Page 1
The audio portion of the conference may be accessed via the telephone or by using your computer's
speakers. Please refer to the instructions emailed to registrants for additional information. If you
have any questions, please contact Customer Service at 1-800-926-7926 ext. 10.
Presenting a live 90-minute webinar with interactive Q&A
Pharmaceutical Waste Management:
Compliance for Hospitals, Pharmacies,
and Other Healthcare Facilities Leveraging Recent Environmental Enforcement Actions
and Understanding Policy Shifts to Ensure Regulatory Compliance
Today’s faculty features:
THURSDAY, JULY 30, 2015
Gregory W. Blount, Partner, Troutman Sanders, Atlanta
Charlotte A. Smith, Senior Regulatory Advisor, WMSS PharmEcology Services, Houston
Darrell J. Oman, Program Manager – Consulting Services, Stericycle Environmental Solutions,
Blaine, Minn.
1pm Eastern | 12pm Central | 11am Mountain | 10am Pacific
Page 2
Tips for Optimal Quality
Sound Quality
If you are listening via your computer speakers, please note that the quality
of your sound will vary depending on the speed and quality of your internet
connection.
If the sound quality is not satisfactory, you may listen via the phone: dial
1-866-927-5568 and enter your PIN when prompted. Otherwise, please
send us a chat or e-mail [email protected] immediately so we can
address the problem.
If you dialed in and have any difficulties during the call, press *0 for assistance.
Viewing Quality
To maximize your screen, press the F11 key on your keyboard. To exit full screen,
press the F11 key again.
FOR LIVE EVENT ONLY
Page 3
Continuing Education Credits
In order for us to process your continuing education credit, you must confirm your
participation in this webinar by completing and submitting the Attendance
Affirmation/Evaluation after the webinar.
A link to the Attendance Affirmation/Evaluation will be in the thank you email
that you will receive immediately following the program.
For additional information about CLE credit processing call us at 1-800-926-7926
ext. 35.
FOR LIVE EVENT ONLY
Page 4
Program Materials
If you have not printed the conference materials for this program, please
complete the following steps:
• Click on the ^ symbol next to “Conference Materials” in the middle of the left-
hand column on your screen.
• Click on the tab labeled “Handouts” that appears, and there you will see a
PDF of the slides for today's program.
• Double click on the PDF and a separate page will open.
• Print the slides by clicking on the printer icon.
FOR LIVE EVENT ONLY
Page 5
Pharmaceutical Waste Management:
Compliance for Hospitals, Pharmacies, and
Other Healthcare Facilities
Gregory W. Blount, Esq., Troutman Sanders LLP
Charlotte A. Smith, R. Ph., M.S., WM Sustainability Services, PharmEcology Services
Darrell J. Oman, Stericycle Environmental Solutions
July 30, 2015
Page 6
Gregory W. Blount
Troutman Sanders LLP [email protected]
Pharmaceutical Waste Management
6
Page 7
Roadmap
7
Resource Conservation and Recovery Act
(RCRA) Basics
What is pharmaceutical waste?
Why are regulators concerned?
How do RCRA and state programs cover this
waste?
Recent Enforcement
Federal and state reform efforts
Page 8
RCRA Basics
Congress Enacted in 1976
Governs disposal of solid waste and hazardous waste; encourages waste minimization
Drafted for industrial facilities, but applicable to medical facilities and retail pharmacies.
Two types of Hazardous Waste: Characteristic – exhibit one of four traits
Toxicity, Ignitability, Reactivity, Corrosivity
Listed Wastes: P List (acute) and U List (toxic)
Regulated from Point of Generation through point of ultimate disposal.
8
Page 9
What is Pharmaceutical Waste?
May include dropped pills, compounding chemicals,
Warfarin containers, expired Tylenol, nicotine
replacement therapy, IV bags, vials, spill cleanup
materials, medicated shampoo and cough drops
Regulated by U.S. EPA and U.S. DEA
Small amount are RCRA Hazardous Waste
States may consider additional pharmaceuticals as
hazardous waste (e.g., MN Lethality)
CA Medical Waste Management Act
“Medical waste” includes OTCs
9
Page 10
Why Are Regulators Concerned with
Pharmaceutical Waste? Why Now?
New focus on drugs in the water supply (E.g., 2008
Associated Press Study; USGS Studies)
Nicotine replacement therapy waste triggers LQG
registration and heightened scrutiny
Significant enforcement precedent in California and
Connecticut
U.S. EPA foot-dragging on RCRA reform and drug risk
assessment per Inspector General
RCRA ill-suited for retail and many health care
providers (“Square peg in a round hole”)
10
Page 11
EPA Regulation of
Hazardous Waste Pharmaceuticals
Managed under RCRA or more stringent state program
2008: U.S. EPA proposed to add hazardous waste pharmaceuticals to the
Universal Waste rule
“Universal Waste”: a subset of Hazardous Waste that have
streamlined management standards.
2012: U.S. EPA rescinded the 2008 proposal
Lack of tracking for shipments of hazardous waste pharmaceuticals
Lack of notification by most handlers managing hazardous waste
pharmaceuticals
May 2012: Office of Inspector General recommended EPA establish a
process for reviewing whether pharmaceuticals are hazardous waste.
Expected Summer 2015: New U.S. EPA proposed rule related to
hazardous waste pharmaceuticals
11
Page 12
Patchwork of State Requirements
States are not always consistent with U.S. EPA
Some have adopted U.S. EPA guidance and exemptions; others have not
E.g., “empty” containers do not count toward generator status
Reverse Distribution Policies
E.g., NM and MN
State-specific requirements
E.g., Waste Determinations
E.g., CA-only Toxics; CA Medical Waste Management Act
State Universal Pharmaceutical Waste Rules
Florida and Michigan
12
Page 13
Point of Generation Issues
Waste Determination: If a pharmaceutical is a “waste,” the generator must determine whether it is hazardous.
When does a pharmaceutical become a waste?
At the retailer? At the Reverse Distribution facility?
Confusion and risk for Retailers’ using Reverse Distribution for prescription pharmaceuticals
If Nondispensed Pharmaceuticals Qualify for Reverse Distribution Procedures:
Not subject to hazardous waste regulations
If Pharmaceuticals do not Qualify for Reverse Distribution:
Pharmaceutical waste must be managed as hazardous waste (storage, transportation, disposal, etc.)
13
Page 14
Point of Generation Issues
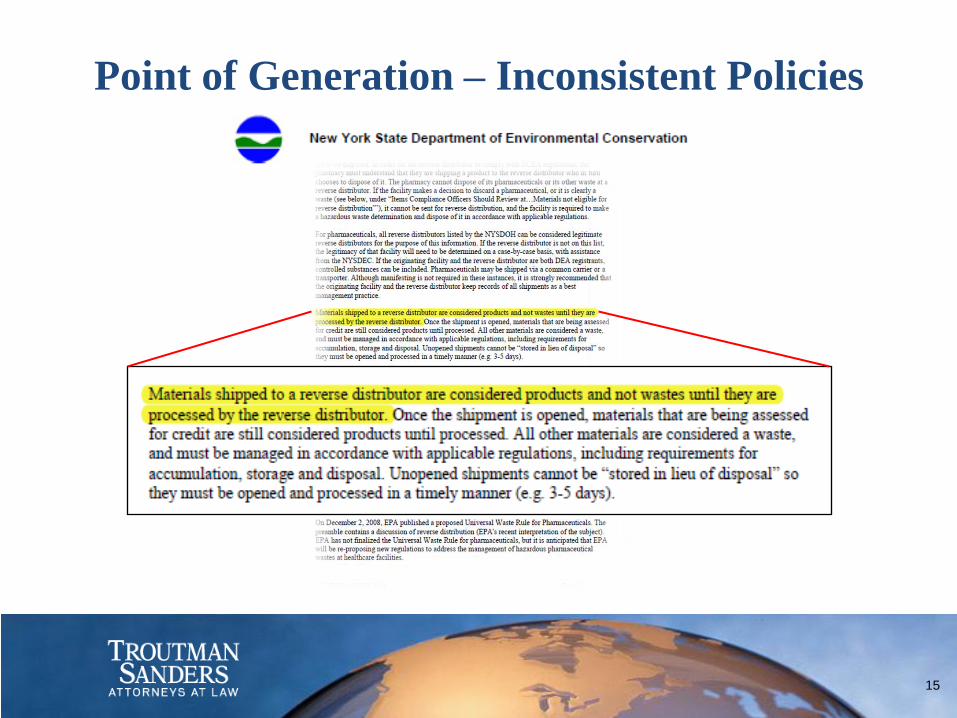
U.S. EPA’s “position” – Not binding
Pharmaceutical products returned through reverse
distribution do not become “wastes” until a determination
is made to discard them.
States are Inconsistent
Most appear to embrace U.S. EPA’s position
Some are more stringent
E.g., Minnesota; New Mexico; Colorado
14
Page 15
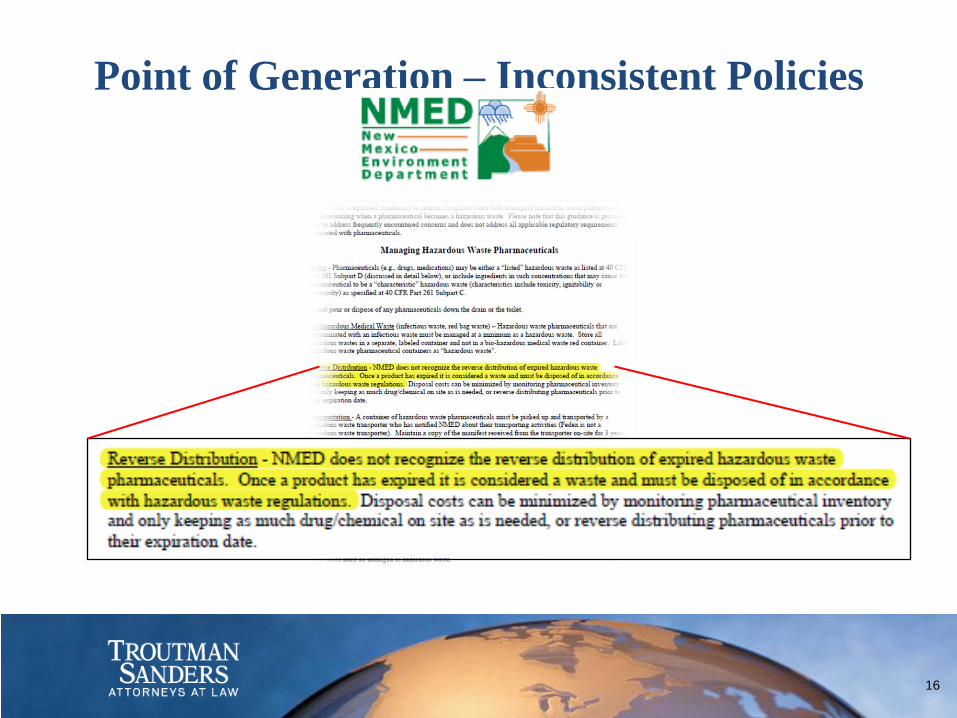
Point of Generation – Inconsistent Policies
15
Page 16
Point of Generation – Inconsistent Policies
16
Page 17
Point of Generation – Inconsistent Policies
17
Page 18
RCRA Enforcement –
Common Misconception
18
Page 19
RCRA Enforcement: Who is Liable?
Hospitals; Retail Pharmacies; Retail Groceries;
Manufacturers; Wholesalers; Reverse Distributors;
Clinics; Surgery Centers; Veterinary Practices; Long
term care facilities
Federal and State liability
Criminal and Civil liability
U.S. EPA fines: Up to $37,500 violation/day.
Potential Debarment or Suspension
19
Page 20
Wal-Mart Plea Agreement
U.S. DOJ in California and Missouri announced on May
28, 2013
Totaled $81 million
Investigation began in approx. 2006
Investigation focused primarily on retail and
pharmaceutical hazardous waste mismanagement
Retail Industry Leaders Association (RILA) Outreach
20
Page 21
Retail Enforcement Cases
21
Page 22
Retail Enforcement Cases
22
Page 23
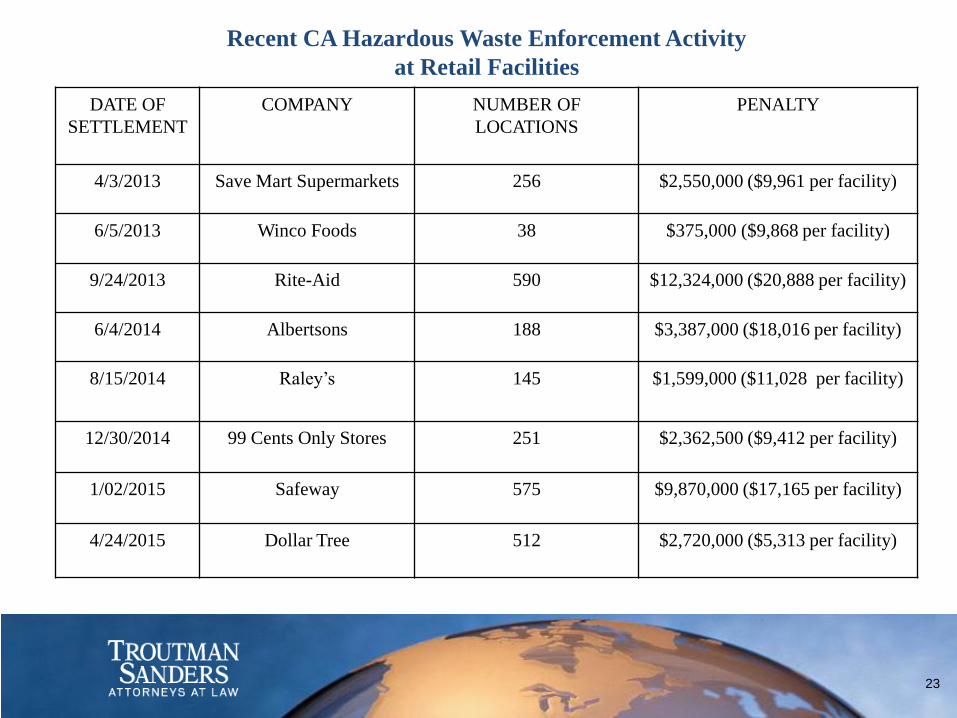
Recent CA Hazardous Waste Enforcement Activity
at Retail Facilities
DATE OF
SETTLEMENT
COMPANY NUMBER OF
LOCATIONS
PENALTY
4/3/2013 Save Mart Supermarkets 256 $2,550,000 ($9,961 per facility)
6/5/2013 Winco Foods 38 $375,000 ($9,868 per facility)
9/24/2013 Rite-Aid 590 $12,324,000 ($20,888 per facility)
6/4/2014 Albertsons 188 $3,387,000 ($18,016 per facility)
8/15/2014 Raley’s 145 $1,599,000 ($11,028 per facility)
12/30/2014 99 Cents Only Stores 251 $2,362,500 ($9,412 per facility)
1/02/2015 Safeway 575 $9,870,000 ($17,165 per facility)
4/24/2015
Dollar Tree 512 $2,720,000 ($5,313 per facility)
23
Page 24
Recent Hazardous Waste Enforcement
Activity at Healthcare Facilities
Concord Hospital, Concord, NH fined $205,000 by NH
Department of Environmental Services in December 2014.
Aurora Health Care, Milwaukee, WI settled hazardous waste
case for $340,000 in May 2014.
SUNY Downstate Medical Center, Brooklyn, NY fined
$156,710 by U.S. EPA in August 2014.
Danbury Hospital, Danbury, CT fined $41,855 by CT
Department of Energy and Environmental Protection in
September 2012.
Sentara Norfolk General Hospital, VA settled with U.S. EPA
for $19,920 in May 2012.
24
Page 25
Current Reform Efforts
Retailers and Healthcare are hopeful RCRA
reform will provide clarity.
Current reform efforts include:
Generator rule change
Pharmaceutical waste reform
Retail waste reform
California Medical Waste Management Act
25
Page 26
Important Issues Noted by U.S. EPA as
Expected for EPA’s Proposed Rule
Regulatory status of creditable pharmaceuticals
Point of generation
LQG status due to P-listed hazardous waste
Better fix for containers with P-listed pharmaceutical
residues
Intersection of U.S. EPA and U.S. DEA regulations
26
Page 27
Operationalizing the DEA and EPA Compliance Challenges Charlotte A Smith, R. Ph., M.S.
WM Sustainability Services,
PharmEcology Services
Pharmaceutical Waste Management:
Compliance for Hospitals, Pharmacies,
and Other Healthcare Facilities
July 30th, 2015
Page 28
Legal Disclaimer
This course is solely for educational purposes and provides only
a general description of various regulatory requirements. For a
complete description, please consult the relevant federal and
state regulatory statutes. Nothing in this presentation
constitutes legal advice and you should not legally rely on any
information provided in this presentation. We make no
warranty, express or implied, with respect to such information
and disclaim all liability resulting from any use or reliance of
this information.
© 2015 WM National Services, Inc.
28
Page 29
Drug Enforcement Administration
• Stocking, dispensing, and disposing of controlled substances
involves a high level of risk and regulation, as defined under
the Controlled Substances Act (CSA)
• Healthcare facilities and pharmacies are registered with the
DEA as “registrants” and must meet a variety of security and
documentation requirements
• During the medication administration process in a hospital,
ambulatory surgery center (ASC), or other medical clinic, it is
common for “wastage” of controlled substances to occur
• Such wastage is usually documented in an automated
dispensing cabinet at hospitals and may be documented
manually in the ASC or clinic environment
• Retail pharmacies usually do not generate controlled
substance waste but may have outdated controlled substances
that must be managed through reverse distribution
©2015 WM National Services, Inc. 29
Page 30
The CSA Regulates Drugs of Abuse into Five Schedules Schedule I: Illegal substances not recognized for medical use, e.g.
heroin, LSD, psilocybin, mescaline
Schedule II: medically available under strict controls, high
potential for abuse leading to severe psychological or physical
dependence e.g. oxycodone, fentanyl, morphine, codeine,
amphetamine. Designated as CII on label.
Schedule III: medically available under somewhat less strick controls,
moderate or low physical dependence, high psychological
dependence e.g. codeine combination products, thiopental, anabolic
steroids. Designated as CIII.
Schedule IV: medically available, low potential for abuse, e.g.
Xanax®, Tranzene®, Valium®, Versed®, Halcion® Designated as CIV.
Schedule V: Low potential for abuse and limited concentrations of
narcotics e.g. codeine cough syrups. Designated as CV.
©2015 WM National Services, Inc.
30
Page 31
The New DEA Disposal Regulation
• Published September 9th, 2014; took effect October 9th,
2014
• Requirements to govern the secure disposal of controlled
substances by both DEA registrants and ultimate users
• Regulations implement the Secure and Responsible Drug
Disposal Act of 2010
• Expands options for take-back events
• Creates mail-back programs and collection receptacle
locations
• Reorganizes and consolidates regulations on disposal
and role of reverse distributors
© 2015 WM National Services, Inc.
31
Page 32
Healthcare Sectors Impacted by DEA Rule Changes • Registrant Disposal
• Hospitals, clinics, physicians, veterinarians, dentists
• Retail Pharmacies including LTCF Provider Pharmacies
• Reverse Distributors
• Non-Registrant Disposal
• “Ultimate User” collection programs, including law enforcement
– Mail-back
– Receptacles (kiosks)
– Single day events
• “Ultimate User” long term care facilities (LTCFs)
– Receptacles provided and managed by retail pharmacies
© 2015 WM National Services, Inc.
32
Page 33
Definition of Terms Disposal and dispose: to refer generally to the wide range
of activities that result in CS being unavailable for further
use or one entity ridding themselves of such substances
(e.g., returns). (FR53547 col 2)
A controlled substance can be “disposed of” by
destruction, return, recall, sale, or through the
manufacturing process.
The new rule eliminates the authority of the Special Agent
in Charge (SACs) to individually authorize disposal methods
for non-practitioners, and retains this option for
practitioners (1317.05)
© 2015 WM National Services, Inc.
33
Page 34
Definition of Terms 1300.05 Methods of Destruction (FR 53522 col1): Intention to allow
public and private entities to develop a variety of
destruction methods that are secure, convenient, and
responsible. Must also meet all other applicable Federal,
State, tribal and local laws and regulations. Once “non-
retrievable,” no longer subject to DEA regulations.
Supersedes all existing MOAs and MOUs.
Retains ability for practitioners to request assistance from
the local special Agent in Charge (SAC). (1317.05(a)(5)).
© 2015 WM National Services, Inc.
34
Page 35
Definition of Terms 1300.05 Non-retrievable: the condition or state to which a
controlled substance shall be rendered following a process
that permanently alters that controlled substance’s
physical or chemical condition or state through
irreversible means and thereby renders the controlled
substance unavailable and unusable for all practical
purposes.
Cannot be transformed to a physical or chemical condition
or state as a controlled substance or controlled substance
analogue.
© 2015 WM National Services, Inc.
35
Page 36
Definition of Terms Destruction (1317.90): Must be rendered non-retrievable.
Incineration is the ONLY method currently accepted by
DEA. Sewering and landfill disposal (mixing with kitty
litter, etc.) do not meet non-retrievable standard.
(FR53547 col 3)
The healthcare industry expressed serious concerns about
how to meet this definition.
DEA issued a clarification letter exempting administered
medications from the new rule.
© 2015 WM National Services, Inc.
36
Page 37
Registrant Disposal Concerns Expressed to DEA
• Ability to render a drug “non-retrievable” in an
institutional setting
• Ability to transfer drug wastage to a reverse distributor
from an institutional setting
• Requirement to double witness the destruction of the CS until
it is rendered non-retrievable
© 2015 WM National Services, Inc.
37
Page 38
DEA Clarification Letter: October 17, 2014 • “…once a controlled substance has been dispensed to a patient by
an institutional practitioner on the basis of an order for immediate
administration to a patient at the registrant's registered location,
the substance is no longer in the practitioner's inventory. For
example, after a pre-filled syringe or a single-dose vial or syringe is
administered to a patient, any remaining substance in the syringe or
vial is not required to be destroyed in accordance with new Part
1317.”
• Such wastage cannot be disposed in a receptacle for ultimate user
collection
• Controlled substances from the pharmacy’s inventory cannot be
disposed in a receptacle for ultimate user collection.
• All destruction must be in accordance with Federal, State, tribal,
and local laws and regulations
© 2015 WM National Services, Inc.
38
Page 39
DEA Clarification Letter: October 17, 2014
• “Although Part 1317 does not apply to pharmaceutical
wastage, the DEA strongly encourages all practitioners to
continue to adhere to security controls and procedures
that ensure pharmaceutical wastage is not diverted.
For example, most institutional practitioners have
implemented policies that require two persons to
witness and record destruction of pharmaceutical
wastage.”
• http://www.deadiversion.usdoj.gov/drug_disposal/dear
_practitioner_pharm_waste_101714.pdf
© 2015 WM National Services, Inc.
39
Page 40
Disposal Options for Controlled Substance Waste
• VERY few controlled substances are EPA hazardous waste
• Chloral hydrate U034
• Alcoholic formulations: diazepam injection, undiluted
• Consider using a method for discouraging diversion
• Cactus Smart Sink®
• Activated carbon options
• DO NOT dispose in regular trash
• Pharmaceutical waste – usually non-hazardous
• Drain dispose if permitted by state and local publicly owned
treatment works
• DO NOT place into sharps or other waste container “as is”
© 2015 WM National Services, Inc.
40
Page 41
Operationalizing the EPA Compliance Challenges – Federal Regulations
(c) WM National Services, Inc.
41
Page 42
Defining “Hazardous” Within the Organization
• EPA Hazardous Waste: meets one of the definitions of
hazardous waste federally or at the state level; must
be a waste
• OSHA Hazardous Drug: a risk to employees due to
occupational exposure; may be a product or a waste
• DOT Hazardous Material: a risk to health and safety
while in transit; may be a product or a waste
• Biohazardous: meets the definition of an infectious risk
at the state level; may be a product or a waste
• Regulated medical waste
© 2015 WM National Services, Inc.
42
Page 43
Identifying Hazardous Pharmaceutical Waste Under RCRA • P-listed pharmaceuticals (acutely hazardous)
• Sole active ingredient; unused; empty containers
• LD50 (oral) 50mg/kg
• Examples: nicotine, warfarin
• U-listed pharmaceuticals (toxic)
• Sole active ingredient; unused
• Examples: cyclophosphamide, mitomycin, lindane, selenium sulfide
• Pharmaceuticals that exhibit a characteristic of hazardous waste (D codes)
• Ignitability D001
• Toxicity D004 – D043
• Corrosivity D002
• Reactivity D003 © 2015 WM National Services, Inc.
43
Page 44
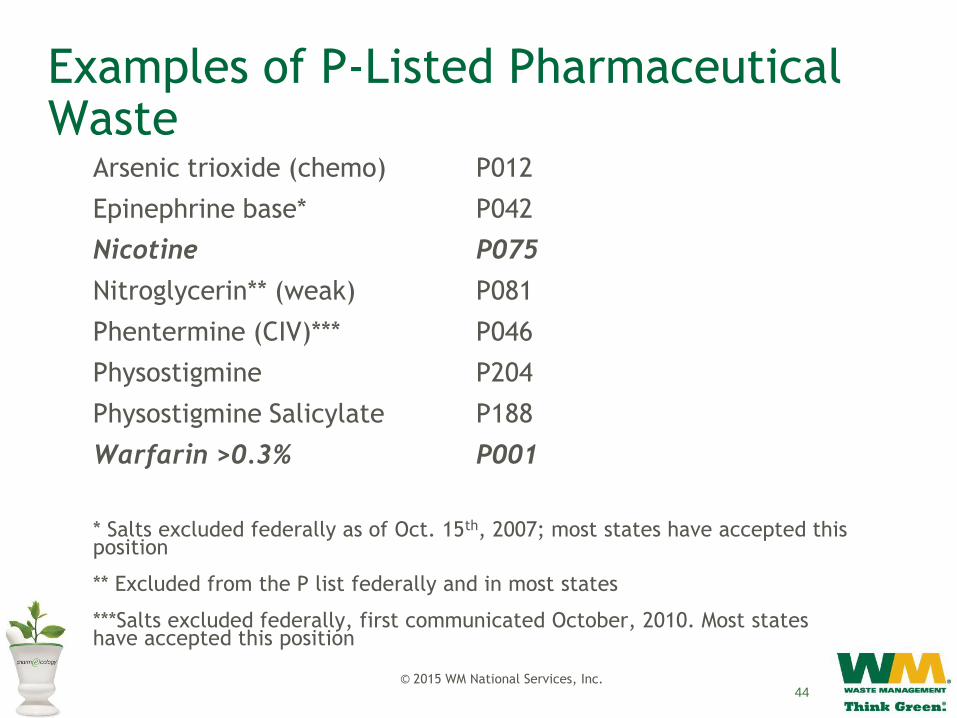
Examples of P-Listed Pharmaceutical Waste
Arsenic trioxide (chemo) P012
Epinephrine base* P042
Nicotine P075
Nitroglycerin** (weak) P081
Phentermine (CIV)*** P046
Physostigmine P204
Physostigmine Salicylate P188
Warfarin >0.3% P001
* Salts excluded federally as of Oct. 15th, 2007; most states have accepted this position
** Excluded from the P list federally and in most states
***Salts excluded federally, first communicated October, 2010. Most states have accepted this position
© 2015 WM National Services, Inc. 44
Page 45
Examples of U-Listed Pharmaceutical Waste
• Chloral Hydrate(CIV) U034
• Chlorambucil U035
• Cyclophosphamide U058
• Daunomycin U059
• Lindane U129
• Melphalan U150
• Mitomycin C U010
• Streptozotocin U206
• Selenium Sulfide U205
© 2015 WM National Services, Inc.
*Italicized items are chemotherapy agents.
45
Page 46
Characteristic of Toxicity
• 40 chemicals which must be below specific leaching
concentrations
• Fail the Toxicity Characteristic Leaching Procedure (TCLP)
• Must evaluate IVs, such as total parenteral nutrition (TPN)
• May come out of regulation due to dilution (chromium,
selenium)
• Examples of potentially toxic pharmaceutical ingredients:
• Chromium D007
• m-Cresol D024
• Mercury (Thimerosal) D009
• Selenium D010
• Silver D011
© 2015 WM National Services, Inc. 46
Page 47
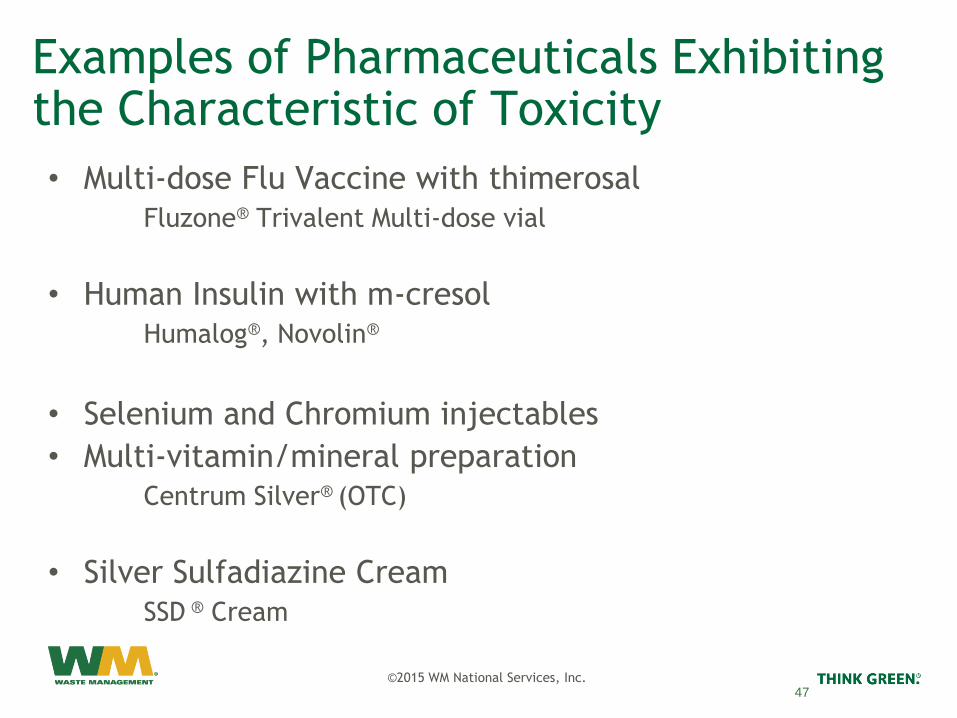
Examples of Pharmaceuticals Exhibiting the Characteristic of Toxicity
• Multi-dose Flu Vaccine with thimerosal
Fluzone® Trivalent Multi-dose vial
• Human Insulin with m-cresol
Humalog®, Novolin®
• Selenium and Chromium injectables
• Multi-vitamin/mineral preparation
Centrum Silver® (OTC)
• Silver Sulfadiazine Cream
SSD ® Cream
©2015 WM National Services, Inc.
47
Page 48
Characteristic of Ignitability
• Aqueous solution containing 24% alcohol or more by
volume and flash point < 140°F
• Non-aqueous solutions with flash points < 140°F
• Oxidizers
• Flammable aerosols e.g. Proventil® Inhaler
• Hazardous waste code D001
• Rubbing alcohol
• Topical preparations: Clindamycin®
• Some injections: Paclitaxel
©2015 WM National Services, Inc. 48
Page 49
Definition of Empty
• To be “RCRA empty”, P-listed containers must be
triple rinsed & rinsate discarded as hazardous
waste; only used syringes excluded – EPA regulation
(in practice, no triple rinsing)
• The EPA requires P-listed wrappers & packaging to
be managed as RCRA hazardous waste because of
the residue remaining in them
• U-listed and D codes: empty if all contents
removed that can be removed by normal means
and no more than 3%, by weight, remaining
• Aerosols – never considered “empty”
©2015 WM National Services, Inc. 49
Page 50
Pharmaceutical Waste Management Programs: Insuring Compliance
• Identifying relevant stakeholders
• COO, CNO (Chief Nursing Officer or comparable)
• Risk Management/Legal
• Director of Pharmacy
• Nurse Educators
• Infection Control Officer
• Environmental Health & Safety Officer
• Environmental Services Manager
• Obtaining “buy-in” from the C Suite down
• Appointing a Champion
• Developing a Core Team with a mandate
©2015 WM National Services, Inc. 50
Page 51
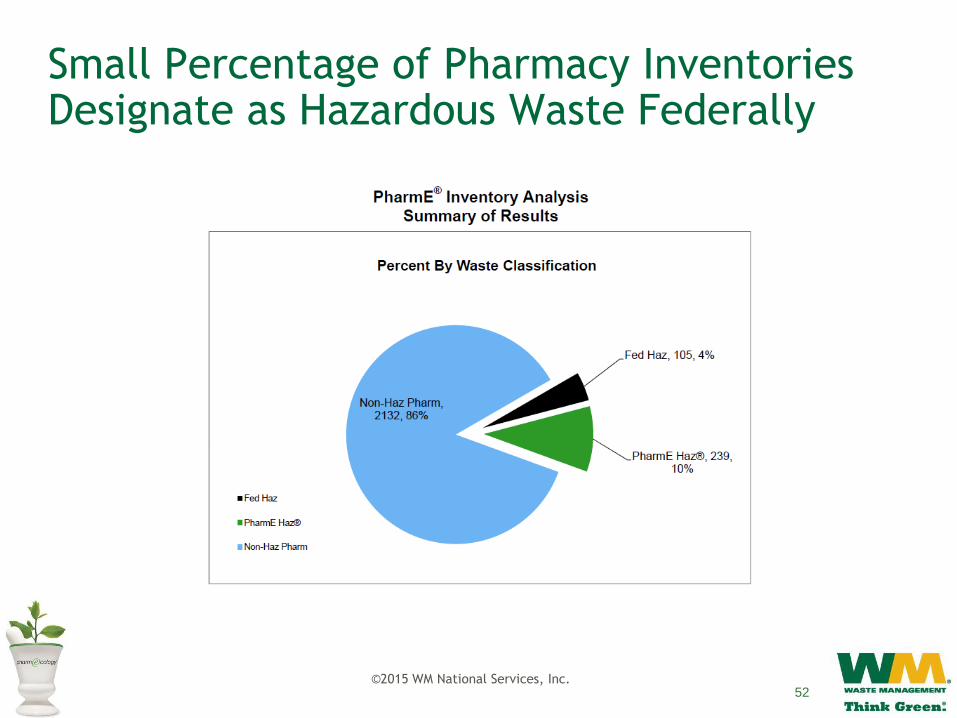
Determining Which Drugs Become a Hazardous Waste
• Utilize the services of a specialized consulting firm
• Initial Inventory Analysis followed by method for
maintaining the waste categorization for new drugs
entering the system
51
Page 52
Small Percentage of Pharmacy Inventories Designate as Hazardous Waste Federally
©2015 WM National Services, Inc. 52
Page 53
Label the Shelves in Pharmacy
Identify
Hazardous
Waste
Choose
Container Sizes
and Locations
Pharmacy Implementation
Launch
Disposal in
Pharmacy
Label
Pharmacy
Shelves
©2015 WM National Services, Inc. 53
Page 54
Role of Nursing in the Disposal of Pharmaceuticals
• Define prompts that will help nursing readily
recognize hazardous pharmaceutical waste.
• Messages on automated dispensing cabinets
dispensing screens
• Labeling bins / containers
• Messages on the electronic medication
administration records (eMARS) and Bar Code
Medication
Administration (BCMA) dispensing screens
• Messages on medication labels
• Select size, type, and location of containers
that will be used to dispose of pharmaceutical
waste ©2015 WM National Services, Inc. 54
Page 55
Commonly Used Color Codes
Hazardous Pharmaceutical Waste
Trace Chemotherapy Waste Regulated Medical Waste
Non-Hazardous Pharmaceutical
Waste
©2015 WM National Services, Inc. 55
Page 56
Summary of Pharmaceutical Waste Streams: Acute Care Hospital
Aerosols
Municipal
Solid
Waste
• Most packaging
• Most empty
bottles and vials
• Most empty IVs
• Paper
• Plastic
• No drugs
• No P-waste
containers
© 2015 WM National Services, Inc.
Sewer
System
Compatible Hazardous
Waste*
Trace
Chemo
(Sharps)
Trace
Chemo
(Soft)
Non -
Hazardous
Drugs
Red
Sharps
• P-listed
(inc. containers)
• U-listed
• D-listed t toxic,
• Ignitable
• Bulk chemo
• Haz/Chemo spill
clean up
Lined Non-Hazardous Waste Landfill
Medical Waste Incinerator
Municipal
Incinerator
Permitted for
Special Waste
(inc. drugs)
Autoclave/
Microwave
Shredded (Most states) Ash Ash
Lined Hazardous Waste Landfill
Federally Permitted Hazardous Waste Incinerator
• Ignitable
aerosols
• Pressurized
aerosols
Ash
• IVs
o Dextrose
o Saline
o Sterile Water
o Lactated
Ringer’s
o K salts
o Ca salts
o Mg salts
• Controlled
substances?
• No other drugs
• Empty vials and
ampules
• Empty syringes
and needles
• Empty IVs
• Gowns
• Gloves
• Tubing
• Wipes
• Packaging
• All non-hazardous
pharmaceutical
waste
• No biohazardous
drugs
• No sharps
• Empty syringes,
needles, ampules
(except chemo)
• Bio-hazardous
drugs
* Dual waste for sharps
Publicly
Owned
Treatment
Works
( POTW)
Water
Supply
Page 57
Next Steps
• Determination of Generator Status
• Recordkeeping and reporting requirements
• Training and emergency response requirements
• Planning for RCRA inspections/enforcement
actions
• Lessons learned and best practices observed
©2015 WM National Services, Inc. 57
Page 58
Next Steps for Program Management, Planning for Inspections and Best
Practices
July 30, 2015
Darrell J. Oman; Program Manager – Consulting Services
Stericycle Environmental Solutions
Pharmaceutical Waste Management: Compliance for Hospitals, Pharmacies,
and Other Healthcare Facilities
Page 59
Next Steps to Program Compliance
1. Identify and Evaluate All Waste Streams and determination of generator status
2. Collect and Store Hazardous Waste Properly
3. Train Employees
4. Prepare and Save Documentation
5. Know Emergency and Spill Response Procedures
IMPORTANT REMINDER
Your generator “status” determines compliance requirements •Large Quantity Generator (LQG) •Small Quantity Generator (SQG)
•Conditionally Exempt Small Quantity Generator (CESQG)
59
Page 60
Next Steps
Once you’ve identified all waste streams and made determinations on which are hazardous waste streams then generator status is determined. Next file (with the state usually) a Notification of Regulated Waste Activity form and receive a site specific USEPA generator I.D. #.
NOTE: generator status may change at any time due to: New waste stream(s) identified and generated
Changes in monthly generation rate of wastes
Therefore compliance requirements may change accordingly and immediately
60
Page 61
RCRA Generator Status
Under the Federal rules there are three classes of generators (NOTE: State/Local regulations may be more stringent). 1. Conditionally Exempt Small Quantity Generator (CESQG)
Generate no more than 100 kg of hazardous waste, 1 kg of acutely hazardous waste, or 100 kg of contaminated waste from an acutely hazardous waste spill in a month. Accumulate no more than 1,000 kg of hazardous waste at any time.
2. Small Quantity Generator (SQG) Generate between 100 and 1,000 kg of hazardous waste and no more than 1 kg of acutely hazardous waste in one month. Accumulate no more than 6,000 kg of hazardous waste for up to 180 days (270 days if waste is to be transported over 200 miles).
3. Large Quantity Generator (LQG) Generate greater than 1,000 kg of hazardous waste or greater than 1 kg of acutely hazardous waste in one month. Accumulate greater than 6,000 kg of hazardous waste for up to 90 days.
61
Page 62
Next Steps
Collect and Store Waste Properly Satellite Accumulation Areas (know rules)
Hazardous Waste Storage Area (know rules)
Train Employees According to Job Responsibilities
Within 6 Months of Hire or Job Change
Annual Training Required for Some Generators (LQGs)
Prepare and Save Documentation Inspections and Training Records
Uniform Hazardous Waste Manifests
62
Page 63
Hazardous Waste Containers Hazardous Waste Containers can be placed
throughout a facility.
Hazardous Waste Containers must be:
under the control of the staff,
near the point of waste generation AND
closed unless being used.
Containers in the Satellite Accumulation Areas (SAA) must be moved to the Hazardous Waste Storage Area within 3 days of becoming full.
SAA Volume limits for P-List (1 quart ) and regular hazardous waste (55 gallons)
Containers are then considered a Hazardous Waste Storage Container and must be shipped off-site within 90 days if a LQG and 180 days if a SQG.
Waste Collection and Storage
63
Page 64
Employee Training
Personnel must be trained
Employees whose responsibilities include hazardous waste management, storage, transport or recordkeeping must be trained within 6 months of starting or a job change
The type and degree of training required depends on each employee’s responsibilities associated with his/her job function
Generator status establishes training requirements:
LQGs – most stringent – annual training
SQGs and CESQGs – less stringent
64
Page 65
Hazardous Waste Storage Area
Must be inspected weekly (inspection records maintained)
Meet all storage area requirements as described in 40 CFR 262.34 and 265.32 & 174 including but not limited to: Adequate aisle space
Impermeable floor surface
Secondary containment
Prepare Uniform Hazardous Waste Manifest (EPA Form 8700-22) for each hazardous waste shipment
Inspections and Reporting
65
Page 66
Permitted Hazardous Waste vendors pick-up your wastes and provide a shipping manifest The UHWM is multi-copy shipping paper
required for shipments of hazardous waste
Why is Manifesting Important? A record to ensure that waste is managed
properly - “Cradle to Grave” record The generator (each location) is ultimately
responsible for the information contained on the manifest
Land Disposal Restriction Notification Form (LDR) also required
Uniform Hazardous Waste Manifest (UHWM)
66
Page 67
Next Step
Know Emergency and Spill Response Procedures LQGs need a Haz Waste Contingency Plan
SQGs need elements of a Plan
Hazardous Waste Contingency Plan - a written document describing: Emergency response procedures including the following:
Emergency coordinator(s)
Emergency telephone numbers
Hazardous wastes generated
Arrangements with local emergency response services
Measures to prevent the release of hazardous waste
Emergency equipment
Evacuation plan
67
Page 68
Hazardous Waste - Inspections, Best Practices and Lessons Learned
Inspections and Enforcement USEPA/State Inspections
Recent cases
How to handle an inspection
Examples of common violations
Hazardous Waste Program Management – Best Practices and Lessons Learned Program management champion
Executive leadership and risk management perspective
Departments and department leadership perspective
68
Page 69
Federal/State Hazardous Waste Program Inspections
Can be brief or comprehensive and unannounced USEPA (Federal) inspections can
take 2-3 days
Can focus on certain hazardous waste streams or be building-wide or campus-wide inspections
No facility employees or leadership are exempt from being questioned or interviewed
Examples of typical areas of inspection: Waste determinations documentation
Recordkeeping/training/emergency response
Storage areas and containers
69
Page 70
RCRA Inspection Recommendations
When an inspector or inspection team arrives: Understand that the inspection is an opportunity to learn
and to find areas of program improvement
Gather and make available the best team of management and subject matter expertise to accompany the inspector(s)
Answer questions to the best of your knowledge - if an answer is not known then say so
Expect a closing summary meeting where preliminary findings (including alleged violations) are identified and discussed
70
Page 71
Inspection and Enforcement Efforts – Examples of Violations
Hazardous wastes are not identified
Open, unlabeled or mislabeled storage containers
Storage area is not adequate
Satellite accumulation issues
Training records/Manifest records
Exceeding storage time limit
Storage area inspection records
Outdated Contingency Plan
71
Page 72
Lessons Learned – Program Management
Facility/Corporate Executive Team and Risk Management Perspective Regulatory compliance with RCRA is not generally on the
radar screen unless there has been an incident or inspection
In Healthcare the TJC (The Joint Commission) has trained over 500 accreditation surveyors on the proper management of hazardous and pharmaceutical wastes
Operations structure, outsourcing and staff turnover can have a large impact on the compliance performance of the hazardous and Rx waste management program at any facility
Many hospitals, hospital systems, retail pharmacies and retailers don’t have RCRA environmental compliance expertise onsite or in-house.
72
Page 73
Lessons Learned – Program Management (cont.)
Store Operations, Facilities, Safety, Laboratory, Pharmacy, Clinical and Housekeeping Management and Staff Perspective
Hazardous waste management impacts nearly every department and professional discipline in a Healthcare facility and nearly all Retail operations (stores, distribution centers, etc.)
Generally the more centralized the management of the hazardous waste program is the more compliant the program
Recommend naming a Program Champion for the entire facility or company
Recommend centralizing all waste determinations documentation, inspection reports, waste generation reports and training documentation with the Program Champion
Recommend local onsite Program Coordinator and local access to required program documentation
73
Page 74
Gregory W. Blount
Troutman Sanders LLP
404-885-3291
[email protected]
Charlotte A. Smith, R. Ph., M.S.
Senior Regulatory Advisor
PharmEcology Services
WM Sustainability Services
713-725-6363
[email protected]
Darrell J. Oman
Program Manager – Consulting Services
Compliance & Regulatory Affairs
Stericycle Environmental Solutions
612-360-1213
[email protected]
Questions?
74
Page 75
15 Most Common Hazardous Waste Violations and Problems Found at Hospitals
Improper or lack of hazardous waste (HW) labeling (go to HW labeling).
No or infrequent weekly inspections of HW storage/satellite areas (go to for inspections
requirements).
Open containers of HW (go to container sealing requirement).
Improper disposal of chemotherapy drugs (go to hazardous waste determinations and see
information for U-list waste).
Failure to perform or improper hazardous waste determinations (go to hazardous waste
determinations).
No or inadequate HW manifests (go to hazardous waste manifest).
Throwing HW down the drain.
Improper management of mercury-containing wastes, including but not limited to, fluorescent light
bulbs, mercury vapor lights, thermometers, sphygmomanometer, gastric tubes, thermostats, etc.
(go to mercury in healthcare facilities)
Improper management of expired pharmaceuticals, paints, etc. (go to pharmaceuticals in
healthcare facilities)
Lack of a contingency plan (go to emergency planning).
Lack of or inadequate training of employees in HW management (go to personnel training).
Failure to ensure that HW meets Land Disposal Restrictions (go to shipping wastes off-site).
Failure to upgrade/close underground storage tanks (USTs) by 12/22/98 (go to UST inspection
protocol).
Malfunctioning leak detection systems.
Improper consolidation of wastes from nearby facilities.
Source: EPA Region 2.
75
Page 76
References and Resources
Healthcare Sector Environmental Laws and Regulations
http://www.epa.gov/lawsregs/sectors/healthcare.html
RCRA/Hazardous Waste Resource Locator
http://www.envcap.org/statetools/hzrl/index.cfm
Profile of the Healthcare Industry – USEPA Document
http://www.epa.gov/compliance/resources/publications/assistance/sectors/n
otebooks/health.pdf
Managing Pharmaceutical Waste – A Discussion Guide for Health-
System Pharmacists
http://www.ashpadvantage.com/docs/PharmaWaste-Discussion-Guide.pdf
Table of Common Wastes in Health Care (Wisconsin version)
http://dnr.wi.gov/files/PDF/pubs/wa/wa1259.pdf
Self-audit Checklists for LQGs and SQGs (Wisconsin examples)
http://dnr.wi.gov/files/PDF/pubs/wa/wa1263.pdf
http://dnr.wi.gov/files/PDF/pubs/wa/wa1264.pdf
76
Page 77
Resources
Environmental Leader • www.environmentalleader.com
Environmental Law & Policy Monitor www.environmentallawandpolicy.com
EPA Management of Hazardous Waste Pharmaceuticals
http://www2.epa.gov/hwgenerators/management-pharmaceutical-hazardous-waste
Hazardous Waste Pharmaceuticals Wiki http://hwpharms.wikispaces.com/
77
Page 78
78
References
• Managing Pharmaceutical Waste: A 10-Step Blueprint for
Healthcare Facilities in the United States
http://www.hercenter.org/hazmat/tenstepblueprint.pdf
• Management of Hazardous Waste Pharmaceuticals:
http://www2.epa.gov/hwgenerators/management-
pharmaceutical-hazardous-waste
©2015 WM Healthcare Solutions, Inc.
Page 79
Retail Inspection Tracker
Created through Troutman Sanders subsidiary, eMerge
Secure, easy to use inspection tracking application
Track each inspection finding in detail
Beneficial tracking options including: Calendar of upcoming corrective action and response due dates
State-by-state inspection trends
Analysis of common findings to assist with program improvement
Monthly/yearly comparison of inspection activity
Comparison of inspections with and without findings
Customizable for each retailer’s specific issues and preferences
Receive automatic, customized alerts for desired metrics E.g., hot states, high-priority inspection findings
79