92
FISCAL YEAR 2012 DEPARTMENT OF STATE HEALTH SERVICES PRIMARY HEALTH CARE PROGRAM 2012 POLICY MANUAL
| Date post: | 14-Apr-2018 |
| Category: |
Documents |
| Upload: | rory-rose-perea |
| View: | 235 times |
| Download: | 0 times |

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 1/92
FISCAL YEAR 2012
DEPARTMENT OF STATE HEALTH SERVICES
PRIMARY HEALTH CARE PROGRAM
2012
POLICY MANUAL
8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 2/92
SECTION ONE
GENERAL INFORMATION

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 3/92
SECTION ONEGENERAL INFORMATION
1
September 2011
Chapter 31,Health &Safety Code
In the early 1980’s, economic recession and cost containment measureson the part of employers and government agencies led to a decrease in theavailability and accessibility of health care services for many Texans. Agubernatorial and legislative task force identified the provision of primaryhealth care to the medically indigent as a major priority. The task forcerecommended the following:
• A range of primary health care services shall be made available tothe medically indigent residing in Texas.
• The Department of State Health (DSHS) shall provide or contract toprovide primary health care services to the medically indigent.These services should complement existing services and/or shouldbe provided where there is a scarcity of services.
• Health education should be an integral component of all primarycare services delivered to the medically indigent population.
Preventive services should be marketed and made accessible toreduce the use of more expensive emergency room services.
These recommendations become the basis of the indigent health carelegislative package enacted by the 69th Texas Legislature in 1985. ThePrimary Health Care Services Act, HB 1844, was part of this legislation andis the statutory authority for Primary Health Care Services (PHC)administered by DSHS. The Act delineates the specific target population,eligibility, reporting, and coordination requirements for PHC. Internet linksto the relevant Health and Safety Code and Texas Administrative Code canbe found in Appendix C of this manual.
Support for the Primary Health Care Services Act is broad-based andincludes local government associations, health professional organizations,religious organizations, citizen coalitions, and consumers. It is recognizedthat primary health care is of major importance in reducing the burden ofunnecessary illness and premature death, as well as reducing overallhealth care expenditures incurred by expensive crisis-oriented care.
PHC Rules The state rules for Primary Health Care Services in Texas can be found inthe Texas Administrative Code (TAC), Title 25, Part 1, Chapter 39,Subchapter A. Section 39.2 of the Texas Administrative Code (TAC) statesthat PHC services include:
• Diagnosis and treatment• Emergency services• Family planning services
• Preventive health services, including immunizations• Health education• Laboratory, x-ray, nuclear medicine, or other appropriate diagnostic
services

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 4/92
SECTION ONEGENERAL INFORMATION
2
September 2011
PHC Rules(continued)
• Nutrition services
• Health screening
• Home health care• Dental care•
Transportation• Prescription drugs and devices, and durable supplies• Environmental health services• Podiatry services• Social Services
TAC §39.3 and 39.4 state that, at a minimum, a PHC contractor mustprovide the following six priority primary health care services either directlyor through agreements or subcontracts with other providers:
• Diagnosis and treatment• Emergency services
• Family planning services• Preventive health services, including immunizations
• Health education
• Laboratory, x-ray, nuclear medicine, or other appropriate diagnosticservices
The Primary Health Care Services Act seeks to provide access to primaryhealth care services for those individuals, at or below 150% of the FederalPoverty Level (FPL), who are unable to access the same care throughother funding sources or programs. Contractors must assure that theservices they provide either directly or indirectly (through a system ofreferrals and/or subcontracts) are accessible to clients in terms of cost,
scheduling, distance, and cultural sensitivity.
Definitions Below are some general definitions of terms or phrases that are usedthroughout this manual.
Age – For a child to be counted as part of the household, the child must beunder 18 years of age and unmarried. The provider staff should terminatethe child’s eligibility at the end of the month the child become 18 unless thechild:
• Is a full-time student (as defined by the school) in high school,attends an accredited GED class, or regularly attends vocational ortechnical training as an equivalent to high school attendance, and
• Is expected to graduate before or during the month of his/her 19 th birthday. If the child does not meet the above criteria, he/she willbe considered a separate household of one.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 5/92
SECTION ONEGENERAL INFORMATION
3
September 2011
Definitions(continued)
Client – An individual who has been screened, determined to be eligible forservices, and has successfully completed the eligibility process.
Community Assessment – Tool used to identify factors that affect thehealth of a population and to determine the availability of resources withinthe community to impact these factors.
Contractor – The entity the Department of State Health Services hascontracted with to provide services. The contractor is the responsible entityeven if there is a subcontractor involved who actually provides the services.
Co-Payment (co-pay) – Monies collected directly from clients for services.The amount collected each month should be deducted from the MonthlyPurchase Voucher (Form B -13) and is considered program income.
Dental Services – Periodic exams, fillings, prophylactic cleaning, etc.performed in a dental office or clinic.
Department of State Health Services (DSHS) – The agency responsiblefor administering physical and mental health-related prevention, treatment,and regulatory programs for the State of Texas.
Diagnosis – The recognition of disease status determined by evaluatingthe history of the client and the disease process, and the signs andsymptoms present. (Determining the diagnosis may require microscopic(i.e. culture), chemical (i.e., blood tests), and/or radiological examinations(x-rays).
Eligibility Date – Date the individual submits a completed application tothe provider. The eligibility expiration date will be twelve months from theeligibility date.
Emergency Services – Services provided to individuals when there is anunexpected health condition that requires immediate attention.
Environmental Health – The provision of treating a person’s surroundingsin regards to a health condition.
Family Composition/Household – A person living alone or a group of twoor more persons related by birth, marriage (including common law) oradoption, who reside together and who are legally responsible for the
support of the other person.
Family Planning Services – Assisting women and men in planning theirfamilies, whether it is to achieve, postpone, or prevent pregnancy. Familyplanning services include the following: pregnancy test (if indicated),health history, risk assessment, physical examinations, lab tests,counseling/education, and contraceptive supplies.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 6/92
SECTION ONEGENERAL INFORMATION
4
September 2011
Definitions(continued)
Federal Poverty Level (FPL) – The set minimum amount of income that afamily needs for food, clothing, transportation, shelter and othernecessities. In the United States, this level is determined by theDepartment of Health and Human Services. FPL varies according to familysize. The number is adjusted for inflation and reported annually in the formof poverty guidelines. Public assistance programs, such as Medicaid in theU.S., define eligibility income limits as some percentage of FPL.
Fiscal Year – State fiscal year, September 1 – August 31.
Health and Human Services Commission (HHSC) – State agency thathas oversight responsibilities for designated Health and Human Servicesagencies, including DSHS, and administers certain health and humanservices programs including the Texas Medicaid Program, Children’sHealth Insurance Program (CHIP), and Medicaid waste, fraud, and abuseinvestigations.
Health Screening – The provision of tests, i.e. blood glucose, serumcholesterol, fecal occult blood, as a meansFor determining the need for intervention and perhaps morecomprehensive evaluation.
Health Service Region – For administrative purposes, DSHS has groupedcounties within a specified geographic area into 11 Health ServiceRegions.
Home Health Care – Services include Registered Nurse (RN) visits forskilled nursing observation, assessment, evaluation, and treatmentprovided by a physician specifically requests the RN visit for this purpose.
A home health aide to assist with administering medication is also covered.
Laboratory, X-Ray, or other Appropriate Diagnostic Services – Studiesor tests ordered by the client’s health care practitioner(s) to evaluate anindividual’s health status for diagnostic purposes.
Medicaid – Title XIX of the Social Security Act; reimburses for health careservices delivered to low-income clients who meet eligibility guidelines.
Minor – A person who has not reached his/her 18 th birthday and who hasnot had the classification of minor removed in court or who is not or neverhas been married or recognized as an adult by the State of Texas.
Nutritional Services – The provision of services to identify the nutritionalstatus of an individual, and instruction which includes appropriate dietaryinformation based on the client’s needs, i.e. age, sex, health status, culture.Information may be provided on an individual, one- to-one basis, or to agroup of individuals.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 7/92
SECTION ONEGENERAL INFORMATION
5
September 2011
Definitions(continued)
Outreach – Activities that are conducted with the purpose of informing andeducating the community about services and increasing the number ofparticipants.
Podiatry Services – The study and care of the foot, including its anatomy,pathology, and medical/surgical treatment.
Prescription Drugs and Devices and Durable Supplies – Medicallynecessary pharmaceuticals, medical supplies (capable of withstandingwear) which are needed for the treatment of a diagnosed condition.
Presumptive Eligibility – Short-term availability and access to health careservices (90 days) when an immediate medical need exists as determinedby a medical professional and the client screens potentially eligible forservices.
Preventive Health Care Services – The major emphasis is placed onguarding or defending an individual or group against specific illness orinjury. Included are immunizations, risk assessments, health histories, andbaseline physicals for early detection of disease and restoration to aprevious state of health, and prevention of further deterioration and/ordisability.
Program Income – Monies collected directly by the contractor/provider forservices provided under the grant award.
Provider – An individual clinician or group of clinicians who provideservices.
Re-certification – The process of re-screening and determining eligibilityfor the next year.
Resident Alien – A person who is not an U.S. citizen, and has animmigration document.
Service – Any client encounter at a facility that results in the client having amedical or health-related need met.
Social Services – The provision of counseling and guidance; assistance toclient and family in locating, accessing, and utilizing appropriate communityresources.
Texas Resident – An individual who resides within the geographicboundaries of the state.
Transportation – Services provided to a client for the purpose of receivinga required health care service. Transportation could be provided viaprivate vehicle, public transportation, project site vehicle, or emergencymedical vehicle.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 8/92
SECTION ONEGENERAL INFORMATION
6
September 2011
Definitions(continued)
Treatment – Any specific procedure used for the cure or the improvementof a disease or pathological condition.
Undocumented Alien – A person who is not an U.S. citizen, and has noimmigration documentation.
Unduplicated Client – Clients are counted only regardless of the numberof services they receive. One client seen four times is counted as oneunduplicated client and a family of three seen once is counted as threeunduplicated clients.
Acronyms
Acronym Term
ADA Americans with Disabilities Act
BCCS Breast and Cervical Cancer ServicesCAM Complementary and Alternative MedicationsCDSB Contract Development and Support BranchCFTR Cystic Fibrosis Transmembrane Conductance
RegulatorCHIP Children’s Health Insurance ProgramCIHCP County Indigent Health Care ProgramCLIA Clinical Laboratory Improvement AmendmentsCMB DSHS Contract Management BranchCPR Cardiopulmonary ResuscitationDES DiethylstilbestrolDHHS U.S. Department of Health and Human Services
DSHS Texas Department of State Health ServicesEMR Electronic Medical RecordFPL Federal Poverty LevelFQHC Federally Qualified Health CenterFSR Financial Status ReportHIPPA Health Insurance Portability and Accountability
Act of 1996HHSC Texas Health and Human Services CommissionHPV Human Papilloma VirusHSR DSHS Health Service RegionIRB Institutional Review BoardLEP Limited English Proficiency
MCH Maternal and Child Health ServicesOTC Over the CounterPMU DSHS Performance Management UnitPHC Primary Health CarePPCU DSHS Preventive and Primary Care UnitQA Quality AssuranceQM Quality ManagementQMB DSHS Quality Management Branch

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 9/92
SECTION ONEGENERAL INFORMATION
7
September 2011
RFP Request for ProposalRSDI Retirement Survivors Disability IncomeSDO Standing Delegation OrdersSSA Social Security AdministrationSSDI Social Security Disability Income
SSI Supplemental Security IncomeSTI Sexually Transmitted InfectionSTL South Texas LabTAC Texas Administrative CodeTANF Temporary Assistance for Needy FamiliesTMHP Texas Medicaid Healthcare PartnershipTMPPM Texas Medicaid Provider Procedures ManualWHL Women’s Health Lab

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 10/92
SECTION TWO
PROGRAM ADMINISTRATION

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 11/92
SECTION TWOPROGRAM ADMINISTRATION
1
September 2011
Client Access The contractor must ensure that clients are provided services in a timelyand non-discriminatory manner. The contractor must:
Have a policy in place that delineates the timely provision of
services; Comply with all applicable civil rights laws and regulations including
Title VI of the Civil Rights Act of 1964, the Americans withDisabilities Act of 1990, the Age Discrimination Act of 1975, andSection 504 of the Rehabilitation Act of 1973, and ensure servicesare accessible to persons with limited English proficiency (see:http: www.lep.gov/ ) and speech or sensory impairments;
Have a system to prioritize client’s needs;
Have a triage system that utilities qualified staff;
Screen clients in a way that is respectful and convenient;
Provide referral resources for individuals that cannot be served orcannot receive a specific service;
Continue to provide services to established clients once funds havebeen expended, and
A contractor that is designated as a FQHC shall operate extendedweekend and evening hours a minimum of one time per month.
AbuseReporting
DSHS CHILD ABUSE COMPLIANCE AND MONITORING
Chapter 261 of the Texas Family Code requires child abuse reporting.Contractors/providers are required to develop policies and procedures thatcomply with the child abuse reporting guidelines and requirements set forthin Chapter 261 and the DSHS Child Abuse, Screening, Documenting and
Reporting Policy for Contractors/Providers. Contractors must adopt theDSHS Child Abuse Screening, Documenting and Reporting Policy forContractors/Providers and develop an internal policy specific tohow these reporting requirements will be implemented throughout theiragency, how staff will be trained and how internal monitoring will be doneto ensure timely reporting.
The following outlines how the DSHS Quality Management Branch (QMB)staff will review for contractor compliance with these requirements.
Policy – Contractors/providers will be monitored to ensure compliance withscreening for child abuse and reporting according to Chapter 261 of the
TexasFamily Code and the DSHS Child Abuse Screening, Documenting, andReporting Policy for Contractors/Providers.
Procedures – During site monitoring of contractors by QMB the followingprocedures will be utilized to evaluate compliance:
1) The contractor's process used to ensure that staff is reporting accordingto Chapter 261 and the DSHS Child Abuse Screening, Documenting and

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 12/92
SECTION TWOPROGRAM ADMINISTRATION
2
September 2011
AbuseReporting(continued)
Reporting Policy for Contractors will be reviewed as part of the Core Tool.To verify compliance with this item, monitors must review: a) that thecontractor adopted the DSHS Policy; b) the contractor's internal policywhich details how the contractor will determine, document, report, andtrack instances of abuse, sexual or non-sexual for all clients under the ageof 17 in compliance with the Texas Family Code, Chapter 261 and theDSHS Policy; c) the contractor followed their internal policy and the DSHSPolicy; and d) the contractor documentation of staff training on child abusereporting requirements and procedures.
2) All records of clients under 14 years of age who are pregnant or have aconfirmed diagnosis of an STD acquired in a manner other than throughperinatal transmission or transfusion will be reviewed for appropriatescreening and reporting documentation as required in the clinic or sitebeing visited during a site monitoring visit. The review of the records willinvolve reviewing that the DSHS Child Abuse Reporting Form was utilized;a report was made; and the report was made in the proper timeframesrequired by law.
3) If during the record review process, noncompliance is identified, the staffperson responsible will be notified and asked to make a report as requiredby law. The agency director will also be notified of the problem.Noncompliance will again be identified during the Exit Conference with thecontractor.
4) If it is found during routine record review of other records for servicesthat a report should have been made as evidenced by the age of the clientand evidence of sexual activity, the failure to appropriately screen andreport will be identified as lack of compliance with the DSHS Policy; and
the QMB will identify the need for the contractor to train staff. Failure toreport will be brought to the attention of the staff person who should havemade the report or the appropriate supervisor with a request to immediatelyreport. This failure to report will also be discussed with the agency director.
5) The report sent to the contractor will also indicate the number ofapplicable records reviewed in each clinic and the number of records thatwere found to be out of compliance. This report will be sent to thecontractor 4 to 6 weeks from the date of the review, which is theusual process for Site Monitoring Reports.
6) The contractor will then be given 6 weeks to respond with written
corrective actions to all findings. If the contractor has other findings thatwarrant technical assistance or accelerated monitoring review, eitherregional or central office staff will make the necessary contacts. Recordsand/or policies will again be reviewed to ensure compliance with Chapter261 and the DSHS Policy requirements. If any subsequent finding ofnoncompliance is identified during a subsequent monitoring or technicalassistance visit, the contractor will be referred for financial sanctioning.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 13/92
SECTION TWOPROGRAM ADMINISTRATION
3
September 2011
AbuseReporting(continued)
7) If the contractor does not provide corrective actions during the requiredtime period, the contractor will be sent a past due letter with a time periodof 10 days to submit the corrective actions. If the corrective actions are notsubmitted during the time period given, failure to submit the correctiveaction is considered a subsequent finding of noncompliance and thecontractor/provider will be referred for financial sanctioning due tononcompliance with Chapter 261 and the DSHS Policy.
8) If a contractor is found to have minimal findings overall but did havefindings of noncompliance with Chapter 261 and the DSHS Policy, anadditional sanction accelerated monitoring visit solely to review child abusereporting will not be conducted. For agencies that receive technicalassistance visits as a result of a quality assurance review, the agency willagain be reviewed for compliance with child abuse reporting for therequirements with which the agency did not comply. In all cases, thecorrective actions submitted by the contractor will be reviewed toensure that the issues have been addressed. Agencies who do not receivea sanction or technical assistance visit will be required to complete theDSHS Progress Report, Compliance with Child Abuse Reporting within 3months after the corrective actions are begun (no later than 6 months fromthe initial visit). Failure to submit a Progress Report within the required timeperiod or submission of a report that is not adequate constitutes asubsequent finding of noncompliance with the DSHS Child AbuseScreening, Documenting, and Reporting Policy for Contractors/Providersand the contractor will be referred for financial sanctions.
Information about this topic is available on the internet at:http://www.dshs.state.tx.us/childabusereporting/default.shtm.
.
Confidentiality All contracting agencies must be in compliance with the U.S. HealthInsurance Portability and Accountability Act of 1996 (HIPPA) establishedstandards for protection of client privacy. Information about HIPPA can befound at: http://www.dshs.gov/ocr/hipaa/ .
Employees and volunteers must be made aware during orientation thatviolation of the law in regard to confidentiality may result in civil damagesand criminal penalties.
The client’s preferred method of follow-up to clinic services (cell phone,email, work phone) and preferred language must be documented in theclient’s record. (See Client Health Record Section Four, page 8).
Each client must receive verbal assurance of confidentiality and anexplanation of what confidentiality means (kept private and not sharedwithout permission) and any applicable exceptions such as abuse reporting(See Abuse Reporting, Section Two, page 1).
8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 14/92
SECTION TWOPROGRAM ADMINISTRATION
4
September 2011
Non-Discrimination
Non-Discrimination(continued)
DSHS contractors must comply with state and federal anti-discriminationlaws, including without limitation:
1. Title VI of the Civil Rights Act of 1964 (42 U.S.C. §2000d et seq.);2. Section 504 of the Rehabilitation Act of 1973 (29 U.S.C. §794);3. Americans with Disabilities Act of 1990 (42 U.S.C. §12101 et seq. 4. Age Discrimination Act of 1975 (42 U.S.C. §§6101-6107);5. Title IX of the Education Amendments of 1972 (20 U.S.C. §§1681-
1688);6. Food Stamp Act of 2008 (7 U.S.C. §2011 et seq .); and7. HHSC’s administrative rules, as set forth in the Texas
Administrative Code, to the extent applicable.
To ensure compliance with DSHS non-discrimination policies DSHScontractors must:
Have a written policy that states the agency does not discriminateon the basis of race, color, national origin including LEP, religion,disability, age, or sex;
Sign a written assurance as to compliance with applicable federaland state civil rights laws and regulations;
Have procedures for notifying the HHSC Civil Rights Office of anyprogram or service-related discrimination allegation or complaint within
ten (10) calendar days after receipt of the allegation or complaint.
Notice provided pursuant to this section must be directed to:
HHSC Civil Rights Office701 W. 51st Street, Mail Code W206
Austin, Texas 78751
Phone Toll Free: (888) 388-6332Phone: (512) 438-4313TTY Toll Free: (877) 432-7232
Fax: (512) 438-5885 Notify all clients and applicants of the contractors non-
discrimination policies and complaint procedures;
Ensure that all contractor staff is trained in the agency’s non-discrimination policies and complaint procedures;
Take reasonable steps to ensure that LEP persons havemeaningful access to its programs and services, and not require aclient with LEP to use friends or family members as interpreters.
However, a family member or friend may serve as their interpreterat the client’s request, and the family member or friend does notcompromise the effectiveness of the service or violate clientconfidentiality
The contractor must prominently display in client common areas, includinglobbies and waiting rooms, front reception desks and locations whereclients apply for services, the following three posters:

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 15/92
SECTION TWOPROGRAM ADMINISTRATION
5
September 2011
“Know Your Rights” [English] [Spanish]
Size: 8.5” x 11” (standard size sheet of paper)Posting Instructions: Post the English and Spanish versions ofthis poster next to each other Questions: Contact the HHSC CivilRights Office
“Need an Interpreter” [Language Translation] [American SignLanguage]
Size: 8.5” x 11” (standard size sheet of paper)Posting Instructions: Post the “Language Translation” versionand American Sign Language” version next to each otherQuestions: Contact the HHSC Civil Rights Office
Americans with Disabilities Act [English A] [Spanish A][English B] [Spanish B]
Size: 8.5” x 11” or 8.5” x 14” Postinginstructions: Post with other civil rights postersQuestions: Contact the HHSC Civil Rights Office
The contractor must have available, completed, and signed copies of theNon-Discrimination Policies and Procedures Survey, ADA/Section 504Policies and Procedures, and Limited English Proficiency (LEP) Policiesand Procedures Survey prior to any scheduled on-site review by theQuality Management (QMB) review team.
More information about applicable laws and regulations can be
found on HHSC Office of Civil Rights Office website at:http://www.hhs.state.tx.us/aboutHHS/CivilRights.shtml.
The Non-Discrimination Policies and Procedures Survey,ADA/Section 504 Policies and Procedures Survey, and LimitedEnglish Proficiency (LEP) Policies and Procedures Survey and theirinstructions can be downloaded at the QMB Website at: http://www.dshs.states.tx.us/qmb/contact.shtm.
Termination ofServices
Clients must never be denied services due to an inability to pay.
Contractors have the right to terminate services to a client if the client isdisruptive, unruly, threatening, or uncooperative to the extent that the clientseriously impairs the contractor’s ability to provide services or if the client’sbehavior jeopardizes the safety of himself or herself, clinic staff, or otherclients. Contractors have the right to terminate services to a client if theclient is disruptive, unruly, threatening, or uncooperative to the extent thatthe client seriously impairs the contractor’s ability to provide services or ifthe client’s behavior jeopardizes his or her own safety, clinic staff, or otherclients.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 16/92
SECTION TWOPROGRAM ADMINISTRATION
6
September 2011
Any policy related to termination of services must be included in thecontractor’s policy and procedures manual.
Resolution of
Complaints
Contractors must ensure that clients have the opportunity to express
concerns about care received and to further ensure that those complaintsare handled in a consistent manner.
Contractor’s policy and procedure manuals must explain the processclients will follow if they are not satisfied with the care received or feel theyhave been discriminated against or treated inappropriately or unfairly. Inaccordance with PHC rule, 25 TAC §39.10 (relating to Appeals), anapplicant or client may appeal a decision according to the proceduresoutlined in 25 TAC §§1.51 – 1.55 (relating to DSHS Fair HearingsProcedures). If an aggrieved client requests a hearing, contractors shallnot terminate services to the client until a final decision is rendered.
Any client complaint must be documented in the client’s record.
Client RecordsManagement
Client RecordsManagement(continued)
DSHS contractors must have an organized and secure client recordsystem. The contractor must ensure that the record is organized, readilyaccessible, and available to the client upon request with a signed releaseof information. The records must be kept confidential and secure, asfollows:
Safeguarded against lost and used by unauthorized persons;
Secured by lock when not in use or inaccessible to unauthorizedpersons; and
Maintained in a secure environment in the facility as well as duringtransfer between clinics and in between home and office visits.
The written consent of the client is required for the release of personallyidentifiable information, except as may be necessary to provide services tothe client or as required by law, with appropriate safeguards forconfidentiality. HIV information should be handled according to law.(See: http://www.dshs.state.tx.us/hivstd/policy/laws.shtm).
When information is requested, contractors should release only the specificinformation requested. Information collected for reporting purposes may bedisclosed only in summary, statistically, or in a form that does not identifyparticular individuals. Upon request, clients transferring to other providers
must be provided with a copy or summary of their record to expeditecontinuity of care. Electronic records are acceptable as medical records.
Contractors, providers, sub-recipients, and subcontractors must maintainfor the time period specified by DSHS all records pertaining to clientservices, contracts, and payments. Record retention requirements arefound in 15 TAC §354.1004 (relating to Time Limits for Submitted MedicaidClaims) and 22 TAC 165 (relating to Medical Records). Contractors must

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 17/92
SECTION TWOPROGRAM ADMINISTRATION
7
September 2011
follow contract provisions and the DSHS Retention Schedule for MedicalRecords. All records relating to services must be accessible forexamination at any reasonable time to representatives of DSHS and asrequired by law. DSHS guidelines for medical record retention areavailable at: http://www.dshs.state.tx.us/records/medicalrec.shtm
All medical records and supporting documentation for Title XIX Medicaidservices must be maintained in accordance with Medicaid rules as outlinedin the 2010 Texas Medicaid Provider Procedures Manual, Section 1.4.3(page 1-18).
http://www.tmhp.com/TMPPM/2010/Vol1_01_Provider_Enrollment.pdf
PersonnelPolicy andProcedures
Contractors must develop and maintain personnel policies and proceduresto ensure that clinical staff are hired, trained, and evaluated appropriatelyto their job position. Personnel policies and procedures must include jobdescriptions, a written orientation plan for new staff to include skillsevaluation and/or competencies appropriate for the position, andperformance evaluation process for all staff. Job descriptions, includingthose for contracted personnel, must specify required qualifications andlicensure. All staff must be appropriately identified with a name badge.
Contractors must show evidence that employees meet all requiredqualifications and are provided annual training. Job evaluations shouldinclude observation of staff/client interactions during clinical, counselingand educational services.
Contractors shall establish safeguards to prohibit employees from usingtheir positions for a purpose that constitutes or presents the appearance of
personal or organizational conflict of interest or personal gain.
Contractors must provide medical care services under the supervision,direction, and responsibility of a qualified medical director.
Contractors must have a documented plan of organized staff developmentbased on an assessment of:
Training needs;
Quality assurance indicators; and
Changing regulations/requirements.
Contractors must also include orientation and in-service training for allpersonnel, including volunteers. There must be documentation of initialemployee orientation and continuing education.
Facilities andEquipment
DSHS contractors are required to maintain a safe environment at all times.Contractors must have written policies and procedures that addresshazardous waste, fire safety, and medical equipment.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 18/92
SECTION TWOPROGRAM ADMINISTRATION
8
September 2011
Hazardous Materials – Contractors must have written policies andprocedures that address:
The handling, storage, and disposing of hazardous materials andwaste according to applicable laws and regulations;
The handling, storage, and disposing of chemical and infectiouswaste including sharps; and
An orientation and education program for personnel who manage orhave contact with hazardous materials and waste
Fire Safety – Contractors must have a written fire safety policy thatincludes a schedule for testing and maintenance of fire safety equipment.Evacuation plans for the premises must be clearly posted and visible to allstaff and clients.
Medical Equipment – Contractors must have a written policy and maintaindocumentation of the maintenance, testing, and inspection of medicalequipment. Documentation must include:
Assessments of the clinical and physical risks of equipment throughinspection, testing and maintenance;
Reports of any equipment management problems, failures and useerrors;
An orientation and education program for personnel who usemedical equipment; and
Manufacturer recommendations for care and use of medicalequipment.
Smoking Ban – Contractors must have written policies that prohibitsmoking in any portion of their indoor facilities. If a contractor subcontractswith another entity for the provision of health services, the subcontractor
must also comply with this policy.
Disaster Response Plan – Written and oral plans that address how staffsare to respond to emergency situations (i.e., fires, flooding, power outage,bomb threats, etc.). A disaster response plan must be in writing, formallycommunicated to staff, and kept in the workplace available to employeesfor review. For an employer with 10 or fewer employees, the plan may becommunicated orally to employees.
For additional resources on facilities and equipment, you can visit:http://osha.gov/ .

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 19/92
SECTION TWOPROGRAM ADMINISTRATION
9
September 2011
QualityManagement
Organizations that embrace Quality Management (QM) concepts andmethodologies and integrate them into the structure of the organization andday-to-day operations discover a very powerful management tool. QualityManagement programs can vary in structure and organization and will bemost effective if they are individualized to meet the needs of a specific
agency, services and the populations served.
Contractors are expected to develop quality processes based on the fourcore Quality Management principles of focusing on: the client, systemsand processes, measurement and teamwork. Contractors must have aQuality Management program individualized to their organizationalstructure and based on the services provided. The goals of the qualityprogram should ensure availability and accessibility of services, and qualityand continuity of care.
A Quality Management program must be developed and implemented thatprovides for ongoing evaluation of services. Contractors should have a
comprehensive plan for the internal review, measurement and evaluation ofservices, the analysis of monitoring data, and the development ofstrategies for improvement and sustainability. Contractors who subcontractfor the provision of services must also address how quality will beevaluated and how compliance with policies and basic standards will beassessed with the subcontracting entities.
The Quality Management Committee, whose membership consists of keyleadership of the organization, including the Executive Director/CEO andthe Medical Director, where applicable, annually reviews and approves thequality work plan for the organization. The Quality ManagementCommittee must meet at least quarterly to:
Receive reports of monitoring activities; Make decisions based on the analysis of data collected;
Determine quality improvement actions to be implemented; and
Reassess outcomes and goal achievement.
Minutes of the discussion and actions taken by the committee must bemaintained.
The quality work plan at a minimum must:
Include clinical and administrative standards by which services willbe monitored;
Include process for credentialing and peer review of clinicians;
Identify individuals responsible for implementing monitoring,evaluating and reporting;
Establish timelines for quality monitoring activities;
Identify tools/forms to be utilized; and
Outline reporting to the Quality Management Committee.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 20/92
SECTION TWOPROGRAM ADMINISTRATION
10
September 2011
QualityManagement(continued)
Although each organization’s quality program is unique, the followingactivities must be undertaken by all agencies providing client services:
On-going eligibility, billing, and clinical record reviews to assurecompliance with program requirements and clinical standards ofcare;
Tracking and reporting of adverse outcomes;
Client satisfaction surveys;
Annual review of facilities to maintain a safe environment, includingan emergency safety plan; and
Annual review of policies, clinical protocols and standing delegationorders (SDOs) to ensure they are current.
Data from these activities must be presented to the Quality ManagementCommittee. Plans to improve quality should result from the data analysisand reports considered by the committee and should be documented.
Information on the operating process of DSHS’s Quality ManagementBranch as well as policies and review tools can be located at:http://www.dshs.state.tx.us/qmb/default.shtm.
ProgrammaticEligibility DeskReviews
Contractor shall provide information and supporting documentation asrequested by DSHS to conduct programmatic desk reviews to verify clienteligibility for PHC Program. Failure to submit requested information in atimely manner may result in sanctions according to provisions of the
contract. If contractor’s desk reviews results in a finding ofmisappropriation of DSHS PHC co-payment (co-pay) policy, contractorshall reimburse client(s).

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 21/92
SECTION THREE
ELIGIBILITY CRITERIA
& CLIENT SERVICES

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 22/92
SECTION THREEELIGIBILITY CRITERIA
1
PHC 10-1September 2010
GeneralPrinciples
For an individual to receive PHC services, three (3) criteria must be met:
•
Not eligible for other programs/benefits providing the same services;• Texas resident; and• Gross family income at or below 150% of the adopted Federal
Poverty Level (FPL).
Contractor Responsibilities – The contractor must ensure the eligibilityprocess is complete and includes documentation of the following:
• Individual/family name, present address, date of birth, and whetherthe individual/family members are currently eligible for Medicaid orother benefits;
• Health insurance policies, if applicable, providing coverage for the
individual, spouse, and dependent(s);• Monthly income of individual and spouse; and• Other benefits available to the family or individual. Any specified or
other supporting documentation necessary for the contractor todetermine eligibility;
The contractor will:
• Use the DSHS Funding Source - Application For Health CareAssistance (Form EF05-13229); DSHS Funding Source – Worksheet(Form EF05-13227); and verification/documentation proceduresestablished by DSHS or completion of a comparable paper or
electronic screening and eligibility tool that has the required DSHSinformation for determining eligibility;• Assist the applicant with accurately completing the application for
screening and eligibility determination purposes;• Ensure that the verification the individual provides is sufficient to
make an eligibility decision. Request for Information (Form 104) maybe used to assist applicants with requested verification requirements;
• Document oral designations of any additional contacts;• Determine eligibility for PHC services based on the three (3) eligibility
criteria;• Provide the eligible individual information regarding the services
he/she is entitled to receive and his/her rights and responsibilities;• Advise the client of his/her responsibility to report changes; and• Determine the effect reported changes have on the client’s eligibility
by re-screening and completing the eligibility determination process.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 23/92
SECTION THREEELIGIBILITY CRITERIA
2
September 2011
GeneralPrinciples(continued)
The contractor shall allow the individual an opportunity to resolve anydiscrepancy by providing documentary evidence or by designating a suitablecontact to verify information. If the individual fails or refuses to do so,eligibility can be denied. Document this information on the DSHS FundingSource - Worksheet.
Special circumstances may occur in the disclosure of information,documentation of pertinent facts, or events surrounding the client’sapplication for services that make decisions and judgments by the contractorstaff necessary. These circumstances should be documented in the caserecord on the DSHS Funding Source - Worksheet.
Applicant’s Responsibility –
• Complete the DSHS Funding Source - Application For Health CareAssistance (Form EF05-13229) or request assistance for completion;
• Provide requested verification by the contractor. Failure to provide all
required information will result in denial of eligibility. If verification isnot available or is insufficient to determine eligibility, contractor staffshould ask the individual to designate a contact person to provide theinformation.
Client’s Responsibility for Reporting Changes – A client must reportchanges in the following area: income, family composition, residence,address, employment, types of medical insurance coverage, and receipt ofMedicaid and/or third-party coverage benefits. The client may reportchanges by mail, telephone, in-person, or through someone acting on theindividual’s behalf. Changes must be reported no later than 14 days after theclient is aware of the change. If changes result in the client no longer
meeting eligibility criteria, the individual is denied continued services. Bysigning the required forms, the individual attests to the truth of theinformation provided.
Screening &EligibilityDetermination
Clients Screened Potentially Eligible for Other Benefits – Contractorsmust work to ensure that individuals seeking PHC covered services useother programs or benefits first. If individuals are determined potentiallyeligible for other benefits, contractors must refer them to the specificprograms and assist them in completing the eligibility determination process.It is possible that a family will be referred to several programs as a result ofthe eligibility determination process. Programs/benefits that must be used
first include:• Private/Employer Insurance;• Medicare;• Medicaid;• TRICARE;• County Indigent Health Care;• Children with Special Health Care Needs;

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 24/92
SECTION THREEELIGIBILITY CRITERIA
3
September 2011
Screening &EligibilityDetermination(continued)
• CHIP (other than family planning services);• CHIP Perinatal;• Title V, Title X, Title XIX (including WHP), and Title XX Family
Planning;•
Breast and Cervical Cancer Services;• Women’s Health Program;• Worker’s Compensation;• Veteran’s Administration Benefits; or• Other comprehensive healthcare plans.
Individuals must be screened for potential Medicaid, CHIP, or other programsby using the DSHS Funding Source – Application For Health CareAssistance (Form EF05-13229) or a comparable paper or electronicscreening and eligibility tool that has the required DSHS information andapplicant’s signature for determining eligibility. A copy of the Application ForHealth Care Assistance must be maintained in the medical record.
For PHC purposes, contractors may use the Health and Human ServicesCommission’s (HHSC) Your Texas Benefits website(www.yourtexasbenefits.com) to assist in the screening of client eligibility.The website offers access to information on HHSC benefits includingMedicaid, Supplemental Nutrition Assistance Program (SNAP), TemporaryAssistance for Needy Families (TANF), Children’s Health Insurance(CHIP), and nursing home care and other services for people who are elderlyor have disabilities. The use of this system may replace the DSHS FundingSource – Worksheet (Form EF05-13227), but can not replace the DSHSFunding Source – Application (Form EF 05-13299). More information aboutHHSC benefits can also be obtained by calling 2-1-1.
The applicant is responsible for completing page one of his/her own DSHSFunding Source – Application For Health Care Assistance (Form EF05-13229). If the applicant is incompetent, or incapacitated, someone actingresponsibly for the client (a representative) may represent the applicant inthe application and the review process, including signing and dating the FormEF05-13229 on the applicant’s behalf. This representative must beknowledgeable about the applicant and his household. A copy of this formand instructions can be found in the Forms Section of the Policy andProcedures Manual. If assistance is needed in completing the form, thecontractor shall provide knowledgeable staff to assist. It is acceptable to fillout the form once and photocopy the form for the number of family members
needed. The family member name listed under the family composition charton question 1 can be (highlighted/circled) to indicate the intended clientrecord in which it shall be filed. If the applicant is married and his/her spouseis a household member, the spouse must also sign and date the DSHSFunding Source – Application For Health Care Assistance (Form EF05-13229). If confidentiality of services is a concern, separate forms forspouses may be completed. The signature of anyone assisting in completionof the form is required as well. The form is filed in the client record.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 25/92
SECTION THREEELIGIBILITY CRITERIA
4
September 2011
Screening &EligibilityDetermination(continued)
Family Composition/Household
Establishing family composition/household is an important step in theeligibility process. Assessment of income eligibility relies on an accuratecount of family members. A family is defined as a person living alone or a
group of two or more persons related by birth, marriage (including common-law), or adoption, which reside together and are legally responsible for thesupport of the other person. Unborn children are also included in family size.
Children and Family Composition – A child must be under 18 years of age tobe counted as part of a family. Eligibility will end on the last day of the monththe child become 18 years of age unless the child is:
• A full-time high school student as defined by the school, attends anaccredited GED class, or regularly attends vocational or technicaltraining in place of high school, and
•
Expected to graduate from one of the above before or during themonth of his/her 19th birthday.
A child who is 18 years of age or older and resides with his/herparent(s)/guardian(s), but is not currently attending high school is considereda family of one.
A child may be considered part of a family when living with relatives otherthan natural parents if documentation can be provided that verifies therelationship. Acceptable documents include birth certificates or other legaldocuments that demonstrate the relationship between the caretaker and thechild. If no biological relationship exists between the caretaker ordocumentation is not provided to verify biological relationship:
• The child becomes a separate PHC household;• The situation must be explained on the worksheet; and• Caretaker may apply for PHC benefits on child’s behalf.
Verification/Documentation of Family Composition – To verify familyrelationships, one of the following items may be provided, if questionable:
• Birth certificate;• Baptismal certificate;• School records; or• Other documents or proof of family relationship determined valid by
the contractor to establish the dependency of the family member
upon the client or head of household.
Family members who receive other health care benefits are included in thefamily count. The contractor has discretion to document specialcircumstances in the calculation of family composition. Additionally, if aseparate family group is established within the household based on thedocumentation gathered, document the basis used for determining separatehouseholds on the DSHS Worksheet (Form EF05-13227).

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 26/92
SECTION THREEELIGIBILITY CRITERIA
5
September 2011
Screening &EligibilityDetermination(continued)
Residency
To be eligible for PHC, an individual must be physically present within thegeographic boundaries of Texas and:
• Has the intent to remain within the state, whether permanently or for
an indefinite period;• Does not claim residency in any other state or country; and/or• Is less than 18 years of age and his/her parent, managing
conservator, or guardian is a resident of Texas.
There is no requirement regarding the amount of time an individual must livein Texas to establish residency for the purpose of PHC eligibility.
Although the following individuals may reside in Texas, they are notconsidered Texas residents for the purpose of receiving PHC services andare considered ineligible:
• Inmates of correctional facilities;• Residents of state or federal schools; and• Patients in federal institutions or state psychiatric hospitals.
Verification/Documentation of Residency – Document proof of residencyprovided by the client on the DSHS Funding Source – Worksheetand explain why residency is questionable, if necessary. For verification ofresidency, one of the following items shall be provided:
• Valid Texas Drivers License;• Current voter registration;• Rent or utility receipts for one month prior to the month of application;• Motor vehicle registration;
• School records;• Medical cards or other similar benefit cards;• Property tax receipt;• Mail addressed to the applicant, his/her spouse, or children if they live
together; or• Other documents considered valid by the contractor.
If none of the listed items are available, residence may be verified through:• Observance of personal effects and living arrangement, or• Statement from landlords, neighbors, other reliable sources.
Temporary Absences from State – Individuals do not lose their residency
status because of temporary absences from the state. For example, amigrant or seasonal worker may travel during certain times of the year butmaintains a home in Texas and returns to that home after these temporaryabsences. If a family is otherwise eligible, but residence is inquestion/dispute, the household is entitled to services until factualinformation regarding residency change proves otherwise.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 27/92
SECTION THREEELIGIBILITY CRITERIA
6
September 2011
Screening &EligibilityDetermination(continued)
Income
To be eligible for PHC, clients must have a gross family income at or below150% FPL. The table below details sources of income that contribute to thecalculation of gross family income as well as income that is exempt from
being counted.
Types of Income Countable Exempt
Adoption Payments X
Cash Gifts and Contributions* X
Child Support Payments* X
Child's Earned Income X
Crime Victim's Compensation * X
Disability Insurance Benefits/SSDI* X
Dividends, Interest, and Royalties* X
Educational Assistance X
Energy Assistance X
Foster Care Payment X
In-kind Income X
Job Training X
Loans (Non-educational)* X
Lump-Sum Payments* X X
Military Pay* X
Mineral Rights* X
Pensions and Annuities* X
Reimbursements* X
RSDI /SSDI/Social Security Payments* X
Self-Employment Income* XSSI Payments X
TANF X
Unemployment Compensation* X
Veteran's Administration* X X
Wages and Salaries, Commissions* X
Worker's Compensation* X
*Explanation of countable income provided below
Cash Gifts and Contributions – Count unless they are made by a private, non-profit organization on the basis of need; and total $300 or less per household ina federal fiscal quarter. The federal fiscal quarters are January – March, April – June, July – September, and October –December. If these contributions exceed$300 in a quarter, count the excess amount as income in the month received.
Exempt any cash contribution for common household expenses, such as food,rent, utilities, and items for home maintenance, if it is received from a non-certified household member who:

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 28/92
SECTION THREEELIGIBILITY CRITERIA
7
September 2011
Screening &EligibilityDetermination(continued)
• Lives in the home with the certified household member,• Shares household expenses with the certified household member, and• No landlord/tenant relationship exists.
Child Support Payments – Count income after deducting $75 from the total
monthly child support payments the household receives.
Disability Insurance Payments/SSDI – Countable. Social Security DisabilityInsurance is a payroll tax-funded, federal insurance program of the SocialSecurity Administration. Medical condition prohibits work for one year or resultsin death.
Dividends, Interest and Royalties – Countable. Exception: Exempt dividendsfrom insurance policies as income.
Count royalties, minus any amount deducted for production expenses andseverance taxes.
In-Kind Income – Exempt. An in-kind contribution is any gain or benefit to aperson that is not in the form of money/check payable directly to the household,such as clothing, public housing, or food.
Loans (Non-educational) – Count as income unless there is an understandingthat the money will be repaid and the person can reasonably explain how he/shewill repay it.
Lump-Sum Payments – Count as income in the month received if the personreceives it or expects to receive it more often than once a year.
Exempt lump sums received once a year or less, unless specifically listed as
income.
Military Pay- Count military pay and allowances for housing, food, base pay,and flight pay, minus pay withheld to fund education under the G.I. Bill.
Mineral Rights – Countable. A payment received from the excavation ofminerals such as oil, natural gas, coal, gold, copper, iron, limestone, gypsum, sand, gravel, etc.
Pensions and Annuities – Countable. A pension is any benefit derivedfrom former employment, such as retirement benefits or disability pensions.
Reimbursements – Countable, minus the actual expenses. Exempt areimbursement for future expenses only if the household plans to use it asintended.
RSDI/SSDI/Social Security Payments – Count the Retirement, Survivors,and Disability Insurance (RSDI) benefit amount including the deduction forthe Medicare premium, minus any amount that is being recouped for a priorRSDI overpayment.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 29/92
SECTION THREEELIGIBILITY CRITERIA
8
September 2011
Screening &EligibilityDetermination(continued)
Self-Employment Income – Count total gross earned, minus the allowablecosts of producing the self-employment income.
SSI Payments – Exempt Supplemental Security Income (SSI) benefits.
Terminated Employment – Count terminated income in the month received.Use actual income and do not use conversion factors if terminated income isless than a full month’s income. Income is terminated if it will not be receivedin the next usual payment cycle.
Unemployment Compensation Payments – Count the gross benefit lessany amount being recouped for a UIB overpayment.
VA Payments – Count the gross Veterans Administration (VA) payment,minus any amount being recouped for a VA overpayment. Exempt VAspecial needs payments, such as annual clothing allowances or monthlypayments for an attendant for disabled veterans.
Wages, Salaries, Tips and Commissions – Count the actual (not taxable)gross amount.
Worker’s Compensation – Count the gross payment, minus any amountbeing recouped for a prior worker’s compensation overpayment or paid forattorney’s fees. NOTE: The Texas Workforce Commission (TWC) or a courtsets the amount of the attorney’s fee to be paid.
Verification/Documentation of Income – Verification and documentation ofincome must be provided to complete the DSHS Funding Source -Worksheet. Declarations of “unknown” will not be accepted as
representations of required facts and documentation. Incomplete orinadequately documented eligibility determination will result in limitations inthe provision of funded services. To verify income, one of the following mustbe provided: a minimum of three (3) consecutive, current pay periods or onemonth’s pay only if paid same gross amount on a monthly basis, unlessspecial circumstances are noted on the DSHS Funding Source - Worksheet:
• Copy(ies) of the most recent paycheck stub/monthly earningstatement(s);
• Employer’s written verification of gross monthly income or theEmployment Verification Form (Form 128);
• Award letters;• Domestic relation printout of child support payments;• Letter of support• Unemployment benefits statement or letter from the Texas Workforce
Commission;• Award letters, court orders, or public decrees to verify support
payments ; or• Notes for cash contributions.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 30/92
SECTION THREEELIGIBILITY CRITERIA
9
September 2011
Screening &EligibilityDetermination(continued)
If all attempts to verify income are unsuccessful because the employer/payerfails or refuses to provide information or threatens continued employment,and no other proof can be found, staff may determine an amount to use onthe form based on the best available information and document thedetermined income on the DSHS Funding Source – Worksheet.
Income Determination Procedure
• Count income already received and any income the householdexpects to receive. When an individual has not yet received incomefor new employment, use the best estimate of the amount to bereceived. If telephone verification regarding new or terminatedemployment is made, it must be documented by the contractor on theDSHS Funding Source – Worksheet (Form EF05-13227).
• Count terminated income in the month received. Use actual incomeand do not use conversion factors if terminated income is less than a
full month’s income.
• Use at least three consecutive, current pay periods to calculateprojected monthly income. If client is paid one time per month andreceives the same gross pay each month, then one pay period willsuffice.
• If actual or projected income is not received monthly, convert it to amonthly amount using one of the following methods:
o Weekly income x 4.33;o Every two weeks x 2.17; oro Twice a month x 2.0.
• Dependent childcare expenses shall be deducted from total income indetermining eligibility. Allowable deductions are actual expenses upto $200 per child per month for children under age 2 and $175 perchild per month for children age 2 to 12 or age 2 to 18 if child isdisabled.
• Legally obligated child support payments made by a member of thehousehold group shall also be deducted. Payments made weekly,every two weeks or twice a month must be converted to a monthlyamount by using one of the above listed conversion factors.
Self-Employment Income – If an applicant earns self-employment income,it must be added to any income received from other sources.
• Annualize self-employment income that is intended for an individualor family’s annual support, regardless of how frequently the income isreceived.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 31/92
SECTION THREEELIGIBILITY CRITERIA
10
September 2011
Screening &EligibilityDetermination(continued)
Determine the costs of producing self-employment income by accepting thedeductions listed on the 1040 U.S. Individual Income Tax Return statement or by allowing the following deductions:
o Capital asset improvements;o Capital asset purchases, such as real property, equipment,
machinery and other durable goods, i.e., items expected tolast at least 12 months;
o Fuel;o Identifiable costs of seed and fertilizer;o Insurance premiums;o Interest from business loans on income-producing property;o Labor;o Linen service;o Payments of the principal of loans for income-producing
property;o Property taxes;o Raw materials;o Rent;o Repairs that maintain income-producing property;o Sales tax;o Stock;o Supplies;o Transportation costs. The person may choose to use 50.0
cents per mile instead of keeping track of individualtransportation expenses. Do not allow travel to and from theplace of business, and
o Utilities.
NOTE: If the applicant conducts a self-employment business in his
home, consider the cost of the home (rent, mortgage, utilities) asshelter costs, not business expenses, unless these costs can beidentified as necessary for the business separately.
• If the self-employment income is only intended to support theindividual or family for part of the year, average the income over thenumber of months it is intended to cover.
• If the individual has had self-employment income for the past year,use the income figures from the previous year’s business records ortax forms.
• If current income is substantially different from income the previousyear, use more current information, such as updated businessledgers or daybooks. Remember to deduct predictable businessexpenses.
• If the individual or family has not had self-employment income for thepast year, average the income over the period of time the businesshas been in operation and project the income for one year.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 32/92
SECTION THREEELIGIBILITY CRITERIA
11
September 2011
Screening &EligibilityDetermination(continued)
• If the business is newly established and there is insufficientinformation to make a reasonable projection, calculate the incomebased on the best available estimate and follow-up at a later date.
•
A signed statement from individuals who are self-employed and haveno documentation of their income will be accepted for a period of sixmonths. PHC coverage cannot be extended on subsequentapplications without formal verification and documentation of self-employment income.
Seasonal Employment – Include the total income for the months worked inthe overall calculation of income. The total gross income for the year can beverified by a letter from the individual’s employer, if possible.
Statements of Support – Unless the person providing the support to theindividual is present during the interview and has acceptable documentationof identity, a statement of support will be required. The Statement of Supportis used to document income when no supporting documentation is availableor when income is irregular. If questionable, the contractor may documentproof of identification such as a Texas Drivers License, Social Security card,or a birth certificate of the supporter.
Eligibility Determination
The contractor must consider the information provided by the client anddocument the basis for the eligibility decision on the DSHS Funding Source – Worksheet (Form EF05-13227). The client must sign the Statement ofApplicant’s Rights and Responsibilities (Form 101) to complete the eligibilitydetermination.
This form does not have to be signed again unless there is a break inservices for two years or longer. It is required that after determiningeligibility, the provider stating that either the family or individual is:
• Eligibleo The individual/family is eligible for assistance;o The date eligibility begins and expires; ando The services the individual/family is entitled to receive.
• Ineligibleo The individual/family is denied eligibility;o The reason the application was denied;o The effective date of denial;o The individual’s right to appeal; ando The appropriate referrals to alternative agencies/programs for
services.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 33/92
SECTION THREEELIGIBILITY CRITERIA
12
September 2011
Screening &EligibilityDetermination(continued)
Appeal of Eligibility Determination – Individuals and families can appeal toDSHS regarding the eligibility determination for PHC if they feel thatinformation was incorrectly considered. Applicants may submit additionalinformation to establish eligibility, or repeat the application process.
Date Eligibility Begins – An individual/family is entitled to servicesbeginning with the date the completed application was submitted.
Presumptive Eligibility – Households, who have not had a final eligibilitydetermination and a member in the household presents with an immediatemedical need, may receive PHC funded services on a presumptive eligibilitybasis during the time that eligibility for services is pending. Presumptiveeligibility is effective for 90 days from the date the member of the household is first seen by the medical provider. The household shall be enrolled on apresumptive eligibility basis only once in a 12-month period. If a medicalcondition makes eligibility determination impossible and the applicant’sspouse (if applicable) is not present to sign and date the DSHS Funding
Source – Application For Health Care Assistance (Form EF05-13229),provide immediate treatment and send a copy of the application with theclient for spouse’s signature. The Presumptive Eligibility Form (102) is not tobe used in lieu of the DSHS Funding Source – Application For Health CareAssistance (Form EF05-13229). An appointment to complete the processshould be made at the first possible opportunity. If the household hasapplied for another program, the contractor is responsible for updating theeligibility status on a timely basis.
Documented proof of eligibility within the other funding sources is required. Ifemergency services are needed immediately and are not provided byanother program, services shall be provided during this 90-day period. If a
household member becomes Medicaid eligible, the services must be billed toMedicaid under the 90-days prior provision.
PHC emphasizes the importance of prevention and early intervention. Thegoal of PHC is for clients to be part of the health care system and not rely onepisodic, acute care. An applicant’s medical needs shall be met quickly andappropriately using whatever resources are available.
Two exceptions to using other benefits in place of PHC include:
• If the benefits were created by the establishment of a city or countyhospital, a joint city-county hospital, a county hospital authority, ahospital district, or by the facilities of a publicly supported medicalschool. Benefits created by any of these entities would not disqualifyindividuals from using PHC services.
• Contractors are not expected to refer clients to the County IndigentHealth Care Program (CIHCP) if the county of residence is coveredby a hospital district to provide CIHCP services, or the client does notmeet the county’s eligibility criteria for the program.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 34/92
SECTION THREEELIGIBILITY CRITERIA
13
September 2011
Screening &EligibilityDetermination(continued)
Individuals potentially eligible for Medicaid or CHIP should be referred to theYour Texas Benefits website (www.yourtexasbenefits.com) or 2-1-1 forcomprehensive Medicaid or CHIP eligibility determination.
Clients who are determined eligible or potentially eligible for CHIP may alsobe eligible for PHC-funded services during the waiting period until CHIPcoverage begins. Contractors are allowed to continue providing PHC-fundedservices after the initial 90-day period only if the client has applied for CHIP,is waiting on approval, and until the date CHIP enrollment is effective. Acopy of the CHIP eligibility card showing when CHIP coverage will beginmust be kept in the clients’ medical records.
Individuals who are determined potentially eligible for another benefit by theDSHS Funding Source – Application for Health Care Assistance (Form EF05-13229), but fail to fully complete the required application process for thebenefit, will not be eligible to receive PHC-funded services beyond thoseservices delivered during the 90-day presumptive eligibility period. If within
90 days a client fails to complete the eligibility determination process foranother benefit, the contractor may bill PHC for the services delivered duringthe 90-day period only. Contractors should make clients aware that failing orrefusing to complete the appropriate eligibility determination processes mayresult in their determination as self-pay clients.
Supplemental Benefits – In some cases, individuals receiving benefits fromother sources such as Medicaid, Medicare, CHIP, Title V, Title X, and TitleXX may be eligible for partial PHC coverage. This coverage is limited toservices provided by PHC but not covered by other sources. Wheneverfederal, state, private, or other benefits are available for payment of servicesfor clients, no PHC funds shall be used to pay for such care. An example of
a client receiving supplemental benefits would be a contractor providinghealth education services to a Medicaid eligible individual since Medicaiddoes not provide health education services. The contractor mustcommunicate to the client that supplemental services are limited scope.
Annual Re-certification – The contractor will determine the system used totrack clients’ status and renewal eligibility. Eligibility determination using theDSHS Funding Source – Application for Health Care Assistance (FormEF05-13229) form is required for all clients. Eligibility services must be re-determined for each individual/family every 12 months.
At least 30 days prior to the anniversary date of their original eligibility date,
client should be notified that they must renew eligibility by the anniversarydate or lose their benefits until they are re-certified by the program. Ifrenewal has not been completed by the anniversary date, theindividual/family record should be removed from active status and placed inthe inactive files. The individual family should be notified of the statuschange. A client can be a new client only once. Regardless of the timelapse between the initial application and the renewal application, formerclients will not be classified as new.
8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 35/92
SECTION THREEELIGIBILITY CRITERIA
14
September 2011
Screening &EligibilityDetermination(continued)
Contractors should mail out notices, either postcards or letters, requestingthat the individual or family representative come to the office for re-certification. A contractor may include a new application in the letter and askthe individual to return with documentation.
If an actual interview is chosen, appointment times may be given to prevent
long waiting periods.
For each record being renewed, whether in person or by mail, the eligibilityprovider staff shall complete a new DSHS Funding Source – Application forHealth Care Assistance (Form EF05-13229) using updated informationprovided by the client. Sending a Notice of Eligibility is required to inform theindividual/family of continued eligibility. The contractor shall assist clientswho request help in completing forms or providing documentation.
Co-pay/Fees PHC contractors may assess a fee for services (co-pay) from PHC clientswhose family income is at or below 150% FPL. Client co-pays may be the
lesser of $40 or 25% of the Medicaid reimbursement rate. The contractormust waive the fee if a client self-declares an inability to pay. No PHC clientshall be denied services based on an inability to pay. Client co-pays must bereported as program income on the monthly State Purchase Voucher (FormB-13) and the quarterly Financial Status Report (FSR or Form 269a).Example: CPT Code – 99213 = $33.95
CPT Code – 80053 = $14.53 CPT Code – 80061 = $18.42
$66.90 x 25% = $16.72 (client co-pay/fee)
Other Fees Clients shall not be charged administrative fees for items such as processingand/or transfer of medical records, copies of immunization records, etc.
Contractors are allowed to bill clients for services outside the scope of PHCallowable services, if the service is provided at the client’s request, and theclient is made aware of his/her responsibility for paying for the charges.
Continuationof Services
Contractors who have expended their awarded PHC funds are required tocontinue to serve their existing PHC eligible clients.
If other funding sources are used to provide PHC services, the funds must bereported as non-DSHS funds on the monthly State Purchase Voucher (FormB-13) and the quarterly Financial Status Report (FSR or Form 269a).

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 36/92
SECTION FOUR
CLINICAL INFORMATION

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 37/92
SECTION FOURCLINICAL INFORMATION
1
September 2011
ClinicalInformedConsent
General Informed Consent
Contractors must obtain the patient’s written, informed, voluntary generalconsent to receive services prior to receiving any clinical services. Ageneral informed consent explains the types of services provided and howclient/patient information may be shared with other entities forreimbursement or reporting purposes. If there is a period of time of threeyears or more during which a patient does not receive services a newgeneral consent must be signed prior to reinitiating delivery of services.
Consent information must be effectively communicated to every patient in amanner that is understandable by that patient and allows her/him toparticipate and make sound decisions regarding her/his own medical carein compliance with Limited English Proficiency regulations and addressingany disabilities that impair communication. Only the patient may consent.For situations when the patient is legally unable to consent (e.g., a minor oran individual with development disability), a parent, legal guardian orcaregiver must consent. Consent must never be obtained in a manner thatcould be perceived as coercive.
In addition, as described below, the contractor must obtain the informedconsent of the patient for procedures as required by the Texas MedicalDisclosure Panel. DSHS contractors should consult a qualified attorney todetermine the appropriateness of the consent forms utilized by their healthcare agency.
Method Specific Consent
The method specific consent and/or the patient health record mustdocument that the patient has received and understands informationconcerning the method effectiveness, appropriate use, benefits, potentialside effects and complications, alternatives and discontinuation issues.
Procedure Specific Consents
Sterilization Procedures – There are two consent forms required forsterilization procedures: the Sterilization Consent Form and the TexasMedical Disclosure Panel Consent.
The Sterilization Consent Form – This sterilization consent form is
provided in the Texas Medicaid Provider Procedures Manual and is theonly acceptable consent form for sterilizations funded by regular Medicaid(Title XIX), the Women’s Health Program, Title V, Title X, or Title XX. Anelectronic copy may be found on the Texas Medicaid HealthcarePartnership website: http://www.tmhp.com/default.aspx. The federallymandated consent form is necessary for both abdominal and transcervicalsterilization procedures in women and vasectomy in men.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 38/92
SECTION FOURCLINICAL INFORMATION
2
September 2011
ClinicalInformedConsent(continued)
In brief, the individual to be sterilized must:• Be at least 21 years old at the time the consent is obtained;• Be mentally competent;•
Voluntarily give his or her informed consent;• Sign the consent form at least 30 days but not more than 180* days
prior to the sterilization procedure; and• May choose a witness to be present when the consent is obtained.
*An individual may consent to be sterilized at the time of premature deliveryor emergency abdominal surgery, if at least 72 hours have passed after heor she gave informed consent to sterilization. In the case of prematuredelivery, the informed consent must have been given at least 30 daysbefore the expected date of delivery.
The consent form must be signed and dated by:•
The individual to be sterilized;• The interpreter, if one is provided;• The person who obtains the consent;• The physician who will perform the sterilization procedure
Informed consent may not be obtained while the individual to be sterilizedis:
• In labor or childbirth;• Seeking to obtain or obtaining an abortion; or• Under the influence of alcohol or other substances that affect the
individual’s state of awareness.
Texas Medical Disclosure Panel Consent
The Texas Medical Disclosure Panel (TMDP) was established by theTexas Legislature to determine which risks and hazards related to medicalcare and surgical procedures must be disclosed by health care providers orphysicians to their patients or persons authorized to consent for theirpatients, and to establish the general form and substance of suchdisclosure. TMDP has developed a List A (informed consent requiring fulland specific disclosure) and a List B (informed consent not requiringspecific disclosures) for certain procedures. More information about theTMDP can be found at: http://www.dshs.state.tx.us/hfp/tmdp.shtm
List A procedures can be found at the following Texas Administrative Codelink:http://info.sos.state.tx.us/pls/pub/readtac$ext.ViewTAC?tac_view=4&ti=25&pt=7&ch=601&rl=Y.
With regard to Tubal Sterilization and Vasectomy, List A procedures, theTMDP required Disclosure and Consent Form for contractors who

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 39/92
SECTION FOURCLINICAL INFORMATION
3
September 2011
ClinicalInformedConsent(continued)
directly perform the procedure can be found at:http://info.sos.state.tx.us/fids/200504268-1.html This consent is in additionto the Sterilization Consent Form noted on the previous page.
The required disclosures for Tubal Sterilization are:(A) Injury to the bowel and/or bladder;(B) Sterility;(C) Failure to obtain fertility (if applicable);(D) Failure to obtain sterility (if applicable); and(E) Loss of ovarian functions or hormone production from
ovary(ies).
The required disclosures for Vasectomy are:(A) Loss of testicle; and(B) Failure to produce permanent sterility.
For all other procedures not listed on List A, the physician must disclose,through a procedure specific consent, all risks that a reasonable patientwould want to know about. This includes all risks that are inherent to theprocedure (one which exists in and is inseparable form the procedure itself)and that are material (could influence a reasonable person in making adecision whether or not to consent to the procedure).
Parental Consent for Services Provided to Minors
The general rule is that parents must consent for minors (Family Code§151.001). A minor is defined as a person less than 18 years of age whohas never been married. However there are certain circumstances underwhich a minor may consent for her/his own treatment. Requirements forparental consent for provision of family planning services to minors varyaccording to the funding source subsidizing the services. The departmentand providers may provide family planning services, including prescriptiondrugs, without the consent of the minor’s parent, managing conservator, orguardian only as authorized by Chapter 32 of the Texas Family Code or byfederal law or regulations.
Title X projects may not require consent of parents or guardians for theprovision of services to minors. Nor can the project notify parents orguardians before or after a minor has requested and received Title X familyplanning services (see Table at end of Chapter). When parental consent isrequired, the parent must sign both the general consent for treatment and
the method specific consent for prescription birth consent.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 40/92
SECTION FOURCLINICAL INFORMATION
4
September 2011
ClinicalInformedConsent(continued)
There are instances in which a minor may consent to his/her own medical,dental, psychological and surgical treatment by a licensed physician ordentist if the minor:
•
Is on active duty with the armed services;• Is at least 16 years old, living apart from a parent or guardian and
managing his or her own financial affairs. You do not have toprovide the child is emancipated if the minor so declares in writing;
• Is consenting to diagnosis and treatment of an infectious,contagious, or communicable disease required to be reported to thelocal health officer or the Department of State Health Services;
• Consents to examination and treatment for drug or chemicaladdiction , dependency or any other condition directly related todrug or chemical use;
• Is unmarried and pregnant and seeking treatment related to thepregnancy, unless it’s an abortion;
•
Has custody of his/her biological child and also consents to thechild’s medical, dental psychological or surgical treatment of thechild;
• Is seeking a diagnosis or treatment for a sexually transmitteddisease, including HIV;
• Is seeking counseling for chemical dependency or addiction, suicideprevention or sexual, physical or emotional abuse.
The Texas Family Code, Chapter 32, may be found at the followingwebsite: http://www.statutes.legis.state.tx.us/?link=FA.
Consent for HIV Tests
Texas Health and Safety Code §81.105 and §81.106 is as follows:
§81.105. Informed Consenta) Except as otherwise provided by law, a person may not perform a
test designed to identify HIV or its antigen or antibody without firstobtaining the informed consent of the person to be test.
b) Consent need not be written if there is documentation in themedical record that the test has been explained and the consenthas been obtained.
§81.106 General Consenta) A person who has signed a general consent form for theperformance of medical tests or procedures is not required to alsosign or be presented with a specific consent form relating to medicaltest or procedures to determine HIV infection, antibodies to HIV, orinfection with any other probable causative agent of AIDS that willbe performed on the person during the time in which the generalconsent form is in effect.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 41/92
SECTION FOURCLINICAL INFORMATION
5
September 2011
ClinicalInformedConsent(continued)
ClinicalGuidelines
b) Except as otherwise provided by the chapter, the result of a test orprocedure to determine HIV infection, antibodies to HIV, or infectionwith any probable causative agent of AIDS performed under theauthorization of a general consent form in accordance with thissection may be used only for diagnostic or other purposes directlyrelated to medical treatment.
Texas Health and Safety Code may be found at the following website:http://www.statutes.legis.state.tx.us/?link=HS.
The PHC Clinical Guidelines gives providers guidance in providing directpatient care services. The guidelines are in a table format at the end of thischapter.
Specific requirements for PHC are:• Comprehensive medical and social history and updated as clinically
indicated;• Baseline and periodic physical exam (PE) initially and updated as
clinically indicated;• Health Risk Assessment (HRA) initially and updated as clinically
indicated; and• Patient education for health risks identified in the HRA.
Services operating under specific DSHS guidelines/standards should beprovided according to that particular program’s requirements in addition toPHC requirements. Specific guidelines cover, but are not limited to,services such as family planning, child health, immunizations, maternity,diabetes management, and case management.
Protocols, Standing Delegation Orders and Procedures
Contractors that provide clinical services must develop and maintain writtenclinical protocols and standing delegation orders (SDOs) in compliancewith statutes and rules governing medical and nursing practice andconsistent with national evidence-based clinical guidelines. The writtenclinical protocols and/or SDOs must be signed by the Medical Director orsupervising physician on an annual basis or more often if changes arerequired. When DSHS revises a policy, contractors need to incorporate therevised policy into their written procedures.
ProtocolsContractors that employ Advanced Practice Nurses or Physician Assistantsmust have written protocols to delegate authorization to initiate medicalaspects of client care. The protocols must be agreed upon and signed bythe supervising physician and the physician assistant and/or advancedpractice nurse, reviewed and signed at least annually, and maintained onsite. The protocols need not describe the exact steps that an advancedpractice nurse or a physician assistant must take with respect to eachspecific condition, disease, or symptom.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 42/92
SECTION FOURCLINICAL INFORMATION
6
September 2011
ClinicalGuidelines(continued)
Standing Delegation Orders Contractors that employ unlicensed and licensed personnel, other thanadvanced practice nurses or physician assistants, whose duties includeactions or procedures for a patient population with specific diseases,disorders, health problems or sets of symptoms, must have written SDOsin place. SDOs are instructions, orders, rules, regulations or proceduresthat specify under what set of conditions and circumstances actions shouldbe instituted. The SDOs delineate under what set of conditions andcircumstances an RN, LVN, or non-delineate under what set of conditionsand circumstance an RN, LVN, or non-licensed health care provider(NLHP) actions or tasks may be initiated in the clinical setting, and provideauthority for use with patients when a physician or advance practiceprovider is not on the premises, and or prior to being examined orevaluated by a physician or advance practice provider. Example: SDO forassessment of Blood Pressure/Blood Sugar which includes an RN, LVN orNLHP that will perform the task, the steps to complete the task, thenormal/abnormal range, and the process of reporting abnormal values.Other applicable SDOs when a physician is not present on-site mayinclude, but are not limited to:
• Obtaining a personal and medical history;• Performing an appropriate physical exam and the recording of
physical findings;• Initiating/performing laboratory procedures;• Administering or providing drugs ordered by voice
communication with the authorizing physician;• Providing pre-signed prescriptions for:
o Oral contraceptives;o
Diaphragms;o Contraceptive creams and jellies;o Topical anti-infective for vaginal use;o Oral anti-parasitic drugs; oro Antibiotic drugs for treatment of venereal disease
• Handling medical emergencies – to include on-site managementas well as possible transfer of client;
• Giving immunizations; or• Performing pregnancy testing.
SDOs are distinct from specific orders written for a particular patient. TheSDOs must be dated and signed by the physician who is responsible for
the delivery of medical care covered by the orders. The SDOs must bereviewed and signed at least annually.
Patient EducationIn addition to the above, contractors must have written plans for patienteducation that include goals and content outlines to ensure consistencyand accuracy of information provided. Plans for patient education must bereviewed and signed by the Medical Director.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 43/92
SECTION FOURCLINICAL INFORMATION
7
September 2011
ClinicalGuidelines(continued)
ResourcesRequirements addressing scope of practice and delegation of medical andnursing acts can be accessed at the following websites:
http://www.tmb.state.tx.us/ (Texas Medical Board); andhttp://www.ben.state.tx.us/ (Board of Nurse Examiners for the State ofTexas.
Rules that are most pertinent to this topic are:Texas Administrative Code, Title 22, Part 9, Chapter 193;Texas Administrative Code, Title 22, Part 11, Chapters 221 and 224; andTexas Administrative Code, Title 22, Part 9, Chapter 185 (PhysicianAssistant Scope of Practice).
Emergency Responsiveness
Contractors must be adequately prepared to handle clinical emergencysituations, as follows:
• There must be a written plan for the management of on-site medicalemergencies, emergencies requiring ambulance services andhospital admission, and emergencies requiring evacuation of thepremises.
• Each site where sterilization procedures are performed must havean arrangement with a licensed facility for emergency treatment ofany surgical complication. If sterilization procedures are performedin a freestanding surgical care center or on an inpatient basis in ahospital, Medicare standards applicable to the facility and staff mustbe met.
• Each site must have staff trained in basic cardiopulmonaryresuscitation (CPR) and emergency medical action. Staff trained inCPR must be present during all hours of clinic operation.
• There must be written protocols to address vaso-vagal reactions,anaphylaxis, syncope, cardiac arrest, shock, hemorrhage, andrespiratory difficulties.
• Each site must maintain emergency resuscitative drugs, supplies,and equipment appropriate to the services provided at that site andappropriately trained staff when patients are present.
• Documentation must be maintained in personnel files that staff hasbeen trained regarding these written plans or protocols.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 44/92
SECTION FOURCLINICAL INFORMATION
8
September 2011
ClinicalGuidelines(continued)
Patient Health Record (Medical Record)
Contractors must ensure that a patient health record (medical record) isestablished for every client who obtains services. These records must bemaintained according to accepted medical standards and State laws,including those governing record retention.
All client records must be:• Complete, legible, and accurate documenting all clinical
encounters, including those by telephone;• Written in ink without erasures or deletions; or documented by
Electronic Medical Record (EMR);• Signed by the provider making the entry, including name of
provider, provider title and date for each entry;o Electronic signatures are allowable to document provider
review of care. However, stamped signatures are notallowable.
• Readily accessible to assure continuity of care and availability toclient;
• Systematically organized to allow easy documentation and promptretrieval of information;
• Maintained to safeguard against loss or unauthorized access and toassure confidentiality (complying with HIPAA regulations); and
• Secured by lock when not in use.
The patient health record must include:• Client identification and personal data;• Completed Screening and Eligibility Determination Form for Medical
Services Assistance;• Completed Statement of Applicant’s Rights and Responsibilities
signed by the client or responsible party;• Copies of acceptable documentation establishing income,
residency, and family composition;• Copy of Medicaid and/or CHIP denial letter, if applicable;• Preferred language/method of communication;• Patient contact in formation with the best way to reach patient in
such a manner that facilitates continuity of care, assuresconfidentiality, and adheres to HIPAA* regulations;
• Medical history, (in Medical History and Risk Assessment);• Physical examination (in Physical Assessment);•
Laboratory and other diagnostic tests orders, results and follow-up;• Assessment or clinical impression;• Plan of care, including education/counseling, treatment, special
instructions scheduled antenatal visits and referrals;• Documentation on follow-up of missed appointments;• Informed consent documentation;• Refusal of services documentation;• Medication and other allergic reactions recorded prominently in
specific location; and

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 45/92
SECTION FOURCLINICAL INFORMATION
9
September 2011
ClinicalGuidelines(continued)
• Problem list.
Preventive Services
PHC providers may, but are not required to, use the current edition of theGuide to Clinical Preventive Services, developed by the U.S. PreventiveServices Task Force, as guidelines for providing clinical preventiveservices such as health screening and client education. The guide can beaccessed at: http://www.ahrg.gov/clinic/prevenix.htm.
Vaccines
PHC contractors are encouraged to become a Texas Vaccines for Children(TVFC) provider. The TVFC program supplies free vaccines to providers tovaccinate eligible patients from birth through age 18 years. All vaccinesroutinely recommended by the Advisory Committee on ImmunizationPractices (ACIP) and approved by the Centers for Disease Control andPrevention (CDC) are offered by the TVFC program.
Additional information on provider enrollment can be found at:http://www.dshs.state.tx.us/immunize/tvfc/default.shtm or by calling 1-800-252-9152.
To be eligible to enroll in the TVFC, providers must be one of the following:• Physician (Medical Doctor (MD) or Doctor of Osteopathy (DO));• Nurse Practitioner (NP);• Certified Nurse Midwife (CNM); or•
Physician Assistant (PA).
All other health care providers must enroll under the standing delegationorders of a physician including:
• Pharmacists (RPH);• Nurses (Registered Nurses (RN) or Licensed Vocational Nurses
(LVN);• Medical Assistants (MA);• Nurse Assistants (NA); or• Emergency Medical Technicians (EMT).
Medicaid and CHIP providers must enroll in the TVFC or use their privately
purchased vaccines. They may not refer children to Local HealthDepartments (LHD) or other entities for routinely recommendedvaccinations. A TVFC Provider Enrollment Form is included in theMedicaid provider enrollment packet.
NOTE: Medicaid and CHIP programs do not reimburse providers forthe cost of routinely recommended childhood vaccines but doreimburse an administration fee.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 46/92
SECTION FOURCLINICAL INFORMATION
10
September 2011
ClinicalGuidelines(continued)
Pharmaceuticals
Pharmaceuticals for the treatment of patients with gonorrhea, chlamydia,and syphilis may be obtained from the DSHS STD/HIV throughparticipating Local Health Departments and DSHS regional offices.Contractors may use PHC funds for pharmaceuticals provided to patientsreceiving PHC services with the approval of PHC through the Request forProposal (RFP) and contract processes. Contractors are encouraged toaccess Prescription Drug Patient Assistance Programs in order to obtainprescription medications at no cost or low cost to clients. Many programsare listed in the Pharmaceutical Research and Manufacturers of America(PhRMA) directory published online at: http://www.phrma.org andhttp://www.rxxassist.org.
Medicare Prescription Drug Plan
On January 1, 2006, the Medicare Prescription Drug Plan, Medicare PartD, was introduced to provide elderly and disabled Medicare beneficiariesaccess to prescription drug coverage. Texas beneficiaries pay monthlypremiums, deductibles, and co-payments as part of program participationand can choose from a number of plans with distinct formularies. Medicareprovides various premium and cost-sharing subsidies (“extra help”) toassist beneficiaries below 150% FPL with limited assets. The applicationprocess for extra help, coordinated by the Social Security Administration, isa separate process from enrolling in the drug plan. If beneficiaries do notenroll when they are first eligible, they may have to pay a higher premiumamount if they join at a late date. If they have prescription drug coveragefrom other insurance that is the same or better than the Medicare plans,they can keep their current coverage and will not have to pay a higherpremium if they decide to join Part D later.
Enabling legislation mandates that PHC can only provide services that aclient is not eligible for through another resource; therefore, Medicare-eligible PHC clients must access their prescriptions through a MedicarePrescription Drug Plan. PHC contractors that provide supplementalprescription drug benefits may provide these benefits to client during theapplication process for Medicare Part D for a period up to 9-days, unlessextenuating circumstances occur and clients would be harmed if access tomedication ceased. Contractors must document such circumstances in thepatient health record.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 47/92
SECTION FOURCLINICAL INFORMATION
11
September 2011
ClinicalGuidelines(continued)
Screening for Part D – PHC rules mandate that all PHC contractors,regardless of whether or not they provide supplemental prescription drugbenefits, must screen clients for Medicare Part D eligibility. Applicants andclients are eligible for Medicare Part D if they are eligible for Medicare.These individuals must be referred to the local health and human servicesagency, local Area Agencies on Aging, Medicare and/or the Social SecurityAdministration to enroll in the Medicare Prescription Drug Plan andpossible extra help in paying for out-of-pocket expenses associated withthe plans. Resources are provided below.
Out-of-Pocket Expenses – The Medicare Prescription Drug Plan requiresbeneficiaries to pay out-of-pocket expenses such as premiums,deductibles, and co-payment. Beneficiaries that qualify for cost-sharingsubsidies will receive assistance from Medicare in paying for theseexpenses. In addition, a catastrophic benefit is available when a certainthreshold of out-of-pocket expenses is reached. In some cases,
beneficiaries may pay more for their prescription under Medicare Part DPHC rules allow contractors to reimburse clients for cost of cost sharingincurred through participation in the Medicare Prescription Drug Plan uponthe availability of funds. Contractors are responsible for establishingagreements with pharmacies participating in the Medicare plans and/orimplementing a system in which clients are reimbursed their co-payments.
Resources – General information from Medicare for beneficiaries andservice providers on Part D:
Call 2-1-1 for local assistance in applying for Part D and the extra help.
1-800-MEDICARE / http://www.medicare.gov
Information on Outreach and Partnerships from Medicare:http://www.cms.hhs.gov/partnerships/
Information on extra help from SSA:1-800-772-1213http://www.ssa.gov/prescriptionhelp/
Area Agencies on Aging:1-800-252-9240http://www.medicarerxoutreach.org
General information and fact sheets on Medicare Part D:www.kff.org/rxdrugs/medicare.cfm

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 48/92
SECTION FOURCLINICAL INFORMATION
12
September 2011
Reserved for future use.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 49/92
SECTION FOUCLINICAL INFORMATIO
September 20
CLINICAL GUIDELINESSTANDARD STATEMENT POLICIES & PROCEDURES EVALUATION CRITERIA
HEALTH ASSESSMENT
A. At sites providing medical care,a complete initial health history,signed and dated by the
provider, is obtained andupdated periodically, or at leastannually, for all patients.
Policy: At sites providing medical care, the providerensures a complete health history is obtained.
Procedures: The health history includes a medical andsocial history.
1. The medical history includes the following:a. Current historyb. Hospitalizationsc. Allergies, sensitivities or reactions to medicines orother substancesd. Family historye. Obstetric history and gynecologic history asindicatedf. Sexual behavior history, including family planningpracticesg. Mental health history, to include depression andsuicidal thoughts or gesturesh. Nutritional historyi. Developmental (pediatric)
j. Immunization historyk. Occupational hazards or environmental toxin
exposure
2. The social history includes the following:a. Home environment, to include living arrangementsb. Tobacco/alcohol/drugs use/abuse and exposurec. Family dynamics/problems; e.g., abuse
Evidence of health history in the record
DSHS may distribute or provide appropriated
funds only to patients who show good faith effortto comply with all child abuse reporting guidelineand requirements set forth in Chapter 261 of theTexas Family Code.
DSHS may distribute funds for medical, dental,psychological, or surgical treatment provided to aminor only if consent to treatment is obtainedpursuant to Chapter 32 of the Texas FamilyCode.
Documentation of social history

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 50/92
SECTION FOUCLINICAL INFORMATIO
September 20
CLINICAL GUIDELINESSTANDARD STATEMENT POLICIES & PROCEDURES EVALUATION CRITERIA
B. At sites providing medical care,a health risk assessment iscompleted for all patients.
Policy: Medical care providers assess health risk onall clients served.
Procedures: Patients must have a health riskassessment according to the following:1. Children ages birth through 20 years of age have
health risk assessments done according toperiodicity of visits, e.g., periodicity chart
2. People aged 21 years and older must have aninitial health risk assessment, which is updatedannually or with change in client status. HealthRisk Assessment includes but is not limited to:a. Diabetesb. Heart diseasec. High-risk sexual behaviord. Violencee. Injuryf. Malignancy
Health recordEvidence of health assessment
C. At sites providing medical care,all patients shall receivepreventive health education.
Policy: The providers of medical care shall providepreventive education based on health risk or patientneed.
Procedures: All patients must receive anticipatoryguidance at each visit that covers the followingappropriate areas:1. Violence
a. Family/domestic
Documentation of education provided based ohealth risk assessment or patient need.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 51/92
SECTION FOUCLINICAL INFORMATIO
September 20
CLINICAL GUIDELINESSTANDARD STATEMENT POLICIES & PROCEDURES EVALUATION CRITERIA
b. Gangc. Other types of violence
2. Injury preventiona. Fire armsb. Car safety restraints
c. Helmetsd. Prevention of other types of injuries3. Behavior
a. Substance abuse, e.g., tobacco, alcohol,chemicals and drugs
b. Safe sex practices4. Nutrition
a. Healthy dietsb. Weight managementc. Folic acidd. Calciume. Other vitamins and minerals
5. Health promotiona. Immunizationsb. Dental carec. Physical activity
d. Family planninge. Prenatal caref. Newborn care
6. Other education based on specific problems orhealth risk
7. Anticipatory guidance for teens in addition to abovealso includes:a. School performanceb. Depressionc. Suicide
For infants: Pediatric Nutrition Handbook, 5 th Edition from the American Academy ofPediatrics, 2003; Keep Kids Healthy at:http://www.keepkidshealthy.com/infant/infantntrition.html
For children:www.kidshealth.org/kid/stay_healthy/food/pyramid.html
For adults:www.lifeclinic.com/focus/nutrition/food-pyramid.asp andwww.nal.usda.gov/fnic/Fpyr/pmap.htm

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 52/92
SECTION FOUCLINICAL INFORMATIO
September 20
CLINICAL GUIDELINESSTANDARD STATEMENT POLICIES & PROCEDURES EVALUATION CRITERIA
D. All patients or their guardiansshall provide consent forservices/treatment.
Policy: Providers shall ensure that all patientsconsent for services.
Procedures:1. Notification and consent of the parent/legalguardian for all services provided to a minorpatient is required except for those patients forwhom the minor may consent independentlyaccording to those stated in Family Code §32.003.
2. All patients and/or guardians must provide signedconsent for immunizations.
Health recordA signed and dated consentTexas Family Code, Chapter 32
E. At sites providing medicalcare, a baseline physical exam(PE) is conducted on allpatients. Periodic physicalexams are conducted based
upon presenting symptoms,health risk factors, a review ofsystems, or according to theTHSteps Periodicity Schedulesfor children.
Policy: At sites providing medical services, a baselinePE is conducted in conjunctions with the initial history,laboratory tests, and interventions. In addition, onsubsequent visits a targeted PE, screening procedures,and interventions are conducted.
Procedures:1. As an integral part of the complete health assessment,the PE is based upon the patient’s presenting symptoms,review of systems (ROS), past history, and health riskfactors.
2. Laboratory and interventions (general non-high riskpopulation)
a. Blood pressure
Reference for interventions: Guide to Clinical Preventive Services . This reference alsocontains interventions for high-risk individuals.
THSteps Periodicity Schedule can be found at:http://www.dshs.state.tx.us/thsteps.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 53/92
SECTION FOUCLINICAL INFORMATIO
September 20
CLINICAL GUIDELINESSTANDARD STATEMENT POLICIES & PROCEDURES EVALUATION CRITERIA
Health Risk Conditions Addressed: Coronaryheart disease, congestive heart failure, cerebralvascular accident (stroke), ruptured aortic aneurysm,renal disease, and retinopathy.
Recommended Practice:1. At least once every two years for 140/852. Annually if diastolic blood pressure of 85-893. Higher blood pressure require more frequent
measurements4. Children and adolescents – annually for ages
3-20
b. Height, weight and BMI or appropriateassessment for overweight/obesity.
Health Risk Conditions Addressed: Overweightand obesity, which are associated with adult-onsetdiabetes, hypertension, et al.
Recommended Practice: Initial visit, then
periodically.
c. Total blood cholesterol
Recommended Practice: If no risk factors forcoronary heart disease, routinely test men starting at35 years old and women starting at age 45. If riskfactors for coronary heart disease are present,routinely screen men and women starting at age 20.
d. Cervical Cancer Screening for women
Centers for Disease Control and Preventionhttp://www.cdc.gov/bloodpressure/about.htm
http://wonder.cdc.gov/wonder/prevguid/p0000109 /p0000109.asp#head008001000000000
U.S. Preventive Services Task Forcehttp://www.ahrq.gov/clinic/uspstfix.htm

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 54/92
SECTION FOUCLINICAL INFORMATIO
September 20
CLINICAL GUIDELINESSTANDARD STATEMENT POLICIES & PROCEDURES EVALUATION CRITERIA
Health Risk Conditions Addressed: CervicalCancer
Recommended Practice: • Cervical cancer screening test (i.e., Pap test)
In 2009, ACOG updated their cervical cancerscreening guidelines to include:
• Cervical cancer screening should begin at age 21years.
• Cervical cytology screening is recommendedevery 2 years for women between the ages of 21years and 29 years.
• Women aged 30 years and older who have threeconsecutive negative cervical cytology screeningtest results and who have no history of CIN 2 or3, are not HIV infected, are notimmunocompromised, and were not exposed to
DES in utero, may extend the interval betweencervical cytology examinations to every 3 years.
• Both liquid-based and conventional methods ofcervical cytology are acceptable of screening.
Note: Regardless of the frequency of cervical cancerscreening, annual gynecologic examinations are stillrecommended, including pelvic exams, when indicated.
http://www.acog.org/departments/dept_notice.cfm?recno=20&bulletin=5021
http://www.acog.org/from_home/publications/pressreleases/nr11-20-09.cfm
Other organizational resources:
http://www.cancer.org/docroot/NWS/content/NW _1_1x_ACOG_Revises_Cervical_Cancer _Screening_Guidelines.asp
http://www.ahrg.gov/clinic/uspstf/uspscerv.htm
American Cancer Societyhttp://gantdaily.com/2010/08/03/whtf-new-cervical-cancer-screening-guidelines-the-pap-test/

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 55/92
SECTION FOUCLINICAL INFORMATIO
September 20
CLINICAL GUIDELINESSTANDARD STATEMENT POLICIES & PROCEDURES EVALUATION CRITERIA
e. Colorectal Screening
Health Risk Conditions Addressed: ColorectalCancer.
Recommended Practice:
1. Average risk – screen men and women 50 yearsof age and older.
2. High risk – screen prior to 50 years and/or moreoften if have any colorectal cancer risk factors.
3. Patient to visit with physician about which test isbest.
4. Screening options are fecal occult blood testing(FOBT), flexible sigmoidoscopy, combination ofFOBT and flexible sigmoid, colonoscopy, ordouble-contrast barium enema, or CTcolonography.
f. Mammography
Health Risk Conditions Addressed: Breast cancer
Recommended Practice: Every 1-2 years, withmammography and annual CBE, for women aged50-69.
g. Immunizations
Health Risk Conditions Addressed: Tetanus (lock jaw), Rubella (measles), Influenza (includinginfluenza pneumonia), and Pnuemococcalpneumonia.
American Cancer Societyhttp://www.nccrt.org/Standards/STDDetail.aspx?rticle_id=374
Center for Disease Control and Preventionhttp://www.cdc.gov/cancer/breast/fact_mammograms.htm
America Cancer Societyhttp://ww2.cancer.org/docroot/NWS/content/NW
_1_1x_Updated_Breast_Cancer_Screening_Guelines_Released.asp
http://www.dshs.state.tx.us/immunize/schedule/default.shtm
http://www.dshs.state.tx.us/immunize/adult_sched.htm

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 56/92
SECTION FOUCLINICAL INFORMATIO
September 20
CLINICAL GUIDELINESSTANDARD STATEMENT POLICIES & PROCEDURES EVALUATION CRITERIA
Recommended Practice: 1. Tetanus, diphtheria, pertussis (Td/Tdap) booster
- Every 10 years2. Rubella – Based on a history of rubella
vaccination or documented serology. Non-pregnant female patients of childbearing age with
unknown or inadequate rubella immunity must beprovided vaccination on-site or referredappropriately.
3. Influenza – annually beginning at age 504. Pneumococcal – once beginning at age 65,
however a repeat may be indicated after fiveyears.
h. Vision and hearing screening
Health Risk Conditions Addressed: Visual andhearing impairment.
Recommended Practice: Periodically beginning atage 65 (optimal frequency not determined).
http://www.dshs.state.tx.us/immunize/adult_sched
F. Episodic or Acute Care Visit Policy: The physical assessment and laboratorytests/interventions must be based on the presentingcomplaints.
G. All clients shall be referred toother appropriate services asneeded.
Policy: Providers must refer patients to their providernetwork as necessary.
Procedures: All patients who require a referral will be referred to theappropriate provider within their provider network.
Health record Documentation of a referral

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 57/92
SECTION FOURCLINICAL INFORMATION
21
September 2011
ClinicalGuidelines(continued)
1. For services determined to be necessary, but which are notprovided by the contractor, patients must be referred to otherresources for care. Contractors are expected to have establishedcommunications with Federally Qualified Health Centers (FQHCs)or DSHS funded organizations that provide primary care services orbreast cancer and cervical cancer screening and diagnosticservices for referral purposes if there are any such providers withintheir service area. Whenever possible, patients should be given achoice of referral resources from which to select. When a patient isreferred to another resource because of an abnormal finding or foremergency clinical care, the contractor must:
• Make arrangements for the provision of pertinent patientinformation to the referral resource (obtaining requiredpatient consent with appropriate safeguards to ensureconfidentiality – i.e., adhering to HIPPA* regulations);
•
Advise patient about his/her responsibility in complying withthe referral;• Counsel patient on the importance of the referral and follow-
up method; and• Follow up to determine if the referral because of an
abnormal finding was completed and document the outcomeof the referral.
*Health Insurance Portability and Accountability Act of 1996
Patients who have abnormal clinical breast exam (CBE) or cervicalcytology findings may be scheduled to return for repeat exams if this isconsidered to be appropriate follow up by the clinician. For patients whosecervical cytology test or CBE results in an abnormal finding that requiresreferral for services beyond those available through primary health care,contractors are encouraged, whenever possible, to refer to a DSHS Breastand Cervical Cancer Services contractor. In order to promote the mosteffective use of limited resources, primary health care contractors’clinicians should be familiar with nationally recognized guidelines andalgorithms describing recommended practice regarding abnormal cervicalcytology and CBE results (See Appendices).

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 58/92
SECTION FIVE
REIMBURSEMENT, DATACOLLECTION & REPORTING

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 59/92
SECTION FIVEREIMBURSEMENT, DATA COLLECTION & REPORTING
1
September 2011
Reimbursement The Health and Safety Code and Texas Administrative Code require PHCactivities to be evaluated on an annual basis. The evaluation processincludes monthly, quarterly, and annual program and fiscal reporting as wellas desk and/or site reviews by DSHS staff. Instructions for reimbursementand/or data collections are included in this section of the manual. Forms forreimbursement and data collection are located in the Forms section.
Billing
Primary Health Care services contract amounts are ceilings against whichcontractors may bill for providing primary health care services to PHC eligibleclients. Once this dollar ceiling has been reached, no further funds will beavailable for reimbursement. Contractors may only bill for services providedto clients who have been screened for potential Medicaid, CHIP, Title V, TitleX, and Title XX eligibility and been deemed as full-service, supplemental, orpresumptive eligible.
Categorical reimbursement for cost of providing services shall be billed onthe State of Texas Purchase Voucher (Form B-13) and submittedsimultaneously to the Contract Development & Support Branch (CDSB)([email protected]) and the Accounting Section/Claims Processing Unit(CPU) ([email protected]). See Form B-13 in the Forms Section forthe PHC State of Texas Purchase Voucher and an example of a completedPHC Purchase Voucher.
Reimbursement request for direct care services will be submitted on amonthly basis. Each request will cover services provided, or expensesincurred, in the preceding month as applicable to the contract attachment.Requests should be submitted within 30 days of the end of the precedingmonth and within 60 days of providing the service. Appropriate financialrecords must be maintained for review by DSHS through the qualityassurance review process and/or fiscal monitoring and/or programmatic deskreviews.
To be paid promptly, Purchase Vouchers must identify the VendorIdentification Number, DSHS document number and Attachment number,and the 10-digit Purchase Order Number. Incorrect identification numbersmay delay payment. Failure to complete these sanctions will delay payment.The Purchase Voucher must also include the total number of unduplicatedclients determined eligible and provided a primary care service for the month
(bottom of box #20 on the voucher). The number of clients entered on thevoucher must match the number of unduplicated clients served that isreported on the corresponding monthly PHC– 200 Report. If a supplementalor amended voucher is submitted, an amended PHC–200 Report must alsobe submitted to the PHC mailbox to reflect the changes in client numbersand/or dollar amounts. The PHC program
must approve the monthly PHC-200 Report before the corresponding

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 60/92
SECTION FIVEREIMBURSEMENT, DATA COLLECTION & REPORTING
2
September 2011
Reimbursement
(continued)
monthly voucher may be processed for payment. Requests submittedwithout the required program reports will not be approved for payment.Vouchers and/or reports submitted with incorrect or missing information willbe rejected and the contractor will be contacted to remedy the problem.
Contractors must continue to submit a State Purchase Voucher andsupporting monthly program reports even after they have reached contractceilings. Any cost over the contract ceiling after deducting program incomeshould be reflected under “Non-DSHS Funding” on the voucher and on theFSR. This submission is required to continue reporting expenditures on anyprogram income collected monthly, and to provide DSHS with statisticalinformation about the use of services.
Non-Reimbursable Expenditures
PHC will not reimburse services for individuals eligible for another program orclients who do not complete the respective eligibility process. Failure to fullycomply with all requirements to apply for Medicaid or CHIP services does notdeem a client eligible for PHC services.
Services are often provided to clients whose screening results indicate theyare potentially Medicaid or CHIP eligible, but the client has not yet completedor received notification of acceptance or rejection of an application. PHCmay cover services delivered on the initial date of contact after the eligibilitydetermination is complete and Medicaid and/or CHIP deny eligibility. Such adenial of eligibility must be documented in the client’s file for the contractor tobill for the initial day’s services to PHC. Once the program’s denial letter isreceived, with the exception of presumptive eligibility, the services providedon the initial day of service may be billed to PHC for reimbursement.
Services delivered to PHC clients with supplemental service benefits mayonly be billed if a supplemental service was provided at the time of the visit.
Submission of Vouchers
Monthly reimbursement requests should be submitted within 30 daysfollowing the end of the month covered by the bill. All claims forreimbursement for services delivered must be submitted within 60 days ofthe end of the contract term. If contractors have services that occurredduring the contract period left to bill after the August Purchase Voucher hasbeen submitted, contractors can bill those services using a Purchase
Voucher and a PHC-200 report marked FINAL and submit the forms on orbefore October 31. PHC contracts require closure of the contract attachmentwithin 60 days of the end of the contract term. All requests forreimbursement must be submitted by email (preferred), or fax to CDSB.
The Purchase Voucher must be submitted by fax or email to CPU. Requestspostmarked more than 60 days following the end of the Contract Attachmentwill not be paid. An original mailed Financial Status

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 61/92

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 62/92
SECTION FIVEREIMBURSEMENT, DATA COLLECTION & REPORTING
4
September 2011
DataCollection &Reporting
PROGRAM INFORMATION
Program Name: Primary Health Care
Contract Type: Categorical
Contract Term: September 1—August 31
VOUCHER: Voucher 1Voucher Name: State of Texas Purchase Voucher Form B-13
Submission Date: Within 30 days following the end of the month. Final due within 60 daysafter end of contract term.Submit Copy to:
Name of Unit/Branch OriginalRequired
Accepted Method ofSubmission
#Copies
Yes No
Contract Development &Support Branch (CDSB)
X Email (preferred), or Fax 1
Claims Processing Unit(CPU)
X Email or Fax 1
Instructions: Submit one Form B-13 voucher to CDSB and one Form B-13 voucher to CPU.Must submit to both.
REPORT: Report 1
Report Name: PHC 200 Monthly Report FormSubmission Date: Within 5 working days following the end of each month.
Submit Copy to:Name of Unit/Branch Original
RequiredAccepted Method of
Submission#
Copies
Yes No
Primary Care Group(PCG)
X Email (preferred), or Fax 1
Instructions: Submit PHC 200 Monthly Report Form to PCG only.
For CY 11, reports are due 1/7, 2/7, 3/7, 4/7, 5/6, 6/7, 7/8, 8/5, 9/8, 10/7, 11/7, 12/7.For CY 12, reports are due 1/6.2/7,3/7,4/6,5/7,6/7,7/9, 8/7, 9/7, 10/5, 11/7, 12/7
NOTE: If you do not submit your PHC 200 by the due date, voucher payments may beheld.
REPORT: Report 2
Report Name: Financial Status Report 269A
Submission Date: Quarterly, Sep 1-Nov 30, Dec 1-Feb 28, Mar 1-May 31, and Jun 1-Aug31. Submit 30 days after the end of each quarter. The 4
thquarter is the final report and due
within 60 days after the end of the contract term. The 4th
quarter report includes all finalcharges and expenses associated with the program contract. Mark the 4
thquarter report as
“Final”.
Name of Unit/Branch OriginalRequired
Accepted Method ofSubmission
#Copies
Yes No
CDSB X Email (preferred), or Fax 1
CPU X Email scanned signeddocument, fax or mail
1
Instructions: Form 269A must have an original signature f(scanned email or fax)..

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 63/92
SECTION FIVEREIMBURSEMENT, DATA COLLECTION & REPORTING
5
September 2011
DataCollection &Reporting(continued)
REPORT: Report 3
Report Name: PHC 300 Annual Report
Submission Date: Within 60 days following the end of the contract period
Submit Copy to:
Name of Unit/BranchOriginalRequired
Accepted Method ofSubmission # Copies
Yes No
Primary Care Group(PCG) X Email (preferred), or Fax 1
Instructions: Submit PHC 300 Annual Report Form to PCG only.
Email CDSB [email protected] Addresses: CPU [email protected]
Fax CDSB (512) 776-7521 Numbers: CPU (512) 776-7442
PCG (512) 776-7713Please use mail codes on all mail cominginto DSHS to ensure accurate delivery.
Mail CDSB Mail code 1914Codes: CPU Mail code 1940
PCG Mail code 2831
Claims Processing Unit, Mail Code 1940Mailing Address Department of State Health Services
for CPU: P.O. Box 149347Austin, TX 78714-9347
Last Updated Reviewed: 6/8/10
Quarterly Financial Status Report (FSR or Form 269a) must be submitted
directly to the DSHS Accounting Section, Claims Processing Unit and theCDSB within 30 days of the completion of the quarter. This form requires anoriginal signature for CPU. ** New For FY10: Scanned signed FSRs areacceptable. A scanned document may be emailed or faxed to CPU.
The fourth quarter Financial Status Report should be marked as “FINAL” and submitted within 60 days of the completion of the contract year to theDSHS Accounting Section, Claims Processing Unit and to CDSB. This formrequires an original signature for CPU.
ProgramActivityReports
Program
PHC-200 Monthly Report – The following instructions are provided to helpcomplete the monthly PHC-200. For the purposes of this report, the term“unduplicated” is defined as counting a client/individual only once during thereporting time specified. (See Form 200 reporting form)
The purpose of the PHC-Form 200 Monthly report is to provide the following

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 64/92
SECTION FIVEREIMBURSEMENT, DATA COLLECTION & REPORTING
6
September 2011
ActivityReports(continued)
information to DSHS:• PHC caseload, and• Contractor’s expenditure levels by PHC service
PHC-200 Monthly report must be completed and submitted to DSHS PrimaryCare Group (PCG) within 5 working days of the month following the reportmonth.
Email Form 200 to PCG – [email protected] (preferred), orfax to DSHS PCG at 512/ 776-7713.
General Information:Contractor: Name of contractor on DSHS contractReport or Amended Report: Enter month and year the expenditures arespent/paid.
Any amendments to a report should be marked as “Amended” and submittedon the Form 200. The amended item(s) should be circled, highlighted,bolded or identified in some way.
Sanctions
Sanctions
Sanctions Due to Non-Compliance With Reporting
The Performance Management Unit will apply the following procedures whenreports and/or vouchers are not received by the required deadlines:
Fifteen (15) calendar days after any report or voucher is due – DSHS notifiesthe contractor to request that the monthly report or voucher be submittedwithin five (5) business days. Note: Payments cannot be processed untilcorrect and complete information is received.
Five (5) business days after the written notice is sent – The manager of theContract Management Branch (CMB) will determine if technical assistance(TA) should be provided. If the contract has frequently been late insubmitting reports and billing, contract sanctions may be imposed.
Contract sanctions – According to Article XIV of the DSHS Contract GeneralProvisions (Core/Sub-recipient), the list of sanctions that may be imposed isnot limited to the following:
• Require contactor to receive technical or managerial assistance;• Temporary withhold cash payments;• Permanently withhold cash payments;• Disallow use of all or part of the funds allocated to the contract;• Delay execution of a new contract or renewal;• Reduce funding for the contract;• Suspend all or part of the contract;• Terminate the contract; or• Deny additional or future contracts or renewals.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 65/92
SECTION FIVEREIMBURSEMENT, DATA COLLECTION & REPORTING
7
September 2011
Reserved for future use.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 66/92
FORMS

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 67/92
DSHS FUNDING SOURCE – Application for Health Care AssistanceFUENTE DE FONDOS DEL DSHS – Solicitud de asistencia médica
Applicant Information / Información del solicitante Name (Last, First, Middle) / Nombre (apellido y primer y
segundo nombre)Home Telephone Number / Teléfono de la casa Email Address / Correo
electrónico
Texas Residence Address (Street or P.O. Box) / Direcciónresidencial en Texas (calle o apartado postal)
City / Ciudad County / Condado State / Estado ZIP / Códigopostal
Household Information / Información de la unidad familiar Fill in the first line with information about yourself. Fill in the remaining lines for everyone who lives in the house with you for which you arelegally responsible. / Llene la primera línea con información acerca de usted mismo. Llene las líneas restantes por todas las personas que viven con
usted, y por las que es legalmente responsable. Name (Last, First, Middle)
Nombre (apellido y primer y segundonombre)
SSN (optional)Núm. del Seguro Social
(opcional)
Date of BirthFecha de
nacimiento
AgeEdad
SexSexo
RaceRaza
What Relation toyou?
Parentesco con usted
U.S. CitizenCiudadano
estadounidense
Yes / Sí No1. Self / Yo mismo
2.
3.
4.
5.
6.
List all of your household’s income below. Be sure to include the following: Government checks; money from work; money you collect fromcharging room and board; cash gifts, loans, or contributions from parents, relatives, friends, and others; sponsor’s income; school grants orloans; child support; and unemployment. / Haga una lista de los ingresos de su unidad familiar a continuación. Asegúrese de incluir: cheques delgobierno; dinero por trabajo; dinero que recibe por cobros de hospedaje y comida; regalos en efectivo, préstamos, o aportaciones de sus padres,familiares, amigos y otras personas; ingresos del patrocinador; becas o préstamos escolares; manutención de niños o pagos por desempleo.
Name of person receivingmoney
Nombre de la persona querecibe el dinero
Name of agency, person, oremployer who provides the
moneyNombre de la agencia, persona oempleador que provee el dinero
Amount receivedCantidad recibida
How often received? (daily, weekly,every two weeks, twice a month,
monthly?) ¿Con qué frecuencia lorecibe? (Diariamente, semanalmente,quincenalmente o mensualmente)
Do you have an immediate medical need? ¿Tiene usted alguna necesidad médica inmediata? Yes / Sí No Do you – does any one in your household – have health care coverage (Medicaid, Medicare, CHIP, healthinsurance, V.A., Tricare, etc.)? ¿Tiene usted o alguien de su unidad familiar cobertura médica (Medicaid, Medicare,CHIP, seguro medico, V.A., Tricare, etc.)?If yes, who? / Si contestó que “Sí”, ¿quién?
Yes / Sí No
Do you – does any one in your household – have any special circumstances? ¿Tiene usted o alguien de su unidad
familiar alguna circunstancia especial?If yes, who? Si contesta que “Sí”, ¿quién?
Yes / Sí No
The statement I have made, including my answers to all questions, are true and correct to the best of my knowledge and belief. I agree to giveeligibility staff any information necessary to prove statements about my eligibility. I understand that giving false information could result indisqualification and repayment. A mi leal saber y entender, la declaración que he hecho y mis respuestas a todas las preguntas son verdaderas y
correctas. Me comprometo a dar al personal de verificación de requisitos toda la información necesaria para comprobar mis declaraciones sobre dichosrequisitos. Yo entiendo que dar información falsa podría causar que me descalifiquen y que tenga que devolver el pago al Programa. Signature – Applicant / Firma – Solicitante Date / Fecha Signature – Spouse (if applicable) / Firma – Cónyuge (de ser aplicable) Date / Fecha
Signature – Person Who Helped Complete this Application –Firma – Persona que ayudó a completar esta solicitud
Relationship to Client / Relación con el cliente Date / Fecha
EF05-13229

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 68/92
DSHS FUNDING SOURCE – Application for Health Care AssistanceFUENTE DE FONDOS DEL DSHS – Solicitud de asistencia médica
APPLICATION FOR HEALTH CARE ASSISTANCE
1. Complete name and address;2. Applicant and spouse (if applicable) must sign and
date the application; and3. Answer as many questions as possible on this
application
Turn in or mail back the application today even if all thequestions are not answered.
RESPONSIBILITIES
Applicants are responsible for completing page one of thescreening and eligibility form for medical services assistance.
Applicants are responsible for providing documents requestedby the contractor. Some examples of items that may be neededfor proof and documents that can be used for proof are:
Where Applicant Lives and Plans to Continue Livingo Possible Proof: Valid Texas Drivers Licenseo Current voter registrationo Rent or utility receipts for one month prior to the
month of applicationo Motor vehicle registrationo School recordso Medical cards or other similar benefit cards
o Property tax receipto Mail addressed to the applicant, his / her spouse, or
children if they live togethero Other documents considered valid by the contractor
Applicant Incomeo Possible Proof: Pay check stubs
o Pay checkso W-2 tax forms or income tax returnso Sales recordso Statements from employers
o Award letterso Legal documentso Statements from persons giving you money
Other Health Care Coverageo Possible Proof: Award or claim letterso Insurance policieso Court documents
o Other legal papers
Information on social security numbers should be given if this
information is available. Information on sex (Male / Female) isvoluntary. These types of information will not affect youreligibility.
Applicant must give information about health care insurance and
any other third party financially liable for health care services.
SOLICITUD DE ASISTENCIA MÉDICA
1. Nombre y dirección completos;
2. El solicitante y el/la cónyuge (de ser aplicable) debenfirmar y fechar la solicitud y
3. Conteste tantas preguntas como pueda en esta solicitud
Entregue su solicitud, o mándela por correo, hoy mismo aunque noconteste todas las preguntas.
RESPONSABILIDADES
Los solicitantes son responsables de completar la primera página
del formulario de evaluación y determinación de requisitos deservicios de asistencia médica.
Los solicitantes son responsables de proporcionar los documentossolicitados por el contratista. Los siguientes son ejemplos de lascosas podrían necesitar como comprobantes y los documentos quepueden usarse como comprobantes:
Lugar donde vive y planea seguir viviendo el solicitanteo Posibles comprobantes: licencia de conducir de Texas
válida
o Inscripción en el registro de votantes actualo Recibos de renta o servicios públicos del mes anterior al
mes de la solicitudo Registro de automóvil
o Registros escolareso Tarjetas médicas o de otras prestaciones similareso Recibo de impuestos sobre la propiedad inmobiliariao Correo dirigido al solicitante, su cónyuge o sus hijos si
viven juntoso Otros documentos considerados válidos por el contratista
Ingresos de los solicitanteso Posibles comprobantes: talones de cheque de pagao Cheques de pagao Formularios W-2 de declaración de impuestoso Registros de ventaso Declaraciones de empleadores
o Cartas de asignación de dineroo Documentos legaleso Declaraciones de las personas que le dan dinero
Otra cobertura médicao Posibles comprobantes: cartas de asignación de dinero o
reclamacióno Pólizas de seguro
o Documentos de la corteo Otros documentos legales
Debe darse la información sobre los números del Seguro Social sila información está disponible. La información sobre su sexo (si eshombre o mujer) es voluntaria. Estos tipos de información noafectarán su derecho a participar.
El solicitante debe dar información sobre seguros médicos y
cualquier tercera persona económicamente responsable de losservicios médicos.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 69/92
DSHS FUNDING SOURCE - Worksheet
Today’s Date Client/Case # Type of DeterminationNew Re-certification
Applicant Name Case Record Action
Approved Presumptive Supplemental Denied
Eligibility Effective Date(MM-DD-YYYY)
Eligibility Items Documentation (if applicable)Family Composition – Legal Responsibility
1.
2.
3.
4.
5. .
6.
Residency – Must be physically present within the geographicboundaries of Texas.
Documentation of Residency (if applicable) Type of Income Name of Member w/Income Documentation of Income (if applicable)
Gross Earned Income
Cash Gifts/Contributions
Child Support Payments
Dividends/Interest/Royalties
Loans (Non-educational)
Lawsuit/Lump-sum Pymts.
Mineral Rights
Pensions/Annuities
Reimbursements
Social Security Payments
Unemployment Payments
VA Payments
Worker’s Compensation
Total Countable Income
Minus Dependent Care - - FPL Used: 100% > 133% 150%Net Countable Income 185% 200% 225% 250%Other Benefits – Such as Medicaid, Medicare, CHIP, CIHCP, private health insurance, V.A., Tricare, etc.
Special Circumstances – Document any special circumstances as needed and applicable to this application
Co-Pay Fees – DOCUMENT CO-PAY BELOW:
Eligible Household Member(s):
1.
BCCS PHC DSHS FPTitle V/MCH
2.
BCCS PHC DSHS FPTitle V/MCH
3. BCCS PHC DSHS FPTitle V/MCH
4.
BCCS PHC DSHS FPTitle V/MCH
5.
BCCS PHC DSHS FPTitle V/MCH
6. BCCS PHC DSHS FPTitle V/MCH
Provider-Staff Signature: Date:
EF05-13227
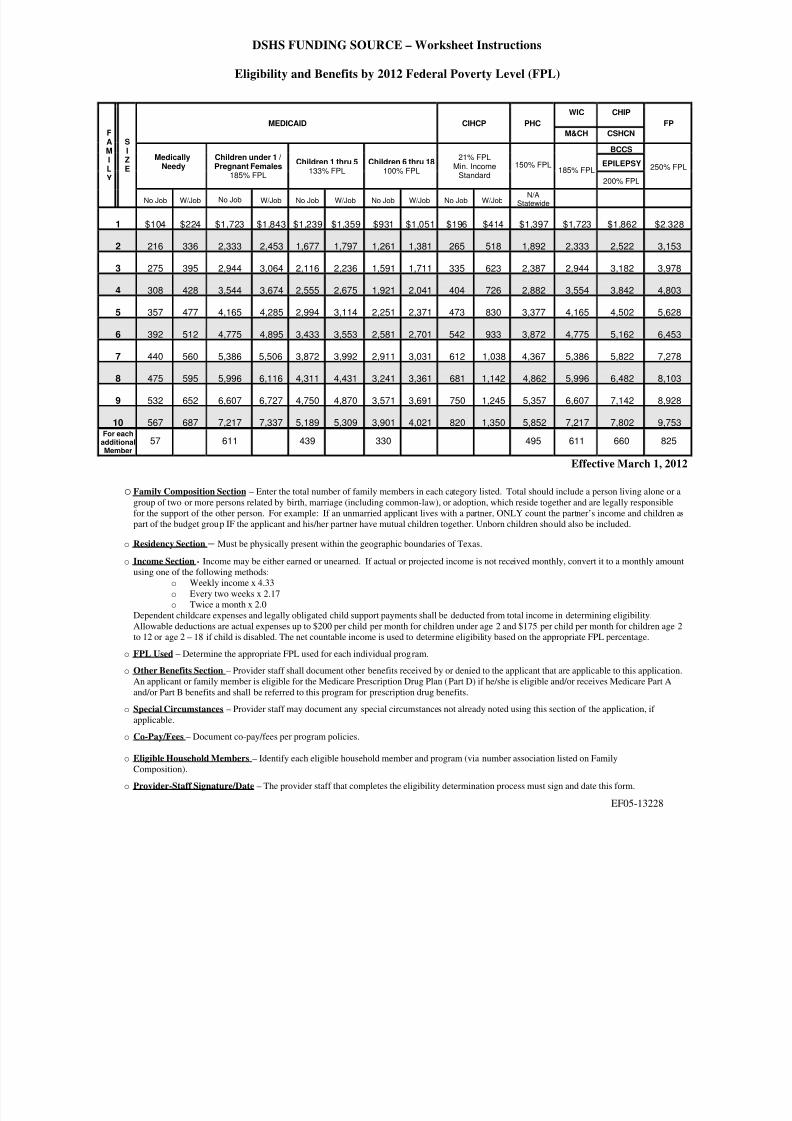
8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 70/92
DSHS FUNDING SOURCE – Worksheet Instructions
Eligibility and Benefits by 2012 Federal Poverty Level (FPL)
WIC CHIP
MEDICAID CIHCP PHC
M&CH CSHCN
FP
BCCS
EPILEPSYMedicallyNeedy Children under 1 /Pregnant Females185% FPL
Children 1 thru 5133% FPL
Children 6 thru 18100% FPL
21% FPLMin. IncomeStandard
150% FPL 250% F185% FPL
200% FPL
Effective March 1, 20
FAM
ILY
SI
ZE
No Job W/Job No Job W/Job No Job W/Job No Job W/Job No Job W/JobN/A
Statewide
1 $104 $224 $1,723 $1,843 $1,239 $1,359 $931 $1,051 $196 $414 $1,397 $1,723 $1,862 $2,32
2 216 336 2,333 2,453 1,677 1,797 1,261 1,381 265 518 1,892 2,333 2,522 3,153
3 275 395 2,944 3,064 2,116 2,236 1,591 1,711 335 623 2,387 2,944 3,182 3,978
4 308 428 3,544 3,674 2,555 2,675 1,921 2,041 404 726 2,882 3,554 3,842 4,803
5 357 477 4,165 4,285 2,994 3,114 2,251 2,371 473 830 3,377 4,165 4,502 5,628
6 392 512 4,775 4,895 3,433 3,553 2,581 2,701 542 933 3,872 4,775 5,162 6,453
7 440 560 5,386 5,506 3,872 3,992 2,911 3,031 612 1,038 4,367 5,386 5,822 7,278
8 475 595 5,996 6,116 4,311 4,431 3,241 3,361 681 1,142 4,862 5,996 6,482 8,103
9 532 652 6,607 6,727 4,750 4,870 3,571 3,691 750 1,245 5,357 6,607 7,142 8,928
10 567 687 7,217 7,337 5,189 5,309 3,901 4,021 820 1,350 5,852 7,217 7,802 9,753For each
additionalMember
57 611 439 330 495 611 660 825
o Family Composition Section – Enter the total number of family members in each category listed. Total should include a person living alone orgroup of two or more persons related by birth, marriage (including common-law), or adoption, which reside together and are legally responsiblefor the support of the other person. For example: If an unmarried applicant lives with a partner, ONLY count the partner’s income and childrenpart of the budget group IF the applicant and his/her partner have mutual children together. Unborn children should also be included.
o Residency Section – Must be physically present within the geographic boundaries of Texas.
o Income Section - Income may be either earned or unearned. If actual or projected income is not received monthly, convert it to a monthly amouusing one of the following methods:
o Weekly income x 4.33o Every two weeks x 2.17o Twice a month x 2.0
Dependent childcare expenses and legally obligated child support payments shall be deducted from total income in determining eligibility.Allowable deductions are actual expenses up to $200 per child per month for children under age 2 and $175 per child per month for children age
to 12 or age 2 – 18 if child is disabled. The net countable income is used to determine eligibility based on the appropriate FPL percentage.
o FPL Used – Determine the appropriate FPL used for each individual program.
o Other Benefits Section – Provider staff shall document other benefits received by or denied to the applicant that are applicable to this applicatioAn applicant or family member is eligible for the Medicare Prescription Drug Plan (Part D) if he/she is eligible and/or receives Medicare Part Aand/or Part B benefits and shall be referred to this program for prescription drug benefits.
o Special Circumstances – Provider staff may document any special circumstances not already noted using this section of the application, if applicable.
o Co-Pay/Fees – Document co-pay/fees per program policies.
o Eligible Household Members – Identify each eligible household member and program (via number association listed on FamilyComposition).
o Provider-Staff Signature/Date – The provider staff that completes the eligibility determination process must sign and date this form.
EF05-13228
8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 71/92
STATEMENT OF APPLICANT’S RIGHTS AND RESPONSIBILITIESDECLARACIÓN DE LOS DERECHOS Y DEBERES DEL SOLICITANTE
By signing this application for assistance, I affirm the following: Al firmar esta solicitud para recibir asistencia, yo afirmo lo siguiente:
The information on the application and its attachments is trueand correct. This application is a legal document. Deliberatelyomitting information or giving false information may cause theProvider to terminate services to a member of myhousehold/family or me.
La información escrita en la solicitud y en sus anexos es verdadera ycorrecta. Esta solicitud es un documento legal. El deliberadamente omitirinformación o el proporcionar información falsa podría dar lugar a que elProveedor cancele los servicios a uno de los miembros de mi hogar, de mifamilia o los míos propios.
If I omit information, fail or refuse to give information, or givefalse or misleading information about these matters, I may berequired to reimburse the State for the services rendered if I amfound to be ineligible for services. I will report changes in my
household/family situation that affect eligibility during thecertification period (changes in income, household/familymembers, and residency).
Si yo omito información, dejo de proporcionar o me niego a proporcionarinformación o; proporciono información falsa o engañosa acerca de estosasuntos, podría requerírseme que reembolse al Estado el costo de losservicios recibidos, si acaso se determina que no califico para los servicios.
Yo reportaré los cambios en la situación de mi hogar, de mi familia, queafecten la elegibilidad durante el período de certificación (cambios en elingreso, en los miembros del hogar, en la familia y, cambios de residencia.)
I authorize release of all information, including but not limited to,income and medical information, by and to the Texas Departmentof State Health Services (DSHS) and Provider in order todetermine eligibility, to bill, or to render services to myhousehold/family or me.
Yo autorizo la divulgación de toda la información, incluyendo pero nolimitada a, el ingreso y a la información médica, de parte de y para, elTexas Department of State Health Services (DSHS) [Departamento Estatal de Servicios de Salud de Texas ] y, al Proveedor para poder determinar laelegibilidad, para poder cobrar o, proporcionar servicios en mi hogar, a mifamilia o, a mí personalmente.
I understand I may be asked by Provider to provide proof of anyof the information provided in this application.
Entiendo y acepto que podría pedirme el Proveedor que proporcionecomprobantes de cualquiera de la información proporcionada en estasolicitud.
Health insurance coverage, including but not limited to individualor group health insurance, health maintenance organizationmembership, Medicaid, Medicare, Veterans Administrationbenefits, TRICARE, and Worker’s Compensation benefits, mustbe reported to Provider. Benefits from health insurance may beconsidered the primary source of payment for health carereceived. I hereby assign to Provider any such benefits. I alsoassign payment for benefits and services received from andthrough Provider directly to the service providers.
La cobertura de seguro de salud, incluyendo pero no limitada a seguropara un individuo o seguro de salud para un grupo de personas; los demembresía proporcionados por organizaciones para el mantenimiento de lasalud [como HMO], Medicaid , Medicare ; beneficios de la Veterans Administration; de la TRICARE y Worker’s Compensation [beneficios deCompensación Laboral], deben ser reportados al Proveedor. Losbeneficios provenientes de esos seguros de salud pudieran serconsiderados como la fuente principal de pago de la atención de saludrecibida. Por este medio yo, asigno al Proveedor cualquiera de dichosbeneficios. También asigno el pago de los beneficios y servicios recibidosde parte de y, a través del Proveedor, directamente a los proveedores deservicios.
I understand that, to maintain program eligibility, I will berequired to reapply for assistance at least every twelve months.
Yo entiendo y acepto que, para mantener la elegibilidad para el programa,se me va a requerir que vuelva a solicitar para recibir asistencia, por lomenos cada doce meses.
I am a bona fide resident of Texas or a dependent. I physicallylive in Texas, maintain living quarters in Texas, and do not claimto be a resident of another state or country, or am a dependent of
a bona fide Texas resident.
Soy residente legítimo de Texas o bien, dependiente del territorio. Yo vivofísicamente en Texas, mantengo residencia en Texas y, no afirmo serresidente de otro estado o país o bien, soy un dependiente de un residente
legítimo de Texas. Some programs provide care through program-approvedproviders. I understand that, to receive benefits from suchprograms, treatment must be received through those program-approved providers.
Algunos programas proporcionan atención a través de proveedoresaprobados por los programas. Yo entiendo y acepto que, para recibirbeneficios de dichos programas, el tratamiento debe ser recibido a travésde esos proveedores aprobados por el programa.
I understand that criteria for participation in the program are thesame for everyone regardless of sex, age, disability, race, ornational origin.
Yo entiendo y acepto que el criterio para la participación en el programa esel mismo para todos sin importar sexo, edad, discapacidad, raza o bien,origen de nacionalidad.
I understand I have the right to file a complaint regarding thehandling of my application or any action taken by the programwith the HHSC Civil Rights Office at 1-888-388-6332.
Yo entiendo y acepto que tengo el derecho de registrar una queja conrelación al manejo de mi solicitud o con relación a cualquier acción tomadapor el programa con HHSC Civil Rights Office de 1-888-388-6332.
I understand that I will receive written documentation concerningthe services for which my household/family or I is eligible orpotentially eligible.
Yo entiendo y acepto que recibiré documentación por escrito concernientea los servicios para los cuales mi hogar, mi familia o yo calificamos o,potencialmente lleguemos a calificar.
With few exceptions, you have the right to request and beinformed about information that the State of Texas collects aboutyou. You are entitled to receive and review the information uponrequest. You also have the right to ask the state agency tocorrect any information that is determined to be incorrect. Seehttp://www.dshs.state.tx.us for more information on PrivacyNotification. (Reference: Government Code, Section 552.021,522.023 and 559.004)
Tan solo por unas cuantas excepciones, usted tiene el derecho de solicitary de ser informado sobre la información que el Estado de Texas reúnesobre usted. A usted se le debe conceder el derecho de recibir y revisar lainformación al requerirla. Usted también tiene el derecho de pedir que laagencia estatal corrija cualquier información que se ha determinado seaincorrecta. Diríjase a http://www.dshs.state.tx.uspara más informaciónsobre la Notificación sobre privacidad. (Referencia: Government Code ,sección 552.021, 522.023 y 559.004)
I understand and agree that the program does not providepayment for inpatient care. I understand that I must make my ownarrangement for hospital care and that I am responsible for thecost of the care.
Entiendo y acepto que el programa no proporciona pago por la atención depacientes internos. Entiendo y acepto que yo debo hacer mis propiosarreglos de atención en el hospital y que yo soy responsable por el costode la atención.
Signature – Applicant / Firma – Solicitante Date / Fecha Provider Staff Signature Date
PHC 10-1September 2010
FORM 101

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 72/92
Presumptive Eligibility - Title V and Primary Health Care
Name/Nombre Home Telephone No./Teléfono de la casa(If no phone, give number of person who can reach applicant/ de no tenerteléfono, proporcione el teléfono de la persona que pueda ponerse en contacto
con el solicitante)
Mailing Address (Street or P.O. Box)/Dirección Postal (Calle oApdo.)
City/Ciudad State /Estado ZIP/Zona Postal
Home Address, if different from above. Domicillio particular, si es diferente a la dirección de arriba.
1. Are you or the person applying for services a resident of Texas?¿Son residents de Texas, usted o la persona que solicita servicios?….…………………………….. Yes /Sí No
2. How many family members live with you? (Count only applicant, spouse and children for whom applicant islegally responsible.)¿Cuántos miembros de la familia viven con usted? (Cuente únicamente al solicitante,esposo(a) y niños de los que el solicitante es legalmente responsable.) __________________________________
3. How much money (before deductions) does your family receive each month? ¿Cuánto dinero (antes de lasdeducciones) recibe su familia por mes? __________________________________________________________
I am in need of immediate medical care. To the best of my knowledge, I have no other way to receive medicalcare and am applying for Presumptive Services. I understand that within 90 days following the delivery ofservices, I will submit a completed application for eligibility determination. The above information is true,correct, and complete to the best of my knowledge.
Yo estoy necesitando atención médica inmediata. En lo que a mí concierne carezco de cualquier otro medio para
recibir atención médica y estoy solicitando Presumptive Services [Servicios Condicionales.] Yo entiendo y acepto quedentro de 90 días después de recibir los servicios yo entregaré una solicitud completamente llena, para que se lleve acabo la determinación de elegibilidad. La información arriba proporcionada es verdadera, correcta y completa según mleal saber y entender.
Signature – Applicant / Firma – Solicitante Date / Fecha Signature – Provider Staff / Firma – Oficinista Date / Fecha
I was not able to complete the eligibility determination process for the Program. My appointment for returningmy complete application and interview is:No me fue posible completar el proceso de determinación de elegibilidad para el Programa. La cita para devolver msolicitud ya llenada y para la entrevista es
Date and Time / Hora y Fecha Location and Phone/ Lugar y Teléfono
I understand this is my obligation for the services received.Yo entiendo y acepto que esta es mi obligación por los servicios recibidos.
EF21-11817 PHC 10-1September 2010
FORM 102

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 73/92
PHC 10-1September 2010
Presumptive Eligibility FormInstructions
PURPOSE1. If applicant cannot fulfill application procedures AND applicant is in need of immediate medical services, the
Presumptive Eligibility Form is to be completed. Additionally, a Statement of Applicant’s Rights andResponsibilities must be completed.
2. To establish if applicant appears to be eligible for Title V and/or Primary Health Care.
PROCEDUREWhen to PrepareComplete for persons in medical need who appear to be eligible for Title V and/or Primary Health Care but time orlack of materials prevent screening and eligibility determination.
Number of Copies
Complete an original and one copy.
TransmittalGive a copy of the form to the applicant with an appointment time for application process. File original.
Form RetentionKeep the case record copy for three state fiscal years after services rendered.
DETAILED INSTRUCTIONSComplete the date, name of applicant, name of legally responsible adult if applicant is a minor, address andphone number where applicant (legally responsible adult) can be reached. Agency staff is responsible forensuring appropriate completion of the Presumptive Eligibility Form and a Statement of Applicant’s Rights and
Responsibilities.
1. Verify the residency of applicant and mark yes or no. Refer to the policy manual for definition of residency.2. Enter the number of members in the immediate family. Refer to the policy manual for definition of family.3. Enter the gross monthly income of the immediate family. Refer to the policy manual for definition of income if
applicant falls within Program guidelines.
The applicant appears to be potentially eligible for services on a Presumptive Eligibility basis if the applicant:1. is a Texas resident, and2. gross monthly family income (based on family size) falls at or below income guidelines.
NOTE:If the contractor renders services and the above two criteria were not met, Title V and/or PHC will not reimburse.If applicant does not meet these two criteria it is up to the Contractor to determine where and when services willbe provided. Although Title V and PHC are under strict eligibility guidelines, it is encouraged that an applicant'smedical needs be met quickly and appropriately using whatever resources are locally available.
FORM 102AINSTRUCTIONS
8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 74/92
Notice of Eligibility/Aviso de Elegibilidad - Title V and Primary Health Care
Date/Fecha Case No./ Número de caso Expiration Date/ Fecha de vencimiento
Office Address/ Dirección de la oficina Office Telephone /Teléfono de la oficina
Provider Staff Name/Nombre del trabajador
1. Your individual / family application for Title V / Primary Health Care is APPROVED / DENIED.
Su solicitud individual / familiar para el Título V / Programa de Atención Médica Primaria ha sido APROBADA / NEGADA.
2. If approved, the following services will be provided beginning ______________________. (MM/DD/YYYY)
Si tiene derecho, se ofrecerán los siguientes servicios a partir del ______________________.(mes/día/año)
Name/NombreDate of Birth/
Fecha denacimiento
Services/Servicios
a.
b.
c.
d.
e.
3. Your co-pay is $______________ for services and $______________ for prescriptions.
Su copago es $______________ por servicios y $_______________ por recetas médicas.
4. You must notify this office as soon as possible of any changes in your situation such as changes inincome, property, health insurance, family members or address. Usted tiene que avisar a esta oficina tanpronto sea posible de cualquier cambio en su situación como cambios de ingresos, propiedad, seguro medico,personas de la familia o dirección.
5. If a change occurs that makes you ineligible, and you fail to report the change as required, you may beresponsible for payment of any medical services you receive after you become ineligible, or you may besubject to prosecution under the Texas Penal Code. Si ocurre un cambio que hace que pierda laelegibilidad y usted no informa del cambio como se exige, es posible que sea responsable de pagar cualquierservicio médico que reciba después de perder la elegibilidad, o puede ser que sea sujeto a enjuiciamiento bajoen Código Penal de Texas.
6. You are responsible for renewing your eligibility prior to your certification expiration date. A DSHSFunding Source - Application for Health Care Assistance must be completed and submitted within thirty(30)-days of your anniversary eligibility date. Assistance will be provided if needed. Usted esresponsable de renovar su elegibilidad antes de la fecha de vencimiento de la certificación. Tiene que llenar y
entregar un Screening and Eligibility Determination Form for Medical Services Assistance dentro de los treinta(30) días de la fecha de su aniversario. Recibirá ayuda si es necesario.
7. If not eligible, your application for Title V/Primary Health Care benefits has been denied due to: Si no tiene derecho, su solicitud para beneficios del Programa de Atención Médica Primaria/Title V se hanegado porque:
If you believe this decision is not correct, you may request an appeal from this office. Si cree que estadecisión no está correcta, puede pedir una súplica de esta officina.
September 2011
FORM 103

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 75/92
PHC 10-1September 2010
Notice of Eligibility FormInstructions
PURPOSE1. To notify Title V and/or Primary Health Care applicants that they are either eligible or not
eligible for assistance.2. To notify Title V and/or Primary Health Care clients of their responsibilities to report
changes in their situation and their liability if they fail to report changes.
PROCEDUREWhen to PrepareComplete form for individuals applying for Title V and Primary Health Care.
Number of CopiesComplete an original and one copy.
TransmittalFace-to-face or mail form to the individual applying for assistance. File copy in the caserecord.
Form RetentionKeep the case record copy for three state fiscal years after eligibility begins. However,eligibility is valid for a maximum of twelve months.
DETAILED INSTRUCTIONSComplete the information listed on the form.
FORM 103AINSTRUCTIONS

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 76/92
Form 104
PHC 10-1September 2010
PRIMARY HEALTH CARE PROGRAMREQUEST FOR INFORMATION
PROGRAMA PRIMARIO de ASISTENCIA MEDICASOLICITUD DE INFORMACIÓN
Date /Fecha
Case Record No. /Núm de Caso
Office Address and Telephone No./Oficina y Teléfono
Your application for assistance is not complete. To determine your eligibility, we need the followingadditional information. /Su solicitud de asistencia no está completa. Para determinar su elegibilidad,necesitamos la siguiente información.
ONLY THE CHECKED BOXES APPLY TO YOU. /SOLAMENTE LAS CASILLAS MARCADAS SE APLICAN A SU CASO.
Mail Addressed to You or Another Household Member Federal Income Tax Return
Correo Dirigido a Usted o a Otra Persona de su Casa Declaración de los Impuestos Federales Sobre los Ingresos
Texas Driver’s License or Other Official Identification Self-Employment Bookkeeping, Sales, Expenditure Records
Licencia de Manejar de Texas u Otra Identificación Oficial Comprobantes de Cuentas, Ventas, Gastos de Trabajo Independiente
Voter Registration Card Social Security Award Letter, Check, or Denial Notice
Certificado de Registro Electoral Cheque de Seguro Socil o Carta Diciendo si se lo Van a Dar o No
Notice of TANF, SNAP/ Food Stamps, or Medicaid Benefits Disability Insurance Award Letter or Check
Aviso de Beneficios de TANF,Estampillas para Comida o Medicaid Cheque de Seguro por Incapacidad or Carta Diciendo que Van a Dárselo
Paychecks or Paycheck Stubs Unemployment Compensation Award Letter or Check
Cheques de Paga o Talones de Cheques de Paga Cheque de Compensación de Desempleo o Carta Diciendo que Van a Dárselo
Earnings Statement from Employer Veterans Administration Award Letter or Check
Verificación de Sueldo Preparada por el Empleador Cheque de la Administración de Veteranos o Carta Diciendo que Van a Dárselo
Worker’s Compensation Award Letter or Check Other ItemsCheque del Seguro Obrero o Carta Diciendo que Van a Dárselo Otra
PLEASE RETURN THE ITEMS CHECKED ABOVE BY:HAGA EL FAVOR DE ENVIAR LOS DOCUMENTOS ENUMERADOS PARA EL:
If we do not receive the information we need and you do not contact me, I will assume that you do
not want assistance. Call me if you have any questions. / Si no recibimos la información quenecesitamos y usted no se comunica conmigo, supondré que usted no quiere asistencia. Si tiene algunapregunta, hábleme.
Signature/Firma:
8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 77/92
Form 128
Page 1 of 2
PHC 10-1September 2010
PRIMARY HEALTH CARE PROGRAMEMPLOYMENT VERIFICATION
Date/Fecha
Case Record No. /Núm de Caso
Office Address and Telephone No./Oficina y Teléfono
Fax:
Employee Social Security Number
This individual is a member of a household applying for health care assistance from the PrimaryHealth Care Program. To determine this household’s eligibility, it is necessary to verify allearnings. Since this individual is/was/will be your employee, your help is needed.
Please completely and accurately provide the information requested on the back of this letter. Ifa question does not apply, mark it N/A. After you complete this form, give it to your employee,mail it in the envelope provided, or fax it to the number listed above.
This information is needed by this date: ______________________. If you could send it beforethis date, it would be most appreciated.
Thank you for helping. If you have questions, please feel free to call.
I give my permission to release the information requested on this form.
Yo doy mi permiso para que mi empleador dé la información que se pide en esta forma.
Signature / Firma Date / Fecha
Comments:

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 78/92
Form 128
Page 2 of 2
PHC 10-1September 2010
EMPLOYMENT VERIFICATION
Employee Name (as shown on your records)
Employee Address – Street, City, State, ZIP (as shown on your records)
Is/was/will this person (be) employed by you? Is FICA or FIT withheld?
Yes No If yes Permanent Temporary Yes No
Rate of Pay Average Hours per Pay Period How often is employee paid?
$PerHour
PerDay
PerWeek
PerMonth
PerJob
On the chart below, list all wages receivedby this employee during the months of: _______________________________________________________
Date Pay Period Ended
Date Employee
Received Paycheck Actual Hours Gross Pay
Other Pay *(Bonuses, Commissions,
Overtime, Pension Plan,Profit Sharing, Tips)
* In Comments Section below, please explain when and how Other Pay is received.
Date Hired Date First Paycheck Received If employee is/was on Leave Without Pay
Start Date: End Date:
If this person is no longer in your employ
Date Final Paycheck Received: Gross Amount of Final Paycheck: $
Is health insurance available?
Yes No If Yes, employee is Not EnrolledEnrolled forSelf Only
Enrolled withFamily Members
Comments:
Signature and Title of Person Verifying This Information Date
Company or Employer Address (Street, City, State, ZIP) Telephone Number (Include area code.)

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 79/92
Form 14
Page 1 of
PHC 10-1
September 2010
STATEMENT OF SELF-EMPLOYMENT INCOMEDECLARACIÓN DE INGRESOS DEL NEGOCIO PROPIO
See Instructions on Page 2. /Vea las Instrucciones en la página 2.
Case Record Name Case Record Number
1. Name of Person Having Self-Employment Income /Nombre de la persona que tiene ingresos de negocio propio.
2. Give the number of months covered by this income statement.Dé el número de meses que cubre esta declaración de ingresos. .............................................................................
3. Describe what you did to earn this money. /Describa lo que hizo para ganarse este dinero.
4. List your business expenses and income. IMPORTANTE: Attach receipts, invoices, or other verifying papers. Anote los gastos y ingresos de su negocio. IMPORTANTE: Adjunte recibos, facturas, u otros comprobantes.
DateFecha
EXPENSESGASTOS
AmountCantidad
Date Fecha
INCOMEINGRESOS
AmountCantidad
$ $
Total Expenses
Total de Gastos$
SUBTOTAL $
Enter expenses here and subtract.Anote el total de gastos y reste. —
NET SELF-EMPLOYMENT INCOMEINGRESOS NETOS DEL NEGOCIO PROPIO $
The above information is true, correct, and complete to the best of my knowledge. I understand that givingfalse information to the provider could result in my being disqualified for fraud. /Según mi leal saber y entendertoda esta información es cierta, correcta y completa. Comprendo que si doy información falsa al proveedo puedo sedescalificado por fraude.
Signature of anyone helping you to prepare this form / DateFirma de la persona que le ayudó a llenar la forma / Fecha
Signature / Firma Date / Fecha

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 80/92
Form 149, Statement of Self-Employment Inco
Page 2 o
PHC 10
September 20
If you or any member of your household has any kind of self-employment income, fill out this form and attach it to yourapplication. You may attach a copy of the latest income tax formsin place of this form. If your accounting system is not the same asthis form, you may substitute a copy of your accountingstatement. You must answer all questions and sign and date atthe bottom. Use additional sheets of paper if you need to.
Sign and date each sheet. Remember, this is your swornstatement. You will need to bring with you to the interview: bills,receipts, checks or stubs, and any other business records youhave. Your worker will need to see them. Your records will be
returned to you.
Self-employment Income. This is any money you earn workingfor yourself. It is not money you earn working for someone else. Ifyou are in doubt, ask your caseworker.
Questions 1, 2, and 3. These questions are self-explanatory.
Question 4. List your business income and expenses. In theboxes on the left side of the form, list your business expenses (see the information below). Write in the dates you paid theexpenses and the amount of each expense. Add the amounts,and enter your total in the box "total self-employment expenses."In the boxes on the right side of the form, list your income (seethe information below). List the dates you received the income,your sources of income, and the amounts. Add the amounts, andenter your total in the box "total self-employment income."Subtract your expenses from your total self-employment income,and enter your "net self-employment income."
Expenses are your costs of doing business. Examples ofexpenses are supplies, repairs, rent, utilities, seed, feed, businessinsurance, licenses, fees, payments on principal of loans forincome-producing property, capital asset purchases (such as realproperty, equipment, machinery, and other durable goods andcapital asset improvements), your social security contribution forpeople who worked for you, and labor (not salaries you payyourself). If you claim labor costs, list each person and the
amount you paid them. If you have any other kinds of businessexpenses, be sure to list them and the date they were paid.
You may not claim:• Rent, mortgage, taxes, or utilities on your business if it
operates out of your home (unless these costs are separatefrom the costs of your home);
• Cost of goods you buy for the business but use yourself;• Net business loss from a prior period and• Depreciation.
If you are in doubt, bring proof of the expense and ask yourworker.
Income includes money from sales, cash receipts, crops,commissions, leases, fees, or whatever you do or sell for money.If you have any other kind of income from your business, be sureto list it. Be sure to list the dates income was received.
Who must sign. The form must be signed by the applicant,spouse, or authorized representative. Anyone may help youcomplete the form, but that person must also sign and date theform. Ask your worker if anyone else needs to sign the form.
Si usted u otra persona de su casa tiene algún tipo de ingresos de negociopropio, llene esta forma y adjúntela a su solicitud. En lugar de esta forma,puede adjuntar una copia de la declaración de impuestos sobre ingresosmás reciente. Si el sistema de contabilidad que usa no es igual al de estaforma, puede substituir la forma con una copia de su registro decontabilidad. Tiene que contestar todas las preguntas y firmar y fechar laforma al final. Use hojas adicionales si las necesita. Firme y feche cadahoja. Recuerde que ésta es una declaración jurada. Tiene que llevar a laentrevista: cuentas, recibos, cheques o talones de cheques y cualquier otradocumentación que tenga del negocio. El trabajador tendrá que verlos.Estos documentos le serán devueltos.
Ingresos del Negocio Propio. Este término se refiere al dinero que ganacuando trabaja por su propia cuenta. No es el dinero que recibe cuandotrabaja para otra persona. Si tiene alguna duda, consulte con sutrabajador de casos.
Preguntas 1, 2, y 3. Estas preguntas no necesitan más explicación.
Pregunta 4. Apunte los ingresos y gastos de su negocio. En las cajas dellado izquierdo de la forma, enumere los gastos de su negocio (vea lainformación abajo). Ponga la fecha en que pagó los gastos y la cantidadde cada gasto. Sume las cantidades y ponga el total en la caja que dice"total de gastos del negocio propio". En las cajas a la derecha de laforma, enumere los ingresos (vea la información abajo). Ponga la fechaen que recibió cada ingreso, la fuente del ingreso y la cantidad. Sume lascantidades y ponga el total en la caja que dice "total de ingresos delnegocio propio". Reste los gastos del total de ingresos del negocio propioy anote sus "ingresos netos del negocio propio".
Los gastos son los costos de un negocio. Algunos ejemplos de posiblesgastos son: provisiones, reparaciones, renta, servicios públicos, semilla,forraje, seguro del negocio, licencias, cuotas, pagos del capital depréstamos para propiedades que generan ingresos, compras de bienes decapital (como bienes raíces, equipo, maquinaria y otros bienes duraderos ymejoras de bienes de capital), su aportación al seguro social de laspersonas que trabajan para usted y sueldos (pero no los que se paga a símismo). Si declara el costo de sueldos, ponga el nombre de cada personay la cantidad que le pagó a cada quien. Si tiene cualquier otro tipo degastos del negocio, asegúrese de anotarlos y poner la fecha en que lospagó.
No puede declarar:• El pago de la renta, la hipoteca, los impuestos o los servicios públicos
del negocio si lo opera de su casa (a no ser que estos costos son apartede los costos de la casa);
• El costo de artículos que compra para el negocio pero que usapersonalmente;
• La pérdida neta del negocio de un periodo anterior; and• La depreciación.
Si tiene alguna duda, lleve comprobantes del gasto y consulte con eltrabajador.
Los ingresos son, entre otros, el dinero de ventas, el ingreso de caja, lascosechas, las comisiones, las rentas, las cuotas o cualquier cosa que haceo que vende por dinero. Si usted tiene cualquier otro tipo de ingresos delnegocio, asegúrese de anotarlo. No olvide poner las fechas en que recibióel ingreso.
Quién debe firmar. El solicitante, su cónyuge o su representante autorizadpara firmar la forma. Cualquier persona puede ayudarle a llenar la formpero esa persona también tiene que firmar y poner le fecha en la formaConsulte con el trabajador para saber si alguien más tiene que firmar.
With a few exceptions, you have the right to request and be informed about the information that the county obtains about you. You are entitled to receive review the information upon request. You also have the right to ask the county to correct information that is determined to be incorrect (Government CSections 552.021, 552.023, 559.004). To find out about your information and your right to request correction, please contact your local county office. / Con alguexcepciones, usted tiene el derecho de saber qué información obtiene sobre usted el condado de pedir dicha información. Si desea recibir y estudiar la información, tienderecho de solicitarla. También tiene el derecho de pedir que el condad corrija cualquier información incorrecta (Código Gubernamental, Secciones 552.021, 552.0559.004). Para enterarse sobre la información y el derecho de pedir que la corrijan, favor de ponerse en contacto con la oficina local del condado.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 81/92
FORM 200
PHC - 200 MONTHLY REPORTING FORM
Report or Amended
Contractor: ____________________________________ Report for (Month/Year) ______
Location: ____________________________________
Phone number: _________________________________
I. TOTAL NUMBER OF UNDUPLICATED CLIENTS DETERMINED ELIGIBLE AND
PROVIDED A PRIMARY CARE SERVICE: ______________ (must match # in Box #20 of voucher)
TOTAL NUMBER OF INELIGIBLE APPLICANTS:_______________
II. COSTS OF PHC FUNDED SERVICES DURING THIS REPORTING MONTH
Diagnostic and Treatment 1
Emergency Services 2
Family Planning Services 3
Preventive Health Services 4
Health Education Services 5
Laboratory/X-Ray Services 6
PHC 08-2September 2008
Nutrition 7
Health Screening 8
Dental 9
Transportation 10
Prescription Drugs 11
Social Services 12
Other Optional Services 13
Administrative Costs 14
Total (1 - 14= 15)(Amount of Requested Reimbursement) 15 -$
Signature of Person Submitting Form Date
PHC 08-2September 2008

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 82/92
FORM 200AMonthly ReportINSTRUCTIONS
PHC 11-1February 2011
PURPOSE Use to provide information to DSHSabout: PHC caseload and
Contractor’s expenditure levels by
PHC service.
PROCEDUREForm 200 must be completed andsubmitted to DSHS PCG in Austin within5 working days of the month following thereport month.
Fax or email Form 200 to DSHS PCGat 512/458-7713 /([email protected] )
DETAILED INSTRUCTIONSGeneral Information:Contractor: Name of contractor on DSHScontractReport or Amended Report: Enter monthand year the expenditures are spent/paid.
Any amendments to a report should bemarked “Amended” and submitted onthe Form 200. The amended item(s)should be circled.
I. Caseload Data.
Total number of unduplicated clients served. Enter the total number of alleligible individuals that were providedany of the six priority and/or optionalservices (i.e. presumptive, full-service,supplemental). Regardless of the numberof PHC services or visits, only count theindividual once. DO NOT count thatindividual again during the report monthor in any other month the remainder ofthe fiscal year. If an eligibility
determination was made, but no PHCservice was given, do not count until aPHC service is provided. This numbermust match number reported on voucher.
Total number of ineligible applicants: Enter the total number of individuals weredetermined ineligible for PHC services.
II. Cost of Services During Month: Enterthe dollar amount spent/paid in thecalendar report month for each of thecategories in Items 1-14. List only expenditures that are applicable to
DSHS PHC funds and services.
Item 1-13 enter costs for providing theservices associated with providing directpatient care; costs may include salaries ofindividuals providing healthcare services,medical supplies and equipment,contractor costs, etc.
Item 2 enter costs associated withproviding emergency services, however,DO NOT count costs associated withhospital emergency room costs.
Item 3 enter costs associated withpregnancy tests, physicals, contraceptive,etc.
Item 4 enter costs associated withimmunizations, annual Pap smears, routineeye exams, etc.
Item 5 enter associated with any othercosts such as, education materials, etc.
Item 6 same as noted in item 1.
Item 7-13 enter the costs associated witheach service.
Item 14 administrative costs may includecosts not associated with direct patientcare, such as salaries for non-healthcareindividuals, administrative supplies,screening and eligibility and other costs notlisted in Items 1-13.
Item 15 enter the total of 1-14. The Total
costs listed in Item 15 should equal thetotal requested reimbursement amount onthe monthly voucher. (See PHC State ofTexas Purchase Voucher {FORM B-13}.)

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 83/92
FORM 300
September 2011
Contractor Name:
Contact Name
Contact Phone:
Fiscal Year
Age Number of Males Number of Females
0 to 17 years
18 – 64 years65 years +
TOTAL 0 0
Race Number Served
White
Black or African American
American Indian or Alaska Native
Asian
Native Hawaiian or Pacific IslanderUnknown
TOTAL 0
Ethnicity Number Served
Hispanic or Latino
Not Hispanic or Latino
TOTAL 0
Citizenship Number ServedUS Citizens or legal Residents
Non-citizens
TOTAL 0
2. Number of unduplicated DSHS PHC clients served by age and gender:
3. Number of unduplicated DSHS PHC clients served by race/ethnici ty:
4. Number of unduplicated DSHS PHC clients served by ci tizenship:
PRIMARY CARE ANNUAL REPORT
1. Total number of unduplicated DSHS PHC clients served this fiscal year: _______

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 84/92
FORM 300
September 2011
5. Number of unduplicated DSHS PHC clients served according to income levels based on Federal
Poverty Level (FPL):
Percent of FPL Number Served
150 - 101%
100 - 51%50 - 22%
21 - 0%
TOTAL 0
Services Number Served
Full-services
Presumptive services only
Supplemental services
TOTAL 0
7. a. Number of counties in DSHS PHC service area:
County Name Number of Clients
1
2
3
4
5
6. Number of undupli lcated DSHS PHC clients by type of service:
7. b. Number of unduplicated DSHS PHC eligible clients served by county of residence:
8. List the top five diagnoses of unduplicated DSHS PHC clients:

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 85/92
FORM 300
September 2011
If the FY 12 Performance Measure was not met, provide an explanation.
9. List the number of undupl icated clients to be served on the FY 12 Contract Performance Measure
____________.
10. Program accomplishments: In narrative form, highlight accomplishments of your DSHS PHC
project in providing primary health care sevices to unduplicated PHC clients during this fiscal year.

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 86/92
FORM 300APHC-300 Annual Report
INSTRUCTIONS
September 2011
PURPOSE Use to provide information to TDSHS about:
• PHC demographic information
PROCEDURE
Form 300 must be completed and submitted toTDSHS PHC in Austin by the 60th
day of thefollowing fiscal year.
Fax the Form 300 to PCG at 512/776-7713
or email
DETAILED INSTRUCTION
Item 1: Enter the total number of unduplicatedPHC clients who received a PHC service thisyear. Do not count individuals more than
once regardless of the number visits orservices.
Item 2: Enter the total unduplicated clientcount served by age and gender.
Item 3. List the total unduplicated client count
served by race and by ethnicity. The“unknown” category is for those clients who
did not specify or no information is available.The total for race should equal the total forethnicity.
Item 4. List the total unduplicated client count
served by citizenship status. U.S. citizens or Legal Residents are born in the U.S. or have
documentation for legal residency at the timeservices are provided. Non-citizens are those
individuals not born in the U.S. and have nodocumentation of legal residency. ( Acceptself declaration as listed on the Screening and
Eligibility Application.)
Item 5. List the total unduplicated client countby poverty level.
Item 6. List the total unduplicated client countby PHC eligibility status. Full-service = PHC
Clients with no other payment source;Supplemental = clients that have another
source of payment; and Presumptive =Individuals receiving immediate PHC services
but are potentially eligible for another paymentsource such as Medicaid, Medicare, etc. Only count these individuals in one of the above
eligible categories.
NOTE: The number listed under TOTAL
in 1, 2, 3, 4, 5, and 6 should be the same
number. Each total should equal theunduplicated client count as listed in Item 1.
Item 7: List the counties that are in yourproject’s service area. Next to county name,
list the number of PHC clients servedaccording their county of residence. The total
number of clients served for all countiesshould equal the unduplicated client count in
Item 1.
Item 8: List the top five health care problems
most frequently encountered, with numberone being the most frequent.
Item 9. Provide the number of unduplicatedDSHS clients that were listed for FY 12contract performance measure. If you wereunable to serve the number listed, pleaseprovide an explanation.
Item 10: Write a summary of PHC programobjectives or accomplishments achieved inthe fiscal year.
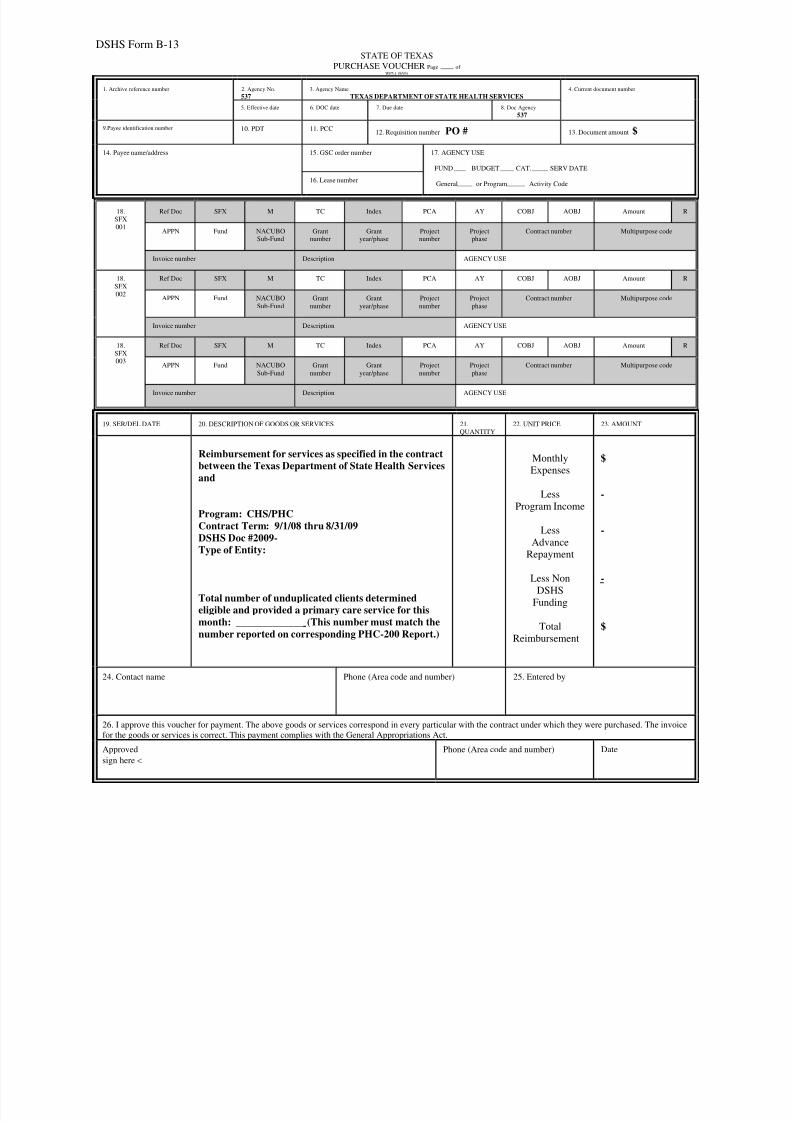
8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 87/92
DSHS Form B-13
STATE OF TEXAS
PURCHASE VOUCHER Page of WP5.1 (9/93)
1. Archive reference number 2. Agency No.
537
3. Agency Name
TEXAS DEPARTMENT OF STATE HEALTH SERVICES
4. Current document number
5. Effective date 6. DOC date 7. Due date 8. Doc Agency
537
9.Payee identification number 10. PDT 11. PCC12. Requisition number PO # 13. Document amount $
14. Payee name/address 15. GSC order number 17. AGENCY USE
FUND BUDGET CAT. SERV DATE
General or Program Activity Code16. Lease number
18.
SFX
001
Ref Doc SFX M TC Index PCA AY COBJ AOBJ Amount
APPN Fund NACUBOSub-Fund
Grantnumber
Grantyear/phase
Projectnumber
Projectphase
Contract number Multipurpose code
Invoice number Description AGENCY USE
18.
SFX
002
Ref Doc SFX M TC Index PCA AY COBJ AOBJ Amount
APPN Fund NACUBO
Sub-Fund
Grant
number
Grant
year/phase
Project
number
Project
phase
Contract number Multipurpose code
Invoice number Description AGENCY USE
18.
SFX
003
Ref Doc SFX M TC Index PCA AY COBJ AOBJ Amount
APPN Fund NACUBO
Sub-Fund
Grant
number
Grant
year/phase
Project
number
Project
phase
Contract number Multipurpose code
Invoice number Description AGENCY USE
19. SER/DEL DATE 20. DESCRIPTION OF GOODS OR SERVICES 21.
QUANTITY
22. UNIT PRICE 23. AMOUNT
Reimbursement for services as specified in the contractbetween the Texas Department of State Health Services
and
Program: CHS/PHCContract Term: 9/1/08 thru 8/31/09DSHS Doc #2009-Type of Entity:
Total number of unduplicated clients determinedeligible and provided a primary care service for thismonth: _____________ (This number must match the
number reported on corresponding PHC-200 Report.)
Monthly
Expenses
Less
Program Income
Less
Advance
Repayment
Less Non
DSHS
Funding
Total
Reimbursement
$
-
-
-
$
24. Contact name Phone (Area code and number) 25. Entered by
26. I approve this voucher for payment. The above goods or services correspond in every particular with the contract under which they were purchased. The invoi
for the goods or services is correct. This payment complies with the General Appropriations Act.
Approved
sign here <
Phone (Area code and number) Date

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 88/92
DSHS Form B-13
STATE OF TEXAS EXAMPLE ONLY
PURCHASE VOUCHER Page of WP5.1 (9/93)
1. Archive reference number 2. Agency No.
537
3. Agency Name
TEXAS DEPARTMENT OF STATE HEALTH SERVICES
4. Current document number
5. Effective date 6. DOC date
Submit Date7. Due date 8. Doc Agency
537
9.Payee identification number
1234567890123410. PDT 11. PCC
12. Requisition number PO #0000123456 13. Document amount $12,345.67
14. Payee name/address
Contractor Agency NameStreet/P.O. Box Address as set up with ComptrollerCity, State 12345-1234
15. GSC order number 17. AGENCY USE
FUND BUDGET CAT. SERV DATE
General or Program Activity Code16. Lease number
18.
SFX
001
Ref Doc SFX M TC Index PCA AY COBJ AOBJ Amount
APPN Fund NACUBO
Sub-Fund
Grant
number
Grant
year/phase
Project
number
Project
phase
Contract number Multipurpose code
Invoice number Description AGENCY USE
18.
SFX
002
Ref Doc SFX M TC Index PCA AY COBJ AOBJ Amount
APPN Fund NACUBO
Sub-Fund
Grant
number
Grant
year/phase
Project
number
Project
phase
Contract number Multipurpose code
Invoice number Description AGENCY USE
18.
SFX
003
Ref Doc SFX M TC Index PCA AY COBJ AOBJ Amount
APPN Fund NACUBO
Sub-Fund
Grant
number
Grant
year/phase
Project
number
Project
phase
Contract number Multipurpose code
Invoice number Description AGENCY USE
19. SER/DEL DATE 20. DESCRIPTION OF GOODS OR SERVICES 21.
QUANTITY
22. UNIT PRICE 23. AMOUNT
Month & Year of services
Reimbursement for services as specified in the contractbetween the Texas Department of State Health Services
and (Contractor Agency Name).
Program: CHS/PHCContract Term: 9/1/08 thru 8/31/09DSHS Doc #2009-123456-123Type of Entity: University, Gov, Non-Profit, etc
Total number of unduplicated clients determinedeligible and provided a primary care service for thismonth . (This number must match the
number reported on corresponding PHC-200 Report.)
Monthly
Expenses
Less
Program Income
Less
Advance
Repayment
Less Non
DSHS
Funding
Total
Reimbursement
$12,895.67
- 300.00
- 0.00
- 250.00
$12,345.67
24. Contact name
Person to be contacted when questions arisePhone (Area code and number)
Contact person’s phone andextension
25. Entered by
26. I approve this voucher for payment. The above goods or services correspond in every particular with the contract under which they were purchased. The invoi
for the goods or services is correct. This payment complies with the General Appropriations Act.
Approved
sign here <
Phone (Area code and number) Date
8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 89/92
4:43 PM Page 1
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
B C D E F
Contractor Name: DSHS Program:
Payee Name:
Address:
Address:
City, ST, Zip: from: to:
Payee Vendor ID No.:
Final Report?
PO Number:
BUDGET APPROVED CURRENT PERIOD CUMULATIVE BUDGET BALANCE
CATEGORIES BUDGET Col 1 Col 2 Col 3
SALARIES -$
FRINGE BENEFITS -
TRAVEL -
EQUIPMENT -
SUPPLIES -
CONTRACTUAL -
OTHER -
SUB-TOTAL -$ -$ -$ -$
INDIRECT -
TOTAL -$ -$ -$ -$
-
-
SUBTOTAL: DSHS SHARE -
-$ -$ -$
-$
Prepared by:
Title: Telephone #:
Telephone #:
Fax #:
Date Submitted:
FSR Receipt Date:
NON-DSHS FUNDING
Contract Term: ( Month / Day / Year ):
Name of Authorized Certifying Official:
Title of Certifying Official:
CERTIFICATION: I certify to the best of my knowledge and belief that this report is correct and complete a
that all outlays and unliquidated obligations are for the purposes set forth in the award documents.
DEPARTMENT OF STATE HEALTH SERVICES
FINA NCIAL STATUS REPORT
Form 269A
DSHS Document # Year Attachment #
1100 West 49th Street Austin, Texas 78756-3
REIMBURSEMENTS (net of advances)
ADVANCE:
Received (Col1) - Repaid (Col 2) = Balance Owed (Col 3)
Period Covered by this Report:
LESS: PROGRAM INCOME
Cash Accrual
9/2/2010 33-Financial Status Report 269a

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 90/92
APPENDICES
8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 91/92
September 2011
The Primary Health Care Program may be contacted at:
Texas Department of State Health ServicesCommunity Health Services
Primary Care Group
1100 West 49
th
StreetAustin, Texas 78756-3168Phone: (512) 776-7111Fax: (512) 776-7713
www.dshs.state.tx.us/phc Jan Maberry, Group Manager(All aspects of the Program)Ext: 7728E-mail: [email protected]
Gina Baber, Program Specialist(Program Lead )Ext: 2023E-mail: [email protected]
Carolyn Wachel, Program Specialist(Policy, Desk Reviews and Reports))Ext: 2141E-mail: [email protected]
Karen Gray, Program Specialist(PHC Eligibility Training)Ext: 2752E-mail: [email protected]
Sheila Rhodes, RN(Region 1 – Contract Coordinator)Phone: (806) 783-6485 / Fax: (806)783-6435E-mail: [email protected]
Jamie Moore, RN(Region 1 – Contract Coordinator)Phone: (806) 655-7151 X1113 / Fax: (806) 655-7159E-mail: [email protected]
Laticcia Riggins(Region 2/3 – Contract Coordinator)Phone: (817) 264-4658 / Fax: (817)264-4555E-mail : [email protected]
Jim Conditt, Program Specilaist(Policy and Desk Reviews)Ext: 3529E-mail: [email protected]
Chrysanne Randal, RN(Region 2/3 – Contract Coordinator)Phone: (940) 888-8019 / Fax: (940) 888-3364E-mail: [email protected]
Lucille Coggins, RN(Region 2/3 – Contract Coordinator)Phone: (817) 573-8186 / Fax: (817) 578-3310E-mail: [email protected]
Della Mendez(Region 4/5N – Contract Coordinator)Phone: (903) 533-5334 / Fax: (903) 533-5367E-mail: [email protected]
Waseem Ahmed(Region 6/5S – Contract Coordinator)Phone: (713) 767-3011 / Fax: (713)767-3408E-mail: [email protected]
Ngozi Adimora, RN
(Region 6/5S – Contract Coordinator)Phone: (713) 767-3014 / Fax: (713) 767-3408E-mail: [email protected]
Chesca Thurman
(Region 7 – Contract Coordinator)Phone: (254) 771-6764 / Fax: (254) 778-6819E-mail: [email protected]

8/2/2019 Phc Manual
http://slidepdf.com/reader/full/phc-manual 92/92
APPENDIX B
RESOURCES
DSHS Standards and Policy
More information on department-wide standards and policy for contractors maybe found on the Quality Management Branch website:
http://www.dshs.state.tx.us/qmb/default.shtm
Enabling Legislation
Enabling PHC legislation and Texas Administrative Code Rules may be found atthe following web site locations:
Texas Administrative Code:http://info.sos.state.tx.us/pls/pub/plsql/readtac$ext.ViewTAC?tac_view=4&ti=25&pt=1&ch=39
Texas Health and Safety Code:http://www.capitol.state.tx.us/statutes/hs.toc.htm

















