167
Pharmacology in Dentistry Dr. Peter Nkansah Winter Clinic November 8, 2013

Pharmacology in Dentistry Dr. Peter Nkansah
Winter Clinic
November 8, 2013

Pharmacokinetics & pharmacodynamics
Review of local anaesthetics
Review of analgesics
Review of anti-infectives
Sedative drugs
Bisphosphonates
Herbal supplements
Drug interactions
Overview

Pharmacokinetics & Pharmacodynamics

What the body does to drugs
Absorption
Distribution
Metabolism
Elimination
Pharmacokinetics

What drugs do to the body
Includes duration and magnitude of responses
Dose-response considerations
Pharmacodynamics

Local Anaesthetics

Local anaesthetics have been isolated since the 1860s (cocaine)
Sensory nerve blockade was first described by Halsted in 1884
“Novocaine” (procaine) was the first commonly used LA in dentistry
Lidocaine is the original amide LA Commercially available in 1948
Articaine is the newest popular LA
Released in Canada in 1982 (US in 2000)
History of Local Anaesthetics
To stop the generation and conduction of nerve impulses
To abort impulses from stimuli, like tooth extraction
E.g. To stop the patient from feeling pain
Purpose of LA

Mechanism of Action
Local anaesthetics bind to site on Na+ channel
Inhibits the permeability to Na+
Block propagation of action potential
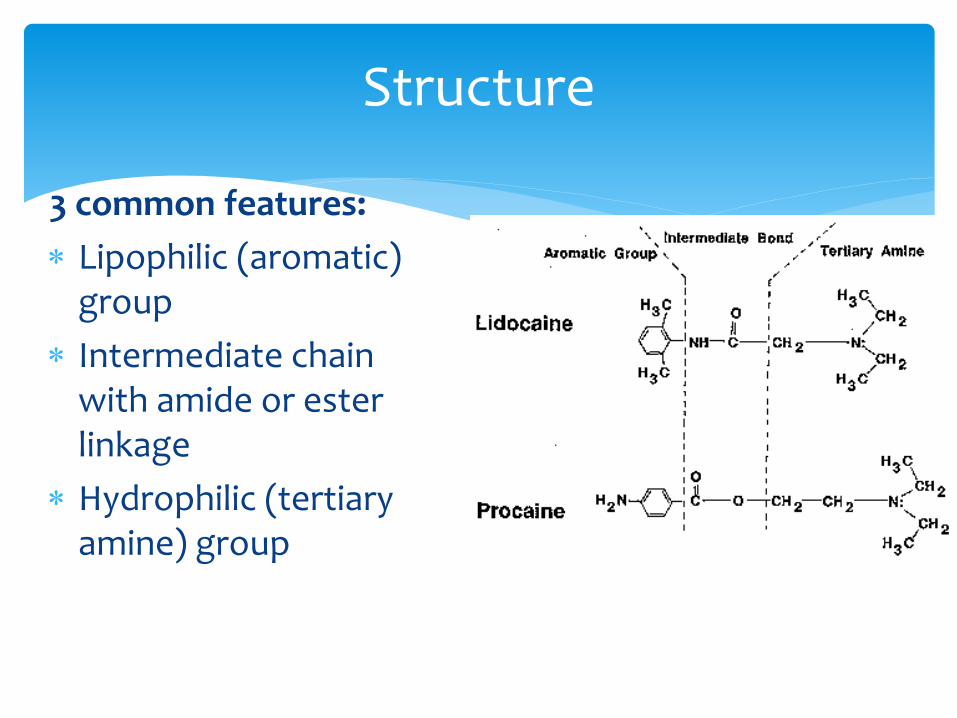
Structure
3 common features:
Lipophilic (aromatic) group
Intermediate chain with amide or ester linkage
Hydrophilic (tertiary amine) group

By themselves, LA solutions are weakly basic, poorly soluble in water and unstable
Used as salt solutions (usually HCl) which are water-soluble and stable
With the addition of vasopressors, the solutions become acidic
LA Solutions

Amide LA’s are primarily biotransformed in the liver
Cytochrome P450 CYP3A4
Medical history concerns:
Severe liver dysfunction
Pseudocholinesterase deficiency (for esters)
Biotransformation & Elimination

Proximity to target site
Concentration
Lipid solubility
Nerve morphology
pH of the tissue
pKa
Onset determinants
pH at which amount of base = amount of cation
All LA’s have pKa > 7.4
pKa = potency
Dissociation Constant (pKa)

pKa of Local Anaesthetics
pKa % base at pH 7.4
Time to onset (min)
Mepivacaine 7.6 40 2-4
Articaine 7.8 29 2-4
Lidocaine 7.9 25 2-4
Prilocaine 7.9 25 2-4
Bupivacaine 8.1 18 5-8
Procaine 9.1 2 14-18

Henderson-Hasselbalch Equation
pKa – pH = log 10 Ionized (BH+) Unionized (B)

Example: Lidocaine
pKa – pH = log [ionized/un-ionized]
7.9 – 7.4 = log [ionized/un-ionized]
100.5 = ionized / un-ionized
~3 / 1 = ionized / un-ionized
Drug Ionization

Concentration
Protein binding
Lipid solubility
Redistribution from site
Duration determinants

Maxillary Paraperiosteal (min) IAN Block (min)
Preparation Pulp Soft Tissue Pulp Soft Tissue
Lidocaine w epi 60 150 75 180-300
Articaine w epi 60 120-360 75 120-360
Prilocaine w epi 40 120 75 180
Prilocaine plain 15 60-90 60 150
Mepivacaine w levo 50 180-300 75 180-300
Mepivacaine plain 20 120-180 40 120-180
Bupivacaine w epi 60 240-540 180 240-540
Duration of action

LA maximum doses
Drug Max (mg/kg)
Max (mg) Max
(mg w/o epi)
# cart. (for 70 kg
adult)
lidocaine 7 500 300 13
articaine 7 500 300 7
prilocaine 8 600 400 8
bupivacaine 2 200 75 10
mepivacaine 7 450 300 8

Expressing a % solution
in mg/ml
Local Anaesthetic Toxicity Signs and Symptoms
Mild
Confused
Talkative
Slurring
Muscle twitch
BP, HR and RR
Severe
Tonic-clonic seizures
CNS depression
Drowsiness
Loss of consciousness
BP, HR and RR
CV collapse

Epinephrine or levonordefrin are added to LA solutions to increase duration and depth of anaesthesia
Use their alpha-agonist interaction with adrenoceptors
Short-lasting drugs by themselves
Vasoconstrictors

Epinephrine
rapid onset
exogenous epinephrine is metabolized by COMT
short duration of action
5 to 10 minutes if intravenous injection
10 to 20 minutes if intraoral injection

Vasoconstrictors
Epinephrine
1:50,000
1:100,000
1:200,000
Levonordefrin
1:20,000

Trade name = Neocobefrin
1:20,000 = 90 μg per cartridge
Similar concerns to those when using epinephrine
Consider the maximum dose of 0.2 mg
Levonordefrin

Beware of interactions with:
Non-selective β-blockers
Tricyclic antidepressants
Cocaine or amphetamine use
COMT inhibitors (e.g. Comtan™ for Parkinson’s disease)
Not an issue with MAOI
Vasoconstrictors

Local anaesthetic reversal agent for adults and children
Safe and effective for patients ≥ 6 years and 15 kg
2003 report by Rafique et al. (Caries Research, 37: 360-364) noted that 86% of patients receiving LA had moderate dislike of postop numbness
14% report high dislike
www.novalar.com
Phentolamine Mesylate (OraVerse™)

A non-selective α-adrenergic antagonist
Blocks the effects of vasoconstrictors in LA preparations
Increases the redistribution of LA away from injection site
Phentolamine Mesylate

Reduces duration of anaesthesia by 50%
Non-toxic and well-tolerated < age 6 years
Only observed adverse effect is a minor increase in postoperative pain shortly after return to normal sensation
Phentolamine Mesylate

Administered via standard dental cartridge in a 1:1 volume dose ratio to local anaesthetic
Supplied as 0.4 mg/1.7 mL
$13-$17+ per cartridge
Possible uses:
Bilateral mandibular work requiring LA
Paediatric patients
Mentally challenged patients
Phentolamine Mesylate

Placebo vs. Pharmacology?
If pharmacology works, then topicals must be placed on dried mucosa for 1-2 minutes
NB: Topical anaesthetics are ester LA’s
Some new research into gels containing KNO3 and sprays using ethyl chloride
Topical Anaesthetics

Adverse reactions to LA
Toxicity of LA or vasoconstrictor
Psychogenic reactions
Allergic reactions to LA or to metabisulfite
Methemoglobinemia
Paraesthesia

Psychogenic reactions
Syncope is the most common medical emergency
Occurs most often at the time of injection
Changes in heart rate +/- blood pressure
Hyperventilation
Nausea and vomiting
Adverse reactions

Allergic reactions
The component ingredients in a cartridge are:
Local anaesthetic
Vasoconstrictor
Metabisulfite
Adverse reactions

Adverse reactions
Methemoglobinemia
Condition in which cyanosis develops in the absence of cardiac or respiratory abnormalities
May be congenital or acquired through drugs or chemicals
MetHb is normally <1%
Cyanosis and respiratory distress may occur with MetHb >10%

Methemoglobinemia
Associated with prilocaine (or severe benzocaine) overdose
Prilocaine’s metabolite o-toluidine can block MetHb reductase, leading to MetHb
Appears 3 - 4 hours after administration
Adverse reactions

Methemoglobinemia
Unresponsive to O2
Pulse oximeter readings are abnormal (~85%)
Blood is chocolate brown
Treated by 1% methylene blue IV
Avoid prilocaine or benzocaine if congenital methemoglobinemia
Adverse reactions

Paraesthesia

There are numerous reports regarding the association between 4% solutions and a higher-than-expected incidence of paraesthesias
Note the risk:benefit equation
Overall paraesthesia incidence is 1:800,000 injections
There has been an RCDSO advisory regarding 4% solutions used for blocks
Paraesthesias
Paraesthesia
Broad term for prolonged anaesthesia or altered sensation, beyond expected duration of action of local anaesthetic
Adverse reactions
Paraesthesia
Most are transient, usually resolving within 8 weeks
If not, prognosis is very poor
Precise cause not known with certainty
Hemorrhage into nerve sheath
Scar formation
Alcohol or sterilizing solution
Neurotoxicity - controversial
Adverse reactions

A 21-YEAR RETROSPECTIVE STUDY OF REPORTS OF PARESTHESIA FOLLOWING LOCAL ANESTHETIC ADMINISTRATION
Haas and Lennon, JCDA, 1995, 61:319-330
Adverse reactions

The overall incidence of paraesthesia following local anesthetic administration for non-surgical procedures in dentistry is very low 1:785,000
If, however, paresthesia does occur, the results suggest that it is more likely if either articaine or prilocaine is used
Reasons are speculative only
Adverse reactions

Results (1973-1993)
0
10
20
30
40
50
60
Articaine Bupivacaine Lidocaine Mepivacaine Prilocaine
1973-1993
Tongue = 64.3%
Lip = 29.4%
Lip & Tongue = 6.3%
1994-1998
Tongue = 70%
Lip = 20%
Chin = 9%
Cheek = 9%
Other = 14%
Sites of Paraesthesia

Nerve injury caused by mandibular block analgesia
Hillerup and Jensen, Int J Oral Maxillofac Surg, 2006, 35: 437-443
Prospective study in Denmark
Results: Neurologic evidence of neurotoxicity, not mechanical injury
Articaine had > 20-fold in paraesthesia compared to all other locals combined
Adverse reactions

Practice Alert: Paraesthesia Following Local Anaesthetic Injection
“Until more research is done, it is the College’s view that prudent practitioners may wish to consider the scientific literature before determining whether to use 4% local anaesthetic solutions for mandibular block injections.”
RCDSO Dispatch (2005)
Retrospective Review of Voluntary Reports of Non-Surgical Paresthesia in Dentistry Gaffen and Haas, 2009, Journal of the Canadian Dental
Association, 75(8): 579
OBJECTIVES: To analyze cases of paresthesia associated with local
anesthetic injection that were reported to the province of Ontario’s Professional Liability Program (PLP) from 1999 to 2008 inclusive
To update previous study (1995)
Adverse reactions

Sites:
Tongue: 79.1%
Chin/lower lip: 28.0%
Tongue and lower lip together: 9.9%
Cheek 4.4%
Symptoms:
Altered taste: 14.3%
Pain on injection: 19.2%
Dysesthesia: 9.9%
Results

Results: Percentage of paresthesia

JADA (July 2010)

JADA (July 2010)

Incidence is very low
Yet data are strongly suggestive of an association
No proof of cause-effect
It is not the drug per se
Higher concentrations may simply predispose to greater effect
Conclusions

Analgesics

Eliminate the source of pain
Consider adjusting regimens according to the patient’s needs and response
Maximize NSAID/acetaminophen doses before adding opioids
Patients who do not respond to one NSAID may respond to another
Avoid chronic use
General guidelines

AA
lipoxygenase
Leukotrienes
Bronchospasm
Inflammation
COX-1
PG’s
GI protection
Uterine cont.
Renal function
TXA’s
Platelets
COX-2
PG’s
Pain
Inflammation
Arachidonic Acid Cascade
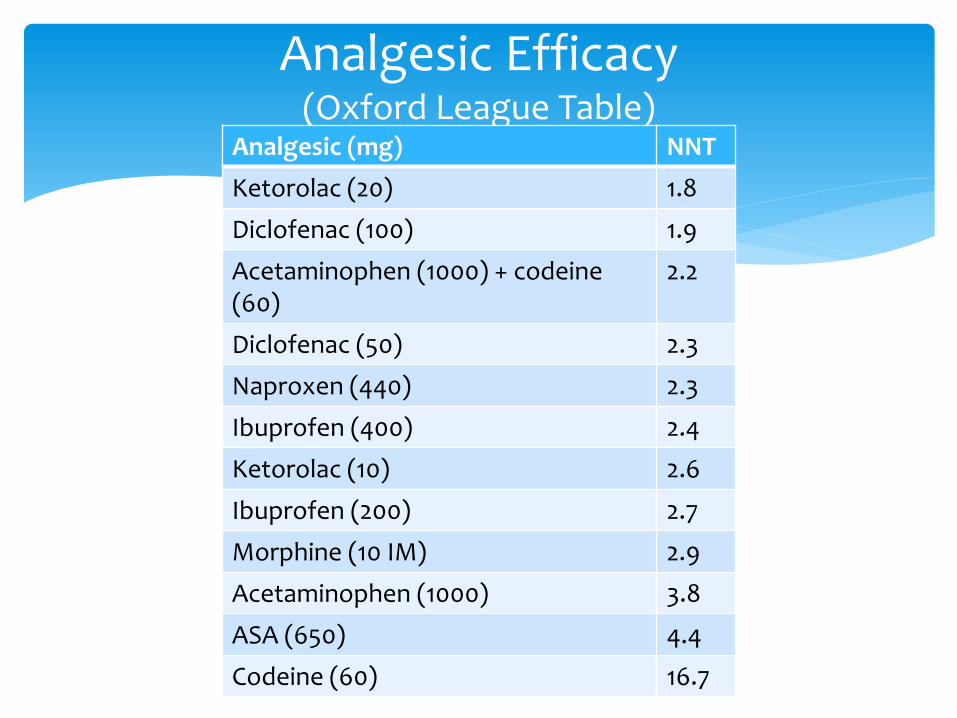
Analgesic Efficacy (Oxford League Table)
Analgesic (mg) NNT
Ketorolac (20) 1.8
Diclofenac (100) 1.9
Acetaminophen (1000) + codeine (60)
2.2
Diclofenac (50) 2.3
Naproxen (440) 2.3
Ibuprofen (400) 2.4
Ketorolac (10) 2.6
Ibuprofen (200) 2.7
Morphine (10 IM) 2.9
Acetaminophen (1000) 3.8
ASA (650) 4.4
Codeine (60) 16.7

Non-steroidal anti-inflammatory agents are central to pain control in dentistry
They inhibit COX-2 +/- COX-1 enzymes
Tissue damage activates COX-2
NSAID
Analgesic
Anti-inflammatory
Anti-pyretic
Anti-dysmenorrheal
NSAID Therapeutic Effects

Drug Adult Dose (mg) Frequency Daily Maximum
ASA 325-1000 q 4-6 h 4,000
Ibuprofen 400 q 4-6 h 2,400
Diflunisal 1000, then 500 q 12 h 1,500
Naproxen 500, then 250 q 6-8 h 1,375
Ketorolac 10 q 4-6 h 40 (5 days)
NSAID* Dosages for Post-Op Pain

An effective and popular NSAID
Analgesic, anti-inflammatory and antipyretic
Effective doses are 200 mg – 400 mg q 4-6 h
Maximum daily dose = 1200 mg
Loading doses are effective
Solubilized liquigels and ibuprofen lysine have faster onset and better peak analgesia than conventional tablets
Ibuprofen
Vioxx® and Celebrex® are the famous examples
The benefits should be:
Less GI bleeding
Fewer gastroduodenal ulcers
Is there a predisposition to myocardial infarction?
Vioxx® voluntarily withdrawn from the market in 2004
COX-2 Inhibitors

Dosage is 200 mg bid
Equal efficacy to 650 mg ASA in dental pain studies
Less effective than ibuprofen or naproxen
Celebrex®

Increased bleeding*
Gastric mucosal damage
Dyspepsia
Renotoxicity
Anaphylactoid reactions
NSAID Adverse Effects

Gastric ulcers
Bleeding dyscrasias or concerns
Significant renal disease
asa (or other NSAID) hypersensitivity
Combination of severe asthma, nasal polyps and multiple allergies
Can lead to ARDS
NSAID contraindications

Pregnancy
Especially in the 3rd trimester
Children
asa only
Elderly
Concurrent use of certain other drugs
NSAID contraindications
Consider:
Pre-operative dosing
Loading doses
4-hour interval instead of prn for the first day
NSAID strategies

Analgesic of choice in dentistry
Effective analgesic and anti-pyretic
No NSAID side effects
Not anti-inflammatory
Very safe at normal doses
Hepatotoxic at high doses
Mechanism of action not entirely clear
Acetaminophen
Dosages
Adult dose is 500-1,000 mg q 4-6 h to a maximum of 4 grams per day
Paediatric dose is 10-15 mg/kg q 4-6 h to a maximum of 80 mg/kg
Acetaminophen

Two different mechanisms of action for analgesia
Potentially synergistic in the short-term
Potentially renotoxic in the long-term
NSAID & Acetaminophen

Usually used for analgesia for moderate to severe pain in dentistry
Other opioid effects: Sedation
Mood alteration
Antitussive
Respiratory depression
Nausea and vomiting
Constipation
Opioids
Mechanism of action
Analgesia site of action is the CNS
Possible peripheral anti-inflammatory action
One study compared supplemental PDL injections with fentanyl vs. mepivacaine with epi
Ref.: Elsharrawy and Elbaghdady, Journal of Pain and Symptom Management, 33(2), 2007
Opioids

Equipotent doses
Opioids
Drug Oral dose (mg) IM dose (mg)
Morphine 60 10
Codeine 200 120
Oxycodone 30 10
Meperidine 300 75

Recommended oral doses
Codeine = 60 mg
Oxycodone = 5-10 mg
Meperidine = 100 mg
Opioids

They have the advantage of convenience
They do not have sensible formulations
Opioid Combinations
Drug Acetaminophen (mg) Codeine (mg)
Tylenol #1 300 8
Tylenol #2 300 15
Tylenol #3 300 30
Tylenol #4 300 60
Addiction is a real possibility
The public (and the government) are currently on high alert about the use of opioids in healthcare
Opioids

Maximize NSAID (or acetaminophen) before adding opioid
Optimize dosing regimen before switching
If the patient does not respond to one NSAID, they may respond to another
Consider pre-operative or loading doses
Analgesic Tips

Mild to moderate pain
Acetaminophen
(up to 1000 mg)
NSAID
Add codeine to NSAID or acetaminophen
Add oxycodone w/ acetaminophen
Add codeine or oxycodone
Analgesic algorithm

Antibiotics

Use only when there is an indication
Choose the narrowest spectrum drug that will be effective
Consider the risk/benefit equation
Prescribe an adequate dose
Adequate frequency
Adequate duration
Prescribing Principles

Wrong drug or dose
Bacterial resistance
Host defences depressed
Poor compliance
Reasons for Failure

Antibiotic Actions
Bactericidal
Penicillins
Metronidazole
Cephalosporins
Aminoglycosides*
Vancomycin*
Bacteriostatic
Clindamycin
Erythromycin
Tetracyclines

Oral penicillins are penicillin V and amoxicillin
Pen V is narrow-spectrum against gram-positive Strep and others
Drug of choice for orofacial infections
Dose = 300-600 mg q6h
Amoxicillin is broad-spectrum and better absorbed orally
Dose = 250-500 mg q8h
Penicillins

Adverse reactions
Allergy
Diarrhea
Nausea and vomiting
Pseudomembranous colitis
Candidiasis
Penicillins

Allergy rate is 1-10% of the population
Penicillins responsible for 75% of anaphylaxis deaths
400-800 deaths per year in the US
Mild anaphylaxis occurs 1:200 courses
Severe anaphylaxis occurs 1:2,000 courses
Penicillins

An alternative for penicillin-allergic or penicillin-resistant patients
Active against gram-positive and gram-negative anaerobes and facultative/aerobic bacteria
Dose = 150-300 mg q6h
Clindamycin

Also known as antibiotic-associated diarrhea (AAD)
Broad-spectrum antibiotic use alters the composition of gut bacteria
This allows the overgrowth of other bacteria
Clostridium difficile (C. difficile) is the beneficiary of interest here
The presence of C. difficile and its toxins cause pseudomembranous colitis
Characterized by diarrhea, fever and abdominal pain
Pseudomembranous colitis

Risk factors Drugs include:
Penicillins (esp. ampicillin)
Cephalosporins
Clindamycin
Erythromycin
Advanced age
Females with genitourinary disease
Uremic patients (e.g. kidney dialysis patients)
Pseudomembranous colitis

Treatment Stop all antibiotics Keep the patient hydrated Refer to a physician Prescribe:
Vancomycin 500 mg po qid for 2 days (if severe) Vancomycin 125 mg po qid for 10-14 days Metronidazole 500 mg po tid for 7-14 days Metronidazole IV Probiotic therapy (Saccharomyces boulardii) has been tried
adjunctively
Pseudomembranous colitis

Group includes erythromycin, clarithromycin and azithromycin
Erythromycin was the former drug of choice for penicillin-allergic/penicillin-resistant patients
Numerous GI adverse effects
Active against gram-positive aerobic/facultative staph and strep and gram-negative anaerobes
Macrolides

Trade name is Flagyl™
Active against obligate, gram-negative anaerobes only
Used in combination with penicillin
Avoid concurrent use of alcohol or warfarin
Dose = 250-500 mg tid
Metronidazole

Group includes tetracycline, doxycycline (Vibramycin, Periostat) and minocycline (Minocin)
Broad-spectrum, bacteriostatic
Useful in treatment of periodontal disease
Widespread resistance
Host of adverse effects including: tooth staining, photosensitivity, blood dyscrasias, GI effects
Tetracyclines
From Resnick and Misch (2008):
Overall incidence is 6-7%
Possible reactions include:
GI tract complications
Colonization of resistant or fungal strains
Cross reactions with other medications
Pseudomembranous colitis
Development of resistant bacteria and superinfection
Little concern about short-term use
Antibiotic Adverse Reactions

Antibiotic Prophylaxis

Indicated for patients with: Prosthetic heart valves
History of infective endocarditis
Cardiac transplant with subsequent heart valve problem
Some congenital heart conditions
Unrepaired cyanotic disease (incl. shunts and conduits)
Repaired defect (<6 months) with prosthetic material or device
Repaired defect with residual defect at or adjacent to the site of repair
Antibiotic Prophylaxis

Coverage is not indicated for patients with:
Surgically constructed systemic pulmonary shunts
Isolated secundum atrial septal defect
Previous coronary artery bypass graft surgery
Physiologic (functional, innocent) heart murmurs
Pacemakers and implanted defibrillators
Antibiotic Prophylaxis
Indicated for the following procedures: Implant placement
Extractions
Periodontal procedures
Reimplantation of avulsed teeth
Endodontics beyond the apex of the tooth
Intraligamentary injections
Subgingival placement of fibres or strips
Placement of orthodontic bands
Polishing of teeth or implants where bleeding is expected
Antibiotic Prophylaxis

Drug Adult Dose Paedo Dose
Amoxicillin 2 g 50 mg/kg
Clindamycin 600 mg po/IV 20 mg/kg po/IV
Azithromycin 500 mg 15 mg/kg
Clarithromycin 500 mg 15 mg/kg
Ampicillin 2 g IM/IV 50 mg/kg IM/IV
Antibiotic Prophylaxis

Patients already taking an antibiotic used for prophylaxis should:
Be prescribed an antibiotic from a different class
Be scheduled at least 9 days after the completion of the current prescription
Antibiotic Prophylaxis

May be indicated for patients at increased risk including:
< 2 years post-surgery
Inflammatory joint disease
Immunosuppression (incl. drug-induced, radiation-induced, HIV)
Previous joint infections
Type I diabetes mellitus
Total Joint Prosthesis

Prophylaxis may be indicated for patients at increased risk including: < 2 years post-surgery Inflammatory joint disease (e.g. rheumatoid arthritis, lupus) Immunosuppression (incl. drug-induced, radiation-induced,
HIV) Previous joint infections Type I diabetes mellitus Hemophilia Malignancy
The literature is unclear
Prophylaxis for Total Joint Prostheses

Regimens:
Amoxicillin or cephalexin 2 g po, 1 hour pre-op
Clindamycin 600 mg po/IV, 1 hour pre-op
Total Joint Prostheses

CYP3A4 is a major metabolizing enzyme
Part of the cytochrome P450 enzyme system
Clarithromycin, erythromycin and the azole antifungals (e.g. ketoconazole, fluconazole) are potent inhibitors of CYP3A4
Single-dose regimens, as in antibiotic prophylaxis are not of major concern
Antibiotic Drug interactions

Anecdotally reported
Scientific evidence implies rifampin (Rifadin®, Rofact™) only
Virtually untestable
Rationale is that antibiotics reduce enterohepatic recycling of estrogen → subtherapeutic blood levels that allow ovulation
Antibiotics and Oral Contraceptives
The concept of using antibiotics to enhance the outcome of implant surgery is not new
Adel et al. (1981) used Penicillin V for 10 days
Adel (1985) used 2 g Penicillin V for 10 days
Buser et al. (1990) used short-term amoxicillin or erythromycin
Antibiotics & Implant Surgery

Cochrane Review by Esposito et al. (2008) investigated the use of antibiotics to prevent complications in implants
Two randomized controlled studies were subjected to meta-analysis
Showed a statistically significant higher number of implant failures in the group that did not receive antibiotics
“It might be recommendable to suggest the use of one dose of prophylactic antibiotics prior to dental implant placement
2 g of amoxicillin preoperatively?
Antibiotics & Implant Surgery

Clavulin® = amoxicillin and clavulanic acid
Dose = 875/125 mg bid for 7 days
Chlorhexidine 0.12% rinse
Start both medications 1 day pre-operatively
Sinus lift pre-/perioperative medication

Possible complications that may require medications are:
Site infection
Chlorhexidine 0.12% mouthrinse bid for 2 weeks
Nasal congestion
Pseudoephedrine (Sudafed®) 120 mg q12h
Phenylephrine (Sudafed PE®) 10 mg q4h
Oxymetazoline 0.05% (Claritin® Nasal Pump, Drixoral®) 2 sprays in each nostril q12h
Afrin® in the US
NB: other formulations of Claritin® are loratidine, an antihistamine
Sinus lift postoperative considerations

Bisphosphonates
They inhibit bone resorption by inhibiting osteoclasts and impairing angiogenesis
Indicated in the treatment of: Osteoporosis
Paget’s Disease
Prolonged glucocorticoid therapy
Metastatic cancers (e.g. breast, lung, prostate and renal)
Osseous lesions associated with multiple myeloma
Bisphosphonates
Associated with osteonecrosis of the jaws
Other bones rarely affected
Oral vs. intravenous
Consider as 2 distinct risk groups
Oral formulations include alendronate (Fosamax™), risedronate (Actonel™), ibandronate (Boniva™) and etidronate (Didrocal™)
Bisphosphonates

Bisphosphonate-associated osteonecrosis (BON) incidence estimates:
~0.8%-20% of patients in cancer therapy
0.01%-0.04% of patients taking oral formulations
0.09%-0.34% in cases of dental extractions
30 million prescriptions in the US in 2006
< 10% of BON cases associated with oral bisphosphonates
Ref.: ADA, JADA 139(12): 1674-1677, 2008
Osteonecrosis Incidence

General dentistry
Areas of bony infection should be treated immediately
No change in routine care
Periodontal disease
Try to use non-surgical therapies with re-evaluation in 4-6 weeks
Use bone grafting and guided tissue regeneration judiciously
ADA Recommendations
Oral and maxillofacial surgery Discuss risks (though small) and alternate treatments
(e.g. RCT, FPD’s, RPD’s)
Post-operative prophylactic antibiotic use should be for risk of infection vs. use of bisphosphonates
Implants Placement of implants may pose increased risk
Peri-implantitis should be approached non-surgically first
ADA Recommendations

Sedative Agents

Conscious Sedation (minimal and moderate*)
Deep Sedation
General Anaesthesia
Spectrum of Anaesthesia
“… a minimally to moderately depressed level of consciousness that retains the patient’s ability to…maintain an airway and respond appropriately to physical stimulation and verbal command.”
Ref: RCDSO, 2008
Conscious Sedation Definition

“… a controlled state of depressed consciousness, accompanied by partial loss of protective reflexes, including inability to respond purposefully to verbal command.”
Ref.: RCDSO, 2008
Deep Sedation Definition

“… a controlled state of unconsciousness accompanied by partial or complete loss of protective reflexes including inability to maintain an airway independently …”
Ref.: RCDSO, 2008
General Anaesthesia Definition

Warning:
Any method of sedation and any choice of drug can lead to any level of
consciousness
Nitrous Oxide
Benzodiazepines
Antihistamines*
Useful Conscious Sedation Drugs

The Good:
Fast onset, fast offset
Easy to administer
No lasting effects
0.004% metabolized
Very safe
Nitrous Oxide and Oxygen

The Bad:
Difficult for claustrophobic patients
May not be strong enough
Requires active dentist participation
Nitrous Oxide and Oxygen

The Good: Familiar, noninvasive route of administration
No special office equipment is needed*
The Bad: Not titratable or recoverable
Benzodiazepines are reversible but not orally
Beware of DOCS* protocols
Slow onset
Patients must be accompanied home
Ref.: Donaldson et al., Anesthesia Progress, 54:118, 2007
Oral Medications

An anxiolytic-specific category of drugs
Act on GABAA receptors in the CNS to hyperpolarize cells
Lowers brain activity
Little effect on the respiratory and central nervous systems
Benzodiazepines

Effects are sedation, anterograde amnesia and anxiolysis
Popular choices are midazolam, triazolam, diazepam and lorazepam
Peak of action in about 1 hour, except for midazolam
Be careful with multiple doses or alternate routes of administration (e.g. sublingual)
Benzodiazepines

Agents include:
Zolpidem (Ambien)
Fast onset, short duration, no active metabolites
Zopiclone (Imovane)
Similar pharmacologic profile to zolpidem
Ramelteon (Rozerem)
A melatonin receptor agonist
Non-BZD GABA Agonists

Sedation is a side effect
Agents include hydroxyzine (Atarax), diphenhydramine (Benadryl) and promethazine (Phenergan)
Very safe
Antihistamines

Warning:
Oversedation = medical emergency

Drug Therapy in the Elderly

Pharmacokinetic changes
Pharmacodynamic changes
Systemic disease
Polypharmacy
Factors to consider

CNS drugs have magnified effects (e.g. benzodiazepines)
Can result in
Excessive sedation
Mental confusion
Delirium
Respiratory depression
Pharmacodynamics

Some examples of diseases that affect pharmacologic effects include:
Systemic disease
Disease Effect
Renal disease ↑ serum half-life and concentration
Congestive heart disease ↑ serum half-life and concentration
Benign prostatic hypertrophy ↑ urinary retention with anticholinergics
Dementia ↓ ability to comply with prescriptions
Use of prescription medications, OTC medications, natural medicines and alternative medicines is very widespread in Canada
Concerns for adverse drug reactions and drug interactions
According to a 2009 report from Ramage-Morin (Statistics Canada)
In 2005, pharmacists dispensed an average of 35 prescriptions per person aged 60 to 79 74 prescriptions per person aged 80 or older
Compared with an overall average of 14 prescriptions per Canadian
Math, co-morbidities and physiologic changes put seniors at risk
Polypharmacy
53.1% of institutionalized seniors and 12.8% of seniors in private households reported polypharmacy (taking 5 medications or more in the past 2 days)
97% of institutionalized seniors reported taking some medication in the past 2 days
76% of seniors living in private households
Ramage-Morin (2009)

Local anaesthetics
No change in administration
Consider reducing maximum dose if the patient has congestive heart disease
Limit vasoconstrictor dose to 40 μg per appointment
Specific considerations

Acetaminophen
Analgesic of choice
Dosage of 325-1000 mg q4h to a daily maximum of 4 g
Reduce the daily maximum if there is alcoholism or significant liver disease
Specific considerations

NSAIDs
Note the possibilities for bleeding, ulceration or perforation
Increased risk of GI toxicity
Increased risk of renal toxicity
Increased risk of hepatic toxicity
Consider celecoxib (Celebrex®) as your NSAID
Specific considerations

Opioids
Level of effect increased
Duration of effect prolonged
Increased likelihood of adverse reactions
Consider using a reduced dose or avoid opioids
Specific considerations
Antibiotics
Increased risk of pseudomembranous colitis
No need to alter regimens solely because of age
Specific considerations

Nitrous oxide & oxygen First choice for conscious sedation
Advantages
Titratability
Rapid onset and offset
Disadvantages
Patient acceptance
Limited effectiveness
Equipment costs
Not useful for Alzheimer’s/dementia patients
Specific considerations

Oral sedation Advantages
Easy to administer No equipment costs*
Disadvantages Dosage is a guess Onset is delayed and unreliable Effects are prolonged Limited efficacy Many side effects May not be suitable/effective for dementia patients
Specific considerations

Goals
Review the patient’s current drug list
Simplify the treatment regimens
Reduce the number of drugs and the dosing frequency
Monitor the patient after providing a prescription
Pharmacotherapy for the elderly patient
Herbal Supplements

A survey by Prevention Magazine in 2000 suggested that 33% of American adults used herbal supplements
70% of the consumers may not tell their healthcare providers about this
Government oversight is not as strict as with conventional drugs
2013 study at U of Guelph showed that one-third of the products did not contain what they said they did
Suggested reading: Do You Believe In Magic by Paul Offitt
Overview
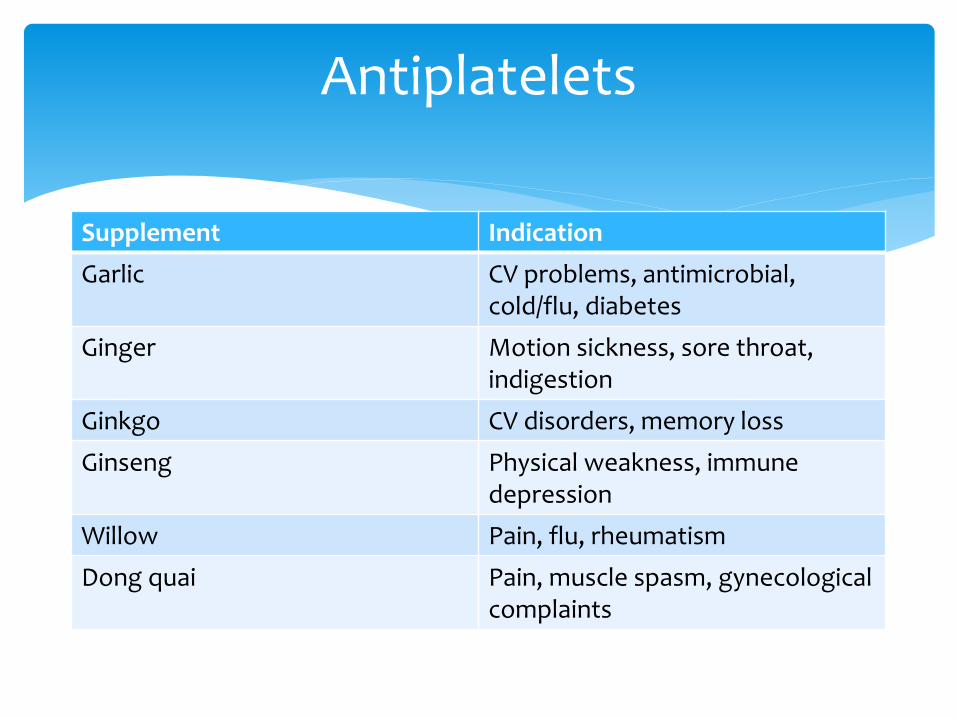
Antiplatelets
Supplement Indication
Garlic CV problems, antimicrobial, cold/flu, diabetes
Ginger Motion sickness, sore throat, indigestion
Ginkgo CV disorders, memory loss
Ginseng Physical weakness, immune depression
Willow Pain, flu, rheumatism
Dong quai Pain, muscle spasm, gynecological complaints

Anticoagulants
Supplement Indication
Horse chestnut Varicose veins, hemorrhoids
Red clover Skin conditions, cough
Fenugreek Diabetes, GI disorders, inflammation
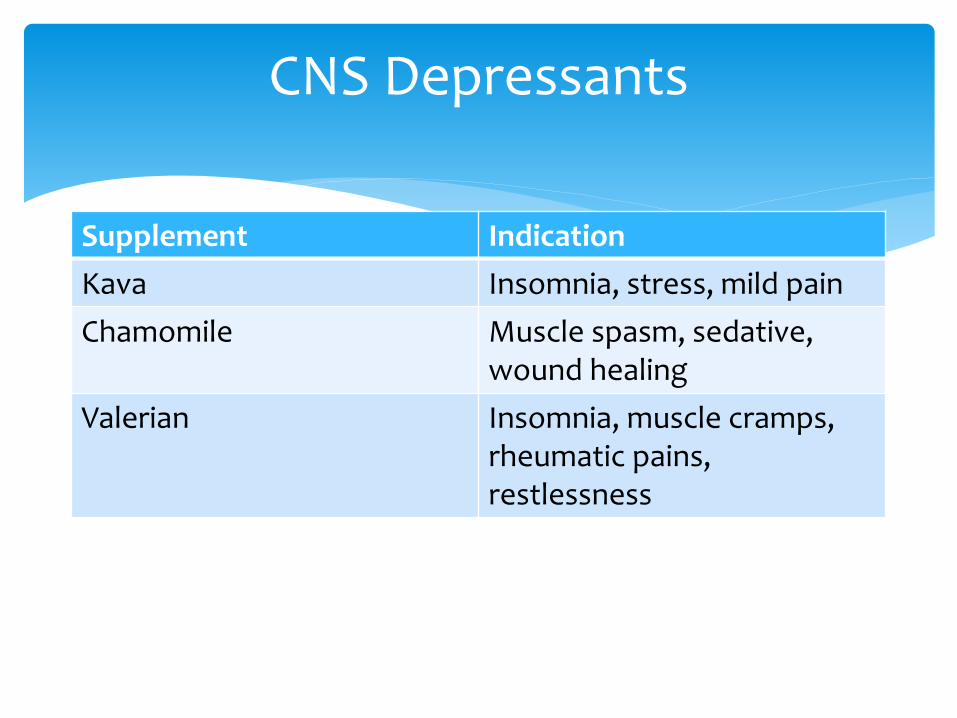
CNS Depressants
Supplement Indication
Kava Insomnia, stress, mild pain
Chamomile Muscle spasm, sedative, wound healing
Valerian Insomnia, muscle cramps, rheumatic pains, restlessness

Popular supplement used for depression, anxiety, and insomnia
May interact with the CYP-450 enzyme system, which may increase metabolism and excretion of benzodiazepines
St. John’s wort

Also known as Ma-huang
Used for weight reduction, energy enhancement, and asthma treatment
Produces increased sympathomimetic activity
Contains ephedrine and pseudoephedrine
May reduce effectiveness of anxiolytics, sedatives, anaesthetics, and other CNS depressants
Ephedra
Drug Interactions

There is a decreased antihypertensive effect with ACE inhibitors, diuretics and β-blockers
The production of some renal vasodilatory prostaglandins are dependent on active COX-1 and COX-2 enzymes
ASA is the exception
OK when co-prescribed for a short term (5 days or less)
NSAIDs and Antihypertensives

All non-specific NSAID drugs are highly protein-bound (99%) and interfere with clotting
Warfarin is highly protein-bound (99%) and has a low therapeutic index An increase to 3% circulating warfarin can be significant
Same with methotrexate
The same increase in effect is true for NSAIDs and oral hypoglycemics (e.g. glyburide) The result is hypoglycemia
NSAIDs and Warfarin

SSRIs (e.g. fluoxetine [Prozac], paroxitene [Paxil], sertraline [Zoloft]) can interfere with platelet aggregation
Increased risk of upper GI bleeding
NSAIDs and SSRIs

May be synergistic in the short-term
Can cause renal damage over time
This holds true NSAID combinations also
NSAIDs and Acetaminophen

Lithium toxicity may result, but the evidence is not clear
Avoid this combination, especially in the elderly
NSAIDs and Lithium
Toxicity to methotrexate may result
Low-dose methotrexate (e.g. for arthritis) is OK
High-dose methotrexate (e.g. for cancer) should be avoided
NSAIDs and Methotrexate

Cocaine is a vasoconstricting stimulant that works by blocking the reuptake of the neurotransmitter norepinephrine
This stimulates the myocardium and the CNS
Administering epinephrine can result in seizures, stroke, cardiac dysrhythmias or myocardial ischemia
Cocaine and LA

While the mechanisms of action with these drugs is distinct, they both affect the CNS
Can get additive sedative effects
Opioids and Alcohol

This a metabolic issue with the cytochrome P450 system
P450 CYP3A4 is the most abundant of these enzymes
Affects midazolam, triazolam and diazepam
Inhibited by grapefruit juice, erythromycin and clarithromycin and the azole antifungals (e.g. ketoconazole)
Leads to a greater effect and longer duration
BZD and grapefruit juice
Metronidazole and alcohol
Acetaminophen and alcohol
Bactericidal and bacteriostatic antibiotics
NSAIDs and cardioprotective doses of ASA
Antibiotics and oral contraceptives
Other interactions

Adverse Events During Paediatric Dental Anaesthesia
Article by Chicka et al. in Pediatric Dentistry, 2012; 34: 231-238
Analyzed 17 closed malpractice insurance claims in the US from 1993-2007
1 GA, 3 LA, 13 sedation & LA
9 outcomes of “major” severity (i.e. death or brain damage)
8 outcomes of “minor” severity (i.e no permanent morbidity)

Adverse Events During Paediatric Dental Anaesthesia
Article by Chicka et al. in Pediatric Dentistry, 2012; 34: 231-238
82% of the claims involved children < 6 years
Most sedated children are < 6 years (78%)
Average age of “major” outcomes = 3.6 years
There is an inverse relationship between patient age and sedation risk
47% of the outcomes were “minor”
Good management vs. self-limiting events

Adverse Events During Paediatric Dental Anaesthesia
Article by Chicka et al. in Pediatric Dentistry, 2012; 34: 231-238 No single sedative agent was most frequently associated with
“major” outcomes
Drug dose more important than drug choice
41% of the claims involved an overdose of LA
LA toxicity may be masked by concomitant BZD use
Most claims involved events at the dental office
The dentist is likely to be the first responder Important for the dentist and the team to be ready


















