33
Pharmacotherapy of Comorbities: Cancer Patients with HIV/AIDS MICHELLE A. RUDEK, PHARM.D., PH.D. ASSOCIATE PROFESSOR OF ONCOLOGY AND MEDICINE JOHNS HOPKINS UNIVERSITY

Pharmacotherapy of Comorbities: Cancer Patients with HIV/AIDSMICHELLE A. RUDEK, PHARM.D., PH.D.ASSOCIATE PROFESSOR OF ONCOLOGY AND MEDICINEJOHNS HOPKINS UNIVERSITY

DisclosuresSpouse Employed – Novavax
Stock – Novavax
Research Funding – Celgene Corporation, Taiho Oncology
NON FDA/EMEA Approved use of drugs or products will be referenced with regards to AIDS Malignancies.
Michelle A. Rudek, Pharm.D., Ph.D.

Overview• Trends of AIDS malignancies• Goals of HIV management• How to manage individual patients and develop clinical trials
for HIV patients with cancer• Discuss current Guidance Documents
Cancers in Patients with HIV/AIDS
AIDS-DEFINING:
• Kaposi’s sarcoma• Non-Hodgkin’s lymphoma• Cervical cancer
NON‐AIDS-DEFINING:
• Anal cancer• Colorectal• Head and neck cancer• Hepatocellular carcinomas• Hodgkin’s lymphoma• Leukemia• Lung cancer• Melanoma• Renal• Vaginal
Clin Infect Dis. 2010;50(10):1387-96.; Ann Intern Med. 2008;148(10):728-36; J Clin Oncol. 2008;26(29):4834-42.

Incidence of AIDS Malignancies
J Natl Cancer Inst 2011;103:753-762
Number of people living with AIDS, AIDS-defining cancers, non-AIDS-defining cancers, and all cancers in the United States during 1991–2005.

J Natl Cancer Inst. 2015;107: dju503
Excess Cancer Cases in People Living with HIV (PLWH)

HIV Treatment• Goal: To suppress plasma HIV RNA, preserve or improve immune function while
preventing transmission and decreasing HIV-associated morbidity/mortality while improving the duration and quality of survival
• In developed countries, initiate antiretroviral therapy (ART):• In all individuals with HIV regardless of CD4 counts with increased urgency in:
• Initial regimens selected for maximal compliance considering:• Pretreatment viral load, CD4 count, and HIV genotypic drug resistance testing• HLA-B*5701 status • Comorbidities and Coinfections• Individual preference • Drug-specific factors• Anticipated adherence
DHHS Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. October 2017; 1-298
Pregnancy Lower CD4 counts (<200 cells/mm3)
AIDS-defining conditions HIV-associated nephropathy
Acute opportunistic infections Acute/early infection
HIV/hepatitis B virus coinfection HIV/hepatitis C virus coinfection

Drug Interaction Potential: AntiretroviralsDrug Class Route of Elimination
Effect on CYP450/ transporter
Drug Interaction PotentialAs a Perpetrator
Nucleoside reverse-
transcriptase inhibitor
Renal excretion, ABC and
SLC transporter, UGT
No known effect or no
clinically relevant effect Unlikely
Nucleotide reverse-
transcriptase inhibitor
Renal excretion, ABC and
SLC transporter
CYP450 and ABC transporter
inhibitorPossible
Non-nucleoside reverse-
transcriptase inhibitor
CYP450, UGT, ABC
transporter
CYP450 and transporter
inhibitor and inducer Critical or Significant
HIV-1 protease inhibitor CYP450, UGT, ABC
transporter
CYP450 and transporter
inhibitor and inducer Critical or Significant
Integrase strand-transfer
inhibitor
UGT, ABC and SLC
transporter
CYP450 and transporter
inhibitor and inducer Critical or Significant
Fusion inhibitor Catabolism No known effect or no
clinically relevant effectPossible or Unlikely
Entry inhibitor (chemokine
receptor antagonists)CYP450, ABC and SLC
transporter
No known effect or no
clinically relevant effectPossible or Unlikely
Ritonavir- or cobicistat-
boosted regimensCYP450, ABC transporter
CYP450 and transporter
inhibitorContraindicated or Critical
DHHS Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. October 2017; 1-298
Lancet Oncol. 2011;12(9):905-12. Micromedex; UpToDate Online v. 18.1

General Considerations in Treating PLWH with Cancer• What is the treatment goal for the stage of cancer?• How advanced is the HIV infection? Are there multiple
complications (opportunistic infections)?• When does cancer diagnosis occur relative to HIV-
infection diagnosis?• Management complicated by:• Lymphadenopathy complicates staging• Perceived significant comorbidities• Perceived to be poor surgical candidates• Combination of ART with chemotherapy• Drug-drug interactions• Overlapping toxicity• Prophylaxis for opportunistic infections• Hematopoietic growth factor support
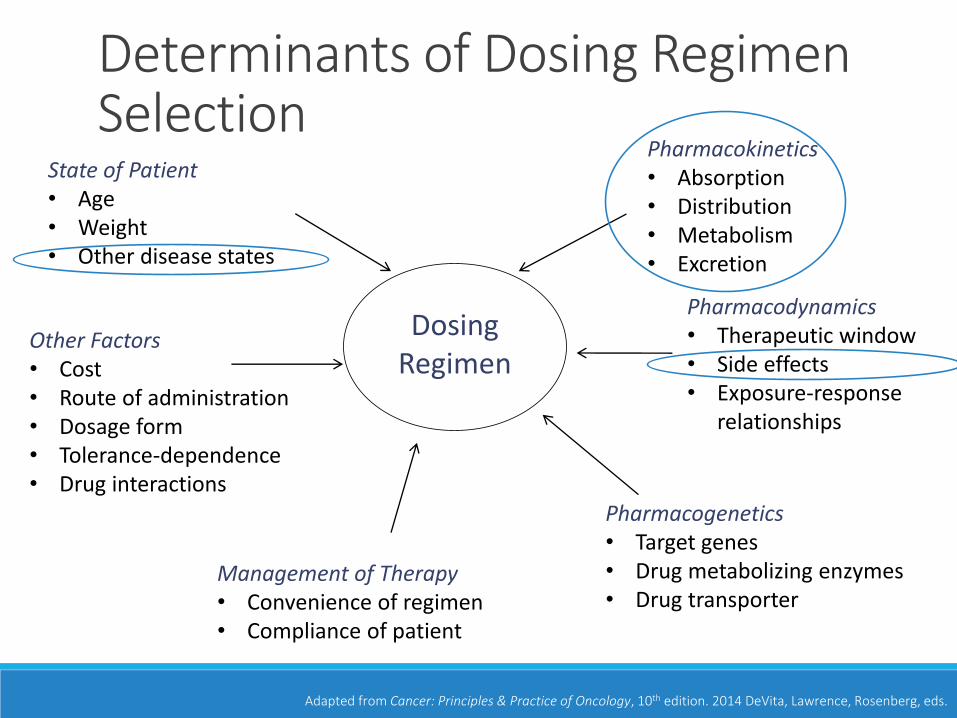
Dosing Regimen
Pharmacokinetics• Absorption• Distribution• Metabolism• Excretion
Other Factors• Cost• Route of administration• Dosage form• Tolerance-dependence• Drug interactions
Pharmacodynamics• Therapeutic window• Side effects• Exposure-response
relationships
Adapted from Cancer: Principles & Practice of Oncology, 10th edition. 2014 DeVita, Lawrence, Rosenberg, eds.
State of Patient• Age• Weight• Other disease states
Management of Therapy• Convenience of regimen• Compliance of patient
Pharmacogenetics• Target genes• Drug metabolizing enzymes• Drug transporter
Determinants of Dosing Regimen Selection

Toxicity-Related ConcernsAIDS Cancer
Neutropenia ZidovudineRitonavir-boosted ART
Cytotoxic Agents
Neuropathy Didanosine*Stavudine*
BortezomibPlatinumsTaxanes
Vinca alkaloids
QT Prolongation AtazanavirRitonavir-boosted lopinavir
Saquinavir
AnthracyclinesArsenic trioxide
Tyrosine kinase inhibitor Tamoxifen
Hepatic Function More Hepatotoxic Unconjugated hyperbilirubinemia
Lactic acidosisAssociated with allergic features
HepatitisHepatic dysfunction adjusted
based on bilirubin
*Due to toxicity concerns, these agents are not first-line in developed countries.

Docetaxel vs Paclitaxel with ART
Mir O, et al. Br J Clin Pharmacol. 2010;69(1):99-101.Rudek MA, et al. Cancer Chemother Pharmacol. 2014;73(4):729-36
In mice, the CYP3A4 inhibitors ritonavir and ketoconazole resulted in a 6.9- and 3.1-fold increase in AUC, respectively.

Special PopulationsOrgan dysfunction
Pregnant/breastfeeding women
Elderly
Pediatric
Obese
Cancer patients with HIV/AIDS
Therapeutic
Window

xIND
IND or Clinical Trial Application
Drug Development Paradigm in Oncology
Phase 0
• First-in-Human
•Microdose Study
• Lack of Therapeutic Intent
Phase 1
• First-in-Human
•All-comers
•Dose escalation
•Tolerability (MTD)
•PK
•n=20-100
Phase 2
• Specific tumor types
•One dose level
•Efficacy
•Tolerability
•n=100s
Phase 3
• Specific tumor types
•Efficacy vs. standard of care
•Tolerability vs. standard of care
•n=1000s
FDA or EMEA Approval
•Phase 4 (Post-Marketing)
•MedWatch by FDA (Long-term risks/ benefits/ use)
NDA or Marketing
Authorization
Special PopulationsHIV Patients with Cancer

Typical Clinical Trial Population•Relapsed/refractory disease • all-comers vs. select tumors
•Good performance status
•Adequate marrow and organ function
•Exclude co-morbidities
•Exclude potentially interacting drugs

Clinical Trial Design ConsiderationsConsider the overall objective of the trial.◦ Proof-of-concept vs. Therapeutic Intent vs. Maximum Tolerate Dose
Further considerations based on anticancer agent:◦ Is there a probable cause for interaction (PK or PD)?
◦ What is the likely magnitude of the interaction?
◦ What should a reasonable starting dose of anticancer drug X be in patients on ART?
◦ Is there a potential for overlapping toxicity?

Unable to utilize traditional drug-drug interaction designs:◦ Randomized crossover◦ One-sequence crossover◦ Parallel
If ART drug-drug interactions likely, utilize a stratum design:◦ ART regimens containing enzyme/transporter inducers◦ ART regimens containing enzyme/transporter inhibitors◦ Neutral ART regimens
Other considerations:◦ Exclude other concomitant medications with potential drug-drug
interactions◦ Monitor ART adherence, viral load, and CD4+ count
Clinical Trial Design

Clinical Trial Design Without Stratification
RAPAMYCIN

AMC-051 Rapamycin Pilot Study• Rapamycin is an mTOR inhibitor and a sensitive CYP3A4
substrate.• The a priori trough level of 5-10 ng/mL was more readily
achieved in the NNRTI setting.
• In patients with Kaposi’s sarcoma, rapamycin induced tumor regression and affected its molecular targets.
J Acquir Immune Defic Syndr. 2012;59(5):447-54.

Clinical Trial Design with Stratification
SUNITINIB

Sunitinib in Combination with ART in PLWHPrimary Endpoint:
◦ Determine the safety of sunitinib in patients receiving ART therapy
Secondary Endpoints: ◦ Determine the PK of sunitinib in patients receiving ART
◦ Detect alterations in immune parameters during sunitinib therapy
◦ Efficacy
QD for 4 weeks with 2 week rest.

ART Significantly Alters SunitinibMetabolite
**Efavirenz>Ritonavir but neither different than NNRTI.Sunitinib sold symbols; metabolite open symbols
Cancer. 2014;120(8):1194-202.
Ritonavir Ritonavir Efavirenz NNRTI
Sunitin
ib C
max
(ng/m
L)
0
10
20
30
40
N-d
eseth
yl s
unitin
ib C
max (n
g/m
L)
0
10
20
30
40
50
25 mg 37.5 mg 50 mg 50 mg
Sunitinb P=0.08Metabolite P=0.0008**
48%**
410%**5%
41%
Single Dose
Ritonavir Ritonavir Efavirenz NNRTI
Sunitin
ib C
min
,ss (
ng/m
L)
0
20
40
60
80
100
N-d
eseth
yl s
unitin
ib C
min
,ss (n
g/m
L)
0
10
20
30
40
50
60
70
25 mg 37.5 mg 50 mg 50 mg
Sunitinb P=0.07Metabolite P=0.006**Neutropenia P>0.05
12%
234%
3%58%
Steady-State

AMC-061 Clinical Trial Conclusion• Patients on non-ritonavir based ART regimens tolerated
standard dosing of sunitinib.
• Patients receiving ritonavir-based ART regimens who were treated with a dose of 37.5 mg/day experienced higher toxicities and dose reductions may be warranted.
Cancer. 2014;120(8):1194-202.


HIV-related eligibility in New Drug Applications (2011-2015)
J Clin Oncol. 2017; 35(33):3774-80.

HIV Eligibility Criteria in Select NCI-supported Trials (2011-2015)
J Clin Oncol. 2017; 35(33):3774-80.

Eligibility Criteria Principals
J Clin Oncol. 2017; 35(33):3774-80.
1. Criteria to define a population with HIV that is sufficiently healthy from this comorbid perspective to participate in almost any oncology study are recommended.
2. Criteria should select patients with probable long-term survival in the absence of cancer.
3. The later the phase of the trial, the more information is known about a particular therapeutic agent for the treatment of a particular condition. The level of experience with a given agent may inform eligibility criteria.
4. Criteria should not be more stringent than for HIV uninfected patients with the same disease or treatment history.

Eligibility Criteria Recommendations: Immune Criteria
J Clin Oncol. 2017; 35(33):3774-80.
1. Patients with CD4+ T-cell counts ≥350 cells/mL
• Lower CD4+ count eligibility is often appropriate
2. Patients with no active history of AIDS-defining opportunistic infections
3. Exclusion of AIDS-defining opportunistic infections:
• No opportunistic infections within past 12 months
• For studies of AIDS-defining cancers with curative potential, exclusion limited to uncontrolled opportunistic infections may be appropriate
• Patients on prophylactic antimicrobials need not be excluded due to DDI or toxicity-related concerns
Eligibility Criteria Recommendations: HIV Therapy
J Clin Oncol. 2017; 35(33):3774-80.
1. Concurrent treatment with ART according to DHHS treatment guidelines
2. Recommend criteria specifying timing of ART initiation that are appropriate for study goals and considerations for recently diagnosed PLWH or those not on effective ART.
3. Recommend exclusion of specific ART agents, when indicated, based on predicted drug-drug interactions or potential overlapping toxicities.
4. Although effective ART is generally recommended, exceptions should be considered:
• Treatment interruption or deferred initiation is appropriate in curable malignancies when ART may compromise intended full-dose oncology therapy with investigational agent(s).
• Treatment interruptions for toxicity management
• Treatment interruptions to meet scientific objective of study


NCCN Guideline Recommendations• Most PLWH who develop cancer should be offered the same cancer
therapies as HIV-negative individuals, and modifications to cancer treatment should not be made solely on the basis of HIV status.
• Care for patients diagnosed with HIV should be co-managed with an oncologist and an HIV specialist.
• Oncologists and HIV clinicians, along with HIV and oncology pharmacists, if available, should review proposed cancer therapy and ART for possible drug-drug interactions and overlapping toxicity concerns prior to initiation of therapy.

Conclusions• Patients with HIV should not be excluded from cancer clinical
trials nor from standard of care
Clin Pharmacol Ther. 2014;95(4):370-372.


















