30
Pharmaceutical Care in Asthma Omotola Morakinyo
| Date post: | 27-Dec-2015 |
| Category: |
Documents |
| Upload: | anne-obrien |
| View: | 217 times |
| Download: | 0 times |
Pharmaceutical Care in Asthma
Omotola Morakinyo
FLOW
• OVERVIEW OF ASTHMA
• IMPROVING ASTHMA MANAGEMENT
• INHALER DEVICES
• SOAP
• CASE STUDY
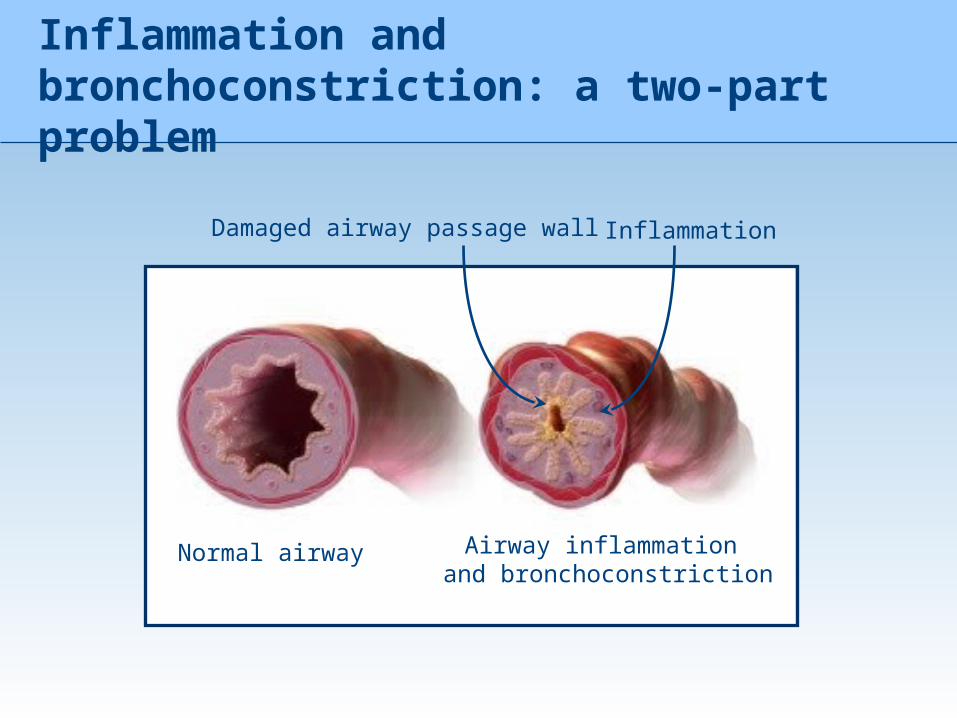
Inflammation and bronchoconstriction: a two-part problem
Normal airway Airway inflammation and bronchoconstriction
InflammationDamaged airway passage wall
Aims of treatment
People with asthma should:-Achieve and maintain control of symptoms-Prevent asthma exacerbations-Maintain normal activity levels, including exercise-Maintain pulmonary function as close to normal levels as possible
Asthma – a global healthcare issue
• Asthma is a worldwide problem• Approximately 300 million individuals are affected1
• Over the last 40 years there has been a sharp increase in the global prevalence, morbidity, mortality, and economic burden associated with asthma
• Asthma prevalence is expected to increase by 50% every decade
First, let’s define the terms
• ICS- Inhaled CorticoSteroid e.g Fluticasone propionate in Seretide• LABA- Long Acting Beta-2 Agonist e.g Salmeterol in Seretide• SABA- Short Acting Beta-2 Agonist e.g Salbutamol in Seretide• Daily ICS + Daily LABA e.g Fluticasone propionate + Salmeterol
(Seretide)• Theophylline SR- e.g in Franol• Oral corticosteroid e.g Prednisolone• LTRA – LeukoTriene Receptor Antagonist e.g Montelukast in Singulair,
Montiget.• GINA – Global INitiative for Asthma
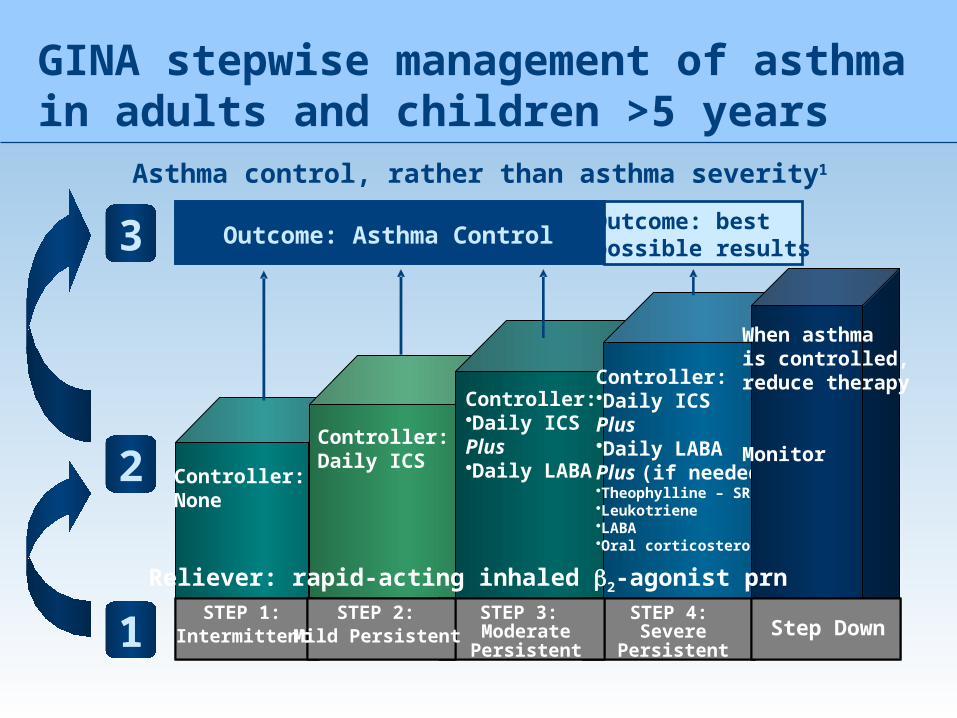
GINA stepwise management of asthma in adults and children >5 years
Asthma control, rather than asthma severity1
3
2
1STEP 1:
IntermittentSTEP 2:
Mild PersistentSTEP 4:
Severe Persistent
Outcome: Asthma Control
STEP 3:Moderate Persistent
Step down
Outcome: best possible results
Controller:None
Controller:Daily ICS
Controller:•Daily ICSPlus•Daily LABA
Controller:•Daily ICSPlus•Daily LABAPlus (if needed)•Theophylline – SR•Leukotriene•LABA•Oral corticosteroid
When asthma is controlled, reduce therapy
Monitor
Step Down
Reliever: rapid-acting inhaled b2-agonist prn
If a patient’s asthma is controlled, they should not experience asthma symptoms or exacerbations
• Exacerbations of asthma are episodes of progressive increase in shortness of breath, cough, wheezing, or chest tightness
• Severe exacerbations are potentially life-threatening and treatment requires close supervision
• GINA defines clinical control of asthma as involving no exacerbations
1. Global Initiative for Asthma (GINA): Global strategy for asthma management and prevention. Revised Edition 2007.
• The Global Initiative for Asthma (GINA) defines clinical control of asthma as:1
The goal of asthma management:guideline-defined control
1. Global Initiative for Asthma (GINA): Global strategy for asthma management and prevention. Revised Edition 2007.
• No (twice or less/week) daytime symptoms• No limitations of daily activities, including exercise• No nocturnal symptoms or awakening because of asthma• No (twice or less/week) need for reliever treatment• Normal or near-normal lung function• No exacerbations
Any symptoms of asthma are a sign of inflammation
• Inflammation in asthma patients can be present during symptom-free periods:1
• Symptoms resolve quickly. Inflammation, however, as measured by airway hyperresponsiveness, takes far longer1
• As chronic inflammation causes an increase in airway hyperresponsiveness, if the inflammation is not controlled, symptoms are likely to reoccur.
1. Woolcock AJ. Clin Exp Allergy Rev 2001; 1: 62–64.

The inhaler “buffet”
The large number of inhalers marketed itself creates problems for healthcare professionals and patients !!
Inhaler Techniques
Idealhaler The ideal inhaler
• Patient friendly
• 100% lung deposition
• Dose indicator
• Small
• Attractive
• Competely safe
• Inspiratory flow independent
• Easy to use
• Friendly to environment
• Discrete
• Inexpensive
• Moisture proof
• Multi-dose system
• etc..
Borgström L. Medicinskt Forum 1997; 4: 4-10
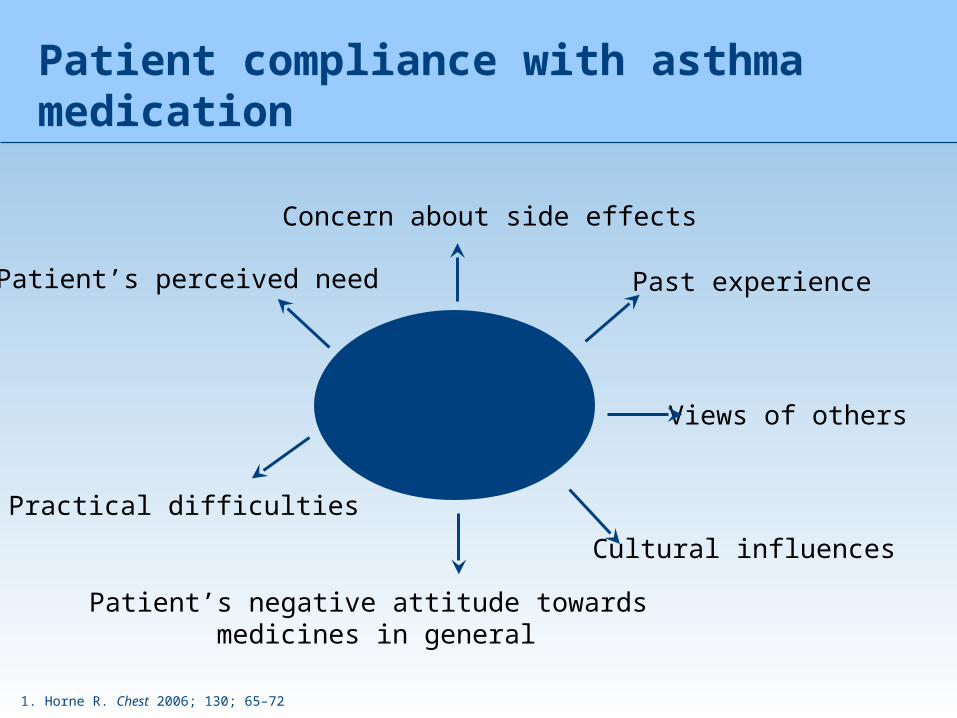
Patient compliance with asthma medication
1. Horne R. Chest 2006; 130; 65–72
PoorCompliance
Concern about side effects
Patient’s negative attitude towards medicines in general
Past experience
Views of others
Cultural influences
Practical difficulties
Patient’s perceived need
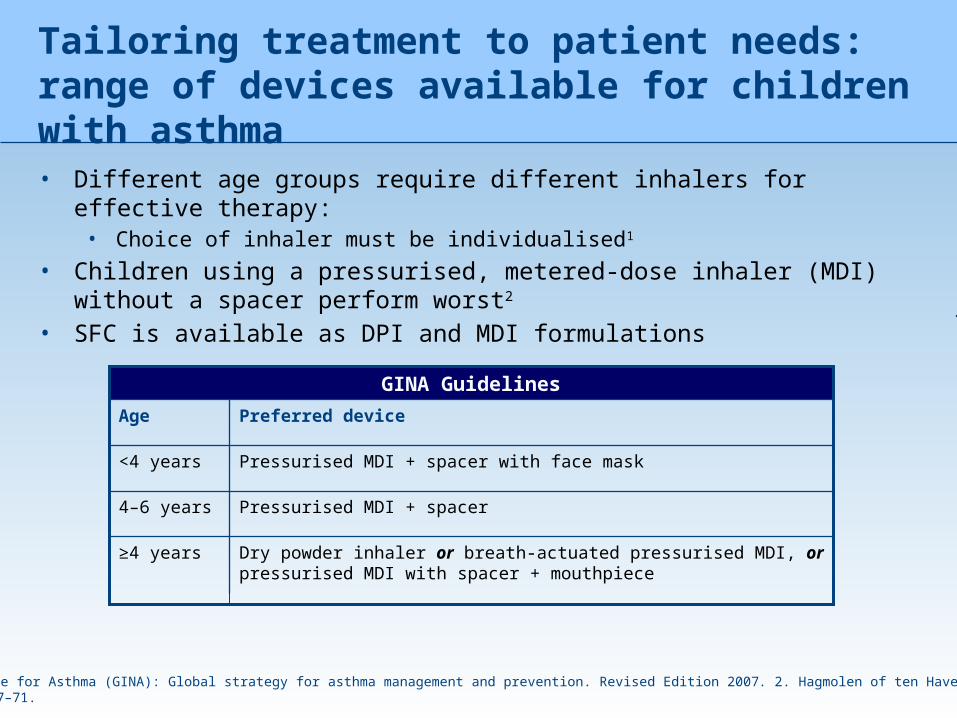
Tailoring treatment to patient needs: range of devices available for children with asthma
• Different age groups require different inhalers for effective therapy:• Choice of inhaler must be individualised1
• Children using a pressurised, metered-dose inhaler (MDI) without a spacer perform worst2
• SFC is available as DPI and MDI formulations
1. Global Initiative for Asthma (GINA): Global strategy for asthma management and prevention. Revised Edition 2007. 2. Hagmolen of ten Have W et al. J Asthma 2008; 45: 67–71.
Dry powder inhaler or breath-actuated pressurised MDI, or pressurised MDI with spacer + mouthpiece
≥4 years
Pressurised MDI + spacer4–6 years
Pressurised MDI + spacer with face mask<4 years
Preferred deviceAge
GINA Guidelines
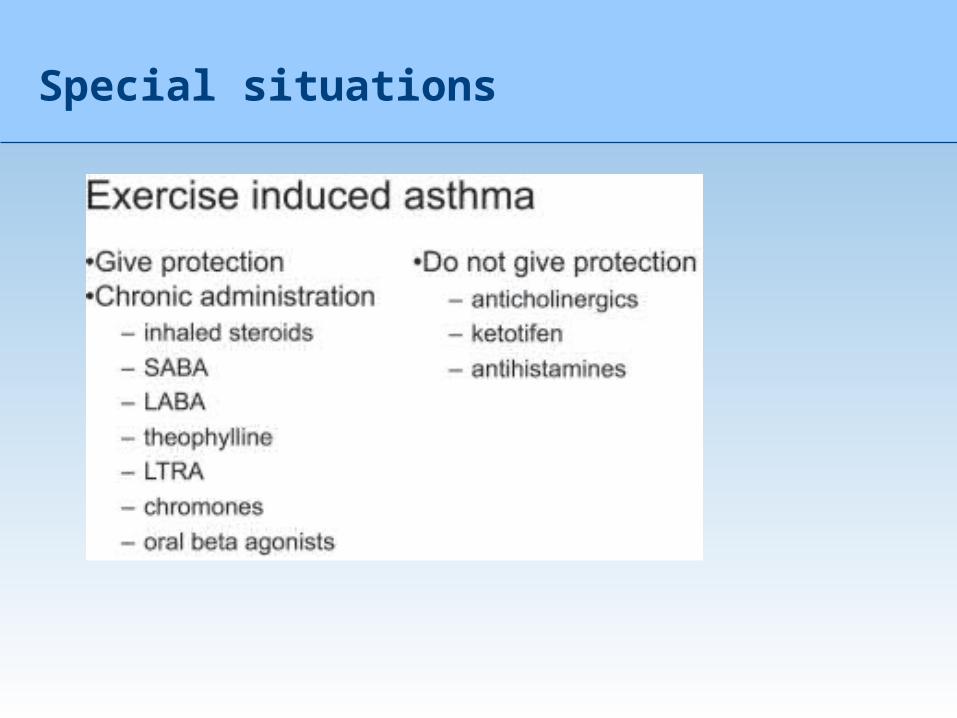
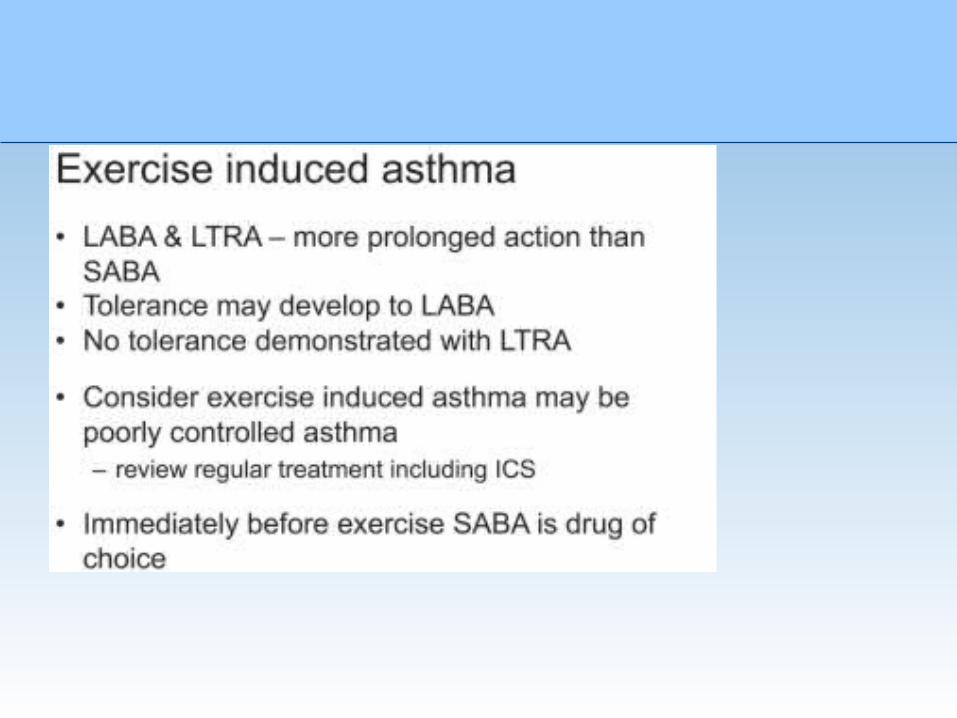
Special situations
Occupational asthma
• Remove precipitating factor• Treat as normal
Developing Pharmaceutical Care plan
• Step 1. Gathering Information• Step 2. Identifying Problems• Stop 3. Assessing Problems• Step 4. Developing the Plan• Step 5. Evaluating the Achievement of Outcomes
Gathering information
The pharmacist should gather both OBJECTIVE and SUBJECTIVE DATA
- an accurate medication history, including both prescription and nonprescription medications and the reasons the medications were prescribed or taken.
Vital signs
The pharmacist may have to obtain some information from the physician, such as laboratory test results and hospitalizations.
If so, the pharmacist should get written permission from the patient before soliciting this information. Once this information is compiled, the preparation of a PCP can begin.
Identifying drug therapy problems
• From the patient's medication profile, only one problem is evident: diagnosis of asthma. If applicable, other problem should also be listed.
• Subjective and objective findings correlated to the problem are listed. Subjective findings are those that the patient describes (e.g., 'I feel
• tired all the time, “I feel bloated,” or "I woke up coughing• Objective findings are those that can be observed or measured by the
pharmacist (e.g., patient appears tired, blood pressure is 180/105, pitting edema in ankles).
• The pharmacist would have the patient use a peak expiratory flow meter and record the results.
Assessing DTP
• The pharmacist analyzes and integrates the information gathered, draws conclusions in preparation for developing a patient-specific PCP. The pharmacist may first investigate the etiology of the factors that exacerbated the asthma. The pharmacist should attempt to determine if drugs (eg., aspirin, nonsteroidal anti-inflammatory agents, or beta-blockers) caused or exacerbated the asthma in the patient. Thus, the importance of an accurate and complete drug history becomes evident.
• Next, the pharmacist assesses the severity of the asthma.• This could be accomplished by determining the PEFR, examining
the patient's daily symptom and peak flow diary, or determining if the patient had been hospitalized and placed on steroids or nebulized.
Developing plan
• The pharmacist establishes goals linked to each of the patient's problems and specifies a course of action aimed at meeting each goal.
• Each goal (i.e., desired improvement) should be stated in terms of measurable outcomes that indicate the extent to which the particular problem has been resolved.
• Often, the patient has several problems, and the plan must be comprehensive enough to have a positive effect on the overall health of
the patient.
Evaluating the Achievement of Outcomes
• Outcomes must be meaningful, measurable, and manageable. Outcomes are specific, measurable indicators for the goals of treatment. Thus, they should be identified in the planning process.
• The outcomes for asthma include,• lower frequency and severity of acute exacerbations, • fewer physician office visits, • elimination of side effects, • PEFRs that never fall below 80% of previous personal-best predicted
rates, • fewer emergency department visits, and• maintenance of activities that enhance the patient's quality of life.
Documentation should include these components
• 1. Patient data such as name, medical record number, location, date of hospital admission (if applicable). age, sex, height, weight, known medication
• or other allergies, and medication history.• 2. Name of pharmacist(s) responsible for developing and implementing
the PCP.• 3. Patient problem(s) listed Individually in order of potential
pharmacotherapeutic impact (highest to lowest priority). Subjective and objective data that lead to identification of a specific problem and potential drug-related problems should also be included.
• 4. Date on which a patient problem is identified. Many diseases remain chronic throughout the patient's life. Problems such as urinary tract infection or upper respiratory tract infection usually resolve in 10 to 14 days.
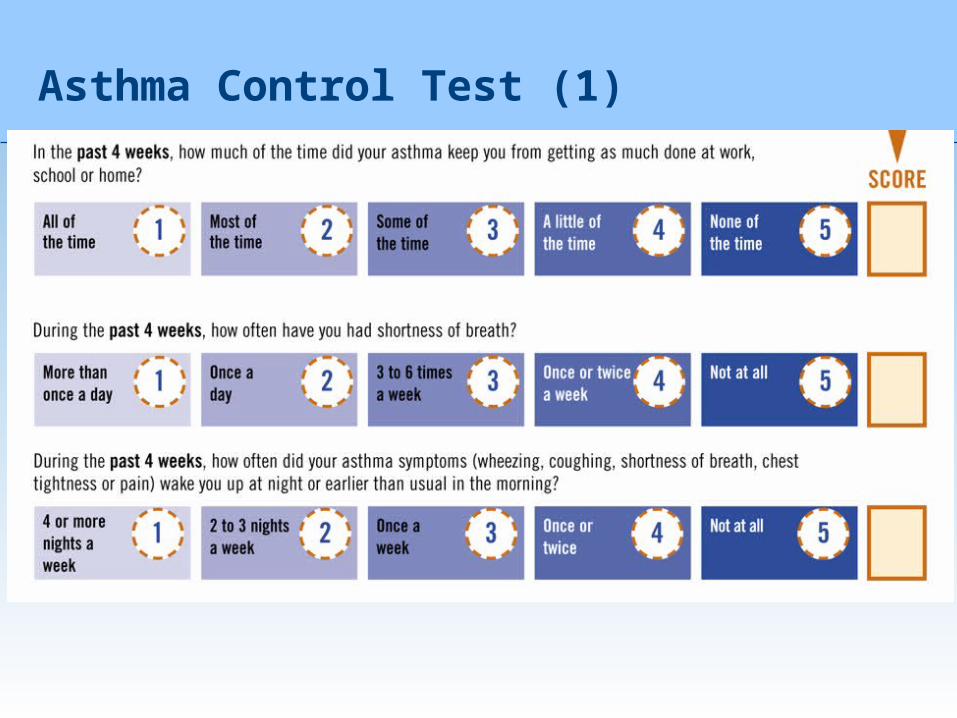
Asthma Control Test (1)
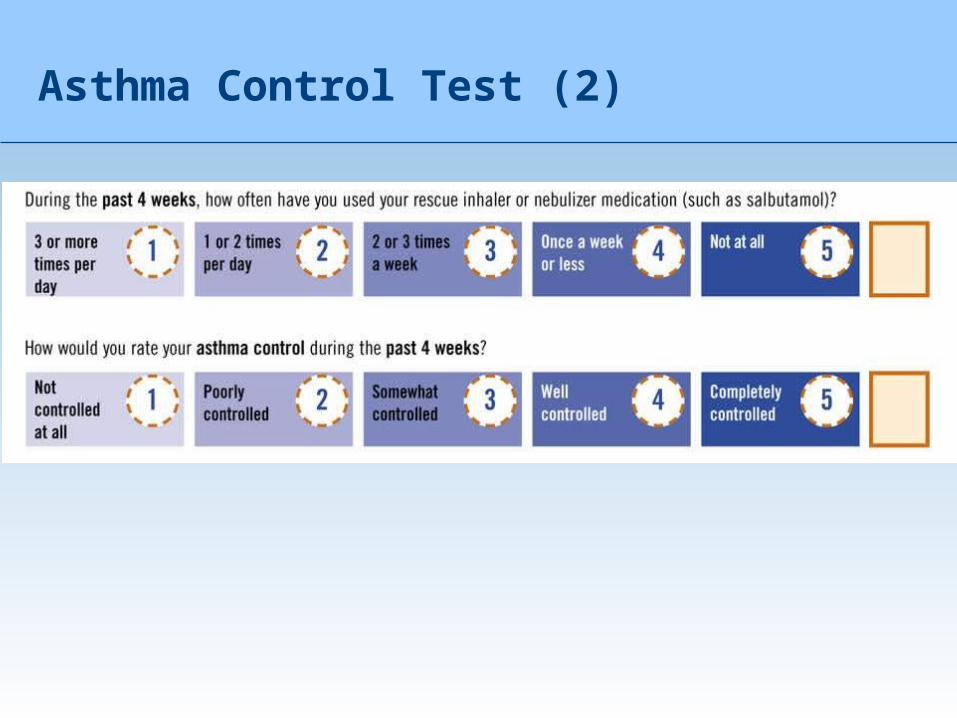
Asthma Control Test (2)

THANK YOU

















