37 Philippine College of Chest Physicians Officers and Board of Trustees President Vice President Secretary Treasurer Board Members Immediate Past President 84-A Malakas St., Barangay Pinyahan, Quezon City Telephone Nos.: 924-9204, 927-0343 Telefax: 924-0144 E-mail: [email protected]Website: http://www.philchest.org Marilyn Ong-Mateo, M.D., FPCCP Renato B. Dantes, M.D., FPCCP Mario Joselito M. Juco, M.D., FPCCP Gracita Rigonan-Ramos, M.D., FPCCP Abundio A. Balgos, M.D., FPCCP Sylvia Banal-Yang, M.D., FPCCP Charles Y. Yu, M.D., FPCCP Ma. Encarnita Blanco-Limpin, M.D., FPCCP Isagani C. Rodriguez, M.D., FPCCP Rodolfo Roman T. Bigornia, M.D., FPCCP Contributors Chairperson, 1998-2004 Project Chairman Project Secretary Dina V. Diaz, M.D., FPCCP Tito C. Atienza, M.D., FPCCP Eloisa S. de Guia, M.D., FPCCP Glen Elmer I. Alvarado, M.D., FPCCP Eileen G. Aniceto, M.D., FPCCP Roberto A. Barzaga, M.D., FPCCP Ma. Elizabeth V. Cadena, M.D., FPCCP Manuel C. Jorge II, M.D., FPCCP Isaias A. Lanzona, M.D., FPCCP Ma. Theresa C. Magtibay, M.D., FPCCP Ma. Piedad R. Natividad, M.D., FPCCP Josephine B. Ramos, M.D., FPCCP Camilo C. Roa Jr., M.D., FPCCP Ma. Bella R. Siasoco, M.D., FPCCP Aileen D. Wang, M.D., FPCCP Jennifer M. Wi, M.D., FPCCP Sylvia B. Yang, M.D., FPCCP Ricardo C. Zotomayor, M.D., FPCCP
Dina V. Diaz, M.D., FPCCPTito C. Atienza, M.D., FPCCPEloisa S. de Guia, M.D., FPCCP
Glen Elmer I. Alvarado, M.D., FPCCPEileen G. Aniceto, M.D., FPCCP
Roberto A. Barzaga, M.D., FPCCPMa. Elizabeth V. Cadena, M.D., FPCCP
Manuel C. Jorge II, M.D., FPCCPIsaias A. Lanzona, M.D., FPCCP
Ma. Theresa C. Magtibay, M.D., FPCCPMa. Piedad R. Natividad, M.D., FPCCP
Josephine B. Ramos, M.D., FPCCPCamilo C. Roa Jr., M.D., FPCCP
Ma. Bella R. Siasoco, M.D., FPCCPAileen D. Wang, M.D., FPCCPJennifer M. Wi, M.D., FPCCPSylvia B. Yang, M.D., FPCCP
Ricardo C. Zotomayor, M.D., FPCCP
ASthmA CPm 8th EDItION
38
Consultant Panel of Reviewers/Advisers
Fernando G. Ayuyao, M.D., FPCCPRodolfo M. Carungin, M.D., FPCCP
Renato B. Dantes, M.D., FPCCPTeresita S. de Guia, M.D., FPCCP
Tiburcio A. Leonin, Jr., M.D., FPCCPMadeleine W. Sumpaico, M.D., FPSAI
Charles Y. Yu, M.D., FPCCP
Asthma Council, 2004
Tito C. Atienza, M.D., FPCCP, Chairman, 2004-presentGlen Elmer I. Alvarado, M.D., FPCCP
Eileen G. Aniceto, M.D., FPCCPRoberto A. Barzaga, M.D., FPCCP
Ma. Theresa H. Bernardo, M.D., FPCCPMa. Elizabeth V. Cadena, M.D., FPCCP
Eloisa S. de Guia, M.D., FPCCPChristine Marie A. dela Cruz, M.D., FPCCP
Dina V. Diaz, M.D., FPCCPRaymond F. Diga, M.D.Anderson U. Dy, M.D.
Joven Roque V. Gonong, M.D.Malbar G. Ferrer, M.D., FPCCP
Renato B. Herradura, M.D., FPCCPFidelinda E. Ilano, M.D.
Manuel C. Jorge II, M.D., FPCCPIsaias A. Lanzona, M.D., FPCCP
Ma. Theresa C. Magtibay, M.D., FPCCPLalaine L. Mortera, M.D.
Ma. Piedad R. Natividad, M.D., FPCCPOgee Mer A. Panlaqui, M.D.
Rosemarie R. Pingol, M.D., FPCCPJosephine B. Ramos. M.D., FPCCPRhoderick Ian Reyes, M.D., FPCCP
Camilo C. Roa Jr., M.D., FPCCPMa. Bella R. Siasoco, M.D., FPCCP
Rollin P. Tabuena, M.D.Cynthia R. Talla, M.D., FPCCPAileen D. Wang, M.D., FPCCPJennifer M. Wi, M.D., FPCCPSylvia B. Yang, M.D., FPCCP
Ricardo C. Zotomayor, M.D. FPCCP
CPm 8th EDItION ASthmA
39
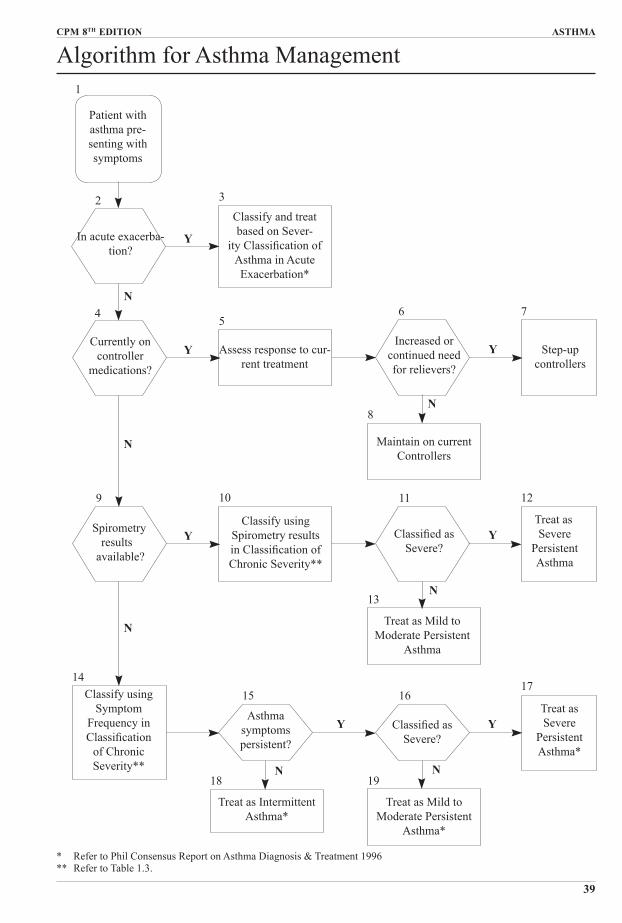
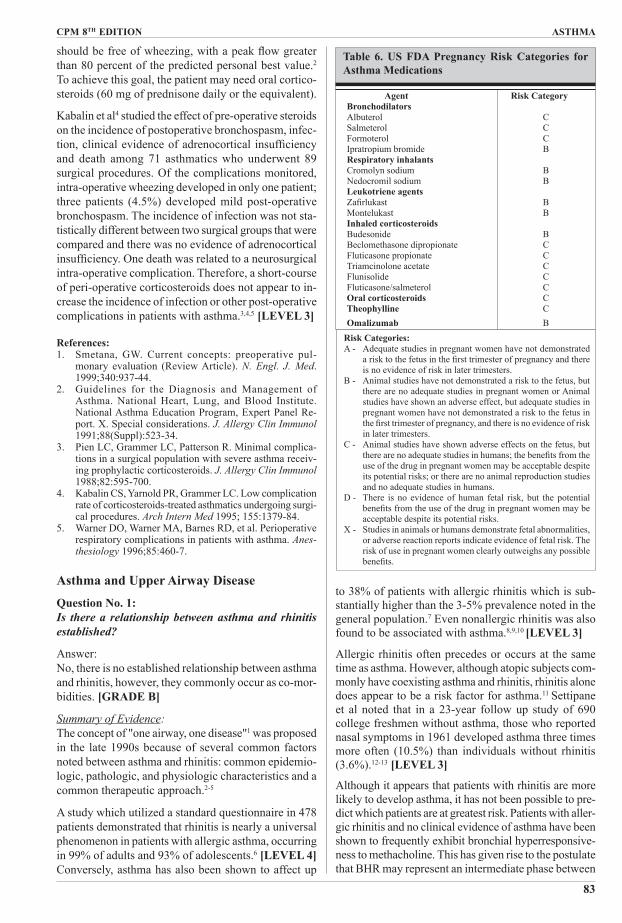
algorithm for Asthma Management
Patient with asthma pre-senting with symptoms
In acute exacerba-tion?
Currently on controller
medications?
Spirometry results
available?
Classify and treat based on Sever-
ity Classification of Asthma in Acute Exacerbation*
Assess response to cur-rent treatment
Increased or continued need for relievers?
Step-up controllers
Classify using Symptom
Frequency in Classification
of Chronic Severity**
Classify using Spirometry results in Classification of Chronic Severity**
Classified as Severe?
Treat as Severe
Persistent asthma
Maintain on current Controllers
Treat as Mild to Moderate Persistent
asthma
asthma symptoms persistent?
Classified as Severe?
Treat as Severe
Persistent Asthma*
Treat as Mild to Moderate Persistent
Asthma*
Treat as Intermittent Asthma*
1
2 3
45
6 7
8
9 10 11 12
13
1415 16
17
18 19
Y
Y
Y
Y
Y
Y Y
N
N
N
N
N
N N
* Refer to Phil Consensus Report on Asthma Diagnosis & Treatment 1996** Refer to Table 1.3.
ASthmA CPm 8th EDItION
40
Philippine Consensus Report on Asthma 2004Chapter 1Epidemiology, Diagnosis and Classification of AsthmaQuestion No. 1:Is asthma a common condition worldwide?
Answer:Yes, asthma is a common disease worldwide and, over the past two decades, is showing an increasing trend for all ages, sex, and racial groups.
Summary of Evidence:In 1995, the International Study of Asthma and Allergies in Children (ISAAC) conducted Phase I of a worldwide study to describe the prevalence and severity of asthma, rhinitis, and eczema among school children. One hundred fifty five centers in 56 countries participated, including the Philippines.1 More than 450,000 children were interviewed using a one-page written questionnaire or a video asthma questionnaire. The study showed that the prevalence of asthma symptoms in children varied greatly in different populations with differences ranging between 20- and 60-fold. The highest prevalence was found from centers in the United Kingdom, Australia and New Zealand.2,3
Prevalence of asthma is increasing by 4% each year.4 In the United States, the prevalence of asthma cases was noted to be increasing since the early 1980s for all ages, sex, and racial groups.5,6 The prevalence is higher among children than adults and higher among blacks than whites. In the general population, the prevalence of asthma is higher among females, however, in children, the prevalence is higher among males. Furthermore, the prevalence among impoverished inner city children has been much higher.7,8
References: 1. Asher MI, Keil U, Anderson HR, et al. International Study
of Asthma and Allergies in Childhood (ISAAC): rationale and methods. Eur. Respir J. 1995;8:483-91.
2. Asher MI, Anderson HR, Stewart AW, et al. The Inter-national Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Worldwide variations in the prevalence of symptoms of asthma, allergic rhinoc-onjunctivitis and atopic dermatitis: ISAAC. Eur. Respir. J. 1998;12:315-35.
3. Beasley R, Keil U, von Mutius E, Pearce N. ISAAC Steer-ing Committee: Worldwide variations in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis and atopic dermatitis: ISAAC. Lancet. 1998;351:1225-32.
4. Barbers R. Asthma in Y2K and beyond. Curr Opin Pulm. Med. 2000;6:1-3.
5. U.S. Department of Health and Human Services. National Heart, Lung and Blood Institute Data Fact Sheet Asthma Statistics. 1999. Jan.
6. Mannimo DM, Homa DM, Pertowski CA, et al. Surveil-lance for asthma - United States, 1950-1995. MMWR Mortal. Morb. Wkly Rep. 1998;47;1-27.
7. Crain EF, Weiss KB, Bijur PE, Hersh M, Westbrook L, Stein RE. An estimate of the prevalence of asthma and wheezing among inner-city children. Pediatrics. 1994;94:356-62.
8. Persky VW, Slezak J, Contreras A, et al. Relationship of race and socioeconomic status with prevalence, severity, and symptoms of asthma in Chicago school children. Ann. Aller. Asthma Immunol. 1998;81:266-71.
Question No. 2:How common is asthma in the Philippines?
Answer:There are no available nationwide data published on asthma prevalence. However, the limited reports gath-ered showed a prevalence of 12% in children aged 13-14 years and 17-22% in older age groups.
Summary of Evidence:Three thousand two hundred and seven children in Metro Manila aged 13-14 years participated in the ISaaC.1 Participants accomplished a 12-month preva-lence of self-reported asthma symptoms from written questionnaires and from video questionnaires. The results showed that approximately 12% and 8% preva-lence based on responses to the written questionnaire and to the video questionnaire respectively. In a sub-sequent study, 12.3% of the same population reported wheezing.2 [LEVEL 3]A local study estimating the prevalence of asthma and allergies in adults was completed in Malolos, Bulacan in 1998.3 [LEVEL 3] One thousand five (1,005) adults (ages 18-44 years) were interviewed using a pre-tested questionnaire adapted from the European Community Health Survey (ECHRS) and the ISAAC. The study showed a prevalence of 17.2% for asthma and 49.9% for allergy among adults. Another study conducted at the Lung Center of the Philippines reported a prevalence of 22% in adults.4
References:1. Asher MI, Anderson HR, Stewart AW, et al. The Inter-
national Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Worldwide variations in the prevalence of symptoms of asthma, allergic rhinoc-onjunctivitis and atopic dermatitis: ISAAC. Eur. Respir. J. 1998;12:315-35.
2. Beasley R, Keil U, von Mutius E, Pearce N. ISAAC Steer-ing Committee: Worldwide variations in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis and atopic dermatitis: ISAAC. Lancet. 1998;351:1225-32.
3. Cua-Lim F, Roa CC, Pagkatipunan R. Prevalence of adult asthma and allergies in Malolos, Bulacan, Metro Manila, Philippines. Presented as a poster study at the 3rd asian Pacific Congress of Allergology and Clinical Immunology, PICC, Manila, Philippines, 1998. Dec 9-11.
4. Diaz DV. A prevalence survey of asthma in a Filipino population in Metro Manila. Phil. J. Chest Dis. 1996; 4:68-73.
CPm 8th EDItION ASthmA
41
Question No. 3:What is the current concept of asthma as a disease?
Answer:In the last four decades, asthma was considered as predominantly a disease of airway smooth muscle.1,2 However, based on the National Institute of Health (NIH) guidelines in 1997, the understanding of asthma has shifted from a disease of airway smooth muscle to one of airway inflammation.3 This concept of bronchial inflammation arose from studies of bronchial hyper-responsiveness, bronchioalveolar lavage (BAL), bron-chial biopsies and induced sputum from asthmatics, and observations made postmortem of patients who died from asthma.Interestingly, structural abnormalities in the airways have been observed even on patients maintained on anti-inflammatory medications and on those with mild asthma.4,5,6 Evidently, the incessant release of inflam-matory mediators from eosinophils and mast cells results in persistent bronchial inflammation of the airways. Eventually the airways undergo structural abnormalities resulting in the following: fibrosis, increase in mass of smooth muscle and mucus glands,7,8,9 epithelial shed-ding, thickening of the reticular basement membrane,10 and fibronectin deposition in the subepithelial layer.11 Histological sections show thickening of the airway walls by 50-300% of normal.12 These changes in the composition and organization of the cellular and mo-lecular components of the airway wall result in a process called airway remodeling.13 Figure 1 shows a proposed mechanism of airway remodeling.14
Airway remodeling results in the following physiologic
consequences: 1) increase in airway hyperresponsive-ness,15 2) non-reversibility of airway obstruction and residual obstruction after bronchodilator and anti-in-flammatory therapy,4,16 and 3) accelerated decline in FEV1 in a subset of asthmatic patients.14
References: 1. Ciba Guest Symposium: Terminology, definitions and clas-
sifications of chronic pulmonary emphysema and related conditions. Thorax. 1959;14:286-99.
2. American Thoracic Society. Definition and classification of chronic bronchitis, asthma, and pulmonary emphysema. Am. Rev. Respir. Dis. 1962;85:762-8.
3. National Asthma Education and Prevention Program. Expert Panel Report 2: Guidelines for the Diagnosis and Management of Asthma. U.S. Dept of Health, Education, and Welfare. Bethesda, MD: National Institutes of Health; National Heart, Lung, and Blood Institute 1997: NIH Publication No. 97-4051A.
4. Lange P, Parner J, Vestibo J, Schnor P, Jensen G. A 15-year follow-up study of ventilatory function in adults with asthma. N. Engl. J. Med. 1998; 339:1194-200.
5. Urik CS. Outcome of asthma: longitudinal changes in lung function. Eur. Respir. J. 1999; 13:904-18.
6. Roche WR, Beasley R, Williams JH et al. Subepithelial fibrosis in the bronchi of asthmatics. Lancet 1989;1: 520-523.
7. Elias JA. Airway remodeling in asthma: unanswered questions. Am. J. Respir. Crit. Care Med. 2000; 161: S168-S171.
8. O’Hollaren MT. Airway remodeling; where’s the evi-dence? American College of Allergy, Asthma and Immu-nology Annual Meeting 1999.
9. Hossain S, Heard BE. Hyperplasia of bronchial muscle in chronic bronchitis. J Pathol 1970;101:171-84.
10. Roche WR. Inflammatory and structural changes in the small airways in bronchial asthma. Am. J. Respir Crit. Care Med. 1998;157:S191-S194.
12. Jeffrey PK. Remodeling in asthma and chronic obstructive lung disease. Am. J. Respir. Crit. Care Med. 2001;164:S28-S38.
13. Nakano Y, Miller N, King G, et al. Quantitative assessment of airway remodeling using high-resolution CT Chest. 2002;122:271S-275S.
14. Bousquet J, Jeffrey PK, Busse WW, et al. State-of-the-Art: asthma-from bronchoconstriction to airways Inflam-mation and remodelling. Am J Respir Crit Care Med. 2000;161:1720-45.
15. Kips JC, Pauwells RA. Airway wall remodeling: Does it occur and what does it mean? Clin. Exp. Allergy. 1999; 29:1457-66
16. Brown PJ, Greville HW, Finucane KE. Asthma and irreversible airflow obstruction. Thorax. 1984;39:131-136.
Question No. 4:How is asthma diagnosed?
Answer:Asthma is diagnosed using a combination of history, clinical findings and objective measurements of vari-able airflow obstruction and/or bronchial hyperrespon-siveness.However, in some cases, the medical history and physi-cal examination may not be reliable in diagnosing asthma. Furthermore, the physical examination may be normal as asthma symptoms are characteristically episodic. An objective measure is required to diagnose asthma accurately. [GRADE A]
Summary of Evidence:1. Screening Strategiesa. HistoryAsthma should be suspected in any patient who presents with any of the following: (1) cough, which worsens at night; (2) wheeze; (3) difficulty in breathing; and (4) chest tightness.1,2 [LEVEL 1] The diagnostic accuracy increases when more than one symptom is present.3 [LEVEL 3] Diagnosis of asthma is strengthened by the presence of the following: history of temporal waxing and waning of symptoms4 often provoked by exogenous factors such as allergens, irritants, exercise, and virus infections;5 a positive family history;6 and improvement in symptoms from use of anti-asthma medications.7
B. Physical ExaminationThe physical examination of the respiratory system may be normal in patients with asthma. Widespread, high-pitched, musical wheezes are characteristic auscul-tatory findings,2 however, they are not very specific for asthma.8,9,10 [LEVEL 1] The presence of wheezes correlates poorly with the severity of airflow limitation. Some patients with asthma may have normal ausculta-tion but exhibit significant airflow obstruction when measured objectively. A better clinical parameter for severity of airflow obstruction is prolonged forced expi-ratory time of six seconds or more, which correlates well with FEV1 in patients with moderate to severe airway obstruction.11,12 [LEVEL 1]
2. Strategies for Confirmationa. Forced expiratory volume in 1 second (FEV1)Spirometry is useful in documenting airflow obstruc-tion in asthma. Variable airflow obstruction can be documented by a spontaneous variability in FEV1 or by improvement 15 minutes after inhaled ß2-agonist administration. A 12% (at least 200 mL) improvement in FEV1, either spontaneously or after inhalation of a ß2-agonist is considered significant.13,14 [LEVEL 1] a positive test increases the likelihood that a symptomatic patient with baseline airway obstruction has asthma. If the initial test is not significant, asthma can be diagnosed by demonstrating at least a 20% (minimum of 250 mL) increase in FEV1 after one week with or without oral steroids, or after two weeks of inhaled steroids.15,16 [LEVEL 4]
B. Peak Expiratory Flow Rate (PEFR)In the absence of spirometry, home measurement of peak expiratory flow (PEF), incorporating response to inhaled ß2-agonist, may be used to document variable airflow obstruction. PEF variability is computed as the mean percentage difference between the post-bronchodilator evening (p.m.) value and pre-bronchodilator morning (a.m.) value over a period of several weeks. Another method is the minimum morning pre-bronchodilator PEF over 1 week expressed as a percent of the recent best (Min%/Max). A PEF variability of 20% or more is indicative of asthma. [LEVEL 4] PEF measurement is also an important diagnostic tool in the clinic, emer-gency department and hospital. Demonstrating a 20% or greater improvement in PEFR 15 minutes after the administration of 200 to 400 µg inhaled salbutamol or the equivalent may be used as an indicator of asthma.16 [LEVEL 4]The PEFR correlates closely with the FEV1 (r= 0.85).17,18 However, this close correlation speaks more of PEFR as a tool better suited for monitoring rather than for diagnosis. There can be a wide variability when PEFR and FEV1 are compared directly. PEFR is, therefore, best used as an adjunct to and not as a substitute for spirometry.19 [LEVEL4]
C. Airway hyperresponsiveness If asthma is still suspected in subjects with a normal FEV1, excessive bronchial hyperresponsiveness can be documented by performing a methacholine or hista-mine inhalation challenge.20,21[LEVEL 1] The optimal diagnostic value of these challenge tests occurs when the pretest probability of asthma based on symptoms is 30-70%.22 [LEVEL 2] However, a negative broncho-provocation test is more reliable in excluding a diagnosis of asthma.23 The test is usually available only in spe-cialized centers with a competent staff. Presently, local guidelines on the performance, dosing, cut-off values, and interpretations have not been established.
References:1. McFadden ER, Gilbert IA. Asthma. N. Engl. J. Med.
1992;327:1928-37.
CPm 8th EDItION ASthmA
43
2. Li JTC, O’Connel EJ. Clinical evaluation of asthma. Ann. Allergy Asthma Immunol. 1996;76:1-14.
3. Pratter MR, Curley FJ, Dubois J, Irwin RS. Cause and evaluation of chronic dyspnea in a pulmonary disease clinic. Arch. Int. Med. 1989;149:2277-82.
4. Guidotti TL. Consistency of diagnostic criteria for asthma from Laennec (1819) to the National Asthma Education Program (1991). J. Asthma 1994;31:329-38.
6. Sandford, AT, et al. The genetics of asthma. Am J Respir Crit Care Med. 1996;153:1749-65.
7. Hargreave FE, Dolovich J, Newhouse MT. The assessment and treatment of asthma: a conference report. J. Allergy Clin. Immunol. 1990;85:1098-111.
8. Holleman DR and Simel DL. Does the clinical exami-nation predict airflow limitation? J. Am. Med. Assoc. 1995;273:313-19.
9. Straus SE, McAlister FA, Sackett DL, Decks JJ. The accuracy of patient history, wheezing, and laryngeal mea-surements in diagnosing obstructive airway disease. J. Am Med. Assoc. 2000;283:1853-7.
10. Hollerman DR Jr, Simel DL, Goldberg JS. Diagnosis of obstructive airway disease from the clinical examination. J. Gen. Int. Med. 1993:8:63-8.
11. Kern DG, Patel SR. Auscultated forced expiratory time as a clinical and epidemiologic test of airway obstruction. Chest. 1991;100:636-9.
12. Schapira RM, Schapira MM, Funahashi A et al. The value of the forced expiratory time in the physical diag-nosis of obstructive airways disease. J. Am. Med. Assoc. l993;270:731-6.
13. Crapo RO. Pulmonary function testing. N. Engl. J. Med. 1994;331:25-30.
14. Becklake M, Crapo RO, Buist AS, et al. Lung function testing: selection of reference values and interpretative strategies. Official Statement of the American Thoracic Society. Am. Rev. Respir. Dis. 1991;144:1202-18.
15. British Thoracic Society. Guidelines for the management of asthma in adults: I. Chronic persistent asthma. Br. Med. J. 1990; 301:651-3.
16. Boulet LP (Chairman) for Summary of Recom mendations
from the Canadian Asthma Consensus Report, CMAJ-JAMC. 1999;161 (11 Suppl) S1-S12.
17. Quanjer PH, Lebowitz MD, Gregg I, Miller MR, Pederson OF. Peak expiratory flow: conclusions and recommendations of a Working Party of the European Respiratory Society. Eur. Respir. J. 1997;24 Suppl: 2S-8S.
18. Connelly CK, Chan NS. Relationship between different measurements of respiratory function in asthma. Res-piration. 1987;52:22-33.
19. Nowak RM, Pensler MI, Sarkar DD, etal. Comparison of peak expiratory flow and FEV1 admission criteria for acute bronchial asthma. Ann. Emerg. Med. 1982; 11: 64-9.
20. Li JC. Do peak flow meters lead to better asthma control? J. Respir Dis. 1995;16:381-98.
21. Adelroth E, Hargreave FE, Ransdale EH. Do physicians need objective measurements to diagnose asthma? Am. Rev. Respir. Dis. 1986;134:704-7.
22. American Thoracic Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. Guidelines for methacholine and exercise challenge testing-1999. Am. J. Respir. Crit. Care Med. 2000; 161; 309-29.
23. Perpiña M, Pellicer C, de Diego A, Compte L, and Maclan V. Diagnostic value of the bronchial provocation test with methacholine in asthma. Chest. 1993; 104:149-54.
Question No. 5:How is asthma classified?
Answer: Asthma can be classified according to: 1) etiology, and 2) severity (clinical condition on presentation whether the patient is in acute state or in a chronic state).1
a. EtiologyClassification of asthma according to etiology is limited as no environmental cause can be identified. However, a rigorous search for a specific environmental cause should be part of the initial clinical assessment. Identifi-
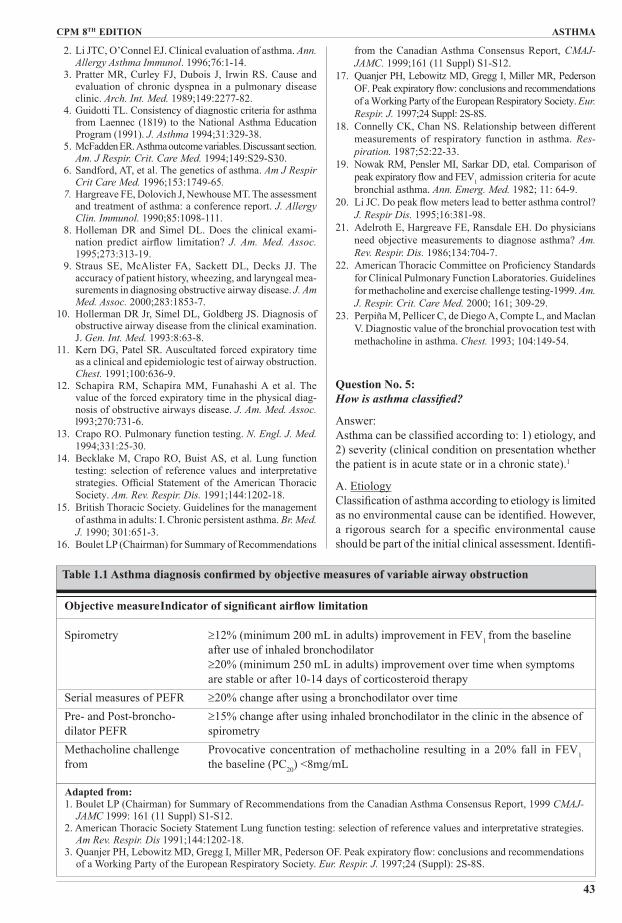
Objective measure Indicator of significant airflow limitation
Spirometry ≥12% (minimum 200 mL in adults) improvement in FEV1 from the baseline after use of inhaled bronchodilator ≥20% (minimum 250 mL in adults) improvement over time when symptoms are stable or after 10-14 days of corticosteroid therapySerial measures of PEFR ≥20% change after using a bronchodilator over timePre- and Post-broncho- ≥15% change after using inhaled bronchodilator in the clinic in the absence of dilator PEFR spirometryMethacholine challenge Provocative concentration of methacholine resulting in a 20% fall in FEV1 from the baseline (PC20) <8mg/mL
Table 1.1 Asthma diagnosis confirmed by objective measures of variable airway obstruction
Adapted from:1. Boulet LP (Chairman) for Summary of Recommendations from the Canadian Asthma Consensus Report, 1999 CMAJ-
JAMC 1999: 161 (11 Suppl) S1-S12.2. American Thoracic Society Statement Lung function testing: selection of reference values and interpretative strategies.
Am Rev. Respir. Dis 1991;144:1202-18.3. Quanjer PH, Lebowitz MD, Gregg I, Miller MR, Pederson OF. Peak expiratory flow: conclusions and recommendations
of a Working Party of the European Respiratory Society. Eur. Respir. J. 1997;24 (Suppl): 2S-8S.
ASthmA CPm 8th EDItION
44
cation of the specific etiology will guide both the physi-cian and the patient on the use of avoidance strategies in management.
B. SeverityAcute state (in exacerbation)For the physician, the initial step is to recognize decisive-ly if the patient is in acute exacerbation. Such exacerba-tion can be fatal if not treated appropriately.2 It is impor-tant to emphasize that any patient with chronic asthma, however mild, may have an acute exacerbation. Any patient, even with mild symptoms, should be considered as having an asthma exacerbation if there is: 1) history of life threatening acute attacks; 2) hospitalization within the previous year; 3) psychosocial problems; 4) history of intubation for asthma; 5) recent reductions or cessa-tion of glucocorticosteroid therapy; and 6) noncompli-ance with recommended medical therapy. These clinical conditions are associated with a higher risk of asthma mortality.3 Since acute exacerbation demands an urgent need to intervene and to modify existing treatment, this problem will be discussed in detail separately. (Refer to Chapter 5)
Chronic StateAssessment of asthma severity follows the Global Initiative on Asthma classification Classification of severity is subdivided into four steps: intermittent, mild persistent, moderate persistent and severe persistent. (See Table 1.2)
Recent publications criticized the GINA classification on severity based on symptoms and frequency of at-
tacks,4,5 and PEF and FEV1 values.6 Long-term mental retention of and adherence to the classification details have not been satisfactory even after intensive dissem-mation workshops.7
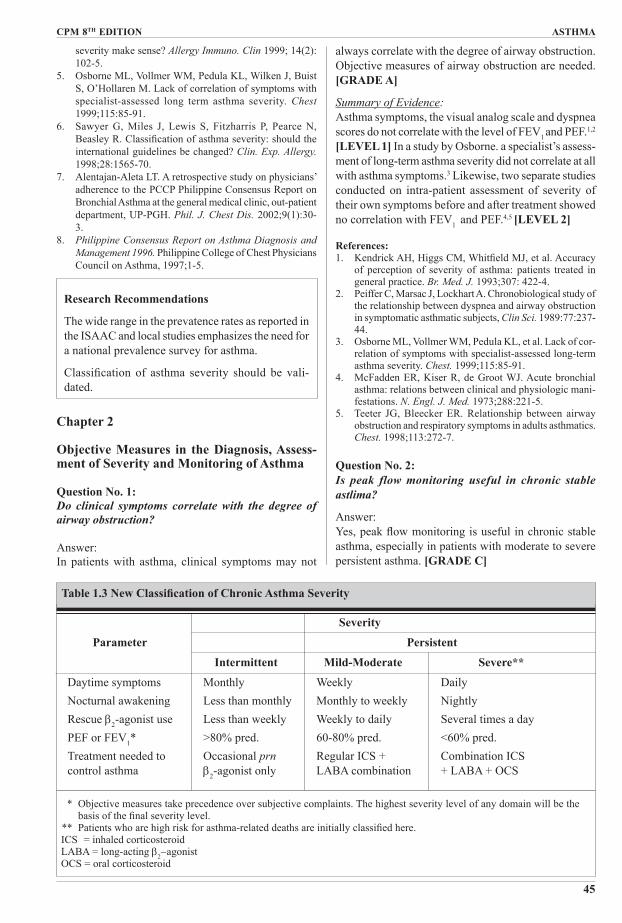
Because asthma is a chronic inflammatory disease, the severity of its chronic state exists in a continuum. Numeric cut-off values of frequency and intensity of symptoms, and parameters of physiologic dysfunction currently used to classify asthma in different levels of severity are artificial and transitory. Of note is the fact that the l994 GINA severity classification, which was recommended in the first Philippine Consensus Report on Asthma Diagnosis and Management (1996)8, has not been validated.Table 1.3 shows a revised classification combining mild persistent and moderate persistent categories into one. This new asthma severity classification, beyond its scientific soundness, is more comprehensible and readily applicable to clinical work. [LEVEL 4]
References:1. Guidelines for the Diagnosis and Management of Asthma;
National Asthma Education and Prevention Program. Expert Panel Report 2. Bethesda, MD: National Institutes of Health; National Heart, Lung and Blood Institute 1997; NIH Publication No. 97-4051A.
2. Strunk SC. Identification of the fatality-prone subject with asthma. J. Allergy Clin. Immunol. 1989: 83:477-85.
3. Jalaludin BB, Smith MA, Chey T, Orr NJ, Smith WT, Leeder SR. Risk factors for asthma deaths: a popula-tion-based case-control study. Aust. NZ. J. Publ.Health. 1999;23:595-600.
4. Garcia HJ. Does a classification of asthma based on its
StEP 1: Intermittent Symptoms less than once a week Brief exacerbations Nocturnal symptoms not more than twice a month - FEV1 or PEF >80% predicted - PEF variability <20%StEP 2: mild Persistent Symptoms more than once a week but less than once a day Exacerbations may affect activity and sleep Nocturnal symptoms more than twice a month - FEV1 or PEF > 80% predicted - PEF variability 20-30%StEP 3: moderate Persistent Symptoms daily Exacerbations may affect acitivity and sleep Nocturnal symptoms not more than once a week Daily use of short-acting β2-agonist - FEV1 or PEF 60-80% predicted - PEF variability >30%STEP 4: Severe Persistent Symptoms daily Frequent exacerbations Frequent nocturnal activities Limitation of activities - FEV1 or PEF <60% predicted - PEF variability >30%
Table 1.2 GINA Classification of Asthma Severity by Clinical Features
CPm 8th EDItION ASthmA
45
severity make sense? Allergy Immuno. Clin 1999; 14(2): 102-5.
5. Osborne ML, Vollmer WM, Pedula KL, Wilken J, Buist S, O’Hollaren M. Lack of correlation of symptoms with specialist-assessed long term asthma severity. Chest 1999;115:85-91.
6. Sawyer G, Miles J, Lewis S, Fitzharris P, Pearce N, Beasley R. Classification of asthma severity: should the international guidelines be changed? Clin. Exp. Allergy. 1998;28:1565-70.
7. Alentajan-Aleta LT. A retrospective study on physicians’ adherence to the PCCP Philippine Consensus Report on Bronchial Asthma at the general medical clinic, out-patient department, UP-PGH. Phil. J. Chest Dis. 2002;9(1):30-3.
8. Philippine Consensus Report on Asthma Diagnosis and Management 1996. Philippine College of Chest Physicians Council on Asthma, 1997;1-5.
Research Recommendations
The wide range in the prevatence rates as reported in the ISAAC and local studies emphasizes the need for a national prevalence survey for asthma.
Classification of asthma severity should be vali-dated.
Chapter 2
Objective Measures in the Diagnosis, Assessment of Severity and Monitoring of Asthma
Question No. 1:Do clinical symptoms correlate with the degree of airway obstruction?
Answer:In patients with asthma, clinical symptoms may not
always correlate with the degree of airway obstruction. Objective measures of airway obstruction are needed. [GRADE A]
Summary of Evidence:Asthma symptoms, the visual analog scale and dyspnea scores do not correlate with the level of FEV1 and PEF.1,2 [LEVEL 1] In a study by Osborne. a specialist’s assess-ment of long-term asthma severity did not correlate at all with asthma symptoms.3 Likewise, two separate studies conducted on intra-patient assessment of severity of their own symptoms before and after treatment showed no correlation with FEV1 and PEF.4,5 [LEVEL 2]
References:1. Kendrick AH, Higgs CM, Whitfield MJ, et al. Accuracy
of perception of severity of asthma: patients treated in general practice. Br. Med. J. 1993;307: 422-4.
2. Peiffer C, Marsac J, Lockhart A. Chronobiological study of the relationship between dyspnea and airway obstruction in symptomatic asthmatic subjects, Clin Sci. 1989:77:237-44.
3. Osborne ML, Vollmer WM, Pedula KL, et al. Lack of cor-relation of symptoms with specialist-assessed long-term asthma severity. Chest. 1999;115:85-91.
4. McFadden ER, Kiser R, de Groot WJ. Acute bronchial asthma: relations between clinical and physiologic mani-festations. N. Engl. J. Med. 1973;288:221-5.
5. Teeter JG, Bleecker ER. Relationship between airway obstruction and respiratory symptoms in adults asthmatics. Chest. 1998;113:272-7.
Answer:Yes, peak flow monitoring is useful in chronic stable asthma, especially in patients with moderate to severe persistent asthma. [GRADE C]
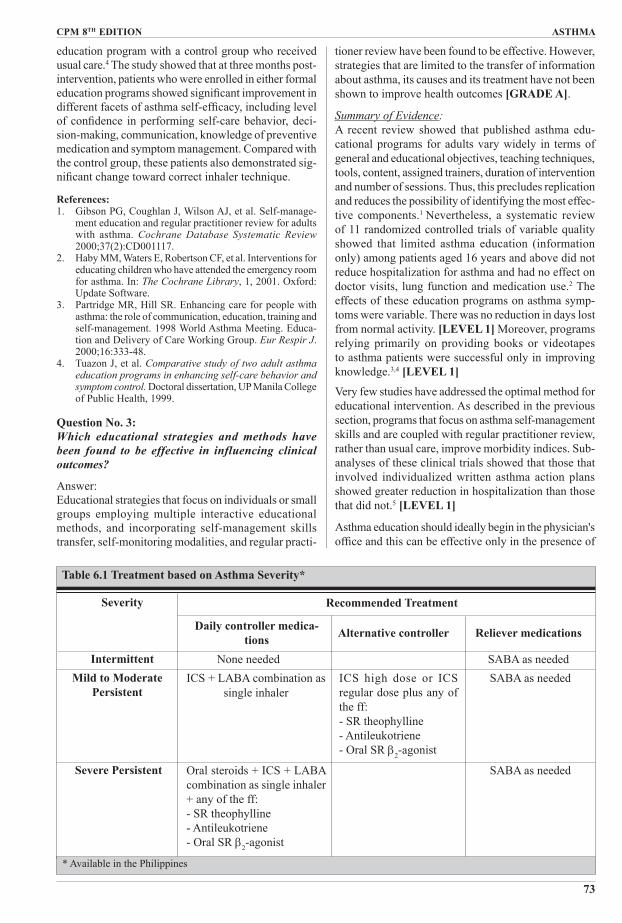
Severity
Parameter Persistent
Intermittent MildModerate Severe**
Daytime symptoms Monthly Weekly DailyNocturnal awakening Less than monthly Monthly to weekly NightlyRescue β2-agonist use Less than weekly Weekly to daily Several times a dayPEF or FEV1* >80% pred. 60-80% pred. <60% pred.Treatment needed to Occasional prn Regular ICS + Combination ICS control asthma β2-agonist only LABA combination + LABA + OCS
Table 1.3 New Classification of Chronic Asthma Severity
* Objective measures take precedence over subjective complaints. The highest severity level of any domain will be the basis of the final severity level.
** Patients who are high risk for asthma-related deaths are initially classified here.ICS = inhaled corticosteroidLABA = long-acting β2−agonistOCS = oral corticosteroid
ASthmA CPm 8th EDItION
46
Summary of Evidence:Although clinical trials show conflicting results, evi-dence suggests that PEFR monitoring improves patient outcome.1 The Grampian Asthma Study of Integrated Care Trial2 (GRASSIC) is a randomized controlled trial comparing the effect of PEF-based self management against conventional treatment on patient outcome. At the end of a 12-month observation period, the authors showed there was no statistically significant difference in patient outcome between the two groups. However, higher number of physician consultations was seen in the PEF-based group, reflecting closer monitoring of asthma by the health care professionals. PEF-based self-management is especially beneficial for patients with severe asthma since it will facilitate closer monito-ring by general practitioners and encourage prompt administration of oral steroids whenever appropriate [LEVEL 3].
References:1. Jain P. Kavuru M, et al. Utility of peak expiratory flow
monitoring. Chest 1998;114:3:861-75.2. Grampian Asthma Study of Integrated Care. Effectiveness
of routine self-monitoring of peak flow in patients with asthma. Br. Med. J. 1994;308:564-7.
Question No. 3:Does peak flow variability correlate with worsening asthma?
Answer:Yes, and despite the lack of clear evidence to support its use, peak flow variability is a useful indicator of worsening airflow obstruction [GRADE D]
Summary of Evidence:Population-based studies show that excessive diurnal PEF variation correlated with a higher incidence of respiratory symptoms, poor asthma control, and sudden death.l,2 [LEVEL 2]Clinical and epidemiological studies have reported good correlation between peak flow variability and the degree of bronchial hyperresponsiveness (BHR) observed after histamine or methacholine inhalation challenge. BHR is currently considered the best available clue to the presence of airway inflammation. Taken together, the available data suggest that PEF variability is loosely associated with the presence of airway inflammation. This finding is further strengthened by studies that dem-onstrate improvement in PEF 3,4,5 and decrease in vari-ability6,7,8 after effective control of airway inflammation with inhaled corticosteroids (ICS). [LEVEL 3]
References:1. Quackenboss JJ, Lebowitz MD, Krzyzanowski M. The
normal range of diurnal changes in peak expiratory flow rates: relationship to symptoms and and respiratory dis-ease. Am. Rev. Respir. Dis. 1991;143:323-30.
2. Boezen HM, Schouten JP, Postma DS, et al. Relation bet-ween respiratory symptoms, pulmonary function and peak flow variability in adults. Thorax.1995;5; 50:121-6.
3. Haahtela T, Jarniven M, Kava T, et al. Comparison of β2-agonist terbutaline with an inhaled corticosteroid budesonide in newly detected asthma. N. Engl. J. Med. 1991;325:388-92.
4. Griffin E, Hakansson L, Formgren H, et al. Blood eo-sinophil number and activity in relation to lung function in patients with asthma and eosinophilia. J. Allergy Clin. Immunol. 1991;87:548-57.
5. Molema J, van Herwaarden CL, Folgering HT. Effects of long-term treatment with inhaled cromoglycate and budesonide on bronchial hyperresponsiveness in patients with allergic asthma. Eur Respir. J. 1989;2: 308-16.
6. Waalkens HJ, Gerritsen J, Koeter GH, et al. Budesonide and terbutaline or terbutaline alone in children with mild asthma: effects on bronchial hyperresponsiveness and diurnal variation in peak flow. Thorax 1991; 46:499-503.
7. Van Esne-Zandvliet EE, Hughes MD, et al. Effects of 22 months of treatment with inhaled corticosteroids and/or β2-agonists on lung function, airway responsiveness, and symptoms in children with asthma. The Dutch Chronic Nonspecific Lung Disease Study Group. Am Rev. Respir. Dis. 1992;146:547-54.
8. Kerstjens HA, Brand PL, de Jong PM, et al. Influence of treatment on peak expiratory flow and its relation to airway hyperresponsiveness and symptoms: the Dutch CNSLD Study Group. Thorax 1994;49:1109-15.
Question No. 4:Is peak flow monitoring useful in acute exacerbation of asthma?
Answer:Yes, the measurement of PEFR provides useful infor-mation on the severity of asthma attack, response to therapy, need for hospital admission, and risk of early relapse. [LEVEL 2]
Summary of Evidence:The use of PEF monitoring in the treatment of acute asthma has been shown to reduce unnecessary asthma-related hos-pital admissions from the emergency department (ED).1-7 In studies involving patients treated for acute asthma exacerbation in the ED setting, PEF before and after treatment were taken and compared for admitted and discharged patients.2,3,4,5 Patients who eventually needed hospitalization have lower PEF both at the beginning and at the end of the ED treatment, indicating a greater severity of airflow obstruction in those who need in-pa-tient care. Other studies suggest that failure of FEV1 or PEF to improve promptly after bronchodilator adminis-tration predicts longer ED stay and more frequent need for hospital admission.6,7 [LEVEL 2]Thus, available data indicate that individuals showing higher pre-treatment PEFR and an early response to initial bronchodilator administration are less likely to require hospital admission. [LEVEL 2]
References:1. Taylor MR. Asthma: audit of peak flow rate guidelines for
admission and discharge. Arch. Dis Child. 1994;70:432-4.
2. Kwong T, Town I, Holst PE, et al. A study of the manage-
CPm 8th EDItION ASthmA
47
ment of asthma in a hospital emergency department. N. Z. Med. J. 1989;102:547-9.
3. Chidley, KE, Wood-Baker R, Town GI, et al. Reassess-ment of asthma management in an accident and emergency department. Respirol.Med. 1991;85:373-7.
4. Gibson PG, Talbot PI, Hancock J, et al. A prospective audit of asthma management following emergency asthma treat-ment at a teaching hospital. Med. J. Aust. 1993;158:775-8.
5. Kerem E, Tibshirani R, Canny G, et al. Predicting the need for hospitalization in children with acute asthma. Chest. 1990;98:1355-61.
6. Stein LM, Cole RP. Early administration of corticosteroids in emergency room treatment of acute asthma. Ann. Intern. Med. 1990;112:822-7.
7. Rodrigo G, Rodrigo C. Assessment of the patient with acute asthma in the emergency department: a factor ana-lytic study. Chest. 1993;104:1325-8.
Research Recommendation
Further local setting studies validating the clinical significance of peak expiratory flow measurements and the predictive value of variability monitoring are needed.
Chapter 3Control of Triggershouse Dust mitesQuestion no. 1:Are house dust mites a significant cause of asthma?
Answer:Worldwide, investigators have found that the dust mite is a significant cause of allergic asthma. [LEVEL 1]
Summary of evidence:In 1964, mite extracts from house dust were found to produce positive skin reactions. Moreover, patients who had positive bronchoprovocative tests improved when they were removed from contact with mites. These findings led to the conclusion that Dermatophagoides species was a principal source of house dust allergens.1-
5 More recent studies confirmed Dermatophagoides pteronyssinus to be the most abundant mite species worldwide.6 [LEVEL 1]
The allergenic proteins are actually contained in the fe-cal pellets of the mite. The allergens fall mainly into two immunologically important groups which are clinically relevant to asthma, atopic dermatitis and allergic rhinitis. These allergens persist for months despite eradication of live mites.7 In investigating for the possibility of exposure, it is best to measure mite allergens in dust vacuumed from surfaces because the fecal pellets remain aerosolized for only a few minutes after they are stirred from a resting place.
Is mite the producer of the house dust allergen? Allergy
Asthma. 1964;10:329.2. Voorhorst AS. The house dust mite (Dermatophagoides
pteronyssinus) and the allergens it produces: identify with the house dust allergen. J. Allergy Clin. Immunol. 1967;39:325.
3. Nagakura T, Yasueda H, Obata T, et al. Major dermato-phagoides mite allergen, Der I, in soft toys. Clin Exp Allergy. 1996;26:585-9.
4. Platts-Mills TAE, Chapman MD. Dust mites: immunology, allergic disease, and environmental control. J. Allergy Clin. Immunol. 1987,80:755.
5. Maunsell K, Wraith DG, Cunnington AM. Mites and house-dust allergy in bronchial asthma. Lancet. 1968; 1:1267.
6. Lecks HI. The mite and house dust allergy. A review of current knowledge and its clinical significance. Clin Pediatr. 1973;12:514.
7. Sears MR, Herbinson GP, Holdaway MD, et al. The rela-tive risks of sensitivity to grass pollen house, dust mite and cat dander in the development of childhood asthma. Clin. Exp. Allergy. 1989;19:419-24.
Question No. 2:Are mechanical measures effective in reducing or eradicating house dust mites?
Answer:Although mechanical removal methods are partly suc-cessful in reducing allergens and killing mites, there is no evidence showing long-term improvement in allergy symptoms among sensitized individuals.
Summary of Evidence:The most effective, and probably the most important avoidance measure is to encase mattresses, pillows, and duvet with covers that are impermeable to mite al-lergens. By encasing beds and pillows in plastic, dust mite populations were found to be reduced by as much as 75% on both mattresses and surrounding carpets.1
[LEVEL 1 ]
Low humidity is an important requirement for dust mite survival. The levels of mite allergens are dramatically reduced at high altitude (>1500 m) where humidity is too low to support mite populations. Theoretically, if relative humidity is kept below 50% for prolonged periods, the mites can be eradicated. Two separate studies showed that mite-sensitive asthmatic children had a progressive reduction in non-specific BHR2 and a progressive improvement in asthma symptoms3 when brought to higher altitude environments. Further studies showed a reversal of this trend after 15 days of allergen re-exposure at sea level.4 [LEVEL 1]
Investigations on the effectiveness of portable dehumi-difiers failed to show any reduction in house dust mite population and allergen levels.5 Another approach in reducing humidity levels is by using mechanical ventila-tion with a heat recovery unit. This method produced a 100% mite reduction in bedroom mattresses one month after operation and 99.9% reduction after 2 months.6 Levels of antigen in carpets were found to drop by 86.7% after steam-cleaning7 or wet cleaning rugs.8
ASthmA CPm 8th EDItION
48
To kill mites by washing, the water temperature must be >54.4oC. The dry cleaning process is found to be ef-fective in eliminating mites.9 One study comparing the effectiveness of dry cleaning with hot-water washing showed that both cleaning methods successfully reduced allergen levels on blankets.10
Other mechanical measures to eradicate house dust mites remain to be controversial. Use of high efficiency particulate air (HEPA) filters appears to be an insuffi-cient substitute for standard avoidance measures in mite-sensitive patients.11 Increasing the frequency of vacuuming to at least once per week is controversial because although this practice has shown reduction in mite numbers, the activity may reintroduce allergens to the air.12
References: 1. Mulla MS, Harkrider JR, Galant SP, et al. Some house
dust mite control measures and abundance of Derma-tophagoides mites in California. J. Med. Entomol. 1975;12:5.
2. Platts-Mills TAE, Chapman MD. Dust mites: immunology, allergic disease and environmental control. J. Allergy Clin. Immunol. 1987;80:755-75.
3. Boner AL, Niero E, Antolini I, et al. Pulmonary function and bronchial hyperreactivity in asthmatic children with house dust mite allergy during prolonged stay in the Italian Alps (Misuria 1756 m). Ann. Allergy. 1985; 54:42-5.
4. Piacentini GL, Martinati L, Fornari A, et al. Antigen avoid-ance in a mountain environment: influence on basophil releasability in children with allergic asthma. J. Allergy Clin. Immunol. 1993;92:644-50.
5. Custovic A. Taggart SCO, Kennaugh JH, et al. Portable humidifiers in the control of house dust mites and mite allergens. Clin. Exp. Allergy. 1995;25:312.
6. Htut T, Houlbrook K, Lumley E, et al. A novel physical method to control mites and their allergens in bedding. Int J Environ Health Res. 1996;6:233.
7. Collof MJ, Taylor C, Merretts TG. The use of domestic steam cleaning for the control of house dust mites. Clin. Exp. Allergy. 1995;25:1061.
8. de Boer R, van der Hoeven W, Kuller K. The control of
house dust mites in rugs through wet cleaning. J. Allergy Clin. Immunol. 1996;97:1214.
9. McDonald LG, Tovey E. The role of water temperature and laundry procedures on reducing house dust mite populations and allergen content of bedding. J. Allergy Clin. Immunol. 1992;90:599-608.
10. Watanabe M, Sagakuchi M, Inouve S, et al. Removal of mite allergens from blankets: comparison of dry clean-ing and hot water washing. J. Allergy Clin. Immunol. 1995;96:1010.
11. Antonicelli L. Bilo MB, Pucci S, et al. Efficacy of an air-cleaning device equipped with a high efficiency particulate air filter in house dust mite respiratory allergy. Allergy. 1991;46:594-600.
12. Massey JE, Massay DG. Effect of vacuum cleaning on house dust mites. Hawaii Med. J. 1984:43:404.
Question No. 3:Are chemical measures effective in reducing or eradi-cating house dust mites?
Answer:Currently available chemical products for control of
dust mites and their allergens offer only short-term effectivity. [GRADE A]
Summary of Evidence:Current strategies for mite control frequently employ chemicals that serve to either eradicate the mites or denature the allergens. These chemicals include benzyl benzoate, permethrin, pirimiphos methyl, phenyl sali-cylate, tannic acid, common household disinfectants, combinations of these, and insect growth regulators. Potential acaricides have had varying degrees of suc-cess in both laboratory and clinical trials.1-3 [LEVEL 1] However, allergen levels rebounded after two months suggesting that repeated application every two to three months is necessary to control mite allergen levels.A study by Dietemann and colleagues4 showed that application of benzyl benzoate in households of asth-matic patients improved their clinical symptoms over a period of one year. However, another study using benzyl benzoate5 showed that although the mite morta-lity drop is 100% two months after treatment, this has decreased significantly to 60% by the third month. Phen-yl salicylate, a compound structurally similar to benzyl benzoate, was observed to retain its acaricidal activity three months post-application.Varying degrees of success have been noted with the use of pirimiphos methyl,6 an organophosphate insecticide, and permethrin,7 a synthetic pyrethroid. Insect growth regulators (e.g., methoprene and hydropene) act by mimicking normal hormonal activity and significantly suppress mite populations up to 30 days.8
Tannic acid, a denaturant capable of breaking down mite fecal allergens,9 was shown to decrease bronchial hyperreactivity in patients only on the eighth month after treatment of mattress casings and carpets.10 a major practical disadvantage of using tannic acid is that it stains fabric.Studies on combined products that employ various con-centrations of an acaricide, denaturant and/or fungicide to kill mites and remove allergens had only significant short-term activity ranging from 10-16 weeks post-ap-plication.11-12
References:1. Hayden ML, Rose G, Diduch KB, et al. Benzyl benzoate
moist powder: investigation of acaricidal activity in cul-tures and reduction of dust mite allergens in carpets. J. Allergy Clin. Immunol 1992;89:536-45.
2. Huss RW, Huss K, Squire EN, et al. Mite allergen control with acaricide fails. J. Allergy Clin. Immunol. 1994;94:27-32.
3. Lau-Schadendorf S, Rusche AF, Weber AK, et al. Short-term effects of solidified benzyl benzoate on mite allergen concentration in house dust. J. Allergy Clin. Immunol. 1991;87:41.
4. Dietemann A, Bessot JC, Hoyet C, et al. A double-blind placebo controlled trial of solidified benzyl benzoate applied in dwellings of asthmatic patients sensitive to mite: clinical efficacy and effect on mite allergens. J. Allergy Clin. Im-munol 1993;91:738-46.
CPm 8th EDItION ASthmA
49
5. Kalpaklioglu AF, Ferizli AG, Misirligil A, et al. The ef-fectiveness of benzylbenzoate and different chemicals as acaricides. Allergy. 1996;51:164.
6. Mitchell EB, Wilkins S, Deighton J, Platts-Mills TAE. Reduction of house dust mite allergen levels in the home: uses of acaricide, pirimiphos methyl. Clin Allergy 1985;15:235-40.
7. Glass EV, Needhan GR. Evaluation of the acaricide permethrin against all stages of the American house dust mite Dermatophagoides farinae, in Mitchell R, Horn DJ, Welbourn WC (eds): Acarology IX proceedings. Colum-bus, Ohio Biological Survey 1997; 693-5.
8. Downing AS, Wright CG, Farrier MH. Effects of five insect growth regulators on laboratory populations of the North American house-dust mite Dermatophagoides farinae. Exp. Appl Acarology 1990;9:123.
9. Green WF. Abolition of allergens by tannic acid [Letter]. Lancet. 1984;2:160.
10. Ehnert B, Lau-Schadendorf S, Weber A, Beuttner P, Schou C, Wahn U. Reducing domestic exposure to dust mites allergen reduces bronchial hypersensitivity in sensitive children with asthma. J. Allergy Clin. Immunol. 1992;90:135-8.
11. Green WF, Nicholas NR, Salome CM, et al. Reduction of house dust mites and mite allergens: effects of spraying carpets and blankets with Allersearch DMS, an acaricide combined with an allergen reducing agent. Clin Exp Al-lergy 1989;19:203.
12. Hart BJ, Greurin B, Nolard N. In vitro evaluation of acaricidal and fungicidal activity of the house dust mite acaricide Allerbiocid. Clin Exp Allergy 1992; 22:923.
Question No. 4:Will patients with asthma who are sensitized to house dust mites benefit from measures designed to reduce their exposure to mite antigen in the home?
Answer:Current methods aimed at reducing exposure to allergens from house dust mites seem to be ineffective and cannot be recommended as prophylactic treatment for asthma patients sensitive to mites [GRADE B]
Summary of Evidence:A meta-analysis of randomized trials investigated the effects of mite antigen reducing measures on asthma compared to an untreated control group.1 There were 23 studies included, six of which used chemical methods, 13 used physical methods, and four used a combination of both. Altogether, 41/113 patients exposed to treatment interventions improved compared with 38/117 in the control groups leading the investigators to conclude that there is no clinical benefit from measures designed to reduce exposure to mites among asthma mite-sensitive patients. [LEVEL 1] The lack of benefit may be due to failure of the methods used to adequately reduce levels of mite antigen.Some studies were able to show effective reduction in mite exposure, but these did not show more positive re-sults when compared to studies that failed to reduce mite exposure. This may be because patients with asthma who are sensitive to mites are usually also sensitive to other
allergens. Therefore, the successful elimination of only one allergen may be of limited benefit.
Reference:1. Gotzche PC, Hammarquist C, Burr M. House dust mite
control measures in the management of asthma: meta-analysis. Br. Med. J. 1998;317:1105-10.
Conclusion and Recommendation
House dust mite antigens are significant causes of asthma in mite-sensitive individuals.Despite the absence of larger and more rigorous studies on methods of mite control, health care givers should continue to institute avoidance and control measures.
Cockroach AllergensQuestion No. 1:Are cockroach allergens an important risk factor for asthma?
Answer:Yes, among the insects, cockroaches are the most recog-nized common source of allergens [LEVEL 1]
Summary of Evidence:Cockroaches are tropical in origin and thrive in houses that are continuously warm. However, unlike mites, they are not dependent on ambient humidity and show great talent in finding water sources within a building. Of the seven or eight indoor species, the American cockroach (Periplaneta americana) is the most common cockroach in the Philippines.
Cockroaches can be safely presumed to cause significant asthma in areas where crowded living conditions exist such as urban slums. Socio-economic status and race are independent risk factors for cockroach allergen exposure both in the home and school settings.1,2 There is also a clear dose-response relationship between cockroach allergen exposure and sensitization in children with asthma.3 [LEVEL 1]
References:1. Sarpong SB, Hamilton RG, Eggleston PA, Adkinson NF
Jr. Socio-economic status and race as risk factors for cock-roach allergen exposure and sensitization in children with asthma. J. Allergy Clin. Immunol. 1996; 97:1393-401.
2. Sarpong SB, Wood RA, Karrison T, et al. Cockroach al-lergen (Bla g1) in school dust. J. Allergy Clin. Immunol. 1997;99:486-92.
3. Sarpong SB, Corey JP. Assessment of indoor environment in respiratory allergy. Ear, Nose, and Throat J. 1998; 77:960,962-4.
Question No. 2:Are control measures designed to reduce or control levels of cockroach allergens in houses effective?
ASthmA CPm 8th EDItION
50
Answer:At present, there are no clear data on the effect of era-dication measures on cockroach allergens. [LEVEL3]
Summary of Evidence:The effect of cockroach control measures on allergen levels in houses has not been extensively studied; al-though a number of trials are under way.1 Both physical and chemical procedures are used to control cockroach populations in houses. These include the following:
• Fastidious cleaning to reduce food supplies• Reducing access to food and water by: - Removal of waste food - Containment of surface water by reducing leakage - Reducing condensation by improved ventilation1
• Restricting cockroach access by closing all entry points through caulking and sealing cracks and holes in the plasterwork and flooring.
• Using chemicals like diazinon, chlorpyrifos and boric acid to control infestation
• Using bait stations containing hydramethylnon or avermectin which are generally effective in reducing cockroach levels for two to three months2.
Professional extermination is needed to eliminate cock-roaches in multi-family dwellings because repopulation can occur from other roach colonies found elsewhere in the building.
References:1. Custovic A, Simpson A, Chapman MD, Woodcock A.
Allergen avoidance in the treatment of asthma and atopic disorders. Thorax. 1998;53:63-72.
2. Guidelines for the Diagnosis and Management of Asthma: National Asthma Education and Prevention Program. Expert Panel Report 2. Bethesda, MD: National institutes of Health; National Heart, Lung, and Blood Institute 1997. NIH Publication no. 97-4051A.
Animal AllergensQuestion No. 1:Can cat allergens cause asthma?
Answer:Yes. Cats are a major source of allergen in the home and and are capable of inducing symptoms in sensitive patients [LEVEL 1].
Summary of Evidence:Cat allergens are found in households with cats and have been confirmed to cause asthma in studies using a special cat challenge room.1 [LEVEL 1] The major cat allergen, Fel d 1, is produced primarily in the sebaceous glands and in the basal squamous epithelial cells of the skin of cats. Very high levels of this allergen were also demonstrated in cat anal secretions.2,3,4 Soft furnishings, carpets and mattresses serve as reservoirs for the aller-gen. Individuals who have never had a cat may become allergic by exposure to the allergen from contact with cats belonging to others. Furthermore, Fel d 1 has been
detected in carpet dust of houses where cats have never been present, suggesting it can be carried into cat-free buildings on the clothing of people exposed to cats.5
Because of the small particle size (≤5 mm in diameter) of these allergens, they can be detected in wall surfaces and in the air of undisturbed rooms.5 This may explain why a sensitized person may experience immediate symptoms when entering a home with a cat, even without direct exposure to the cat.
References:1. de Blay F, Chapman MD, Platt-Mills TAE. Airborne cat
allergen (Fel d 1): environmental control with the cat in situ. Am. Rev. Respir. Dis. 1991;143:1334-9.
2. Charpin C, Mata P, Charpin D, et al. Fel d 1 allergen distribution in cat fur and skin. J. Allergy Clin Immunol. 1991;88:77-82.
3. Dabrowski AJ, Van Ber Brempt X. Soler M, et al. Cat skin as an important source of Fel d 1 allergen. J. Allergy Clin Immunol. 1990;86:462-5.
4. Domelas de Andrede A, Bimbaum J, Magalon C, et al. Fel d 1 levels in cat anal glands. Clin Exp Allergy. 1996;26:178-80.
5. Bollinger ME, Eggleston PA, Flanagan E, et al. Cat antigen in homes in and without cats may induce allergic symptoms. J. Allergy Clin. Immunol. 1996;97: 904-16.
Question No. 2:Can exposure to dog allergens also cause asthma?
Answer:Yes, although obvious allergic reactions to dogs are less common than those to cats. [LEVEL 2]
Summary of Evidence:From preliminary results of studies, it appears that dog allergens, like cat allergens, also become and remain airborne. Thus, it is likely that the same rules apply to dog allergen as to cat. However, most studies report that children have fewer symptoms as a result of dog allergens than cat allergens: in one study, one in ten reacted to cat allergens, whereas only one in 100 re-acted to dog allergens.1 This despite the fact that more individuals own dogs than cats. However, intimacy of exposure may be a factor − many dogs are kept outside whereas cats more often go into the house and into the bedroom of children. However, in areas where dogs are kept in houses, they can become an important source of allergens.2 [LEVEL 4]
Dog saliva and dog dander appear to be the main sources of dog allergen (Can f 1). Dog allergen, like cat allergen, can be detected in public places, including schools.3
Cross-reactivity between dog and cat allergens has been demonstrated, suggesting the presence of common im-munologic determinants.
References:1. Murray AB, Ferguson AC, Morrison BJ. The frequency and
severity of cat allergen vs. dog allergen in atopic chilldren. J. Allergy Clin Immunol 1983;72:145-9.
2. Ingram JM, Sporik R, Rose G, et al. Quantitative as-
CPm 8th EDItION ASthmA
51
sessment of exposure to dog (Can f 1) and cat (Fel d 1) allergens: relationship to sensitization and asthma among children living in Los Alamos, NM. J. Allergy Clin. Im-munol 1995;96:449-56.
3. MunirAKM, Einarson R, Shou C, et al. Allergens in school dust I. The amount of the major cat (Fel d 1) and dog (Can f 1) allergens in dust from Swedish schools is high enough to probably cause perennial symptoms in most children with asthma who are sensitized to cat and dog. J. Allergy Clin. Immunol. 1993:91:1067-74.
Question No. 3:Are measures to control cat or dog allergen levels effective?
Answer:There are no existing studies dealing with effectiveness of control measures on cat or dog allergens.
Summary of Evidence:The best way to reduce exposure to cat or dog allergen is to remove the animal from the home. The clinical benefit of control measures in person, who insist on keeping their pets despite continued symptoms has not yet been established. Airborne allergen levels increase by approximately fivefold when the pet is in the room, indicating that the immediate presence of a pet contrib-utes to airborne allergen levels.1
The accepted control measures to control animal aller-gens are as follows:
1. Remove reservoirs such as carpets and sofas.2. Keep the cat or dog outside as much as possible.3. Use room air cleaners (e.g., High-efficiency particu-
late air cleaner or HEPA), which can reduce aller-gens if the reservoirs are removed first.
4. Bathe the animal weekly. However, even aggres-sive washing can only remove about 40 to 70 % of allergens.2,3
References:1. Custovic A, Green R, Fletcher A, et al. Aerodynamic
properties of the major dog allergen, Can f 1: distribution in homes, concentration and particle size of allergen in air. Am. J. Respir. Crit. Care Med. 1997; 155:94-8.
2. Avner DB, Perzanowski MS, Platts-Mills TAE, Wood-folk JA. Evaluation of different techniques for washing cats: quantitation of allergen removed from the cat and the effect on airborne Fel d 1. J. Allergy Clin. Immunol. 1997;100:307-12.
3. Green R, Custovic A, Smith A, et al. Avoidance of dog allergen Can f 1 with the dog in situ: washing the dog and use of a HEPA air filter. J. Allergy Clin. Immunol. 1996;97:302.
Indoor and Outdoor Repiratory IrritantsQuestion No. 1:Is there a relationship between outdoor air pollution and asthma attacks?
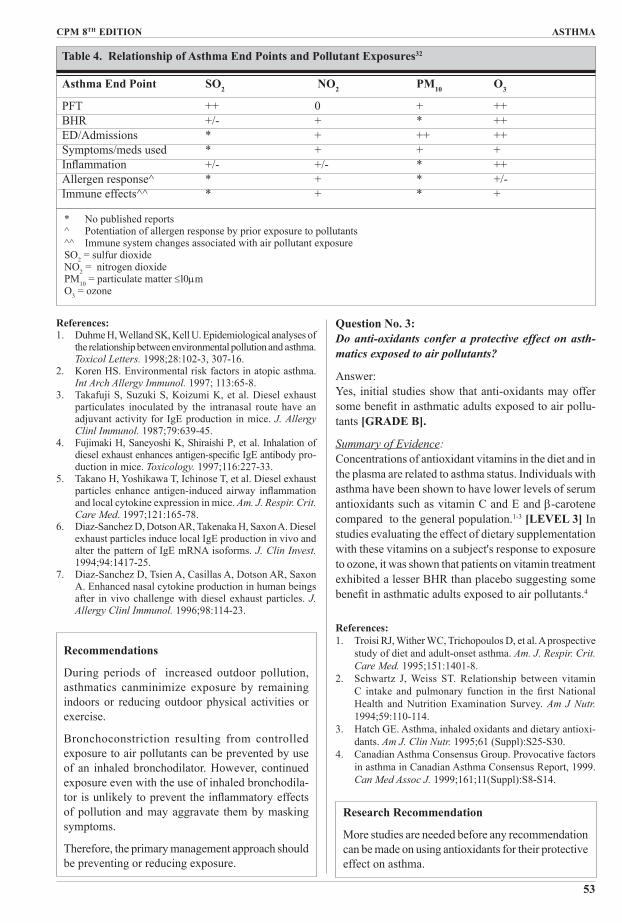
Answer:Yes, outdoor air pollution aggravates asthma. [LEVEL 2]
Summary of Evidence:Several epidemiological studies have shown that of all outdoor pollutants, inhalable particulates ≤10 µm (PM10 ) in diameter are the single greatest hazard to asthma ex-acerbation.1,2 Likewise, the peak hourly nitrogen dioxide (NO2) concentrations,3,4,5 increased ozone (03) and sulfur dioxide (SO2) have individually6,7 or in combination,8 been reported to significantly increase emergency room visit of asthmatics, 9,10,11,12,13-15[LEVEL 2]
Particulate matter (PM) exposure is difficult to achieve in a controlled laboratory setting. However, controlled stud-ies on the effect of sulfuric acid show that asthmatics are more “sensitive” than healthy subjects after exposure.16
High SO2 concentration has been associated with short-term increases in morbidity and mortality in the general population during dramatic air population episodes in the past.17 [LEVEL 3] Exposure to concentrations of SO2 as low as 0.2 ppm appear to have a significant ef-fect in patients who are mouth-breathing or undergoing heavy exercise. However, these effects are short-lived and not increased by prolonged exposure.18 a combi-nation of low concentration of SO2 and NO2
__ often increased in heavy traffic-has been shown to enhance airway responsiveness to inhaled allergen.19,20
Although controlled clinical trials using ozone are equi-vocal,21 studies combining allergen challenges after O3 exposure showed worsening of atopic asthma.22,23
[LEVEL 3]
Several studies have evaluated the relationship of lung function and exposure to pollutants. In one study, healthy and asthmatic patients were exposed for two hours to 0.40 ppm O3eand lung function changes were monitored. Results showed that asthmatic patients have greater PEF decrements and with enhanced reponses to methacholine provocation challenge.24vOther studies showed greater degree of airway inflammation in asthmatics exposed to pollutants25 with higher levels of IL8 and proteins in bronchoalveolar level (BAL) fluid even in the absence of any PEF change.26-31 [LEVEL 3]
In summary, particulate matter exposure is associated with decreased lung function, increased symptoms and unscheduled visits to the emergency room. Exposure to pollutants like SO2 causes dramatic bronchoconstriction accompanied by shortness of breath and wheezing in many subjects with asthma. Likewise, such exposure is associated with many signs of asthma aggravation: decreased lung function, airway inflammation, both emergency department visits and hospital admissions, and enhanced response to common aeroallergens. Thus, asthmatics have been shown to be a sensitive population relative to ozone and other air pollutants.
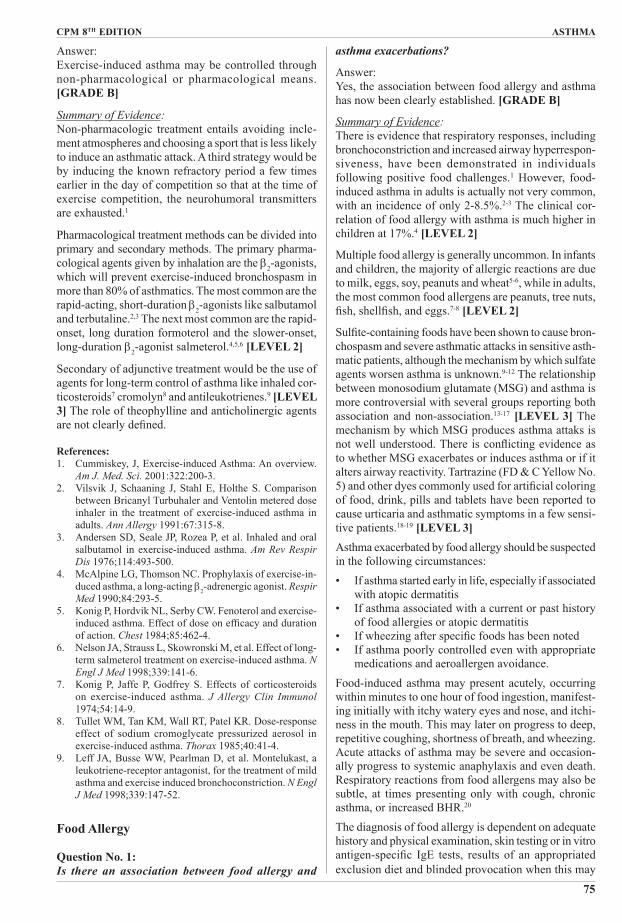
Further researches linking epidemiological, clinical and toxicological approaches are required to better under-stand and characterize the risk of exposing asthmatics to these pollutants. (See Table 4 on page 53)
between respiratory illness and PM10 air pollution. Arch. Environ Health. 1997;52:113-7.
2. Canadian Asthma Consensus Group. Provocative factors in asthma in Canadian Asthma Consensus Report, 1999. Can Med Assoc J. 1999;161:11 (Suppl): S8-S14.
3. Lipsett M, Hurley SB, Ostro B. Air pollution and emergency room visits for asthma in Santa Clara County, California. Environ Health Perspect. 1997;105:216-22.
4. Pantazopoulou A, Katsouyanni K, Kourea-Kremastinou J, Trichopoulos D. Short-term effects of air pollution on hospital emergency outpatient visits and admissions in the greater Athens. Greece area. Environ Res. 1995;69:31-6
5. Castellsague J, Sunyer J, Saez M, Anto JM. Short-term associa-tion between air pollution and emergency room visits for asth-ma in Barcelona. Thorax 1995; 50: 1051-6.
6. Romieu I, Meneses F, Sienra-Monge JJL, Huerta J, et al. Effects of urban air pollutants on emergency room visits for childhood asthma in Mexico City. Am J Epidemiol. 1995;141:546-53.
7. White MC, Etzel RA, Wilcox WD, Lloyd C. Exacerba-tions of childhood asthma and ozone pollution in Atlanta. Environ Res. 1994;65:56-68.
8. Atkinson RW, Anderson HR. Strachan DP, et al. Short-term associations between outdoor air pollution and visits to accident and emergency departments in London for respiratory complaints. Eur Respir J. 1999: 13:257-65.
9. Schwartz J. Slater D, Larson T, Pierson W, Koenig J. Particulate air pollution and hospital emergency room visits for asthma in Seattle. Am. J Respir. Crit. Care Med. 1993;147:826-31.
10. Gordian ME, Ozkaynak H, Xue J, et al. Particulate air pollution and respiratory disease in Anchorage, Alaska. Environ Health Perspect. 1996;104: 290-7.
11. Yang W, Jennison BL, Omaye ST. Air pollution and asthma emergency room visits in Reno, Nevada. Inhal Toxicol.1997;9:15-29.
12. Norris G, YoungPong SN. Koenig JQ, et al. An association between fine particles and asthma emergency department visit for children in Seattle. Environ Health Perspect 1999;107:489-93;
13. Peters A, Wichmann E, Tuch T, Heinrich J, Heyder J. Respiratory effects are associated with the number of ultrafine particles. Am. J. Respir. Crit. Care Med. 1997; 155:1376-83.
14. Timonen KL, Peldcanen J. Air Pollution and respiratory health among children with asthmatic or cough symptoms. Am. J. Respir. Crit. Care Med. 1997:156: 546-52.
15. Vedal S. Petlau J, White R, Blair J. Acute effects of am-bient inhalable particles in asthmatic and non-asthmatic children. Am J. Respir. Crit. Care Med. 1998;157: 1-10.
16. Committee of the Environmental and Occupational Health Assembly of the American Thoracic Society. Health ef-fects of outdoor air pollution. Am J. Respir. Crit. Care Med 1996:153;3-50.
17. Bates DV, Baker-Anderson M, Sixto R. Asthma attacks periodicity. A study of hospital emergency visits in Van-couver. Environ Res. 1990;51:51-70.
18. Pekkenan J, Timonen KL, Ruuskanen J, et al. Effects of ultrafine and fine particles in urban air on peak expiratory flow among children with asthmatic symptoms. Environ Res 1997;74:24-33.
19. Rusznak C, Devalia JL, Davies RJ. Airway response of asthmatic subjects to inhaled allegen after exposure to pollutants. Thorax. 1996;51:1105-8.
20. Rossi OV, Kinnula VL, Tienari J, Huhti E. Association of severe asthma attacks with weather, pollen and air pollut-
ants. Thorax 1993;48:244-8.21. Zhong NS. New insights into risk factors for asthma.
Respirology. 1996: 1: 159-66.22. Hanley QS, Koenig JQ: Larson TV, et al. Response of
young asthmatic patients to inhaled sulfuric acid. Am. Rev. Respir Dis 1992;145:326-31.
23. Koenig JQ, Laarson TV, Hanley QS, et al. Pulmonary func-tion changes in children associated with fine particulate matter. Environ Res. 1993;63:26-38.
24. Koren HS. Associations between criteria air pollutants and asthma. Environ Health Perspect. 1995;103 (Suppl)6:235-42.
25. Koenig JW, Pierson WE, Horike M, et al. Effects of SO2 plus NaCl aerosol combined with moderate exercise on pulmonary function in asthmatic adolescents. Environ Res 1981;25:340-8.
26. Wardlaw AJ. The role of air pollution in asthma. Clin Exp Allergy 1993;23:81-96.
27. Koren HS. Environmental risk factors in atopic asthma. Int Arch Allergy Immunol 1997;113:65-8.
28. Molfino NA, Wright SC, Katz I, et al. Effect of low concentrations of ozone on inhaled allergen responses in asthmatic subjects. Lancet 1991; 338: 199-203.
29. Kreit JW, Gross KB, Moor TB, et al. Ozone-induced changes in pulmonary function and bronchial responsiveness in asth-matics. J Appl Physio. 1989;66:217- 22.
30. Basha MA, Gross KB, Gwizdala CJ, et al. Bronchoalveolar lavage neutrophilia in asthmatic and healthy volunteers after controlled exposure to ozone and filtered purified air. Chest. 1994;106:1757-65.
31. Scannel C, Chen L, Aris RM, et al. Greater ozone-induced inflammatory responses in subjects with asthma. Am. J. Respir. Crit. Care Med. 1996:154:24-9
32. Koenig J, Air pollution and asthma. J. Allery Clin. Im-munol. 1999;104:717-22.
Question No. 2:Does air pollution cause an increase in asthma prevalence?
Answer:There is no consistent evidence that common air pollu-tants are involved in the development of asthma.
Summary of Evidence:Because genetics alone is unlikely to explain the increas-ing prevalence of asthma worldwide, it is very tempting to attribute the epidemic to environmental factors suchas indoor and outdoor air pollution1.
In many regions of the world, asthma prevalence has increased just as the populations have become wester-nized.2,3 However, studies comparing asthma and allergy prevalence between highly polluted Leipzig and clean Munich in Germany showed no significant difference between the two weternized cities.4,5,6,7 Air pollution may aggravate existing asthma, but it is unlikely to be responsible for the asthma epidemic. [LEVEL 3]Various studies strongly suggest that air pollution can modulate or enhance airway inflammation associated with allergic and asthmatic diseases. There is now ex-tensive evidence demonstrating adjuvant effects of air pollutants on the formation of specific IgE antibodies and cytokines in both animals and man.4,5,6,7
CPm 8th EDItION ASthmA
53
References:1. Duhme H, Welland SK, Kell U. Epidemiological analyses of
the relationship between environmental pollution and asthma. Toxicol Letters. 1998;28:102-3, 307-16.
2. Koren HS. Environmental risk factors in atopic asthma. Int Arch Allergy Immunol. 1997; 113:65-8.
3. Takafuji S, Suzuki S, Koizumi K, et al. Diesel exhaust particulates inoculated by the intranasal route have an adjuvant activity for IgE production in mice. J. Allergy Clinl Immunol. 1987;79:639-45.
4. Fujimaki H, Saneyoshi K, Shiraishi P, et al. Inhalation of diesel exhaust enhances antigen-specific IgE antibody pro-duction in mice. Toxicology. 1997;116:227-33.
5. Takano H, Yoshikawa T, Ichinose T, et al. Diesel exhaust particles enhance antigen-induced airway inflammation and local cytokine expression in mice. Am. J. Respir. Crit. Care Med. 1997;121:165-78.
6. Diaz-Sanchez D, Dotson AR, Takenaka H, Saxon A. Diesel exhaust particles induce local IgE production in vivo and alter the pattern of IgE mRNA isoforms. J. Clin Invest. 1994;94:1417-25.
7. Diaz-Sanchez D, Tsien A, Casillas A, Dotson AR, Saxon A. Enhanced nasal cytokine production in human beings after in vivo challenge with diesel exhaust particles. J. Allergy Clinl Immunol. 1996;98:114-23.
Recommendations
During periods of increased outdoor pollution, asthmatics canminimize exposure by remaining indoors or reducing outdoor physical activities or exercise.
Bronchoconstriction resulting from controlled exposure to air pollutants can be prevented by use of an inhaled bronchodilator. However, continued exposure even with the use of inhaled bronchodila-tor is unlikely to prevent the inflammatory effects of pollution and may aggravate them by masking symptoms.
Therefore, the primary management approach should be preventing or reducing exposure.
Question No. 3:Do anti-oxidants confer a protective effect on asth-matics exposed to air pollutants?
Answer:Yes, initial studies show that anti-oxidants may offer some benefit in asthmatic adults exposed to air pollu-tants [GRADE B].
Summary of Evidence:Concentrations of antioxidant vitamins in the diet and in the plasma are related to asthma status. Individuals with asthma have been shown to have lower levels of serum antioxidants such as vitamin C and E and β-carotene compared to the general population.1-3 [LEVEL 3] In studies evaluating the effect of dietary supplementation with these vitamins on a subject's response to exposure to ozone, it was shown that patients on vitamin treatment exhibited a lesser BHR than placebo suggesting some benefit in asthmatic adults exposed to air pollutants.4
References:1. Troisi RJ, Wither WC, Trichopoulos D, et al. A prospective
study of diet and adult-onset asthma. Am. J. Respir. Crit. Care Med. 1995;151:1401-8.
2. Schwartz J, Weiss ST. Relationship between vitamin C intake and pulmonary function in the first National Health and Nutrition Examination Survey. Am J Nutr. 1994;59:110-114.
3. Hatch GE. Asthma, inhaled oxidants and dietary antioxi-dants. Am J. Clin Nutr. 1995;61 (Suppl):S25-S30.
4. Canadian Asthma Consensus Group. Provocative factors in asthma in Canadian Asthma Consensus Report, 1999. Can Med Assoc J. 1999;161;11(Suppl):S8-S14.
Research Recommendation
More studies are needed before any recommendation can be made on using antioxidants for their protective effect on asthma.
Table 4. Relationship of Asthma End Points and Pollutant Exposures32
* No published reports^ Potentiation of allergen response by prior exposure to pollutants^^ Immune system changes associated with air pollutant exposureSO2 = sulfur dioxideNO2 = nitrogen dioxidePM10 = particulate matter ≤l0µmO3 = ozone
ASthmA CPm 8th EDItION
54
Question No. 4:Can indoor air pollution trigger asthma exacerba-tion?
Answer: Yes, indoor air pollution, the most common of which is tobacco smoke, has been shown to definitely increase asthma exacerbation [LEVEL 1].
Summary of Evidence:There is a significant body of evidence linking tobacco smoke, an indoor pollutant, to asthma exacerbation.1-5
[LEVEL 1] Findings suggest that nitrogen dioxide at concentrations encountered in the home environment can potentiate the specific airway response of patients with mild asthma to inhaled house dust mite allergen.6
Consensus from recent literature reviews and meta-ana-lyses reinforce previous conclusions of health effects of environmental tobacco smoke (ETS) on children.7-10
Although a genetic etiology for asthma is assumed, the development of asthma is considered to be dependent on environmental factors, such as exposure to allergens including ETS. This exposure may cause asthma onset in children and adults and early non-allergenic wheezing in infants and children. It also increases the frequency and severity of symptoms among those with established disease. 10,11,12 Environmental tobacco smoke exposure is thus an accepted risk condition for pulmonary and other dis-eases.
References: 1. Martinez FD, Wright AL, Taussig IM, et al. Asthma and
wheezing in the first six years of life. N. Engl J Med. 1995;322:133-7.
2. Young S, Le Souef PJ, Geelhoed GC, et al. The influ-ence of a history of asthma and parental smoking on airway responsiveness in early infancy. N. Engl J Med. 1991;324:1168-73.
3. Samet JM, Lange P. Longitudinal studies of active and passive smoking. Am. J. Respir. Crit. Care Med. 1996;154:S257-S265.
4. Weitzman M, Gortmacher SL, Walker DK, et al. Maternal smoking and childhood asthma. Pediatrics. 1990;85:505-11.
5. Dezateux C, Stocks J, Dundas I, Fletcher ME. Impaired airway function and wheezing in infancy: the influence of maternal smoking and a genetic predisposition to asthma. Am. J. Respir. Crit. Care Med. 1999;159:403-10.
6. Tunnicliffe, WS, Burge PS, Ayres JG. Effect of do-mestic concentrations of nitrogen dioxide on airway responses to inhaled allergen in asthmatic patients. Lancet 1994;344:1733-6.
7. California Environmental Protection Agency. Health effects of exposure to environmental tobacco smoke. California Environmental Protection Agency, Office of Environment Health Hazard Assessment. September 1997.
8. Scientific Committee on Tobacco and Health. Report of the Scientific Committee on Tobacco and Health. 1988.
9. Cook DG, Strachan DP. Summary of effects of prenatal smoking on the respiratory health of children and implica-tions of research. Thorax. 1999;54:357-66.
10. Cook DG, Strachan DP. Background paper: Effects of maternal and parental smoking on children's respiratory
health. International Consultation on Environmental To-bacco Smoke and Child Health. World Health Organiza-tion, 1999.
11. Coultas DB. Health effects of passive smoking. Passive smoking and risk of adult asthma and COPD: an update. Thorax. 1998;53:381-7.
Research Recommendation
More research is necessary to clarify the pathologic mechanisms by which environmental tobacco smoke causes or aggravates asthma.
Infections and Asthma DevelopmentQuestion No. 1:Is there an association between respiratory infections and the development of asthma?
Answer:Yes, there is emerging evidence that infections early in life (i.e., in utero and in early infancy) have profound influence on the development of asthma in later life. [LEVEL 2]
Summary of Evidence:Since asthma is an inflammatory disease,1 the main im-munoglobulin implicated (IgE) and the kind of inflam-matory cytokines predominating (IL-4, IL-5, IL-13) point to a predominance of the T-helper lymphocyte-22 response.2 T-helper lymphocyte-21 response is further characterized by increased production of IFN-γ and Ipterlevel-12.3 It is now known that the intrauterine milieu is skewed towards the TH2 phenotype. The most vulnerable period for the switch from TH1 to TH2 is dur-ing pregancy and early infancy.4,5 Some viral infections like the RSV6,7 and EBV8,9 favor the TH2 responses and has been associated with increased allergen sensitization in later life.10-13 Respiratory Syncitial virus infection has been associated with increased Epstein Barr virus in children regardless of asthma history.14,15,16 On the other hand, absence of the more common infections (Mycobacterium tuberculosis,17 measles,18 Hepatitis A,19 other respiratory viruses20 and helminthic infestations) during early childhood impairs the drive to maturation of the TH1 pathway,20 causing a relative increase in TH2. This phenomenon is believed responsi-ble, at least in part, for the higher prevalence of asthma in families with fewer siblings, in affluent societies, and in the western, industrialized world. These conditions, resulting in a cleaner environment, avert exposure to and development of common childhood infections.21-22 However, in these same conditions. the prevalence of asthma and other atopic diseases, which were considered rare a few decades ago, appear to have doubled every 10-15 years, with the highest prevalence rates seen in the industrialized western world.23
References:1. Guidelines for the Diagnosis and Management of Asthma:
CPm 8th EDItION ASthmA
55
National Asthma Education and Prevention Program. Expert: Panel Report 2. Bethesda, MD: National Institutes of Health; National Heart, Lung and Blood Institute 1997:NIH Publication No. 97-4051A.
2. Holgate S. Mediator and cytokine mechanisms in asthma. Thorax 1993;48:103-9.
3. Maggi E, Parronchi P, Manetti R, et al. Reciprocal regula-tory role of IFN-γ and IL-4 on the in vitro development of human TH1 and TH2 cells. J. Immunol 1992;148:2142-7.
4. Warner JA, Miles EA, Jones AC, Quint DC, Colwell BM, Warner J. Is deficiency of interferon-γ production by al-lergen-triggered cord blood cells a predictor of atopic eczema? Clin Exp Allergy. 1994;24:423-30.
5. Martinez FD, Stern DA, Wright AL, Holberg CJ, Taussig LM, Halonen M. Association of interleukin-2 and inter-feron-γ production by blood mononuclear cells in infancy with parenteral allergy skin tests and with subsequent de-velopment of atopy. J. Allergy Clin Immunol 1995;96:652-60.
6. Sigurs N, Bjarnason R, Sigurbergsson F, Kjellman B, Björkstén B. Asthma and immunoglobulin E antibodies after respiratory synctial virus bronchiolitis: a prospec-tive cohort study with matched controls. Pediatrics. 1995;95:500-5.
7. Sigurs N, Bjarnason R, Sigurbergsson F, Kjellman B, Respiratory syncytial virus bronchiolitis in infancy is an important risk factor for asthma and allergy at age 7. Am. J. Respir. Crit. Care Med. 2000;161:1501-7.
8. Strannegård I-L, Strannegård Ö. Epstein-Barr virus anti-bodies in children with atopic disease. Intern Arch Allergy Appl Immunol. 1981;64:314-9.
9. Rystedt I, Strannegård I-L, Strannegård Ö. Increased serum levels of antibodies to Epstein-Barr virus in adults with history of atopic dermatitis. Intern. Arch Allergy Appl Immunol. 1984;75:179-83.
10. Grunberg K, Smits HH, Timmers MC, de Klerk EP, Dolhain RJ, Dick EC, et al. Experimental rhinovirus 16 infection. Effects on cell differentials and soluble markers in spu-tum in asthmatic subjects. Am. J. Respir. Crit. Care Med. 1997;156:609-16.
11. Rager KJ, Langhand JO, Jacobs BL, Proud D, Marsh DG, Imani F. Activation of antiviral protein kinase leads to immunoglobulin E class switching in human B cells. J Virology 1998;72:1171-6.
12. Terajima MN, Yamaya M, Sekizawa, Okinaga S, Suzuki T, Yamada N, et al. Rhinovirus infection of primary cultures of human tracheal epthelium: role of ICAM-1 and IL-1. Am J. Physio 1997;273:749-59.
13. Johnston S, Johnston SL. Influence of viral and bacterial infections on exacerbations and symptom severity in child-hood asthma. Pediatr. Pulmonol. 1997;16 (suppl): 88-9.
14. Schwarze J, Hamelman E, Bradley KL, Takeda K, Gelfand EW. Respiratory syncytial virus infection results in airway hyperresponsesiveness and enhanced airway sensitization to allergen. J. Clin. Invest. 1997; 100: 226-33.
15. Robinson PJ, Hegele RG, Schellenberg RR. Allergic sen-sitization increases airway reactivity in guinea pigs with respiratory syncytial virus bronchiolitis. J. Allergy Clin Immunol. 1997;100:492-8.
16. Cua-Lim F, Roa CC, Pagkatipunan R. Prevalence of adult asthma and allergies in Malolos, Bulacan, Metro Manila, Philippines. Presented as a poster study at the 3rd asian Pacific Congress of Allergology and Clinical Immunology, PICC, Manila, Philippines. Dec 9-11, 1998.
17. Shirakawa T, Enomoto T, Shimazu S, Hopkin J. The in-verse association between tuberculin responses and atopic disorder. Science. 1997;275:77-9.
18. Shaheen SO, Aaby P, Hall AJ, Barker DJ, Heyes CB, Shiell AW, Goydiaby A. Measles and atopy in Guinea-Bissau.
tional retrospective study of prevalence of atopy among Italian military students with antibodies against hepatitis A virus. Br Med J. 1998;314:999-1003.
20. Martinez FD. Role of viral infections in the inception of asthma and allergies during childhood: could they be protective? Thorax. 1994;49:1189-91.
21. Strachan DP, Harkins LS, Johnston ID, Anderson HR. Childhood antecedents of allergic sensitization in young British adults. J. Allergy Clin. Immunol. 1997; 99:6-12.
22. von Mutius E, Martinez F, Fritsch C, Nicolai T, Reitmeir P, Theimann H. Skin test reactivity and number of siblings. Br Med J. 1994;308:692-5.
23. International Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunc-tivitis, and atopic eczema: ISAAC. Lancet 1998;351:1225-32.
Question No. 2:Is there an association between tuberculosis infections and the development of asthma?
Answer:Existing data show that asthma is less likely to occur in tuberculin skin test (PPD) positive patients. [LEVEL 2]
Summary of Evidence:The association of asthma and tuberculosis (TB) is not as easy to explain. In a study among 867 Japanese school children aged 12-13 years, asthmatic symptoms were one half to one third less likely in positive tuber-culin responders as in negative responders. Remission of atopic symptoms between the ages of 7 and 12 years was 6-9 times more likely in positive tuberculin respond-ers. In the investigation of this possible association, it was established that the positive tuberculin responders had significantly lower levels of the TH2 cytokines IL-4, IL-10, and IL-13 and higher levels of the TH1 cy-tokine IFN-γ.1 Apparently, this ability to stimulate TH1 response suppresses TH2 sensitization which, in turn, curbs the inflammatory cascade in asthma. Therefore, asthmatic subjects may be tuberculin negative although not necessarily uninfected since the skin test reaction is just being naturally suppressed in the asthmatic TH2 phenotype.2,3
Aside from tuberculin reactivity, other indicators ap-pear to prove the purported protection. In one study, the asthma prevalence established with the ISAAC project was correlated with the WHO data on smear-positive tuberculosis (TB) cases in countries where TB information was deemed reliable. There were less questionnaire-based asthma cases wherever active TB prevalence was high.4 Furthermore, there was low asthma occurrence among children in high TB preva-lence areas which may indeed be indicative of asthma protection from M. TB infection.
References:1. Shirakawa T, Enomoto T, Shimazu S, Hopkin J. The in-
verse association between tuberculin responses and atopic
negård Ö. Prevalence of allergy in children in relation to prior BCG vaccination and infection with atypical mycobacteria. Allergy 1998;53:249-54.
3. Yilmaz M, Bingol G, Altinas D, Kendirli SG. Correlation between atopic diseases and tuberculin responses. Allergy. 2000;55:664-7.
4. Von Mutius, et al. International patterns of tuberculosis and the prevalence of symptoms of asthma, rhinitis, and eczema. Thorax. 2000;55:449-53.
Question No. 3:Is there an association between respiratory infections and acute exacerbations of asthma?
Answer:Yes. Respiratory infections have been shown to trigger asthma exacerbations. [LEVEL 1]
Summary of Evidence:Respiratory infections are among the most common triggers for asthma exacerbations.1-2 [LEVEL 1] It seems that once asthma is established, re-exposure to most infections tend to disturb the airway, inducing more symptoms and, in many cases, frank exacerba-tion. Routine antibiotic use is not justified since most infections are viral and self-limiting. Sputum purulence may just reflect eosinophilia and does not by itself justify antibiotic use.
References:1. Nocholson KG, Kent J, Ireland DC. Respiratory vi-
ruses and exacerbations of asthma in adults. Br. Med J. 1993;307:982-6.
2. Busse WW, Lemanske RF Jr, Stark JM, Calhoun WJ. The role of respiratory infections in asthma: In: Holgate ST, Austen KF, Lichtenstein LM, Kay AB, eds. Asthma: Physiology, Immunopharmacology and Treatment. London: Academic Press 1993. pp. 345-53.
Chapter 4
Inhalational Devices
Question no. 1:Is the inhalational route preferred over systemic ad-ministration of asthma medications?
Answer:Yes, inhalational route is preferred over systemic ad-ministration [GRADE A].
Summary of Evidence:The effects of nebulized and intravenous salbutamol in severe and acute asthma were compared in two separate studies. Both studies demonstrated better and faster response rates in the nebulized group.1,2 [LEVEL 1] Decreases in serum potassium were noted more often in the intravenous treated group.1 However, there was a higher incidence of tremors and palpitations in the nebulized group, most likely due to the relatively higher dose of salbutamol used in nebulization.2
Nebulized salbutamol was likewise compared with subcutaneous epinephrine in children with acute at-tacks.3 There were no differences noted in the clinical, physiologic and pulmonary parameters measured in both treatment arms. However, there were more reports of nausea, vomiting, tremors, headaches, palpitations, excitement and pallor in the subcutaneous group.
References:1. Salmeron S, Brochard L, Real H, et al. Nebulized versus
intravenous salbutamol in hypercapneic acute asthma. Am. J. Respir. Crit. Care Med. 1994;149: 1466-70.
2. Swedish Society of Chest Medicine. High dose inhaled versus intravenous salbutamol combined with theophylline in severe acute asthma. Eur Respir J. 1990; 3:163-70.
3. Becker AB, Nelson NA, Simons FER. Inhaled salbutamol versus injected epinephrine in the treatment of acute asthma in children. J Pediatr. 1983;162:465-9.
Question No. 2:Is there a difference among the various inhalational devices in terms of drug deposition, efficacy, safety and promotion of compliance?
Answer:There is no clear evidence that any one device is superior over the other. Although lung deposition studies show superiority of some inhaler devices, it is not clear whether this translates to improved efficacy [LEVEL 2].
Summary of Evidence:The pressurized metered dose inhaler (pMDI), when used with optimal technique, delivers about 10-20% of the nominal per puff dose to the targeted airways.1 In normal patients, lung deposition with directly labeled salbutamol can reach from 21.6 +/- 8.9% while patients with reversible airflow obstruction achieve lung deposi-tion of 18.2 +/- 7.8%.2,3 [LEVEL 3]
Certain maneuvers appear to improve lung deposi-tion. Lung deposition was 18.7% when inhaling from residual volume and 33% when inhaling from 50% of vital capacity.4 [LEVEL 5] Use of spacers increased the amount of drug deposited in the airways in both normal and asthmatic patients (12.4 +/- 3.5% and 19.0 +/- 8.9%, respectively) possibly because spacers act to condition the aerosol, slowing the jet of medication and allowing the propellant to evaporate. In another study on mild to moderate asthmatics, use of a spacer device increased lung deposition to 44.1 +/- 10.1%.5 [LEVEL 2] In comparison, single dose dry powder inhalers (DPIs) show lung deposition between 9.1 and 12.4% 2,3. Some DPIs like the Turbuhaler, deliver 20-30% of the nominal dose in adults,5,6,7 whereas the Diskus delivers about half of that to the lungs with about 1.28 fold dif-ference.8 [LEVEL 2]
Regardless of the significant differences in lung deposi-tion among the inhaler devices, it is not clear whether these differences are clinically important. For broncho-
CPm 8th EDItION ASthmA
57
dilators, especially, only a very small amount of the drug is needed to produce a useful clinical effect. In a Cochrane Review on "Pressurized Metered Dose Inhalers versus All other Handheld Inhalers Devices to Deliver β2-ago-nists Bronchodilators for Non-acute asthma", results show that there were no differences between devices for most clinical outcomes.9 [LEVEL 1]
In any inhaler device used in the treatment of asthma, systemic adverse events may be expected from the drug being absorbed from the lung or from the gastrointestinal tract. In a study on normal subjects treated with inhaled beclomethasone, sytemic activity was greater using a DPI (52%) than using a MDI with a large volume spacer (28%).10 For the two commonly prescribed dry powder inhalers, systemic bioavailability was higher for bude-sonide via Turbuhaler (39%) compared to fluticasone via Diskus (13%), however, plasma cortisol levels did not differ significantly between the two groups. [LEVEL 2]
References: 1. Newman SP. Aerosol deposition considerations in inhala-
SG. Lung deposition patterns of directly labeled salbutamol in normal subjects and inpatients with reversible airflow obstruction. Thorax. 1993;48:506-11.
3. Zainudin BM, Biddescombe M, Tolfree SE, Short M, Spiro SG. Comparison of bronchodilator responses and deposi-tion patterns of salbutamol inhaled from a pressurized metered dose inhaler, as a dry powder and as a nebulized solution. Thorax. 1990;45:469-73.
4. Kohler D, Fleischer W, Matthys H. New method for easy labelling of β2-agonist in the metered dose inhaler with Technetium99 Respiration. 1988;53:65-73.
5. Hirst PH, Bacon RE, Pitcaim GR, Silvasti UK. A compari-son of the lung deposition of budesonide from Easyhaler, Turbuhaler, and pMDI plus spacer in asthmatic patients. Respir. Med. 2001;95:720-7.
6. Everard ML. Drug delivery from Turbuhaler dry powder inhaler to children with cystic fibrosis. Am. J. Respir. Crit. Care Med 1996;153:a70.
7. Thorrson L et al. Lung deposition of budesonide from Turbuhaler is twice that from a pressurized metered dose inhaler. Eur. Respir. J. 1994;7:1839-44.
8. Lipworth BJ, Clark DJ. Comparative lung delivery of sal-butamol given Turbuhaler and Diskus dry powder inhaler devices. Eur. J. Clin. Pharmacol. 1997;53:47-9.
9. Ram FSF, Brocklebank DM, White J, Wright JP, Jones PW. Pressurized metered dose inhalers versus all other handheld inhaler devices to deliver β2-agonists broncho-dilators for non-acute asthma (Cochrane Review). The Cochrane Library 1, 2002. Oxford.
10. Trescoli C, Ward MJ. Systemic activity of inhaled and swallowed beclomethasone dipropionate and the effect of different inhaler devices. Postgrad. Med. J. 1998;74:675-7.
Question No. 3:Is wet nebulization better than other inhalational delivery devices in the acute care setting?
Answer:No. Wet nebulization is not any better than other inha-
lational delivery devices in the acute care setting. In fact, the use of a metered-dose ihaler (MDI) with or without a chamber (valve spacer device) is preferred over the use of a wet nebulizer for patients with mild to moderate asthma. A spacer device is recommended whenever the MDI is used for severe asthma [GRADE A].
Summary of Evidence:Three randomized, double-blind studies compared the efficacy of salbutamol administered either by nebulization (NEB) or by MDI with a spacer in adults with moderate to severe acute asthmatic attacks.1,2,3 all studies consistently demonstrated that NEB and MDI are equally efficacious in improving FEV1, PEFR and clinical symptoms. [LEVEL 1] However the NEB group reported more headaches, palpitations, tremors3 and anxiety1. In another randomized open design trial, the use of NEB, MDI and dry powder was evaluated in acute severe asthma in adults. The three delivery systems were found to improve FEV1 similarly. [LEVEL 1] No evidence of cardiovascular adverse events were seen.4
Two studies involving children compared the effects of NEB and MDI in mild5 and severe6 acute asthma. In both studies, FEV1 was shown to improve with both devices. However the improvement in FEV1 was higher in the severe attack group using the MDI. [LEVEL 2] The NEB group had higher heart rates, while the MDI group reported more dryness of mouth, throat irritation and more coughing. Despite these side effects, most of the children preferred MDI over the NEB because of its shorter administration time.
References:1. Rodrigo C, Rodrigo G. Salbutamol treatment of acute
severe asthma in the ED: MDI vs. hand-held nebulizer. Am. J. Emerg. Med. 1998;16(7).
2. Colacone, Afilalo, Wolkove. A comparison of salbutamol administration by metered-dose inhaler and holding cham-ber or wet nebulizer in acute asthma. Chest 1993;104:835-41.
3. Mandelberg A, Chen E, Noviski N, Priel I. Nebulized wet aerosol treatment in ED − is it essential? Comparison with large spacer device for metered dose inhaler. Chest 1997;112:1501-5.
4. Raimondi C, Schottlender J, Lombardi D, Molfino N. Treatment of acute severe asthma with inhaled albuterol delivered via jet nebulizer, metered dose inhaler with spacer, or dry powder. Chest 1997;112:24-8.
5. Schub S, Johnson DW, Stephen D. Comparison of sal-butamol by metered dose inhaler with spacer versus a nebulizer in children with mild acute asthma. J. Pediatr. 1999;135:22-7.
6. Fuglsang G, Pederson S. Comparison of nebuhaler and nebulizer treatment of acute severe asthma in children Eur. J. Respir. Dis. 1986;69:109-13.
Chapter 5Acute CareQuestion No. 1:What is the ideal first line therapy for asthma exac-erbations?
ASthmA CPm 8th EDItION
58
Answer:Inhaled β2-agonists, due to their rapid onset of action, are recommended as first line therapy in the management of acute asthma [GRADE A].
Summary of Evidence:Inhaled short-acting β2-agonists are the drugs of choice for the initial management of acute exacerbations of asthma. They are effective bronchodilators [LEVEL 1] and have the fewest side effects. The minimum dose of short-acting β2-agonists that will effectively control asthma symptoms should be used2 and they should be used on an as-needed (not regular) basis. [LEVEL 2]
References:1. Guidelines for the Diagnosis and Management of Asthma:
National Asthma Education and Prevention Program. Expert Panel Report 2. Bethesda, MD: National Institutes of Health; National Heart, Lung, and Blood Institute 1997. NIH Publication No. 97-4051A.
2. The British guidelines on asthma management: 1995 review and position statement. Thorax 1997; 52 (Suppl 1):S1-S21.
Question No. 2:Is nebulization better than MDI in the delivery of short-acting β2-agonists during acute asthma exac-erbations?
Answer:No, there is no difference between nebulized and MDI-administered β2-agonist concentrations in the lungs [GRADE A].
Summary of Evidence:In certain studies using salbutamol, doses are calcu-lated on the basis of the percentage of the drug that reaches the lower airway. These studies show that in patients with severe asthma, bronchodilation achieved was equivalent regardless of whether β2-agonist was administered by either MDI-spacer or nebulization.1,2,3,4,5 [LEVEL 2] However, the groups given nebulization showed greater side effects most likely due to increased systemic absorption and higher plasma levels. Hence, the nebulization route should only be used if the patient cannot adequately perform the metered-dose inhalation technique.
References:1. Rodrigo C, Rodrigo G. Salbutamol treatment of acute
severe asthma in the ED: MDI vs. hand-held nebulizer. Am J. Emerg. Med. 1998;16(7).
2. Raimondi C, Schottlender J, Lombardi D, Molfino N. Treat-ment of acute severe asthma with inhaled albuterol delivered via jet nebulizer, metered dose inhaler with spacer, or dry powder. Chest 1997;112:24-8.
3. Mandelberg A, Chen E, Noviski N, Priel I. Nebulized wet aerosol treatment in ED - is it essential? Comparison with large spacer device for metered dose inhaler. Chest 1997;112:1501-5.
4. Giannini D, di Franco A, Bacci E, et al. The protective effect of salbutamol inhaled using different devices on metacholine bronchoconstriction. Chest 2000; 117;1319-23.
5. Hindle M, Newton D, Chrystyn H. Dry powder inha-lers are bioequivalent to metered-dose inhalers. Chest 1995;107;629-33.
Question No. 3:Does systemically administered β2-agonists have a role in acute asthma exacerbations?
Answer:No, there is no evidence to support the use of intra-venously administered β2-agonists in acute asthma exacerbations [GRADE A].
Summary of Evidence:A meta-analysis addressing the issue on the advantages using intravenous (IV) β2-agonists in acute asthma exac-erbations was recently published by Travers et al. In this review, 15 randomized clinical trials spanning a period of 25 years involving 584 patients were analyzed. The authors concluded that the use of IV β2-agonists, either as an adjunct to, or a replacement of, inhaled broncho-dilator therapy appears to offer no clinical benefit in acute asthma. [LEVEL 1]Other issues, however were not addressed in this meta-analysis are:1. Benefit of IV therapy in ventilated patients2. Efficacy in the pediatric population since there were
very few pediatric clinical trials identified3. The efficacy of IV β2-agonists in patients who are
unable to use inhaled β2-agonists 4. The administration of β2-agonists via subcutaneous
route
Reference:1. Travers A, Jones AP, Kelly K, Barker SJ, Camargo CA,
Rowe BH. The intravenous β2-agonists for acute asthma in emergency department. The Cochrane Database of Systematic Reviews. Volume 2001 (Issue 3).
Question No. 4:Should intravenous aminophylline be used as first line drug for acute asthma?
Answer:No, intravenous aminophylline should not be used as a first line for the treatment of acute asthma. [GRADE A]
Summary of Evidence:Intravenous aminophylline offers little benefit over β2-agonist in the treatment of acute asthma.1 In a study assessing the role of aminophylline in adults, 44 asthmatics were initially treated with nebulized β2-agonist, then randomized to receive either an infu-sion of aminophylline or placebo if their peak flow rates did not improve to more than 40% predicted.2 For both groups, nebulized β2-agonist was continued and intravenous methylprednisolone was started. There was no clinical benefit observed in the aminophylline group over the placebo group. Furthermore, higher incidence of side effects was noted in the aminophylline group. [LEVEL 2]
trials of aminophylline compared to placebo in the acute treatment of adults3,4 and children5,6 clearly demonstrate a lack of benefit in major outcomes such as pulmonary functions and admission rates.[LEVEL 1] These studies also identified excessive side effects which outweighed the benefits of aminophylline in this setting.
Currently, aminophylline can only be used as an op-tion for patients where all other modalities had failed (β2-agonists, corticosteroids, ipratropium bromide, magnesium, oxygen, IV salbutamol, etc.) and even then should be used cautiously.7,8
References:1. Littenberg B. Aminophylline treatment in severe, acute
asthma. a meta-analysis. J. Am. Med. Assoc. 1988; 259:1678-84.
2. Murphy DG, McDermott MF, Rydman RJ, Sloan EP, Za-lenski RJ. Aminophylline in the treatment of acute asthma when β2-adrenergics and steroids are provided. Arch Intern Med 1993;153:1784-8.
3. Beveridge R, Grunfeld A, Hodder R, Verbeek P. Guidelines for the emergency management of asthma in adults. Can Med Assoc J. 1996;155:25-37.
4. Coleridge J, Cameron P, Epstein J, Teichtahl H. Intrave-nous aminophylline confers no benefit in acute asthma treated with intravenous steroids and inhaled bronchodila-tors. Aust N. Z. J. Med. 1993;23:348-54.
5. Yung M, South M. Rsandomized controlled trial of aminophylline for severe acute asthma. Arch. Dis. Child. 1998;79:405-10.
6. Goodman D, Littenberg B, O' Connor G, Brooks J. The-ophylline in acute childhood asthma: a meta-analysis of its efficacy. Pediatr Pulmol. 1996;21:211-8.
7. Rossing TH, et al. Emergency therapy of asthma com-parison of the acute effects of parenteral and inhaled sympathomimetics and infused aminophylline. Am. Rev. Respir. Dis. 1980;122:365-71.
8. Murphy DG, McDermott MF, Rydman RJ, Sloan EP, Zalenski RJ. Aminophylline in treatment of acute asthma when β2-agonist and steroid are provided. Arch Intern Med. 1993;153:1784-8.
Question No. 5:Should systemic steroids be used in acute exacerba-tions of asthma?
Answer:Yes. The use of short course systemic steroids has been shown to shorten duration of attacks, prevent relapse in the outpatient treatment of asthma exacerbations and reduce subsequent hospital admissions [GRADE A].
Summary of Evidence:A meta-analysis of studies on systemic steroids clearly shows the benefit of systemic steroids in patients with asthma exacerbation.1,2,3 [LEVEL 1] This review sug-gests that the early administration of corticosteroids may reduce rates of admissions to the hospital. The treatment appears to be most effective in patients who have severe asthma and who have not received inhaled corticosteroids during their initial presentation.
Use of corticosteroids in acute asthma is effective not only in reducing hospital admission rates, but also in improving pulmonary function, and reducing relapses of asthma.4 Since it is difficult to predict which patients
will improve spontaneously, corticosteroids should be offered to every patient who presents with an acute exacerbation of asthma.
References:1. Rowe B, Keller J, Oxman A. Steroid use in the emergency
department treatment of asthma exacerbation: a meta-analy-sis. Am. J. Emerg. Med 1992;10:301-10.
2. Fanta SB, et al. Glucocorticoids in acute asthma: a clinical controlled trial. Am J. Med. 1983;74:845-51.
3. Fiel SB, et al. Efficacy of short-term corticosteroid therapy in outpatient treatment of acute bronchial asthma. Am. J. Med. 1983;75:259-62.
4. Chapman KR, et al. Effect of a short-course of prednisone in the prevention of early relapse after the emergency room treatment of acute asthma. N. Engl. J. Med. 1991;324:788-94.
Question No. 6:In the treatment of acute exacerbations, are oral ste-roids as effective as parenteral steroids?
Answer:Yes, oral steroids are just as effective as parenteral steroids [GRADE A].
Summary of Evidence:The onset of effect in pulmonary function occurs within three hours and reaches a peak effect within 8 to 12 hours following a single dose of oral prednisolone.1 Following intravenous prednisolone, the effect on pulmonary func-tion can be measured after 60 minutes, with maximal improvement occurring in about 5 hours. However, comparative studies have not shown a significant benefit of IV over oral administration in the initial treatment of severe asthma. In fact, systematic reviews show that oral steroids are just as effective as IV steroids in controlling acute asthma.2,3,4 Based on these findings, it is recom-mended that corticosteroids be administered early and by mouth; intravenous treatment should be reserved for those who cannot tolerate food intake.
References:1. Chung KF, Wiggins J, Collins J. Corticosteroids In: Weiss,
EB, Stein M. (eds). Bronchial Asthma− Mechanisms and Therapeutics, 3rd edition. Little Brown, Boston 1993. pp 800-817.
2. Rowe B, Keller J, Oxman A. Steroid use in the emergency department treatment of asthma exacerbation: a meta-analy-sis. Am J. Emerg. Med. 1992;10:301-10.
3. Fanta SB, et al. Glucocorticoids in acute asthma: a clinical controlled trial. Am. J. Med. 1983;74:845-51.
4. Fiel SB, et al. Efficacy of short-term corticosteroid therapy in outpatient treatment of acute bronchial asthma. Am. J. Med. 1983;75:259-62.
Question No. 7:What is the effective dose of corticosteroids for acute asthma?
Answer:The recommended dosage is hydrocortisone 50 mg four-times-a-day for 48 hours, followed by oral prednisone. [GRADE A]
ASthmA CPm 8th EDItION
60
Summary of Evidence:Twelve controlled clinical trials examined the dose-res-ponse effect of corticosteroids. Of these, only 2 stud-ies were able to show a difference between doses.1 [LEVEL 1]
Generally, the literature does not support the use of high dose corticosteroids in acute asthma. Hydrocortisone 50 mg four-times-a-day for 48 hours, followed by oral prednisone, was as effective as 200 mg or 500 mg of hydrocortisone followed by high dose prednisone.2,3 The effective dose of oral prednisolone was established to be between 30-50 mg daily.3 Furthermore, the use of high doses of steroids are associated with increased adverse effects, such as mood disturbance and myopathy.3
References:1. Engel T, Hering JH. Glucocorticosteroid therapy in
acute severe asthma - a critical review. Eur. Respir. J. 1991;4:881-8.
2. Bowler SD, Mitchell CA, Armstrong JG. Corticosteroid in acute severe asthma: effectiveness of low doses. Thorax 1992;47:584-7.
3. Webb JR. Dose response of patients to oral corticoste-roid treatment of exacerbation of asthma. Br. Med. J. 1986;292:1045-7.
Question No. 8:What is the recommended dose interval for oral steroids?
Answer:The recommended dose interval of oral steroids is every 12 hours. [GRADE A]
Summary of Evidence:Since the duration of action of corticosteroids on lung function in unstable asthma is 9 hrs, oral steroids should be given every 12 hours.1,2 One study suggests a decline in the efficacy of steroids over 7-12 hours, so four-times-a-day dosing is suggested until the FEV1/PEFR is 50-60% of predicted, when the dose may be decreased and given twice a day.3
References:1. Ellul-Micallef R, Johansson SA. Acute dose response
studies in bronchial asthma with a new corticosteroid, budesonide. Br. J. Clin. Pharmaco 1983;15:419-22.
2. Beam WR, Weiner DE, Martin RJ. Timing of prednisone and alterations of airways inflammation in nocturnal asthma. Am. Rev. Respir. Dis. 1992;146:1524-30.
3. Kelly, Murphy. Corticosteroids for acute severe asthma. Ann. Pharmaco. 1991;25:72.
Question No. 9:What is the role of ipratropium bromide in the ma-nagement of acute asthma?
Answer:The use of ipratropium bromide alone for acute asthma has been shown to be inferior to β2-agonists in terms of bronchodilating properties. The addition of nebulized ipratropium bromide to salbutamol, however, further improves the FEV1 or PEFR in the initial treatment of acute asthma attacks [GRADE A].
Summary of Evidence:A pooled analysis of three randomized double-blinded clinical trials conducted in the United States, Canada, and New Zealand involving 1,064 patients (18-55 yrs), clearly demonstrated that the addition of ipratropium to salbutamol in the treatment of acute asthma produces a small improvement in lung function, and reduces the risk of the need for additional treatment, subsequent asthma exacerbations, and hospitalizations.1
A meta-analysis of ten randomized, placebo-controlled, double blinded trials involving 1,377 patients (>18 yrs) showed a modest but statistically significant improve-ment in airway obstruction (improvement of FEV1 by 100 mL or a PEFR improvement by 31.5 L/min) among patients who were given a combination of ipratropium bromide plus salbutamol; (either in metered dose or wet nebulization). However, the clinical significance of this improvement remains unclear. It is interesting to note that none of the trials analyzed reported serious adverse effects attributable to either the combination therapy or the single-therapy regimen.2 [LEVEL 1]
A smaller randomized, double-blinded clinical trial in-volving 180 patients compared the effect of salbutamol plus placebo with ipratropium bromide plus salbutamol at higher doses, using metered dose inhaler and spacers at 10-minute intervals for three hours (24 puffs or 2880 µg of salbutamol and 504 µg of ipratropium bromide each hour). The results of this study showed that there may be substantial therapeutic benefit from the addition of ipratropium bromide to salbutamol administered in high doses through MDI plus spacer, particularly in patients with FEV1 less than 30% and with long dura-tion of symptoms before presentation at the Emergency Department.3 [LEVEL 2]
References:1. Lanes SF et al. The effect of adding ipratropium bromide
to salbutamol in the treatment of acute asthma; a pooled analysis of three trials, Chest 1998 Aug; 114(2):365-72.
2. Stoodley RG, Aaron SD, Dales RE. The role of ipratropium bromide in the emergency management of acute asthma exacerbation: a meta-analysis of randomized clinical trials. Ann. Emerg. Med. 1999;34:8-18.
3. Rodrigo GJ, Rodrigo C. First-line therapy for adult patients with acute asthma receiving a multiple-dose protocol of ipratropium bromide plus salbutamol in the emergency department. Am. J. Respir. Crit. Care Med. 2000;161:1862-8.
Research RecommendationFurther studies are needed to determine if the initial use of combined ipratropium bromide and a β2-ago-nist will cause significant clinical improvement in terms of patient's symptom relief, duration of stay in the Emergency Department (ED), and the probability of hospitalization.
CPm 8th EDItION ASthmA
61
Chapter 6
Chronic Management of Asthma
Controller Medications
Question No. 1:Are inhaled corticosteroids effective in the chronic management of asthma?
Answer:Yes. Inhaled corticosteroids (ICS) are the mainstay therapy for persistent asthma [GRADE A].
Summary of Evidence:Long-term treatment with inhaled corticosteroids sup-presses the disease by affecting the underlying airway inflammation. Several studies demonstrate that inhaled corticosteroids are effective in reducing symptoms and exacerbations, improving lung function, and decreas-ing the need for bronchodilator rescue therapy.1,2 a reduction of airway inflammation, manifested both by airway histology findings and improved airway hyperres-ponsiveness (AHR), has also been documented.3,4,5,6
[LEVEL 1]
The outcome parameter responding most rapidly to the initiation of inhaled corticosteroids is symptom relief. The PEF values improve more gradually, while improvements in AHR may continue over many months or even years.1,3,7
References:1. Haahtela T, Jarvinen M, Kava T, Kiviranta K, Koskinen
S, Lehtonen K, Nikander K, Persson T, Reinikainen K, Selroos O, et al. Comparison of a β2-agonist, terbutaline, with an inhaled corticosteroid, budesonide, in newly detected asthma. N. Engl. J. Med. 1991;325:388-92.
2. Busse, WW. What role for the inhaled steroids in chronic asthma? Chest 1993;104:1565-71.
3. Laitinen LA, Laitinen A, Haahtela T. A comparative study of the effects of an inhaled corticosteroid, budesonide, and a β2-agonist, terbutaline, on airway inflammation in newly diagnosed asthma: a randomized, double blind, parallel-group controlled trial. J. Allergy Clin. Immunol. 1992;90:32-42.
4. Jeffrey PK, Godfrey RW, Adelroth E, Nelson F, Rogers A. Johansson SA. Effects of treatment on airway inflamma-tion and thickening of basement membrane reticular col-lagen in asthma. Am Rev. Respir. Dis. 1992;145:890-9.
5. Wilson JW, Djukanovic R, Howarth PH, Holgate ST. In-haled beclomethasone dipropionate downregulates airway lymphocyte activation in atopic asthma. Am J Respir Crit Care Med 1994;149:86-90.
6. Djukanovic R, Wilson JW, Britten KM, Wilson SJ, Walls AF, Roche WR, Howarth PH, Holgate ST. Effect of an inhaled corticosteroid on airway inflammation and symp-toms in asthma. Am Rev. Respir. Dis 1992;145:669-74.
7. Haahtela T, Jarvinen M, Kava T, Kiviranta K, Koskinen S, Lehtonen K, Nikander K, Persson T, Selroos O, So-vijarvi A. Effects of reducing or discontinuing inhaled budesonide in patients with mild asthma. N Engl J. Med. 1994;331:700-5.
Question No. 2:Does early intervention with inhaled corticosteroids result in a better outcome?
Answer:Yes. Anti-inflammatory therapy, specifically inhaled cor-ticosteroids when started early in the course of asthma, diminishes the adverse effects of airway inflammation [GRADE A].
Summary of Evidence:Long standing uncontrolled asthma is associated with lower levels of lung function, greater airway hyperreac-tivity, more symptoms and greater use of β2-agonists.1 Lung function in uncontrolled asthma deteriorates progressively over time and leads to irreversible ob-struction in 80% of elderly patients.2 The decrease in FEV1 among asthmatics is 38 mL/year, compared with 22 mL/year in non-asthmatics. Delay in initiating therapy with inhaled steroids for as little as two years, is associated with a blunted improvement in lung func-tion (FEV1) when compared with patients treated with inhaled corticosteroids one to two years earlier.3 Patients with symptoms of asthma for less than two years prior to initiation of inhaled corticosteroids had higher mean FEV1 and PEF values than those who had symptoms for a longer period of time prior to initiation of inhaled corticosteroid therapy.4 These studies suggest that inhaled corticosteroid therapy, in addition to suppress-ing the disease, may also modify the disease outcome if prescribed early enough and given long enough.3,5,6 [LEVEL 1]
References:1. Agertoft L, Pedersen S. Effects of long-term treatment
with an inhaled corticosteroid on growth and pulmonary function in asthmatic children. Respir. Med. 1994;88:373-81.
2. Lange P, Parner J, Vestibo J, Schnohr P, Jensen G.A 15-year follow-up of ventilatory function in adults with asthma. N. Engl J. Med. 1998;101:720-5.
3. Haahtela T, Jarvinen M, Kava T, Kiviranta K, Koskinen S, Lehtonen K, Nikander K, Persson T, Selroos O, So-vijarvi A. Effects of reducing or discontinuing inhaled budesonide in patients with mild asthma. N Engl J. Med. 1994;331:700-5.
4. Selroos O, Pietinalho A, Loofros AB, Riska H. Effect of early versus late intervention with inhaled corticosteroids in asthma. Chest 1995;108:1228-34.
5. Haahtela T, Jarvinen M, Kava T, Kiviranta K, Koskinen S, Lehtonen K, Nikander K, Persson T, Reinikainen K, Selroos O, et al. Comparison of a β2-agonist, terbutaline with an inhaled corticosteroid, budesonide, in newly detected asthma. N Engl J. Med 1991;325:388-92.
6. Laitinen LA, Laitinen A, Haahtela T. A comparative study of the effects of an inhaled corticosteroid, budesonide, and a β2-agonist, terbutaline, on airway inflammation in newly diagnosed asthma: a randomized, double blind parallel-group controlled trial. J. Allergy Clin. Immunol. 1992;90:32-42.
Question No. 3:Are inhaled steroids safe in the chronic management
ASthmA CPm 8th EDItION
62
of asthma?
Answer:Yes, inhaled steroids are relatively safe. At low to mode-rate doses, inhaled steroids do not frequently exhibit clinically important side effects and provide asthmatics a good risk-benefit profile [GRADE A].
Summary of Evidence:The occurrence and magnitude of adrenal suppression is the most extensively studied systemic effect of inhaled corticosteroids. However, even if moderate and high doses of exogenous corticosteroids affect the hypotha-lamic-pituitary-adrenal (HPA) axis, the resulting adrenal suppression does not appear to be clinically important, as there were no cases of adrenal crisis reported in adults using only inhaled corticosteroids. [LEVEL 3] In children, only two such cases have been reported, each patient having received 400 and 1000 µg of budesonide for several years.1
In patients reporting any bony abnormality from inhaled steroid use, a causal link between the abnormality found and inhaled therapy is often impossible to prove.2 Many such patients would have previously received short- or long-term therapy with oral steroids, which in turn would likely to have effects on bone turnover with resultant structural abnormalities. Even in studies involving patients who have never received exogenous steroids, the bone mineral density (BMD) results are conflicting. Moreover, severe asthma may in itself affect BMD through its effect on the lifestyle of the patient (e.g. less exercise, different dietary habits).
Data on the causal relationship between ICS use and development of cataracts and glaucoma also show conflicting results. Currently available data suggest that the risk of developing posterior subcapsular cataract is not increased in patients being treated with inhaled corticosteroids alone, even when high doses (up to as mean dose of 1,500 µg/day) were used for a mean of nine years of treatment.3 A more recent epidemiologic study conducted in Canada suggested that patients aged 66 and older receiving high-dose inhaled corticosteroids (1,500 µg/day) continuously for at least three months have an increased risk of glaucoma (odds ratio 1.4, CI 1.1-3.0).4 [LEVEL 3] This observation needs further assessment in controlled, preferably prospective studies.
Thinning skins and easy bruisability are unwanted ef-fects that occur in a dose-dependent fashion with inhaled corticosteroids. It appears to have a higher prevalence in older female patients.5,6 The effects are due to a reduction in extracellular ground substance in the dermis possibly because of reduced dermal fibroblast activity. The effects are very rarely seen when total daily doses of inhaled corticosteroid are less than 1,000 µg. [LEVEL 3]
Oral candidiasis, or thrush, has been reported in up to 5% of adult patients receiving inhaled corticosteroids.
When it occurs this can be easily managed by nystatin mouthwash. The risk of occurrence can be greatly re-duced by mouth rinsing with water immediately after inhalation, or with the use of a spacer device (with a MDI) or Turbuhaler.7
Dysphonia, or nonspecific throat symptoms are reported to occur in up to 58% of patients taking inhaled corti-costeroids via MDI.8 These effects were not diminished by the use of spacer devices. However, in studies using the Turbuhaler, the prevalence of this local side effect appears to be lower,9 probably owing to the different po-sition of the vocal cords during the inhalation process.
References:1. Wong J, Black P. Acute adrenal insufficiency associated
with high dose inhaled steroids. Br. Med. J. 1992;304:14-15.
2. Toogood JH, Sorva R, Puolijoki H. Review of the effects of inhaled steroid therapy on bone. Int J Risk Saf Med 1994;5:1-14.
3. Toogood JH, Markov AE, Baskerville J, Dyson C. As-sociation of ocular cataracts with inhaled and oral steroid therapy during long-term treatment of asthma. J. Allergy Clin. Immunol. 1993;91:571-9.
4. Garbe EJ, LeLorier J, Boivin J-F, Suissa S. Inhaled and nasal glucocorticoids and the risk of ocular hypertension or open-angle glaucoma. J. Am. Med. Assoc. 1997;337:8-14.
5. Mak VH, Melchor R, Spiro SG. Easy bruising as a side ef-fect of inhaled corticosteroids. Eur Respir. J. 1992;5:1068-74.
6. Roy A, Leblanc C, Paquette L, Ghezzo H, Cote J, Cartier A, Malo JL. Skin bruising in asthmatic subjects treated with high doses of inhaled steroids: frequency and association with adrenal function. Eur Respir. J 1996;9:226-31.
7. Boulet LP. Summary of recommendations from the Cana-dian Asthma Consensus Report. Can. Med. Assoc J. 1999; 161(11):S1-S12.
8. Williamson IJ, Matusiewicz SP, Brown PH, Greening AP, Cromptom GK. Frequency of voice problems and cough in patients using pressurized aerosol inhaled steroid prepara-tions. Eur Respir. J. 1995;8:590-7.
9. Selroos O, Backman R, Forsen KO, Lofross AB, Niemisto M, Pietinalho A, Aikas C, Riska H. Local side effects during 4-year treatment with inhaled corticosteroids: a comparison between pressurized metered-dose inhalers and turbuhaler. Allergy 1994; 49:888-90.
Question No. 4:Does the addition of long-acting bronchodilator to inhaled corticosteroid produce better control of asthma than corticosteroid alone?
Answer:Yes, combining a long-acting inhaled β2-agonist like salmeterol or formoterol with inhaled corticosteroids leads to greater improvement in the control of symp-toms and lung function among patients with persistent asthma [GRADE A].
Summary of Evidence:This recommendation is based upon the results of two
CPm 8th EDItION ASthmA
63
landmark placebo-controlled clinical studies. Greening et. al. compared the effect of adding 50 µg of salmeterol with doubling the steroid dose in asthmatics who remain symptomatic despite maintenance treatment with low dose inhaled beclomethasone dipropionate (BDP) at 400 µg. This study showed that the increase in mean morning PEF was greater when salmeterol was added than when BDP dose was doubled.1 [LEVEL1] Wool-cock et al performed a similar study on asthmatics using higher doses of BDP. Compared to doubling the dose of BDP, the addition of salmeterol to moderate doses of BDP improved lung function and increased the number of symptom-free days.2 [LEVEL 1] These two studies clearly demonstrate that regular, long-acting β2-agonist therapy improves lung function in patients already on inhaled glucocorticoids.
Subsequent studies3,4 strengthen further the conclusion that, in patients not ideally controlled on moderate doses of inhaled steroids, the best clinical decision is to add a long-acting β2-agonist. However, fears have been raised about the effects of regular treatment with long-acting β2-agonists on tolerance or its ability to mask an increase in airway inflammation because of the lower doses of inhaled corticosteroids used. This concern was addressed adequately in the Formoterol and Corticosteroid Establishing Therapy (FACET) study.5 The FACET study has shown that inhaled formoterol and budesonide have independent effects on asthma exacerbation rates and that formoterol improves lung function. Furthermore, these effects were maintained over the entire one-year study period with no adverse safety implications. Regular treatment with formoterol combined with budesonide did not cause any long-term loss of control of asthma. Previous studies did show that there were no signs of worsening of disease or tolerance to the effects of long-acting β2-agonist (LABA) with regard to any clinical or functional variable examined.6-9 [LEVEL 1]
References:1. Greening AP, Ind PW, Northfield M, Shaw G. Added
salmeterol versus higher dose corticosteroid in asthma patients with symptoms on existing inhaled corticosteroid. Lancet 1994;334:219-24.
2. Woolcock A, Lundback B, Ringdal N, Jacques L. Com-parison on addition of salmeterol to inhaled steroids with doubling the dose of inhaled steroids. Am J. Respir. Crit. Care Med. 1996;153:1481-8.
3. Ind PW, Dal Negro R, Colman N, et al. Inhaled flutica-sone propionate and salmeterol in moderate adult asthma I: Lung function and symptoms (abstract). Am J. Respir. Crit. Care Med. 1998;157(Pt 2) Suppl; A416.
4. Ind PW, Dal Negro R, Colman N, et al. Inhaled fluticasone propionate and salmeterol in moderate adult asthma II: Exacerbations (abstract). Am J. Respir. Crit. Care Med. 1998; 157 (Pt 2) Suppl; A415.
5. Pauwels RA, Claes-Goran L, Postma DA, Tattersfield AE, O'Byrne P, Barnes PJ, Ulman A. Effect of inhaled formoterol and budesonide on exacerbations of asthma. N. Engl. J. Med. 1997;337:1405-11.
6. Kalrea S, Swystun VA, Bhagat R, Cockroft DW. Inhaled corticosteroids do not prevent the development of toler-ance to the bronchoprotective effect of salmeterol. Chest
1996;109;953-6.7. O'Connor BJ, Aikman SL, Barnes PJ. Tolerance to the non-
bronchodilator effects of inhaled β2-agonists in asthma. N. Engl. J. Med. 1992;327:1204-8.
8. Cockroft DW, Swystun VA, Bhagat R. Interaction of inhaled β2-agonist and inhaled corticosteroid on airway responsiveness to allergen and methacholine. Am J. Respir. Crit. Care Med. 1995;152:1485-9.
9. Yates DH, Sussman HS, Shaw MJ, Barnes PJ, Chung KF. Regular formoterol treatment in mild asthma: effect on bronchial responsiveness during and after treatment. Am J. Respir. Crit. Care Med. 1995; 152:1170-4.
Question No. 5:Is there a role for fixed dose combination therapy (long-acting β2-agonist and inhaled corticosteroids) in the management of persistent asthma?
Answer:Yes, recent studies suggest that additional clinical benefit can be achieved with fixed dose combination therapy of LABA and ICS [GRADE A].
Summary of Evidence:Numerous researches, all randomized, double-blind, placebo-controlled and parallel group design com-pared the effects of the fixed combination therapy of salmeterol and fluticasone to either steroid alone (either BDP, budesonide or fluticasone), salmeterol alone and placebo. These studies unequivocally demonstrated that addition of an inhaled LABA to the ICS treatment im-proves all aspects of asthma control.1,2,3,4 [LEVEL 1]
The additional clinical benefit derived from the fixed-combination therapy results not only from the LABA-glu-cocorticoid interaction but also from the steroid-induced transcription of β2-adrenoceptor gene with the resultant increased synthesis of the β2-receptor protein. This in-teraction between the LABA and the ICS increased the efficacy of both drugs. Fixed dose combination therapy has likewise been found to be beneficial in terms of other aspects of asthma management such as cost of treatment3 and patient compliance.5,6,7,8,9 [LEVEL 2]
References:1. Kavuru, et al. Salmeterol and fluticasone propionate com-
bined in a new powder inhalation device for the treatment of asthma: a randomized, double-blind placebo-controlled trial. J Allergy Clin Immunol 2000; 105:1108-16.
2. Lundback B, et al. Cost-effectiveness of salmeterol/fluti-casone propionate combination product 50/250 µg twice daily and budesonide 800 µg twice daily in the treatment of adults and adolescents with asthma. Respir. Med. 2000;94:724-32.
3. Jenkins C, et al. Salmeterol/fluticasone propionate com-bination therapy 50/250 µg twice daily is more effective than budesonide 800 µg twice daily in treating moderate to severe asthma. Respir. Med. 2000; 94:715-23.
4. Shapiro G, et al. American Thoracic Society. Combined salmeterol 50 µg and fluticasone propionate 250 µg in the diskus device for the treatment of asthma. Am J. Respir. Crit. Care Med. 2000;161:527-634.
5. van den Berg NJ, et al. Salmeterol/fluticasone propionate
ASthmA CPm 8th EDItION
64
(50/100 µg) in combination in a diskus inhaler (Seretide) is effective and safe in children with asthma. Pediatr Pulmol. 2000;30:97-105.
6. Bateman ED, et al. Salmeterol/fluticasone combination inhaler - a new effective and well-tolerated treatment for asthma. Clin Drug Invest 1998;16(3):193-201.
7. Chapman K, et al. Salmeterol and fluticasone propionate (50/250 µg) administered via combination diskus inhaler: as effective when given via separate diskus inhalers. Can Respir J. 1999; 6(1):45-51.
8. Aubier M, et al. Salmeterol/fluticasone propionate (50/500 µg) in combination in a diskus inhaler (Seretide) is effec-tive and safe in the treatment of steroid-dependent asthma. Respir Med 1999;93:876-84.
9. Chrystyn H. The diskus inhaler: a review of its phar-maceutical and clinical performance. Clin. Drug Invest. 1999;18(4):287-96.
Question No. 6:Can oral steroids be used as alternative controller to the combination of inhaled corticosteroids and long-acting β2-agonist in persistent asthma?
Answer:Although prednisolone 7.5 to 12 mg/day is as efficacious as inhaled steroid (800-2000 µg/day), no study has been made on how oral steroids compare to the ICS plus LABA combination in controlling persistent asthma.
Summary of Evidence:Daily doses of prednisolone 7.5-10 mg/day are equiva-lent to moderate to high doses of inhaled corticosteroids. On the other hand, alternate-day doses of oral steroids and doses of less than 5 mg/day appear to be less effec-tive than low to moderate doses of inhaled steroids. No published information about the long-term side effects of oral steroids in asthma is available, thus, if there is no alternative to oral steroids, the lowest effective dose (which appears to be 7.5 mg/day) should be given.1 [LEVEL 2]
Reference:1. Mash B, Bheekie A, Jones PW. Inhaled versus oral ste-
roids for adults with chronic asthma (Review) Cochrane Database of Systemic Reviews. Vol 2000 (issue 3).
Research Recommendation
A well-designed study should be conducted to de-termine how oral steroids alone compare with com-bined ICS with LABA in controlling the symptoms and improving the lung function of patients with persistent asthma.
Question No. 7:Does theophylline have a role in the management of chronic asthma?
Answer:Yes, theophylline has a role in the management of
chronic asthma, but because of its low bronchodilating effect and potential for significant adverse effects, it should not be used as first line therapy [GRADE B].
Summary of Evidence:Theophylline is a commonly prescribed bronchodilator therapy, preferred by some physicians because of the oral administration and relatively low cost.
Recent studies indicate that theophylline, when added to a medium dose or low dose of inhaled steroids (Budesonide (BUD) 800 µg/day or BPD 400 µg/day), was more effective in controlling asthma than doubling the inhaled steroid dose.1,2 [LEVEL 3] Theophylline was also found to be useful for the control of nocturnal asthma because it improved airflow during the early hours of the morning and reduced bronchial hyper-reactivity.3,4 It was effective when given as a nocturnal slow-release (SR) preparation in patients with nocturnal asthma and when wheezing is not responsive to inhaled long-acting β2-agonists. [LEVEL 2]
Recent evidence shows that theophylline improves lung function at serum levels below the accepted therapeutic range (<10 mg/L) in patients with moderate asthma who are already on high dose inhaled steroids.5,6 [LEVEL 3] Furthermore, withdrawal of theophylline from an asthma regimen results in an increase in asthmatic symptoms and a need for higher dose of oral steroids.7 In one study, theophylline was found to be as effective as beclomethasone even when serum theophylline con-centrations were lower than traditional levels of normal therapeutic range for bronchodilation.8
Theophylline was also found to exhibit anti-inflam-matory effects. In patients with atopic asthma given an allergen challenge, theophylline appeared to inhibit the late response to allergen and cause a reduction in bronchial mucosal eosinophils.9 [LEVEL 3]
Common adverse effects of theophylline include nausea, vomiting, and other gastrointestinal symptoms. Cardio-pulmonary effects include tachycardia, arrhythmias, and occasionally, stimulation of respiratory center. Appropri-ate dosing and monitoring can generally avoid these. A general approach is to aim for a steady state serum concentration of between 5-15 µg/mL. Previous studies have shown that theophylline levels of 8.7 µg/mL were achieved in patients given slow-release theophylline in a dose of 500-750 mg/day.1
Doxofylline is a newer xanthine derivative with claims of equivalent bronchodilating property and less side ef-fects.11,12 However, there is very little available evidence to support this. Data to support its anti-inflammatory effects is likewise lacking.
References: 1. Evans DJ, Tylor DA, Zetterstrom O, et al. A comparison of
low-dose inhaled budesonide plus theophylline and high-dose inhaled budesonide for moderate asthma. N. Engl J. Med 1997;337:1412-8.
2. Ukena D, Harnest U, Sakalauskas R, et al. Comparison of
CPm 8th EDItION ASthmA
65
addition of theophylline to inhaled steroid with doubling of the dose of inhaled steroid in asthma. Eur Respir J. 1997;10:2754-60.
3. Milgrom H, Barnhart A, Gaddy J, Bush W. The effect of a 24-hour sustained theophylline (Uniphyl) on diurnal varia-tions in airway responsiveness (abstract). J. Allergy Clin. Immunol 1990;85:144.
4. Bush RK. Nocturnal asthma: mechanism and the role of theophylline in treatment. Postgrad Med J. 1991; 67 (Suppl):S20-S24.
5. Kidney J, Dominguez M, Taylor PM, et al. Immunomo-dulation by theophylline in asthma. Demonstration by withdrawal of therapy. Am J. Respir. Crit. Care Med 1995;151:1907-14.
6. Nassif EG, Weinberger M, Thompson R, Huntley W. The value of maintenance theophylline in steroid-dependent asthma. N. Engl J. Med 1981;304:71-5.
7. Brenner M, Berkowitz R, Marshall N, Strunk RC. Need for theophylline in severe steroid-requiring asthmatic. Clin. Allergy 1988;18:143-50.
8. Chung KF. Theophylline in asthma - evidence for disease modifying properties. Clin. Exp. Allergy 1996;26:22-7.
9. Sullivan P, Bekir S, Jaffar Z, et al. Anti-inflammatory ef-fects of low-dose theophylline in atopic asthma. Lancet 1994;343:1006-8.
10. Ernst P, Fitzgerald JM, Spier S. Canadian Asthma Con-sensus Conference Summary of recommendations. Can. Respir. J. 1996;3(2):89-100.
11. Dini FL, Cogo R. Doxofylline: a new generation xanthine bronchodilator devoid of major cardiovascular adverse ef-fects. Curr Med Res Opin 2001;16(4);258-68.
12. Gross E. Doxofylline: drug profile and review of clinical studies. Eur Rev. Med. Pharm. Sci. 1988:10:1-16.
Question No. 8:What is the role of anti-leukotrienes in asthma treat-ment?
Answer:Anti-leukotrienes (Anti-LTs) or leukotriene-receptor an-tagonists (LTRAs) may be given as a controller drug for mild persistent asthma whenever inhaled corticosteroid (ICS) are not in use. [GRADE A]
For moderate to severe persistent asthma, they may be used as an add-on therapy. [GRADE B]
Summary of Evidence:Studies comparing anti-LTs and ICS consistently show the latter to be the more potent controller.1,2 [LEVEL 2] However, there were some non-ICS-responders who showed significant improvement with anti-LTs. Further-more, some patients clearly preferred anti-LTs over ICS despite the greater improvement of lung function as-sociated with the steroid.3 The oral formulation and the positive feedback of symptom relief argue for the use of the anti-LTs as first-line controller therapy. Therefore, under selected circumstances, particularly when inhaled corticosteroids are not available or the patient refuses to take ICS, the anti-LTs would be suitable first-line or substitute controllers. [LEVEL 4]
Among patients already on low or high dose inhaled steroids and who are still symptomatic, the addition of anti-LTs provides for additional control.5-8 Several studies show that asthma symptoms and lung function
improved, and that frequency of exacerbations were significantly reduced. Furthermore, the use of anti-LT can facilitate dose reduction of the maintenance inhaled and/or oral steroids.9,10,11 [LEVEL 2]
References: 1. Malmstrom K, Rodriguez-Gomez G, Guerra J, et al. Oral
montelukast, inhaled beclomethasone, and placebo for chronic asthma: a randomized controlled trial. Monte-lukast/Beclomethasone Study Group. Ann Intern. Med 1999;130:487-95.
2. Laitinen LA, Naya IP, Binks S, Harris A. Comparative efficacy of zafirlukast and low dose steroids in asthmatics on prn β2-agonists. Eur Respir J. 1997; 10:419S.
3. Ringdal N, Whitney JG, Summerton L. A comparison of patient preference for treatment with oral zafirlukast or inhaled beclomethasone. Eur Respir J. 1997; 10:437S.
4. Reiss TF, Chervinsky P, Edwards T, Dockhorn R, Nayak A, Hess J et al. Montelukast (MK-0476), a CysLT1 receptor antagonist, improves asthma outcomes over a three-month period. Am J. Respir. Crit. Care Med 1997.
5. Dahlén B, Nizankowska E, Szczeklik A, Zetterström O, Bochenek G, Kumlin M et al. Benefits from adding the 5-lipoxygenase inhibitor zileuton to conventional therapy in aspirin-intolerant asthmatics. Am J. Respir. Crit. Care Med 1998;157:1187-94.
6. Dahlén SE, Malmström K, Kuna P, Nizankowska E, Kowalski M, Stevenson D, et al. Improvement of asthma in aspirin-intolerant patients by montelukast (MK-0476), a potent and specific CysLT1 receptor antagonist: correla-tions with patient's baseline characteristics. Eur Respir J 1997;10:419.
7. Virchow JC, Hassall SM, Summerton L, Harris A. Im-proved asthma control over 6 weeks with Accolate (zaf-irlukast) in patients on high-dose inhaled corticosteroids. J. Invest. Med. 1997;10:286A.
8. Israel E, Cohn J, Dubé L, Drazen JM and the Zileuton Clinical Trial Group. Effect of treatment with zileuton, a 5-lipoxygenase inhibitor in patients with asthma. J. Am. Med. Assoc. 1996;275:931-6.
9. Tamaoki J, Kondo M, Sakai N, Nakata J, Takemura H, Na-gai A, et al. Leukotriene antagonist prevents exacerbation of asthma during reduction of high-dose inhaled corticoste-roid. Am J. Respir. Crit. Care Med. 1997;155:1235-40.
10. Bateman ED, et al. A multicentre study to assess the steroid-sparing potential of Accolate (zafirlukast; 20 mg b.d.) Allergy 1995; 50 (Suppl 26): Abs P-0709.
Question No. 9:Are anti-leukotrienes comparable with the currently available add-on controllers?
Answer:Anti-LTs have less bronchodilating effect and symptom relief compared to inhaled long acting bronchodila-tors1 [LEVEL 1] but have similar effects compared to theophylline. [LEVEL 4]. However, anti-LTs have greater anti-inflammatory activity over both LABA and theophylline. [LEVEL 2]
Summary of Evidence:The addition of either anti-LTs or LABA to inhaled steroids as maintenance therapy has resulted in less
ASthmA CPm 8th EDItION
66
asthma symptoms, better quality of life and fewer exacer-bations.1,2-4,5,6 [LEVEL 1] In a study comparing mon-telukast and salmeterol as add-on therapy in subjects on concurrent ICS, there was no difference in asthma exacerbation and adverse reaction rates. Before and after within group analysis, nonetheless, showed that both treatments are equally effective.7 [LEVEL 3]
In a double blind randomized study involving 197 pa-tients with mild exercise-induced bronchospasm (EIB), wherein 25% of the subjects were on concurrent ICS, salmeterol protection waned significantly more than montelukast by the 4th and 8th week.7 In contrast, a study by Busse on 289 adult subjects with mild to moderate asthma, 80% of whom were on concurrent ICS, showed that, when compared to zafirlukast, salmeterol produced significantly greater improvement in A.M. and P.M. PEFR, less diurnal PEFR variability, fewer symptoms, and less prn use of short-acting β2-agonist (SABA).5 [LEVEL 3]
Based on these head-on comparative studies, LABA is the preferred drug over anti-LTs in the majority of asthmatics still symptomatic despite use of ICS. Some patients, particularly those with EIB and those in whom inhaler compliance is not assured, may respond better to anti-LTs. Anti-LTs should be considered if patients on both ICS and LABA are still not controlled.
Since anti-leukotrienes appear to modulate leukotriene activity whose production is not decreased by ICS, it naturally poses as a more attractive anti-inflammatory agent than LABA or theophylline. The bronchodilator effects seen with Zileuton, a leukotriene synthesis modi-fier, were greater than that reported with theophylline given on top of ICS.8 No other head-on comparison of these two class of compounds as add-on therapy has been done.
References:1. Busse W. Comparison of inhaled salmeterol and oral zaf-
irlukast in patients with asthma. J. Allergy Clin. Immunol. 1999;103:1075-80.
2. Reiss TF, Chervinsky P, Dockhorn RJ, et al. Montelukast, a once-daily leukotriene receptor antagonist, in the treatment of chronic asthma: a multicenter, randomized, double-blind trial. Montelukast Clinical Research Study Group. Arch Intern. Med 1998; 158: 1213-20.
3. Dahlén B, Nizankowska E, Szczeklik A, Zetterström O, Bochenek G, Kumlin M et al. Benefits from adding the 5-lipoxygenase inhibitor zileuton to conventional therapy in aspirin-intolerant asthmatics. Am J. Respir. Crit. Care Med. 1998;157:1187-94.
4. Dahlén SE, Malmström K, Kuna P, Nizankowska E, Kowalski M, Stevenson D et al. Improvement of asthma in aspirin-intolerant patients by montelukast (MK-0476), a potent and specific CysLT1 receptor antagonist: correla-tions with patient's baseline characteristics. Eur Respir J. 1997;10:419.
5. Virchow JC, Hassall SM, Summerton L, Harris A. Im-proved asthma control over 6 weeks with Accolate (zafir-lukast) in patients with high-dose inhaled corticosteroids. J. Invest Med. 1997;10:286A.
6. Villaran C, O'Neill S, Helbling A, et al. Montelukast com-
pared to salmeterol in the treatment of exercise-induced asthma (EIA). Eur Respir. J. 1998; 12 (Suppl): 361S.
7. Evans DJ, Taylor DA, Zetterstrom O, Chug KF, O'Connor BJ, Barnes PJ. A comparison of low-dose inhaled budesonide plus theophylline and high-dose in-haled budesonide for moderate asthma. N. Engl. J. Med 1997;337:1412-8.
8. Schwartz HJ, Petty T, Dube LM, Swanson LJ, Lancaster JF. A randomized controlled trial comparing zileuton with theophylline in moderate asthma. Arch Intern Med 1998;158:141-8.
Question No. 10:How safe are the anti-leukotrienes?
Answer:Anti-leukotrienes (anti-LTs) are safe drugs even for prolonged use [GRADE A].
Summary of Evidence:The Antileukotriene Working Group has clearly es-tablished the safety of anti-LTs even when given for prolonged periods of time.1 [LEVEL 1] an analysis of four 13-week RCTs of similar methodology assess-ing efficacy and safety of anti-LTs, showed that of the 1484 asthmatics, 560 or 64% in the zafirlukast group and 391 (65%) in the placebo group developed adverse effects.2 In one of these studies, extended by Grossman to 39 more weeks, the most common adverse events noted were pharyngitis (zafirlukast and placebo 24.2%) and headache (zafirlukast, 13.0%; placebo, 10.9%).3,4
A similar study assessing safety and tolerability of montelukast reported the same frequency of adverse reactions.5 [LEVEL 1]
Anti-LTs should be used with caution among patients with liver disease, although more recent studies failed to implicate direct hepatotoxicity with leukotriene receptor antagonist use. Churg-Strauss syndrome, a rare severe eosinophilic granulomatous lung disease, has been re-ported to be associated with anti-LT use (1:20,000 asthma cases), noted particularly during the period of oral steroid tapering.6,7,8,9 It was proposed that this situation may be due to the unmasking, rather than causation of Churg-Strauss syndrome. The syndrome may have mistakenly diagnosed as asthma and initially controlled with oral steroids. Once the oral steroid dose has decreased during tapering, then the syndrome resurfaced.9-11
References:1. Spector SL. Safety of antileukotriene agents in asthma
management. AntiLeukotriene Working Group. Ann Al-lergy Asthma Immunol. 2001;86(Suppl):18-23.
2. Tashkin DP, Nathan RA, Howland WC, et al. An evaluation of zafirlukast in the treatment of asthma with exploratory subset analyses. J. Allergy Clin. Immunol 1999;103:246-54.
3. Fish JE, Kemp JP, Lockey RF, et al. Zafirlukast for symp-tomatic mild-to-moderate asthma: a 13-week multicenter study. Clin Therap. 1997;19:675-90.
4. Grossman J, et al. Long-term safety and efficacy of zaf-irlukast in the treatment of asthma interim results of an open-label extension trial. Ann Allergy Asthma Immunol 1999;82:361-9.
5. Knoor B. Matz J, Bernstein JA, et al. Montelukast for
CPm 8th EDItION ASthmA
67
chronic asthma in 6-to 14-year-old children: a randomized double-blind trial. J. Am. Med Assoc. 1998; 279:1181-6.
6. Weschler ME, Garpestad E, Flier SR, et al. Pulmonary infiltrates, eosinophilia, and cardiomyopathy following corticosteroid withdrawal in patients receiving zafirlukast. J. Am. Med Assoc. 1998;279:455-7.
7. Knoell DL, Lucas J, Allen JN. Churg-Strauss syndrome associated with zafirlukast. Chest 1998;114:332-4.
8. Franco J, Artes MJ. Pulmonary eosinophilia associated with montelukast. Thorax 1999;54:558-60.
9. Weschler ME, Finn D, Gunawardena D, et al. Churg-Strauss syndrome in patient receiving montelukast as treatment for asthma. Chest 2000;117:708-13.
10. Churg A, Brallas M, Cronin SR, Churg J. Formes frustes of Churg-Strauss syndrome. Chest 1995;108:320-3.
11. Churg A, Churg J. Steroids and Churg-Strauss syndrome. Lancet 1998;352:32-3.
Question No. 11:What is the recommended dose for anti-leukotrienes in asthma?
Answer:Below are the recommended initial adult dosages of the available anti-LTs in the Philippine market: Montelukast: 10 mg (5 - 10 mg) H.S., P.O. Zafirlukast: 20 mg (range: 20 - 80) b.i.d. (one hour
before or two hours after a meal) P.O.In both preparations, higher dosages have been used, but only modest additional improvements of asthma parameters were seen.1,2 The effective dose is continued up to 3 months after which, the anti-LT can be stopped if asthma control is good. [LEVEL 4]
References:1. Noonan MJ, Chervinsky P, Brandon M, et al. Montelukast,
a potent cysteinyl leukotriene antagonist, causes dose related improvements in chronic asthma. Eur Respir J. In press.
2. Altman. A placebo-controlled, dose-ranging study of montelukast, a cysteinyl leukotriene-receptor antagonist. J. Allergy Clin. Immunol. 1998;102:50-6.
Reliever Medications
Question No. 1:Are inhaled short-acting β2-agonists administered reg-ularly safe and effective for maintenance therapy?
Answer:No, inhaled short-acting β2-agonists (SABA) adminis-tered regularly is neither safe nor effective as mainte-nance therapy. Regular use of SABA has been shown to increase hyperresponsiveness, significantly decrease asthma control, cause deterioration in the objective measures of pulmonary function, and increase mortal-ity. Therefore, inhaled SABA should only be used on an 'as-needed' basis [GRADE A].
Summary of Evidence:A 26-week, randomized, multi-center, double-blind placebo-controlled trial conducted by the National In-
stitute of Health in patients with mild asthma, compared effects of regularly scheduled salbutamol with as-needed dosing.1 There were no deleterious nor beneficial effects derived from the regular use of inhaled salbutamol be-yond those derived from the use of the drug on as-needed basis. [LEVEL 1] Lower values in the evening peak flow and short-term bronchodilator response to inhaled salbutamol were noted in the regularly scheduled group, but these were judged to be not clinically significant. During a withdrawal period in the study, there was no deterioration in lung function observed in either group. In one of the treatment groups, an increase in airway hyperresponsiveness was observed after two weeks of regular therapy. The study concluded that inhaled salbutamol should be prescribed for patients with mild asthma on an 'as-needed' basis.
Similar studies done by Sears2 and Cockroft,3 also showed that regular four-times-a-day treatment with SABA is not more beneficial than its use on a prn basis. Although regular use of SABA showed a consistent trend toward more symptoms, reduced lung function and increased airway responsiveness, the differences for all outcomes except airway hyperresponsiveness, did not achieve significant levels.3 [LEVEL 1]
The more potent SABA, like fenoterol, seem to have more adverse effects when taken regularly. Several studies demonstrated clear evidence that regular use of fenoterol was associated with increased morbidity and mortality due to increased severity of asthma.4,5,6,7 In New Zealand, the use of high-dose fenoterol was associated with a second epidemic of asthma mortality during the late 1970s. Case control studies subsequently confirmed that fenoterol use was a significant predictor of mortality independent of asthma severity.7 Other stud-ies further demonstrated that the higher risk associated with fenoterol was attributed solely to the use of higher doses,8,9 and that regular use of fenoterol resulted in poorer asthma control, compared with as-needed use.10,11 The decline in the use of fenoterol in New Zealand in 1990 led to reduction in both asthma mortality and hos-pitalizations for severe asthma. These findings suggested that the excess mortality was related to severe asthma exacerbated by fenoterol use.10,11,12 a meta-analysis of epidemiological studies concluded that the apparent as-sociation between β2-agonist use and increased mortality applied only to nebulized therapy.13 [LEVEL 1]
References:1. Guidelines for the Diagnosis and Management of Asthma.
National Asthma Education, and Prevention Program: Expert Panel Report 2. Bethesda, MD: National Institutes of Health; National Heart, Lung, and Blood Institute 1997, NIH Publication No. 97-4051A.
2. Sears MR, Taylor DR. The β2-agonist controversy. Observations, explanations and relationships to asthma epidemiology. Drug Safety 1994;11:259-83.
3. Cockroft DW, McParland CP, Britto SA, et al. Regular inhaled salbutamol and airway responsiveness to allergen. Lancet 1993;342:833-7.
4. Canadian Asthma Consensus Report. Can Med Assoc J
ASthmA CPm 8th EDItION
68
1999;161(11 Suppl):S28-S30. 5. Cockroft DW, O'Byrne PM, Swystun VA, Bhagat R.
Regular use of inhaled salbutamol and the allergen-in-duced late asthmatic response. J. Allergy Clin. Immunol. 1995;96:44-9.
6. Inman MD, O'Byrne PM. The effect of regular inhaled albuterol on exercise-induced bronchoconstriction. Am. J. Respir. Crit. Care Med. 1996;153-65-9.
7. Crane J, Pearce N, Flatt A, et al. Prescribed fenoterol and death from asthma in New Zealand, 1981-1983: case control study. Lancet 1989;1:917-22.
8. Spitzer WO, Suissa S, Ernst P, et al. The use of β2-agonists and the risk of death and near death from asthma. N. Engl. J. Med. 1992;326:501-6.
9. Suissa S, Ernst P, Boivin J-F, Horwitz RI, Habbick B, Cockroft D, et al. A cohort analysis of excess mortality in asthma and the use of inhaled β2-agonists. Am. J. Respir. Crit. Care Med 1994;149:604-10.
10. Sears MR, Taylor DR, Print CG. Regular inhaled β2-ago-nist treatment in bronchial asthma. Lancet 1990; 336:1391-6.
11. Taylor DR, Sears MR, Herbison GP, et al. Regular inhaled β2-agonist in asthma: effects on exacerbations and lung function. Thorax 1993;48:134-8.
12. Pearce N, Beasley R, Crane J, et al. End of New Zealand asthma mortality epidemic. Lancet 1995;345: 41-4.
13. Mullen M, Mullen B, Carey M. The association between β2-agonist use and death from asthma. A meta-analytic integration of case-control studies. J. Am. Med Assoc 1993;270:1842-5.
Question No. 2:Is there a role for long acting β2-adrenergic agonists as rescue medication?
Answer:Yes, long-acting β2-agonists with rapid onset of action may be used as rescue medication [GRADE B].
Summary of Evidence:Of the two inhaled LABA available, formoterol has a more rapid onset of action, and its role as rescue medication has been investigated extensively. Studies have shown that it relieves bronchoconstriction as rap-idly as salbutamol1 and as effectively as terbutaline.2,3,4 [LEVEL 2]
A study by Ind comparing the clinical efficacy and safety of terbutaline and formoterol used as rescue medica-tions3 showed that both drug were similarly effective. The probability of not having a severe exacerbation was similar for both groups and the difference was not sta-tistically significant. For both groups, the mean number of rescue inhalations used was similar. In another study by Tattersfield et al, patients who used formoterol as rescue medication had 38% fewer severe exacerbations per patient than those who used terbutaline.4
Furthermore, as-needed formoterol use significantly increased the time to first severe exacerbation over a period of 12 weeks compared with terbutaline. [LEVEL 2]
The safety of 'as-needed' formoterol was also evaluated and compared to that of terbutaline. These studies show that formoterol, when used as rescue medication, was as
safe and well tolerated as terbutaline. No relevant diffe-rences were noted between treatments in terms of adverse events, ECG changes, serum potassium concentrations, or other potential systemic side effects. Moreover, no toler-ance to the bronchodilating effect was observed.
Another study evaluated the initial effects of treatment with formoterol in children over 12-16 years using an open, randomized, and parallel-group design.5 This study likewise show that, in children, treatment with formoterol was as well tolerated as treatment with terbutaline.
References:1. Politiek MJ, Boorsma M, Aalbers R. Comparison of
formoterol, salbutamol and salmeterol in methacho-line-induced severe bronchoconstriction. Eur Respir J. 1999;13:988-92.
2. Malolepszy J, Boszormeny Nagy G, Brander R., Larson P. Formoterol 90 µg via Turbuhaler was safe in patients with acute bronchoconstriction. Eur Respir J. 1998:12 (Suppl 28):323s.
3. Ind P, Borszormenyi Nagy G, Pietinalho A, Shiner R, et al. The safety of formoterol and terbutaline given on de-mand via Turbuhaler on top of formoterol bid in patients with moderate asthma. Eur Respir J. 1999;14 (Suppl 30):341s.
4. Tattersfield A, Lofdahl C, Postma D, et al. On demand treatment: Comparison of formoterol and terbutaline in moderate asthma. Am. J. Respir. Crit Care Med 1999;159:A636.
5. Behling B, Matthys H. Comparison of efficacy and safe-ty of formoterol with terbutaline in children with mild to moderate asthma. Eur Respir J. 1999;14(Suppl 30):43s.
Recommendation
Although limited evidence exists on the usefulness of LABA as rescue medication, its role as such should always be with caution. More controlled studies along this line will validate its role.
Other Treatment/MedicationQuestion No.1:Can allergen-specific immunotherapy be used in the management of asthma?
Answer:Yes, numerous studies have shown that allergen specific immunotherapy can be used in the management of asthma [GRADE A].
Summary of Evidence:Several double-blind, placebo-controlled studies have been conducted on the efficacy of specific immuno-therapy, using various allergens such as house dust mites, pollens, cat and dog dander. These studies show that specific immunotherapy may result in a significant decrease in asthma medication consumption and im-provement in symptom scores and FEV1.
Likewise, there is decreased skin and bronchial sensitivi-ty to the allergen among patients undergoing immuno-
CPm 8th EDItION ASthmA
69
therapy. Some of the most significant improvements were seen in the studies involving dust mite allergens. However, many trials involving cat, dog, cockroach and pollens have also shown significant results.1-10 [LEVEL 1] A meta-analysis of randomized controlled trials on immunotherapy clearly demonstrated symp-tomatic improvement with immunotherapy (odds ratio of 2.7, 95% CI: 1.7 to 4.4); medication reduction with house dust mite immunotherapy (odds ratio of 4.2, 95% CI: 2.2 to 7.9) and reduction in bronchial hyper-reactivity (odds ratio of 13.7, 95% CI 3.8 to 50).7 [LEVEL 1]
References:1. Olsen OT, et al. A one-year, placebo-controlled, double-
blind house dust mite immunotherapy study on asthmatic adults. Allergy 1997;52:853-9.
2. Jacobsen L et al. Immunotherapy with partially purified and standardized tree pollen extracts. IV. Results from long term (six-year) follow up. Allergy 1997; 52:914.
3. Hirsch T, et al. Double-blind placebo-controlled study of sublingual immunotherapy with house dust mite extract (D. pt.) in children. Pediatr Allergy Immunol. 1997;8:21-7.
4. Tari MG, et al. Immunotherapy with an alum-adsorbed pa-rietaria pollen allergoid: a two-year double-blind placebo controlled study. Allergy 1997;52:65-74.
5. Dolz I, et al. A double-blind placebo-controlled study of immunotherapy with grass pollen extract alutard subcutaneous during a three-year period with initial rush immunotherapy. Allergy 1996;51:489-500.
6. Platts-Mills T. Immunotherapy in the treatment of asthma. UpToDate May 3, 1999; vol 7, no.2.
7. Abramson M, et al. Is allergen immunotherapy effective in asthma? A meta-analysis of randomized controlled trials. Am. J. Respir. Crit. Care Med. 1995; 151:969-74.
8. Haugaard L, et al. Immunotherapy in patients allergic to cat and dog dander. I. Clinical results. Allergy 1992; 47:249-54.
Question No. 2:Is immunotherapy safe?
Answer:Yes, immunotherapy is a relatively safe treatment mo-dality [GRADE A].
Summary of Evidence:Most studies did not reveal any significant harmful effects from immunotherapy.1-4 [LEVEL 1] a meta-analysis done in 1995 revealed systemic reactions in 32% (95% CI) of patients receiving immunotherapy as compared with 18% of patients receiving placebo.3 It is strongly advised that patient selection be strict, and that a specialist perform this procedure in a clinic setting, with emergency drugs on hand. Patients undergoing immunotherapy should be observed for up to two hours after the procedure, as this is the time when the most serious complications (e.g. anaphylaxis) may occur. Patients with unstable or steroid dependent asthma are usually at an increased risk for severe reactions and therefore should be excluded from receiving im-munotherapy.
References:1. Giovane AL, et al. A three-year double blind placebo
controlled study with specific immunotherapy to derma-tophagoides: evidence of safety and efficacy in pediatric patients. Clin Exp. Allergy. 1994:24:53-9.
2. Alvarez Cuesta E et al. Monoclonal antibody-standard-ized cat extract immunotherapy: risk benefit effects from a double blind placebo study. J. Allergy Clin. Immunol. 1994;93:556-66.
3. Abramson M et al. Is allergen immunotherapy effective in asthma? A meta-analysis of randomized controlled trials. Am. J. Respir. Crit. Care Med. 1995; 151:969-74.
4. Fish JE, Peters SP. Asthma: clinical presentation and man-agement. In: Fishman AP, Elias JA, Fishman JA, Grippi MA, Kaiser LR, Senior RM, (eds) Fishman's Pulmonary Diseases and Disorders. 3rd edition. New York: McGraw-Hill; 1998. p.766.
Recommendation
Referral to a specialist for specific allergen immu-notherapy should be considered when avoidance measures are not possible and appropriate medication fails to control symptoms of allergic asthma.
Question No. 3:What is the role of cromones in the management of chronic asthma?
Answer:Cromones may be used in young asthmatics and in those with atopy, nocturnal and exercise-induced asthma [GRADE A].
Summary of Evidence:Both cromolyn sodium and nedocromil sodium may be used in the management of asthma particularly in children, in atopic young adults, and in patients with nocturnal asthma and exercise-induced bronchocon-striction. The main hindrances to its efficacy are the frequent daily dosing (up to four-times-a-day) as well as the unpleasant taste.
Several studies have compared the efficacy of cromolyn sodium and nedocromil sodium to placebo, inhaled short-and long-acting β2-agonists, inhaled steroids, oral theophylline, and against each other. Most stud-ies comparing these drugs with placebo have revealed statistically significant improvements in all indexes of asthma symptoms including quality of life, pulmonary function measures and bronchodilator use.1-9 [LEVEL 1] When compared to inhaled SABA, cromolyn sodium and nedocromil sodium showed improved efficacy in pa-tients with atopy.5,6 [LEVEL 2] Long-acting β2-agonist like salmeterol, however, showed greater improvement in most pulmonary parameters when compared to the cro-mones.4 Studies involving theophylline and cromolyn sodium and nedocromil sodium showed that efficacy of these drugs are comparable as far as improvement in asthma symptoms and lung function are concerned.2
ASthmA CPm 8th EDItION
70
[LEVEL 1] However, more significant side effects were noted with the theophylline group.2
In studies comparing these drugs with inhaled steroids, it was demonstrated, that although there was improve-ment in symptoms and lung function in patients on cromolyn sodium and nedocromil sodium, the use of inhaled steroids was far more efficacious.5 [LEVEL 1] Furthermore, the more frequent daily dosing of these drugs as against the twice daily dosing of steroids may contribute to lower patient compliance and, therefore, less efficacy.5
Between the two available cromones, studies have shown that nedocromil sodium is more effective than cromolyn sodium in improving asthma symptoms and pulmonary function tests in adults.2,8,10 [LEVEL 2]
cotherapy. In: Fishman AP, Elias JA, Fishman JA, Grippi MA, Kaiser LR, Senior RM, (eds) Fishman's Pulmonary Diseases and Disorders. 3rd edition. New York: McGraw-Hill; 1998. p. 2654-5.
2. Schwartz HJ, et al. A comparative study of the clinical efficacy of nedocromil sodium and placebo. How does cromolyn sodium compare as an active control treatment? Chest 1998;109:945-52.
3. Marin JM, et al. Effects of nedocromil sodium in steroid-resistant asthma: a randomized controlled trial. J. Allergy Clin. Immunol. 1996;97:602-10.
4. Bousquest J, et al. Comparison of salmeterol with disodium cromoglycate in the treatment of adult asthma. Ann. Al-lergy Asthma Immunol. 1996;76:189-94.
5. Faurschou P, et al. Comparison between sodium cromogly-cate MDI and beclomethasone dipropionate MDI in the treatment of adult patients with mild to moderate bronchial asthma. A double blind, double-dummy randomized parallel group study. Allergy 1994;49:659-63.
6. Fink JN, et al. A double-blind study of the efficacy of nedocromil sodium in the management of asthma in pa-tients using high doses of bronchodilators. J. Allergy Clin. Immunol. 1994;94:473-81.
7. De Jong JW, et al. Nedocromil sodium versus albuterol in the management of allergic asthma. Am. J. Respir. Crit. Care Med 1994;149:91-7.
8. Jones PW. Quality of life, symptoms and pulmonary function in asthma: long-term treatment with nedocromil sodium examined in a controlled-multi-center trial. Nedo-cromil Sodium Quality of Life Study Group. Eur. Respir. J. 1994;7:55-62.
9. Clancy L, et al. Treatment of nocturnal asthma with ne-docromil sodium. Thorax 1994;49:1225-7.
10. Lal S, et al. Nedocromil sodium is more effective than cromolyn sodium for the treatment of chronic reversible airway disease. Chest 1993;104:438-74.
Recommendation
The use of cromones should be limited to patients who are unwilling or unable to include inhaled ste-roids in their asthma regimen.
Question No. 4:Do antihistamines have a role in the management of chronic asthma?
Answer:The role of antihistamines is limited to providing relief of allergic symptoms in some asthmatics. [GRADE B]
Summary of Evidence:Some patients with both atopy and asthma may benefit from antihistamines. Several studies, however, have shown that these drugs may be more useful for allergic rhinitis rather than bronchial asthma as there is no de-crease in bronchial responsiveness to methacholine after antihistamine treatment.1,4,5,6,7,8,9,10 [LEVEL 2]
Other studies also show that although antihistamines may help inhibit the early asthma response, they have no effect on the late asthma response.1,2,8,9,10 [LEVEL 2] Studies involving the use of ketotifen and terfenadine have shown improvement in symptomatology of aller-gic asthmatics compared to placebo, but only after 2-4 weeks of continuous use.8,9 [LEVEL 2] These drugs, therefore, are inferior when compared to long acting β2-agonists and steroids in both the relief and control of asthma symptoms.2,7
References: 1. Twentyman OP, et al. The effect of H1 receptor blockade
on the development of early and late-phase broncho-constriction and increased bronchial responsiveness in allergen-induced asthma. J. Allergy Clin. Immunol. 1993;91:1169-78.
2. Muir JF. Salmeterol versus slow-release theophylline combined with ketotifen in nocturnal asthma: a multicen-ter trial. French Multicenter Study Group. Eur Respir. J. 1992;10:1197-2000.
3. Tamaoki J, et al. Effect of azelastine on sulphur dioxide in-duced impairment of ciliary motility in airway epithelium. Thorax 1993;48:542-6.
4. Nieber K, et al. Effect of azelastine on substance P content in bronchoalveolar and nasal lavage fluids of patients with allergic asthma. Clin Exp. Allergy 1993; 23:69-71.
5. Balzano Gallo, et al. Effect of azelastine on the seasonal increase in non-specific bronchial responsiveness to methacholine in pollen allergic patients. A randomized double-blind placebo-controlled, crossover study. Clin Exp. Allergy 1992;22:371-7.
6. Turco A, et al. Transcutaneous O2 and CO2 monitoring of bronchial responsiveness in FEV1 non-responder asthmat-ics during ketotifen and placebo treatment. Respiration 1993:60:144-8.
7. Manaker S, Tietze KJ, Wittbrodt ET. Pulmonary pharma-cotherapy. In: Fishman AP, Elias JA, Fishman JA, Grippi MA, Kaiser LR, Senior RM, (eds) Fishman's Pulmonary Diseases and Disorders. 3rd edition. New York: McGraw-Hill; 1998 p. 2654.
8. Hoshino, et al. Effects of ketotifen on symptoms and on bronchial mucosa in patients with atopic asthma. Allergy 1997;52:814-20.
9. Tasaka T, et al. The Japanese perspective: effects of ter-fenadine in bronchial asthma: in vitro and in vivo research. Ann Allergy 1993;71:312-6.
10. Cockroft DW, et al. Allergen-induced increase in airway responsiveness is not inhibited by acute treatment with ketotifen or clemastine. Ann Allergy 1992; 68:245-50.
CPm 8th EDItION ASthmA
71
Management Strategy for Chronic AsthmaQuestion No. 1:What is the recommended treatment of chronic asthma?Answer:The management of chronic stable asthma depends on the level of severity of the condition. [GRADE A]In the chronic management: of persistent asthma, con-troller medications which have been invariably used are: inhaled corticosteroids, long acting β2-agonists, leuko-triene antagonists, theophylline and oral steroids. Anti-in-flammatory therapy, specifically inhaled corticosteroids, has been most effective in achieving asthma control in these patients. In contrast, intermittent asthma is not considered an indication for continuous use of ICS. The mainstay reliever medication, however, remains to be a SABA, which is recommended for use on a prn basis for all levels of severity. Table 5 shows the recommended severity-based therapy for chronic asthma.
The introduction of the fixed single inhaler combination ICS plus LABA represents a major advance in asthma treatment since the first edition of the Philippine Con-sensus Report on Asthma. These fixed-combination inhalers are effective across the whole spectrum of per-sistent asthma, from mild to severe persistent disease.1-7 [LEVEL 1] Furthermore, many patients with severe persistent asthma who used to require maintenance oral steroids can be kept under control with the ICS plus LABA single inhaler alone.8,9
With the combination inhaler, a significant propor-tion of mild to moderate persistent asthmatics can be symptom free with even half the ICS dosages previously required.1,5,10-12 The salutary effects of the combination inhaler are thought to be due to the complementary actions of the component drugs acting on the same site of the airways.13-16 Their availability through more user-friendly gadgets and their twice-a-day dosing have contributed to improving patient compliance. Further-more, since lower corticosteroid doses were found to be just as effective in combination with a LABA when compared with previously utilized moderate to higher doses, this has somewhat allayed fears of systemic side effects. Also, the reduced daily drug cost of the combination preparations when compared with the two components taken separately is also likely to enhance patient adherence.17-19
The broad efficacy of combination inhalers makes the strategy of micro-staging of asthma severity unneces-sary. [LEVEL 4] As such, the severity levels of mild persistent and moderate persistent asthma may be lumped together into one category. This revolutionary approach to managing mild and moderate persistent asthma as a single asthma category has gained relevance in the light of recent findings on the underutilization of ICS noted in the asthma survey results conducted in the Philippines. A sub-analysis of the data on the Asthma Insights and Reality in Asia-Pacific (AIRIAP) study
clearly indicates the low usage of ICS is the reason why a big proportion of Filipino asthmatic patients continue to suffer from persistent symptoms.20 A device, which delivers both ICS plus LABA, therefore, is bound to be more acceptable for a greater majority of these patients, especially since ICS itself does not produce the immediate relief experienced with bronchodilators. Better compliance and fewer defaults are, therefore, expected. Continued use of anti-inflammatory medica-tions correlates with better asthma control. With the array of doses available for the combination inhalers, their early use in mild persistent asthma patients is not at all disadvantageous and greatly simplifies the man-agement approach.
For the more severe persistent cases, the combination ICS plus LABA in a single inhaler would also be just as effective. However since the functional airway compro-mise may be more marked in these patients, significant improvement in symptomatology and lung function may take effect only after a few days. Prudence, therefore dictates that these patients be given a course of oral ste-roids at the start of treatment in moderate to high doses which can then be subsequently tapered to a level that would maintain the asthma under control.
References: 1. Condemi JJ, Goldstein S, Karlberg C et al. The addition of
salmeterol to fluticasone propionate versus increasing the dose of fluticasone propionate in patients with persistent asthma. Salmeterol Study Group. Ann Allergy Asthma Immunol 1999;88:383-9.
2. Shrewberry S, Pyke S, Britton M. Meta-analysis of increased dose of inhaled steroid or addition of salmete-rol in symptomatic asthma. (MIASMA) Br. Med J. 2000;320:1368-73.
3. Ind PW, Dal Negro R, Colman N et al. Inhaled fluticasone propionate and salmeterol in moderate adult asthma: Lung Function and symptoms (abstract) Am J. Respir Crit Care Med 1998;157 (Pt 2) Suppl;A416.
4. Jenkins C et al. Salmeterol/fluticasone propionate com-bination therapy 50/250 µg twice daily is more effective than budesonide 800 µg twice daily in treating moderate to severe asthma. Respir Med 2000;94:715-23.
5. Kips JC, O'Connor BJ, Inman MD, Svenson D, Pauwels RA, O'Byrn PM. A long-term study of anti-inflammatory effect of low-dose budesonide plus formoterol versus high-dose budesonide in asthma. Am J. Respir Crit Care Med. 2000;161:996-1001.
6. van Noord JA, Schreurs AJM, Mol SJM, Mulden PGH. Addition of salmeterol versus doubling the dose of flu-ticasone propionate in patients with mild to moderate asthma. Thorax 1999;54:207-212.
7. Ringdal N, Chuchalin AG, Chovan L et al. A comparison of Advair/Seretide (salmeterol 50 µg/fluticasone propionate 250 µg bid) with formoterol 12 µg + budesonide 800 µg bid in moderate-severe asthma (abstract) Am J. Respir Crit Care Med 2000;161(3):A196.
8. Aubier M et al. Salmeterol/fluticasone propionate (50/500 µg) combination in a discus inhaler (Seretide) is effective and safe in the treatment of steroid-dependent asthma. Respir Med 1999;93:876-84.
9. Nielson LP, Pedersen B, Faurschou P et al. Salmeterol reduces the need for inhaled corticosteroid in steroid-dependent asthma. Respir Med 1999;93(12):863-8.
10. Johansson G, Melvor RA, Purelio FDA et al. Salmeterol/fluticasone propionate combination dry powder inhaler
ASthmA CPm 8th EDItION
72
50/100 µg bid) is more effective than budesonide (400 µg bid) in mild to moderate asthma (abstract no. p. 162) Eur Respir J. 1998; 12 Suppl 29:20s.
11. Greening PA, Ind PW, Northfield M, Shaw G. Added salmeterol versus higher dose of corticosteroid in asthma patients with symptoms on existing inhaled corticosteroids. Lancet 1994;334:219-24.
12. Woolcock A, Lundback B, Ringdal N, Jacques L. Com-parison on addition of salmeterol to inhaled steroid with doubling the dose of inhaled steroids. Am J. Respir Crit Care Med 1996;153:1481-8.
13. Chung KF. The complementary role of glucocorticoids and long-acting β2 adrenergic agonist. Allergy 1998;53 Supplement 42:7-13.
14. Jack D. The use of inhaled β2 adrenergic bronchodilators and anti-inflammatory steroids in asthma. J. Pharmaco. Med 1996;6(1-6):5-16.
15. Spencer CM, Jarvis B. Salmeterol/fluticasone propionate combination. Drugs 1999, Jun;57:933-40.
16. Markham A, Jarvis B. Inhaled salmeterol/fluticasone propionate combination: a review of its use in persistent asthma. Drugs 2000 Nov 60(5):1207:33.
17. Lundback B. et al. Cost-effectiveness of salmeterol/flu-ticasone propionate combination product 50/250 µg twice daily and budesonide 800 µg twice daily in the treatment of adults and adolescents with asthma. Respir Med 2000;94:724-32.
18. Pieters WR. Lundback B. Johansson G et al. Cost-ef-fectiveness analyses of salmeterol/fluticasone propionate combination product and fluticasone in patients with asthma II: Study methodologies Pharmacoeconomics 1999;16 Suppl 2:9-14.
19. Palmqvist M, Price MJ, Sondhi S. Cost-effectiveness analysis of salmeterol/fluticasone propionate combination 50/250 µg vs fluticasone propionate 250 µg in adults and adolescents with asthma IV: results. Pharmacoeconomics 1999; 16(Suppl) 2:23-8.
20. Lai CKW on behalf of AIRIAP Steering committee. Clinical Management of asthma in Asia-Pacific in 2000: the asthma insights and reality in Asia-Pacific (AIRIAP) Study. Eur Respir J. 2001;18:441s.
Chapter 7Patient EducationQuestion No. 1:Does patient education have a role in asthma man-agement?
Answer:Yes, patient education is considered by many national and international consensus guidelines as a key and es-sential component of successful asthma management. [GRADE A]
Summary of Evidence:Asthma, although a chronic condition, is also a highly variable and episodic condition. Current management approaches require asthmatics and their families to ef-fectively carry out complex and multiple pharmacologic regimes. Asthmatics, therefore, should possess the basic knowledge and understanding of the mechanisms of ac-tion of the different drug prescriptions, the mastery of inhaler techniques, and the ability to adhere to prolonged and maintained drug therapy, even during asymptomatic periods. In addition, the asthmatic and his or her care-
giver must have the capability to recognize early warn-ing signs of an acute (especially severe) exacerbation, make rapid decisions about symptom severity, institute rational self-medication, and determine when to seek medical advice. Finally, that he or she must be prepared to make lifestyle changes and institute environmental control strategies.
Patient education is thought to be the mechanism through which patients can learn to successfully accomplish these tasks. Education is considered to be necessary "to help patients gain the motivation, skills and confidence to control their asthma."1,2,3,4 [LEVEL 1]
References:1. Guidelines for the Diagnosis and Management of Asthma.
National Asthma Education, and Prevention Program. Expert Panel Report 2: Bethesda, MD: National Institutes of Health; National Heart, Lung, and Blood Institute 1997, NIH Publication 97-4015A.
2. International Consensus Report on Diagnosis and Man-agement of Asthma. National Asthma Education and Prevention Program. Bethesda, MD: National Institutes of Health; National Heart, Lung, and Blood Institute 1995, NIH Publication 95-3659.
3. Canadian Asthma Consensus Report. Can. Med Assoc J. 1999; 161(11 Suppl):S15-S19.
4. Philippine College of Chest Physicians Council on Asthma. Philippine Consensus Report on Asthma Diagnosis and Management 1996, 55-60.
Question No. 2:Does asthma patient education improve health care outcomes?
Answer:Yes, well-designed asthma patient education programs reduce the frequency of asthma morbidity indices over a wide range of patient populations. [LEVEL 1] Formal asthma education programs, aside from improv-ing symptom control, can likewise enhance self-care behavior. [LEVEL 2].
Summary of Evidence:A systematic review of 22 randomized controlled trials recently compared the effects of asthma self-manage-ment education programs coupled with regular prac-titioner review with the usual care in adult patients.1 Self-management education was found to significantly reduce hospitalizations, emergency room visits, unsche-duled visits to the doctor, days off work or school, and nocturnal asthma. However, measures of lung function were not significantly changed. [LEVEL 1] Interven-tions for educating children who have attended the emergency room for an asthma exacerbation have found similar improvement in disease outcomes.2 [LEVEL 1] A recent review by the Education and Delivery of Care Working Group at the first World Asthma Meeting reinforced these findings.3
A local study conducted at the Philippine General Hos-pital compared adult asthmatics enrolled at an existing asthma self-management program and an enriched
CPm 8th EDItION ASthmA
73
education program with a control group who received usual care.4 The study showed that at three months post-intervention, patients who were enrolled in either formal education programs showed significant improvement in different facets of asthma self-efficacy, including level of confidence in performing self-care behavior, deci-sion-making, communication, knowledge of preventive medication and symptom management. Compared with the control group, these patients also demonstrated sig-nificant change toward correct inhaler technique.
References:1. Gibson PG, Coughlan J, Wilson AJ, et al. Self-manage-
ment education and regular practitioner review for adults with asthma. Cochrane Database Systematic Review 2000;37(2):CD001117.
2. Haby MM, Waters E, Robertson CF, et al. Interventions for educating children who have attended the emergency room for asthma. In: The Cochrane Library, 1, 2001. Oxford: Update Software.
3. Partridge MR, Hill SR. Enhancing care for people with asthma: the role of communication, education, training and self-management. 1998 World Asthma Meeting. Educa-tion and Delivery of Care Working Group. Eur Respir J. 2000;16:333-48.
4. Tuazon J, et al. Comparative study of two adult asthma education programs in enhancing self-care behavior and symptom control. Doctoral dissertation, UP Manila College of Public Health, 1999.
Question No. 3:Which educational strategies and methods have been found to be effective in influencing clinical outcomes?
Answer:Educational strategies that focus on individuals or small groups employing multiple interactive educational methods, and incorporating self-management skills transfer, self-monitoring modalities, and regular practi-
tioner review have been found to be effective. However, strategies that are limited to the transfer of information about asthma, its causes and its treatment have not been shown to improve health outcomes [GRADE A].
Summary of Evidence:A recent review showed that published asthma edu-cational programs for adults vary widely in terms of general and educational objectives, teaching techniques, tools, content, assigned trainers, duration of intervention and number of sessions. Thus, this precludes replication and reduces the possibility of identifying the most effec-tive components.1 Nevertheless, a systematic review of 11 randomized controlled trials of variable quality showed that limited asthma education (information only) among patients aged 16 years and above did not reduce hospitalization for asthma and had no effect on doctor visits, lung function and medication use.2 The effects of these education programs on asthma symp-toms were variable. There was no reduction in days lost from normal activity. [LEVEL 1] Moreover, programs relying primarily on providing books or videotapes to asthma patients were successful only in improving knowledge.3,4 [LEVEL 1]
Very few studies have addressed the optimal method for educational intervention. As described in the previous section, programs that focus on asthma self-management skills and are coupled with regular practitioner review, rather than usual care, improve morbidity indices. Sub-analyses of these clinical trials showed that those that involved individualized written asthma action plans showed greater reduction in hospitalization than those that did not.5 [LEVEL 1]
Asthma education should ideally begin in the physician's office and this can be effective only in the presence of
Table 6.1 Treatment based on Asthma Severity*
Severity Recommended Treatment
Daily controller medications Alternative controller Reliever medications
Intermittent SABA as neededICS + LABA combination as
single inhalerICS high dose or ICS regular dose plus any of the ff:- SR theophylline- Antileukotriene- Oral SR β2-agonist
mild to moderate Persistent
Severe Persistent Oral steroids + ICS + LABA combination as single inhaler + any of the ff:- SR theophylline- Antileukotriene- Oral SR β2-agonist
SABA as needed
SABA as needed
None needed
* Available in the Philippines
ASthmA CPm 8th EDItION
74
appropriate asthma therapy.6 [LEVEL 3] With regards to the comparison between educational programs focused on individuals versus those using small groups, there appeared to be few differences in outcomes, although small-group teaching resulted in a slight decrease in frequency of exacerbations, possibly because of the influence of peer support.6,7 [LEVEL 2]
As to the issue of PEF self-monitoring, this practice may be useful in some patients, particularly those who are poor perceivers of airflow obstruction. Patient self-monitoring may be effective using either measurement of PEF or monitoring of symptoms.8,9,10 [LEVEL 1]
References: 1. Sudre P. Jacquemet S, et al. Objectives, methods and
content of patient education programmes for adults with asthma: systematic review of studies published between 1979 and 1998. Thorax 1999;54:681-7.
2. Gibson PG, Coughlan J, et al. Limited (information only) patient education programs for adults with asthma. In: The Cochrane Library, 4, 1999. Oxford: Update Software.
3. Hilton S, Sibbald B, et al. Controlled evaluation of the ef-fects of patient education on asthma morbidity in general practice. Lancet 1986;1:26.
4. Jenkinson F, Davidson J, et al. Comparisons of effects of a self-management booklet and audiocassette for patients with asthma. Br Med J. 1988;297:267-70.
5. Gibson PG, Coughlan J, Wilson AJ, et al. Self-manage-ment education and regular practitioner review for adults with asthma. Cochrane Database Syst Rev 2000; 37(2):CD001117.
6. Canadian Asthma Consensus Report. Can Med. Assoc J. 1999;161(11 Suppl):S15-S19.
7. Wilson SR. Individual versus group education: is one better? Patient Educ. Couns 1997;32(1 Suppl):S67-S75.
8. Ignacio-Garcia JM, Gonzales-Santos P. Asthma self-management education program by home monitoring of peak exploratory flow. Am J. Respir Crit Care Med 1995;151:353-9.
9. Jones KP, et al. Peak-flow based asthma self-management: a randomized controlled study in general practice. Thorax 1995;50:851-7.
10. Cowie RL, Revitt SG, et al. The effect of a peak-flow based action plan in the prevention of acute exacerbations of asthma. Chest 1997;112:1534-8.
11. Wilson SR. Patient Education. The 3rd Triennial World Asthma Meeting Syllabus. Chicago, July 15, 2001.
Recommendation
Patient education is a key and essential component of successful asthma management. Education is a necessary tool not only as means to acquire knowl-edge about the condition but also to help patients gain the motivation, skills and confidence to control their asthma.
Well-designed asthma education programs have been shown to be effective in reducing asthma morbidity indices over a wide range of patient population.
Question no. 1:What is the mechanism of exercise-induced asthma (EIA)?
Answer:The heat exchange theory is currently one of the top theories for bronchoconstriction associated with exer-cise (EIA).1,2,3,4,5,6,7 [LEVEL 2]
During exercise, the humidification and heating func-tion of the nose is bypassed and cold air reaches the airways, which in turn produces bronchial spasm. This theory also suggests that the cold air may produce a humoral effect or a nerve reaction in the small airways that leads to bronchospasm.8 Neurohumoral transmitters like leukotrienes have also been implicated in mediating a portion of the airway narrowing.9,10
Leukotrienes have been found to play a role in airway refractoriness with repeated bouts of exercise. They may act through release of inhibitory prostaglandins or by inhibiting other mediator release. [LEVEL 3]
References: 1. Wells RE, Walker JEC, Hecklen RB. Effects of cold air on
respiratory airflow resistance in patients with respiratory tract disease. N. Engl. J. Med. 1960; 263: 268-73.
2. Strauss RH, McFadden ER, Ingram RH, Deal EC, Jae-ger JJ. Influence of heat and humidity on the airway obstruction induced by exercise asthma. J. Clin. Invest 1978;61:433-40.
3. Deal EC, McFadden ER, Ingram RH, et al. Role of respi-ratory heat exchange in production of exercise-induced asthma. J. Appl Physio. 1979;46:467-75.
4. Anderson SD, Schoeffel RE, Follet R, Perry CP, Daviskas E, Kendall M. Sensitivity to heat and water loss at rest during exercise in asthmatic patients. Eur J. Respir. Dis. 1982;63:459-71.
5. Anderson SD, Schoeffer RE, Black JL, et al. Airway cooling as the stimulus to exercise-induced asthma: re-evaluation. Eur J. Respir. Dis. 1985;67:20-30.
6. McDonald J, Nelson J, Lenner K, McLane M, McFad-den EJ. Effects of the combination of skin cooling and hyperpnea of frigid air in asthmatic and normal subjects. J. Appl Physio. 1997;82:453-9.
7. Banner AS, Chausow A, Green J. The tussive effect of hyperpnea with cold air. Am Rev Respir Dis 1985; 131:362-7.
8. McFadden ER Jr. Exercise-induced airway obstruction. Clin Chest Med 1995;16:671-82.
9. Israel E, Dermarkarian R, Rosenberg MA, et al. The effects of a 5-lipoxygenase inhibitor on asthma induced by cold, dry air. N Engl J Med 1990;323:1740-4.
10. Manning PJ, Watson RM, Margolskee DJ, et al. Inhibition of exercise-induced bronchoconstriction by MK-571, a potent leukotriene D4-receptor antagonist. N Engl J Med 1990;323:1736-9.
Question No. 2:How is exercise-induced asthma controlled?
CPm 8th EDItION ASthmA
75
Answer:Exercise-induced asthma may be controlled through non-pharmacological or pharmacological means. [GRADE B]
Summary of Evidence:Non-pharmacologic treatment entails avoiding incle-ment atmospheres and choosing a sport that is less likely to induce an asthmatic attack. A third strategy would be by inducing the known refractory period a few times earlier in the day of competition so that at the time of exercise competition, the neurohumoral transmitters are exhausted.1
Pharmacological treatment methods can be divided into primary and secondary methods. The primary pharma-cological agents given by inhalation are the β2-agonists, which will prevent exercise-induced bronchospasm in more than 80% of asthmatics. The most common are the rapid-acting, short-duration β2-agonists like salbutamol and terbutaline.2,3 The next most common are the rapid-onset, long duration formoterol and the slower-onset, long-duration β2-agonist salmeterol.4,5,6 [LEVEL 2]
Secondary of adjunctive treatment would be the use of agents for long-term control of asthma like inhaled cor-ticosteroids7 cromolyn8 and antileukotrienes.9 [LEVEL 3] The role of theophylline and anticholinergic agents are not clearly defined.
References:1. Cummiskey, J, Exercise-induced Asthma: An overview.
Am J. Med. Sci. 2001:322:200-3.2. Vilsvik J, Schaaning J, Stahl E, Holthe S. Comparison
between Bricanyl Turbuhaler and Ventolin metered dose inhaler in the treatment of exercise-induced asthma in adults. Ann Allergy 1991:67:315-8.
3. Andersen SD, Seale JP, Rozea P, et al. Inhaled and oral salbutamol in exercise-induced asthma. Am Rev Respir Dis 1976;114:493-500.
4. McAlpine LG, Thomson NC. Prophylaxis of exercise-in-duced asthma, a long-acting β2-adrenergic agonist. Respir Med 1990;84:293-5.
5. Konig P, Hordvik NL, Serby CW. Fenoterol and exercise-induced asthma. Effect of dose on efficacy and duration of action. Chest 1984;85:462-4.
6. Nelson JA, Strauss L, Skowronski M, et al. Effect of long-term salmeterol treatment on exercise-induced asthma. N Engl J Med 1998;339:141-6.
7. Konig P, Jaffe P, Godfrey S. Effects of corticosteroids on exercise-induced asthma. J Allergy Clin Immunol 1974;54:14-9.
8. Tullet WM, Tan KM, Wall RT, Patel KR. Dose-response effect of sodium cromoglycate pressurized aerosol in exercise-induced asthma. Thorax 1985;40:41-4.
9. Leff JA, Busse WW, Pearlman D, et al. Montelukast, a leukotriene-receptor antagonist, for the treatment of mild asthma and exercise induced bronchoconstriction. N Engl J Med 1998;339:147-52.
Food Allergy
Question No. 1:Is there an association between food allergy and
asthma exacerbations?
Answer:Yes, the association between food allergy and asthma has now been clearly established. [GRADE B]
Summary of Evidence:There is evidence that respiratory responses, including bronchoconstriction and increased airway hyperrespon-siveness, have been demonstrated in individuals following positive food challenges.1 However, food-induced asthma in adults is actually not very common, with an incidence of only 2-8.5%.2-3 The clinical cor-relation of food allergy with asthma is much higher in children at 17%.4 [LEVEL 2]
Multiple food allergy is generally uncommon. In infants and children, the majority of allergic reactions are due to milk, eggs, soy, peanuts and wheat5-6, while in adults, the most common food allergens are peanuts, tree nuts, fish, shellfish, and eggs.7-8 [LEVEL 2]
Sulfite-containing foods have been shown to cause bron-chospasm and severe asthmatic attacks in sensitive asth-matic patients, although the mechanism by which sulfate agents worsen asthma is unknown.9-12 The relationship between monosodium glutamate (MSG) and asthma is more controversial with several groups reporting both association and non-association.13-17 [LEVEL 3] The mechanism by which MSG produces asthma attaks is not well understood. There is conflicting evidence as to whether MSG exacerbates or induces asthma or if it alters airway reactivity. Tartrazine (FD & C Yellow No. 5) and other dyes commonly used for artificial coloring of food, drink, pills and tablets have been reported to cause urticaria and asthmatic symptoms in a few sensi-tive patients.18-19 [LEVEL 3]Asthma exacerbated by food allergy should be suspected in the following circumstances:• If asthma started early in life, especially if associated
with atopic dermatitis• If asthma associated with a current or past history
of food allergies or atopic dermatitis• If wheezing after specific foods has been noted• If asthma poorly controlled even with appropriate
medications and aeroallergen avoidance.Food-induced asthma may present acutely, occurring within minutes to one hour of food ingestion, manifest-ing initially with itchy watery eyes and nose, and itchi-ness in the mouth. This may later on progress to deep, repetitive coughing, shortness of breath, and wheezing. Acute attacks of asthma may be severe and occasion-ally progress to systemic anaphylaxis and even death. Respiratory reactions from food allergens may also be subtle, at times presenting only with cough, chronic asthma, or increased BHR.20
The diagnosis of food allergy is dependent on adequate history and physical examination, skin testing or in vitro antigen-specific IgE tests, results of an appropriated exclusion diet and blinded provocation when this may
ASthmA CPm 8th EDItION
76
be performed safely.Food-induced asthma is confirmed if food challenge reveals wheezing, a significant drop in FEV1, or a positive methacholine challenge on the test day but not on the placebo day.21 Elimination of the suspected food is often tried as part of a diagnostic approach. If symptoms resolve, confirmation by food challenge is recommended, except in cases wherein the patient has a convincing history of systemic anaphylaxis to a specific food.
Following identification of allergenic food, strict elimi-nation of that food is the only treatment proven effective to prevent reactions. The use of oral desensitization, prophylactic medications, or immunotherapy has not yet been demonstrated in well-designed studies to have clear efficacy in the management of food allergies.1 [LEVEL 2]
Rev. 1998;56:S153-S60. 2. Bock SA, Atkins FM. Patterns of food hypersensitivity
during sixteen years of double-blind, placebo-controlled food challenges (DBPCFC). J Pediatr 1990; 117:561-7.
3. Onorato J, Merland N, Terral C, et al. Placebo-controlled double-blind food challenge in asthma. J Allergy Clin Immunol 1986;78:1139-46.
4. James JM, Bernhisel-Broadbent J, Sampson HA. Respira-tory reactions provoked by double-blind food challenges in children. Am J. Respir Crit Care Med 1994; 49:59-64.
5. Burks AW, Mallory SB, Williams LW, et al. Atopic der-matitis: clinical relevance of food hypersensitivity reac-tions. J. Pediatr. 1988;113:447-51.
6. Burks AW, Sampson HA. Food allergies in children. Curr Prob Pediatr 1993;23:230-52.
7. Metcalfe DD. Allergic gastrointestinal diseases. In: Rich RR, Fleisher TA, Schwartz BD, et al. (eds) Clinical Immunology: Principles and Practice. 1995, St. Louis: Mosby-Year Book, 966-75.
9. Koepke JW, Christopher KL, Chai H, et al. Dose-depen-dent bronchospasm from sulfites in isoetharine. JAMA 1984;251;2982-3.
10. Taylor SL, Bush RK, Selner JC, et al. Sensitivity to sul-fited foods among sulfite-sensitive subjects with asthma. J. Allergy Clin Immunol 1988;81:1159-67.
11. Freedman BJ. Sulphur dioxide in foods and beverages: its use as a preservative and its effect on asthma. Br J. Dis. Chest 1980;74:128-34.
12. Delohery J, Simmul R, Castle WD, et al. The relationship of inhaled sulfur dioxide reactivity to ingested metabisul-fite sensitivity in patients with asthma. Am. Rev. Respir. Dis. 1984;130:1027-32.
13. Allen DH, Delohery J, Baker G. Monosodium L-gluta-mate-induced asthma. J Allergy Clin Immunol 1987; 80:530-7.
14. Germano P, Cohen SG, Hahn B, et al. An evaluation of clinical reactions to monosodium glutamate (MSG) in asthmatics using a blinded, placebo-controlled challenge. J. Allergy Clin Immunol 1991:87:177.
15. Germano P, Cohen S. Hibbard V, et al. Assessment of bron-chial hyperreactivity by methacholine challenge (MTC) in asthmatics before and after monosodium glutamate (MSG) administration. J. Allergy Clin Immunol 1993;91:340.
16. Schwartzstein RM, Kelleher M, Weinberger SE, et al. Airway effects of monosodium glutamate in subjects with chronic stable asthma. J. Asthma 1987;24:167-72.
17. Moneret-Vautrin DA. Monosodium glutamate-induced asthma: study of the potential risk of 30 asthmatics and review of the literature. Allergy Immunol 1987; 19:29-35.
18. Virchow C, Szezeklik A, Bianco S, et al. Intolerance to tartrazine in aspirin-induced asthma: results of a multi-center study. Respiration 1988;53:20-3.
19. Stevenson DD, Simon RA, Lumry WR, et al. Adverse reactions to tartrazine. J. Allergy Clin Immunol 1986; 78:182-91.
20. Bousquet J. Mechanisms in adverse reactions to food. The lung. Allergy 1995;50:52-5.
21. Hodge L, Yan KY, Loblay RL. Assessment of food che-mical intolerance in adult asthmatic subjects. Thorax 1996;51:805-9.
Asthma and Gastroesophageal Reflux Disease
Question No. 1:What is the relationship between asthma and gastro-esophageal reflux disease (GERD)?
Answer:Like asthma and sinusitis, GERD and asthma frequently coexist, but there have been no convincing evidence confirming the role of GERD in triggering or aggravat-ing asthma. [GRADE C]
Summary of Evidence:A relationship between GERD and asthma was first documented in the late 1960s when asthma patients were reported to be "cured" of asthma following surgery for hiatal hernia and/or GERD. Additional research has continued to show that reflux may cause or trigger asthma symptoms.1,2,3,4 [LEVEL 3]
There were two accepted mechanisms for the role of GERD in asthma. The first hypothesis states that the stimulation of esophageal mucosal receptors produces vagally mediated bronchospasm. Prolonged reflux clea-rance time often causes symptomatic esophageal disease and esophagitis, consequently increasing the sensitiv-ity of esophageal receptors to refluxed material. Once stimulated, the receptors transmit a signal that results in constriction of the bronchioles. The second hypothesis is the micro- or macro-aspiration of gastric contents into the lungs, especially in the supine position of sleep, causing a chemical pneumonitis. More recent research, however, has suggested that although aspiration does occur on rare occasions, it is unlikely to be the primary reason for reflux-triggered asthma.5
More recently, a third mechanism being proposed is heightened bronchial reactivity secondary to esophageal reflux.5 In one study of 105 consecutive asthmatics, the degree of methacholine reactivity correlated with the number of episodes of reflux during 24-hour esophageal pH monitoring.6 [LEVEL 3] Furthermore, nocturnal esophageal acid events are associated with lower re-spiratory resistance.7
CPm 8th EDItION ASthmA
77
References:1. Barish CF, Wu WC, Castell DO. Respiratory compli-
cations of gastroesophageal reflux. Arch Intern Med 1985;145:1882-8.
2. Nelson HS. Is gastroesophageal reflux worsening your patient's asthma? J. Respir. Dis. 1990;11:827-44.
3. Simpson WG. Gastroesophageal reflux disease and asthma. Arch Intern Med 1995;155:798-803.
4. Mansfield LE, Hameister HH, Spaulding MS, et al. The role of the vagus nerve in airway narrowing caused by intraesophageal hydrochloric acid provocation and esopha-geal distention. Ann Allergy 1981;47:431.
5. Harding SM, Sontag SJ. Asthma and gastroesophageal reflux. Am J. Gastroentro. 2000;95:S23.
6. Vincent D, Cohen-Jonathan AM, Leport J, et al. Gastro-esophageal reflux prevalence and relationship with bron-chial reactivity in asthma. Eur. Respir. J. 1997; 10:225.
7. Cuttitta G, Cibella F, Visconti A, et al. Spontaneous gastroesophageal reflux and airway patency during the night in adult asthmatics. Am. J. Respir. Crit. Care Med. 2000;161:177.
Asthma and the Menstrual Cycle
Question No. 1:Does menstrual cycle affect the course of asthma?
Answer:No direct correlation exist between the airway hyperres-ponsiveness in asthma and hormonal changes in the menstrual cycle [GRADE C]
Summary of Evidence:Premenstrual asthma (PMA) is a phenomenon first des-cribed by Frank in 1931, as a symptom of "premenstrual tension."1 Large-scale longitudinal studies have not yet been undertaken to adequately address just how preva-lent the condition is. Several small studies, however, seem to suggest that 30-40% of female asthmatics experience a premenstrual worsening of symptoms but these were retrospective and based on patient-recorded recollections of subjective data without any objective finding of increased asthma severity.2,3,4 [LEVEL 4] Modest reductions in peak flow rate at the time of menstruation for affected women compared to unaf-fected women were noted, but these were not usually associated with clinical deterioration.3,5
Two small prospective uncontrolled studies on the influence of menstrual cycle on airway responsiveness reported no significant difference on FEV1 or medica-tion use before or after the menstrual period. Asthma control, however, deteriorated just prior to and during menses.6,7 [LEVEL 4] A small prospective cohort study by Pauli et al in 1989 showed significant worsening of asthma symptoms, slight decline of peak expiratory flow rates but no deterioration in spirometric values showing airway responsiveness among asthmatics du-ring menses.8 A larger prospective analysis of data from 182 nonpregnant asthmatic women presenting to the emergency room for acute asthma reported that nearly half of all exacerbations occurred during the period from two days before until four days after the onset of menses.9 [LEVEL 5]
The weight of evidence seems to suggest that there is at least a subset of female patients with asthma who develop morbidity in conjunction with their menstrual cycle. A study by Shames showed that this distinct subset of women are the older asthmatics with more severe disease and longer duration of symptoms.10
References: 1. Frank RT. The hormonal causes of premenstrual tension.
Arch Neuro. Psych. 1931;26;1053. 2. Rees L. An etiological study of premenstrual asthma. J.
Psycho. Res. 1963;7:191-7. 3. Gibbs CJ, Coutts H, et al. Premenstrual exacerbation of
asthma. Thorax 1984;39:833-6. 4. Eliasson O, Scherzer HH, et al. Morbidity in asthma in
relation to the menstrual cycle. J. Allergy Clin. Immunol 1986;77:87-94.
5. Hanley SP. Asthma variation with menstruation. Br. J. Dis. Chest 1981;75:306-8.
6. Juniper EF, Kline PA, et al. Airway responsiveness to methacholine during the natural menstrual cycle and the effect of oral contraceptives. Am. Rev. Respir. Dis. 1987;135:1039-42.
7. Weinmenn GG, Zacur H, et al. Airway responsiveness to methacholine during the normal menstrual cycle. J. Allergy Clin. Immunol. 1987;79:634-8.
8. Pauli BD, Reid RL, et al. Influence of the menstrual cycle on airway function in asthmatic and normal subjects. Am. Rev. Respir. Dis 1989;140:358-62.
9. Skobeloff EM, et al. The effect of menstrual cycle in asthma presentations in the emergency department. Arch Intern Med 1996;156:1837-40.
10. Shames RS, Heilbron DC, et al. Clinical difference among women with and without self-reported perimenstrual asthma. Ann Allergy Asthma Immunol 1998;81:65-72
Question No. 2:Why does worsening of asthma occur in these patients during menstruation?
Answer:The precise cause of worsening of asthma during mens-truation is thought to be related to changing levels of progesterone or prostaglandins. Current studies, how-ever, presently do not show any definite correlation between airway responsiveness and the absolute levels of these substances [GRADE C].
Summary of Evidence:Progesterone levels fall in the days before menstruation and it has a relaxant effect on airway smooth muscle contractility. Thus, this may lead to cyclic changes in airway responsiveness in women prone to perimen-strual exacerbation of asthma.1 Progesterone-induced hyperventilation may further influence asthma leading to symptomatic deterioration and dyspnea.2 Although an increase in asthma symptoms and a decrease in peak expiratory flow rates have been demonstrated in the luteal phase of the menstrual cycle, there seems to be no deterioration in airway reactivity.3 It must be emphasized, however, that there is no real relation-ship between airway function and absolute levels of progesterone.
Prostaglandins have previously been reported to have
ASthmA CPm 8th EDItION
78
bronchoconstrictive effects; endogenous prostaglandin synthesis, however, has not been shown to correlate with occurrence of premenstrual asthma.4
The lack of definitive evidence for either progesterone or prostaglandin mediation has led to several other theories that are under investigation.5 These theories are as follows:• "Allergy" to endogenous hormones• Psychological changes associated with the premens-
trual syndrome• Progesterone potentiation of an unidentified bron-
chodilator• Progesterone-mediated loss of microvascular integ-
rity with subsequent edema leak• Dynamic fluctuations of estrogen levels after sus-
tained but static elevation• Increase in mucus secretions that may accompany
menstruation
Further clarification of and investigation into these mechanisms need to be undertaken to provide more in-formation and insight into the pathogenesis of the effect of asthma on the menstrual cycle or vice versa.
References:1. Boggess KA, Williamson HO, et al. Influence of the men-
strual cycle on systemic disease. Obst. Gyne. Clin. N. Am. 1990;17:321-42.
2. Moore LG, McCullough RE, et al. Increased HVR in pregnancy: relationship to hormonal and metabolic chal-lenges. J. Appl. Physio. 1987;62:158-63.
3. Pauli BD, Reid RL, et al. Influence of menstrual cycle on airway function in asthmatic and normal subjects. Am Rev Respir Dis 1989;140:358-62.
4. Eliasson O, Densmore MJ, et al. The effect of sodium me-clofenamate in premenstrual asthma: a controlled clinical trial. J Allergy Clin Immunol 1987;79:909-18.
5. Case AM, Reid RL. Effects of menstrual cycle on medical disorders. Arch Intern Med 1998;158:1405-12.
Question No. 3:Does treatment of premenstrual asthma differ from the usual treatment of asthma exacerbations?
Answer:No, the treatment options include the usual medications for asthma. Intramuscular progesterone, however, may be effective in women with severe, refractory peri-menstrual asthma. [GRADE C]
Summary of Evidence:Treatment of perimenstrual asthma entails the usual asthma medications, namely: β2-agonists, anticholi-nergics, and corticosteroids. Intramuscular progesterone was shown to be more effective in women with severe, refractory premenstrual asthma, eliminating the decrease in peak flow rate, as well as reducing total corticosteroid requirement.1 [LEVEL 4]
The use of danazol, intramuscular medroxyprogesterone acetate or gonadotropin-releasing hormone agonists to suppress menstrual cyclicity remains a promising area of investigation.
Reference:1. Beynon HLC, Garbett ND. Severe premenstrual exacer-
bations of asthma: effect of intramuscular progesterone. Lancet 1988:2:370-2.
Occupational Asthma
Question No. 1:Is occupational asthma a common condition?
Answer:Although occupational asthma is the most common occupational lung disease in developed countries,1,2,3 very few prevalence data has been published for many developing countries including the Philippines.
Occupational exposures have been estimated to cause 5-15% of adult-onset asthma.4,5,6 The prevalence of oc-cupational asthma due to agents with high molecular weight is generally less than 5% while prevalence due to low molecular weight agents is 5-10%.7
References:1. Meredith S, Nordman H. Occupational asthma: measures
of frequency from four countries. Thorax 1996; 51:435-40.
2. Toran, K. Self-reported rate of occupational asthma in Sweden 1990-92. Occup Environ Med 1996;53:757-61.
3. Provencher S, Labreche FP, DeGuire L. Physician based surveillance system for occupational respiratory diseases, the experience of PROPULSE, Quebec, Canada. Occup Environ Med 1997;54:272-6.
4. Kogevinas M, Anto JM, Soriano A, et al. The risk of asthma attributable to occupational exposures. A population-based study in Spain. Spanish Group of European Asthma Study. Am. J. Respir. Crit. Care Med 1996;154:137-43.
5. Blanc PD, Casternas M, Smith S, Yelin E. Occupational asthma in a community-based survey of adult asthma. Chest 1996;109 (Suppl1): S56-S78.
6. Fishwick D, Pearce N, D'Sousa W, et al. Occupational asthma in New Zealanders: a population based study. Occup Environ Med 1997;54:301-6.
7. Bernstein IL, Chan-Yeung M, Malo JL, Bernstein DI. Asthma in the workplace. New York, Marcell Dekker Inc. 1993.
Question No. 2:When should you suspect occupational asthma?
Answer:An occupational cause should be considered for all new cases of asthma in adults.1 [GRADE D]
A detailed occupational history of past and current ex-posure to possible causal agents in the workplace, work processes and specific job duties should be obtained. A history of asthma beginning during a working lifetime should lead to consideration of occupational asthma. The classic history is one of a worker whose asthma is worse at work, with improvement during weekends or holidays. However, this pattern may often be absent because symptoms are also usually present outside the workplace, being triggered by exposure to irritants, such
CPm 8th EDItION ASthmA
79
as cold air, fumes or exercise.
Questionnaires, although sensitive and essential in the assessment, are not specific tools. In a study on workers suspected to have occupational asthma, the predictive value of a positive questionnaire was 63% and a negative questionnaire was better at 83%. Another study showed that clinical history has a high sensitivity of 96% but a low specificity of 25% for the diagnosis of occupational asthma.2 [LEVEL 4]
References:1. Cartier A. Occupational asthma: what have we learned? J.
Allergy Clin. Immunol 1998;102 (Suppl 5):S90-S95.2. Malo JL, Ghezzo H, L'Archeveque J, et al. Is the clinical
history a satisfactory means of diagnosing occupational asthma? Am Rev Respir Dis 1991;143:528-32.
Question No. 3:What is the approach to the patient suspected of ha-ving occupational asthma?
Answer:As opposed to other occupational lung diseases like pneumoconiosis in which the diagnosis is based only on exposure history and chest x-ray abnormalities, oc-cupational asthma needs to be confirmed by objective means.1 [GRADE D]
The first step following history and physical exami-nation is to confirm objectively that the patient has asthma. Spirometry before and after bronchodilator therapy should be assessed within 24 hours of typical workplace exposure or at a time when symptoms are present. If spirometry is normal, then bronchoprovo-cation using either methacholine or histamine should be performed to determine the presence or absence of airways hyperresponsiveness. A normal methacholine response in a symptomatic patient who is still working, rules out occupational asthma.
Once the diagnosis of asthma is objectively confirmed by pulmonary function tests, the next step is to assess ob-jectively the relationship of asthma to work. This could be done by challenge testing with the specific suspected agent or by serial monitoring of PEF for a period at work and a similar period away from work.2,3 Sensitivity and specificity of PEF monitoring in confirming occupation-al asthma are 81% and 74%, respectively.4 Combining PEF monitoring with serial assessments of bronchial responsiveness using histamine or methacholine can provide further objective evidence.5 When the above results are inconclusive, serial spirometry performed throughout the work shift is advisable.
Early referral and rapid access to a specialist and a specialized center where investigations can be arranged is needed because the diagnosis is often difficult to es-tablish in those who have left work and cannot or will not return. [GRADE A]
References:1. Cartier A. Occupational asthma: what have we learned?
J. Allergy Clinl Immunol 1998; 102 (Supplement 5): S90-S95.
2. Chan-Yeung M. Assessment of asthma in the workplace. American College of Chest Physicians Consensus State-ment. Chest 1995;108:1084-117.
3. Burge PS. Single and serial measurements of lung function in the diagnosis of occupational asthma. Eur J. Respir. Dis. 1982;63 (Suppl 123):47-59.
4. Perrin B, Lagier F, L'Archeveque J, et al. Occupational asthma: validity of monitoring of peak expiratory flow rates and non-allergic bronchial responsiveness as compared to specific inhalation challenge. Eur Respir J. 1992;5:40-8.
5. Moscato G, Godnic-Cvar J, Maestrelli P. Statement on self-monitoring of PEF in the investigation of occupational asthma. Subcommittee on Occupational Allergy of Euro-pean Academy of Allergy and Clinical Immunology. J. Allergy Clin. Immunol 1995;96:295-301.
6. Lerover C, Perfetti L, Trudeau C, et al. Comparison of PEF and FEV1 monitoring with specific inhalation challenge in the diagnosis of occupational asthma. Am. J. Respir. Crit. Care Med 1997;155 (Part2): A137.
Question No. 4:How should patients with occupational asthma be managed?
Answer:The ideal treatment is the permanent removal of patients with occupational asthma from exposure to the causal agent. [GRADE A]
During the period of diagnostic investigations and fol-lowing diagnosis, the patient should have appropriate treatment for asthma, consistent with recent asthma guidelines.
Unfortunately, studies indicate that the majority of patients with occupational asthma are left with some degree of permanent lung function impairment.1 Over 60% of subjects fail to recover even after removal from exposure. The best prognosis is seen among those with early diagnosis, early removal from further exposure to the sensitizer, and in those with milder asthma at the time of diagnosis.2,3
The patient with occupational asthma should be con-sidered to represent a 'sentinel event' in the workplace. Consideration should be given to the possibility of occupational asthma in other exposure workers, and appropriate measures should be taken to reduce the risk of further exposure to the offending agent. [GRADE A]
References:1. Balkissoon R, Newman L. Occupational Asthma. Med-
scape Respiratory Care 1999;3(6).2. Malo JL, Cartier A, Ghezzo H, et al. Patterns of improve-
ment on spirometry, bronchial hyperresponsiveness and specific IgE antibody levels after cessation of exposure in occupational asthma caused by snow-crab processing. Am Rev Respir Dis 1988;138:807-12.
3. Lemiere, C, Cartier A, Dolovich J, et al. Outcome of specific bronchial responsiveness to occupational agents after removal from exposure. Am. J. Respir. Crit. Care Med 1996;154:329-33.
ASthmA CPm 8th EDItION
80
Asthma and Pregnancy
Question No. 1:Does the course of asthma change during preg-nancy?
Answer:Asthma may remain unchanged, become worse, or improve during pregnancy. [LEVEL 2]
Summary of Evidence:Approximately 4% of pregnancies are complicated by bronchial asthma. The true prevalence may be even higher; at least 10% of the population appears to have nonspecific airway hyperreactivity, a hallmark of asth-ma.1 The course of asthma during pregnancy is variable; it may remain unchanged, become worse or improve during pregnancy. In a prospective study by Steinus-Aarniala et al, 42% of pregnant asthmatics required more medications, 40% were managed with the same medications before pregnancy and 18% actually needed less medications.2 [LEVEL 1]
As a rule, women with more severe asthma prior to preg-nancy are likely to deteriorate during pregnancy. The factors most likely contributing to worsening asthma during pregnancy include upper respiratory tract infec-tions and patient non-compliance with medical regi-men.3 [LEVEL 2] The peak of exacerbations appears between the 24th-36th weeks age of gestation (AOG). Asthma generally remains quiescent during labor and delivery in about 90% of pregnant women. Whatever the course of asthma may be during pregnancy, changes generally revert to pre-pregnancy level of severity within 3 months post-partum.4
References:1. National Heart, Lung and Blood Institute. Management of
asthma during pregnancy. NIH Publication No. 93-3279, September 1993.
2. Steinus-Aarniala B, et al. Asthma and pregnancy: a pro-spective study of 198 pregnancies. Thorax 1988; 43:12-8.
3. Gluck JC, Gluck P. The effects of pregnancy on asthma: a prospective study. Ann Allergy 1976;37 (3):164-8.
4. Schatz M, et al. The course of asthma during pregnancy, post-partum and with successive pregnancies: a prospec-tive study. J. Allergy Clin Immunol 1988; 81(3):509-17.
Question No. 2:How does maternal asthma affect pregnancy out-
come?
Answer:When asthma is properly controlled, pregnant women with asthma can maintain a normal pregnancy with little or no increased risk to themselves or their fetuses. [GRADE B]
Summary of Evidence:Uncontrolled asthma during pregnancy has been proven to produce serious maternal and fetal complications. Both mother and child are at risk if asthma is not well
managed during pregnancy. Severe persistent asthma has been related to the development of maternal com-plications like pre-eclampsia, maternal hypertension, hyperemesis gravidarum, uterine vaginal hemorrhage, toxemia, placenta previa, and induced complicated labors.1,2,3 Fetal complications include increased risk of perinatal mortality, intrauterine growth retardation, preterm birth, low birth weight, and neonatal hypoxia.2 [LEVEL 2]
Studies in which asthma was actively controlled did not show any difference in the overall incidence of adverse fetal outcomes among infants of asthmatic women and non-asthmatic women.4,5 [LEVEL 2] A study involv-ing severe asthma reported that pregnant women with poorly controlled asthma requiring hospital admission gave birth to infants who weighed significantly less than babies whose mothers' asthma is well controlled.6 Severe asthma requiring emergency therapy or corticosteroid seem to be associated with an increased incidence of perinatal complications like pre-eclampsia, low-birth weight infants, perinatal mortality, preterm births and hyperbilirubinemia. However, these associations did not reach statistical significance.4,7
References:1. Alexander S, Dodds L, Armson BA. Perinatal outcomes
in women with asthma during pregnancy. Obstet Gyne. 1998;92:435-40.
2. Demissie K, Breckenridge MB, Rhaods GG. Infant and maternal outcomes in the pregnancies of asthmatic women. Obstet Gyne Survey 1999;54:355-6.
3. Tan KS, Thomson NC. Asthma in pregnancy. Am J Med 2000;109(9):727-33.
4. Schatz M, Zeiger RS, Hoffman CP, et al. Perinatal out-comes in the pregnancies of asthmatic women: a prospec-tive controlled analysis. Am. J. Respir. Crit. Care Med 1995;15:1170-4.
5. Perlow JH, Montgomery D. Severity of asthma and peri-natal outcomes. Obstet Gyne 1992;167:193-7.
6. Greenberger PA, Petterson R. The outcome of pregnancy complicated by severe asthma. Allergy Proc. 1988;9:539-43.
7. Schatz M. The safety of asthma and allergy medica-tions during pregnancy. Can J. Allergy Clin. Immunol. 1998;3:242-54.
Question No. 3:Are asthma medications safe to use during preg-nancy?
Answer:Most asthma medications are safe to use during preg-nancy. [GRADE B]
Summary of Evidence:The use of inhaled β2-agonist, theophylline, cromolyn, antihistaminics and inhaled steroids are not associated with major congenital malformations when used at anytime during gestation, including the first trimester.1 [LEVEL 3] In a review of ten studies on asthmatic women during the first trimester of pregnancy, only three met the relevant quality criteria.1,2,3 There was no significant increase in the rate of congenital malforma-
CPm 8th EDItION ASthmA
81
tions with any of the exposures.4 [LEVEL 2]Because few safety studies on medication use during pregnancy are available, the US Food and Drug Admin-istration (FDA) has published pregnancy risk categories for drugs. (See Table 6) All commonly used asthma medications fall under safety categories B and C. This system was developed from animal exposure data and epidemiologic data from population studies.5
For mild intermittent asthma and acute exacerbations in all asthmatic patients, inhaled short-acting β2-agonists is the preferred treatment. These agents have not been shown to have any adverse effects on pregnancy out-comes or teratogenic effects on the fetus.1 Use of oral and parenteral β2-agonists should be avoided because of lack of safety data, the increased risk of side effects (e.g. tremor), and the potential to inhibit delivery.Inhaled corticosteroids are the 'gold standard' for controlling all forms of persistent asthma. [LEVEL 1] These agents have been shown to decrease asthma exacerbations and mortality and improve overall quality of life. The 2000 position paper of the American College of Obstetricians and Gynecologist and the American College of Allergy, Asthma and Immunology states, "it would not be unreasonable to continue a different inhaled corticosteroid in a patient well-controlled by that drug prior to pregnancy."6
Long-acting β2-agonists, salmeterol and formoterol are the preferred adjunctive therapy to inhaled corticoste-roids for managing moderate to severe persistent asthma. [LEVEL 1] Although no adequate or well-controlled hu-man data are available on salmeterol and formoterol use during pregnancy, there are also no reports of congenital defects. Use of an inhaled long-acting β2-agonist with an inhaled corticosteroid appears to be acceptable during pregnancy, especially if the patient has taken such agents without problems before the pregnancy.7
Long-term safety data are available for inhaled cromo-lyn and it is a feasible option for use during pregnancy especially if there is a concern about prescribing inhaled corticosteroids.8 The leukotriene receptor antagonists, zafirlukast and montelukast sodium are classified as FDA category B because no human or animal terato-genic effects have been seen with agents. Use of oral corticosteroids during pregnancy poses some risk.9
Theophylline has not been shown to have teratogenic effects during pregnancy although its use has radically decreased because of possible toxicity with elevated serum levels and because of the development of newer, safer agents. When used during pregnancy, clearance of the agent decreases, therefore dosing should be carefully watched and adjusted. Theophylline crosses the placenta and the newborn may have jitterness, increased heart rate and even vomiting at birth.5
Nebulized ipratropium can be used for acute asthma not responding well to inhaled β2-agonist. Ipratropium bromide is an inhaled anticholinergic agent that is used as an adjunctive therapy to short-acting β2-agonists
for acute asthma exacerbations. Animal data have not demonstrated any birth defects, but human data are lacking.10
Omalizumab, an IgG monoclonal antibody directed against IgE, was recently approved in the United States for use in moderate to severe allergic asthma that has not responded to moderate to high doses of inhaled corticosteroids. The FDA gave this agent a pregnancy category B rating because no teratogenic effects were seen in animal studies. In clinical studies with omalizu-mab before FDA approval, several women became pregnant and delivered normal infants. Because of the newness of this agent, caution should be exercised when prescribing during pregnancy.11
References: 1. Schatz M, Zeiger RS, Harden K, et al. The safety of asthma
and allergy medications during pregnancy. J Allergy Clin Immunol 1997;100:301-6.
2. Schatz M, et al. The course of asthma during pregnancy, postpartum and with successive pregnancies: a prospective study. J Allergy Clin Immunol 1988; 81:509-17.
3. Rydhstroem KG. Congenital malformations after use of inhaled budesonide in early pregnancy. Obstet Gyne 1999;93:392-5.
4. Jadad A, Sigouin C, et al. Risk of congenital malforma-tions associated with treatment of asthma during early pregnancy. Lancet 2000;355:119.
5. Blaiss, MS, Managing asthma during pregnancy: the whys and hows of aggressive control. Postgrad Med 2004;115(5):55-64.
6. The use of newer asthma and allergy medications during pregnancy. The American College of Obstetricians and Gynecologists (ACOG) and the American College of Al-lergy, Asthma and Immunology (ACAAI). Ann Allergy Asthma Immunol 2000;84(5):475-80.
7. Blaiss, MS, Management of rhinitis and asthma in preg-nancy. Ann Allergy Asthma Immunol 2003; 90 (6 Suppl 3):16-22.
8. Scatz M. The efficacy and safety of asthma medications during pregnancy. Semin Perinatol 2001; 25(3):145-52.
9. Spector SL; Antileukotriene Working Group. Safety of antileukotriene agents in asthma management. Ann Allergy Asthma Immunol 2001;86(6 Suppl 1):18-23.
10. Liccardi G, Cazzola M, Canonica GW, et al. General strat-egy for the management of asthma in pregnancy. Respir. Med 2003;97(7):778-89.
11. Busse W, Corren J, Lanier BQ, et al. Omalizumab, anti-IgE recombinant humanized monoclonal antibody for the treat-ment of severe allergic asthma. J. Allergy Clin Immunol 2001;108(2):164-90.
Question No. 4:Are steroids associated with increased risk of perinatal complications?
Answer:Inhaled corticosteroids have no effect on pregnancy out-come and do not increase the risk to the fetus. [GRADE B] However, the use of oral steroids for severe asthma during pregnancy may be associated with increased perinatal complications.
ASthmA CPm 8th EDItION
82
Summary of Evidence:Review of literature on human studies do not show any evidence of teratogenicity with the use of inhaled corticosteroids during pregnancy. The most published information is on beclomethasone, and it does not ap-pear to have any adverse effect on pregnancy outcome and does not increase the risk to the fetus.1,2,3 Likewise, a study with more than 2000 patients did not show an increased rate of congenital malformations with the use of inhaled budesonide.4 [LEVEL 2]Among 293,948 births identified from 1995 to 1998 derived from the Swedish Medical Birth register, preg-nancy outcomes were compared for mothers reporting asthma medication usage with those for women who reported no usage. Researchers found that 2,968 mothers who reported use of inhaled budesonide during early pregnancy gave birth to infants of normal gestational age, birth weight, and length; there was no increase in rate of stillbirths or multiple births.5 Because of this data, budesonide has been assigned a safety category B rating by the FDA. At present, all other inhaled corticosteroids are category C.On the other hand, oral steroids have been associated with risk for pre-eclampsia in several studies.4,6,7 Whether or not this link represents a drug effect or is a marker of severity cannot be ascertained. [LEVEL 2] The use of oral steroids during the first trimester has also been associated with oral cleft palate deformities.8 [LEVEL 2] and prednisone treatment throughout the pregnancy is associated with lower birth weights.9 The benefit of using oral steroids, when indicated however, far out-weighs the risk of uncontrolled asthma to the mother and fetus.10
References: 1. Schatz M. The safety of asthma and allergy medica-
tions during pregnancy. Can J. Allergy Clin Immunol. 1998;3:242-54.
2. Fitzsimmons R, Greenberger PA, Patterson R. Outcome of pregnancy in women requiring corticosteroids for severe asthma. J. Allergy Clin Immunol 1986;78:349-53.
3. Greenberger PA, Patterson R. Beclomethasone dipro-pionate for severe asthma during pregnancy. Ann Intern Med 1983;98:578-90.
4. Schatz M, Petitti D, Chilinger L, et al. The safety of asthma and allergy medications during pregnancy. J. Allergy Clin Immunol 1997;100:301-6.
5. Norjavaara E, de Verdier MG, Normal pregnancy outcomes in a population-based study including 2,968 pregnant women exposed to budesonide. J. Allergy Clin Immunol 2003;111(4):736-42.
7. Steinus-Aarniala B, et al. The effects of pregnancy on asthma: a prospective study. Ann Allergy 1976;37: 164-8.
8. Alexander S, Dodds L, Armson BA. Perinatal outcomes in women with asthma during pregnancy. Obst Gyne 1998;92:435-40.
9. Rodriguez-Pinilla E, Martinez-Friaz ML. Corticosteroids during pregnancy and oral clefts: a case control study. Teratology 1998;58:2-5.
10. Reinisch JM, Simon NG, et al. Perinatal exposure to pred-nisone in humans and animal retards intrauterine growth. Science 1978;202:436-8.
Asthma and Surgery
Question No. 1:Are patients with asthma undergoing surgery at greater risk for peri-operative complications?
Answer:No, the risk of peri-operative complications in patients with asthma undergoing surgery is low. [GRADE B]
Summary of Evidence:Generally, the risk of peri-operative complications in patients with asthma undergoing surgery is low.1,2,3 [LEVEL 2] Warner et al reviewed the records of 706 diagnosed asthmatics who had at least one surgical procedure involving a general anesthetic or central neuroaxis block.1 The frequency of perioperative bron-chospasm and laryngospasm was low in his cohort of patients with asthma. The frequency of complications was increased in older patients and in those with active asthma. The frequency of complications did not depend on the severity of asthma symptoms or the chronic use of bronchodilators before operation.
A computer-aided study of 136,929 patients by Olsson in 1987 found the incidence of intraoperative bronchospasm to be 0.80% in 3,210 patients with asthma versus 0.16% in those patients without asthma.5 Bronchospasm during anesthesia occured in only one out of 634 anesthetics or 1.7 per 1000 patients. This author concluded that there was the likelihood of increased incidence of intraopera-tive complications (bronchospasm) in the presence of pre-existing airway obstruction, particularly in the face of airway instrumentation. [LEVEL 4]
References:1. Warner DO, Warner MA, Barnes RD, et al. Perioperative
respiratory complications in patients with asthma. Anes-thesiology 1996;85:460-7.
2. Shnider SM, Papper EM. Anesthesia for the asthmatic patient. Anesthesiology 1961;22:886-92.
3. Gold MI, Helrich M. A study of the complications re-lated to anesthesia in asthmatic patients. Anesth Analg 1963;42:283-93.
4. Pien LC, Grammer LC, Patterson R. Minimal complica-tions in a surgical population with severe asthma receiv-ing prophylactic corticosteroids. J Allergy Clin Immunol 1988;82:696-700.
5. Olsson GL. Bronchospasm during anesthesia. A computer-aided study of 136,929 patients. Acta Anaesthesiol Scand 1987;31:244-52.
Question No. 2:Are steroid-controlled asthmatics at risk for developing peri-operative complications?
Answer:No, there is no increased risk for peri-operative compli-cations in steroid-controlled asthma. [GRADE B]
Summary of Evidence:The use of pre-operative steroids to control asthma does not put the asthmatic at greater risk for peri-operative complications.1-5 [LEVEL 2] Prior to surgery, patients
CPm 8th EDItION ASthmA
83
should be free of wheezing, with a peak flow greater than 80 percent of the predicted personal best value.2 To achieve this goal, the patient may need oral cortico-steroids (60 mg of prednisone daily or the equivalent).
Kabalin et al4 studied the effect of pre-operative steroids on the incidence of postoperative bronchospasm, infec-tion, clinical evidence of adrenocortical insufficiency and death among 71 asthmatics who underwent 89 surgical procedures. Of the complications monitored, intra-operative wheezing developed in only one patient; three patients (4.5%) developed mild post-operative bronchospasm. The incidence of infection was not sta-tistically different between two surgical groups that were compared and there was no evidence of adrenocortical insufficiency. One death was related to a neurosurgical intra-operative complication. Therefore, a short-course of peri-operative corticosteroids does not appear to in-crease the incidence of infection or other post-operative complications in patients with asthma.3,4,5 [LEVEL 3]
References:1. Smetana, GW. Current concepts: preoperative pul-
monary evaluation (Review Article). N. Engl. J. Med. 1999;340:937-44.
2. Guidelines for the Diagnosis and Management of Asthma. National Heart, Lung, and Blood Institute. National Asthma Education Program, Expert Panel Re-port. X. Special considerations. J. Allergy Clin Immunol 1991;88(Suppl):523-34.
3. Pien LC, Grammer LC, Patterson R. Minimal complica-tions in a surgical population with severe asthma receiv-ing prophylactic corticosteroids. J. Allergy Clin Immunol 1988;82:595-700.
5. Warner DO, Warner MA, Barnes RD, et al. Perioperative respiratory complications in patients with asthma. Anes-thesiology 1996;85:460-7.
Asthma and Upper Airway Disease
Question No. 1:Is there a relationship between asthma and rhinitis established?
Answer:No, there is no established relationship between asthma and rhinitis, however, they commonly occur as co-mor-bidities. [GRADE B]
Summary of Evidence:The concept of "one airway, one disease"1 was proposed in the late 1990s because of several common factors noted between asthma and rhinitis: common epidemio-logic, pathologic, and physiologic characteristics and a common therapeutic approach.2-5
A study which utilized a standard questionnaire in 478 patients demonstrated that rhinitis is nearly a universal phenomenon in patients with allergic asthma, occurring in 99% of adults and 93% of adolescents.6 [LEVEL 4] Conversely, asthma has also been shown to affect up
to 38% of patients with allergic rhinitis which is sub-stantially higher than the 3-5% prevalence noted in the general population.7 Even nonallergic rhinitis was also found to be associated with asthma.8,9,10 [LEVEL 3]
allergic rhinitis often precedes or occurs at the same time as asthma. However, although atopic subjects com-monly have coexisting asthma and rhinitis, rhinitis alone does appear to be a risk factor for asthma.11 Settipane et al noted that in a 23-year follow up study of 690 college freshmen without asthma, those who reported nasal symptoms in 1961 developed asthma three times more often (10.5%) than individuals without rhinitis (3.6%).12-13 [LEVEL 3]
Although it appears that patients with rhinitis are more likely to develop asthma, it has not been possible to pre-dict which patients are at greatest risk. Patients with aller-gic rhinitis and no clinical evidence of asthma have been shown to frequently exhibit bronchial hyperresponsive-ness to methacholine. This has given rise to the postulate that BHR may represent an intermediate phase between
Risk Categories:A - Adequate studies in pregnant women have not demonstrated
a risk to the fetus in the first trimester of pregnancy and there is no evidence of risk in later trimesters.
B - Animal studies have not demonstrated a risk to the fetus, but there are no adequate studies in pregnant women or Animal studies have shown an adverse effect, but adequate studies in pregnant women have not demonstrated a risk to the fetus in the first trimester of pregnancy, and there is no evidence of risk in later trimesters.
C - Animal studies have shown adverse effects on the fetus, but there are no adequate studies in humans; the benefits from the use of the drug in pregnant women may be acceptable despite its potential risks; or there are no animal reproduction studies and no adequate studies in humans.
D - There is no evidence of human fetal risk, but the potential benefits from the use of the drug in pregnant women may be acceptable despite its potential risks.
X - Studies in animals or humans demonstrate fetal abnormalities, or adverse reaction reports indicate evidence of fetal risk. The risk of use in pregnant women clearly outweighs any possible benefits.
Table 6. US FDA Pregnancy Risk Categories for Asthma Medications
ASthmA CPm 8th EDItION
84
nasal allergy and symptomatic asthma. However, large-scale prospective studies are needed to confirm these findings. It has also not been proven that the presence of rhinitis is related with asthma severity although a few studies suggest that such an occurrence is also related to higher use of anti-asthma medications.14-15
In patients with both asthma and allergy, it has been suggested that treating rhinitis adequately will improve asthma symptoms and lung function. Two small trials show that prevention of seasonal nasal inflammation with topical steroids reduced subsequent exacerbations of allergic asthma.16-17 However, there were no published well-controlled, large-scale clinical trials thus far to quantify the effect of treatment of nasal disease on asthma symptoms and lung function. [LEVEL 3]
References: 1. Grossman J. One airway, one disease. Chest 1997; 111
(suppl 2):11S-6S. 2. Rowe-Jones JM. The link between the nose and lung, pe-
rennial rhinitis and asthma: is it the same disease? Allergy 1997;52:20-8.
3. Vignola Am, Chanez P, Godard P, Bousquet J. Relation-ships between rhinitis and asthma. Allergy 1998; 53:833-9.
4. Corren J. The impact of allergic rhinitis on bronchial asthma. J. Allergy Clin. Immunol 1998;101:S352-S356.
5. Townley RG, Kiboneka A. Allergic rhinitis: relationship to asthma. Similarities, differences, and interactions [editorial]. Ann Allergy Asthma Immunol 1998; 80:137-9.
6. Kapsali T, Horowitz E, Diemer F, Togias A. Rhinitis is ubiquitous in allergic asthmatics [abstract]. J. Allergy Clin. Immunol 1997;99:S138.
7. Evans R III, Mullally DI, Wilson RW, et al. National trends in the morbidity and mortality of asthma in the US: prevalence, hospitalization and death from asthma over two decades: 1965-1984. Chest 1987;91: S65-S74.
8. Leynaert B, Nuekirch F, Pascal D, Bousquet J. Epide-miologic evidence for asthma and rhinitis co-morbidity. J. Allergy Clin. Immunol 2000;106:S201-S205.
9. Sibbald B, Rink E. Epidemiology of seasonal and perennial rhinitis: clinical presentation and medical history. Thorax 1991;46:895-901.
10. Leynaert B, Bousquet J, Neukirch C et al. Perennial rhini-tis: an independent risk factor for asthma in nonatopic sub-jects. Results from the European Community Respiratory Health Survey. J. Allergy Clin. Immunol 1999;104:301-4.
11. Wright AL, Holberg CJ, Martinez FD, et al. Epidemiology of physician-diagnosed allergic rhinitis in childhood. Pediatrics, 1994.
12. Settipane RJ, et al. Long-term risk factors for developing asthma and allergic rhinitis: a 23-year follow-up study of college students. Allergy Proc 1994:21-5.
13. Greisner WA, Settpane, et al. Co-existence of asthma and allergic rhinitis: a 23-year follow-up of college students. Allergy Asthma Proc 1998;19:185-8.
14. Huse DM, Harte SC, Russel MW, et al. Allergic rhinitis may worsen asthma symptoms in children. The inter-national asthma outcomes registry. [abstract]. Am J. Respir. Crit Care Med 1996;153:A860.
15. Halpern M, Richner R, Togias A, et al. Allergic rhinitis may increase asthma costs [abstract] Am J. Respir. Crit Care Med 1996;153:A860.
16. Welsh PW, Stricker EW, Chu-Pin C, et al. Efficacy of beclomethasone nasal solution, flunisolide, and cromolyn in relieving symptoms of ragweed allergy. Mayo Clin Proc 1987;62:125-34.
beclomethasone prevents the seasonal increase in bronchial hyperresponsiveness in patients with allergic rhinitis and asthma. J Allergy Clin Immunol 1992; 90:250-6.
Question No. 2:Is there a relationship between asthma and sinus-itis?Answer:Yes, it appears that asthma and sinusitis frequently co-exist, and sinusitis can trigger asthma. However, as shown in some studies, their causal relationship remains controversial. [GRADE B]Summary of Evidence:Whether the relation between asthma and sinusitis is causal or merely an epiphenomenon of an infectious or immune-mediated disease affecting the entire respira-tory tract is still a matter of debate. However, there are certain characteristics that identify those patients in whom sinusitis may play an important role in the pathogenesis of asthma.1 These are as follows:
• Sinusitis preceding the development of asthma symptoms
• Sinusitis in non-atopic patients (which implies that a fundamental change has occurred in the sinus tissues and airway)
• Aspirin sensitivity• Corticosteroid dependency (suggests that an under-
lying sinus disease may be a trigger for asthma)• Patients with asthma who are refractory to appropri-
ate treatment• When a child with asthma becomes symptomatic while
taking medications that were formerly effective• When a patient receives a short-term course of ste-
roid therapy for an acute episode of asthma and is still symptomatic after several days of treatment
Approximately 40-60% of asthmatic patients will show radiographic evidence of sinusitis. Some patients with recurrent sinusitis will develop chronic tissue inflam-mation with mucosal thickening and formation of nasal polyps, also called chronic hyperplastic sinusitis and nasal polyp formation (CHS/NP). Pathologic examina-tion of this tissue typically shows a striking inflamma-tory infiltrate of eosinophils, somewhat similar to the inflammatory infiltrate seen in asthma.2,3,4 In patients with coexisting asthma, the development of CHS/NP often heralds a worsening in asthma symptoms.
It was also postulated that a sino-nasal bronchial reflex exists which could be mediated by the autonomic nervous system or inflammatory mediators such as leukotrienes, prostaglandin D2 and histamine.5 Other possible explana-tions include micro- or macro-aspiration of sinus drain-age, or a systemic effect of cytokines. These hypotheses have all raised the issue of whether sinusitis can contribute to the development of asthma and whether sinusitis and asthma share a common pathogenetic mechanism.Although etiology may be murky, there are several em-pirical studies, which suggest that treatment of sinusitis or rhinitis may improve asthma symptoms. For example,
CPm 8th EDItION ASthmA
85
in a study of 48 children with sinusitis and asthma, a re-ported improvement in asthma symptoms was generally noted after medical treatment for sinusitis.3 [LEVEL 4] In another series of studies, Slavin and colleagues reported on the effect of sphenoethmoidectomy in a series of adult patients with difficult to control asthma and medically resistant sinusitis.1 A total of 65% of pa-tients reported significant improvement in their asthma symptoms after the procedure.
References:1. Slavin RG. Asthma and sinusitis. J Allergy Clin Immunol
Gleich GJ. A clinical and pathologic study of chronic sinusitis: the role of eosinophil. J Allergy Clin Immunol 1988;81:867-75.
3. Demoly P, Crampette L, Mondain M, et al. Assessment of inflammation in noninfectious chronic maxillary sinusitis. J. Allergy Clin Immunol 1994;94:95-108.
4. Guidelines for the Diagnosis and Management of Asthma. National Asthma Education and Prevention Program. Expert Panel Report 2: Bethesda, MD: National Institutes of Health; National Heart, Lung, and Blood Institute 1997, NIH Publication 97 4051A.
5. Rachelefsky GS, Katz RM, Siegel SC. Chronic sinus diseasee with associated reactive airway disease with as-sociated reactive airway disease in children. Pediatrics. 1984;73:526-9.
Vaccines and Asthma
Question No. 1:Does influenza vaccination have a role in asthma management?
Answer:Yes. Influenza vaccination has been found to decrease the incidence of asthma exacerbations.1-3 [GRADE A]
Summary of Evidence:Immunization with influenza vaccine is safe and not associated with any significant side effects in adult patients with persistent asthma. Although pulmonary function abnormalities may occur as a complication of vaccination, the risk of pulmonary complications is very small and outweighed by the benefits of vaccina-tion.1 [LEVEL 1] There are no data from the published literature on whether pneumococcal vaccines lead to asthma exacerbation.
International guidelines recommend the immunization of patients with chronic pulmonary disease, including asthma, against influenza and pneumococcus. Despite these recommendations, many asthmatic patients do not receive vaccination because of some reports that vaccination, particularly influenza, may lead to asthma exacerbation. A double-blind placebo-controlled multi-centre crossover study was undertaken to assess the safety of influenza vaccine in patients with asthma.2 Among 225 participants with paired data, PEF fell to greater than 20% of baseline in 11 patients given the vaccine compared to three patients on placebo, and PEF fell more than 30% in eight patients given the vaccine
compared with none after placebo. However, when participants with colds were excluded from the analysis, no significant difference was noted in the number of patients whose PEF fell more than 20% between vaccine and placebo. It was also noted that there was a signifi-cant difference in patients whose PEF decreased more than 30% from baseline between the vaccine and the placebo group. These findings indicate that pulmonary function abnormalities may occur as a complication of influenza vaccination, however, the risk of pulmonary complications is very small. [LEVEL 2]
In a double-blind study by Steinus-Aarniala et al in 1988, 318 adult patients with chronic asthma were randomly allocated to receive either active vaccine or placebo.3 Follow-up for eight months after the vac-cination revealed no difference in asthmatic symptoms between the patients treated with active vaccine and those receiving placebo. [LEVEL 2]
References:1. Centers for Disease Control and Prevention. Prevention and
control of influenza. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Mortal Morb Wkly Rep 1993; 42 (No. RR-6):1-14.
2. Nicholson KG, et al. Randomized placebo-controlled crossover trial on effect of inactivated influenza vaccine on pulmonary function in asthma. Lancet 1998; 351:326-31.
3. Steinus-Aarniala, et al. Lack of clinical exacerbation in adults with chronic asthma after immunization with killed influenza virus. Chest 1986;89:786-9.
Appendix A
Abbreviations
AHR/BHR Airway/Bronchial HyperresponsivenessAnti-LTs Anti-leukotrienesaOG age of GestationBAL Bronchoalveolar LavageBDP Beclomethasone DipropionateBMD Bone Mineral DensityBUD BudesonideCS CorticosteroidCHS/NP Chronic Hyperplastic Sinusitis and Nasal PolypDPI Dry Powder InhalerEBV Epstein-Barr VirusECHRS European Community Health SurveyED Emergency DepartmentEIA Exercise Induced AsthmaEIB Exercise Induced BronchoconstrictionETS Environmental Tobacco SmokeFACET Formoterol and Corticosteroids Establishing
TherapyFEV1 Forced Expiratory Volume in 1secondFP Fluticasone PropionateFVC Forced Vital CapacityGERD Gastro Esophageal Reflux DiseaseGINA Global Initiative for AsthmaGRASSIC Grampian Asthma Study of Integrated Care TrialHEPA High Efficiency Particulate Air CleanerHFA HydrofluoralkaneHPA Hypothalamus-Pituitary-AdrenalISAAC International Study of Asthma and Allergy in
table III. Levels of Evidence for Rating Review Articles
Level 1 All of the following criteria are met: a. Comprehensive search for evidence b. Avoidance of bias in the selection of articles c. Assessment of the validity of each cited article; Conclusion supported by the data and analysis presentedLevel 2 3 of the 4 criteria are met. Level 4 1 of the 4 criteria are met.Level 3 2 of the 4 criteria are met. Level 5 None of the 4 criteria are met.
table I. Levels of Evidence for Rating Studies on the Accuracy of Diagnostic Tests
Level 1 All 5 of the following criteria are satisfied: a. There was an independent interpretation of the results of the diagnostic test (without knowledge of the results of the gold standard). b. There was an independent interpretation of the results of the gold standard (without knowledge of the results of the diagnostic test). c. The study of patients consisted patients (but not known) to have the disorder of interest. d. The diagnostic test and gold standard are both described in sufficient detail to allow reproducibility. e. The study population consists of at least 50 patients with and 50 patients without the disorder of interest.Level 2 4 of the 5 criteria are met. Level 5 1 of the 5 criteria are met.Level 3 3 of the 5 criteria are met. Level 6 None of the 5 criteria are met.Level 4 2 of the 5 criteria are met.
Grade A The recommendation is based on one or more studies at Level 1.Grade B The best evidence available is at Level 2.Grade C The best evidence is at Level 3Grade D The best evidence available is lower than 3, and include experts' opinions, clinical experience, and common sense. These recommendations address practical issues of implementation and other factors existing in the local setting.
table IV. Grading System for Recommendation
table II. Levels of Evidence for Rating Studies on the Effectiveness of Treatment
Level 1 A randomized controlled trial (RCT) that demonstrates a statistically significant difference in at least one major outcome - e.g., survival or major illness OR if the difference is not statistically significant, a RCT of adequate size to exclude 25% difference in relative risk with 80% power given the observed results.Level 2 A RCT that does not meet the level 1 criteria.Level 3 A non-randomized trial with concurrent controls selected by some systematic method (i.e., not selected on the basis of perceived suitability for one of the treatment options).Level 4 Before-after study or case series (at least 10 patients) with historical controls or controls drawn from other studies.Level 5 Case series (at least 10 patients) without controlsLevel 6 Case series (fewer than 10 patients) or case reports
IL-8 Interleukin 8IL-12 Interleukin 12IL-13 Interleukin 13IFN-γ Interferon gammaLABA Long Acting β2-antagonistLT LeukotrieneLTRA Leukotriene Receptor AntagonistMDI Metered-dose InhalerMSG Monosodium GlutamateNO2 Nitrogen DioxideNEB NebulizationO3 OzonePCRADM Philippine Consensus on Asthma Diagnosis and ManagementPC20 Provocative Concentration of Methacholine resulting in a 20%
fall in FEV1 from the baselinePEF Peak Expiratory FlowPFT Pulmonary Function TestPM Particulate MatterPMA Pre-Menstrual AsthmaPPD Purified Protein DerivativeRCT Randomized Control TrialRSV Respiratory Syncitial VirusSABA Short Acting β2-Agonist
SO2 Sulfur DioxideSR Slow-releaseTB TuberculosisTH1 T-helper subtype 1 lymphocyteTH2 T-helper subtype 2 lymphocyteWHO World Health Organization
CPm 8th EDItION ASthmA
87
Drugs Mentioned in the Treatment GuidelineThis index lists drugs/drug classifications mentioned in the treatment guideline. Prescribing information of these drugs can be found in PPD reference systems.