Can the cricoid cartilage be ‘tilted’? A literature
review and pilot perceptual study of the extrinsic
muscles of the larynx
Jamie Read, February 2017, London
Introduction
There has been both debate and confusion around the ability of a singer to manipulate the position of the cricoid cartilage whilst singing. Some teachers and researchers, most notably Jo Estill, maintain that it is both possible and desirable to ‘tilt’ the cricoid cartilage backwards in Belt quality singing (Estill, 1988). Others question whether there is musculature capable of achieving this movement and in any case whether it would have any effect on the sound. This paper will look at the function of the extrinsic muscles of the larynx and will focus, in the form of a literature review, on evidence both for and against the muscular capability of singers to manipulate the cricoid cartilage. The author also undertook a short pilot perceptual study of the movement of the cricoid cartilage with 7 singers, the outcome of which when combined with the literature review suggests that such a movement is indeed possible, although the advantages or otherwise of doing so are not within the remit of this study. Literature Review - The Extrinsic Muscles of the Larynx The extrinsic muscles of the larynx which are capable of affecting the voice may be divided into 3 categories: Suprahyoid (laryngeal raising); Infrahyoid (laryngeal lowering); and, Constrictors (swallowing and resonance). These large muscles can help to determine the gross relations between the thyroid and cricoid cartilages (Vilkman et al 1996), whereas the intrinsic muscles control the finer adjustments of the vocal folds. Each of these categories includes several muscles and groups of muscles, many of which are involved in swallowing as well as phonation. Suprahyoid Muscles The suprahyoids extend from the hyoid to the base of the tongue and include the stylohyoid,
mylohyoid, geniohyoid and digastric. The latter three also help to lower the jaw (mandible) when the hyoid bone is stabilised by the Infrahyoid muscle group (Leborgne and Rosenberg, 2014). Infrahyoid Muscles The infrahyoids, by contrast, help to lower the larynx for swallowing and phonation. These include the sternohyoid, omohyoid, sternothyroid and thyrohyoid muscles. Since the classical voice setup is widely considered to require a lowered laryngeal position (Kirkpatrick, 2009), these muscles long been associated with singing, although it is worth noting that a low larynx can make it more laborious for the vocal folds to reach extremes of high pitch (Titze, 1993). Constrictors The constrictor muscles are principally muscles of swallowing, and consist of the superior, middle and inferior constrictors. These muscles constrict in sequence during swallowing, but also have the capability to affect the resonant properties of the vocal tract, creating extra brightness and the so-called ‘singer’s formant’ (Sundberg, 1988). Other Important Extrinsic Muscles in Singing Aside from the extrinsic laryngeal muscles, there are other important muscles which have a direct effect on the voice. The cricothyroid muscle, for example, contracts to lengthen the vocal folds and is therefore an important part of the pitching mechanism when working in opposition to the intrinsic thyroarytenoid muscles (Sonninen et al, 1998). The tongue, which also acts upon the larynx, is a complex structure with several attachments to the larynx and with an important role in vowel shaping and formant tuning (Bunch Dayme, 2005; Miller & Schutte, 1981). Figure 1 shows the muscles of the tongue and the relationships that they have to other extrinsic muscles in the suprahyoid group, such as the geniohyoid and the digastric muscles. Also shown in figure 1 is the soft palate (or velum) which opens and closes the nasopharyngeal port, allowing sound to resonate in the nasal cavity, the oral
PGCERT in Applied Professional Practice (Vocal Pedagogy) – Voice Workshop UK / Cardiff Metropolitan University
cavity, or a combination of both (Miller, 1996). Whilst not an extrinsic muscle of the larynx, the velum is nonetheless important as a structure and has connections to the tongue in the palatoglossus muscle and, by extension, an effect on the larynx of the vocal tract, and is thus worthy of mention.
Figure 1 – The muscles of the tongue (Bunch Dayme, 2005)
It has been noted by Sonninen, Hurme and Laukkanen in their 1998 study of the External Frame Function of the larynx that at times the muscles associated with singing act in an isotonic way (shortening in length when they contract), and at other times they act in an isometric way (contracting without shortening, usually to stabilise against the contraction of opposing muscles). This study, which used radiographic observations of a female singer phonating in 3 modes (Piano ‘Covered’, Forte ‘Covered’ and Forte ‘Open) also noted that the vertical and sagittal movements of the larynx had a complex relationship to both pitch and voice quality, with the extrinsic ‘frame function’ muscles having an effect on both. New technology is increasingly making it easier to get a clear visualisation and evaluation of laryngeal biomechanics in phonation. In a recent pilot study using three-dimensional imaging of singers’ larynges, independent ‘tilting’ of the cricoid cartilage (and also of the arytenoid cartilages) was observed (Vorik et al, 2016). In this pilot study, 10 professional female singers were scanned by 3D imaging equipment to monitor the movements of the major laryngeal cartilages (thyroid, cricoid and cuneiform, or arytenoid cartilages) at a mid-range speaking fundamental frequency (F₀), and then at one octave above F₀ and two octaves above F₀. It was noted by Vorik et al that there was a backward
tilting of the cricoid cartilage in the pitch range between F₀ + 1 octave and F₀ + 2 octaves. In order to establish how this movement may occur, let us consider figure 2 below.
Figure 2 - Image from www.ThoracicKey.com, Themes, 2017
In figure 2, we can see the inferior constrictor muscle separated into two parts. The top portion (above Killian’s dehiscence) is termed the thyropharyngeus, whilst the lower portion, which arises directly from the cricoid cartilage, is labelled the cricopharyngeus (Jiang et al, 2017). The principal function of the cricopharyngeus is as part of the swallow mechanism (Cook, 1993), however the role of the pharyngeal constrictors in formant tuning and larynx raising are also well-documented (Sundberg, 1988; Yanigsawa et al, 1989; Leborgne and Rosenberg, 2014) and so we know that these muscles are active in phonation. The cricopharyngeus muscle has the capability to draw the cricoid cartilage towards the cervical spine (Sonninen et al, 1998), and the constrictor muscles as a group when contracted have the effect of raising the larynx. It is therefore possible to suggest that cricopharyngeus would be able to draw the cricoid cartilage backwards, especially as the larynx rises, which it has been widely observed to do in a belting quality (LeBorgne et al, 2009; Titze, 2016, Sundberg et al, 2010).
Pilot Perceptual Study – Exploring the Research Through Practical Work The author works extensively in the voice studio with musical theatre and pop performers, and for this short pilot study, 7 singers took part in perceptual studies of the movement of the cricoid cartilage and the engagement of the extrinsic muscles of the larynx. Of these 7 singers, 2 were male and 5 were female, ranging in age from 19 to 40. All were either professional singers or in vocational training as professional singers, and so can be classed as experienced, and all were able to produce both a belted and classical sound that they reported as safe and comfortable. All singers gave consent to take part in the pilot study. Method It is noted by the author that this is a pilot perceptual study, and that methods may be called into question. It is not possible to extrapolate clear scientific results from this pilot study, but it provides the worthwhile opportunity to experience physically the evidence found in researching the literature review portion of this paper. Singers undertook a thorough warm-up, and were then taken through the following 3 exercises to try and ‘neutralise’ the laryngeal position (in other words, release any supra- or infrahyoid tensions that might affect the position of the larynx):
1. Breathe silently without any phonation or any effort in the breathing
2. Short massage of the larynx and surrounding muscles
3. Swallow, allowing the larynx to rise and fall naturally and comfortably to its neutral posture
Once these initial exercises had been completed, the author lightly palpated the larynx, to find the cricoid and begin to establish its position in relation to the thyroid. This was done with the singer in a seated position, with the head and neck in a neutral posture (looking neither up nor down) by lying the index finger vertically down the larynx, with the thyroid cartilage prominence in contact
with the middle section of the finger, the first knuckle joint of the finger lying the in cricothyroid space, and the tip of the finger and fingernail in contact with the cricoid cartilage. The remaining thumb and fingers lightly made contact with the muscles on either side of the larynx, predominantly the sternocleidomastoid and sternohyoid muscles (Figure 3). No pressure was applied and no manipulations were made. It should be noted that there are many methods of laryngeal palpation reviewed by Khoddami et al in 2015, with the method used by the author being a simple way of observing cartilage positions without grading associated muscle tensions and based loosely on the Roy et al method (1996).
Figure 3 – Palpation of the Larynx, photo of author
In this position, it is possible to feel the changing relationship between the thyroid and cricoid cartilages and by extension the size of the cricothyroid space. Singers were next asked to perform three simple tasks:
1. Breathe silently once again, so that the position of the larynx might be observed by the author ‘at rest’.
2. Sing a 5 note scale on an /ᴁ/ vowel, in a classical voice quality. The pitch range on this exercise was from E4 (329Hz) to B4 (493Hz) for the female singers, and A3 (220Hz) to E4 (329Hz) for the male singers. During this exercise, the author monitored the position of the thyroid and the cricoid cartilages and the relative size of the cricothyroid space.
3. Repeat the second exercise exactly as before, but this time in a belted quality. The pitch range remained the same as in the second exercise, and once again the
PGCERT in Applied Professional Practice (Vocal Pedagogy) – Voice Workshop UK / Cardiff Metropolitan University
author monitored the position the thyroid and the cricoid cartilages and the relative size of the cricothyroid space.
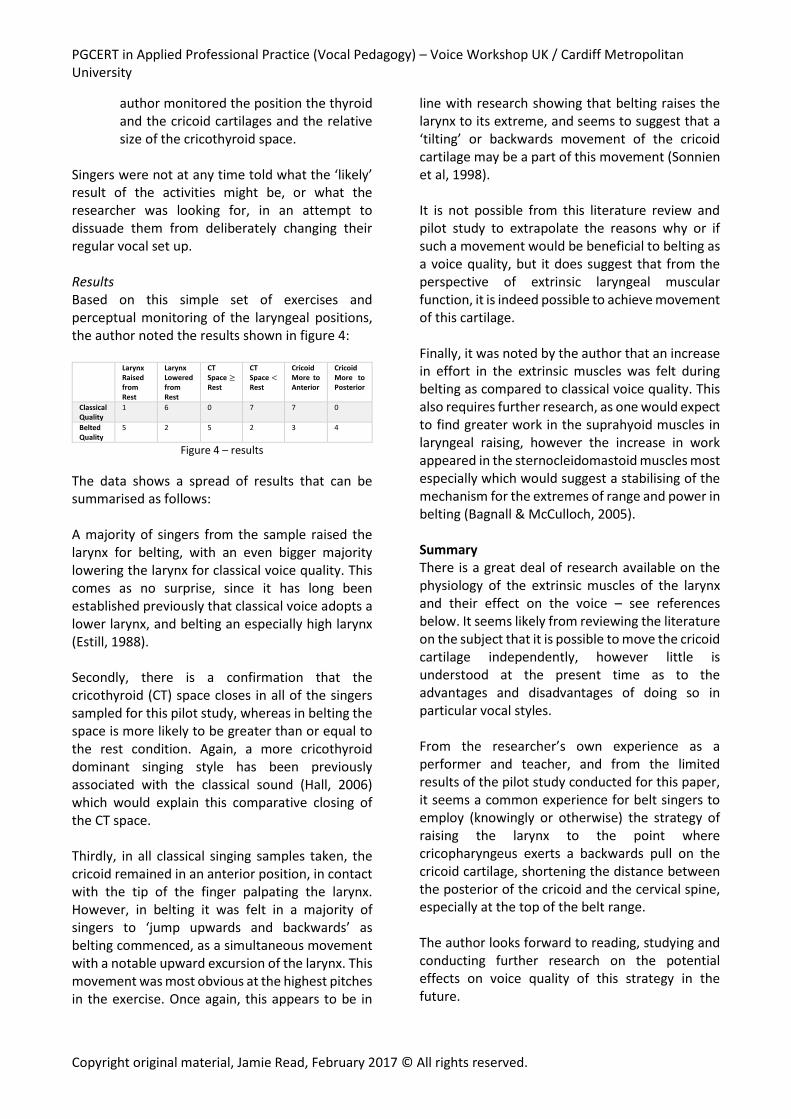
Singers were not at any time told what the ‘likely’ result of the activities might be, or what the researcher was looking for, in an attempt to dissuade them from deliberately changing their regular vocal set up. Results Based on this simple set of exercises and perceptual monitoring of the laryngeal positions, the author noted the results shown in figure 4:
Larynx Raised from Rest
Larynx Lowered from Rest
CT Space ≥ Rest
CT Space < Rest
Cricoid More to Anterior
Cricoid More to Posterior
Classical Quality
1 6 0 7 7 0
Belted Quality
5 2 5 2 3 4
Figure 4 – results
The data shows a spread of results that can be summarised as follows: A majority of singers from the sample raised the larynx for belting, with an even bigger majority lowering the larynx for classical voice quality. This comes as no surprise, since it has long been established previously that classical voice adopts a lower larynx, and belting an especially high larynx (Estill, 1988). Secondly, there is a confirmation that the cricothyroid (CT) space closes in all of the singers sampled for this pilot study, whereas in belting the space is more likely to be greater than or equal to the rest condition. Again, a more cricothyroid dominant singing style has been previously associated with the classical sound (Hall, 2006) which would explain this comparative closing of the CT space. Thirdly, in all classical singing samples taken, the cricoid remained in an anterior position, in contact with the tip of the finger palpating the larynx. However, in belting it was felt in a majority of singers to ‘jump upwards and backwards’ as belting commenced, as a simultaneous movement with a notable upward excursion of the larynx. This movement was most obvious at the highest pitches in the exercise. Once again, this appears to be in
line with research showing that belting raises the larynx to its extreme, and seems to suggest that a ‘tilting’ or backwards movement of the cricoid cartilage may be a part of this movement (Sonnien et al, 1998). It is not possible from this literature review and pilot study to extrapolate the reasons why or if such a movement would be beneficial to belting as a voice quality, but it does suggest that from the perspective of extrinsic laryngeal muscular function, it is indeed possible to achieve movement of this cartilage. Finally, it was noted by the author that an increase in effort in the extrinsic muscles was felt during belting as compared to classical voice quality. This also requires further research, as one would expect to find greater work in the suprahyoid muscles in laryngeal raising, however the increase in work appeared in the sternocleidomastoid muscles most especially which would suggest a stabilising of the mechanism for the extremes of range and power in belting (Bagnall & McCulloch, 2005). Summary There is a great deal of research available on the physiology of the extrinsic muscles of the larynx and their effect on the voice – see references below. It seems likely from reviewing the literature on the subject that it is possible to move the cricoid cartilage independently, however little is understood at the present time as to the advantages and disadvantages of doing so in particular vocal styles. From the researcher’s own experience as a performer and teacher, and from the limited results of the pilot study conducted for this paper, it seems a common experience for belt singers to employ (knowingly or otherwise) the strategy of raising the larynx to the point where cricopharyngeus exerts a backwards pull on the cricoid cartilage, shortening the distance between the posterior of the cricoid and the cervical spine, especially at the top of the belt range. The author looks forward to reading, studying and conducting further research on the potential effects on voice quality of this strategy in the future.
PGCERT in Applied Professional Practice (Vocal Pedagogy) – Voice Workshop UK / Cardiff Metropolitan University
References: Bagnall, A. and McCulloch, K. (2005). The Impact of Specific Exertion on the Efficiency and Ease of the Voice: A Pilot Study. Journal of Voice, 19(3), pp.384-390. Cook, I. (1993). Cricopharyngeal function and dysfunction. Dysphagia, 8(3), pp.244-251. Dayme, M. (2005). The performer's voice. 1st ed. New York: W.W. Norton, pp.94-97. DeLeo LeBorgne, W., Lee, L., Stemple, J. and Bush, H. (2010). Perceptual Findings on the Broadway Belt Voice. Journal of Voice, 24(6), pp.678-689. Edwin, R. (1998). Belting 101. Journal of Singing, 55(1), pp.53-55. Estill, J. (1988). Belting and Classical Voice Quality: Some Physiological Differences. Medical Problems of Performing Artists, 3, pp.37-43. Hall, K. (2006). Music theater vocal pedagogy and styles. 1st ed. Columbia: Columbia University. Jiang, N., Sung, C. and Damrose, E. (2017). Improvement in the Reflux Symptom Index Following Surgery for Cricopharyngeal Dysfunction. Journal of Voice, 31(1), pp.86-89. Khoddami, S., Ansari, N. and Jalaie, S. (2015). Review on Laryngeal Palpation Methods in Muscle Tension Dysphonia: Validity and Reliability Issues. Journal of Voice, 29(4), pp.459-468. Kirkpatrick, A. (2009). Chiaroscuro and the Quest for Optimal Resonance. Journal of Singing, 66(1), pp.15-21. Kmucha, S., Yanagisawa, E. and Estill, J. (1990). Endolaryngeal changes during high-intensity phonation videolaryngoscopic observations. Journal of Voice, 4(4), pp.346-354. Miller, R. (1996). The Velopharyngeal (Palatopharyngeal) Port During Singing. Journal of Singing, 53(1), pp.27-29. Popeil, L. (1999). Comparing Belt and Classical Techniques Using MRI and Video Fluoroscopy. Journal of Singing, 56(2), pp.27-29. Rosenberg, M. and LeBorgne, W. (2014). The vocal athlete. 1st ed. San Diego, Calif.: Plural Publishing, pp.8-9. Sonninen, A., Hurme, P. and Laukkanen, A. (1999). The external frame function in the control of pitch, register, and singing mode: Radiographic observations of a female singer. Journal of Voice, 13(3), pp.319-340. Sundberg, J. (1987). Vocal Tract Resonance in Singing. Journal of Singing, 44(4), pp.11-31. Sundberg, J., Thalén, M. and Popeil, L. (2012). Substyles of Belting: Phonatory and Resonatory Characteristics. Journal of Voice, 26(1), pp.44-50. Themes, U. (2017). Thoracic Key. [online] Thoracic Key. Available at: http://www.thoracickey.com [Accessed 1 Mar. 2017]. Titze, I. (1993). Raised Versus Lowered Larynx Singing. Journal of Singing, 50(2), pp.37-38. Titze, I. (2016). Belting and Trumpeting. Journal of Singing, 73(1), pp.53-54. Vilkman, E., Sonninen, A., Hurme, P. and Körkkö, P. (1996). External laryngeal frame function in voice production revisited: A review. Journal of Voice, 10(1), pp.78-92. Vorik, A., Unteregger, F., Zwicky, S., Schiwowa, J., Potthast, S. and Storck, C. (2017). Three-dimensional Imaging of High-resolution Computer Tomography of Singers' Larynges—A Pilot Study. Journal of Voice, 31(1), pp.115.e17-115.e21. Yanagisawa, E., Estill, J., Kmucha, S. and Leder, S. (1989). The contribution of aryepiglottic constriction to “ringing” voice quality—A videolaryngoscopic study with acoustic analysis. Journal of Voice, 3(4), pp.342-350.