Introduction to medication treatment Introduction to medication treatment approaches for addictive disorders approaches for addictive disorders
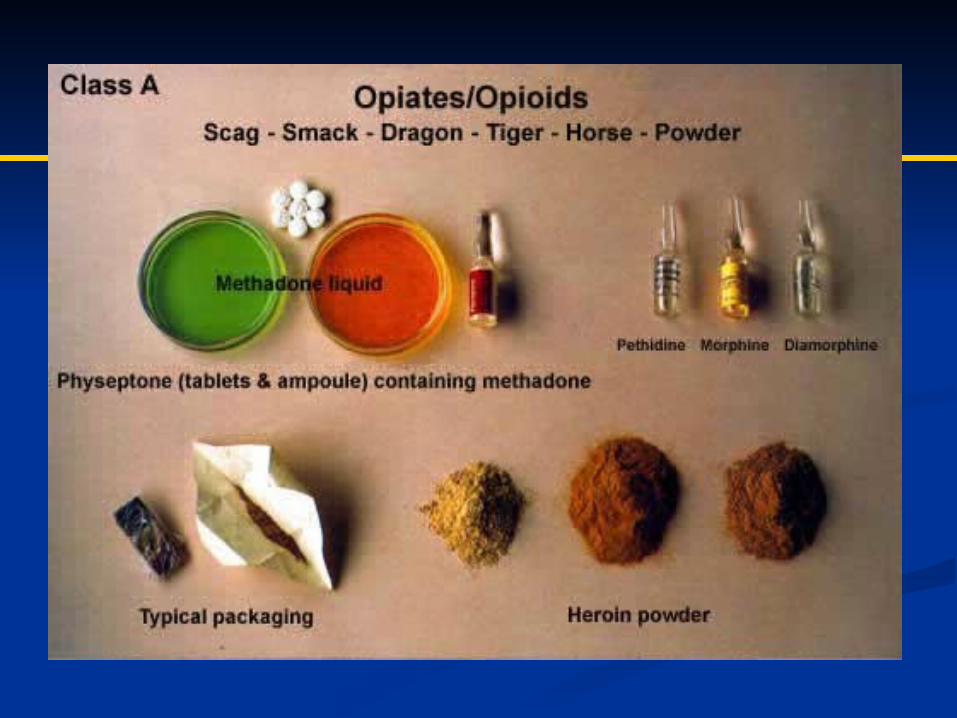
Pharmacological treatment options within Pharmacological treatment options within drug classes:drug classes: AlcoholAlcohol OpioidsOpioids StimulantsStimulants NicotineNicotine
Clinical implications of co-occurring Clinical implications of co-occurring disordersdisorders
IntroductionIntroduction
Addiction is a chronic, relapsing brain Addiction is a chronic, relapsing brain disease characterized by compulsive use disease characterized by compulsive use despite harmful consequencesdespite harmful consequences
Pharmacotherapy as part of Pharmacotherapy as part of multimodalmultimodal treatment plantreatment plan
Thorough evaluation and diagnosis Thorough evaluation and diagnosis essentialessential
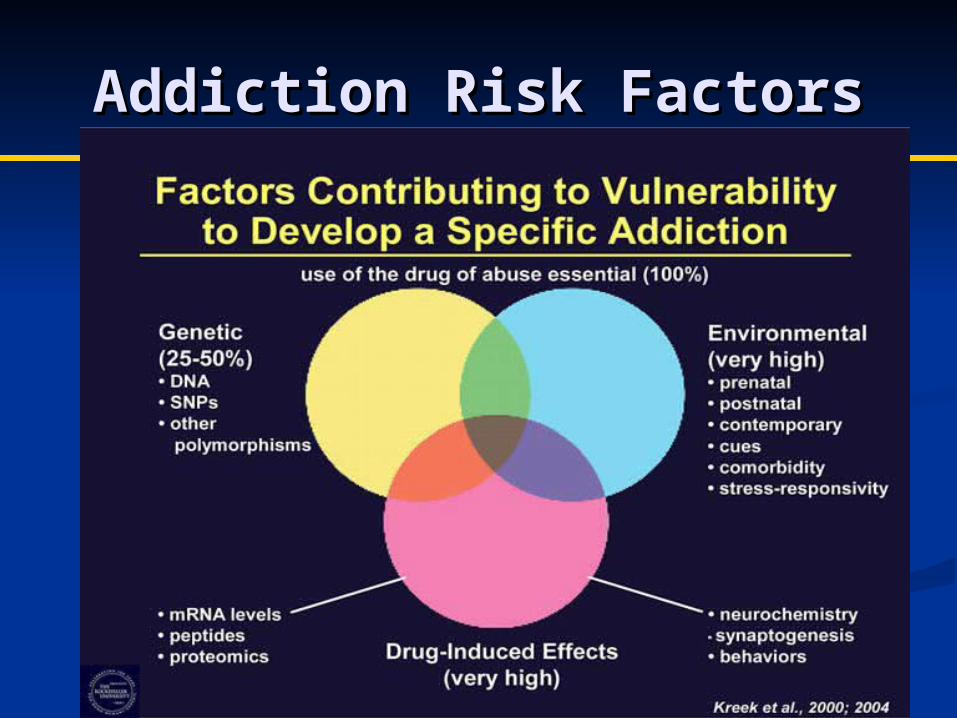
Addiction Risk FactorsAddiction Risk Factors
Neurobiology of Neurobiology of AddictionAddiction
Reward system: mesolimbic dopamine pathwayReward system: mesolimbic dopamine pathway Natural vs. drug rewardsNatural vs. drug rewards Dopamine release: pleasure and reinforcementDopamine release: pleasure and reinforcement
Dopaminergic projections from ventral Dopaminergic projections from ventral tegmental area (VTA) to nucleus accumbens tegmental area (VTA) to nucleus accumbens (NA), amygdala, and prefrontal cortex (PFC) (NA), amygdala, and prefrontal cortex (PFC)
Process of addiction causes dysfunctional Process of addiction causes dysfunctional learning and memory and maladaptive learning and memory and maladaptive behavioral patterns behavioral patterns
““Hypo-frontality”: impaired decision-making, Hypo-frontality”: impaired decision-making, loss of control (orbitofrontal cortex, anterior loss of control (orbitofrontal cortex, anterior cingulate)cingulate)
Altered neurocircuitry: relapse risk even after Altered neurocircuitry: relapse risk even after extended periods of abstinence extended periods of abstinence
Pharmacotherapy in Pharmacotherapy in Substance Use DisordersSubstance Use Disorders
Treatment of withdrawal (“detox”) Treatment of withdrawal (“detox”) Treatment of psychiatric symptoms or Treatment of psychiatric symptoms or
co-occurring disorders co-occurring disorders Reduction of cravings and urgesReduction of cravings and urges Substitution therapySubstitution therapy Prevention Prevention
Medications for Alcohol Medications for Alcohol DependenceDependence
FDA-Approved: FDA-Approved: Disulfuram (Antabuse)Disulfuram (Antabuse) PO naltrexone (Revia)PO naltrexone (Revia) IM naltrexone (Vivitrol)IM naltrexone (Vivitrol) Acamprosate (Campral)Acamprosate (Campral)
FDA approved 2006FDA approved 2006 Dose: 380 mg IM q 4 weeksDose: 380 mg IM q 4 weeks No need for oral lead-inNo need for oral lead-in Stop drinking 7 days prior (ideal)Stop drinking 7 days prior (ideal) Mechanism: opioid antagonistMechanism: opioid antagonist Results: Decreased heavy drinking Results: Decreased heavy drinking
days, decreased frequency of days, decreased frequency of drinking drinking
Acamprosate (Campral)Acamprosate (Campral)
FDA Approved 2004FDA Approved 2004 Dose: 666mg PO tidDose: 666mg PO tid Renal excretion Renal excretion Structural analog of Structural analog of
amino acid taurine and amino acid taurine and GABAGABA
time to relapse, time to relapse, increased total increased total abstinence, reduced abstinence, reduced drinking days drinking days
Clinical Case #1Clinical Case #1
42 y.o. female who lives with her mother and 42 y.o. female who lives with her mother and 12 y.o. son 12 y.o. son
Reports daily use of alcohol and occasional use Reports daily use of alcohol and occasional use of other substancesof other substances
Mother has found hidden bottles of vodkaMother has found hidden bottles of vodka Reports feeling tired, depressed, anxious, and Reports feeling tired, depressed, anxious, and
difficulty “motivating to do anything”difficulty “motivating to do anything” Reports nightmares and difficulty sleeping at Reports nightmares and difficulty sleeping at
night related to trauma (h/o sexual abuse)night related to trauma (h/o sexual abuse) Admits to drinking or taking a pill to help her Admits to drinking or taking a pill to help her
sleepsleep
Evaluation and Evaluation and ManagementManagement
What further evaluation and workup What further evaluation and workup would you recommend?would you recommend?
What is the differential diagnosis?What is the differential diagnosis? What medications would you What medications would you
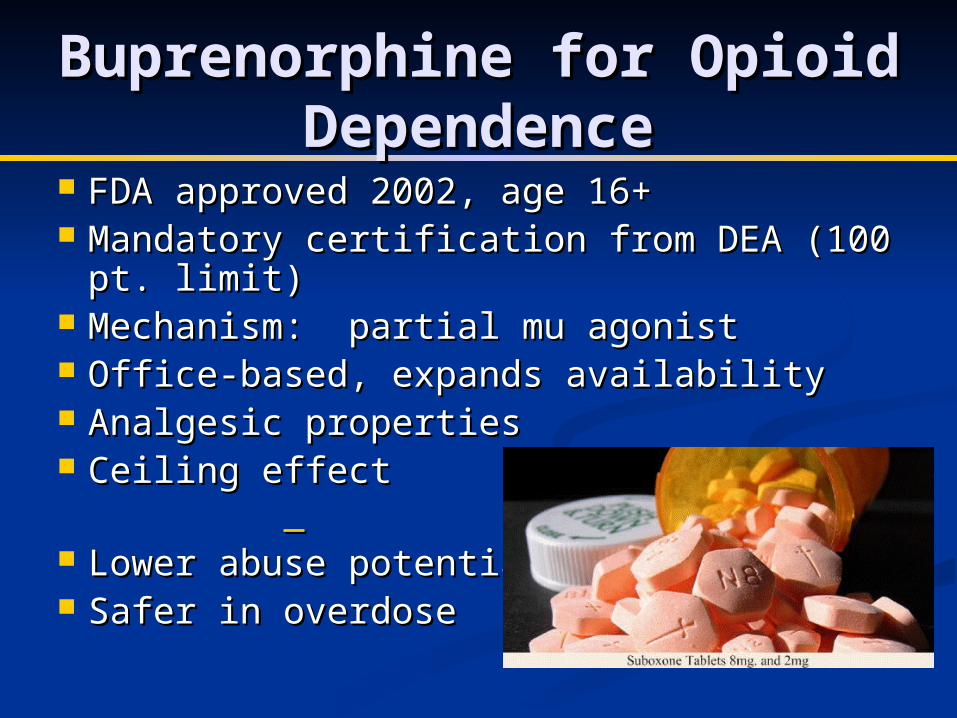
Reduce symptoms & signs of Reduce symptoms & signs of withdrawalwithdrawal
Reduce or eliminate cravingReduce or eliminate craving Block effects of illicit opioidsBlock effects of illicit opioids Restore normal physiologyRestore normal physiology Promote psychosocial rehabilitation Promote psychosocial rehabilitation
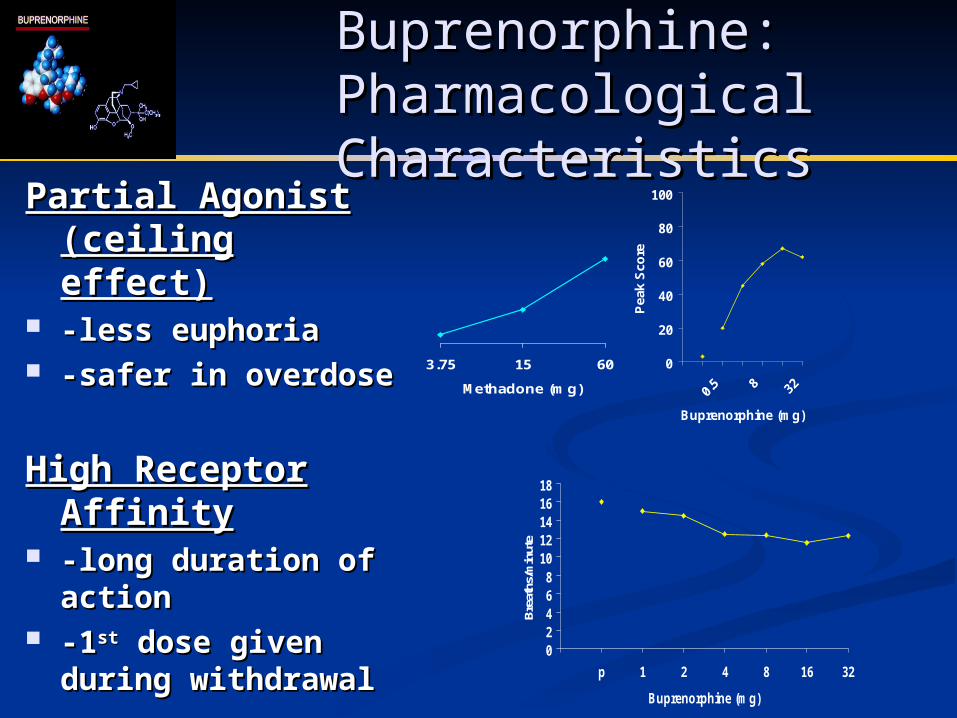
-less euphoria-less euphoria -safer in overdose-safer in overdose
High Receptor High Receptor AffinityAffinity
-long duration of -long duration of actionaction
-1-1stst dose given dose given during withdrawalduring withdrawal 0
2468
1012141618
p 1 2 4 8 16 32
Buprenorphine (mg)
Bre
aths
/min
ute
0
20
40
60
80
100
Buprenorphine (mg)
Pea
k S
core
3.75 15 60
Methadone (mg)
Clinical Case #2Clinical Case #2
34 y/o female with 3-year history of 34 y/o female with 3-year history of Vicodin useVicodin use
Using 10-12 pills/day for back pain Using 10-12 pills/day for back pain suffered in an automobile accidentsuffered in an automobile accident
No history of heroin or other opioid useNo history of heroin or other opioid use Sometimes takes more than prescribed Sometimes takes more than prescribed
by her physician, but would like to stop by her physician, but would like to stop taking all medicationstaking all medications
Employed, lives with her husband and Employed, lives with her husband and two children, and has private insurance two children, and has private insurance
Evaluation and Evaluation and ManagementManagement
What further evaluation would you What further evaluation would you recommend? recommend?
What treatment options would you What treatment options would you consider?consider?
Clinical Case #3Clinical Case #3 18 y/o unemployed male with a two year 18 y/o unemployed male with a two year
history of intravenous heroin use history of intravenous heroin use Criminal convictions for shopliftingCriminal convictions for shoplifting Has attempted outpatient detox on two Has attempted outpatient detox on two
previous occasions; most recent period of previous occasions; most recent period of sobriety lasted 4 months sobriety lasted 4 months
Lives with his parents who are unaware of Lives with his parents who are unaware of his dependence his dependence
Reports that he has done well on Reports that he has done well on methadone though has difficulty obtaining methadone though has difficulty obtaining the funds to remain in treatment the funds to remain in treatment
StimulantsStimulantsCRACK
METHAMPHETAMINE
COCAINE
Methamphetamine vs. Methamphetamine vs. CocaineCocaine
MethamphetaminMethamphetaminee
syntheticsynthetic high lasts 8-24 hourshigh lasts 8-24 hours T ½: 12 hoursT ½: 12 hours mechanism: both DA mechanism: both DA
reuptake and releasereuptake and release limited medical useslimited medical uses
neurotoxicity neurotoxicity
CocaineCocaine plant-derivedplant-derived high lasts 20-30 high lasts 20-30
Clinical Case #4Clinical Case #4 21 y/o marginally-housed male with a history of 21 y/o marginally-housed male with a history of
bipolar D/O and methamphetamine dependencebipolar D/O and methamphetamine dependence History of prior psychiatric admissions, suicide History of prior psychiatric admissions, suicide
attempt three years ago, and prior treatment with attempt three years ago, and prior treatment with lamictal and depakote; currently off medications lamictal and depakote; currently off medications
Previously employed in entertainment industryPreviously employed in entertainment industry Attending a mandated 3-day/wk outpatient drug Attending a mandated 3-day/wk outpatient drug
treatment program after receiving a citation for treatment program after receiving a citation for “solicitation of sex” and arrest for DWI. “solicitation of sex” and arrest for DWI.
After 2 weeks of nonattendance, currently reports After 2 weeks of nonattendance, currently reports insomnia, “racing thoughts”, and intermittent AHinsomnia, “racing thoughts”, and intermittent AH
Has visible excoriations on face; described Has visible excoriations on face; described episodes of picking due to sensations of “pebbles” episodes of picking due to sensations of “pebbles” under his skinunder his skin
Evaluation and Evaluation and ManagementManagement
What further evaluation and workup What further evaluation and workup would you recommend?would you recommend?
What is the differential diagnosis?What is the differential diagnosis? What treatment options would you What treatment options would you
There are no FDA-approved There are no FDA-approved medications for the following medications for the following addictive disorders: addictive disorders: Cocaine Cocaine Methamphetamine Methamphetamine MarijuanaMarijuana Pathological GamblingPathological Gambling Sexual AddictionSexual Addiction Compulsive shopping Compulsive shopping
Co-Occurring Psychiatric Co-Occurring Psychiatric D/O and SUD in AdolescentsD/O and SUD in Adolescents ““Potential problems with the diagnostic Potential problems with the diagnostic
process increase almost exponentially when process increase almost exponentially when substance use disorders and psychiatric substance use disorders and psychiatric disorders occur together.”disorders occur together.” (Schukit, 2006) (Schukit, 2006)
Perform comprehensive psychiatric Perform comprehensive psychiatric evaluation including SUD screeningevaluation including SUD screening
Obtain info from multiple sourcesObtain info from multiple sources Have a high index of suspicion for SUD co-Have a high index of suspicion for SUD co-
morbidity when patient not responding to morbidity when patient not responding to txtx
Clinical Management of Clinical Management of CODsCODs
Individualize and integrate Individualize and integrate treatment for CODs whenever treatment for CODs whenever possiblepossible
Consider random drug testingConsider random drug testing Consider need for higher level of Consider need for higher level of
carecare Consult addiction medicine Consult addiction medicine
specialist if necessaryspecialist if necessary
Medication Management in Medication Management in CODCOD
Ambivalence is common re: use of meds in Ambivalence is common re: use of meds in patients with SUDs. patients with SUDs.
Q: When to initiate pharmacotherapy when Q: When to initiate pharmacotherapy when diagnosis is unclear? diagnosis is unclear? With psychosis, moderate to severe depression, or With psychosis, moderate to severe depression, or
Medication Management in Medication Management in CODCOD
For patients with anxiety d/o’s and SUDs:For patients with anxiety d/o’s and SUDs: Try to avoid BDZsTry to avoid BDZs Consider: SSRIs, buspirone, mirtazapine, Consider: SSRIs, buspirone, mirtazapine,
trazodone, low-dose quetiapine trazodone, low-dose quetiapine For patients with ADHD and SUD, consider:For patients with ADHD and SUD, consider:
Atomoxetine (Strattera)Atomoxetine (Strattera) Bupropion SR or XL (Wellbutrin)Bupropion SR or XL (Wellbutrin) Modafinil (Provigil) Modafinil (Provigil) If stimulant necessary:If stimulant necessary:
Addiction is a serious, chronic and relapsing Addiction is a serious, chronic and relapsing disorder, but treatments are available disorder, but treatments are available
Medications should be considered as part of Medications should be considered as part of a comprehensive treatment plan, addressing a comprehensive treatment plan, addressing both disordered physiology and disrupted both disordered physiology and disrupted liveslives
Medications should be considered for Medications should be considered for treatment of: psychiatric sx’s, addictive d/o’s, treatment of: psychiatric sx’s, addictive d/o’s, and co-occurring d/o’sand co-occurring d/o’s
Emerging literature supports use of meds in Emerging literature supports use of meds in patients with SUDs and psychiatric patients with SUDs and psychiatric comorbiditycomorbidity
References References Anton RF, O’Malley SS, Ciraulo DA, Cisoler RA, Couper Anton RF, O’Malley SS, Ciraulo DA, Cisoler RA, Couper
D, Donovan DM, D, Donovan DM, et alet al., 2006. Combined ., 2006. Combined pharmacotherapies and behavioral interventions for pharmacotherapies and behavioral interventions for alcohol dependence: the COMBINE study. alcohol dependence: the COMBINE study. JAMAJAMA 295(17):2003-17. 295(17):2003-17.
Dackis CA, Kampman KM, Lynch KG, Pettinati HM, & Dackis CA, Kampman KM, Lynch KG, Pettinati HM, & O’Brien, CP, 2005. A double-blind, placebo-controlled O’Brien, CP, 2005. A double-blind, placebo-controlled trial of modafinil for cocaine dependence. trial of modafinil for cocaine dependence. Neuropsychopharmacol Neuropsychopharmacol 30:205-11.30:205-11.
Elkashef A, Vocci F, Hanson G, White J, Wickes W, & Elkashef A, Vocci F, Hanson G, White J, Wickes W, & Tiihonen J, 2008. Pharmacotherapy of methamphetamine Tiihonen J, 2008. Pharmacotherapy of methamphetamine addiction: an update. addiction: an update. Subst AbusSubst Abus 29(3):31-49. 29(3):31-49.
Garbutt JC, 2009. The state of pharmacotherapy for the Garbutt JC, 2009. The state of pharmacotherapy for the treatment of alcohol dependence. treatment of alcohol dependence. J Subst Abuse TreatJ Subst Abuse Treat 36(1): S15-23.36(1): S15-23.
HM, Loewy JW, HM, Loewy JW, et alet al., 2005. Efficacy and tolerability of long-., 2005. Efficacy and tolerability of long-acting injectable naltrexone for alcohol dependence: a acting injectable naltrexone for alcohol dependence: a randomized controlled trial. randomized controlled trial. JAMAJAMA 293(13):1617-25. 293(13):1617-25.
Kreek MJ, Schlussman SD, Bart J, LaForge KS, and Butelman ER, Kreek MJ, Schlussman SD, Bart J, LaForge KS, and Butelman ER, 2004. Evolving perspectives on neurobiological research on the 2004. Evolving perspectives on neurobiological research on the addictions: celebration of the 30addictions: celebration of the 30thth anniversary of NIDA. anniversary of NIDA. NeuropharmacolNeuropharmacol 47 Suppl 1:324-44. 47 Suppl 1:324-44.
Newton TF, Roache JD, De La Garza R 2Newton TF, Roache JD, De La Garza R 2ndnd, Fong T, Wallace CL, Li , Fong T, Wallace CL, Li SH, SH, et alet al., 2006. Bupropion reduces methamphetamine-induced ., 2006. Bupropion reduces methamphetamine-induced subjective effects and cue-induced craving. subjective effects and cue-induced craving. NeuropsychopharmacolNeuropsychopharmacol 31(7):1537-44. 31(7):1537-44.
Vigezzi P, Guglielmino L, Marzorati P, Silenzio R, DeChiara M, Vigezzi P, Guglielmino L, Marzorati P, Silenzio R, DeChiara M, Corrado F, et al., 2006. Multimodal drug addiction treatment: a Corrado F, et al., 2006. Multimodal drug addiction treatment: a field comparison of methadone and buprenorphine among heroin- field comparison of methadone and buprenorphine among heroin- and cocaine-dependent patients. and cocaine-dependent patients. J Subst Abuse TreatJ Subst Abuse Treat 31(1):3-7. 31(1):3-7.
Vocci FJ, Acri J, and Elkashef A, 2005. Medication development Vocci FJ, Acri J, and Elkashef A, 2005. Medication development for addictive disorders: the state of the science. for addictive disorders: the state of the science. Am J PsychiatryAm J Psychiatry 162(8): 1432-40. 162(8): 1432-40.