PERITRAUMATIC DISSOCIATION IN LABOUR: IS IT A SENTINEL SIGNAL OF MOTHERS AT RISK FOR IMPAIRED PARENTING AND A NEW OPPORTUNITY FOR PREVENTIVE INTERVENTION? Julia Seng, PhD, CNM, FAAN Kristen Choi, RN, BSN University of Michigan, Ann Arbor, Michigan, USA
Transcript
PERITRAUMATIC DISSOCIATION IN LABOUR: IS IT A SENTINEL SIGNAL OF MOTHERS AT RISK FOR IMPAIRED PARENTING AND A NEW OPPORTUNITY FOR PREVENTIVE INTERVENTION?
Julia Seng, PhD, CNM, FAAN
Kristen Choi, RN, BSN
University of Michigan,
Ann Arbor, Michigan, USA
A research question from clinical practice
• Nurse-midwife• Working with very young and traumatized clients• Women and girls would “go inside themselves” during the
most intense time of labour• Some felt to me to be experiencing well-being (meditative)• Others felt “absent” or “unreachable”
• This was in the 1990’s, when PTSD among women was not yet well studied, dissociation was not broadly recognized as an aspect of PTSD, and maternity care providers did not have a way to “name” what we observed.
• So…a program of research unfolded.
Dissociation is gaining attention
Defined as “…a disruption in the usually integrated functions of consciousness, memory, identity, or perception of the environment.”
DSM-5 Dissociative Subtype of PTSD includes “substantial depersonalization or derealization.”
WHO epidemiology (n=25,000, 16 nations) indicates approximately ~14% of PTSD cases fit the subtype.
Not broken down by nature or age of trauma.
(A not entirely satisfying nod to Complex PTSD, DESNOS, and Developmental Trauma Disorder)
Dissociation and parenting concerns • Manifestation of trauma to the attachment system• Originally an “escape when there is no escape”• Subsequently a dysregulation in response to triggers or
overwhelm (or no escape/feeling trapped?)• Labour?• Crying infant?
• Risk for maltreatment? (Loss of integration of cognition, perception of the environment, judgment, emotion—at a physiologic level)
• “Ghosts” in the nursery? • Dissociation as a marker of maternal “unresolved trauma”?• Is dissociation “invisible” to birth attendants?
Part of an intergenerational pattern?• Associated with impaired parenting• Risk factor for child maltreatment and sequelae
• Daisy N, Hien D. The role of dissociation in the cycle of violence. J Fam Violence, 2014;29(2):99-107.
• Hulette A, Kaehler L, Freyd J. Intergenerational Associations Between Trauma and Dissociation. J Fam Violence, 2011;26(3):217-225.
• Liotti G. Trauma, dissociation, and disorganized attachment: Three strands of a single braid. Psychotherapy: Theory, Research, Practice, Training, 2004;41(4):472-486.
Body and mind dysregulated3 pillars of adaptation to maltreatment (per Teicher)
• HPA axis, catecholamines, oxytocin
Afternoon cortisol across gestation and postpartum
Qualitative data about labour
Sonya: “…kind of glazed over and drugged is the way it felt.”
Julie: “I was probably being ‘out of it’.”
Elizabeth: “…you know, you may not be dealing with someone who's acting as an adult here. There is stuff getting triggered…”
Terry: “…I can only remember [labour] up to a point, and then it just all goes away…And I picked that up from, you know, when my brother used to molest me…I would just close my eyes real tight and just imagine my spirit being lifted up out of my body and sitting on the bed until he was done. Then I would come back into myself. [And in labour] what happened was I just blocked myself out.
Seng, Kane Low, Sparbel & Killion, Journal of Advanced Nursing, 2004
The STACY Project: Stress, Trauma, Anxiety, and the Childbearing Year
US NIH R01 NR-008767 “Psychobiology of PTSD & Adverse Outcomes of Childbearing”—STACY Project
Not a post-disaster study. Community sample, observing usual care at three different settings to have adequate sample size for complex models. Julia Seng, PhD, CNM (PI) Lisa Kane Low, PhD, CNM (Detroit sites, labor details) David Ronis, PhD (statistician) Israel Liberzon, MD, (neuroendocrinology) Mickey Sperlich, PhD, MSW, CPM (infant mental health, social work, midwifery) OB nurses in three sites Numerous RAs
What are the effects of PTSD on childbearing outcomes?
Settings
UM, Ann Arbor: 90% European American90% insured
Detroit Medical Center (Hutzel Hospital): 90% African-American10% insured
Henry Ford Health System (New Center One): 30% African-American30% insured
All are nulliparas27 is mean age 71% partnered Diverse in race/ethnicityRange of education
Data Collection:
Screen & assign to cohort•Un-exposed controls•Trauma+ controls•PTSD+ cases
34% dismissed due to not fitting a cohort
UNSELECTED
Survey 1Initiating care
Diurnal salivary cortisol by mail
50% return
Next week
Survey 2~35 wks
Survey 3~6 wks pp
After EDD Later
Third trimester items, including interim trauma and PTSD
Medical records review:•Usual•OI-US•ICD-9
Postpartum outcomes:•Labor appraisal•Perception care•Parenting Sense of competence•PDEQ•pp PTSD•pp Depression•Bonding
DNA for SNPs
n=1,581 total,n=1,049 followed
n=425n=576 n=645 n=981 n=564
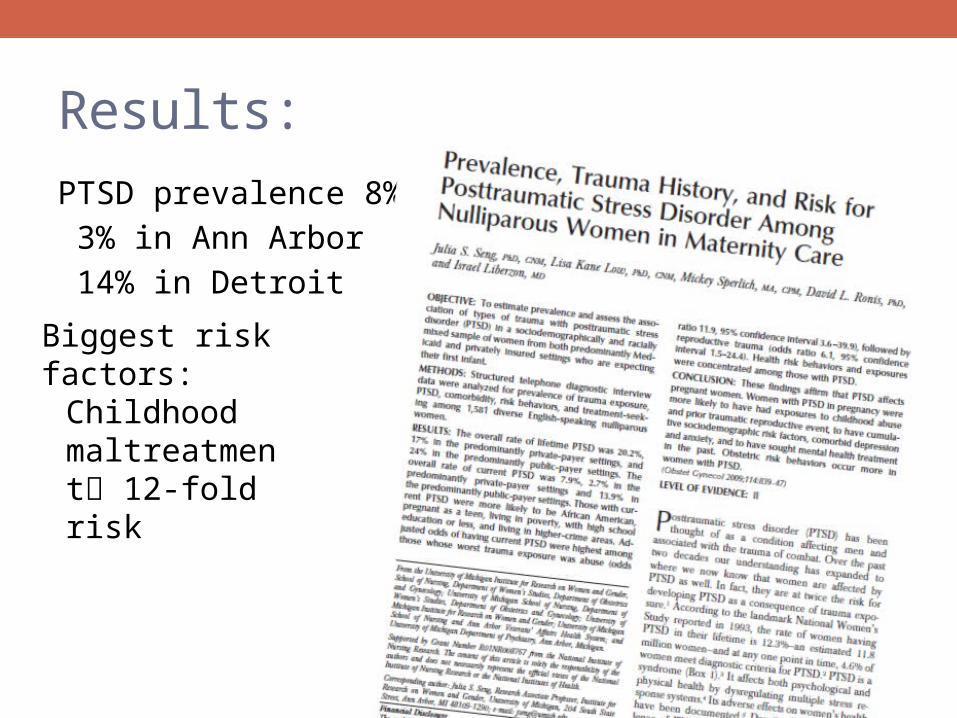
Results:
PTSD prevalence 8%
3% in Ann Arbor
14% in Detroit
Biggest risk factors:
Childhood maltreatment 12-fold risk
Results:Infants of PTSD-affected women weigh 283 grams less than resilient women’s infants.
The relationship of PTSD with adverse outcomes is stronger for women with PTSD subsequent to maltreatment.
Now replicated by Yonkers et al, 2014 and Shaw et al, 2014.
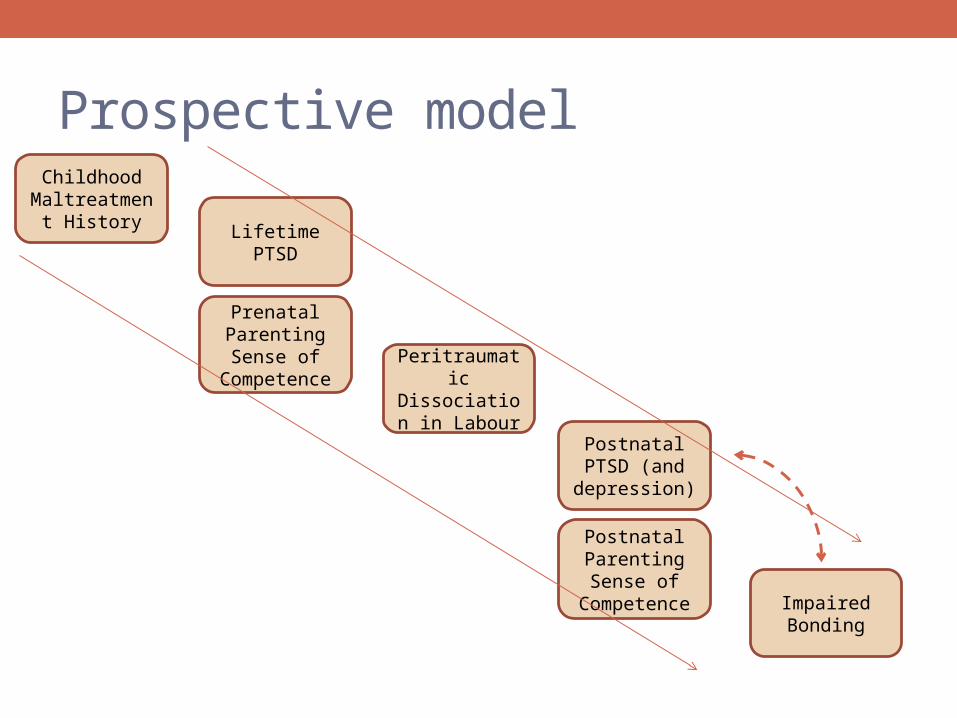
Results:
STACY Projectstatistical models supportintergenerationalpatterns of trauma and psychiatricvulnerability intersecting in thechildbearing year.
Implications for research• Replication of link of peritraumatic dissociation in labour with adverse
parenting outcomes.• Clarifying overlap of dissociation, dissatisfaction with care, and naming
the birth as traumatic—which factor used depends on the researchers’ agenda.
• Specific focus on at-risk and clinical samples—specialist midwives.• Specific focus on dissociation in response to the triggers of infant crying
or young child’s challenging behavior.• Intervention development and testing.
• NAMING it as a concern.• Adapting existing programs to address it with education and skills.• Trauma treatment to reduce response to trigger (i.e., PE, EMDR).• Supportive care and attention for these mothers to prevent need for dissociative
coping: Self-care? Child care? Infant massage?
• Understanding of physiology of dissociation may add weight to our awareness, especially across professions.
Implications for practice• For women with CMT-PTSD, is labour a “stress test” for
parenting difficulties and continuity of vulnerability?• Child welfare and mental health professionals can play a
key role here.• Discuss dissociation as a sentinel signal for parenting difficulties.• Case consults for midwives and obstetricians during learning curve.• Give them the vocabulary to “see” dissociation in labour.• Give them strategies to respond to dissociation in labour.• Be available to visit women in the postnatal days to teach
• strategies to stay grounded, • settling the infant, and • getting help if crying is a trigger.