31
Professor Ajay Kakkar Barts and the London School of Medicine Thrombosis Research Institute, London, UK
| Date post: | 01-Jan-2016 |
| Category: |
Documents |
| Upload: | brianne-banks |
| View: | 222 times |
| Download: | 1 times |

Professor Ajay Kakkar
Barts and the London School of Medicine Thrombosis Research Institute, London, UK

Research Support/P.I.Bayer HealthCare, Sanofi-Aventis, Boehringer Ingelheim, Pfizer, Bristol–Myers Squibb, Eisai
Employee N/A
ConsultantBayer HealthCare, Sanofi-Aventis, Boehringer Ingelheim, Pfizer, Bristol–Myers Squibb, Eisai
Major Stockholder N/A
Speakers Bureau N/A
HonorariaBayer HealthCare, Sanofi-Aventis, Boehringer Ingelheim, Pfizer, Bristol–Myers Squibb, Eisai, GSK
Scientific Advisory BoardBayer HealthCare, Sanofi-Aventis, Boehringer Ingelheim, Pfizer, Bristol–Myers Squibb, Eisai
N/A = not applicable (no conflicts)


4
9
26132 132 postoperative postoperative patientspatients
40
92 normal92 normal
Kakkar VV, et al. Lancet. 1969;2:230-232.
Pati
en
ts w
ith
DV
T (
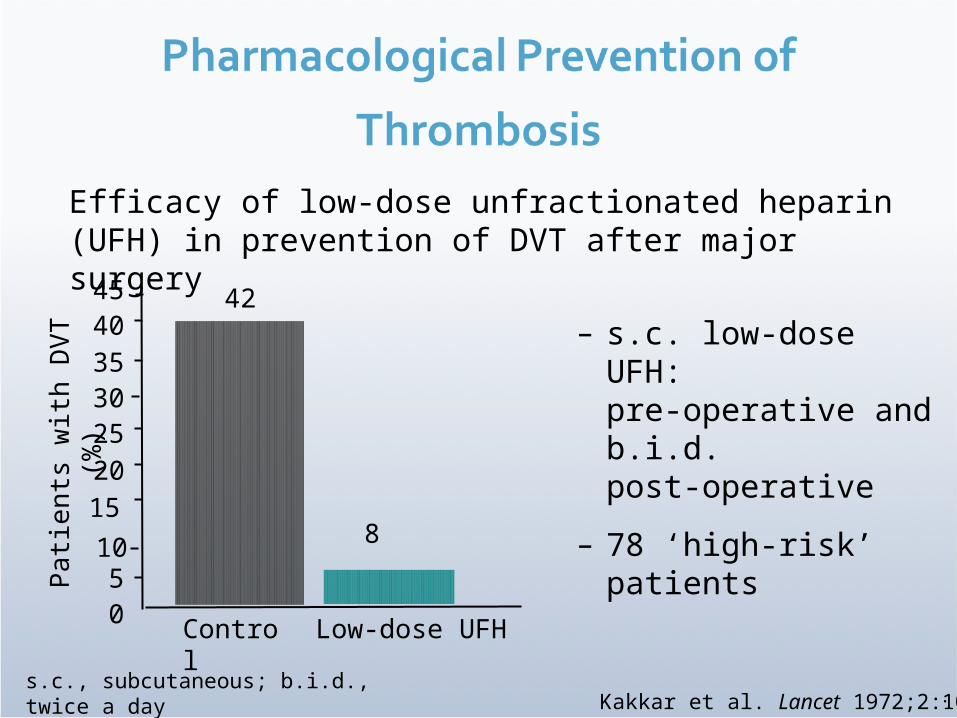
%) 42
8
Control Low-dose UFH
.
Efficacy of low-dose unfractionated heparin (UFH) in prevention of DVT after major surgery
s.c., subcutaneous; b.i.d., twice a day
– s.c. low-dose UFH: pre-operative and b.i.d.post-operative
– 78 ‘high-risk’ patients
05
10
15202530354045
Kakkar et al. Lancet 1972;2:101–6

Kakkar V V et al, Lancet. 1975;2:45-51.

Nu
mb
er
of
pati
en
tsw
ith
fata
l PE
P < 0.005
16
2
02468
1012141618
Control UFH
Low-dose UFH saves 7 lives for every 1000 operated patients.
Kakkar VV et al, Lancet. 1975;2:45-51.
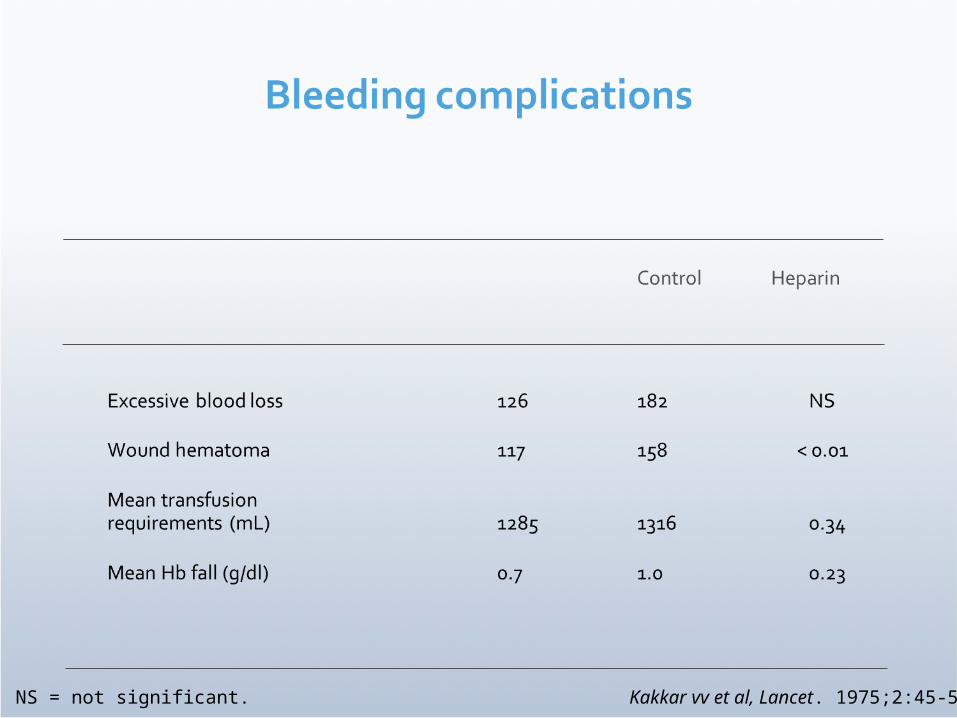
NS = not significant. Kakkar vv et al, Lancet. 1975;2:45-51.

Pre
vale
nce o
f P
roxim
al D
VT (
%)
Asymptomatic DVT
60.5
20.3
RR=67
%
Fatal PE
Fre
qu
en
cy o
f P
E (
%)
RR=68%
Control
UFH
1.9
0.6
Collins R, et al. N Engl J Med. 1988;318:1162-1173.

LMWH
UFH
DVT PE* Major bleeding
25
20
15
10
5
0
RR 0.68
RR 0.43
RR 0.75
Pro
port
ion
of
Pati
en
ts E
xp
eri
en
cin
g
Ou
tcom
e
Nurmohamed MT, et al. Lancet. 1992;340:152-156.
93/672
132/622
10/590
24/582
6/6728/622
0
5
10
15
20
25
Pre
vale
nce o
f D
VT (
%)
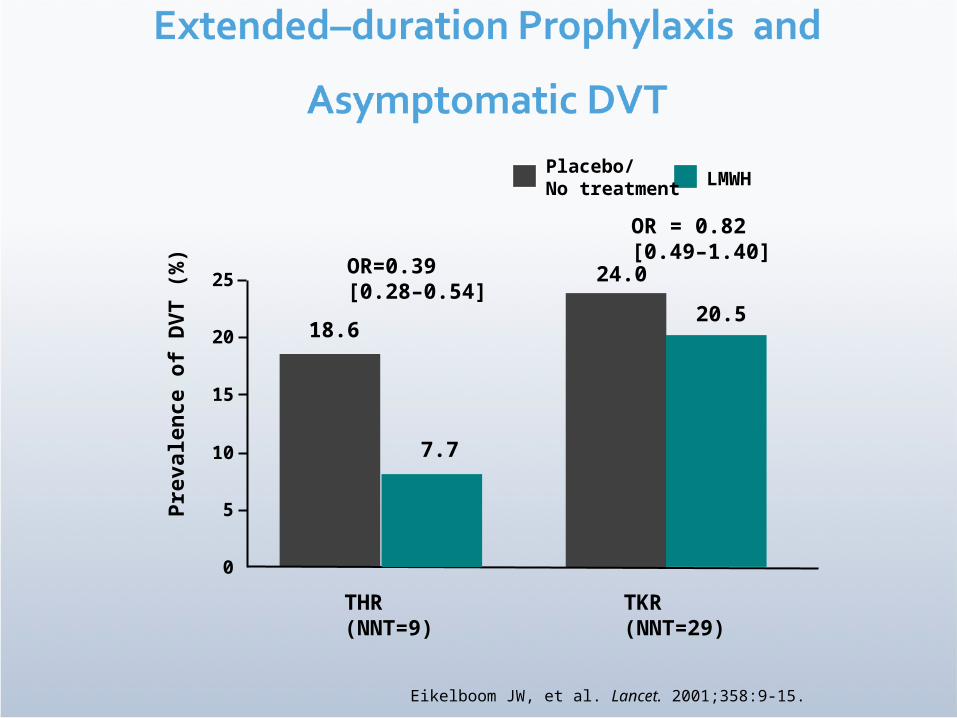
18.6
THR(NNT=9)
OR=0.39[0.28–0.54]
24.0
TKR(NNT=29)
OR = 0.82[0.49–1.40]
7.7
20.5
Eikelboom JW, et al. Lancet. 2001;358:9-15.
Placebo/ No treatment
LMWH

4.3
1.4
OR = 0.33[0.19–0.56]
1.41.0
OR = 0.74[0.26–2.15]
0.0
1.0
2.0
3.0
4.0
5.0
Pre
vale
nce o
f V
TE (
%)
THR(NNT=34)
TKR(NNT=250)
Eikelboom JW, et al. Lancet. 2001;358:9-15.
Placebo/ No treatment
In-hospital prophylaxis followed by: LMWH

Clinical thromboembolism Cancer
0 1.0 2.0 3.0 4.0
Major hemorrhage
Asymptomatic DVT
Clinical PE
Death
Total hemorrhage
Wound hematoma
Transfusion
Non-cancer
Mismetti P et al. Br J Surg 2001;88:913–30.
LMWH better UFH better
Thromboprophylaxis: general surgery
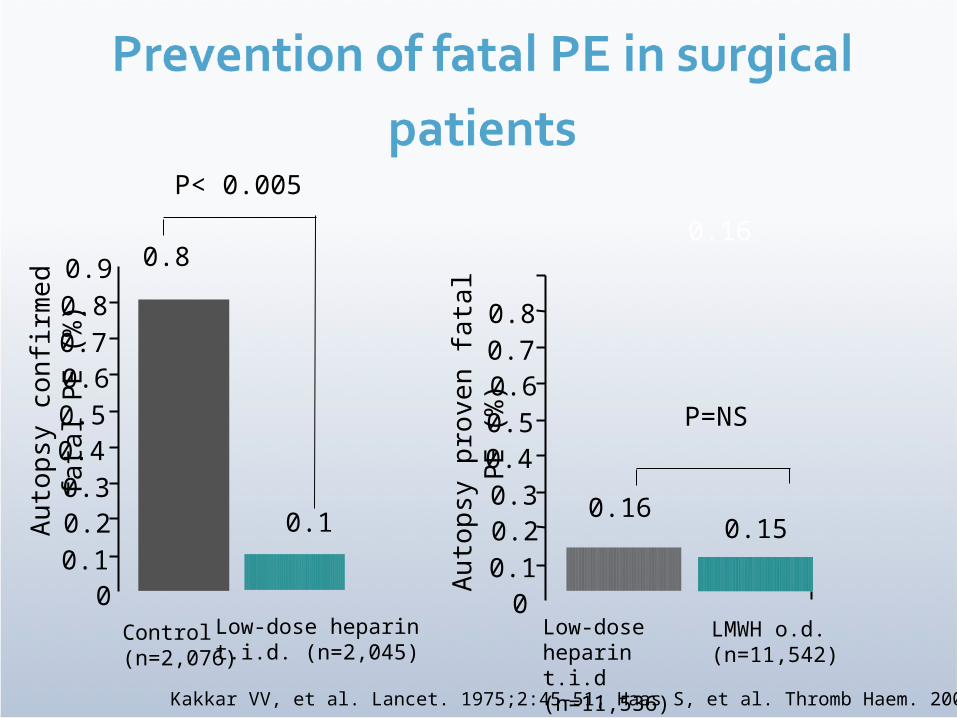
Au
top
sy c
on
firm
ed
fata
l PE
(%
)
Control(n=2,076)
Low-dose heparint.i.d. (n=2,045)
P< 0.005
0.16
0.80.16
Kakkar VV, et al. Lancet. 1975;2:45-51; Haas S, et al. Thromb Haem. 2005;94:814-9.
00.10.20.30.40.50.60.70.80.9
0.1
0.10.20.30.40.50.60.70.8
0
Au
top
sy p
roven
fata
l PE
(%
)0.15
P=NS
Low-dose heparin t.i.d (n=11,536)
LMWH o.d. (n=11,542)

Death (%)
Fatal PE (%)
Non-fatal PE (%)
192 (3.1)
20 (0.31)
5 (0.08)
120 (0.7)
15 (0.09)
4 (0.02)
0.0001
0.0001
Kakkar AK, et al. Thromb Haem 2005. In press
All patients (low-dose UFH or LMWH)
Cancer(n = 6124)
No cancer(n = 16,954)
P
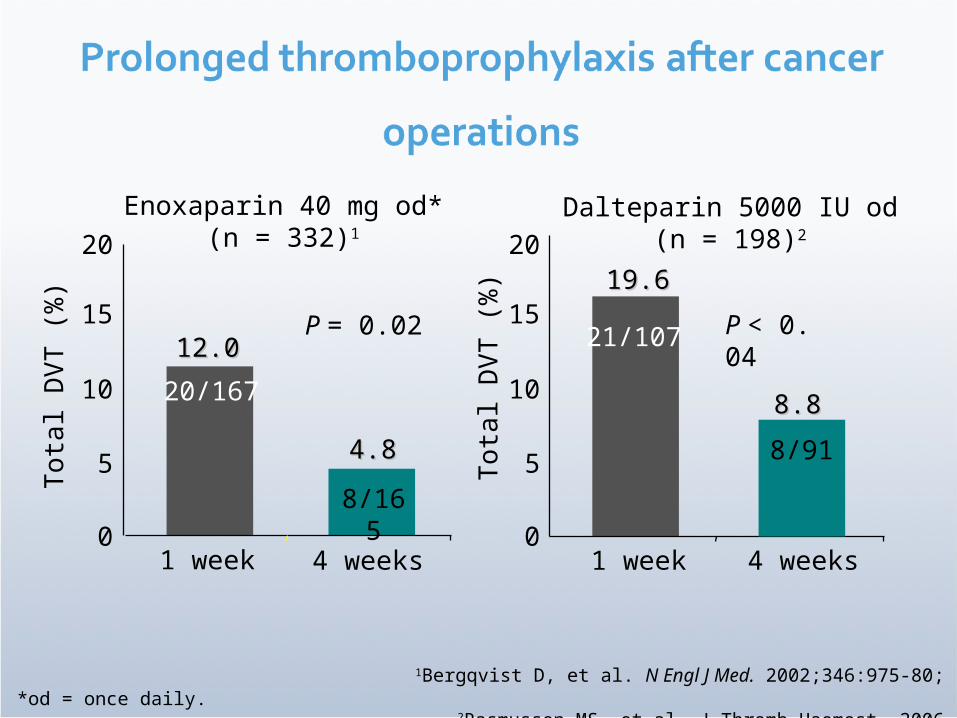
Enoxaparin 40 mg od*(n = 332)1
1Bergqvist D, et al. N Engl J Med. 2002;346:975-80; 2Rasmussen MS, et al. J Thromb Haemost. 2006
Dalteparin 5000 IU od(n = 198)2
*od = once daily.
Tota
l D
VT (
%) 19.619.6
8.88.8
1 week 4 weeks
21/107 P < 0. 04
0
5
10
20
15
Tota
l D
VT (
%)
1 week 4 weeks
1212.0.0
4.84.8
20/167
8/165
P = 0.02
0
5
10
20
15
8/91

Prevention of VTE in Pts Receiving Chemotherapy
Th
rom
boem
bolic E
ven
t (%
) Th
rom
boem
bolic E
ven
t (%
)
16/76916/769 15/38115/381
P= 0.033P= 0.033
RRR = 47.2%
NNT = 54
RRR = 47.2%
NNT = 54
Agnelli G. et al. ASH
2008
Agnelli G. et al. ASH
2008

Geerts et al. Chest 2001; Turpie et al. Arch Intern Med 2002
64.3
56.0
46.8
30.6
12.5
4.87.9
54.2
40.2
22.1
16.1
48.0
34.0
24.027.0
0
10
20
30
40
50
60
70
Placebo/control ASA Warfarin LMWH Fondaparinux
Tota
l D
VT in
cid
en
ce (
%)
Total knee replacement
Total hip replacement
Hip fracture surgery
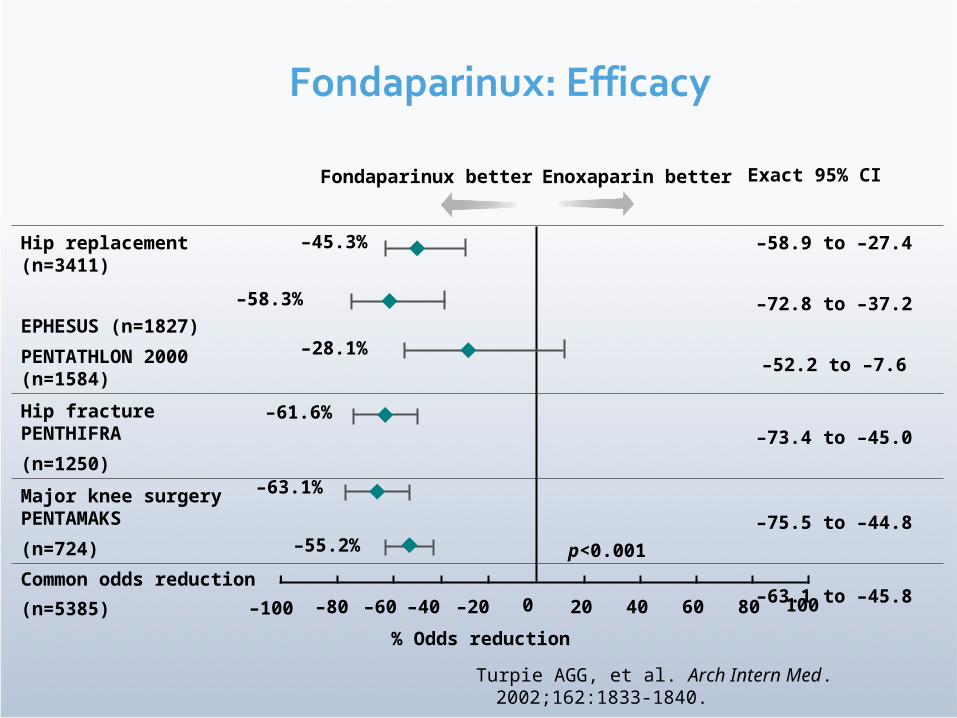
Hip replacement (n=3411)
EPHESUS (n=1827)
PENTATHLON 2000 (n=1584)
–58.9 to –27.4
–72.8 to –37.2
–52.2 to –7.6
Hip fracture PENTHIFRA
(n=1250)
–73.4 to –45.0
Major knee surgery PENTAMAKS
(n=724) –75.5 to –44.8
Common odds reduction
(n=5385)–63.1 to –45.8
Exact 95% CIFondaparinux better Enoxaparin better
–100 –80 –60 –40 –20 200 40 60 80 100
–45.3%
–63.1%
–55.2%
–61.6%
p<0.001
% Odds reduction
–58.3%
–28.1%
Turpie AGG, et al. Arch Intern Med. 2002;162:1833-1840.
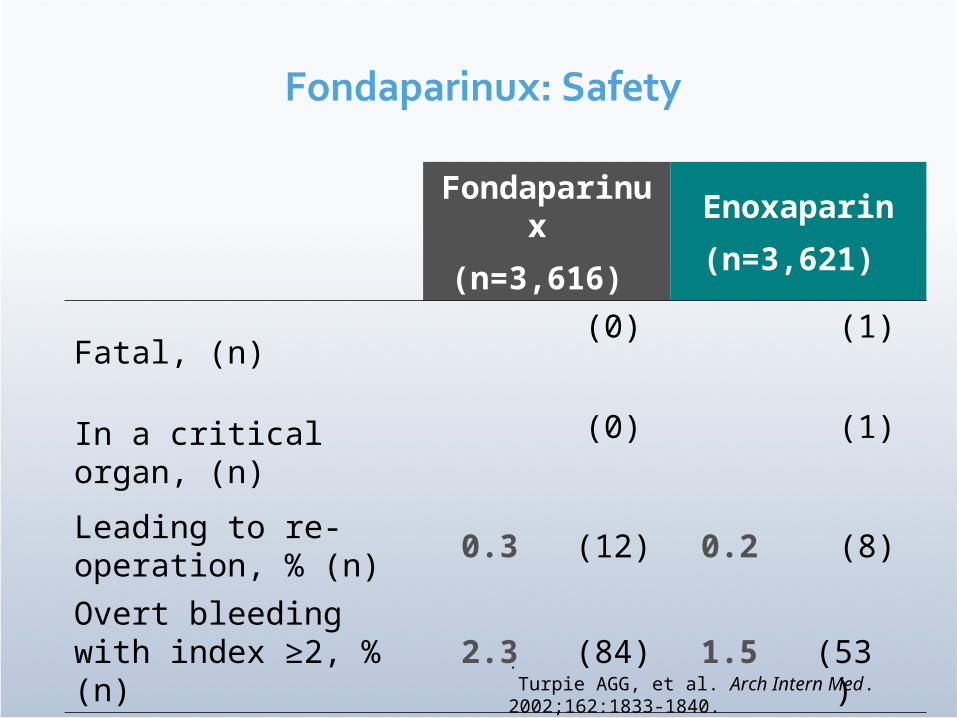
Fondaparinux
(n=3,616)
Enoxaparin
(n=3,621)
Fatal, (n)(0) (1)
In a critical organ, (n)(0) (1)
Leading to re-operation, % (n)
0.3 (12) 0.2 (8)
Overt bleeding with index ≥2, % (n)
2.3 (84) 1.5
(53). Turpie AGG, et al. Arch Intern Med. 2002;162:1833-1840.

MEDENOX1 63% Placebo
Enoxaparin
PREVENT2 49% Placebo
Dalteparin
ARTEMIS 47% Placebo
Fondaparinux
14.9*
5.5
Study RRR Thromboprophylaxis Patients with VTE (%)
5.0*
2.8
10.5†
5.6
*VTE at day 14; †VTE at day 15.1Samama MM, et al. N Engl J Med. 1999;341:793-800.
2Leizorovicz A, et al. Circulation. 2004;110:874-9.3Cohen AT, et al. J Thromb Haemost. 2003;1 (Suppl 1):P2046.
p < 0.001
p = 0.0015
p = 0.029
RRR = relative risk reduction

Studyor subcategory
Cohen 2006Leizorovicz 2004Fraisse 2000Samama 1999
Total (95% CI)
Placebon/N
13 / 42053 / 185010 / 11414 / 371
2755
Anticoagulantn/N
5 / 42927 / 18563 / 1095 / 367
2761
RR (random)95% CI
Weight%
13.0864.968.5713.39
100.00
RR (random)95% CI
0.38 [0.14, 1.05]0.51 [0.32, 0.80]0.31 [0.09, 1.11]0.36 [0.13, 0.99]
0.45 [0.31, 0.65]
0.10.2 0.5 1 2 5 10
FavorsAnticoagulant
FavorsPlacebo
Lloyd NS, et al. J Thromb Haemost. 2008;6:405–414

Studyor subcategory
Cohen 2006Leizorovicz 2004Fraisse 2000Samama 1999
Total (95% CI)
Placebon/N
25 / 420103 / 1850
8 / 11450 / 371
2755
Anticoagulantn/N
14 / 429 107 / 1856
8 / 10941 / 367
2761
RR (random)95% CI
Weight%
12.8051.066.2229.91
100.00
RR (random)95% CI
0.55 [0.29, 1.04]1.04 [0.80, 1.35]1.05 [0.41, 2.69]0.83 [0.56, 1.22]
0.89 [0.70, 1.14]
0.10.2 0.5 1 2 5 10
FavorsAnticoagulant
FavorsPlacebo
Lloyd NS, et al. J Thromb Haemost. 2008;6:405–414
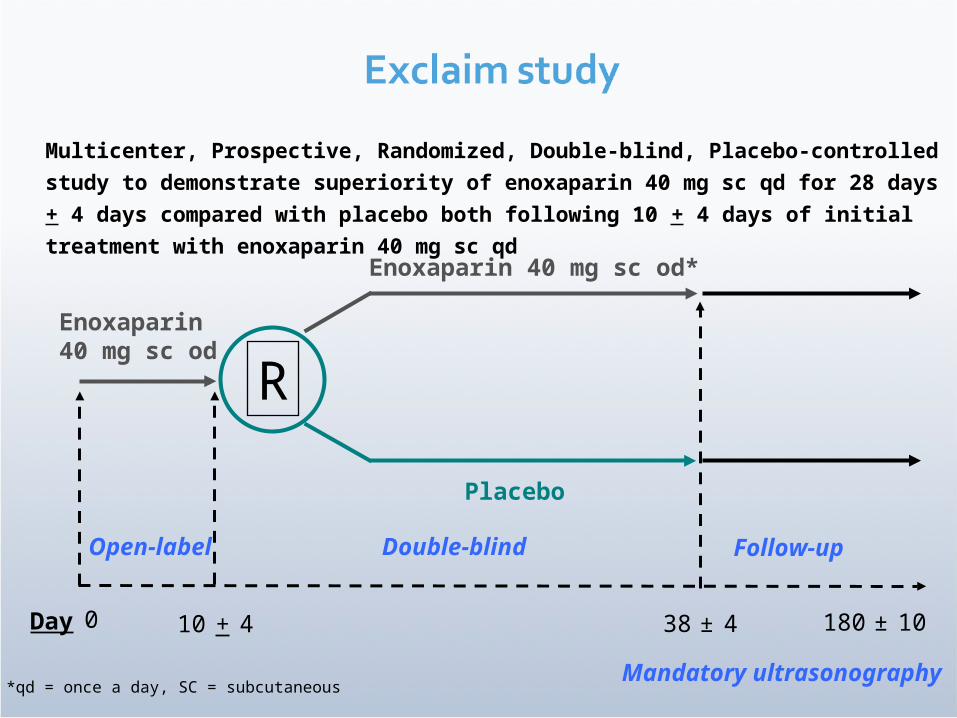
Multicenter, Prospective, Randomized, Double-blind, Placebo-controlled
study to demonstrate superiority of enoxaparin 40 mg sc qd for 28 days +
4 days compared with placebo both following 10 + 4 days of initial
treatment with enoxaparin 40 mg sc qd
10 + 4
Mandatory ultrasonography
0
R
Enoxaparin 40 mg sc od*
Placebo
38 ± 4Day
Follow-up
Enoxaparin40 mg sc od
Open-label Double-blind
180 ± 10
*qd = once a day, SC = subcutaneous

4.9
2.8
3.7
2.5
VTE
Efficacy – VTE Events
Proximal DVT
Symptomatic VTE
1.1
0.3
Placebo
Enoxaparin
Incid
en
ce (%
)
RRR- 44%
RRR
-34%
RRR
-73%
0.20.0
PE
0.10.0
Fatal PE
p = 0.0011
p = 0.0319
p = 0.0044
p = 0.2498
p = 1.0000

3.80
5.70
0.150.60
Total Bleeding
Safety – Bleeding
Major Bleeding
Minor Bleeding
3.70
5.20
Placebo
Enoxaparin
p = 0.007
p = 0.019
p = 0.024
Incid
en
ce (%
)
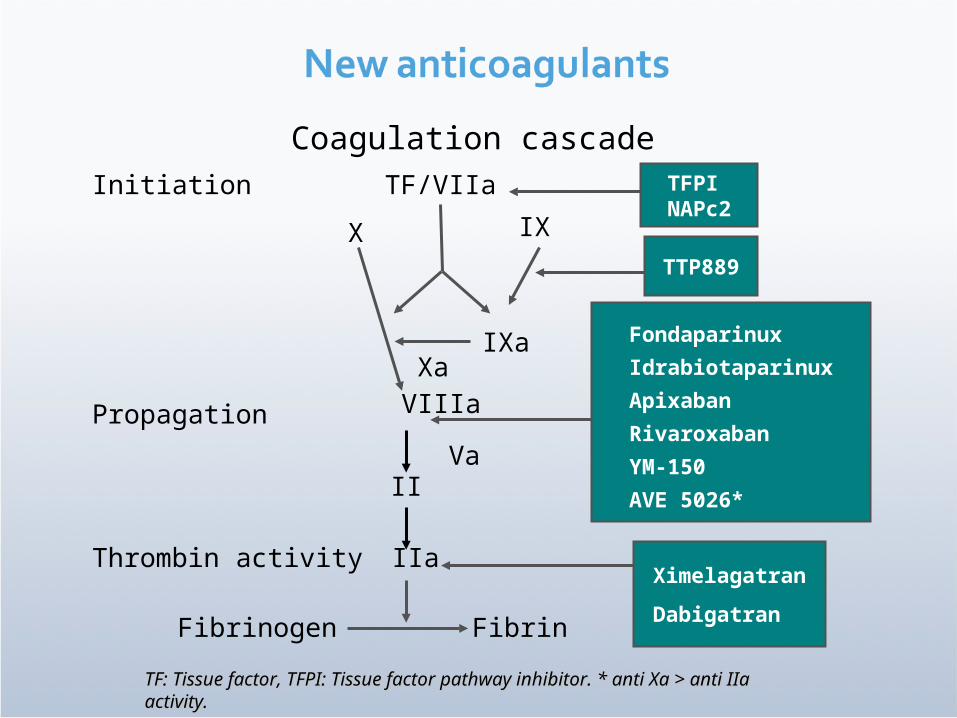
Coagulation cascadeInitiation
Propagation
Thrombin activity
TF/VIIa
VIIIa
IXa
IXX
Xa
VaII
IIa
Fibrinogen Fibrin
TFPINAPc2
TF: Tissue factor, TFPI: Tissue factor pathway inhibitor. * anti Xa > anti IIaTF: Tissue factor, TFPI: Tissue factor pathway inhibitor. * anti Xa > anti IIaactivity.activity.
Fondaparinux
Idrabiotaparinux
Apixaban
Rivaroxaban
YM-150
AVE 5026*
Ximelagatran
Dabigatran
TTP889
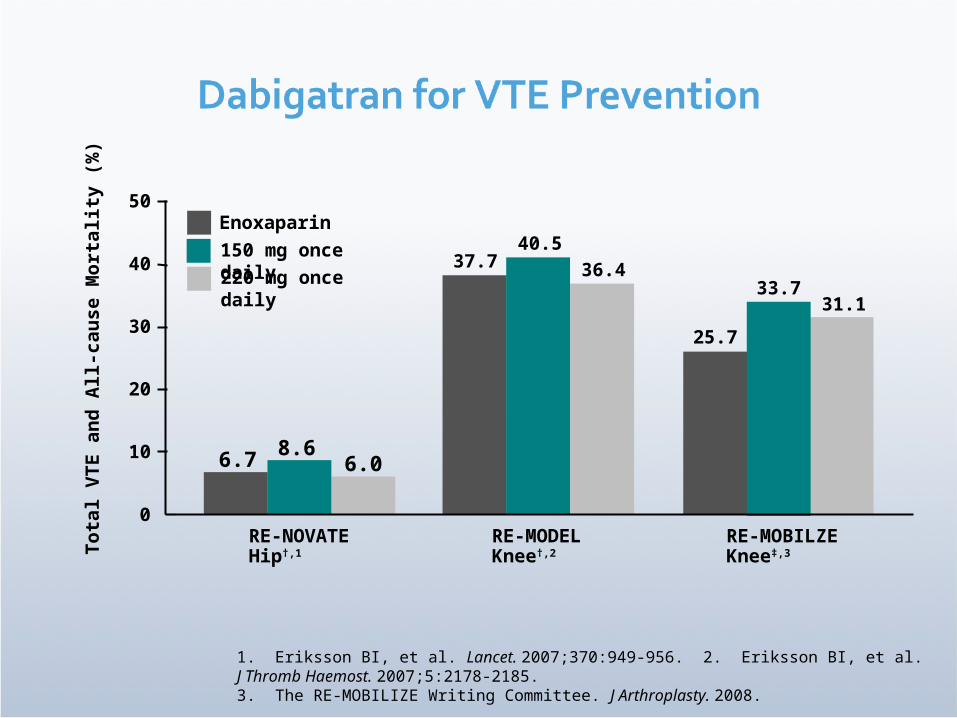
0
10
20
30
40
50
RE-NOVATEHip†,1
Tota
l V
TE a
nd
All-c
au
se M
ort
ality
(%
)
150 mg once daily
RE-MODELKnee†,2
RE-MOBILZEKnee‡,3
8.66.06.7
40.536.437.7
33.731.1
25.7
1. Eriksson BI, et al. Lancet. 2007;370:949-956. 2. Eriksson BI, et al. J Thromb Haemost. 2007;5:2178-2185. 3. The RE-MOBILIZE Writing Committee. J Arthroplasty. 2008.
Enoxaparin
220 mg once daily

Enoxaparin
Dabigatran (150 mg)
Dabigatran (220
mg)
Major VTE, % 3.3 3.8 3.0
Absolute risk difference, %
(95% CI)–
0.5(−0.6−1.6)
−0.2(−1.3−0.9
)
Major bleeding, % 1.4 1.1 1.4
Caprini J, et al. J Thomb Haemost. 2007;5(suppl 2):AO-W-050.

Hip replacement
Rivaroxaban 10 mg o.d.for 35 ± 4 days
vs.
Enoxaparin 40 mg o.d.for 35 ± 4 days
N = 4541
Hip replacement
Rivaroxaban 10 mg o.d.for 35 ± 4 days
vs.
Enoxaparin 40 mg o.d.for 12 ± 2 days
then placebo
N = 2509
Knee replacement
Rivaroxaban 10 mg o.d.for 12 ± 2 days
vs.
Enoxaparin 40 mg o.d.for 12 ± 2 days
N = 2531
Knee replacement
Rivaroxaban 10 mg o.d.
for 12 ± 2 days
vs.
Enoxaparin 30 mg b.i.d.
for 12 ± 2 days
N = 3148 Eriksson BI et al. N Engl J Med 2008;358:2765–75; Kakkar AK et al. Lancet 2008;372:31–9; Lassen MR et al. N Engl J Med 2008;358:2776–86; Turpie AGG et al. Pathophysiol Haemost Thromb 2007/2008;36:A14.