RBx 343E48F0 is a novel, potent, selective and long acting muscarinic receptor antagonist with a potential foruse in the treatment of Chronic Obstructive Pulmonary Disease (COPD). The aim of the present study was todescribe the in vitro and in vivo profile of RBx 343E48F0 and to compare the results with the present daybenchmark therapy, tiotropium. Radioligand binding and isolated tissue based functional assays were used toevaluate the affinity, potency and receptor subtype selectivity of RBx 343E48F0. Inhibition of carbachol-induced bronchoconstriction in the anaesthetized rat and acetylcholine-induced bronchoconstriction in theconscious rat were used to assess the extent and duration of the bronchospasmolytic activity of RBx 343E48F0.In vitro and in vivo pharmacokinetic studies were conducted to evaluate the pharmacokinetic and lungretention properties of the compound. In vitro radioligand binding studies using human recombinantmuscarinic receptors showed that RBx 343E48F0 had a pKi of 9.6 at the M3 receptor and a 60-fold selectivityfor theM3 receptor over theM2 receptor. In isolated tissue bioassays, it exhibited surmountable antagonism atthe guinea pig trachea with a pKB of 9.5. Intratracheal administration to anaesthetized rats demonstrated adose-dependent inhibition of carbachol-induced bronchoconstriction with an ED50 value of 110 ng/kg. RBx343E48F0 also exhibited a fast onset of action and long duration of action of greater 24 h.
ta).ctor 18, Gurgaon, India.Syngene International Ltd.,
COPD is an inflammatory airway disease with a high prevalenceworldwide. It is predominantly a smoker's disease characterized by achronic inflammatory process in the respiratory tract and lungparenchyma. The progressive inflammatory nature of disease leadsto a narrowing of the airway lumen coupled with an increase incholinergic tone resulting in bronchoconstriction and associatedsymptoms, including shortness of breath.
An increased cholinergic neural tone is the only reversiblecomponent in COPD. Anticholinergics inhibit this increased tone anddecrease airway hyperreactivity in patients with COPD and have
become the standard of care in the treatment of COPD since the launchof ipratropium bromide (Koumis and Samuel, 2005; Barnes, 2003).
The Parasympathetic nervous system provides the dominantautonomic control of airway smooth muscle contractility through therelease of acetylcholine which causes tissue bronchoconstriction byactivationof postsynapticmuscarinic receptors (Fryer and Jacoby, 1998).
The Cholinergic response in the airway is mediated through fivedistinctmuscarinic receptor subtypes labeledM1 toM5. The blockade ofM1 and M3 receptors results in bronchodilation and decreased mucussecretion. The blockade of the M2 receptor, however, results in theacetylcholine release, which can potentially offset the bronchodilationachieved through inhibition of the M1 and M3 receptors. The optimuminhibition of the parasympathetic system is achieved, therefore, by theantagonism of M1 andM3 receptors and not M2 receptors (Gross, 2004;Haddad et al., 1999 and Coulson and Fryer, 2003).
Currently, two inhaled muscarinic antagonists are available for themanagement of symptomatic COPD patients: ipratropium, a shortacting agent requiring up to four doses per day, and tiotropium, a long-acting, once-daily treatment (Barnes, 2004; Gross, 2006; Hanania andDonohue, 2007). Tiotropium and ipratropium are non-selective mus-carinic receptor antagonists, although tiotropium exhibits kinetic
220 S. Gupta et al. / European Journal of Pharmacology 658 (2011) 219–228
selectivity by dissociating faster from M2 receptors than the othermuscarinic receptor subtypes. A lot of effort is underway to identifynovel muscarinic receptor antagonist with long duration of action(Fitzgerald and Fox, 2007a, 2007b). In the present study, we reportpharmacological characterization of RBx 343E48F0, (3-benzyl-1-[3-({(2R)-2-[(1R)-3,3-difluorocyclopentyl]-2-hydroxy-2-phenylacetyl}oxy) propyl]-2-methyl-1H-imidazol-3-ium bromide) as a novel, potent,competitive and selective muscarinic M3 receptor antagonist, whichspares M2 muscarinic receptors and exhibits potent, rapid andprolonged inhibition of muscarinic receptor response in experimentalanimal models by the intratracheal route.
2. Materials and methods
2.1. Drugs and chemicals
RBx 343E48F0, tiotropium bromide and aclidinium bromide weresynthesized at Ranbaxy Research Laboratories (Fig. 1). [3H] N-methylscopolamine was obtained from Amersham. Isoflurane was purchasedfrom Baxter Healthcare Corporation. Ketamine was procured fromNeon Laboratories and xylazine was purchased from Indian Immu-nologicals Limited. Methylcellulose was purchased from Loba Chemie.Other chemicals were procured from Sigma Chemicals.
2.2. In vitro studies
2.2.1. Binding affinity of RBx 343E48F0 at human recombinantmuscarinic receptor subtypes
The affinity of RBx 343E48F0 at human muscarinic receptorsubtypes was evaluated in competitive radioligand binding assaysusing [3H] N-methyl scopolamine as ligand. The competitive bindingassays were conducted using membrane preparations from ChineseHamster Ovary cells transfected stably with human M1, M2, M3, M4
and M5 subtypes. Binding assays were performed according to themethod of Moriya et al. (1999), with minor modifications. Briefly,membrane homogenates (5–20 μg protein) along with the com-pounds were incubated in 96 well microtiter plates in 250 μl of assaybuffer (HEPES 20 mM, pH 7.4) at 23–27 °C for 3 h using [3H] NMS asligand. Non-specific binding was determined in the presence of 1 μMatropine. Incubation was terminated by vacuum filtration over 0.1%polyethyleneimine pre-treated GF/B fiber filters using a Skatron cellharvester. Filters were then washed with ice-cold 50 mM Tris–HCl
O
ON
FF
N+
OH
S
SOH
O
O
N+
O
N+
SOH
S
O
O
O
Br -
RBx 343E48F0
Br - Aclidinium Bromide
Br -
Tiotropium bromide
Fig. 1. Structures of RBx 343E48F0, tiotropium and aclidinium.
buffer (pH 7.4) and the filter mats dried and transferred to 24 wellplates. The radioactivity retained on filters was determined using500 μl of supermix scintillant in a Microbeta (Wallac) counter.
2.2.1.1. Data analysis. Specific binding was used for the analysis. IC50 ofthe compounds was determined in competitive binding assays.Saturation binding assays were used to determine Kd (apparentdissociation constant) for [3H] NMS. The IC50 values were determinedby a non-linear curve-fitting program called ‘One site competition'using Graph Pad Prism software version 4. The inhibition constant Kiwas calculated from competitive binding studies using the equation:
Ki = IC50 = 1 + L½ �= Kdð
where [L] is the concentration of ligand and Kd is the dissociationconstant of [3H] NMS (Cheng and Prusoff, 1973).
Subtype selectivity was expressed as the antilogarithm of thedifference of the pKi at each receptor to mean pKi at other receptors.Results were expressed as mean±S.E.M. for each group and statisticalsignificance for pKi values was assessed by a one-way analysis ofvariance (ANOVA) using GraphPad prism software version 4.
2.2.2. Metabolic stability in liver microsomesRBx 343E48F0 (0.5 μM) was incubated in a reaction mixture
consisting of liver microsomes and an NADPH regenerating system.Aliquotswerewithdrawn at 3 min intervals for 30 min and analyzed forparent compound by LC-MS/MS. The loss of parentwas expressed as thepercentage of the test compound remaining and the rate of decay wasestimated by mono-exponential decay kinetics. The rate of decay wasnormalized to microsomal protein expressed as ml/min/g liver.
2.2.3. CYP inhibition studiesThe Cytochrome P450 (CYP) inhibition of RBx 343E48F0 was
evaluated in vitro using a standard commercial kit (BD-Gentest)containing recombinant CYPs. In brief, the tested CYP metabolizes anon-fluorescent fluorogenic substrate into a fluorescent product,which is measured by a fluorescent plate reader. The ability of RBx343E48F0 at tested concentrations to reduce the fluorescence for eachindividual CYP was measured and reported as an IC50 value (μM).
2.2.4. PermeabilityThe permeability of RBx 343E48F0 was measured in a Caco-2 cell
lines at a concentration of 50 μM and reported as an apparentpermeability (Papp).
2.2.5. Plasma protein bindingThe protein binding of RBx 343E48F0 was estimated by ultra-
filtration of human, dog and rat plasma containing 100 and 1000 ng/mlconcentrations of compound. Aliquots of spiked plasma samples werecentrifuged at 2000 rpm for 20 min using Centricon ultrafiltration tubesin triplicate. The Ultra filtrate and retentate were both weighed andanalyzed for unbound and total RBx 343E48F0 content, respectively.
2.2.6. Isolated tissue experimentsFemale Dunkin-Hartley guinea pig (300–900 g), with free access to
food andwater, were procured from the Experimental Animal Facility,Ranbaxy Research Labs Ltd. Guinea pigs were euthanized with anoverdose of thiopentone sodium (~300 mg/kg, i.p.). Trachea wasisolated and kept in oxygenated Krebs Henseleit (KH) buffercontaining (mM): NaCl, 118; KCl 4.7; CaCl2, 2.5; MgSO4, 1.2;NaHCO3, 25; KH2PO4, 1.2, glucose 11.1. The trachea was freed ofconnective tissue and then cut into seven or eight strips of equal size(approx. 6–7 tracheal rings in each strip). The tracheal ringswere thenopened along the mid-dorsal surface with the smooth muscle bandintact and a series of transverse cuts were made from alternate sidesso that they did not transect the preparation completely. The opposite
221S. Gupta et al. / European Journal of Pharmacology 658 (2011) 219–228
ends of cut rings were tied with the help of a thread and the tissueswere mounted in buffer maintained at 37 °C and aerated withcarbogen (95% oxygen and 5% carbon dioxide). A resting tension of1 g was applied and each tissue was equilibrated for 60 min withwashing at 15 min interval. Post equilibration, the tracheal rings werechallenged with 60 mM KCl until two reproducible responses wereobtained. Contractile responses were recorded using a POWERLABdata acquisition system (AD Instruments) or a Grass polygraph(Model 7) and expressed as tension in g.
2.2.6.1. Antagonism of carbachol response. Cumulative concentrationresponse curves to carbachol from 1 nM onwardswere obtained usingguinea pig trachea following which tissues were allowed to relax tothe baseline with tissues being washed every 15 min. Tissues wereincubated with different concentrations of RBx 343E48F0 (1, 3, 10 and30 nM), tiotropium (0.1, 1 and 3 nM) or vehicle for 20 min, afterwhich a second carbachol cumulative concentration response curvewas obtained in trachea.
2.2.6.2. Electrical field stimulation experiment. In order to assess onsetand offset of antagonist from receptors, tissues were stimulated usingplatinum electrodes (4 Hz, 15 s duration, every 4 min). Indomethacin(10 μM) was added to the KH buffer to prevent the formation ofbronchoactive prostanoids for duration of action study. Equilibratedtracheal tissues were pretreated for 10 min with propranolol (1 μM)to prevent the effect of any endogenous catecholamines. Three stableresponses of equal magnitude were obtained. Thereafter minimalconcentration of RBx 343E48F0 (1 nM)/tiotropium (1 nM)/vehiclewere introduced and further stimulation was delivered until themaximum effect of the drug was observed. Treated tissues werewashed and stimulation further applied until the response obtainedwas 50% of the original response. Appropriate time controls were alsostudied in the absence of antagonists. Contractile response to EFS wascompletely blocked under these conditions by both atropine (10 μM)and quinidine (100 μM).
2.2.6.3. Data analysis. For guinea pig trachea, Emax was expressed as apercentage of the maximum response obtained in control tissue. Datawas analyzed using a non-linear curve-fitting program (Graph PadPrism). Potencies were expressed as pD2, the negative log10 (EC50).The pKB value, an index of functional antagonism, was calculated fromthe EC50 data using the following equation:
− log antagonist Mð Þ= DR−1ð Þ½ �
where,
M represents concentration of the antagonist; andDR represents the EC50 values of carbachol in the absence and
presence of the antagonist, respectively.
In cases where the Emax was less than 50%, the pKB was calculatedusing Kenakin's double reciprocal plot (Kenakin, 1993). A P value ofb0.05 was considered to be statistically significant. Values of t1/2[onset], i.e. the time from starting the administration of the testantagonist to the attainment of 50% inhibition of the cholinergicneural response, and t1/2 [offset], i.e. the time fromwashout of the testantagonist to the attainment of 50% recovery of the cholinergicresponse, was computed by interpolation from each time-effect curveusing Graphpad Prism software and expressed as mean±S.E.M.
2.3. In vivo studies
2.3.1. AnimalsThe experiments were conducted on healthy in-bred Wistar rats
obtained from the Experimental Animal Facility, Ranbaxy Research
Laboratories Ltd. Animals were housed in standard cages andmaintained at a temperature of 24±2 °C with controlled illuminationto provide a light–dark cycle of 12 h. All experimental protocols wereapproved by the Institutional Animal Ethics committee (IAEC) ofRanbaxy Research Laboratories Ltd and experiments were conductedas per the Committee for the Purpose of Control and Supervision onExperiments on Animals (CPCSEA) Guidelines for the use and care ofexperimental animals.
2.3.2. Effect of RBx 343E48F0 on carbachol-induced bronchoconstrictionin anaesthetized rat
Rats were anaesthetized with ketamine (40 mg/kg, i.p.) andxylazine (5 mg/kg, i.p.) and vehicle (phosphate buffered saline,PBS), test substance RBx 343E48F0 or standard drug — tiotropium,dissolved in PBS were instilled intratracheally (i.t.) in a dose volume of0.5 ml/kg. At two or twenty four hours post instillation, animals wereanaesthetised with urethane (1.2 g/kg, i.p.) and the jugular veincannulated to allow intravenous administration of carbachol. Trache-otomy was performed and a cannula inserted into the trachea.Subsequent to surgery, the animal was placed in a plethysmographbox (PLY 3114, Buxco Electronics, USA) and the tracheal cannula wasconnected to a port in the chamber wall that was open to theatmosphere. Airflow in the plethysmograph box was measured by aflow transducer (TRD 5700, Buxco Electronics, USA), whereastranspulmonary pressure was measured by placing a cannula in theesophagus, which was connected to an air pressure transducer (TRD5700, Buxco Electronics, USA). One port of the air pressure transducerwas attached to a sidearm adapter of the plethysmograph box thatwas connected to esophageal cannula and the other port was left opento the atmosphere. Airflow and transpulmonary pressure wererecorded using Biosystem XA software with R/C analyser (BuxcoElectronics, USA), which calculated lung resistance (RL) on a breath-by breath basis.
Following stabilization of respiratory parameters saline was admin-istered intravenously and basal RL was recorded. Average lungresistance for first two minutes was tabulated and was taken as thebaselineRL. Thiswas followed by administration of carbachol (16 μg/kg)and the increase in RL from baseline computed. Data was expressed aspercentage increase in RL from baseline values. Percent inhibition intreated animals was computed using the following formula.
% Inhibition =% Increase in R
LVEH� % Increase in R
L TEST
% Increase in RLVEH
× 100
where,
% Increase in RL TEST % Increase in RL from basal value obtained in thepresence of a given dose of test/standardcompound after administration of methacholine(16 μg/kg).
% Increase in RL VEH % Increase in RL from basal value obtained invehicle treated animals after administration ofmethacholine(16 μg/kg).
2.3.3. Effect of RBx 343E48F0 in methacholine-inducedbronchoconstriction in anaesthetized mechanically ventilated rat
The efficacy of RBx 343E48F0 was evaluated in mechanicallyventilated rats and compared with aclidinium bromide. Tiotropiumwas used as method control. Rats were administered vehicle (0.25%methylcellulose) or test compounds intratracheally under transientisoflurane anaesthesia. RBx 343E48F0 and tiotropium were dissolvedin 0.25% methylcellulose whereas aclidinium was administered as asuspension. Two hours after instillation of drug or vehicle, animalswere anaesthetized with urethane (1.2 g/kg, i.p.) and heparinised
222 S. Gupta et al. / European Journal of Pharmacology 658 (2011) 219–228
polyethylene catheters inserted into the carotid artery for recordingthe blood pressure via an MLT 844 transducer (AD instruments) onPowerLab Systems (AD Instruments) and into the jugular vein foradministration of methacholine. Animals were tracheotomised and atracheal cannula inserted. After completion of surgical proceduresanimals were placed in a plethysmograph box (PLY 3114, BuxcoElectronics). To abolish spontaneous breathing, succinylcholine(5 mg/kg) was administered subcutaneously. Following suppressionof spontaneous respiration, rats were mechanically ventilated withatmospheric air through the tracheal cannula using a ventilatorequipped with the Elan® RC system (Buxco Electronics, USA). Theventilator was adjusted to 90 strokes min−1 with a tidal volume of7 ml kg−1. Airflow in the plethysmograph box was measured using anairflow transducer (TRD 5707, Buxco Electronics) and transpulmon-ary pressure was measured by an air pressure transducer (TRD 4517,Buxco Electronics) as the pressure difference between the trachea andoesophagus. Airflow and transpulmonary pressure were monitoredby Biosystem XA software version 2.11 which calculates lungresistance (RL) on a breath-by-breath basis.
Subsequent to stabilization of haemodynamic and respiratoryparameters, rats were intravenously administered saline and recordingof RL was performed for 3 min. Average values obtained after salineadministration were taken as basal RL. This was followed by adminis-tration of methacholine (16 μg/kg, i.v.). The maximal increase in RL
within one min of administration of methacholine was used for all thecalculations and was expressed as the percent of saline response(baseline value). The percentage increase in RL values from eachtreatment group were pooled and expressed as mean±S.E.M. Percentinhibition in the treated animals was computed using the followingformula.
% Inhibition =% Increase in RL VEH � % Increase in RL TEST
% Increase in RL VEH× 100
where,
Percent Increase in RL TEST % increase in RL from basal value obtainedin the presence of a given dose of test/standard compound after administrationof methacholine (16 μg/kg).
Percent Increase in RL VEH % increase in RL from basal value obtainedin vehicle treated animals after adminis-tration of methacholine (16 μg/kg).
2.3.4. Time course of bronchospasmolytic activity of RBx 343E48F0 inanaesthetized rat
The time course of the bronchospasmolytic activity of RBx343E48F0 was studied in anaesthetized rats and compared totiotropium. For this purpose, animals were prepared as describedabove and subsequent to stabilization of haemodynamic parameters,saline was administered intravenously and baseline RL values wererecorded for 3 min. Values obtained after saline administration weretaken as basal RL. This was followed by administration of methacho-line (16 μg/kg, i.v). The maximal increase within 1 min of adminis-tration of methacholine was taken as the response and the changefrom basal RL was calculated. At least two consecutive and stableresponses to methacholine were obtained to verify the stability of thetest system. Between two successive administrations ofmethacholine,a time interval of 5–10 min was allowed. This was followed byintratracheal instillation of vehicle or test compounds directlythrough the tracheal cannula. Animals were allocated into threegroups receiving vehicle (normal saline), RBx 343E48F0 (3 μg/kg) andtiotropium (1 μg/kg). To facilitate the distribution of vehicle or testcompounds in the airways, two successive insufflations of atmo-spheric air were delivered (volume=1.5 ml) through a syringe.
Methacholine challenge was repeated at 5, 15, 25, 35, 45 and 60 minpost-instillation.
The maximal increase in RL obtained after administration ofmethacholine(16 μg/kg) was expressed as the percent of salineresponse (baseline value). The average of two consecutive methacho-line responses were averaged and considered as the pre-treatmentvalue. The effect of treatment at different time-points was expressedas the percentage of the pre-treatment response. The percentageinhibition in the test or reference substance treated groups wascalculated using the following formula.
% Inhibition =% Change in RL VEH � % Change in RL TEST
% Change in RL VEH× 100
where,
% Change RL TEST % change in RL from pre-treatment value obtained inthe presence of a given dose of test/referencecompound after the administration of methacholine(16 μg/kg).
% Change RL VEH % change in RL from pre-treatment value obtained inthe vehicle treated animals after administration ofmethacholine (16 μg/kg).
2.3.5. Effect of RBx 343E48F0 on acetylcholine-inducedbronchoconstriction in conscious rat
Animals were allocated into five groups receiving vehicle(phosphate buffered saline), RBx 343E48F0 (0.3, 1, and 3 μg/kg) andtiotropium(1 μg/kg). On the day of the study, animals were anaes-thetized with ketamine (40 mg/kg) and xylazine (5 mg/kg) injectedintraperitoneally, and vehicle or study drugs were instilled intra-tracheally. Two, eight and twenty four hours post-drug instillation theanimals were transferred to a whole body plethysmograph (BuxcoElectronics, USA). The animals were allowed to acclimatize in thebody box and the basal respiratory parameters were recorded onlineusing Biosystem XA software (PLY 3215, Buxco Electronics, USA). Thiswas followed by successive challenges, each of 2 min duration, withphosphate buffered saline (vehicle for acetylcholine), and thenacetylcholine (i.e. 0.3, 0.6, 1, 3, 6, 12, 24, 48, 72, 96, 144 and192 mg/kg). Following each acetylcholine challenge, respiratoryparameters were recorded for 5 min. A gap of 2–3 min was allowedfor the animals to recover and they were then challenged with thenext higher dose of acetylcholine. This step was repeated until airwayresistance (Penh) of rats attained two-fold of the baseline value i.e.the value obtained after challenging the animal with phosphatebuffered saline. For recording basal respiratory parameters and theresponse to phosphate buffered saline challenge, three consecutive1 min readings were averaged. Each 1 min reading represents anaverage value of each breath taken in that 1 min duration. Followingacetylcholine challenge data was recorded for 5 min respectively.Each 5 min period represents an average of five recordings at one minapart, respectively. Each 1 min recording was an averaged value of allthe breath in 1 min. Penh values (index of airway resistance) in eachrat were obtained in the presence of PBS and different doses ofacetylcholine at different time points. Penh, at any chosen dose ofacetylcholine was expressed as the percent of phosphate bufferedsaline response. The percent of phosphate buffered saline responsevalues thus calculated were fed into Graph Pad Prism software(GraphPad Software Inc., USA, version 4.0) and using point-to pointanalysis the PC100 (2-fold of phosphate buffered saline value) valuewas computed. Data from each group of animals at various time-points were expressed as mean±S.E.M.
2.3.5.1. Statistical analysis. The effect of test or standard substance onany parameter at any time-point post-dosing was determined by
223S. Gupta et al. / European Journal of Pharmacology 658 (2011) 219–228
comparison with the respective vehicle control group using a one-way analysis of variance followed by Dunnett's multiple comparisontest. GraphPad Prism software, version 4 (GraphPad Software Inc.,USA) was used for all statistical analyses. A P value of ≤0.05 wasconsidered statistically significant.
2.3.6. Pharmacokinetics in ratA single dose pharmacokinetic study inWistar rat (220±20 g) was
carried out following 5 mg/kg oral, 1 mg/kg intravenous and 1 mg/kgintratracheal administration of 1, 0.5 and 1 mg/ml solution respectively,prepared in physiological saline. Animals were fasted for 12 h beforeand 2 h post-dosing. Water was allowed throughout the study period.Serial plasma samples, from ~300 μL bleeds, were obtained under etheranesthesia from the orbital venous sinus at predose, at 0.08 h (onlyintratracheal dosed animals), 0.12 h(only intravenous dosed animals)and at 0.25, 0.5, 1, 2, 4, 8, 12 and 24 h post-dose (from all dose groups).
2.3.7. Lung disposition and retention study in ratRBx 343E48F0 at a concentration of 0.5 and 1 mg/ml in
physiological saline was administered to Wistar rats (220±20 g) at1 mg/kg intravenous and intratracheal doses, respectively. Theintravenous dose was given as a 15 min infusion through the tailvein. Lung samples were collected from intravenously dosed animalsat 0.5, 2, 6, 12 and 24 h from the start of infusion and fromintratracheally dosed animals at 0.25, 1, 3, 6, 12 and 24 h post-dose.At each sampling time, three rats were sacrificed and lung sampleswere homogenized in ice cold pH 7.4 phosphate buffer and analysedfor RBx 343E48F0 by LC-MS/MS.
2.3.8. Brain to plasma ratioFollowing a single intravenous 10 mg/kg dose to Wistar rats, brain
and systemic blood samples were collected at 0.25, 1, 3, 6, 12, 24 and48 h post-dose. Plasma was harvested from blood samples and thebrain samples homogenized in ice cold pH 7.4 phosphate buffer andanalysed for RBx 343E48F0 by LC-MS/MS.
3. Results
3.1. In vitro studies
3.1.1. Binding affinity for human recombinant muscarinicreceptor subtypes
The affinity of RBx 343E48F0 at human muscarinic receptorsubtypes was evaluated in competitive radioligand binding assaysusing [3H] N-methyl scopolamine. RBx 343E48F0 exhibited highaffinity for the M3 receptor with a pKi value of 9.6 and had an M3 vs.M2 selectivity of 60-fold. Tiotropium was non-selective (Table 1).
Table 1Binding affinity, functional potency and duration of action of RBx 343E48F0 andtiotropium.
Competitive binding assays were conducted using membrane preparations from CHOcells stably transfected with human M1, M2, M3, M4 and M5 subtypes using [3H] NMSas the ligand. Non-specific binding was determined in the presence of 1 μM atropine(n=3). Functional antagonism is expressed as pKB (Mean±S.E.M.); t1/2[onset]=timefrom start of administration of the test antagonists to attainment of 50% inhibition ofthe cholinergic neural response and t1/2 [offset]=time from washout of the testantagonists to attainment of 50% recovery of cholinergic response (n=3).
3.1.2. In vitro functional assaysIn guinea pig trachea, carbachol produced a concentration depen-
dent increase in the force of tissue contraction. The potency andmaximumcontractile responseof trachea to carbachol in vehicle treatedgroups prior to exposure to RBx 343E48F0 and tiotropiumwere similar(Table 2). Treatment with RBx 343E48F0 shifted the carbacholconcentration response curve to the right in a concentration dependentmanner (Fig. 2)with pD2 of carbachol shifted nearly 100-fold to 4.7-foldin the presence of 30 nM of RBx 343E48F0 (Table 2). The maximumcontractile responseof trachea to carbachol (1.5±0.5 g) in thepresenceof 30 nM RBx 343E48F0 was very similar to that seen in the vehicletreated group (Table 2). Tiotropium shifted the concentration responseto carbachol to the right, at the same time it suppressed the maximumresponse of trachea to carbachol (Fig. 2). The peak response of carbacholin the presence of 3 nM tiotropium was 0.4±0.3 g (Table 2). Thepotencies of RBx 343E48F0 (pKB: 9.5) and tiotropium (pKB: 10) forantagonising the carbachol response were comparable (Table 1).
In electrically field-stimulated trachea (Fig. 3; Table 1), RBx343E48F0 exhibited a faster onset of inhibitory effect (t1/2 onset:29 min) than tiotropium (t1/2 onset: 43 min). The long association ofRBx 343E48F0 (t1/2 offset: 118 min) with the M3 receptor in theisolated trachea was shorter, however, than that of tiotropium (t1/2offset: N240 min) (Fig. 3; Table 1). Contractile responses obtainedwith EFS were completely blocked by atropine [10−5 M] or quinidine[10−4M] which indicates that the contractions were caused bycholinergic nerves stimulation.
3.2. In vivo efficacy
3.2.1. Effect of RBx 343E48F0 on carbachol-induced bronchoconstrictionin anaesthetized spontaneously breathing rats
In vehicle treated animals, the basal RL was 0.22±0.02 cmH2O ml−1
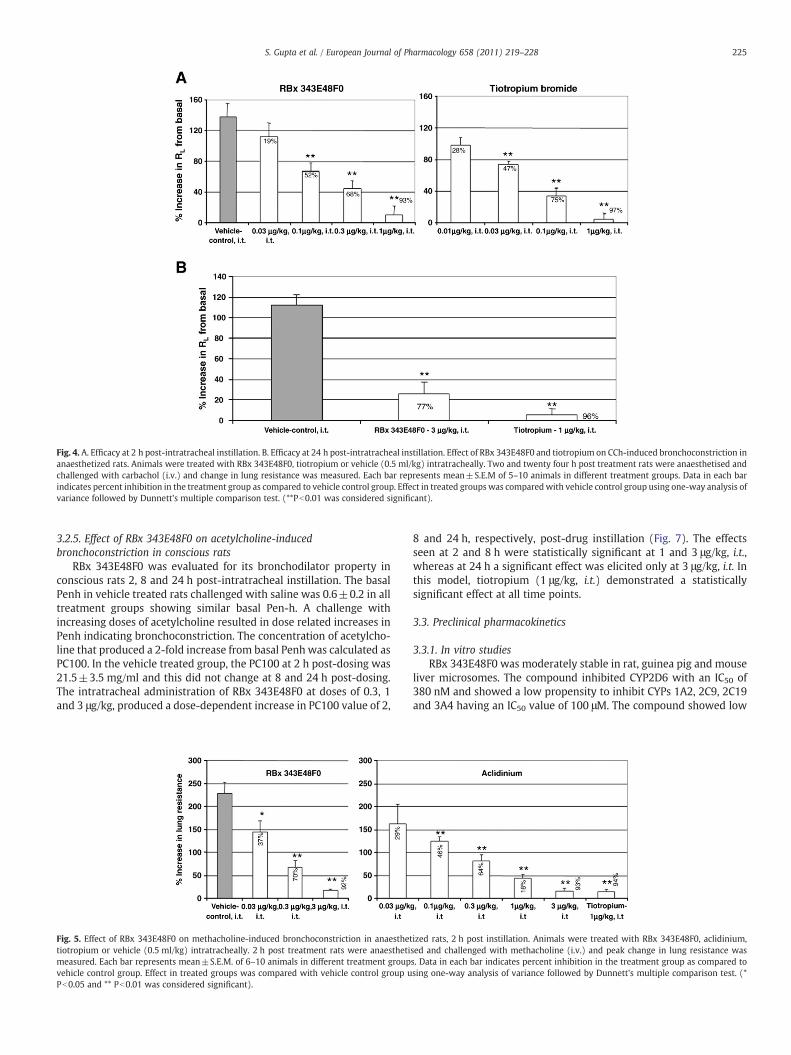
s−1. In rats administered carbachol (16 μg/kg, i.v.), RL increased morethan two-fold to 0.5±0.06 cmH2O ml−1s−1, representing a 138±18%increase in RL (Fig. 4A). RBx 343E48F0 administered intratracheally atdoses of 0.03, 0.1, 0.3 and 1 μg/kg demonstrated a potent and dose-dependent inhibition of the carbachol-induced increase in lungresistance (ED50=0.11 μg/kg, Fig. 4A). Tiotropium, similarly, adminis-tered at doses of 0.01, 0.03, 0.1 and 1 μg/kg, showed a dose-dependentinhibition of the carbachol-induced increase in lung resistance(ED50=0.033 μg/kg). In this study, RBx 343E48F0 was nearly 3.3-foldless potent than tiotropium.
3.2.2. Effect of RBx 343E48F0 in methacholine-inducedbronchoconstriction in anaesthetized mechanically ventilated rats
In this study, the efficacy of RBx 343E48F0 and aclidinium bromidewas determined in methacholine-induced bronchoconstriction inmechanically ventilated anaesthetized rats. In vehicle treated animals,the basal RL was 0.31±0.02 cmH2O ml−1s−1. A challenge with
Table 2Comparative functional potencies and maximum response of RBx 343E48F0 &Tiotropium to carbachol in guinea pig trachea (M3).
Data expressed as Mean values±S.E.M; pD2 : the negative log10 (EC50); Emax:maximum tension developed; n: number of experiments a: Pb0.05 vs. correspondingcontrol; ns: not significant in comparison to corresponding control (PN0.05).
25 50 75 100 125-25
25
75
125
Control[n=4]
Tiotropium-1nM[n=4]
RBx 343E48F0-1nM[n=4]
A Onset of action
Time[mins]
Time[mins]
% In
hib
itio
n o
f C
ho
liner
gic
Res
po
nse
s%
Inh
ibit
ion
of
Ch
olin
erg
icR
esp
on
ses
50 100 150 200 250 300-25
25
75
125
Control[n=4]
Tiotropium-1nM[n=4]
RBx 343E48F0-1nM[n=3]
B Offset of action
Fig. 3. Duration of action of RBx 343E48F0 and tiotropium in guinea pig trachea. Durationof action of RBx 343E48F0 and tiotropium in guinea pig trachea. Data expressed as percentof basal response in each tissue. Each data point represents mean±S.E.M. of number ofexperiments shown in parenthesis.
-10 -9 -8 -7 -6 -5 -4 -3 -20
25
50
75
100
Control 1nM(n=2)
3nM(n=3) 10nM(n=4)
30nM(n=3)
A Effect of RBx 343E48F0
-Log[Carbachol](M)
-Log[Carbachol](M)
% C
on
tro
l Res
po
nse
% C
on
tro
l Res
po
nse
-10 -9 -8 -7 -6 -5 -4 -3 -20
25
50
75
100
Control(n=9) 0.1nM(n=3)
1nM(n=4) 3nM(n=2)
B Effect of Tiotropium
Fig. 2. Antimuscarinic effect of RBx343E48F0 and tiotropium inguineapig trachea. Doublecumulative concentration response curve to carbachol-evoked contractions in guinea pigtrachea.Data expressed asper cent ofmaximumresponse in control tissue. Eachdata pointrepresents mean±S.E.M. of number of experiments shown in parenthesis. RBx 343E48F0and tiotropium produced concentration dependent rightward shift in carbacholconcentration response curve in guinea pig trachea.
224 S. Gupta et al. / European Journal of Pharmacology 658 (2011) 219–228
methacholine (16 μg/kg i.v.) increased the lung resistance by morethan 3-fold to 0.99±0.07 cmH2O ml−1s−1, representing a 228±24%increase in RL (Fig. 5). Intratracheal administration of RBx 343E48F0produced a potent and dose-related inhibition of the methacholine-induced increase in lung resistance with 37, 70 and 92%, inhibition atthe doses of 0.03, 0.3 and 3 μg/kg, respectively (ED50=0.076 μg/kg)(Fig. 5). Aclidinium also showed a potent and dose-dependentinhibition of the methacholine-induced increase in lung resistance(Fig. 5) with an ED50 value of 0.14 μg/kg. Tiotropium (1 μg kg−1) wasused as a method control in this study and it demonstrated a 94%inhibition of methacholine-induced bronchoconstriction.
3.2.3. Onset of action of RBx 343E48F0 in anaesthetized mechanicallyventilated rats
To assess onset of effect of RBx 343E48F0 and tiotropium,equiactive doses based on efficacy studies were chosen. The doseschosen for RBx 343E48F0 and tiotropium for intratracheal adminis-tration were 3 and 1 μg/kg, respectively. The intratracheal instillationof vehicle did not elicit any significant change in the bronchocon-strictor response to the methacholine administration from the basalvalues up to 1 h (data not shown). Basal RL in the vehicle controlgroup was 0.25±0.01 cmH2O ml−1s−1. Methacholine (16 μg/kg i.v.)increased lung resistance 5 min post-dosing to118±28% of the basalresponse. The methacholine response remained stable from 5 min to60 min. RBx 343E48F0 inhibited the methacholine response by 84±4% from 5 min onwards which remained constant up to 60 min(Fig. 6). In tiotropium (1 μg/kg) treated animals, a 64±5% inhibition
of the methacholine response was seen at 5 min post-dosing, withpeak inhibition (83±4%) observed at 35 min post-dosing.
3.2.4. Duration of action of RBx 343E48F0 in anaesthetized ratsThe inhibitory effect of RBx 343E48F0 on the carbachol-induced
increase in lung resistance in spontaneously breathing animals as wellas in mechanically ventilated animal was used to examine duration ofaction. In spontaneously breathing rats 24-h post vehicle treatment,basal RL was 0.2±0.02 cmH2O ml−1s−1. Carbachol (16 μg/kg, i.v.)challenge produced a greater than two-fold increase in lung resistance(0.43±0.04 cmH2O ml−1s−1) representing a percent increase in RL of112±9%. In animal treated with RBx 343E48F0 (3 μg/kg i.t.), thebasal RL of 0.2±0.01 cmH2O ml−1 s−1 was increased to 0.26±0.02 cmH2O ml−1s−1 following carbachol challenge implying a 77%inhibition of carbachol-induced increase in lung resistance (Fig. 4B)and a duration of action N24 h. In the same model 24-h posttreatment, tiotropium (1 μg/kg, i.t.) showed a statistically significant96% inhibition of carbachol-induced bronchoconstriction (basal RL of0.23±0.02 cmH2O ml−1s−1 increased to 0.24±0.01 cmH2Oml−1s−1
following carbachol challenge).In mechanically ventilated rats 36 h post-treatment, basal RL was
0.32±0.01 cmH2Oml−1s−1. Methacholine challenge (16 μg/kg, i.v.)increased lung resistance nearly two-fold to 0.7±0.06 cmH2Oml−1s−1,suggesting a 123±20% increase in RL. RBx 343E48F0 and aclidinium atdoses of 3 μg/kg and tiotropium at a dose of 1 μg/kg were consideredequieffective doses. Thirty six hours post treatment, RBx 343E48F0,aclidinium and tiotropium inhibited the methacholine challenge by60, 67 and 81%, respectively, again indicating a long duration of action(N36 h) for RBx 343E48F0.
Fig. 4. A. Efficacy at 2 h post-intratracheal instillation. B. Efficacy at 24 h post-intratracheal instillation. Effect of RBx 343E48F0 and tiotropium on CCh-induced bronchoconstriction inanaesthetized rats. Animals were treated with RBx 343E48F0, tiotropium or vehicle (0.5 ml/kg) intratracheally. Two and twenty four h post treatment rats were anaesthetised andchallenged with carbachol (i.v.) and change in lung resistance was measured. Each bar represents mean±S.E.M of 5–10 animals in different treatment groups. Data in each barindicates percent inhibition in the treatment group as compared to vehicle control group. Effect in treated groupswas comparedwith vehicle control group using one-way analysis ofvariance followed by Dunnett's multiple comparison test. (**Pb0.01 was considered significant).
225S. Gupta et al. / European Journal of Pharmacology 658 (2011) 219–228
3.2.5. Effect of RBx 343E48F0 on acetylcholine-inducedbronchoconstriction in conscious rats
RBx 343E48F0 was evaluated for its bronchodilator property inconscious rats 2, 8 and 24 h post-intratracheal instillation. The basalPenh in vehicle treated rats challenged with saline was 0.6±0.2 in alltreatment groups showing similar basal Pen-h. A challenge withincreasing doses of acetylcholine resulted in dose related increases inPenh indicating bronchoconstriction. The concentration of acetylcho-line that produced a 2-fold increase from basal Penh was calculated asPC100. In the vehicle treated group, the PC100 at 2 h post-dosing was21.5±3.5 mg/ml and this did not change at 8 and 24 h post-dosing.The intratracheal administration of RBx 343E48F0 at doses of 0.3, 1and 3 μg/kg, produced a dose-dependent increase in PC100 value of 2,
Fig. 5. Effect of RBx 343E48F0 on methacholine-induced bronchoconstriction in anaesthettiotropium or vehicle (0.5 ml/kg) intratracheally. 2 h post treatment rats were anaesthetimeasured. Each bar represents mean±S.E.M. of 6–10 animals in different treatment groupvehicle control group. Effect in treated groups was compared with vehicle control group uPb0.05 and ** Pb0.01 was considered significant).
8 and 24 h, respectively, post-drug instillation (Fig. 7). The effectsseen at 2 and 8 h were statistically significant at 1 and 3 μg/kg, i.t.,whereas at 24 h a significant effect was elicited only at 3 μg/kg, i.t. Inthis model, tiotropium (1 μg/kg, i.t.) demonstrated a statisticallysignificant effect at all time points.
3.3. Preclinical pharmacokinetics
3.3.1. In vitro studiesRBx 343E48F0 was moderately stable in rat, guinea pig and mouse
liver microsomes. The compound inhibited CYP2D6 with an IC50 of380 nM and showed a low propensity to inhibit CYPs 1A2, 2C9, 2C19and 3A4 having an IC50 value of 100 μM. The compound showed low
ized rats, 2 h post instillation. Animals were treated with RBx 343E48F0, aclidinium,sed and challenged with methacholine (i.v.) and peak change in lung resistance wass. Data in each bar indicates percent inhibition in the treatment group as compared tosing one-way analysis of variance followed by Dunnett's multiple comparison test. (*
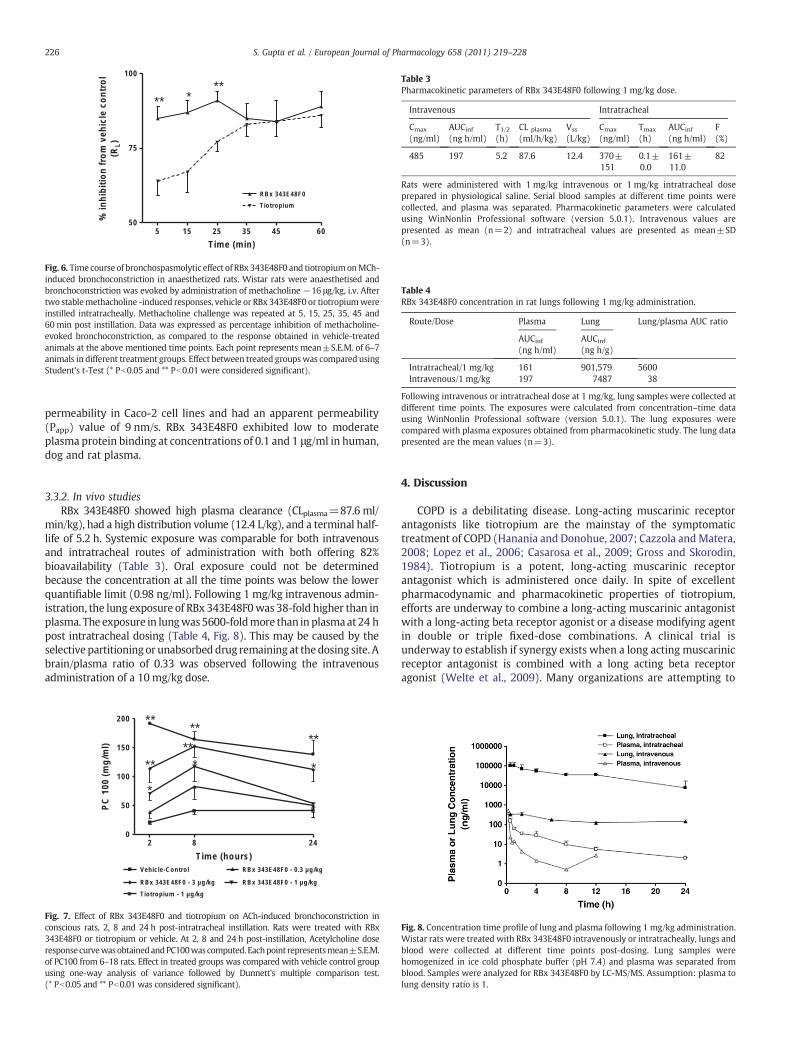
Fig. 6. Time course of bronchospasmolytic effect of RBx343E48F0 and tiotropiumonMCh-induced bronchoconstriction in anaesthetized rats. Wistar rats were anaesthetised andbronchoconstriction was evoked by administration of methacholine −16 μg/kg, i.v. Aftertwo stablemethacholine -induced responses, vehicle or RBx 343E48F0 or tiotropiumwereinstilled intratracheally. Methacholine challenge was repeated at 5, 15, 25, 35, 45 and60 min post instillation. Data was expressed as percentage inhibition of methacholine-evoked bronchoconstriction, as compared to the response obtained in vehicle-treatedanimals at the above mentioned time points. Each point represents mean±S.E.M. of 6–7animals in different treatment groups. Effect between treated groupswas compared usingStudent's t-Test (* Pb0.05 and ** Pb0.01 were considered significant).
Table 3Pharmacokinetic parameters of RBx 343E48F0 following 1 mg/kg dose.
Intravenous Intratracheal
Cmax
(ng/ml)AUCinf(ng h/ml)
T1/2(h)
CL plasma
(ml/h/kg)Vss
(L/kg)Cmax
(ng/ml)Tmax
(h)AUCinf(ng h/ml)
F(%)
485 197 5.2 87.6 12.4 370±151
0.1±0.0
161±11.0
82
Rats were administered with 1 mg/kg intravenous or 1 mg/kg intratracheal doseprepared in physiological saline. Serial blood samples at different time points werecollected, and plasma was separated. Pharmacokinetic parameters were calculatedusing WinNonlin Professional software (version 5.0.1). Intravenous values arepresented as mean (n=2) and intratracheal values are presented as mean±SD(n=3).
Table 4RBx 343E48F0 concentration in rat lungs following 1 mg/kg administration.
Following intravenous or intratracheal dose at 1 mg/kg, lung samples were collected atdifferent time points. The exposures were calculated from concentration–time datausing WinNonlin Professional software (version 5.0.1). The lung exposures werecompared with plasma exposures obtained from pharmacokinetic study. The lung datapresented are the mean values (n=3).
226 S. Gupta et al. / European Journal of Pharmacology 658 (2011) 219–228
permeability in Caco-2 cell lines and had an apparent permeability(Papp) value of 9 nm/s. RBx 343E48F0 exhibited low to moderateplasma protein binding at concentrations of 0.1 and 1 μg/ml in human,dog and rat plasma.
3.3.2. In vivo studiesRBx 343E48F0 showed high plasma clearance (CLplasma=87.6 ml/
min/kg), had a high distribution volume (12.4 L/kg), and a terminal half-life of 5.2 h. Systemic exposure was comparable for both intravenousand intratracheal routes of administration with both offering 82%bioavailability (Table 3). Oral exposure could not be determinedbecause the concentration at all the time points was below the lowerquantifiable limit (0.98 ng/ml). Following 1 mg/kg intravenous admin-istration, the lung exposure of RBx 343E48F0was 38-fold higher than inplasma. The exposure in lungwas5600-foldmore than in plasmaat 24 hpost intratracheal dosing (Table 4, Fig. 8). This may be caused by theselective partitioningor unabsorbed drug remaining at thedosing site. Abrain/plasma ratio of 0.33 was observed following the intravenousadministration of a 10 mg/kg dose.
2 8 240
50
100
150
200
Vehicle-Control RBx 343E48F0 - 0.3 µg/kg
RBx 343E48F0 - 1 µg/kgRBx 343E48F0 - 3 µg/kg
Tiotropium - 1 µg/kg
****
**
****
**
*
Time (hours)
PC
100
(m
g/m
l)
Fig. 7. Effect of RBx 343E48F0 and tiotropium on ACh-induced bronchoconstriction inconscious rats, 2, 8 and 24 h post-intratracheal instillation. Rats were treated with RBx343E48F0 or tiotropium or vehicle. At 2, 8 and 24 h post-instillation, Acetylcholine doseresponse curvewasobtainedandPC100was computed. Eachpoint representsmean±S.E.M.of PC100 from 6–18 rats. Effect in treated groups was compared with vehicle control groupusing one-way analysis of variance followed by Dunnett's multiple comparison test.(* Pb0.05 and ** Pb0.01 was considered significant).
4. Discussion
COPD is a debilitating disease. Long-acting muscarinic receptorantagonists like tiotropium are the mainstay of the symptomatictreatment of COPD (Hanania and Donohue, 2007; Cazzola andMatera,2008; Lopez et al., 2006; Casarosa et al., 2009; Gross and Skorodin,1984). Tiotropium is a potent, long-acting muscarinic receptorantagonist which is administered once daily. In spite of excellentpharmacodynamic and pharmacokinetic properties of tiotropium,efforts are underway to combine a long-acting muscarinic antagonistwith a long-acting beta receptor agonist or a disease modifying agentin double or triple fixed-dose combinations. A clinical trial isunderway to establish if synergy exists when a long acting muscarinicreceptor antagonist is combined with a long acting beta receptoragonist (Welte et al., 2009). Many organizations are attempting to
Fig. 8. Concentration time profile of lung and plasma following 1 mg/kg administration.Wistar rats were treated with RBx 343E48F0 intravenously or intratracheally, lungs andblood were collected at different time points post-dosing. Lung samples werehomogenized in ice cold phosphate buffer (pH 7.4) and plasma was separated fromblood. Samples were analyzed for RBx 343E48F0 by LC-MS/MS. Assumption: plasma tolung density ratio is 1.
227S. Gupta et al. / European Journal of Pharmacology 658 (2011) 219–228
identify amuscarinic receptor antagonist from a different chemical classwith properties comparable to tiotropium (Fitzgerald and Fox, 2007a,2007b). In our search for a distinct chemotype, in the present study wedescribe the preclinical pharmacology of RBx 343E48F0, a novelmuscarinic receptor antagonist. In radioligand binding studies carriedout at equilibrium, RBx 343E48F0 showed high affinity for the M3
receptor with a Ki value of 0.3 nM. In the same study, tiotropiumexhibited 10-fold greater affinity for the M3 receptor subtype. Whiletiotropium did not distinguish between muscarinic receptor subtypes,RBx 343E48F0 exhibited 60-foldM2 vs.M3 receptor selectivity andmorethan 10-fold selectivity over M1, M4 and M5 receptor subtypes. Ligandbinding experiments supported by functional in vitro experiments inisolated guinea pig trachea showed that RBx 343E48F0 antagonised thecarbachol-induced increase in contractile response in a concentration-dependent and competitive manner. In these experiments, RBx343E48F0 was found to have comparable potency to tiotropium.Tiotropiumdemonstratedanunsurmountable antagonism in the guineapig trachea with a depression of Emax at 3 nM. Although tiotropiumexhibited a nearly 10-fold greater affinity forM3muscarinic receptors inligand binding assays, it was only 3-fold potent in isolated tissueexperiment. Although the exact reason for this result is unclear, it ispossible that differences in the physicochemical properties anddifferences in the nature of binding to receptors might contribute tothe results seen with two chemically distinct compounds. This mightcontribute to observed difference in potency in two assays.
In our next series of experiments, we attempted to establish whenadministered intratracheally, does RBx 343E48F0 antagonize musca-rinic agonist mediated increase in contractile response. We found thatintratracheal administration of RBx 343E48F0 to anaesthetized ratsproduced a potent and dose-dependent inhibition of carbachol-induced bronchoconstriction (ED50=110 ng/kg) 2 h post-drug instil-lation. In the same study, tiotropium administered intratracheallyexhibited an ED50 of 30 ng/kg. It is worth observing that rank order ofpotency observed in the isolated tissue experiments is similar to thatseen in in vivo experiments. In another study, the potencies of RBx343E48F0 and aclidinium at antagonizing muscarinic responses werecompared. In this study, RBx 343E48F0 exhibited an ED50 76 ng/kgwhereas aclidinium bromide had an ED50 of 140 ng/kg. It can beconcluded that RBx 343E48F0 exhibited potent antagonism ofmuscarinic receptor mediated bronchoconstriction in vivo.
We studied duration of action of RBx 343E48F0 in rat at 24h post-dosing in anesthetized and conscious rats. In anesthetized and consciousrats, 3 μg/kg RBx 343E48F0 inhibited acetylcholine responses up to 24 h.Themagnitude of antagonistic effect in anesthetized ratswas 67% at 24 h.In a separate study, duration of antagonistic effect of RBx 343E48F0 at36 h was 60% (data not shown). Tiotropium at 1 μg/kg inhibitedmuscarinic responses by more than 80% at 24 and 36 h. Aclidiniumexhibited comparable blockade of muscarinic response at 36 h to RBx343E48F0. Data suggested that although RBx 343E48F0 remained lesspotent and exhibited lesser magnitude of inhibition at 24 and 36 hcompared to tiotropium. However, given the 3-fold lesser potency of RBx343E48F0 in isolated tissue experiments and in vivo studies, it is worthspeculating that increasing dose of RBx 343E48F0 may exhibit compa-rable duration of action of tiotropium. In vivo potency and duration ofaction of RBx 343E48F0 were comparable to that of aclidinium bromide.
The onset of action of RBx 343E48F0 in an anaesthetized rat modelwas 5 min compared to 35 min with tiotropium. Although anexplanation for this observation is not obvious, a similar observationwas made in isolated tissue studies using electrically field stimulatedtracheal strips.
It is known that muscarinic receptors of the M2 subtype are presentat presynaptic terminals (Barnes et al., 1995; Ten Berge et al., 1996).Acetylcholine regulates its own releasebyactingon these autoreceptors.This negative feedback loop will be blocked by tiotropium, and as aresult excess acetylcholine released may interfere with the binding oftiotropium to postsynaptic M3 receptors, resulting in a delay in onset of
action. Because tiotropium dissociates from these receptor slowly, oncetheblockade sets in, it persists for longperiodof time. RBx34348F0has aweak binding to the M2 receptor subtype, and as a result it does notinterfere with the autoregulatory mechanism. It can be postulated,therefore, that the compound might antagonize postsynaptic M3
receptors faster than tiotropium. It is well established that tiotropiumexhibits a long duration of action because of its prolonged binding tomuscarinic receptors. Although RBx 343E48F0 also tends to dissociateslowly fromelectrically-stimulated tracheal strips, this effectmaynot besufficient to explain its long duration of action observed in in vivostudies. In a separate experiment the amount of RBx34348F0 remainingin the lungs following intratracheal administration was shown to benearly 5600-fold higher than in the plasma. This elevated lungconcentration was maintained up to 24 h indicating a good correlationbetween thepharmacodynamic andpharmacodynamic effects. Thiswasconfirmed in a separate study using intravenous administration of RBx343E48F0 in which a 38-fold increase in lung exposure compared toplasma clearly indicated high retention affinity in lung. The longduration of action of RBx 34348F0 is likely to be a combined effect ofhigh lung retention, high intratracheal bioavailability and a moderatelylong terminal half-life (5.2 h), which indicate a good PK-PD co-relation.In a manner similar to tiotropium and ipratropium, RBx 343E48F0 ishighly cleared and extensively distributed into tissues. Its poorgastrointestinal absorption, high plasma clearance and volume ofdistribution may lead to a lower propensity of systemic side effects. Incontrast to the compound's high in vivo plasma clearance, moderateintrinsic clearance was observed in vitro which suggests that theclearance of RBx 343E48F0 is likely to be through non-microsomalmechanisms.We believe that the advantage of kinetic selectivity for M3
and M2 receptors displayed by tiotropium can be achieved by thepotential of “lung accumulation” for our compound (Disse et al., 1993).A low brain to plasma ratio indicated towards lesser probability of CNSrelated adverse events.
Although we have discussed RBx 343E48F0 keeping COPD angle inmind, there is a great potential for muscarinic antagonists with longduration of action in the symptomatic therapy of bronchial asthma(Fitzgerald and Fox, 2007a, 2007b). Both ipratropium and tiotropiumare used in the treatment of asthma in patients that respond poorly tobeta adrenoceptor antagonists. However, it is considered that in thetreatment of bronchial asthma beta adrenoceptor agonists exhibitsuperior efficacy compared to muscarinic antagonists. Muscarinicantagonists have also found utility in the treatment of urinaryincontinence. Recently, we have published a paper describing pharma-cology of a novel muscarinic receptor antagonist for the treatment ofoveractive bladder (Sinha et al., 2010). However, for finding any utilityin the treatment of urinary incontinence, RBx 343E48F0 needs to beadministered by oral route.We have discussed in the preceding sectionsthat RBx 343E48F0 exhibits poor oral bioavailability, thus utility of thiscompound for urinary incontinence may not merit much discussion.
In summary, the results of the present study suggest that RBx343E48F0 a novel muscarinic receptor antagonist from a distinctchemical class capable of antagonizingmuscarinic receptors with highpotency. The antagonistic effect is seen at the level of isolated tissueexperiments as well as in vivo. RBx 343E48F0 exhibited a longduration of action and this effect was supported by its pharmacoki-netic property of being retained in the lung. The compound alsoexhibited a fast onset of action, although it remains to be seen if thiseffect will benefit the overall development of the molecule.
(Ba 679 BR), a novel long-acting muscarinic antagonist for the treatment ofobstructive airways disease. Life Sci. 56, 853–859.
228 S. Gupta et al. / European Journal of Pharmacology 658 (2011) 219–228
Casarosa, P., Bouyssou, T., Germeyer, S., Schnapp, A., Gantner, F., Pieper, M., 2009.Preclinical evaluation of long-acting muscarinic antagonists: comparison oftiotropium and investigational drugs. JPET 330, 660–668.
Cazzola, M., Matera, M.G., 2008. Novel long-acting bronchodilators for COPD andasthma. Br. J. Pharmacol. 155, 291–299.
Cheng, Y., Prusoff, W.H., 1973. Relationship between the inhibition constant (Ki) andthe concentration of inhibitor which causes 50 per cent inhibition (IC50) of anenzymatic reaction. Biochem. Pharmacol. 22, 3099–3108.
Disse, B., Reichl, R., Speck, G., Traunecker, W., Ludwig, Rominger, K.L., Hammer, R., 1993.Ba 679 BR, a novel long-acting anticholinergic bronchodilator. Life Sci. 52, 537–544.
Fitzgerald, M.F., Fox, J.C., 2007a. Emerging trends in the therapy of COPD: novel anti-inflammatory agents in clinical development. Drug Discov. Today 12, 479–486.
Fitzgerald, M.F., Fox, J.C., 2007b. Emerging trends in the therapy of COPD: novel anti-inflammatory agents in clinical development. Drug Discov. Today 12, 472–478.
Fryer, A.D., Jacoby, D.B., 1998. Muscarinic receptors and control of airway smoothmuscle. Am. J. Respir. Crit. Care Med. 158, S154–S160.
Gross, N.J., 2004. Tiotropium bromide. Chest 126, 1946–1953.Gross, N.J., 2006. Anticholinergic agents in asthma and COPD. Eur. J. Pharmacol. 533,
36–39.Gross, N.J., Skorodin, M.S., 1984. Role of the parasympathetic system in airway
obstruction due to emphysema. N. Engl. J. Med. 311, 421–425.Haddad, E., Patel, H., Keeling, J.E., Yocoub, M.H., Barnes, P.J., Belvisi, M.G., 1999.
Pharmacological characterization of the muscarinic receptor antagonist, glycopyr-rolate, in human and guinea-pig airways. Br. J. Pharmacol. 127, 413–420.
Hanania, N.A., Donohue, J.F., 2007. Pharmacologic interventions in chronic obstructivepulmonary disease: bronchodilators. Proc. Am. Thorac. Soc. 4, 526–534.
Kenakin, T., 1993. Synoptic receptor function. Trends Pharmacol. Sci. 14, 431–432.Koumis, T., Samuel, S., 2005. Tiotropium bromide: a new long-acting bronchodilator for
the treatment of chronic obstructive pulmonary disease. Clin. Ther. 27, 377–392.Lopez, A.D., Shibuya, K., Rao, C., Mathers, C.D., Hansell, A.L., Held, L.S., Schmid, V., Buist, S.,
2006. Chronic obstructive pulmonary disease: current burden and future projections.Eur. Respir. J. 27, 397–412.
Moriya, H., Takagi, Y., Nakanishi, T., Hayashi,M., Tani, T., Hirotsu, I., 1999. Affinity profiles ofvarious muscarinic antagonists for cloned human muscarinic acetylcholine receptor(mAChR) subtypes and mAChRs in rat heart and submandibular gland. Life Sci. 64,2351–2358.
Sinha, S., Gupta, S., Malhotra, S., Krishna, N.S., Meru, A.V., Babu, V., Bansal, V., Garg, M.,Kumar, N., Chugh, A., Ray, A., 2010. AE9C90CB: a novel, bladder-selective muscarinicreceptor antagonist for the treatment of overactive bladder. Br. J. Pharmacol. 160,1119–1127.
Ten Berge, R.E., Zaagsma, J., Roffel, A.F., 1996. Muscarinic inhibitory autoreceptors indifferent generations of human airways. Am. J. Respir. Crit. Care Med. 154, 43–49.
Welte, T., Miravitlles, M., Hernandez, P., Eriksson, G., Peterson, S., Polanowski, T.,Kessler, R., 2009. Efficacy and tolerability of budesonide/formoterol added totiotropium in patients with chronic obstructive pulmonary disease. Am. J. Respir.Crit. Care Med. 180, 741–750.