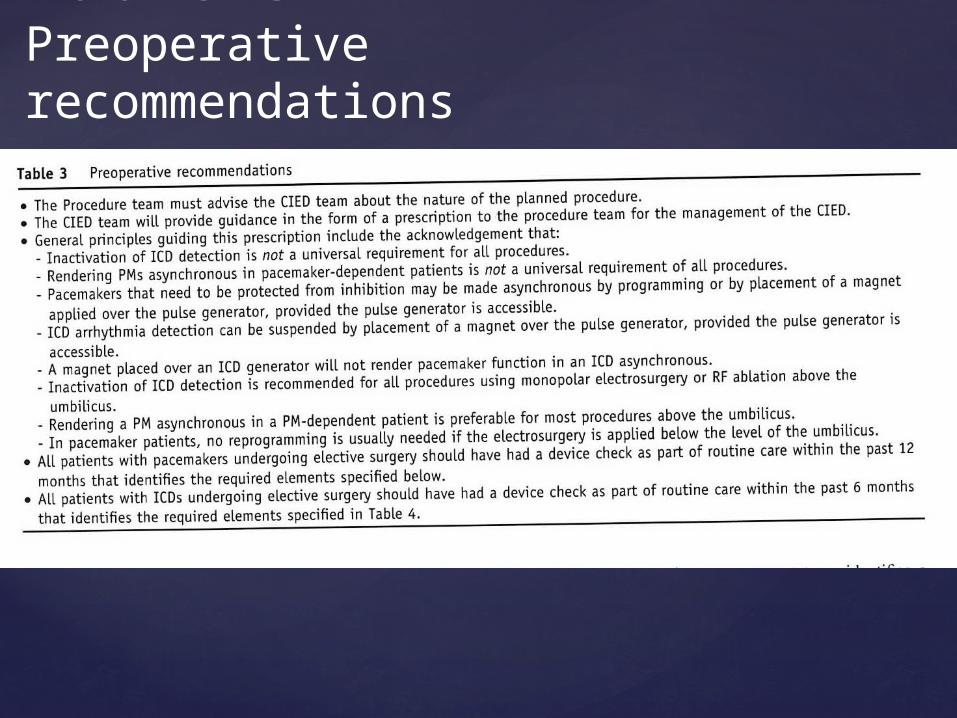
Table 3 Preoperative recommendations

Table 4 Information given to the CEID physician

Table 5
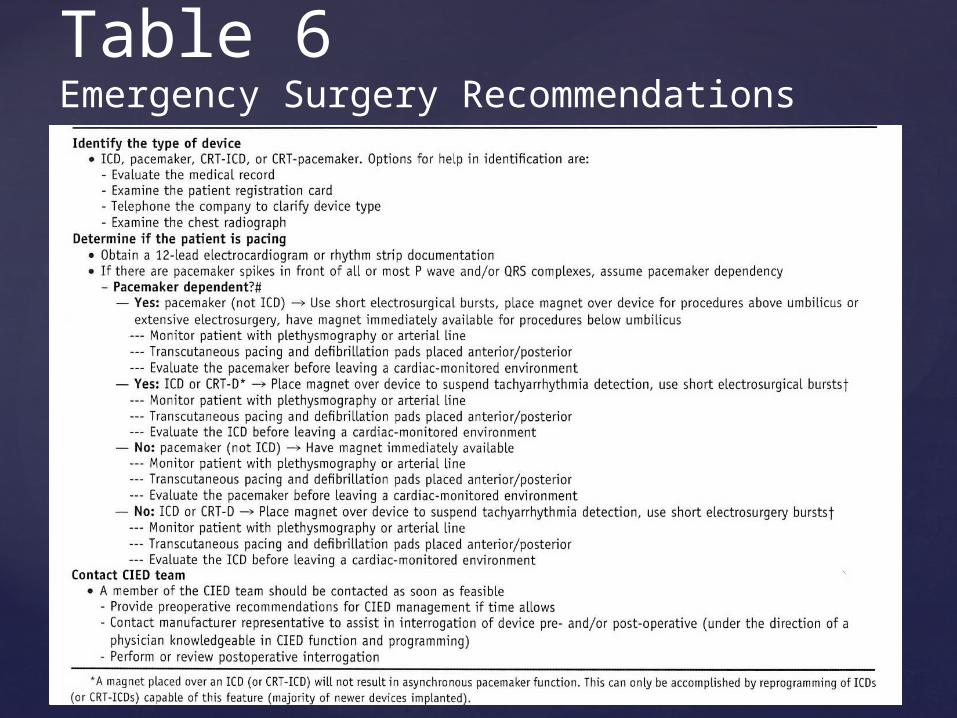
Table 6Emergency Surgery Recommendations

Table 7 Intraoperative Monitoring

Tables 8 and 9 Postoperative evaluation
Notice that even though earlier they said that cardioversion rarely causes problems, that this is one of the three situations that they recommend absolutely be evauated prior to discharge from telemetry.

Table 9 Indication for interrogation of CIEDs prior to patient discharge or transfer from cariac telemetry environment

Which Statement about a DVIR pacemaker is MOST likely true?
A. The atrium and ventricle are sensedB. The paced rate may respond to increases in minute
ventilationC. The paced rate is not influenced by the patient’s
intrinsic HRD. Only the ventricle is paced
Question 1

B
1st letter is chamber paced2nd letter is chamber sensed3rd letter is pacer’s response to the chamber whose rate is sensed(I=inhibited)4th letter is programmability for rate modulation (R) ex. Increasing the paced rate as the paced detects an increase in motion, vibration or minute ventilation
Answer

Which of the following modes of temporary pacing would be MOST appropriate to use in a patient with 3rd degree AV block with a ventricular escape rate of 30 beats/min following mitral valve replacement?
A. AAIB. VOOC. AOOD. DDD
Question 2
D.
Most commonly patients with AV nodal dysfunction are paced with mode DDD following cardiac surgery
Answer

A patient has a pacemaker that detects an atrial stimulus and responds by stimulating the atrium only when the atrial rate is less than the lower rate limit.A) AOOB) DOOC) VVID) AAI
Question 3

AAI
Answer

Your patient has a CIED implanted in left upper chest wall and presents to OR for Left forearm surgery requiring extensive use of monopolar cautery. Where should return electrode be placed?A) Forehead of patientB) Right on top of CIED generatorC) Left armD) Right armE) OR bed
Question 4 (I made this one up)
Extra Credit Question #1Who is this group of young lads?Possibly the anesthesia team for the first implantable pacemaker???

No, it’s Gerry and the Pacemakers!
Also from Liverpool, England1st three singles went to #1 in chartsin early 1960’s .Most popular songs “You’ll never Walk Alone”, and “I Like It”

Extra credit #2What fine Northeast Ohio dining establishment do we see in the photo?
Answer: Pacers14600 Detroit Ave. Lakewood

Crossley GH,Poole JE, Rozner MA, Asrivatham SJ,Cheng A, Chung MK, Ferguson TB, Gallagher JD, Gold MR, Hoyt RH, Irefin S, Kusumoto FM, Moorman LP, Thompson A: The Heart Rhythm Society(HRS)/American Society of Anesthesiologists (ASA) Expert Consensus Statement on the Perioperative Management of Patients with Implantable Defibrillators, Pacemakers and Arrhythmia Monitors: Facilities and Patient Management. Heart Rhythm. 2011;8:1114-1152.
ASA ACE continuing education program (various years 2006-2011)
References:

















