PET/MRI: a new technology in the field of molecular imaging Asim Afaq, Rizwan Syed, and Jamshed Bomanji * Institute of Nuclear Medicine, University College London Hospital NHS Trust, London, UK Background: The introduction of the new simultaneous PET/MRI scanner opens new opportunities in functional imaging. Sources of data: This article is based on the literature review and our personal experience of the first simultaneous PET/MRI scanner in the UK. Areas of agreement: PET/CT is well established and a key component of management guidance in a range of diseases. MRI has superior soft tissue resolution, which is useful in the evaluation of many diseases. Areas of controversy: There are currently no guidelines regarding clinical use of PET/MRI, and those centres with a PET/MRI facility are undertaking research to look for a ‘key application’. Growing points and areas timely for developing research: This review briefly describes some of the technical advances, present comparisons with the diagnostic performance of current imaging modalities (PET/CT and MRI) and identifies potential indications and research directions. Keywords: multimodality imaging/PET/MRI/ 18 F-FDG/oncology/neurology Accepted: October 11, 2013 Introduction The ability to fuse images from two or more modalities is always interest- ing, but to acquire them simultaneously or within a narrow window of a few seconds or minutes is exciting as it opens the potential of utilizing the various functional parameters into a single study. Positron emission tomography (PET) is able to image multiple function- al parameters depending on the radiotracer used. The most common clin- ically available tracer, familiar to most physicians, is Fluorine-18 fluorodeoxyglucose ( 18 F-FDG), which reflects the glucose metabolism in normal and abnormal tissues, including tumours. PET is able to indicate the degree of metabolic activity by providing a semi-quantitative measure of glucose metabolism. Other less common tracers include fluorine-18 British Medical Bulletin 2013; 108: 159–171 DOI:10.1093/bmb/ldt032 & The Author 2013. Published by Oxford University Press. All rights reserved. For permissions, please e-mail: [email protected]*Correspondence address. Institute of Nuclear Medicine, University College London Hospital NHS Trust, 235 Euston Road, London NW1 2BU, UK. E-mail: jamshed. [email protected]Published Online November 13, 2013 Downloaded from https://academic.oup.com/bmb/article-abstract/108/1/159/347300 by guest on 29 March 2018
Transcript
PET/MRI: a new technology in the fieldof molecular imaging
Asim Afaq, Rizwan Syed, and Jamshed Bomanji*
Institute of Nuclear Medicine, University College London Hospital NHS Trust, London, UK
Background: The introduction of the new simultaneous PET/MRI scanner opens
new opportunities in functional imaging.
Sources of data: This article is based on the literature review and our personal
experience of the first simultaneous PET/MRI scanner in the UK.
Areas of agreement: PET/CT is well established and a key component of
management guidance in a range of diseases. MRI has superior soft tissue
resolution, which is useful in the evaluation of many diseases.
Areas of controversy: There are currently no guidelines regarding clinical use of
PET/MRI, and those centres with a PET/MRI facility are undertaking research to look
for a ‘key application’.
Growing points and areas timely for developing research: This review briefly
describes some of the technical advances, present comparisons with the diagnostic
performance of current imaging modalities (PET/CT andMRI) and identifies
The ability to fuse images from two or more modalities is always interest-ing, but to acquire them simultaneously or within a narrow window of afew seconds or minutes is exciting as it opens the potential of utilizing thevarious functional parameters into a single study.Positron emission tomography (PET) is able to image multiple function-
al parameters depending on the radiotracer used. The most common clin-ically available tracer, familiar to most physicians, is Fluorine-18fluorodeoxyglucose (18F-FDG), which reflects the glucose metabolism innormal and abnormal tissues, including tumours. PET is able to indicatethe degree of metabolic activity by providing a semi-quantitative measureof glucose metabolism. Other less common tracers include fluorine-18
British Medical Bulletin 2013; 108: 159–171DOI:10.1093/bmb/ldt032
& The Author 2013. Published by Oxford University Press. All rights reserved.For permissions, please e-mail: [email protected]
Downloaded from https://academic.oup.com/bmb/article-abstract/108/1/159/347300by gueston 29 March 2018
choline (18F-choline), fluorine-18 fluorothymidine (18F-FLT) andFluorine-18-fluoride (Table 1). Each of these tracers reflects a differentparameter, which can be imaged in normal and disease states. The abilityto successfully co-register these functional images with CT and therebycreate PET/CT was first achieved in 1998. The use of PET/CT has steadilyincreased since then, initially for imaging of lung disease and lymphomaand later across a broad range of pathologies. Furthermore, more disease-specific tracers have been increasingly used, including 18F-choline for theevaluation of brain tumours and prostate cancer, 68Ga-DOTATATE forneuroendocrine tumours and 18F-DOPA for insulinomas.1 PET/CT nowhas many approved indications and is included in guidelines for tumourstaging and response assessment in the UK (http://www.rcplondon.ac.uk/resources/evidence-based-indications-use-pet-ct-uk-2012).Magnetic resonance imaging (MRI) is able to provide excellent soft
tissue resolution and therefore anatomic detail and has the benefit of notusing ionizing radiation. In recent years, there has been an ongoing trendtowards expansion of the functional components of MRI and identifica-tion of their clinical utility. As a consequence, MRI can now serve as a
Table 1 Mechanism of action/biological correlate and clinical utility of PET tracers andMRIsequence or analysis method
Downloaded from https://academic.oup.com/bmb/article-abstract/108/1/159/347300by gueston 29 March 2018
combined anatomical and functional imaging modality and is constantlyevolving, with the modification of existing and the development of newsequences.Many studies over the past decade have combined data from independ-
ent PET and MRI studies, showing the potential utility of quantitativebiomarkers from each modality. However, these investigations were notperformed on simultaneous PET/MRI scanners and therefore had majorlimitations in respect of the interval between studies and the potential formisregistration of vital structures.2–5
Although the concept of combining PET and MRI into a single scannerhas been discussed for more than two decades, there have been severalmajor obstacles to the development of a viable scanner. The main hurdleshave included (a) photomultiplier tube technology, requiring replacementwith magnetic field-insensitive photodiodes; (b) the need to create PETdetectors in a format which would not interfere with MRI field gradientsor radiofrequency and (c) the absence of a suitable way to perform at-tenuation correction. Advances in technology have overcome most ofthese hurdles, with the development of MRI-compatible photodiodes(avalanche photodiodes) and the use of a two-point Dixon technique(a method of fat suppression) for attenuation correction.6
These advances resulted in the introduction in 2010 of the first gener-ation of whole-body PET/MRI scanners. This review looks at the poten-tial of this new technology and shares our experience of using PET/MRI(Siemens mMR) in clinical practice. The focus is on potential clinicalapplications in a setting without direct access to a cyclotron.
Sources of data
A PubMed/Medline search across all English language articles wasperformed using the keyword PET/MRI. The search was limited to1 January 2011–31 March 2013. Only those studies and articles wherePET/MRI was performed on a single scanning system were evaluatedfurther, i.e. those studies which performed the investigations independ-ently and/or used fusion techniques were not included in the review.Articles with a focus on potential human applications were selected.Fifty-nine articles were identified. Of these, 22 were of a review format,without original data and 19 addressed technical or physics-based issuessuch as attenuation correction or artefacts. Three articles evaluated abroad range of pathologies in a cross-over comparison format (PET/MRIversus PET/CT), five specifically assessed oncology applications and fivefocussed on neurological or head and neck applications. Of the remainingarticles, one was on a cardiovascular topic, one was an oncology-related
Molecular imaging with PET/MRI
British Medical Bulletin 2013;108 161
Downloaded from https://academic.oup.com/bmb/article-abstract/108/1/159/347300by gueston 29 March 2018
case report and three evaluated potential molecular pharmacologicaladvances in relation to PET/MRI.
Areas of agreement
MRI has better soft tissue contrast than CT, warranting the use of PET/MRI rather than PET/CT when this characteristic is important.Prospective areas of application include, in particular, oncology, cardiacimaging and neurology.
Oncology
Tumour phenotyping is a key potential role of PET/MRI, given the rangeof quantitative biomarkers which are evaluable in a single investigation.The ability to use these parameters to distinguish less from more aggres-sive tumours could have profound effects on risk stratification, prognosti-cation and management strategies.PET/MRI will be of particular benefit for imaging tumour sites, which
have traditionally been better evaluated with MRI than with CT. Theseinclude the head and neck, heart, liver, female pelvis, prostate andrectum and PET imaging in tumours of these sites is known to be ofpotential use.7–10 MRI plays an important role in staging of thesetumours. It has been postulated that combining information from PET,anatomical detail from high-resolution, small field of view T2-weightedimaging and functional MRI sequences, including diffusion, will furtherimprove the accuracy in T staging. In our experience this potential be-nefit has been realized in only a limited number of patients (J. Bomanji,personal communication). Similarly, nodal disease may benefit fromcombined functional assessment, given the well-known limitations ofsize-specific cut-off in distinguishing benign from malignant lymphnodes. However, to date, only similar N staging accuracy has beenfound when PET/MRI is applied as a whole-body staging approach,compared with PET/CT.11
Although no large-scale prospective data are available at present, inour experience there is a potential for PET/MRI to further refine TNMstaging in limited numbers of cases of cervical cancer, prostate cancer,recurrent breast cancer, lymphoma (Fig. 1), myeloma (solitary lesions)and head and neck cancers (Fig. 2). In a multi-reader study of 50 patientsat out institution, there was a 10% improvement in local stagingusing PET/MRI compared with PET/CT and confidence in anatomicallocalization of lesions improved by 5.1%.12 Monitoring of treatmentresponse in these tumours will also benefit from PET/MRI (Fig. 3).
A. Afaq et al.
162 British Medical Bulletin 2013;108
Downloaded from https://academic.oup.com/bmb/article-abstract/108/1/159/347300by gueston 29 March 2018
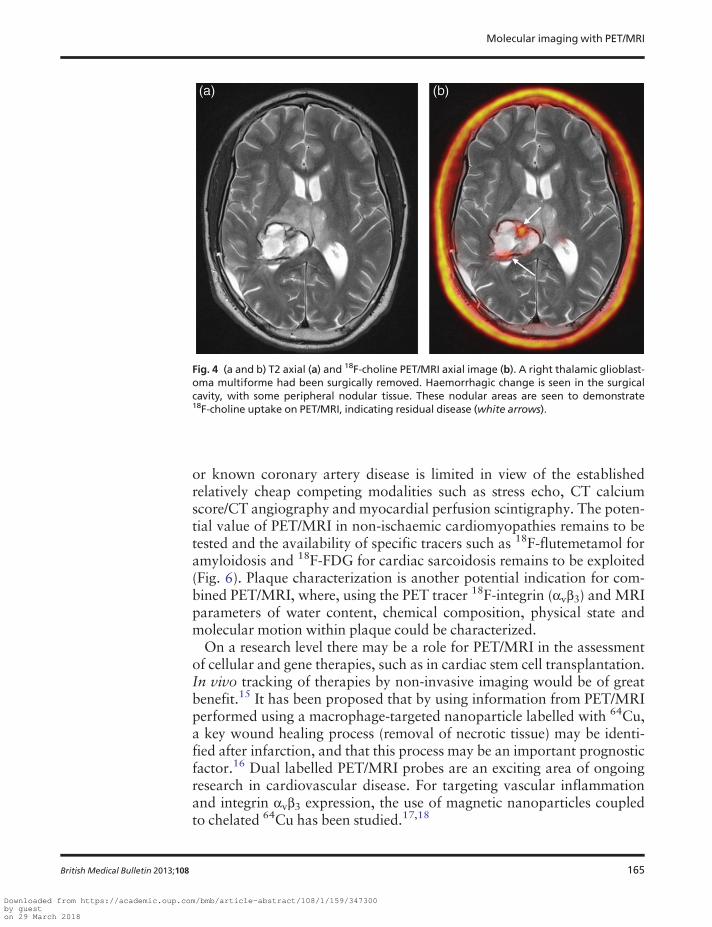
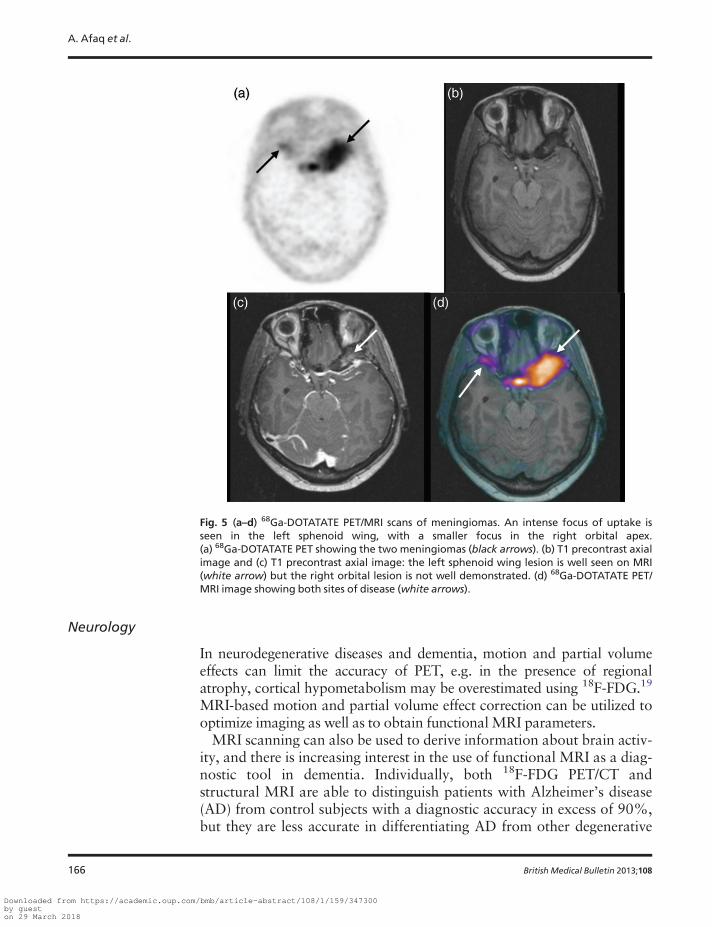
Imaging of brain tumours is a major potential use of PET/MRI, withthe same goals as apply to the imaging of other tumours. Specific tra-cers such as 18F-FLT, 18F-choline (Fig. 4) and 68Ga-DOTATATE (formeningiomas, Fig. 5), when used for PET/MRI, may enable the targetvolume to be altered in radiotherapy planning; this might have a signifi-cant effect on patient outcome and be of key importance when radiother-apy or surgery is being planned in areas of the brain with criticalfunction.13
Fig. 1 Coronal FDG PET/MRI image of a patient with lymphoma. Sites of disease can be seenabove (left supraclavicular disease, short white arrow) and below (abdominal lymph nodes,long white arrow) the diaphragm, which is important in staging the disease.
Molecular imaging with PET/MRI
British Medical Bulletin 2013;108 163
Downloaded from https://academic.oup.com/bmb/article-abstract/108/1/159/347300by gueston 29 March 2018
Cardiac imaging
The expectation remains that the PET/MRI scanner will exploit the super-ior tissue contrast inherent in the MRI component of the machine and themulti-parametric functional information provided by PET in cardiacdisease states.14 Currently, the role of PET/MRI in evaluating suspected
Fig. 3 (a and b) Osteosarcoma of the left mandible. T2 coronal FDG PET/MRI images areshown pre- (a) and post- (b) chemotherapy. Although there is little change in the volume ofthe mass, there is no longer tracer uptake, indicating complete metabolic response (whitearrow).
Fig. 2 (a and b) A tumour of the fossa of Rosenmüller. The small volume lesion is difficult tosee on the T2 axial image (a), but demonstrates the uptake on the FDG PET/MRI image(b,white arrow).
A. Afaq et al.
164 British Medical Bulletin 2013;108
Downloaded from https://academic.oup.com/bmb/article-abstract/108/1/159/347300by gueston 29 March 2018
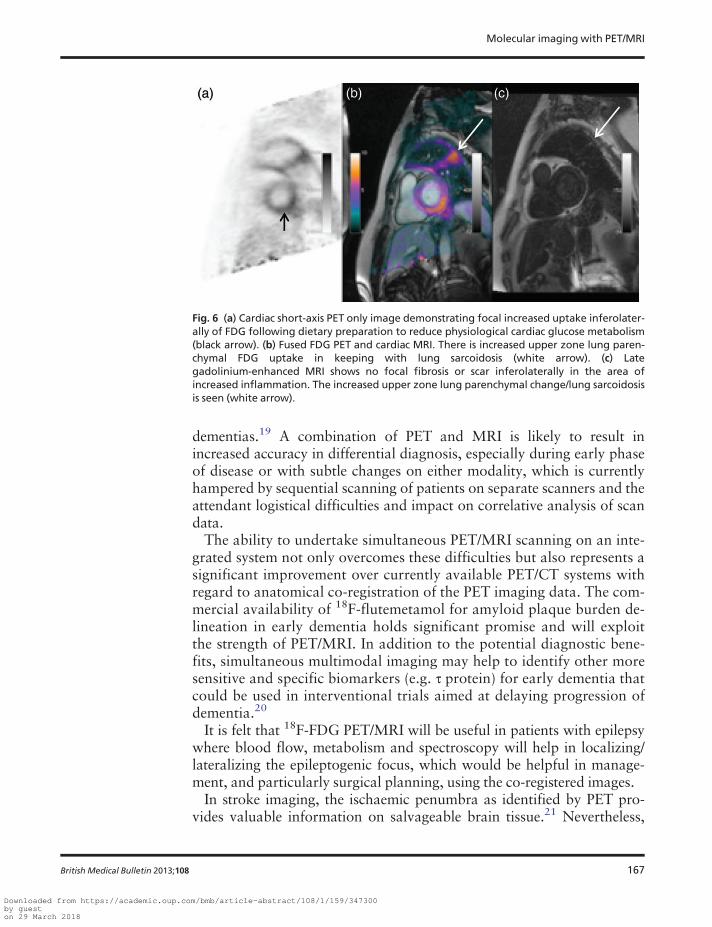
or known coronary artery disease is limited in view of the establishedrelatively cheap competing modalities such as stress echo, CT calciumscore/CT angiography and myocardial perfusion scintigraphy. The poten-tial value of PET/MRI in non-ischaemic cardiomyopathies remains to betested and the availability of specific tracers such as 18F-flutemetamol foramyloidosis and 18F-FDG for cardiac sarcoidosis remains to be exploited(Fig. 6). Plaque characterization is another potential indication for com-bined PET/MRI, where, using the PET tracer 18F-integrin (αvβ3) and MRIparameters of water content, chemical composition, physical state andmolecular motion within plaque could be characterized.On a research level there may be a role for PET/MRI in the assessment
of cellular and gene therapies, such as in cardiac stem cell transplantation.In vivo tracking of therapies by non-invasive imaging would be of greatbenefit.15 It has been proposed that by using information from PET/MRIperformed using a macrophage-targeted nanoparticle labelled with 64Cu,a key wound healing process (removal of necrotic tissue) may be identi-fied after infarction, and that this process may be an important prognosticfactor.16 Dual labelled PET/MRI probes are an exciting area of ongoingresearch in cardiovascular disease. For targeting vascular inflammationand integrin αvβ3 expression, the use of magnetic nanoparticles coupledto chelated 64Cu has been studied.17,18
Fig. 4 (a and b) T2 axial (a) and 18F-choline PET/MRI axial image (b). A right thalamic glioblast-oma multiforme had been surgically removed. Haemorrhagic change is seen in the surgicalcavity, with some peripheral nodular tissue. These nodular areas are seen to demonstrate18F-choline uptake on PET/MRI, indicating residual disease (white arrows).
Molecular imaging with PET/MRI
British Medical Bulletin 2013;108 165
Downloaded from https://academic.oup.com/bmb/article-abstract/108/1/159/347300by gueston 29 March 2018
Neurology
In neurodegenerative diseases and dementia, motion and partial volumeeffects can limit the accuracy of PET, e.g. in the presence of regionalatrophy, cortical hypometabolism may be overestimated using 18F-FDG.19
MRI-based motion and partial volume effect correction can be utilized tooptimize imaging as well as to obtain functional MRI parameters.MRI scanning can also be used to derive information about brain activ-
ity, and there is increasing interest in the use of functional MRI as a diag-nostic tool in dementia. Individually, both 18F-FDG PET/CT andstructural MRI are able to distinguish patients with Alzheimer’s disease(AD) from control subjects with a diagnostic accuracy in excess of 90%,but they are less accurate in differentiating AD from other degenerative
Fig. 5 (a–d) 68Ga-DOTATATE PET/MRI scans of meningiomas. An intense focus of uptake isseen in the left sphenoid wing, with a smaller focus in the right orbital apex.(a) 68Ga-DOTATATE PET showing the two meningiomas (black arrows). (b) T1 precontrast axialimage and (c) T1 precontrast axial image: the left sphenoid wing lesion is well seen on MRI(white arrow) but the right orbital lesion is not well demonstrated. (d) 68Ga-DOTATATE PET/MRI image showing both sites of disease (white arrows).
A. Afaq et al.
166 British Medical Bulletin 2013;108
Downloaded from https://academic.oup.com/bmb/article-abstract/108/1/159/347300by gueston 29 March 2018
dementias.19 A combination of PET and MRI is likely to result inincreased accuracy in differential diagnosis, especially during early phaseof disease or with subtle changes on either modality, which is currentlyhampered by sequential scanning of patients on separate scanners and theattendant logistical difficulties and impact on correlative analysis of scandata.The ability to undertake simultaneous PET/MRI scanning on an inte-
grated system not only overcomes these difficulties but also represents asignificant improvement over currently available PET/CT systems withregard to anatomical co-registration of the PET imaging data. The com-mercial availability of 18F-flutemetamol for amyloid plaque burden de-lineation in early dementia holds significant promise and will exploitthe strength of PET/MRI. In addition to the potential diagnostic bene-fits, simultaneous multimodal imaging may help to identify other moresensitive and specific biomarkers (e.g. τ protein) for early dementia thatcould be used in interventional trials aimed at delaying progression ofdementia.20
It is felt that 18F-FDG PET/MRI will be useful in patients with epilepsywhere blood flow, metabolism and spectroscopy will help in localizing/lateralizing the epileptogenic focus, which would be helpful in manage-ment, and particularly surgical planning, using the co-registered images.In stroke imaging, the ischaemic penumbra as identified by PET pro-
vides valuable information on salvageable brain tissue.21 Nevertheless,
Fig. 6 (a) Cardiac short-axis PET only image demonstrating focal increased uptake inferolater-ally of FDG following dietary preparation to reduce physiological cardiac glucose metabolism(black arrow). (b) Fused FDG PET and cardiac MRI. There is increased upper zone lung paren-chymal FDG uptake in keeping with lung sarcoidosis (white arrow). (c) Lategadolinium-enhanced MRI shows no focal fibrosis or scar inferolaterally in the area ofincreased inflammation. The increased upper zone lung parenchymal change/lung sarcoidosisis seen (white arrow).
Molecular imaging with PET/MRI
British Medical Bulletin 2013;108 167
Downloaded from https://academic.oup.com/bmb/article-abstract/108/1/159/347300by gueston 29 March 2018
since the tracers which are used to generate this information are notwidely available, particularly in an emergency setting, CT and, increas-ingly, MRI are used instead. However, perfusion and diffusion-weightedimaging on MRI does not correlate precisely with the PET penumbra.22
Simultaneous PET/MRI acquisition may lead to optimization of treat-ment planning in patients with ischaemic stroke in the acute setting andalso permit monitoring of lesion progression.The potential to obtain simultaneous quantitative data from PET and
functional MRI may make possible the acquisition of information onneurotransmitter-mediated processes such as in Parkinson’s disease, wherereceptor expression and neuronal activation may be monitored as part ofpharmacological response assessment by PET andMRI, respectively.22
Areas of controversy
The main controversy regarding PET/MR is its specific clinical role andcost-effectiveness.
Financial considerations
Few doubt the potential benefit of using multiple quantitative imagingbiomarkers with PET/MRI. However, the financial burden of running acombined PET/MRI scanner is considerable. In addition, efficientrunning requires dual-trained nuclear medicine physicians, radiologists,technologists, radiographers and physicists who are difficult to findand recruit, a difficulty compounded by lack of formal PET/MRI trainingprogrammes.
Service challenges
As with all new technologies, there are other competing modalities. In thecontext of PET/MRI there is a trend towards the fusion of PET/CT andMRI images acquired on separate machines within a short time interval.This is made possible by recent advances in image registration andmotion correction, which improve the data quality obtained with non-simultaneous PET/CT and MRI. It is therefore arguable if investment in asimultaneous PET/MRI machine is justifiable.Although this review focussed on potential clinical applications of PET/
MRI, there are undoubtedly major potential research applications of thisimaging modality. As acquisition of the scanner may depend on joint clin-ical and research funds, a potential service challenge is to accommodate
A. Afaq et al.
168 British Medical Bulletin 2013;108
Downloaded from https://academic.oup.com/bmb/article-abstract/108/1/159/347300by gueston 29 March 2018
both clinical and research studies throughout the scanning day. This maybe particularly challenging as complex clinical cases, which are evaluatedmay be under time pressure of impending deadlines for surgery and re-search studies may contain multiple experimental sequences, adding tooverall scanning time.Utilization of tracers such as oxygen-15, carbon 11 and other short-
lived radiotracers is not possible without direct access to a cyclotron. It is,however, possible to combine some useful tracers with fluorine, whichincreases half life, for example fluorocholine as an alternative to carboncholine.
Growing points
Many patients undergo PET/CT imaging and MRI during the course oftheir management, often within a short time interval. In such cases, theopportunity to perform a combined scan will be beneficial to the patientpathway by reducing the number of patient visits. Reduction of the ioniz-ing radiation dose with PET/MRI is another advantage. The radiation ex-posure from the hybrid PET/MR imaging has been reportedly 80% lessthan a PET/CT study.23 This is particularly important when consideringserial scans in response assessment and when imaging those most vulner-able to the effects of radiation—the paediatric population.As work with novel tracers continues, it is important to validate
imaging-based phenotyping from both PET andMRI with gold standardssuch as pathological correlates. For example, hypoxia in tumours may beevaluated using FMISO and Blood Oxygen Level-Dependent MRimaging during simultaneous PET/MRI, but this must be evaluatedagainst hypoxia quantified from histopathology. Similarly, angiogenesistracers such as rubidium and dynamic contrast-enhanced MRI performedsimultaneously can be evaluated against histopathological quantificationof angiogenesis. This research may yield important information to guidewhich are the optimum and most accurate phenotyping sequences forfuture protocols.There are also growing points in terms of technology within PET/MRI
to improve image acquisition. Attenuation correction algorithms usingMR data are being continually being developed, particularly in brainimaging. MR-based motion correction technologies to correct for grosspatient motion and breathing are also under development and are par-ticularly important given relatively long PET data acquisition times.The optimal clinical applications of PET/MRI remain to be established.
Finding the ‘key application’ will secure the role of PET/MRI in patientmanagement. Currently, a large-scale indication remains elusive and until
Molecular imaging with PET/MRI
British Medical Bulletin 2013;108 169
Downloaded from https://academic.oup.com/bmb/article-abstract/108/1/159/347300by gueston 29 March 2018
research can prove clinical benefit, against important outcome measures,the technology will remain in its infancy.
Conclusion
PET/MRI is one of the most exciting developments in imaging in recentyears. There is scope within oncology, neurology and cardiac imaging forthis modality to develop, although widely accepted clinical indicationsremain to be defined. The growing use of novel tracers and functionalMRI parameters offers great potential benefit; this is especially evident inresearch but there are also various clinical applications in which optimalmolecular information might be acquired, guiding the management ofpatients. Ultimately, many factors will decide the clinical role of PET/MRI in the NHS. The cost of the system and the clinical benefit to thepatient compared with PET/CT will be the main driving forces in thiscontext.
Acknowledgements
The authors acknowledge the support of the UCLH Charity, whodonated the first UK PETMR scanner.
Funding
The work was undertaken at UCL Hospitals NHS Foundation Trust,which receive a proportion of funding from the Department of Health’sNational Institute for Health Research (NIHR) Biomedical ResearchCentres’ funding scheme.
References
1 Beyer T, Townsend DW, Brun T et al. A combined PET/CT scanner for clinical oncology. J NuclMed 2000;41:1369–79.
2 Hofmann M, Pichler B, Schölkopf B et al. Towards quantitative PET/MRI: a review ofMR-based attenuation correction techniques. Eur J Nucl Med Mol Imaging 2009;36(Suppl. 1):S93–104.
3 Antoch G, Bockisch A. Combined PET/MRI: a new dimension in whole-body oncologyimaging? Eur J Nucl Med Mol Imaging 2009;36(Suppl. 1):S113–20.
4 Kwee TC, Takahara T, Ochiai R et al. Complementary roles of whole-body diffusion-weightedMRI and 18F-FDG PET: the state of the art and potential applications. J Nucl Med2010;51:1549–58.
A. Afaq et al.
170 British Medical Bulletin 2013;108
Downloaded from https://academic.oup.com/bmb/article-abstract/108/1/159/347300by gueston 29 March 2018
5 Gu J, Khong PL, Wang S et al. Combined use of 18F-FDG PET/CT, DW-MRI, and DCE-MRI intreatment response for preoperative chemoradiation therapy in locally invasive rectal cancers.Clin Nucl Med 2013;38:e226–9.
6 Martinez-Moller A, Souvatzoglou M, Delso G et al. Tissue classification as a potential approachfor attenuation correction in whole-body PET/MRI: evaluation with PET/CT data. J Nucl Med2009;50:520–6.
7 Boss A, Bisdas S, Kolb A et al. Hybrid PET/MRI of intracranial masses: initial experiences andcomparison to PET/CT. J Nucl Med 2010;51:1198–205.
8 Eschmann SM, Pfannenberg AC, Rieger A et al. Comparison of 11C Choline PET/CT andwhole bodyMRI for staging of prostate cancer.Nuklearmedizin 2007;46:161–8.
9 Sinoni A, Buda A, Piccio M et al. Lymph node metastasis in patients with clinical early stage cer-vical cancer: detection with integrated FDG PET/CT. Radiology 2006;238:272–9.
10 Floriani I, Torri V, Rulli E et al. Performance of imaging modalities in diagnosis of liver metasta-ses from colorectal cacner: a systematic review and meta-analysis. J Magn Reson Imaging2010;31:19–31.
11 Buchbender C, Heusner TA, Lauenstein TC et al. Oncologic PET/MRI, part 1: tumors of thebrain, head and neck, chest, abdomen, and pelvis. J Nucl Med 2012;53:928–38.
12 Al-Nabhani K, Syed R, Michopoulou S et al. Qualitative and quantitative comparison of PET/CT and PET/MRI in clinical practice. J Nucl Med 2013 (accepted).
13 Heiss WD, Raab P, Lanfermann H. Multimodality assessment of brain tumours and tumour re-currence. J Nucl Med 2011;52:1585–600.
14 Nekolla SG, Martinez-Moeller A, Saraste A. PET and MRI in cardiac imaging: from validationstudies to integrated applications. Eur J Nucl Med Mol Imaging 2009;36(Suppl. 1):S121–30.
15 Zhang WY, Ebert AD, Narula J et al. Imaging cardiac stem cell therapy: translations to humanclinical studies. J Cardiovasc Transl Res 2011;4:514–22.
16 Majmudar MD, Nahrendorg M. Cardiovascular molecular imaging: The road ahead. J NuclMed 2012;53:673–6.
17 Jarrett BR, Gustafsson B, Kukis DL et al. Synthesis of Cu-64 labelled magnetic nanoparticles formultimodal imaging. Bioconjug Chem 2008;19:1496–504.
18 Lee HY, Li Z, Chen K et al. PET/MRI dual modality tumour imaging usingarginine-glycine-aspartic (RGD): conjugated radiolabeled iron oxide nanoparticles. J Nucl Med2008;49:1371–9.
19 Bohnen NI, Djang DS, Herholz K et al. Effectiveness and safety of 18F-FDG PET in the evalu-ation of dementia: a review of the recent literature. J Nucl Med 2012;53:59–71.
20 Ono M, Saji H. Molecular approaches to the treatment, prophylaxis, and diagnosis ofAlzheimer’s disease: novel PET/SPECT imaging probes for diagnosis of Alzheimer’s disease.J Pharmacol Sci 2012;118:338–44.
21 Heiss WD. The ischemic penumbra: correlates in imaging and implications for treatment ofischemic stroke. The Johann JacobWepfer award 2011. Cerebrovasc Dis 2011;32:307–20.
22 Catana C, Drzezga A, Heiss W et al. PET/MRI for neurologic applications. J Nucl Med2012;53:1916–25.
23 Hirsch FW, Sattler B, Sorge I et al. PET/MR in children. Initial clinical experience in paediatriconcology using an integrated PET/MR scanner. Pediatr Radiol 2013;43:860–75.
Molecular imaging with PET/MRI
British Medical Bulletin 2013;108 171
Downloaded from https://academic.oup.com/bmb/article-abstract/108/1/159/347300by gueston 29 March 2018