62
Photon-beams: 3D CRT Narayan Sahoo April 7, 2011 Materials included in this lecture notes are from the previous lecture notes for this course by Karl Prado, Ph.D.

Photon-beams: 3D CRT
Narayan SahooApril 7, 2011
Materials included in this lecture notes are from the previous lecture notes for this course by Karl Prado, Ph.D.

GSBS Med Phys III
3D Conformal Radiation Therapy (3DCRT)
• 3DCRT is an external-beam radiation therapy technique in which treatment fields are designed to irradiate only volumes containing disease, while volumes of normal tissue that may be at risk of damage are spared

GSBS Med Phys III
3D Conformal Radiation Therapy (3DCRT): Concepts and Methods
• Volumes, Targets, and Margins– Definitions– Virtual Simulation– Beam Definition
• Dose Calculation and Plan Evaluation• Treatment Delivery / Verification
– Special Techniques

GSBS Med Phys III
3DCRT: Volumes and Targets
• ICRU 50 and 62• The GTV• The CTV• The PTV• Margins

GSBS Med Phys III
Targets, Volumes, Margins: Rationale
• One of the goals of radiation therapy is to increase the “therapeutic ratio”, i.e. maximize tumor control while minimizing complication probability.
From: Perez and Brady

GSBS Med Phys III
Targets, Volumes, Margins: Rationale
• To accomplish this goal, it is necessary to:– Accurately and
selectively target tumor volumes, and
– Avoid, as much as possible, critical normal structures
Critical Structures
Target Volumes

GSBS Med Phys III
Targets, Volumes, and Margins
• ICRU 50 and 62– Concepts and Definitions
• The GTV and the CTV– Definition and Methods
• The PTV– Margins
• Uncertainties
• Clinical applications: Thoracic XRT

GSBS Med Phys III
ICRU 50 and 62:Concepts and Definitions
• Rationale– Create a treatment-planning paradigm that
is based on physical and biological realities– Standardize this treatment-planning
system and its associated terminology• The GTV, CTV, and PTV
– Concepts and definitions

GSBS Med Phys III
ICRU (50) Volumes
• Gross Tumor Volume (GTV)
• Clinical Target Volume (CTV)
• Planning Target Volume (PTV)
GSBS Med Phys III
ICRU (62) Volumes
• The PTV (continued)– The PTV is designed to account for the
uncertainties in the size, shape, and position of the CTV:• Uncertainties can either be random
(physiological processes, patient movements) or systematic (weight loss, technical limitations)
• Uncertainties can occur either during a single fraction (intrafraction) or between fractions (interfraction)

GSBS Med Phys III
Classifications of Uncertainties
Intra-fractionRandom
Variation:
Intra-fractionSystematicVariation:
Inter-fractionRandom
Variation:
Inter-fractionSystematicVariation:
Variation ofCTV size /position
relative to afixed point in
the patient
Physiologicalprocesses:respiration,peristalsis,circulation
Physiologicalprocesses:bladder /
bowel content
Tumorreduction,weight loss
Variation ofthe patientrelative toisocenter
Patientmovements
Daily set-up Technicalerrors
IMSM

GSBS Med Phys III
Margins: Concepts
• The PTV: – “Planning Target Volume”– “Geometrical concept …”– Geometric uncertainties due to:
• Internal motion (Internal Margin)• Setup uncertainty (Setup Margin)

GSBS Med Phys III
Margins: Concepts / Definitions
• Internal Margin (IM):– Account for motion of internal anatomy
• Either target (CTV) or organs at risk (OAR)• Relative to some fixed point in the patient (i.e.
motion described in a patient coordinate system)
• Internal Target Volume (ITV)– Volume enclosing CTV throughout its
internal motion

GSBS Med Phys III
Margins: Concepts / Definitions
• The PTV• Setup Margin (SM):
– Accounts for patient motion relative to some exterior point of reference (i.e. the isocenter of the treatment unit)
– Depends on immobilization methods and on degree of ‘setup QA’

GSBS Med Phys III
Targets, Volumes, Margins
• The ITV
ITV = CTV + IM
• The PTV
PTV = ITV + SM
ITV
PTV
CTV

GSBS Med Phys III
3DCRT: Virtual Simulation
• Process / Tools– Imaging– Segmentation– Field Definition– Visualization
Tools

GSBS Med Phys III
Targets, and Volumes: Methods
• The GTV: Methods– “Clinically demonstrable …”
• Multi-modality Imaging– CT (Anatomy)– MRI (Proton density)– PET (Function)
• CT– Photon attenuation
• MRI – Magnetization energy
loss to environment• PET (FDG)
– Uptake of 18F-deoxy-D-glucose

GSBS Med Phys III
Virtual Simulation• Virtual Simulation Process
– The patient is set up on the CT scanner in treatment position. Immobilization devices are made and used during the scan.
– Once the patient is positioned on the table, the center of the volume to be scanned is placed at the intersection of the transverse, sagittal, and coronal positioning lasers.
– Preliminary marks are made on the patient and radio-opaque markers are placed to identify the location of patient marks on the CT images.

GSBS Med Phys III
Virtual Simulation• Virtual
Simulation– Isocenter
localization
Transfer the “marked isocenter” to planning system coordinates

GSBS Med Phys III
Virtual Simulation: Tools– Organ Segmentation and Contouring– Beam’s Eye Views (BEV)– Digitally Reconstructed Radiographs (DRR)

GSBS Med Phys III
Virtual Simulation: Tools• Contouring Tools
– Drawing tools that allow the planner to outline structures and planning volumes by creating contours around them
– Process is often called organ segmentation

GSBS Med Phys III
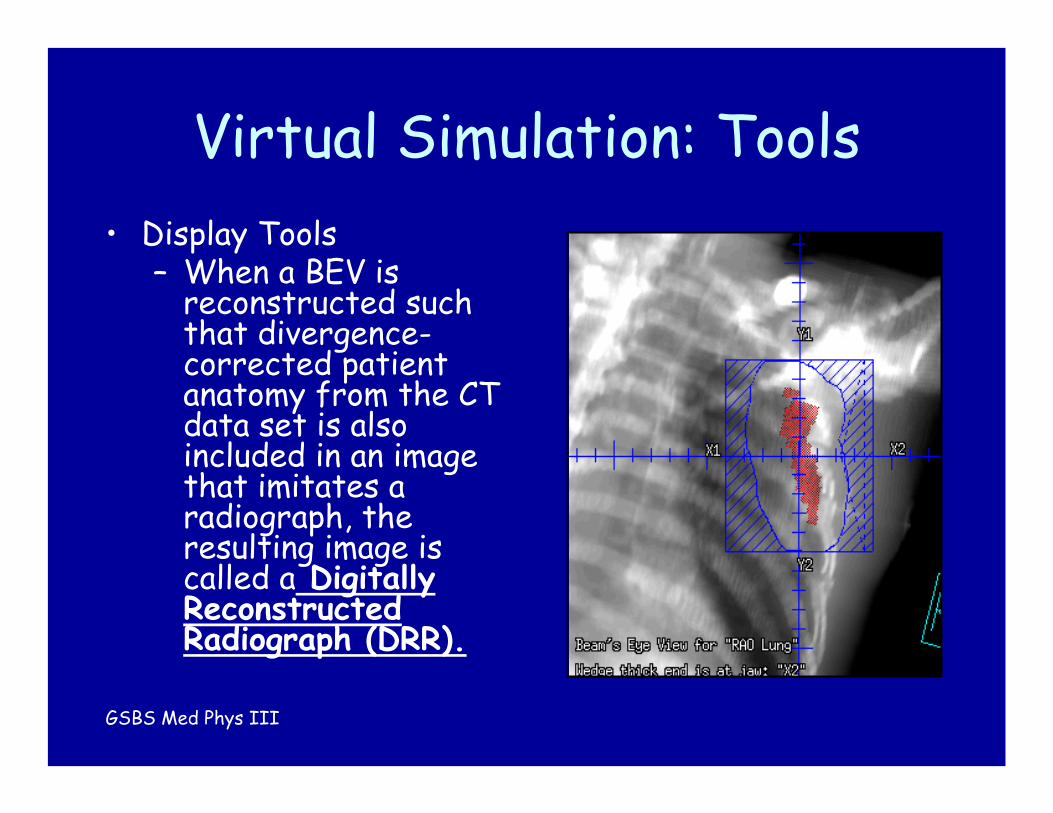
Virtual Simulation: Tools• Display Tools
– The particular view of the patient anatomy from the perspective of the treatment field is called a Beam’s Eye View (BEV).
GSBS Med Phys III
Virtual Simulation: Tools• Display Tools
– When a BEV is reconstructed such that divergence-corrected patient anatomy from the CT data set is also included in an image that imitates a radiograph, the resulting image is called a Digitally Reconstructed Radiograph (DRR).

GSBS Med Phys III
Virtual Simulation: Tools• Other Virtual Simulation Tools
– Skin rendering– Laser display

GSBS Med Phys III
GTV Definition Methods• The GTV: Methods
– “Clinically demonstrable …”– Multi-modality fusion (PET/CT)

GSBS Med Phys III
CTV Definition Methods• The CTV:
– Recall: The CTV encompases “… subclinical, microscopic … suspected …” disease
– Current definition methods: • Pathology

GSBS Med Phys III
CTV Definition Methods
• Topic of ongoing research• For Example: Clinical Trial (Canada):
– Biological imaging for optimization of CTV definition in patients with prostate cancer
– Rationale – Use of multi-modality imaging –dynamic contrast-enhanced MRI, and 11C choline - to better identify CTV

GSBS Med Phys III
ITV Definition Methods
Courtesy of: Thomas Guerrero, M.D. Ph.D., Yerko Borghero, M.D., and Craig Stevens, M.D., Ph.D.
• Relationship between an ITV determined from breath-hold CT, and PET imaging.
FB.
Exp. Insp.

GSBS Med Phys III
ITV Definition Methods• The ITV (more specifically IGTV) can be
determined from Breath Hold or 4DCT scans

GSBS Med Phys III
ITV Definition: 4DCT• Contour determined from a 4D “MIP”
(Maximum Intensity Projection)
Courtesy of: Peter Balter, Ph.D. and Tinsu Pan, Ph.D.

GSBS Med Phys III
Volumes and Margins: Thoracic Example
• Method 1 (Measured ITV):– IGTV = “Envelope” of BH GTVs (MIP)– CTV = GTV + 8 mm (Giraud, et. al.)– PTV = ITV + 7 mm (setup margin) + 3 mm (residual
motion)• Method 2 (Conventional and Gating):
– CTV = GTV + 8 mm– PTV = CTV + 15 mm (8 mm tumor motion + 7 mm
setup uncertainty)

GSBS Med Phys III
The “Final” Thoracic PTV• The ‘Final’ PTV = IGTV + 8 mm + SM + 3 mm
CTV
IG’TV
CTV
SM

GSBS Med Phys III
Treatment Field Definition• Process
– Using both 2D and 3D viewing techniques, the angles of the gantry and couch are adjusted to include the PTV in the beam while excluding critical structures out of the path of the beam.
– The collimator size and rotation can be adjusted also to exclude structures from the beam.

GSBS Med Phys III
Treatment Field Definition• Number and geometry of treatment beams
should be carefully considered
GSBS Med Phys III
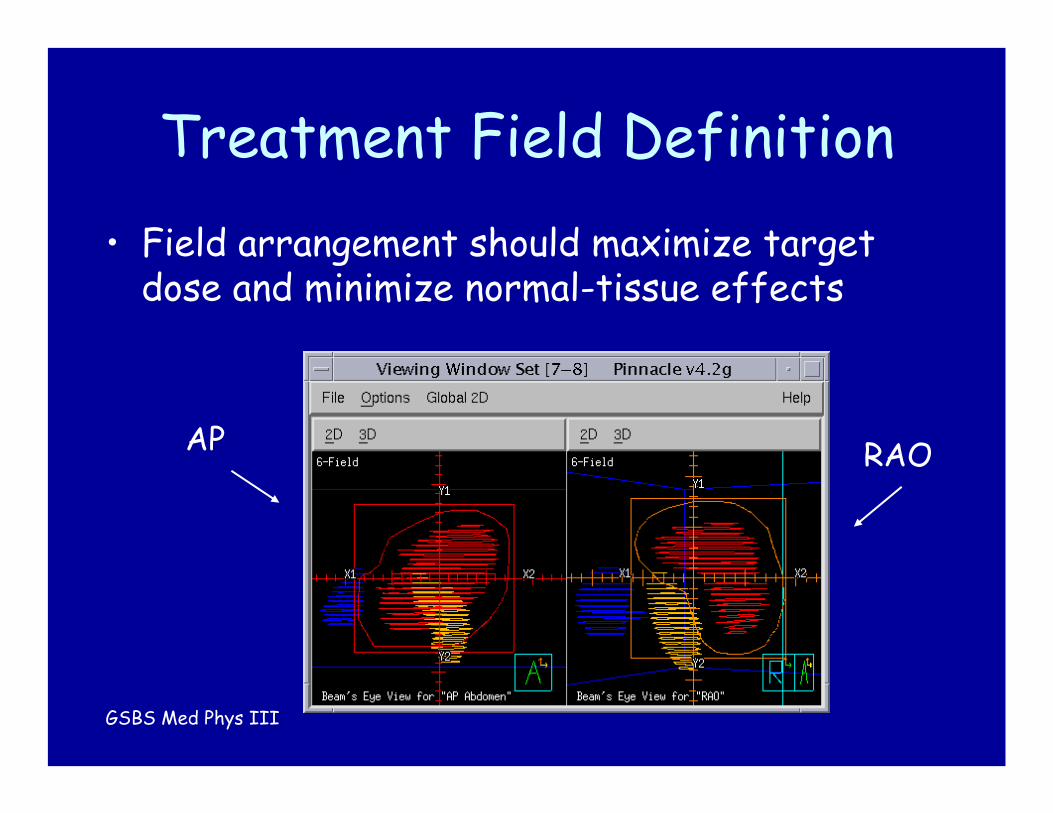
Treatment Field Definition• Field arrangement should maximize target
dose and minimize normal-tissue effects
AP RAO

GSBS Med Phys III
Treatment Field Definition• Process:
– The shape of the treatment field can be fashioned using an MLC or conventional blocking.
• Auto-fielding, a technique used to set an open area around the PTV from the perspective of the beam’s eye view, can be used to shape the field following the contour of the PTV.
• The auto-field should include a margin around the PTV that allows for beam penumbra and block edge effects.
• The margin should be sufficient to allow isodose lines of 90% or greater to cover the PTV

GSBS Med Phys III
Treatment-Field Definition:Distance to Block Edge
• An additional margin is added around the PTV to ensure it is encompassed by a suitable isodosesurface

GSBS Med Phys III
Treatment-Field Definition:Distance to Block Edge
• Distances to Block Edge from a 95% (relative to isocenter) isodose surface depend on:– Number of beams, beams’ field sizes, and
the beams’ “Off-Axis” and (to a smaller degree) penumbral characteristics
– To a much lesser degree, on:• Energy and depth
Rosen, et. al., Unpublished Data

GSBS Med Phys III
Treatment-Field Definition:Distance to Block Edge
• Essentially, distances to block edges will depend on the specifics of the treatment plan:– Number and sizes of beams, isodose
surface of choice, irradiation media (homogeneous vs. heterogeneous)
• Best to evaluate on the basis of resulting dose distribution

GSBS Med Phys III
3DCRT: Dose Calculation and Plan Evaluation
• Dose Calculation Algorithms• The Dose Volume Histogram (DVH)

GSBS Med Phys III
Dose Calculations• Dose is calculated at each voxel within a 3D
dose matrix– Note: The dose matrix is generally of less spatial
resolution than the image matrix (e.g. 4 mm versus 1 mm voxels)
• Calculation algorithms vary in capabilities and complexity– 2D versus 3D, incorporation of scatter,
heterogeneity corrections• We will emphasize 3D Convolution

GSBS Med Phys III
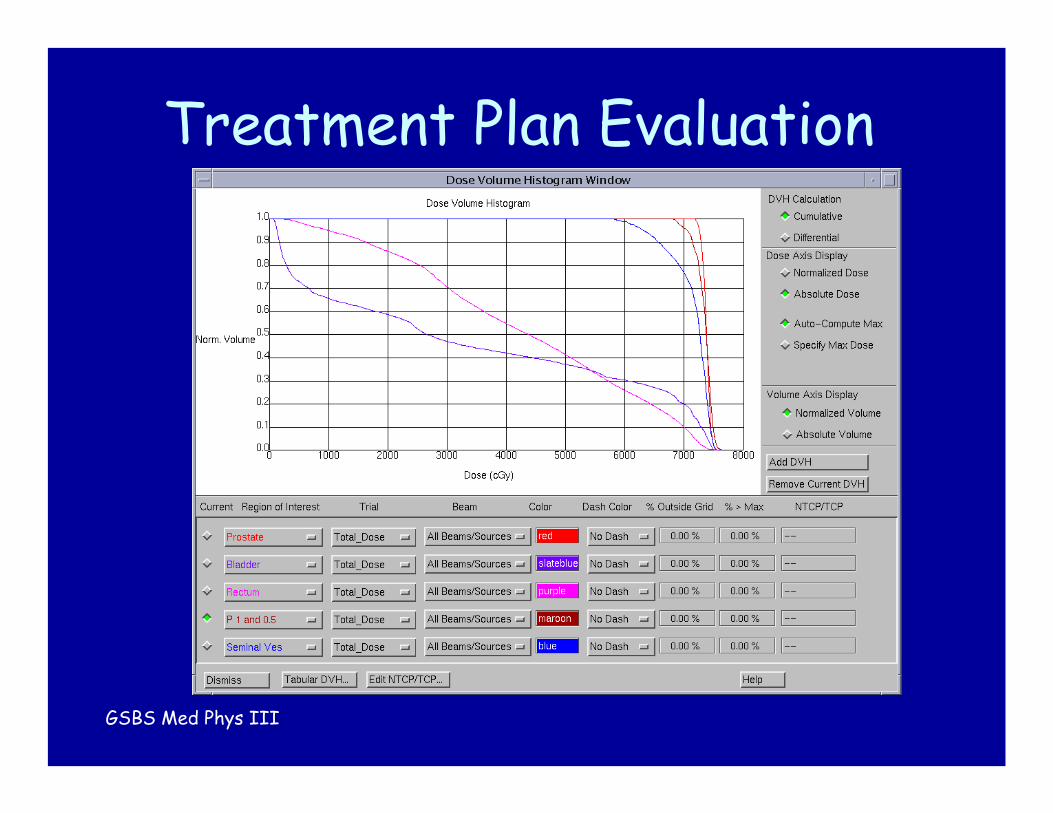
Treatment Plan Evaluation
• Dose Evaluation– Dose “clouds”
• Enclose volumes receiving doses greater than or equal to the value of the dose cloud
Regions outside the dose cloud are under-dosed.
GSBS Med Phys III
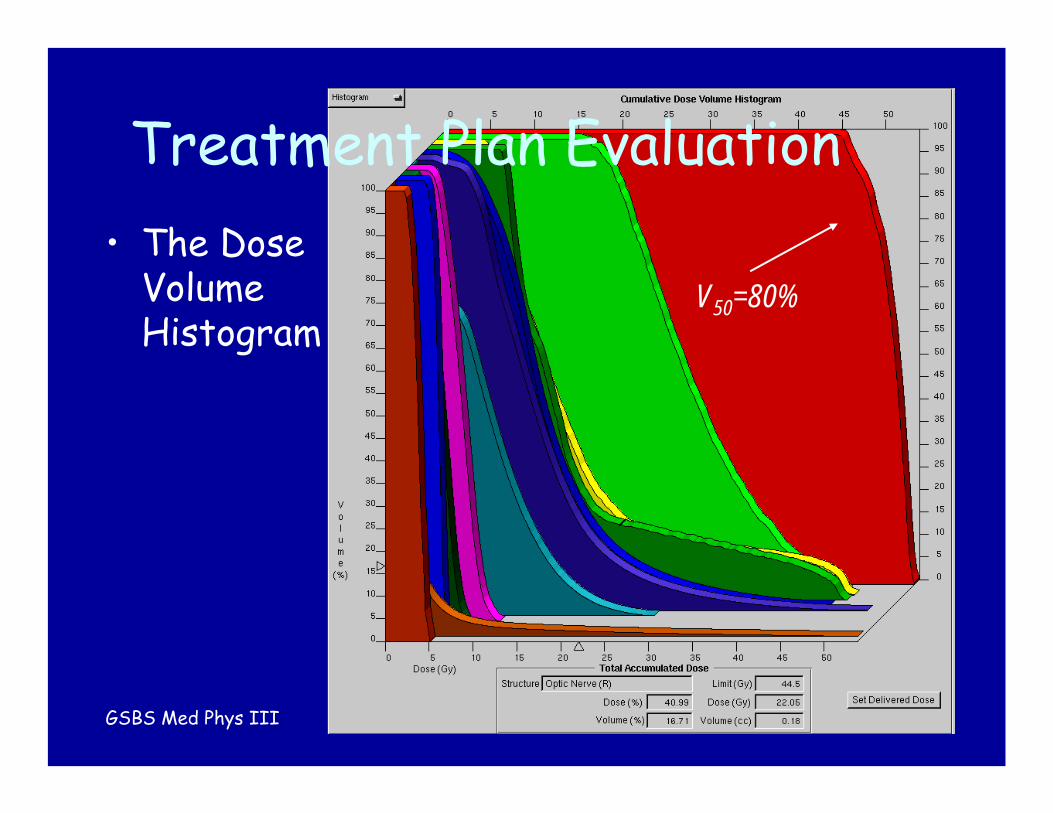
Treatment Plan Evaluation• The Dose
Volume Histogram
V50=80%

GSBS Med Phys III
Treatment Plan Evaluation
• Dose Evaluation– The Dose-Volume Histogram (DVH) is a plot of
target or normal structure volume as a function of dose.
– It is, in essence, a frequency distribution of the number of target or normal-structure voxels (volume elements) receiving a certain dose.
– In its most common form (the “cumulative”DVH), it is a plot of volume versus the minimum dose absorbed within that volume.
GSBS Med Phys III
Treatment Plan Evaluation

GSBS Med Phys III
Treatment Plan Evaluation
• Dose Evaluation– The characteristics of an optimal target-volume
DVH are:• (1) high percentage volume at prescribed target dose
(adequate target volume coverage), and• (2) rapid decrease in volume beyond the prescribed
dose (dose uniformity within target).– Interpretation of Organ-at-Risk (OAR) DVHs is
somewhat more complex.• Serial versus Parallel Structures

GSBS Med Phys III
Treatment Plan Evaluation
• OAR Dose Evaluation– The overall function of organs consisting of
serial response tissues can be affected by the incapacitation of only one element.
• The spinal cord is such an organ. The high-dose region of a serial-tissue DVH is of particular importance.
– The overall function of organs consisting of parallel response tissues, on the other hand, is affected by the injury of a number of elements of that organ above a certain minimum.
• The liver is an example of such an organ.

GSBS Med Phys III
3DCRT: Treatment Deliveryand Verification
• The modern linear accelerator– The Multi-leaf Collimator (MLC)– Image Guided RT– Respiratory Gating
• Treatment Delivery QA

GSBS Med Phys III
The Modern Linear Accelerator
• The MLC– Now “Standard”– Field Shaping– Intensity Modulation– Multiple Designs /
Resolution

GSBS Med Phys III
The Modern Linear Accelerator
• On-Board Imaging (OBI)– MV Imaging (EPID)– kV Imaging
• Orthogonal to MV Beam
– IGRT• Image registration
/ couch positioning software
• Cone-Beam CT

GSBS Med Phys III
The Modern Linear Accelerator
• Respiratory Gating– Treatment beam
can be ‘triggered’based on signal from respiratory marker
-0.2
0
0.2
0.4
0.6
0.8
1
1.2
1.4
0 5 10 15 20 25 30
Time
Dis
plac
men
t

GSBS Med Phys III
Treatment Delivery QA
• GOAL: Ensure that dose prescription is fulfilled– Treatment planning:
• Target volume coverage• Acceptable dose to OARs
– Treatment delivery• Proper transfer of field information• Proper field targeting

GSBS Med Phys III
Treatment Planning Guidelines: Thoracic RT (RT Alone)
V30 < 40%LiverV60 < 50%EsophagusV50 < 50%HeartV20 < 40%Lung50 Gy maxCordVRX > 95%PTVDose/VolumeStructure

GSBS Med Phys III
Treatment Verification

GSBS Med Phys III
Treatment Verification

GSBS Med Phys III
Information Network

GSBS Med Phys III
Verification of Treatment Delivery: Traditional Methods
• MV (and now kV) Images
• Anatomy and reticule based
• With digital imaging can use image-enhancement tool– Histogram
Equalization

GSBS Med Phys III
Newer Image Guidance
• “2D” Match– Image (kV)
registration to plan DRR
– Couch shift computed (and can be applied)
Tina Briere, Ph.D., Patricia Lindsay, Ph.D.
AP Lat
DRR
kV
Varian

GSBS Med Phys III
Courtesy of: Lei Dong, Ph.D., and Associates
Treatment Verification

GSBS Med Phys III
Treatment Verification• Use of implanted fiducial markers to assess
internal / setup uncertainty
Courtesy: C. Nelson, G. Starkschall

GSBS Med Phys III
3D Conformal Radiation Therapy: Summary
• The goal is to target “insightfully”– Define targets and organs at risk as accurately
as possible• Use / understand the technology• Follow ICRU guidance
– Manage margins carefully• First treat the disease
– “The most radio-resistant cell is that outside of the treatment field” – “Anonymous”
• Protect normal structures• Measure uncertainties

GSBS Med Phys III
3D Conformal Radiation Therapy: Summary
• Plan and treat carefully– Make use of 3D tools– Utilize dose/volume information– Exercise caution in treatment delivery
• Verify information transfer– Technology is not perfect
• Use in-room imaging
• Do what is “reasonable and prudent”

















