Neurosurg Focus / Volume 33 / August 2012 Neurosurg Focus 33 (2):E10, 2012 1 T HE unfortunate natural course that brainstem CMs may follow has led to the active cultivation of sur- gical techniques to successfully resect these lesions and halt a commonly seen relentless progression. 1,15,22 Al- though the actual hemorrhage rate may not differ from their lobar counterparts, 2,16,34,37 brainstem CMs clearly follow a more aggressive clinical course, as subtle mor- phological changes of this brainstem lesion can have dra- matic neurological consequences. 15,41 This was elegantly demonstrated by Porter et al., 41 who reported on brain- stem CMs that had an annual event rate of 10.6%. When considering the optimal surgical approach for brainstem CM resection, that which affords the most acute angle to the site of pial representation is most de- sired. A reasonable choice for CMs with pial presentation at the lateral pons, the retrosigmoid approach may not be appropriate for CMs with pial presentation at its anterior or anterolateral surface. For these lesions, it would afford a more tangential line of approach. This has the 3 follow- ing significant disadvantages, particularly in the context of large brainstem CMs: 1) requisite significant retraction of the cerebellum, 2) an inability to adequately visualize and inspect the surgical cavity for residual CM, and 3) potential difficulty operating around and/or identifying and preserving a small associated DVA. All 3 of these limitations are well addressed by the more ventral and lateral exposure afforded by the petrosal approaches. 3,17,21,33,36 The refinement and successful appli- cation of these approaches to neoplastic lesions over the past 3 decades is well presented in the literature. 3,7,8,11,17,18, 20,23,32,33,43,46,47,49 In contrast, their application to brainstem CMs has met with some skepticism. 5 In the present arti- cle, we illustrate the success and relatively low long-term morbidity rate of hearing-preserving petrosal approaches to brainstem CM. Petrosal approaches to brainstem cavernous malformations BRADLEY A. GROSS, M.D., IAN F. DUNN, M.D., ROSE DU, M.D., PH.D., AND OSSAMA AL-MEFTY , M.D. Department of Neurological Surgery, Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts Object. Although they provide excellent ventral and lateral exposure of the brainstem, petrosal approaches to brainstem cavernous malformations (CMs) are infrequently reported. Methods. The authors reviewed their experience with petrosal approaches to brainstem CMs in combination with a comprehensive review of the literature to elucidate resection rates, complication rates, and outcomes. Results. Including their own results, the authors found 65 cases in 20 reports of brainstem CMs treated with pe- trosal approaches. The specific approaches were posterior petrosal in 37 cases (57%), anterior petrosal in 17 (26%), extended posterior petrosal in 10 (15%), and a combined petrosal approach in 1 case (2%). For 50 cases in 16 reports with detailed outcome information, the overall complete resection rate was 90%, with early postoperative morbidity reported in 30% of cases and permanent morbidity in 14%. The rate of CSF leakage was 6%. Conclusions. The versatile petrosal approaches to brainstem CMs are associated with good outcomes and an ac- ceptable morbidity rate. More expansive lesions can be approached using a combination of the standard anterior and posterior petrosal approach, preserving hearing and avoiding the greater complication rates associated with extended posterior petrosal approaches. (http://thejns.org/doi/abs/10.3171/2012.6.FOCUS12110) KEY WORDS • petrosal approach • retrolabyrinthine approach • presigmoid approach • Kawase approach • combined approach • skull base • cavernous malformation • cavernoma 1 Abbreviations used in this paper: CM = cavernous malformation; DVA = developmental venous anomaly.
Transcript
Neurosurg Focus / Volume 33 / August 2012
Neurosurg Focus 33 (2):E10, 2012
1
The unfortunate natural course that brainstem CMs may follow has led to the active cultivation of sur-gical techniques to successfully resect these lesions
and halt a commonly seen relentless progression.1,15,22 Al-though the actual hemorrhage rate may not differ from their lobar counterparts,2,16,34,37 brainstem CMs clearly follow a more aggressive clinical course, as subtle mor-phological changes of this brainstem lesion can have dra-matic neurological consequences.15,41 This was elegantly demonstrated by Porter et al.,41 who reported on brain-stem CMs that had an annual event rate of 10.6%.
When considering the optimal surgical approach for brainstem CM resection, that which affords the most acute angle to the site of pial representation is most de-sired. A reasonable choice for CMs with pial presentation at the lateral pons, the retrosigmoid approach may not be
appropriate for CMs with pial presentation at its anterior or anterolateral surface. For these lesions, it would afford a more tangential line of approach. This has the 3 follow-ing significant disadvantages, particularly in the context of large brainstem CMs: 1) requisite significant retraction of the cerebellum, 2) an inability to adequately visualize and inspect the surgical cavity for residual CM, and 3) potential difficulty operating around and/or identifying and preserving a small associated DVA.
All 3 of these limitations are well addressed by the more ventral and lateral exposure afforded by the petrosal approaches.3,17,21,33,36 The refinement and successful appli-cation of these approaches to neoplastic lesions over the past 3 decades is well presented in the literature.3,7,8,11,17,18,
20,23,32,33,43,46,47,49 In contrast, their application to brainstem CMs has met with some skepticism.5 In the present arti-cle, we illustrate the success and relatively low long-term morbidity rate of hearing-preserving petrosal approaches to brainstem CM.
Petrosal approaches to brainstem cavernous malformations
Bradley a. Gross, M.d., Ian F. dunn, M.d., rose du, M.d., Ph.d., and ossaMa al-MeFty, M.d.Department of Neurological Surgery, Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts
Object. Although they provide excellent ventral and lateral exposure of the brainstem, petrosal approaches to brainstem cavernous malformations (CMs) are infrequently reported.
Methods. The authors reviewed their experience with petrosal approaches to brainstem CMs in combination with a comprehensive review of the literature to elucidate resection rates, complication rates, and outcomes.
Results. Including their own results, the authors found 65 cases in 20 reports of brainstem CMs treated with pe-trosal approaches. The specific approaches were posterior petrosal in 37 cases (57%), anterior petrosal in 17 (26%), extended posterior petrosal in 10 (15%), and a combined petrosal approach in 1 case (2%). For 50 cases in 16 reports with detailed outcome information, the overall complete resection rate was 90%, with early postoperative morbidity reported in 30% of cases and permanent morbidity in 14%. The rate of CSF leakage was 6%.
Conclusions. The versatile petrosal approaches to brainstem CMs are associated with good outcomes and an ac-ceptable morbidity rate. More expansive lesions can be approached using a combination of the standard anterior and posterior petrosal approach, preserving hearing and avoiding the greater complication rates associated with extended posterior petrosal approaches.(http://thejns.org/doi/abs/10.3171/2012.6.FOCUS12110)
Abbreviations used in this paper: CM = cavernous malformation; DVA = developmental venous anomaly.
B. A. Gross et al.
2 Neurosurg Focus / Volume 33 / August 2012
MethodsIn addition to a review of our own experience, we
performed a PubMed search using the terms “caverno-ma,” “cavernous angioma,” “cavernous hemangioma,” “cavernous malformation,” “brainstem,” “transpetrosal,” “petrosal,” “Kawase,” “retrolabyrinthine,” “presigmoid,” “transcrusal,” “translabyrinthine,” “transotic,” and “transcochlear.” References within afforded articles were perused and were included if applicable. We included studies in our analysis that provided outcomes for patients with brainstem CMs specifically treated via a petrosal ap-proach. Including our own experience, we noted patient age, sex, symptoms at presentation, approach used, results of resection, and complications.
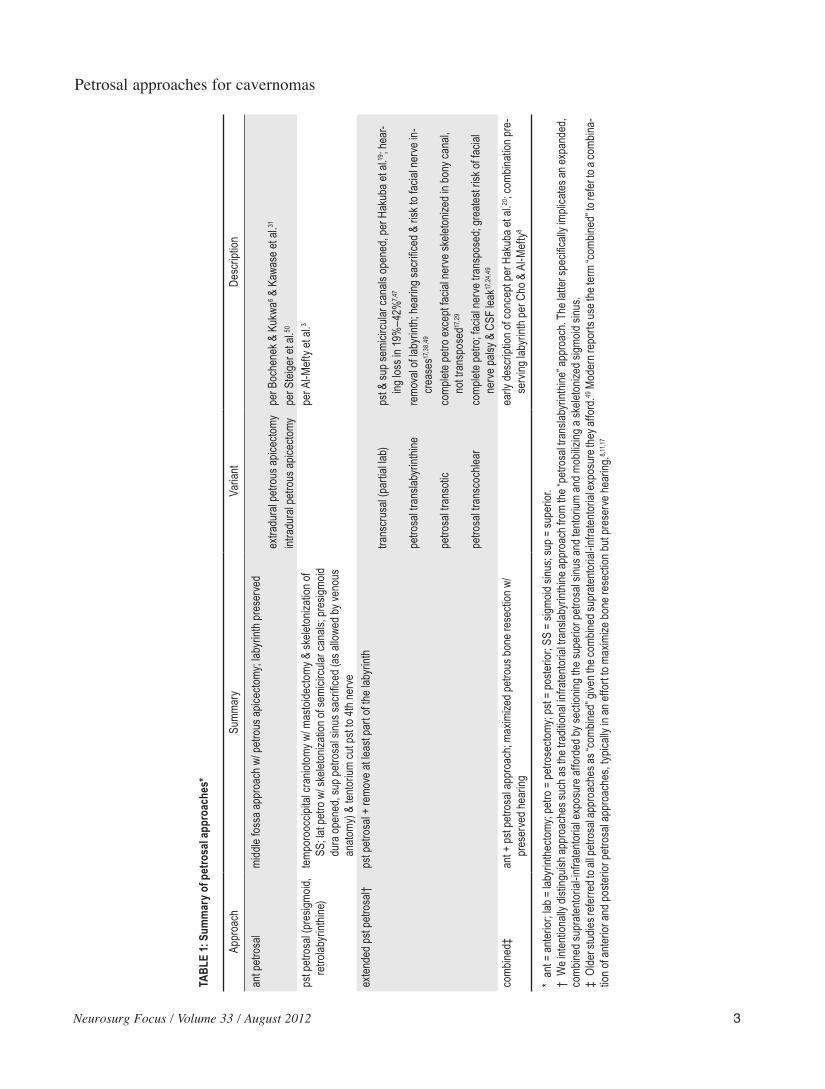
A summary of our classification of petrosal approach-es is provided in Table 1. The term “petrosal” is intention-ally appended to each extended posterior approach. This distinguishes them from smaller infratentorial approach-es using partial or complete labyrinthectomy (traditional translabyrinthine route) without sectioning the superior petrosal sinus and mobilizing a skeletonized sigmoid si-nus.14 It is crucial to emphasize that these maneuvers are distinguishing features of the posterior petrosal approach that allow for the realization of the expansive, combined supra- and infratentorial exposure that it can provide.3,11,17
ResultsIncorporating our own results (with 2 cases not pub-
lished in the literature), we found 65 cases of brainstem CMs resected via a petrosal approach in 20 reports.1,5,7,12,13,
21,25,27,30,32,36,39,40,42,44,46,48,50,51,53 The specific approaches were posterior petrosal in 37 cases (57%), anterior petrosal in 17 (26%), extended posterior petrosal in 10 (15%), and a combined petrosal approach in 1 (2%) (Table 1). Extend-ed posterior petrosal approaches included the transcrusal approach (partial labyrinthectomy) in 5 cases (8%), petro-sal translabyrinthine approach in 4 (6%), and the petrosal transcochlear approach in 1 case (2%).
Individualized patient background information and outcomes were provided for 50 patients in 16 reports, comprising the remainder of our analysis. These 50 cases are summarized in Tables 2–4, stratified by surgical ap-proach. Overall, the mean patient age was 40.2 years, and 34 (68%) of 50 patients were female. Two patients were younger than 18 years. All CMs were pontine except one, which was mesencephalic. All but 1 patient presented with a combination of cranial nerve deficits, motor defi-cits, and/or sensory deficits. Across 14 studies providing details of CM removal, 37 (90%) of 41 CMs were com-pletely resected. Across 13 reports, the status of 23 (61%) of 38 patients was reported as improved at last follow-up. Overall, early morbidity, inclusive of worsening cranial deficits, worsening motor strength, wound infections, and CSF leaks, was reported in 15 cases (30%). Specifically, the rate of CSF leakage was 6%. Permanent morbidity was seen in 7 cases (14%). As we illustrate in the follow-ing stratified analysis, more cases with early and perma-nent morbidity were treated with extended petrosal ap-proaches, resulting in facial weakness, hearing loss, and higher rates of CSF leaks.
Anterior Petrosal ApproachBackground information and results for 17 patients
treated with anterior petrosal approaches in 8 studies are provided in Table 2. Fourteen CMs in 7 of 8 studies were resected via the traditional Kawase approach,31 whereas the 3 CMs described by Steiger et al.50 were approached after an intradural anterior petrosectomy. In 1 challeng-ing case in the latter study, only a partial resection was achieved with a concomitant loss of hearing. The other 2 cases were improved at follow-up with complete resection of their CM.
Overall, complete CM resection was reported in 13 (81%) of 16 cases, with hearing loss reported in 2 (12%). At follow-up, 14 (82%) of 17 patients were improved and 1 additional patient who presented neurologically intact remained so. Thus, excellent outcomes were achieved in 15 (88%) of 17 cases, and permanent morbidity, in the form of hearing loss, was seen in 2 cases (12%).
Posterior Petrosal ApproachOur literature search found that the hearing-preserv-
ing, posterior petrosal retrolabyrinthine approach was the most common petrosal approach used in the treatment of brainstem CMs. Table 3 provides details obtained in 27 patients from 7 reports. Resection was complete in 96%. Hearing loss was reported in only 2 patients (7%) and was permanent in only 1 (4%).
Overall, transient complications were seen in 7 (26%) of 27 cases, including temporary worsening of cranial deficits in 3 (11%), CSF leakage in 2 (7%), temporary worsening of a motor deficit in 1 (4%), and wound infec-tion in 1 (4%). When reported, improvement at follow-up was seen in 9 (60%) of 15 cases, while permanent mor-bidity/worsening was reported in 1 (4%) of 27 cases.
Extended Posterior Petrosal ApproachesAlthough 10 of 65 cases in our reviewed series were
treated with extended posterior petrosal approaches, de-tailed information was only available for 6 (5 treated with the addition of a partial labyrinthectomy [transcrusal] and 1 treated with the addition of a complete labyrinthecto-my).7,48,53 We have grouped these approaches because they all pose a significant threat (transcrusal/partial labyrin-thectomy) or permanently sacrifice hearing (labyrinthec-tomy). Indeed, 3 of 5 patients in whom the transcrusal ap-proach was used had hearing loss after surgery (Table 4). Of the 6 cases reviewed, all but 1 patient suffered either early or permanent complications. Two of 6 patients had postoperative CSF leaks, and new facial nerve palsy was also reported in 2 patients.
DiscussionPetrosal approaches play a crucial role in the man-
agement of complex cerebrovascular lesions.9,46 At the same time that these approaches were being popularized in the late 1980s,3,43 surgical series of brainstem CMs be-gan to accrue.45,52 Results from these series were encour-aging, although complete CM resection was not always
Neurosurg Focus / Volume 33 / August 2012
Petrosal approaches for cavernomas
3
TABL
E 1:
Sum
mar
y of p
etro
sal a
ppro
ache
s*
Appr
oach
Summ
ary
Varia
ntDe
scrip
tion
ant p
etros
almi
ddle
foss
a app
roac
h w/ p
etrou
s apic
ectom
y; lab
yrint
h pre
serv
edex
tradu
ral p
etrou
s apic
ectom
ype
r Boc
hene
k & K
ukwa
6 & K
awas
e et a
l.31
intra
dura
l petr
ous a
picec
tomy
per S
teige
r et a
l.50
pst p
etros
al (p
resig
moid,
retro
labyr
inthin
e)tem
poro
occip
ital c
ranio
tomy w
/ mas
toide
ctomy
& sk
eleton
izatio
n of
SS
; lat p
etro w
/ ske
leton
izatio
n of s
emici
rcula
r can
als; p
resig
moid
dura op
ened, sup pe
trosal sinu
s sacrificed (as allow
ed by
venous
an
atomy
) & te
ntoriu
m cu
t pst
to 4th
nerv
e
per A
l-Mef
ty et
al.3
exten
ded p
st pe
trosa
l†ps
t petr
osal
+ re
move
at le
ast p
art o
f the l
abyr
inth
trans
crus
al (p
artia
l lab)
pst &
sup s
emici
rcula
r can
als op
ened
, per
Hak
uba e
t al.19
; hea
r-
ing lo
ss in
19%
–42%
7,47
petro
sal tr
ansla
byrin
thine
remo
val of la
byrinth; he
aring
sacrific
ed & risk to facia
l nerve in-
cr
ease
s17,3
8,49
petro
sal tr
anso
ticco
mplet
e petr
o exc
ept fa
cial n
erve
skele
tonize
d in b
ony c
anal,
not tr
ansp
osed
17,2
9
petro
sal tr
ansc
ochle
arco
mplet
e petr
o; fac
ial ne
rve t
rans
pose
d; gr
eates
t risk
of fa
cial
ne
rve p
alsy &
CSF
leak
17,2
4,49
comb
ined‡
ant +
pst p
etros
al ap
proa
ch; m
axim
ized p
etrou
s bon
e res
ectio
n w/
pr
eser
ved h
earin
gea
rly de
scrip
tion o
f con
cept
per H
akub
a et a
l.20; c
ombin
ation
pre-
serv
ing la
byrin
th pe
r Cho
& A
l-Mef
ty8
* an
t = an
terior
; lab =
laby
rinth
ectom
y; pe
tro =
petro
secto
my; p
st =
poste
rior;
SS =
sigm
oid si
nus;
sup =
supe
rior.
† We inte
ntionally d
isting
uish a
pproaches s
uch a
s the traditio
nal in
fraten
torial transla
byrinthine
approach from
the “petro
sal transla
byrinthine
” approach. Th
e latter
specific
ally imp
licate
s an e
xpanded,
comb
ined s
upra
tentor
ial-in
fraten
torial
expo
sure
affo
rded
by se
ction
ing th
e sup
erior
petro
sal s
inus a
nd te
ntoriu
m an
d mob
ilizing
a sk
eleton
ized s
igmoid
sinu
s.‡
Olde
r stu
dies r
eferre
d to a
ll petr
osal
appr
oach
es as
“com
bined
” give
n the
comb
ined s
upra
tentor
ial-in
fraten
torial
expo
sure
they
affo
rd.49
Mod
ern r
epor
ts us
e the
term
“com
bined
” to re
fer to
a co
mbina
-tio
n of a
nterio
r and
poste
rior p
etros
al ap
proa
ches
, typ
ically
in an
effo
rt to
maxim
ize bo
ne re
secti
on bu
t pre
serv
e hea
ring.
8,11,1
7
B. A. Gross et al.
4 Neurosurg Focus / Volume 33 / August 2012
achieved. To provide a more expansive exposure of the brainstem and potentially improve the ability to com-pletely resect larger CMs, petrosal approaches were ap-plied to brainstem CMs, as initially described in 1992 by Spetzler et al.49 These applications continue in the most modern series of brainstem CMs13,21,27 and have also been extended to a broad range of cerebrovascular lesions, in-cluding large basilar trunk aneurysms,4,9,46 arteriovenous malformations,28,49 and dural arteriovenous fistulas.10,26,35 Although some are skeptical of petrosal approaches to brainstem CMs,5 the ventral exposure that these routes provide cannot be paralleled by the retrosigmoid approach or its combination with a subtemporal approach. Much of the skepticism stems from concerns of greater rates of postoperative complications including cranial nerve defi-cits and CSF leaks. As we demonstrate, this may be the case for more extensive posterior petrosal approaches, but the traditional anterior petrosal and posterior petrosal ret-rolabyrinthine approaches have lower complication rates comparable with those of other approaches. This may be confounded in part by relatively smaller CMs being managed using less extensive approaches. However, as we demonstrate, much of the morbidity after the extend-ed petrosal approaches is in the form of facial weakness, hearing loss, and/or CSF leakage (approach related).
In a recent comprehensive review of the literature in-corporating 52 surgical series and 821 brainstem CMs, early postoperative morbidity was reported to range from 29% to 67%, with permanent worsening in 14% of the cases.15 This does not significantly differ from our over-all findings in 50 cases treated via petrosal approaches: there was a 30% early morbidity rate and 14% perma-nent morbidity rate. Importantly, these rates decreased
to 12% each for the Kawase approach31 and to 25% and 4% for the standard posterior petrosal retrolabyrinthine approach, respectively. These results reinforce both the feasibility and safety of these approaches in experienced hands. A comparison with results for more extensive pos-terior petrosal approaches illustrates an already-known maxim: extended approaches are accompanied by higher rates of CSF leakage and cranial nerve morbidity. Not surprisingly, in the evolution of petrosal approaches to brainstem CMs, the authors of most modern series have described the application of the standard anterior or pos-terior petrosal approaches to these lesions,13,21,27 avoiding extended approaches to balance morbidity and adequate exposure.
The modern posterior petrosal approach, originally described by Al-Mefty et al.,3 has met with considerable success in the treatment of a wide variety of skull base lesions.8,17,32,33 Following a temporooccipital craniotomy, a mastoidectomy is performed, and meticulous drilling of the lateral petrous bone is performed to skeletonize the semicircular canals. Importantly, the sigmoid sinus should also be skeletonized over a generous segment. This is crucial in allowing for the sinus to be mobilized after dividing the tentorium and superior petrosal sinus. It is this maneuver that allows for a wide, ventral, supra- and infratentorial exposure, providing a shorter, more di-rect line of attack to ventral pontine lesions such as CMs. Importantly, the temporal lobe and dural venous sinuses are retracted as one unit, mitigating the risk to the vein of Labbé, as they are retracted separately in combined subtemporal-retrosigmoid approaches.33 Working around and preserving important associated DVAs is more fea-sible. As illustrated in the report of Kashimura et al.,30 as
TABLE 2: Brainstem CMs resected via the anterior petrosal approach*
Authors & YearAge (yrs),
Sex Presentation Resection Results
MacDonald et al., 1998 41, F HP improvedBertalanffy et al., 2002 22, F intact complete stable, no complicationsSaito et al., 2002 58, M HP, V, ataxia complete improved, no complicationsKashimura et al., 2006 64, F HP, ataxia complete improvedSteiger et al., 2006† 53, F VII complete no complications, improved
38, F “multiple deficits” partial worse hearing45, F V, ataxia complete improved
François et al., 2010 21, F HP, V–VII complete improved32, F HP, V, VI, IX, ataxia partial improved46, F HP, V–VII, ataxia complete improved22, F HP, V, VI complete improved70, F V, VI complete hearing loss27, F HP, V, VI, VIII, IX, ataxia partial improved
Ichinose et al., 2010 50, M HP complete improved64, F HP complete improved43, F HP complete improved
present study 54, M VI, X, ataxia complete improved
* Roman numerals denote deficits of the respective cranial nerve. Abbreviation: HP = hemiparesis.† Intradural petrous apicectomy.
Neurosurg Focus / Volume 33 / August 2012
Petrosal approaches for cavernomas
5
innovative imaging modalities allow for the demonstra-tion of white matter tracts, the location of their displace-ment can help dictate the best approach to the lesion. In the case they present, the white matter tract displacement helped dictate a preferable posterior petrosal approach to the lesion. They successfully resected the CM using this approach without complication.30
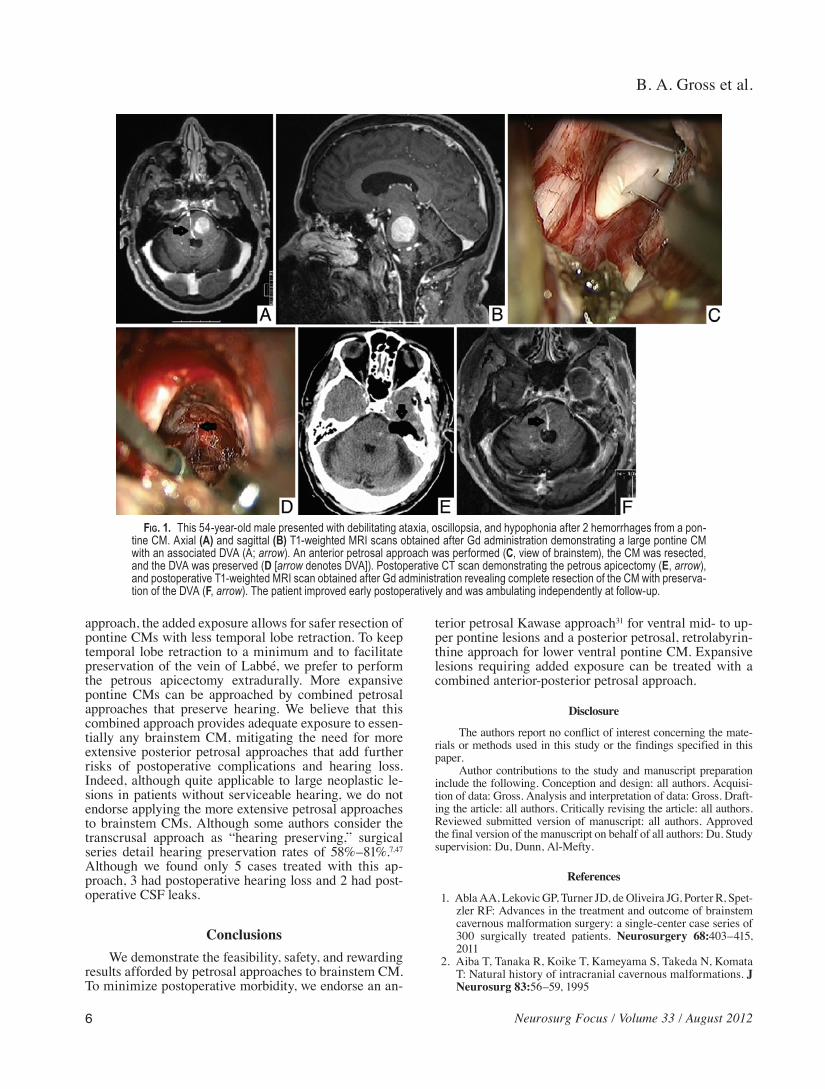
The anterior petrosal approach has also been applied with considerable success in the resection of brainstem CMs (Fig. 1 and Video 1).13,36
VIdeo 1. Video documenting the anterior petrosal approach to a brainstem CM. Click here to view with Media Player. Click here to view with Quicktime.
A logical inferior extension to the traditional middle fossa
TABLE 3: Brainstem CM resected via the posterior petrosal approach*
Authors & Year Age (yrs), Sex Presentation Resection Results
Spetzler et al., 1992 23, F V, dysmetria complete no complications39, M V–IX, ataxia complete no complications32, M HP, VII, XII complete no complications48, M V, VII, VIII complete no complications
King et al., 1993 16, M HP complete improved32, M HP, V complete improved
Oiwa et al., 2002 41, F HP, VI–VIII complete improved, no complications50, F ataxia complete stable, no complications
Viñas et al., 2002 46, F HP wound infection56, M HP postop MI45, F HP no complications38, M HP temporary CND
Seifert et al., 2003 28, M complete transient hearing loss55, F complete CSF leak41, F complete no complications23, M complete transient worse tetraparesis
Hauck et al., 2010 14, F HP, CND, ataxia complete stable, no complications31, F HP, CND complete improved, no complications32, F ataxia complete improved, no complications34, F HP, CND, ataxia complete stable, no complications37, F HP, CND complete stable, no complications47, F HP, CND complete improved, CSF leak59, M CND complete improved, no complications66, F CND, ataxia complete improved, no complications72, F HP, CND, ataxia complete hearing loss, wound infection
present study 22, M HP, VI, VII partial transient worse VII19, M† HP, V, VII complete improved
* Roman numerals denote deficits of the respective cranial nerve. Abbreviations: CND = cranial nerve deficit; MI = myocardial infarction. † Described in a prior report by Klimo et al.
TABLE 4: Brainstem CM resected via extended posterior petrosal approaches*
Authors & YearAge (yrs),
Sex Presentation Extension Resection Results
Ziyal et al., 1999 55, F V–VIII lab complete trans VI, permanent VIIShehab et al., 2001 38, F VI, ataxia partial lab mild hearing loss
44, F V, VI mild hearing loss, trans V, VII25, F VI–VIII, ataxia CSF leak30, F V, ataxia no complications
Brandt et al., 2010 26, M partial lab complete hearing loss, V, CSF leak
* Roman numerals denote deficits of the respective cranial nerves. Abbreviation: trans = transient.
approach, the added exposure allows for safer resection of pontine CMs with less temporal lobe retraction. To keep temporal lobe retraction to a minimum and to facilitate preservation of the vein of Labbé, we prefer to perform the petrous apicectomy extradurally. More expansive pontine CMs can be approached by combined petrosal approaches that preserve hearing. We believe that this combined approach provides adequate exposure to essen-tially any brainstem CM, mitigating the need for more extensive posterior petrosal approaches that add further risks of postoperative complications and hearing loss. Indeed, although quite applicable to large neoplastic le-sions in patients without serviceable hearing, we do not endorse applying the more extensive petrosal approaches to brainstem CMs. Although some authors consider the transcrusal approach as “hearing preserving,” surgical series detail hearing preservation rates of 58%–81%.7,47 Although we found only 5 cases treated with this ap-proach, 3 had postoperative hearing loss and 2 had post-operative CSF leaks.
ConclusionsWe demonstrate the feasibility, safety, and rewarding
results afforded by petrosal approaches to brainstem CM. To minimize postoperative morbidity, we endorse an an-
terior petrosal Kawase approach31 for ventral mid- to up-per pontine lesions and a posterior petrosal, retrolabyrin-thine approach for lower ventral pontine CM. Expansive lesions requiring added exposure can be treated with a combined anterior-posterior petrosal approach.
Disclosure
The authors report no conflict of interest concerning the mate-rials or methods used in this study or the findings specified in this paper.
Author contributions to the study and manuscript preparation include the following. Conception and design: all authors. Acquisi-tion of data: Gross. Analysis and interpretation of data: Gross. Draft-ing the article: all authors. Critically revising the article: all authors. Reviewed submitted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Du. Study supervision: Du, Dunn, Al-Mefty.
References
1. Abla AA, Lekovic GP, Turner JD, de Oliveira JG, Porter R, Spet-zler RF: Advances in the treatment and outcome of brainstem cavernous malformation surgery: a single-center case series of 300 surgically treated patients. Neurosurgery 68:403–415, 2011
2. Aiba T, Tanaka R, Koike T, Kameyama S, Takeda N, Komata T: Natural history of intracranial cavernous malformations. J Neurosurg 83:56–59, 1995
Fig. 1. This 54-year-old male presented with debilitating ataxia, oscillopsia, and hypophonia after 2 hemorrhages from a pon-tine CM. Axial (A) and sagittal (B) T1-weighted MRI scans obtained after Gd administration demonstrating a large pontine CM with an associated DVA (A; arrow). An anterior petrosal approach was performed (C, view of brainstem), the CM was resected, and the DVA was preserved (D [arrow denotes DVA]). Postoperative CT scan demonstrating the petrous apicectomy (E, arrow), and postoperative T1-weighted MRI scan obtained after Gd administration revealing complete resection of the CM with preserva-tion of the DVA (F, arrow). The patient improved early postoperatively and was ambulating independently at follow-up.
Neurosurg Focus / Volume 33 / August 2012
Petrosal approaches for cavernomas
7
3. Al-Mefty O, Fox JL, Smith RR: Petrosal approach for petro-clival meningiomas. Neurosurgery 22:510–517, 1988
4. Aziz KM, van Loveren HR, Tew JM Jr, Chicoine MR: The Kawase approach to retrosellar and upper clival basilar aneu-rysms. Neurosurgery 44:1225–1236, 1999
5. Bertalanffy H, Benes L, Miyazawa T, Alberti O, Siegel AM, Sure U: Cerebral cavernomas in the adult. Review of the lit-erature and analysis of 72 surgically treated patients. Neuro-surg Rev 25:1–55, 2002
6. Bochenek Z, Kukwa A: An extended approach through the middle cranial fossa to the internal auditory meatus and the cerebello-pontine angle. Acta Otolaryngol 80:410–414, 1975
7. Brandt MG, Poirier J, Hughes B, Lownie SP, Parnes LS: The transcrusal approach: a 10-year experience at one Canadian center. Neurosurgery 66:1017–1022, 2010
8. Cho CW, Al-Mefty O: Combined petrosal approach to petro-clival meningiomas. Neurosurgery 51:708–718, 2002
9. Day JD, Fukushima T, Giannotta SL: Cranial base approaches to posterior circulation aneurysms. J Neurosurg 87:544–554, 1997
10. De Jesús O, Rosado JE: Tentorial dural arteriovenous fistula obliterated using the petrosal approach. Surg Neurol 51:164–167, 1999
11. Erkmen K, Pravdenkova S, Al-Mefty O: Surgical management of petroclival meningiomas: factors determining the choice of approach. Neurosurg Focus 19(2):E7, 2005
12. Ferroli P, Sinisi M, Franzini A, Giombini S, Solero CL, Broggi G: Brainstem cavernomas: long-term results of microsurgical resection in 52 patients. Neurosurgery 56:1203–1214, 2005
13. François P, Ben Ismail M, Hamel O, Bataille B, Jan M, Velut S: Anterior transpetrosal and subtemporal transtentorial ap-proaches for pontine cavernomas. Acta Neurochir (Wien) 152: 1321–1329, 2010
14. Graham MD: Surgical exposure of the facial nerve indications and techniques. J Laryngol Otol 89:557–575, 1975
16. Gross BA, Lin N, Du R, Day AL: The natural history of in-tracranial cavernous malformations. Neurosurg Focus 30(6): E24, 2011
17. Haddad GF, al-Mefty O: The road less traveled: transtemporal access to the CPA. Clin Neurosurg 41:150–167, 1994
18. Hafez A, Nader R, Al-Mefty O: Preservation of the superior petrosal sinus during the petrosal approach. Technical note. J Neurosurg 114:1294–1298, 2011
19. Hakuba A, Nishimura S, Jang BJ: A combined retroauricular and preauricular transpetrosal-transtentorial approach to cli-vus meningiomas. Surg Neurol 30:108–116, 1988
20. Hakuba A, Nishimura S, Tanaka K, Kishi H, Nakamura T: Clivus meningioma: six cases of total removal. Neurol Med Chir (Tokyo) 17:63–77, 1977
21. Hauck EF, Barnett SL, White JA, Samson D: The presigmoid approach to anterolateral pontine cavernomas. Clinical ar-ticle. J Neurosurg 113:701–708, 2010
23. Horgan MA, Anderson GJ, Kellogg JX, Schwartz MS, Spektor S, McMenomey SO, et al: Classification and quantification of the petrosal approach to the petroclival region. J Neurosurg 93:108–112, 2000
24. House WF, Hitselberger WE: The transcochlear approach to the skull base. Arch Otolaryngol 102:334–342, 1976
25. Huang AP, Chen JS, Yang CC, Wang KC, Yang SH, Lai DM, et al: Brain stem cavernous malformations. J Clin Neurosci 17:74–79, 2010
26. Hwang G, Kang HS, Oh CW, Kwon OK: Surgical obliteration in superior petrosal sinus dural arteriovenous fistula. J Ko-rean Neurosurg Soc 49:222–225, 2011
roll retractor for surgical resection of brainstem cavernomas. World Neurosurg 73:520–522, 2010
28. Ishii N, Ishii R, Yoshii I, Sekihara Y, Suzuki Y, Hirano K, et al: Resection of arteriovenous malformation in the middle cerebellar peduncle by a posterior transpetrosal approach: illustration of a case and correlative microsurgical anatomy. Surg Neurol 64:50–54, 2005
29. Jenkins HA, Fisch U: The transotic approach to resection of difficult acoustic tumors of the cerebellopontine angle. Am J Otol 2:70–76, 1980
30. Kashimura H, Inoue T, Ogasawara K, Ogawa A: Pontine cavernous angioma resected using the subtemporal, anterior transpetrosal approach determined using three-dimensional anisotropy contrast imaging: technical case report. Neuro-surgery 58 (1 Suppl):ONS-E175, 2006
31. Kawase T, Toya S, Shiobara R, Mine T: Transpetrosal ap-proach for aneurysms of the lower basilar artery. J Neurosurg 63:857–861, 1985
32. King WA, Black KL, Martin NA, Canalis RF, Becker DP: The petrosal approach with hearing preservation. J Neurosurg 79:508–514, 1993
33. Klimo P Jr, Browd SR, Pravdenkova S, Couldwell WT, Walker ML, Al-Mefty O: The posterior petrosal approach: technique and applications in pediatric neurosurgery. Clinical article. J Neurosurg Pediatr 4:353–362, 2009
34. Kondziolka D, Lunsford LD, Kestle JR: The natural history of cerebral cavernous malformations. J Neurosurg 83:820–824, 1995
35. Lewis AI, Rosenblatt SS, Tew JM Jr: Surgical management of deep-seated dural arteriovenous malformations. J Neurosurg 87:198–206, 1997
36. MacDonald JD, Antonelli P, Day AL: The anterior subtempo-ral, medial transpetrosal approach to the upper basilar artery and ponto-mesencephalic junction. Neurosurgery 43:84–89, 1998
37. Moriarity JL, Wetzel M, Clatterbuck RE, Javedan S, Shep-pard JM, Hoenig-Rigamonti K, et al: The natural history of cavernous malformations: a prospective study of 68 patients. Neurosurgery 44:1166–1173, 1999
38. Morrison AW, King TT: Experiences with a translabyrinthine-transtentorial approach to the cerebellopontine angle. Techni-cal note. J Neurosurg 38:382–390, 1973
39. Ohue S, Fukushima T, Kumon Y, Ohnishi T, Friedman AH: Surgical management of brainstem cavernomas: selection of approaches and microsurgical techniques. Neurosurg Rev 33:315–324, 2010
40. Oiwa Y, Nakai K, Masaki Y, Masuo O, Kuwata T, Moriwaki H, et al: Presigmoid approach for cavernous angioma in the pons—technical note. Neurol Med Chir (Tokyo) 42:91–98, 2002
41. Porter PJ, Willinsky RA, Harper W, Wallace MC: Cerebral cavernous malformations: natural history and prognosis after clinical deterioration with or without hemorrhage. J Neuro-surg 87:190–197, 1997
42. Saito N, Sasaki T, Chikui E, Yuyama R, Kirino T: Anterior transpetrosal approach for pontine cavernous angioma—case report. Neurol Med Chir (Tokyo) 42:272–274, 2002
43. Samii M, Ammirati M, Mahran A, Bini W, Sepehrnia A: Sur-gery of petroclival meningiomas: report of 24 cases. Neuro-surgery 24:12–17, 1989
44. Samii M, Eghbal R, Carvalho GA, Matthies C: Surgical man-agement of brainstem cavernomas. J Neurosurg 95:825–832, 2001
45. Scott RM: Brain stem cavernous angiomas in children. Pedi-atr Neurosurg 16:281–286, 1990–1991
46. Seifert V, Raabe A, Zimmermann M: Conservative (laby-rinth-preserving) transpetrosal approach to the clivus and petroclival region—indications, complications, results and lessons learned. Acta Neurochir (Wien) 145:631–642, 2003
B. A. Gross et al.
8 Neurosurg Focus / Volume 33 / August 2012
47. Sekhar LN, Schessel DA, Bucur SD, Raso JL, Wright DC: Par-tial labyrinthectomy petrous apicectomy approach to neoplas-tic and vascular lesions of the petroclival area. Neurosurgery 44:537–552, 1999
49. Spetzler RF, Daspit CP, Pappas CTE: The combined supra- and infratentorial approach for lesions of the petrous and clival regions: experience with 46 cases. J Neurosurg 76: 588–599, 1992
Address correspondence to: Rose Du, M.D., Ph.D., Department of Neurological Surgery, Brigham and Women’s Hospital and Harvard Medical School, 75 Francis Street, Boston, Massachusetts 02115. email: [email protected].