1
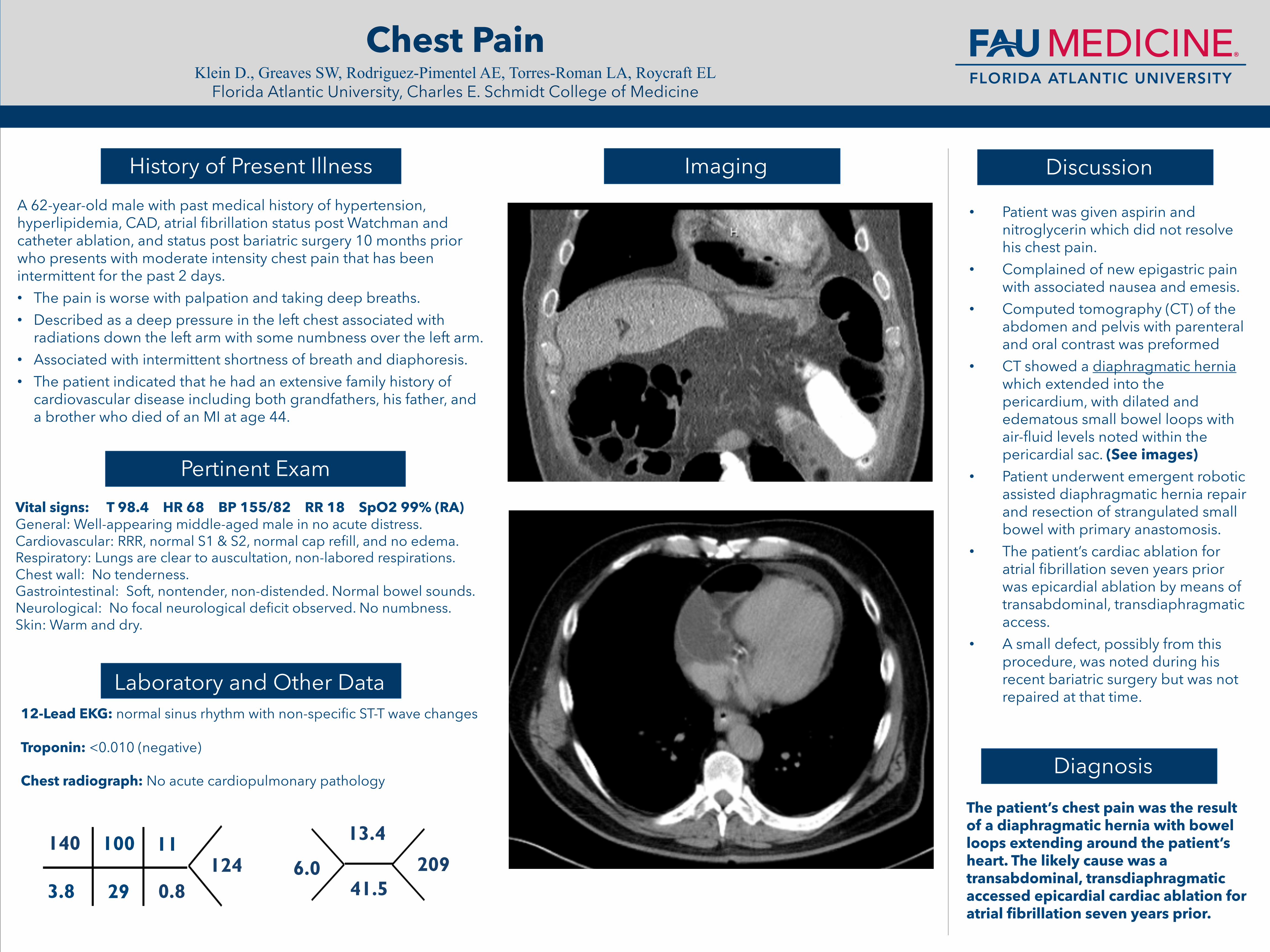
Chest Pain Klein D., Greaves SW, Rodriguez-Pimentel AE, Torres-Roman LA, Roycraft EL Florida Atlantic University, Charles E. Schmidt College of Medicine A 62-year-old male with past medical history of hypertension, hyperlipidemia, CAD, atrial fibrillation status post Watchman and catheter ablation, and status post bariatric surgery 10 months prior who presents with moderate intensity chest pain that has been intermittent for the past 2 days. • The pain is worse with palpation and taking deep breaths. • Described as a deep pressure in the left chest associated with radiations down the left arm with some numbness over the left arm. • Associated with intermittent shortness of breath and diaphoresis. • The patient indicated that he had an extensive family history of cardiovascular disease including both grandfathers, his father, and a brother who died of an MI at age 44. • Patient was given aspirin and nitroglycerin which did not resolve his chest pain. • Complained of new epigastric pain with associated nausea and emesis. • Computed tomography (CT) of the abdomen and pelvis with parenteral and oral contrast was preformed • CT showed a diaphragmatic hernia which extended into the pericardium, with dilated and edematous small bowel loops with air-fluid levels noted within the pericardial sac. (See images) • Patient underwent emergent robotic assisted diaphragmatic hernia repair and resection of strangulated small bowel with primary anastomosis. • The patient’s cardiac ablation for atrial fibrillation seven years prior was epicardial ablation by means of transabdominal, transdiaphragmatic access. • A small defect, possibly from this procedure, was noted during his recent bariatric surgery but was not repaired at that time. Diagnosis History of Present Illness Imaging Pertinent Exam 140 3.8 100 29 11 0.8 124 Laboratory and Other Data Vital signs: T 98.4 HR 68 BP 155/82 RR 18 SpO2 99% (RA) General: Well-appearing middle-aged male in no acute distress. Cardiovascular: RRR, normal S1 & S2, normal cap refill, and no edema. Respiratory: Lungs are clear to auscultation, non-labored respirations. Chest wall: No tenderness. Gastrointestinal: Soft, nontender, non-distended. Normal bowel sounds. Neurological: No focal neurological deficit observed. No numbness. Skin: Warm and dry. 6.0 13.4 41.5 209 12-Lead EKG: normal sinus rhythm with non-specific ST-T wave changes Troponin: <0.010 (negative) Chest radiograph: No acute cardiopulmonary pathology Discussion The patient’s chest pain was the result of a diaphragmatic hernia with bowel loops extending around the patient’s heart. The likely cause was a transabdominal, transdiaphragmatic accessed epicardial cardiac ablation for atrial fibrillation seven years prior.