1 Perioperative Pain Management: The Role of IV Acetaminophen Perioperative Pain Management: The Role of IV Acetaminophen Chris Pasero, MS, RN-BC, FAAN September 14, 2012 Chris Pasero, MS, RN-BC, FAAN September 14, 2012 ■ Acute pain is extremely common 1 ■ Perioperative pain Approximately 46 million inpatient procedures and 35 million outpatient surgeries were performed in the US in 2006 2,3 Despite new treatment standards, guidelines, and educational efforts, acute postoperative pain continues to be undertreated 4 , with up to 75% of patients in the US still failing to receive adequate postoperative pain relief 5 2 Acute Perioperative Pain 1. Apfelbaum Anesth Analg. 2003; 97:534-540. 2. DeFrances CJ, et al. Natl Health Stat Report. 2008 Jul 30;(5):1-20. 3. Cullen KA, et al. Natl Health Stat Report. 2009 Jan 28;(11):1-25. 4. Wu CL, et al. Lancet. 2011;377:2215-2225. 5. Phillips DM. JAMA. 2000; 284(4):428-429. 3 Postoperative Pain Management Did Not Improve from 1995 to 2003 1. Warfield CA, et al. Anesthesiology 1995;83:1090-1094. 2. Apfelbaum JL, et al. Anesth Analg. 2003;97:534-540. Overall Pain After Surgery 1,2 % Adult Patients Reporting Pain
Transcript
1
Perioperative Pain Management:The Role of IV Acetaminophen
Perioperative Pain Management:The Role of IV Acetaminophen
Chris Pasero, MS, RN-BC, FAANSeptember 14, 2012
Chris Pasero, MS, RN-BC, FAANSeptember 14, 2012
■ Acute pain is extremely common1
■ Perioperative pain
Approximately 46 million inpatient procedures and 35 million outpatient surgeries were performed in the US in 20062,3
Despite new treatment standards, guidelines, and educational efforts, acute postoperative pain continues to be undertreated4, with up to 75% of patients in the US still failing to receive adequate postoperative pain relief5
2
Acute Perioperative Pain
1. Apfelbaum Anesth Analg. 2003; 97:534-540. 2. DeFrances CJ, et al. Natl Health Stat Report. 2008 Jul 30;(5):1-20. 3. Cullen KA, et al. Natl Health Stat Report. 2009 Jan 28;(11):1-25. 4. Wu CL, et al. Lancet. 2011;377:2215-2225. 5. Phillips DM. JAMA. 2000; 284(4):428-429.
3
Postoperative Pain Management Did Not Improve from 1995 to 2003
1. Warfield CA, et al. Anesthesiology 1995;83:1090-1094. 2. Apfelbaum JL, et al. Anesth Analg. 2003;97:534-540.
Overall Pain After Surgery1,2
% A
du
lt P
ati
en
ts R
ep
ort
ing
Pa
in
2
■ Multimodal: Two or more analgesic agents or techniques that act by different mechanisms, providing superior analgesic efficacy
■ ASA Task Force: Opioid dose-sparing effects (reduced opioid-related adverse events) can be achieved via the use of non-opioid agents and regional blocks
■ ASA Task Force Recommendations: Unless contraindicated, all patients should receive an around-the-
COXIB=cyclooxygenase-2 specific drug; NSAID=nonsteroidal anti-inflammatory drug.
■ Nurses should act as strong advocates for pain management plans that incorporate opioid dose-sparing strategies initiated early in the course of treatment:
On admission
Before surgery
During surgery
Early after surgery
■ Multimodal analgesic therapy that combines opioids with other analgesics has proven efficacy:
Acetaminophen
NSAIDs
Anticonvulsants
5
ASPMN Recommendations for Multimodal Analgesia
Jarzyna D, et al. Pain Manage Nurs 2011;12:118-145.
Trauma
6
Multimodal Approach to Analgesia
1. Gottschalk A, et al. Am Fam Physician. 2001;63:1979-1984 2. Smith HS. Pain Physician. 2009; 12:269-280. 3. Pertusi RM. JAOA 2004;104(11):S19-S24.
Opioids1
2-Agonists1
Acetaminophen2
NMDA antagonists1
Local anesthetics1
Opioids1
2-Agonists1
Local anesthetics3
NSAIDs3
COXIBs3
NMDA=N-methyl-D-aspartate.
Modified from Gottschalk et al., 2001
3
7
The Historical Acute Pain Paradigm
1. Aubrun F, et al. Anesthesiology. 2003;98(6):1415-1421. 2. Oderda GM, et al. J Pain Symptom Manage 2003;25(3):276-283.
+++Opioids
+Opioids
++Opioids
Mild Pain
Moderate Pain
Severe Pain
■ Opioid-related adverse drug events are common in hospitalized patients2
Aubrun et al., 20031
STEP 3STEP 2
andHigher doses of opioids
STEP 1Acetaminophen, NSAIDs, or COXIBs
andLocal/regional anesthesia
STEP 2STEP 1
andLow doses of opioids
8
Multimodal Approach to Acute Pain Management
1. Crews JC. JAMA. 2002;288:629-632. 2. World Health Organization. Pain relief ladder. http://www.who.int/cancer/palliative/painladder/en/. Accessed November 21, 2011. 3. Ventafridda V, et al. Cancer. 1987;59:850-856. 4. ASA Task Force. Anesthesiology. 2004;100:1573-1581.
Mild Pain
Moderate Pain
Severe Pain
Modified from Crews et al., 20021
■ Pain Establishing and maintaining an institutional pain performance
improvement plan is a Joint Commission requirement1
■ Patient satisfaction Local, regional, or national patient satisfaction data are now being
reported via Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS, also known as CAHPS®
hospital survey)2
As part of the Affordable Care Act 2010, the Centers for Medicare and Medicaid (CMS) have established hospital reimbursement based on HCAHPS scores3
9
Pain and Patient Satisfaction May Affect Hospital Reimbursement
1. Wells N, et al. In: Hughes RG, ed. Patient Safety and Quality: an Evidence-Based Handbook for Nurses. AHRQ Publication No. 80-0043. 2. US Department of Health and Human Services, Centers for Medicare and Medicaid. HCAHPS: Patients' Perspectives of Care Survey. http://www.cms.gov/HospitalQualityInits/30_HospitalHCAHPS.asp . Accessed November 21, 2011. 3. American Hospital Association (AHA) Hospital-based purchasing program: the final rule. May 24, 2011. http://www.americangovernance.com/americangovernance/webinar/policy/pdf/final_rule_vbp_regulatatory_advisory.pdf. Accessed October 11, 2011.
4
OFIRMEV® (acetaminophen) Injection Overview
OFIRMEV® (acetaminophen) Injection Overview
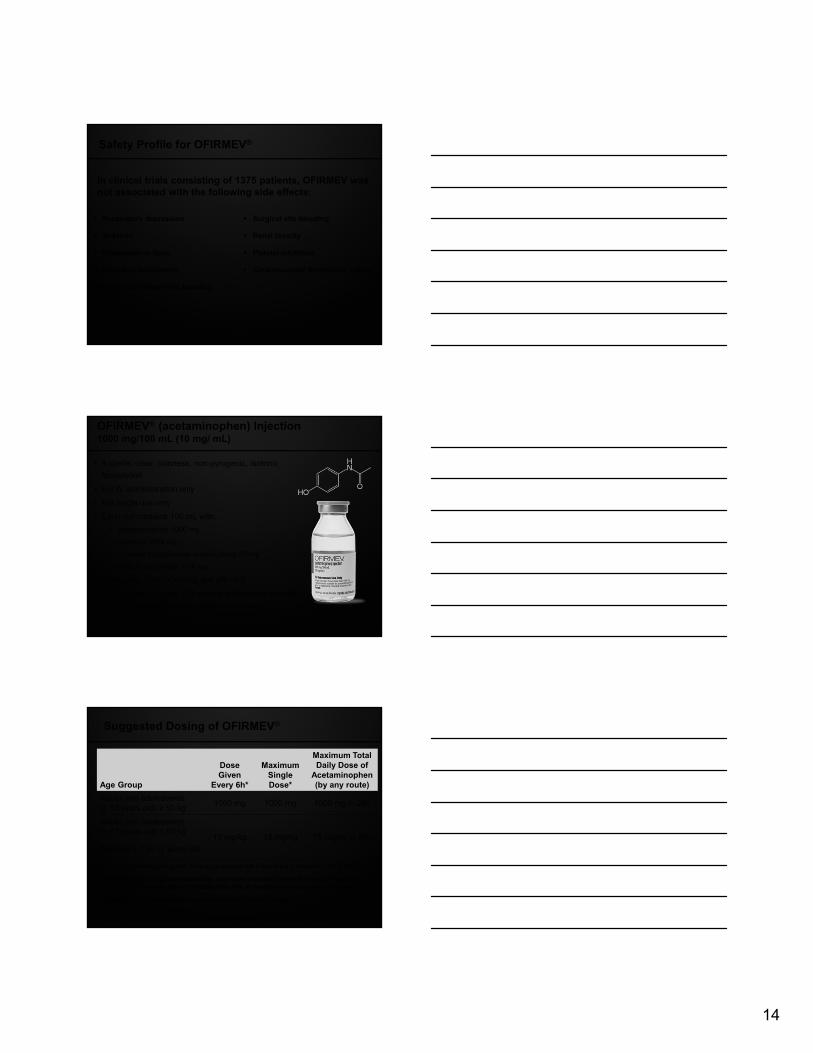
OFIRMEV® (acetaminophen) Injection
■ OFIRMEV (acetaminophen) Injection is indicated for the: management of mild to moderate pain
management of moderate to severe pain with adjunctive opioid analgesics
reduction of fever
■ OFIRMEV is approved for use in adults and children 2 years of age and older
■ Administer only as a 15-minute infusion■ Do not exceed the maximum recommended daily dose of acetaminophen■ Exceeding the maximum daily dose of acetaminophen by any route may result
in hepatic injury, including the risk of severe hepatotoxicity and death■ Contraindicated in patients with severe hepatic impairment, severe active liver
disease or with known hypersensitivity to acetaminophen or excipients in the formulation
■ Use with caution in patients with hepatic impairment or active hepatic disease, alcoholism, chronic malnutrition, severe hypovolemia, or severe renal impairment
■ Discontinue immediately if symptoms associated with allergy or hypersensitivity occur
■ Most common adverse reactions in adult patients: nausea, vomiting, headache, and insomnia
■ Most common adverse reactions in pediatric patients: nausea, vomiting, constipation, pruritus, agitation, and atelectasis
■ Antipyretic effects may mask fever in patients treated for post-surgical pain■ For additional product information, please see full Prescribing Information
Pharmacodynamics of OFIRMEV®
■ Rapid onset of action:
Statistically significant improvement within 15 minutes of administration for both pain and fever1-3
Measurable CSF levels at 15 minutes4
■ Peak effect: within an hour of administration1,2
■ Duration of effect: 4 to 6 hours1-3
■ No significant effect on platelet aggregation5
1. Moller PL, et al. Anesth Analg. 2005;101(1):90-96. 2. Kett DH et al. Clin Pharm Ther 2011; 90:32-9. 3. Sinatra RS et al. Anesthesiol 2005; 102:822-31. 4. Singla N et al. 10th Annual ASRA Pain Medicine Meeting. November 17-20 (New Orleans, LA). 5. OFIRMEV® (acetaminophen) injection [Prescribing Information]. San Diego, CA: Cadence Pharmaceuticals, Inc.; 2010.
14
Study of Acetaminophen Plasma Pharmacokinetics (IV, PO, PR)
(Singla et al., 2011)
The IV route produced a 76% higher mean plasma Cmax (p = 0.0004) than PO, and 256% higher (p < 0.0001) than PR
The median plasma Tmax
for the IV route was earlier (0.25h) than PO (1.0h, p = 0.0018) or PR (2.5h, p = 0.0025)
15
Note: PR acetaminophen data reflects standardization of the 1300 mg dose to 1000 mg (linear kinetics)
Modified from Singla N et al., 2011
IV acetaminophen 1 g
Oral acetaminophen 1 g
Rectal acetaminophen 1 g
Mean Plasma Values
Me
an
(m
cg
/mL
)
Time (hours)
Randomized, 3-way, cross-over design in 6 healthy volunteers; efficacy was not assessed
6
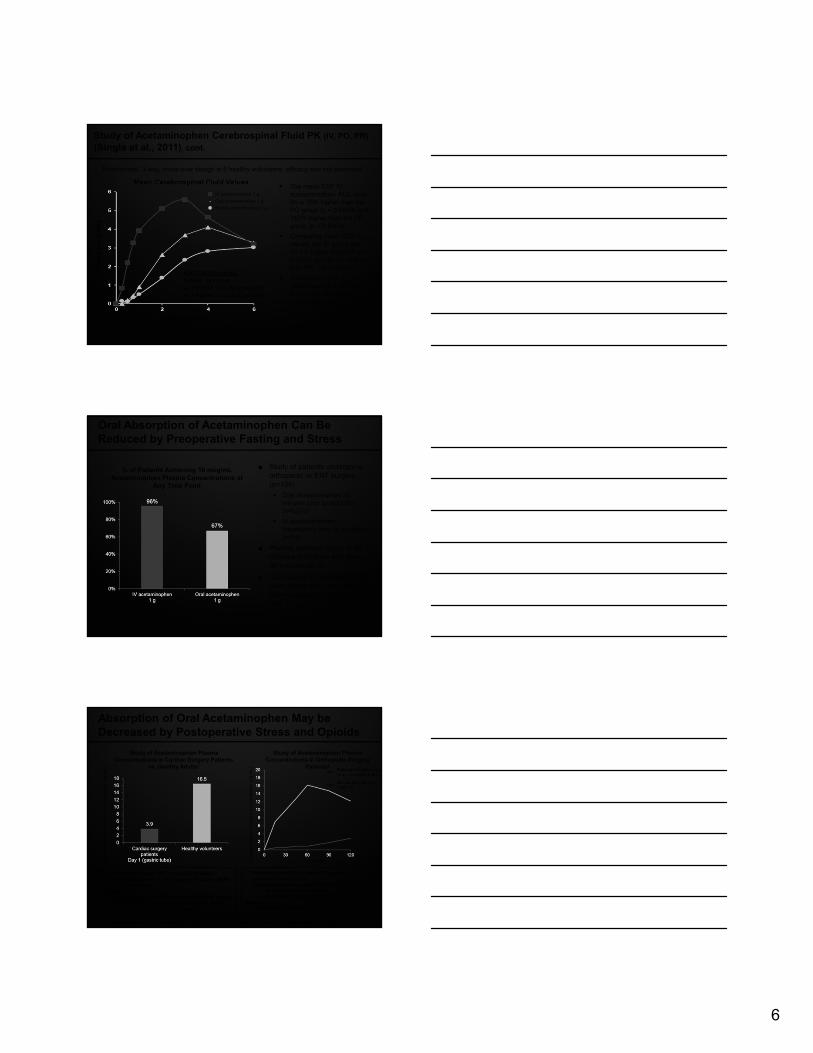
The mean CSF IV acetaminophen AUC over 6h is 75% higher than the PO group (p = 0.0099) and 142% higher than the PR group (p = 0.0004)
Comparing mean CSF Cmax
values, the IV group was 59.7% higher than PO (p < 0.0001) and 86.8% higher than PR (p < 0.0001).
The median CSF Tmax
values were 2.0, 4.0 and 6.0h for IV, PO and PR, respectively
16
Mean Cerebrospinal Fluid Values
AUC0-6 (SD) (µg•h/mL)
IV APAP: 24.9 (17.4)
vs. PO APAP: 14.2 (52.1); p<0.0001
vs. PR APAP: 10.3 (24.5); p<0.0001
*PR acetaminophen data reflects standardization of the 1300 mg dose to 1000 mg (linear kinetics)
Study of Acetaminophen Cerebrospinal Fluid PK (IV, PO, PR)
(Singla et al., 2011), cont.
Me
an
(m
cg
/mL
)
Modified from Singla N et al., 2011
Time (hours)
IV acetaminophen 1 g
Oral acetaminophen 1 g
Rectal acetaminophen 1 g
Randomized, 3-way, cross-over design in 6 healthy volunteers; efficacy was not assessed
17
Oral Absorption of Acetaminophen Can Be Reduced by Preoperative Fasting and Stress
van der Westhuizen J et al. Anaesth Intensive Care. 2011;39(2):242-6.
% of Patients Achieving 10 mcg/mL Acetaminophen Plasma Concentrations at
Any Time Point
■ Study of patients undergoing orthopedic or ENT surgery (n=106)
Oral acetaminophen 30 minutes prior to induction (n=52) or
IV acetaminophen immediately prior to induction (n=54)
■ Plasma samples taken at 30 minutes post-dose and every 30 minutes for 4h
■ Conclusion: IV acetaminophen gave higher and more reliable plasma concentrations than oral
18
Absorption of Oral Acetaminophen May be Decreased by Postoperative Stress and Opioids
1. Berger MM et al. Crit Care Med 2000; 28(7):2217-2223. 2. Petring OU et al. Br J Anaes 1995;74: 257-260.
Minutes
• Patients received IM morphine 10 mg upon first complaint of pain post-op
• Oral acetaminophen solution 20 mg/kg given:• at least 12 hours pre-op, and• 30 minutes after morphine administration
Results• Administration of morphine reduced and delayed oral
acetaminophen absorption
• Patients received IM morphine 10 mg upon first complaint of pain post-op
• Oral acetaminophen solution 20 mg/kg given:• at least 12 hours pre-op, and• 30 minutes after morphine administration
Results• Administration of morphine reduced and delayed oral
acetaminophen absorption
• Oral acetaminophen 1000 mg (liquid formulation) administered on days 1 and 3 post-op through a gastric or post-pyloric tube
Results• Acetaminophen absorption was decreased after gastric
administration on day 1 after cardiac surgery, mainly because of opiate-related gastric stasis
• Oral acetaminophen 1000 mg (liquid formulation) administered on days 1 and 3 post-op through a gastric or post-pyloric tube
Results• Acetaminophen absorption was decreased after gastric
administration on day 1 after cardiac surgery, mainly because of opiate-related gastric stasis
Postoperative (following morphine administration)
Preoperative (at least 12 hours)
Ace
tam
inop
hen
Pla
sma
Con
cent
ratio
n (µ
g/m
L)
Ace
tam
inop
hen
Pla
sma
Con
cent
ratio
n (µ
g/m
L)
Study of Acetaminophen Plasma Concentrations in Cardiac Surgery Patients
vs. Healthy Adults1
Study of Acetaminophen Plasma Concentrations in Orthopedic Surgery
Patients2
7
■ Acetaminophen is primarily metabolized in the liver by first-order kinetics and involves 3 principal separate pathways1
Glucuronidation
Sulfation
Oxidation
■ IV acetaminophen bypasses first-pass liver exposure and metabolism2
19
Metabolism of OFIRMEV®
1. OFIRMEV® (acetaminophen) injection [Prescribing Information]. Cadence Pharmaceuticals, Inc.; San Diego, CA; 2010. 2. National Library of Medicine. Toxicology Tutor II, Influence of Route of Exposure. http://sis.nlm.nih.gov/enviro/toxtutor/Tox2/a32.htm. Accessed February 12, 2010.
Clinical Studies of
OFIRMEV®
(acetaminophen) Injection
Clinical Studies of
OFIRMEV®
(acetaminophen) Injection
■ Randomized, double-blind, placebo-controlled multi-dose study in total hip or knee arthroplasty
■ 7 US centers, N=101 patients (plus 50 patients treated with propacetamol)
■ Started on postoperative day 1 to allow for anesthesia washout (combinations of general, spinal or epidural anesthesia allowed) and to ensure a stable baseline
■ Moderate to severe pain; patients randomly assigned to 1 of 3 treatment groups
1 g OFIRMEV®
2 g propacetamol IV*
Placebo
■ Rescue medication: PCA morphine plus PRN bolus doses available to all patients
■ Endpoints: pain intensity, pain relief, patient satisfaction and morphine use were measured at selected intervals
*Please note: propacetamol is not available for commercial use in the United States.
Sinatra RS, et al. Anesthesiology. 2005;102:822-831.
Study in Major Orthopedic Surgery (Sinatra et al., 2005)
PCA=patient-controlled analgesia; PRN=as needed.
21
8
22
00 11 22 4433 55 66
Mea
n P
ain
Rel
ief
Sco
re
1.01.0
0.60.6
0.80.8
1.21.2
0.40.4
0.20.2
1.61.6
Time (h)
00
1.81.8 IV acetaminophen 1 g q6h + PCA morphine (n=49)
Placebo q6h + PCA morphine (n=52)
IV Acetaminophen Placebo P value
Patient satisfaction: good to excellent at 24 h 40.8% 23.1% 0.004†,2
Median time to first use of rescue 3.0 h 0.8 h 0.0001
Safety (adverse reactions) IV acetaminophen is comparable to placebo
† Based on Cochran-Mantel Haenszel Test‡ The clinical benefit of reduced opioid consumption was not demonstrated
1.41.4** **
****
**** **
** *P<0.05 vs placebo
**P<0.001 vs placebo
1. Sinatra RS, et al. Anesthesiology. 2005;102:822-831. 2. Data on file, Cadence Pharmaceuticals, Inc.
Study in Major Orthopedic Surgery(Sinatra et al., 2005), cont.
23
■ A phase 3, multicenter, randomized, double-blind, placebo-controlled, 24-hour study of the efficacy and safety of IV acetaminophen in abdominal laparoscopic surgery
■ IV or oral rescue medication was available to all patients
■ N=244 subjects; 17 sites in the United States
■ Treatment was initiated morning following surgery
■ Primary Endpoint
Assess the efficacy (pain intensity differences) over the course of 24 hours of repeated doses (q6h) of acetaminophen injection 1000 mg vs. placebo in the treatment of patients with postoperative pain who underwent abdominal laparoscopic surgery
Study in Abdominal Laparoscopic Surgery(Wininger et al., 2010)
Wininger SJ et al. Clin Ther 2010; 32:2348-2369.
24
SPID24=Sum of pain intensity differences, based on VAS score, from baseline at 0 to 24 hVAS=Visual analogue scale
Most common surgical procedures included hysterectomy, cholecystectomy, and hernia repair
Wininger SJ et al. Clin Ther 2010; 32:2348-2369.
Mean Pain Intensity (100-mm VAS)
VA
S (
mm
)
Time (h)
OFIRMEV 1g q6h + rescue (n=92)
Placebo + rescue (n=42)
Mean SPID24 (100-mm VAS)
Study in Abdominal Laparoscopic Surgery(Wininger et al., 2010), cont.
OFIRMEV 1g q6h (n=91)
VA
S (
mm
)
-200
-150
-100
-50
0
P<0.007
-45.2
-194.1
Placebo (n=108)
9
25
Reduced Opioid Consumption
1. Sinatra RS, et al. Anesthesiology. 2005;102(4):822-831. 2. Memis D, et al. J Crit Care. 2010;25(3):458-462. 3. Viscusi E et al. AAPM Annual Meeting. Feb 12-16, 2008 (Orlando, FL). 4. Atef A and Fawaz AA. Eur Arch Otorhinolaryngol. 2008;265(3):351-355.
Note: Opioid consumption reduction is highly dependent on clinical trial design, and the clinical consequence of any amount of opioid consumption reduction may not have been evaluated or demonstrated in a given trial.
Total Hip & Knee Replacement1
Total Hip & Knee Replacement1
Adult Tonsillectomy4
Adult Tonsillectomy4
Major Abdominal Surgery2
Major Abdominal Surgery2
Total Hip Replacement3 *
Total Hip Replacement3 *
(Morphine over 24 h, mg)
P<0.01
33%
(Meperidine doses)
P<0.001
78%
(Meperidine, mg)
P<0.05
61%
(Morphine equivalents 0-6 h, mg)
P=0.016
53%
OFIRMEV 1g
Placebo
*This study was terminated early due to the detection of particulates in some placebo vials
Improved Patient Satisfaction
26
1. Wininger S, et al. Clin Ther 2010.;32:2348-2369. 2. Sinatra RS, et al. Anesthesiology 2005;102:822-831. 3. Gimbel et al. AAPM Annual Meeting. Feb 12-16, 2008 (Orlando, FL).
Total Hip Replacement3 *Total Hip Replacement3 *Total Hip & Knee Replacement2
Total Hip & Knee Replacement2
Abdominal Laparoscopy1Abdominal Laparoscopy1
Placebo
OFIRMEV
Patient Satisfaction at 24 h
P=0.0004
Satisfaction with Treatment at 24 h
P=0.004 P=0.0018
Overall Satisfaction at 24 h
% of Patients Reporting “Good” or “Excellent” Satisfaction% of Patients Reporting “Good” or “Excellent” Satisfaction
86.9%
70.2%
23.1%
40.8%39.3%
85.7%
All patients had access to IV opioid rescue medication as needed
Patient satisfaction was a pre-specified secondary endpoint where subjects were asked to evaluate the study treatments overall using a 4-point categorical scale.
*This study was terminated early due to the detection of particulates in some placebo vials
27
Laparoscopic Hysterectomy Case Study Patient Y: Case Description
■ History & Physical
42yo G4P2A2 female with a 2 year history of worsening menorrhagia and dysmenorrhea
Patient requests definitive surgical correction and cervical preservation
On the pelvic examination, a 14-week-sized uterus was palpated
Pelvic ultrasound revealed an enlarged uterus with multiple fibroids
■ Diagnosis
Symptomatic uterine fibroids
■ Recommended Procedure Type
Laparoscopic supracervical hysterectomy
Case Contributed by: Dr. Craig Saffer, Obstetrician and Gynecologist at West Coast OB/GYN, San Diego, CA
This case study is intended only to provide healthcare professionals with an example of the use of OFIRMEV® (acetaminophen) injection in the treatment of one specific patient. The outcomes described may not be representative of, and may differ significantly from, outcomes that may be obtained in treating other patients. This case study is not intended to provide specific treatment advice, recommendations or opinions, and should not replace a clinician’s judgment with respect to the treatment of any particular patient.
10
28
Laparoscopic Hysterectomy Case Study Patient Y: Perioperative Analgesic Protocol
Do not exceed the maximum total daily dose of acetaminophen of 4 g
†PostOp Day 1 defined as 0–24h after surgery
29
■ Pain Assessment*
PACU: 4-5/10 pain
POD 0: 3/10 pain later that day at rest
POD 1: 5/10 pain with first ambulation in the morning
POD 1: 2-3/10 pain at time of discharge
■ Opioid Consumption
POD 1: Total of 30 mg of PO oxycodone consumed (5-10 mg q3h prn)
POD 1: IV Morphine available prn for breakthrough pain but not utilized
■ Patient Satisfaction
“Excellent” rating for pain control on a 4-point categorical scale
* Based on 10-point numeric rating scale (NRS)
Laparoscopic Hysterectomy Case Study Patient Y: Outcomes
Note: Opioid consumption reduction is highly dependent on clinical trial design, and the clinical consequence of any amount of opioid consumption reduction may not have been evaluated or demonstrated in a given trial.
30
■ Ambulation
Foley catheter removed 6 hours after surgery
Patient up and around room/bathroom the evening of the procedure
Patient walking in hallways the morning of POD 1
■ Discharge
Patient discharged 24 hours after the procedure
Laparoscopic Hysterectomy Case Study Patient Y: Observations
Please see full Prescribing information for complete safety information
11
31
Laparoscopic Colectomy Case Study Patient X: Case Description
■ History & Physical
35 yr old male with 3 month history of crampy abdominal pain, bleeding per rectum and10 lbs unintentional weight loss
Previous open appendectomy and repair of a congenitally rotated kidney
No FH of colorectal cancer or IBD
No abnormalities on physical exam
Case Contributed by: Dr. Christopher Mantyh, Director, Colorectal Surgery, Critical Care, Duke University, Durham, NC
This case study is intended only to provide healthcare professionals with an example of the use of OFIRMEV®
(acetaminophen) injection in the treatment of one specific patient. The outcomes described may not be representative of, and may differ significantly from, outcomes that may be obtained in treating other patients. This case study is not intended to provide specific treatment advice, recommendations or opinions, and should not replace a clinician’s judgment with respect to the treatment of any particular patient.
32
Laparoscopic Colectomy Case Study Patient X: Case Description
■ Tests
Colonoscopy: biopsy confirmed sigmoid adenocarcinoma, remainder of colon normal
CT: thickened sigmoid colon, no visible metastasis
Laparoscopic Colectomy Case Study Patient X: Perioperative Analgesic Protocol
Do not exceed the maximum total daily dose of acetaminophen of 4 g
†PostOp Day 1 defined as 0–24h after surgery‡Lidocaine 5% patch is indicated for post-herpetic neuralgia only
12
34
■ Pain Assessment*
Initial PACU Score: 6/10 pain
Discharge PACU Score: 3/10 pain
POD 1 Score: 4/10 pain (3 mL bolus of epidural given)
POD 2 Score: 0/10 pain
POD 3 Score: 1/10 pain
■ Opioid Consumption
POD 1: epidural + 3 mL bolus for breakthrough pain
POD 2: epidural
POD 3: 20 mg PO oxycodone (5 mg q4h prn)
■ Patient Satisfaction
POD 1-3: “Good-excellent” rating for pain control on a 4-point categorical scale
* Based on 10-point numeric rating scale (NRS)
Laparoscopic Colectomy Case Study Patient X: Outcomes
Note: Opioid consumption reduction is highly dependent on clinical trial design, and the clinical consequence of any amount of opioid consumption reduction may not have been evaluated or demonstrated in a given trial.
35
■ Ambulation/Diet
POD 1: ambulating, clear liquids for breakfast, regular diet for dinner
POD 2: + flatus/BM, tolerating regular diet, foley catheter removed when epidural out
■ Discharge
PACU Discharge Time: 2 hours and 3 minutes
Hospital Length of Stay: 3 days
Discharge medications:
• Acetaminophen 975 mg PO q6h prn
• Oxycodone 5-10 mg q3h prn
• Enoxaparin 40 mg subcutaneously daily for a week
■ Follow-up
Pathology: T3N1M0 tumor, 6.2x5.4x1.2 cm, 3/28 LN +, will receive 6 months of adjuvant chemotherapy
Surgical clinic visit 4 weeks post D/C: all wounds well healed, tolerating regular diet, 2 BM/day, no further bleeding or abdominal pain, Hct normalizing
Laparoscopic Colectomy Case Study Patient X: Observations
Please see full Prescribing information for complete safety information
Safety and Tolerability of
OFIRMEV®
(acetaminophen) Injection
Safety and Tolerability of
OFIRMEV®
(acetaminophen) Injection
13
■ A total of 1020 adult patients have received OFIRMEV in clinical trials supporting approval, including 37.3% (n=380) who received 5 or more doses, and 17.0% (n=173) who received more than 10 doses
86.9% (n=886) patients received a dose of 1000 mg q6h
Peak ALT/AST value postbaseline: % of patients in all repeated-dose, placebo-controlled, all-adult studies*1
38
Hepatic Safety Data for OFIRMEV®
1. Data on file. Cadence Pharmaceuticals, Inc. 2. OFIRMEV® (acetaminophen) injection [Prescribing Information]. Cadence Pharmaceuticals, Inc.; San Diego, CA; 2010.
ALT=alanine aminotransferase; AST=aspartate aminotransferase.*Data from a pooled analysis of 5 repeated-dose placebo-controlled clinical studies involving adult patients.
Acetaminophen is contraindicated in patients with severe hepatic impairment or severe active liver disease and should be used with caution in patients with hepatic impairment or active liver disease2
Treatment-Emergent Adverse Event (TEAE)
OFIRMEV(N=402)
n (%)
Placebo(N=379)
n (%)
Nausea 138 (34%) 119 (31%)
Vomiting 62 (15%) 42 (11%)
Pyrexia† 22 (5%) 52 (14%)
Headache 39 (10%) 33 (9%)
Insomnia 30 (7%) 21 (5%)
† Pyrexia adverse reaction frequency data is included in order to alert healthcare practitioners that the antipyretic effects of OFIRMEV may mask fever.
The differences between treatment groups were not statistically significant for any reported TEAE.
39
Treatment-Emergent Adverse Events Occurring ≥ 3% in Adults Receiving OFIRMEV® and at a Greater Frequency Than Placebo in Repeated-Dose Studies
For instructions regarding q4h dosing, please see full Prescribing Information for OFIRMEV
Administration of acetaminophen by any route in doses higher than recommended may result in hepatic injury, including the risk of severe hepatotoxicity and death
OFIRMEV is not approved for use in patients < 2 years of age
42
15
Administration of OFIRMEV®
OFIRMEV should be administered only as a 15-minute IV infusion
Minimum dosing interval is 4 hours, not to exceed 4 g in 24 hours
An infusion pump is not required except when delivering weight-based calculated doses less than 600 mg (60 mL). Use a syringe pump for administering small volume doses, particularly in young children
No dosage adjustment is required when transitioning to oral acetaminophen
The following clinical scenarios are examples of OFIRMEV dosing intervals but are not intended to replace the dosing instructions included in the product labeling.
OFIRMEV dosing schedule by surgery duration
Point of care PreOp IntraOp PostOpPACU
PostOpSurgical Floor or Step Down Unit
Time of administration
0.5–1 h(presurgery) ≤1 h 2–4 h ≥5 h 90 min ≥90 min
Inpatient:Long procedure
✓ ✓ ✓q6h as indicatedTransition to oral medicationwhen clinically warranted
Inpatient:Short procedure
✓ ✓q6h as indicatedTransition to oral medicationwhen clinically warranted
Inpatient:Trauma ✓ ✓ ✓q6h as indicated
Transition to oral medicationwhen clinically warranted
Outpatient:Day surgery ✓
Indicates approximate duration of surgery
Administration of acetaminophen by any route in doses higher than recommended may result in hepatic injury, including the risk of severe hepatotoxicity and death. 44
45
Summary of OFIRMEV® Data
1. Sinatra RS, et al. Anesthesiology. 2005;102:822-831. 2. Wininger SJ et al. Clin Ther 2010; 32:2348-69. 3. Memis D, et al. J Crit Care. 2010;25:458-462. 4. Atef A, et al. Eur Arch Otorhinolaryngol. 2008;265:351-355. 5. OFIRMEV® (acetaminophen) Injection [Prescribing Information]. Cadence Pharmaceuticals, Inc.; San Diego, CA; 2010.
■ Significant pain relief1,3
■ Reduced opioid consumption1-4
■ Improved patient satisfaction1,2
■ Established safety profile and well tolerated in clinical trials1-5
■ Utilization considerations Early initiation (pre-operative; intra-operative)
Schedule q6h or for as long as clinically warranted
Acetaminophen should be used with caution in patients with the following conditions: hepatic impairment or active hepatic disease, alcoholism, chronic malnutrition, severe hypovolemia, or severe renal impairment5
■ Administer only as a 15-minute infusion■ Do not exceed the maximum recommended daily dose of acetaminophen■ Exceeding the maximum daily dose of acetaminophen by any route may result
in hepatic injury, including the risk of severe hepatotoxicity and death■ Contraindicated in patients with severe hepatic impairment, severe active liver
disease or with known hypersensitivity to acetaminophen or excipients in the formulation
■ Use with caution in patients with hepatic impairment or active hepatic disease, alcoholism, chronic malnutrition, severe hypovolemia, or severe renal impairment
■ Discontinue immediately if symptoms associated with allergy or hypersensitivity occur
■ Most common adverse reactions in adult patients: nausea, vomiting, headache, and insomnia
■ Most common adverse reactions in pediatric patients: nausea, vomiting, constipation, pruritus, agitation, and atelectasis
■ Antipyretic effects may mask fever in patients treated for post-surgical pain■ For additional product information, please see full Prescribing Information