42
Peripheral IVs
| Date post: | 25-Dec-2015 |
| Category: |
Documents |
| Upload: | jodie-caldwell |
| View: | 214 times |
| Download: | 1 times |

Peripheral IVs

Pediatric Challenges
• Smaller Veins• Active• Challenging• Need an assistant• All ages
–Scared of shots

VASCULAR ACCESS DEVICE (VAD) SELECTION ALGORITHM
Expected duration >1 month?
NO YES
Determine length of therapy and need for vascular access
7-30 days
Determine length of therapy
> 1 year
Choose PICC, Tunneled CVC or Port (See Notes)
Choose Tunneled CVC or Port (See
Notes)
1. Consider the need for single vs. multi-lumen CVC, and select the least number of lumens to deliver the required therapy.
2. Consider patient’s current and future setting; (i.e. Home Care?)
3. Select device that is least invasive, with lowest risk of complications, which will last the duration of therapy.
4. Device selection should consider input from the patient/family, safety, patient activity, comfort, body image and medical history.
5. Consider anticipated changes in patient’s medical status?
6. Is vascular access for nutrition only? If so, have enteral feeds been considered?
OTHER DECISIONS TO BE MADE WHEN SELECTING VAD:
* Infusate appropriate for peripheral IV:• < 500 mOsm/L• pH 5-9• Non irritant, non vesicant or vesicant
Using assessment tool is there adequate
vascular integrity?
Choose PICC or Non-tunneled
CVC
Choose Peripheral
IV and reassess
daily*
NOYES
NOYES
0-5 days
Is Infusate appropriate for peripheral IV *
1 month-1 year
Choose PICC
*REMINDER: Discuss IV access on a daily basis during Family Centered Care Rounds.

Prepare Patient
• Infant– Ask parent or someone familiar to assist
during procedure if possible– During the procedure, provide patient
with pacifier – Use soothing voice– Provide music

Prepare Patient• Toddler
– Explain procedure in simple terms– Use medical play– Hold their hand– Allow to have their security item (toy,
blanket)– Limit explanation to 10 minutes and
prepare just before the procedure

Prepare Patient
• Preschooler– Prepare just before– Show procedure on a doll first to lessen
anxiety– Inform patient that it’s okay to cry, just
don’t move– Count 1,2, 3…

Prepare Patient• School age
– Make sure they understand which part of the body will be involved
– Provide detailed explanation– Use a doll to show procedure or other
medical play interventions– Allow to participate in small tasks during
the procedure– Limit explanations to 20 minutes and
prepare ahead of time

Prepare Patient• Adolescent
– Provide detailed explanation– Use visuals during explanation and
correct terminology– Allow time for discussion– If possible, allow them to choose
when to begin the procedure– Allow them to help during the
procedure

Preparing the PatientAdditional Tips• Always have a helper
to hold • Use family to help
support/distract child• May need to mummy
wrap active toddlers• Tell child to be brave,
but that it’s OK to cry

Afterwards…• Rewards
– Have stickers available after IV insertion. Kids love stickers!!
– Cuddle infants after IV insertion
– Have parents/siblings tell child how brave they were

IV Sites• Infants
– Hands– Feet– Scalp
• Toddlers – Hands– Feet– Scalp only if <18
months
• School Age – Hands– Feet
• Adolescents– Hands– Arms – Avoid feet

IV SitesDigital Dorsal veins
Dorsal Metacarpal veins
Dorsal venous network
Cephalic veinBasilic vein

IV Sites
Cephalic vein Median Cubital vein
Accessory Cephalic vein Basilic vein
Cephalic vein Median antebrachial vein

IV Sites-Feet

IV Sites-Scalp

IV Sites
• Tips– Use a tourniquet– Warm extremity– Tap/flick– Palpate with the same
finger– Look at all extremities

Areas to Avoid• Red sclerotic veins• Blown veins• Areas of swelling or
tenderness• Arteries• Infected lesions• Fistulas• AV shunts• Paralyzed extremities

IV Complications
• Infiltration– Swelling– Pain– Cool to touch– Compare both
extremities– IV pump will
continue to run

Grade Clinical Criteria <4kg
Clinical Criteria >4kg
0 No symptoms No symptoms
1 Skin blanched Edema <1CM in any directionCool to touchWith or without pain
Skin blanched Edema <2.5 CM in any directionCool to touchWith or without pain
2 Skin blanched Edema 1-4 CM in any directionCool to touchWith or without pain
Skin blanched Edema 2.5-15 CM in any directionCool to touchWith or without pain
3 Skin blanched, translucentGross edema >4 CM in any direction Cool to touchMild –moderate pain
Skin blanched, translucentGross edema >15 CM in any direction Cool to touchMild –moderate painPossible numbness
4 Skin blanched, translucentSkin tight, leaking or with blistering Skin discolored bruised, swollenGross edema >4 CM in any directionDeep pitting tissue edemaCirculatory impairment Moderate to severe painInfiltration of any blood product, irritant, or vesicant.
Skin blanched, translucentSkin tight, leaking or with blistering Skin discolored bruised, swollenGross edema >15 CM in any directionDeep pitting tissue edemaCirculatory impairment Moderate to severe painInfiltration of any blood product, irritant, or vesicant.

Interventions for Infiltration
Do not immediately remove IVStop infusionElevate effected extremityDetermine infusateIf infusate is a vesicant, refer to Nursing Policy III-306 Monitoring and Management of Infiltration/ExtravastionIf infusate is not a vesicant, remove IVNotify physicianRestart new IV if continued therapy is necessaryContinue assessment of site and surrounding tissue, PRN

Check it HOURLY!
• “The RN is responsible for observing the IV site for signs of infiltration at least hourly and notifying the physician for orders for all IV infiltrates or other delays related to IV therapy.”– II-101 Safe Administration of Parenteral Therapy, Including
Drugs Given Via the Intrathecal Route –Pharmacy and Therapuetics Policy

IV Complications
• Phlebitis– Pain– Red,tender– Heat, inflamed– Streaks along vein– Chances increase
drastically after 3 days

Grade Clinical Criteria0 No symptoms
1 Erythema at access site with or without pain
2 Pain at access site with erythema and/or edema
3 Pain at access site with erythema and/or edemaStreak formationPalpable venous cord
4 Pain at access site with erythema and/or edema Streak formation Palpable venous cord >2.5 CM in lengthPurulent drainage

IV Complications
• Extravasations– Due to
administration of vesicant substance
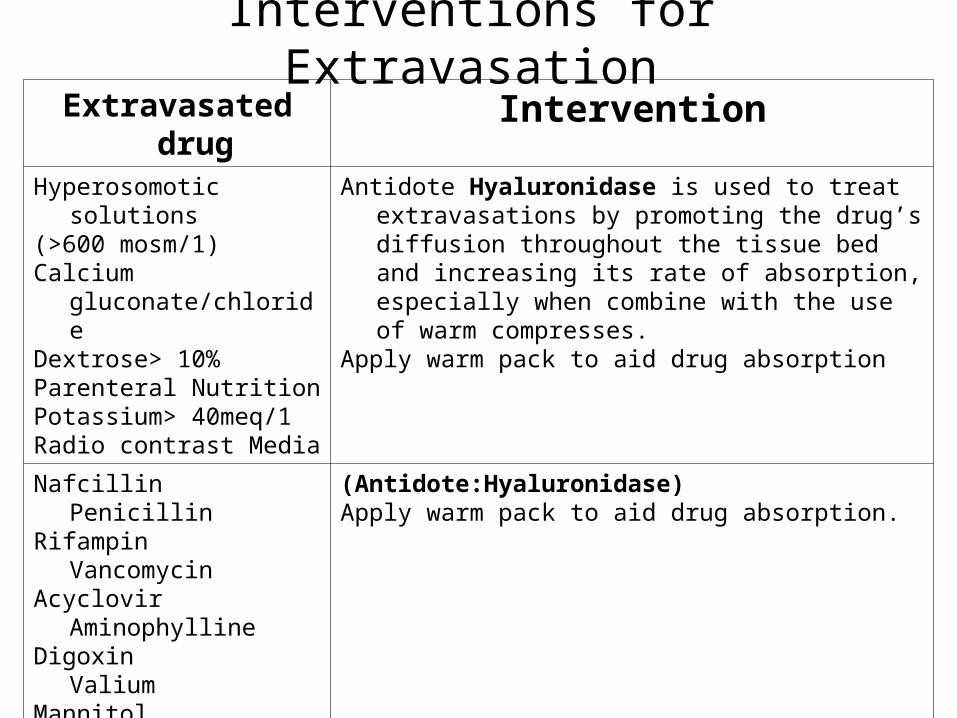
Interventions for ExtravasationExtravasated drug Intervention
Hyperosomotic solutions(>600 mosm/1)Calcium gluconate/chlorideDextrose> 10%Parenteral NutritionPotassium> 40meq/1Radio contrast Media
Antidote Hyaluronidase is used to treat extravasations by promoting the drug’s diffusion throughout the tissue bed and increasing its rate of absorption, especially when combine with the use of warm compresses.
Apply warm pack to aid drug absorption
Nafcillin PenicillinRifampin VancomycinAcyclovir
AminophyllineDigoxin ValiumMannitol
(Antidote:Hyaluronidase)Apply warm pack to aid drug absorption.
SympathomimeticsDopamineEpinephrineNorepinephrinePhenylephrineVasopressin
Antidote: Phentolamine – May cause excessive vasodilation.
If Necrosis present Contact Attending physician

IV Complications
• Infection– Very important to
use aseptic technique and using equipment right after removal from packaging

Other things…
• A. Drawing blood from existing venous access may risk losing the IV access.
• B. Blood cultures can not be sent from any established peripheral line
– III-203 Saline Well Guidelines/Blood Draw from an Established Venous Access

It is the CCHMC Policy…
• “If the procedure on a patient is not successful after three (3) attempts, assistance and advice from a more experienced, qualified professional should be requested.”

IV Supplies• Equipment
1. Select appropriate size steel needle or plastic cannula based on patient's size. 2. Assemble equipment using aseptic technique. - Steel needle or plastic cannula - Normal saline flush - Extension tubing - Gauze pads - Padded armboard - Tape - Protective cup for IV site - Tourniquet - Transparent dressing for cannula use - Gloves - Chlorhexadine swabstick (iodine for CHG sensitivity)

What Size should I use?Sizes• 24g
– Used for infants– Used for small short
veins• 22g
– Used for toddlers and school age
– Good for obtaining blood

Sizes continued…
• 20 g– Used for adolescents
• 18 g– Used for large veins, large volumes, or
trauma patients– Often placed in the O.R.

IV Catheters
Types• AngioCaths
– Must utilize safety needles
• Abbocath– May still see these around
• Do not have safety needle features

IV Insertion• Procedure
– Prepare patient (consider patient’s developmental age when preparing for the procedure)
– Prepare IV supplies– Select catheter size– Insert IV into patient– Monitor IV per policy

IV Insertion• Insertion directions
– Prepare site, alcohol area for 20 seconds
– Quick stick through skin
– Direct method– Watch for blood return– Advance– Disconnect stylet– Flashback, then
advance

IV Insertion
• Use a 1” piece to secure t-connector• Keep site visible• Restrain board (not arm)• Use IV board (only if needed)
– Right size• Small• Medium• Large• Padded

IV Insertion• Use minimal amount of tape• Use Securement Device• Sterile dressing
– Must keep dry
• Keep site visible– Allows you to
• Catch injuries early• Gives you the ability to check site every hour
and before medications

Policies to Check Out…• II-101 Safe Administration of Parenteral Therapy, Including
Drugs Given Via the Intrathecal Route (Pharmacy and Therapuetics Policy Book)
• III-301 IV Insertion (Nursing Policies, Procedures and Standards Manual)
• III-203 Saline Well Guidelines/Blood Draw from an Established Venous Access (Nursing Policies, Procedures and Standards Manual)• III-306 Monitoring and Management of
Infiltration/Extravasation

Key Points
• Find out if patient is right or left handed
• Encourage movement of fingers, can hold a pencil, do homework, toy, doll etc
• Make sure tape is NOT too tight• Chart site check every hour

IV Key Points• Always have a person to
hold• Use butterflies for quick
in and out blood draws i.e. clinics
• Use distal sites first• Tell patient what you are
going to do before you do it

IV Key Points
• Practice• Practice• Practice

Other ways to obtain blood…
• Heel Stick• Finger Stick
– Heel and Finger sticks: blood can be collected in a Capillary tube or the small microtainers
• Butterfly Needles– 27, 25, 23, 21


















