27
Phyllodes breast tumor Joint Hospital Surgical Grand Round 26 April 2014 Ng Yuen Shan, Sandy (Tuen Mun Hospital)
| Date post: | 22-Dec-2015 |
| Category: |
Documents |
| Upload: | dale-joseph-elliott |
| View: | 225 times |
| Download: | 0 times |

Phyllodes breast tumor
Joint Hospital Surgical Grand Round26 April 2014
Ng Yuen Shan, Sandy(Tuen Mun Hospital)

Phyllodes tumor Rare fibroepithelial breast tumor (1% of all
breast tumors, 2.5% of all fibroepithelial tumors)
A spectrum of disease Epithelial and cellular stromal component Histological classification:
Benign (60%) Borderline (20%) Malignant (20%) distant metastasis

Median age of presentation at 40-50 years Palpable mass with rapid growth, large size
(>2cm) Poor pre-operative diagnostic accuracy

Case scenario
F/40 2.5cm L12H breast mass, interval growth. MMG/US: well-circumscribed lobulated mass FNAC: benign. Excisional pathology:
Benign phyllodes tumor Margin POSITIVE

Pok Oi Hospital A review of 28 consecutive patients with phyllodes
tumour excision in 2009-2012 in Pok Oi Hospital 11 operations performed for recurrent phyllodes tumour
(6 patients) have been excluded.
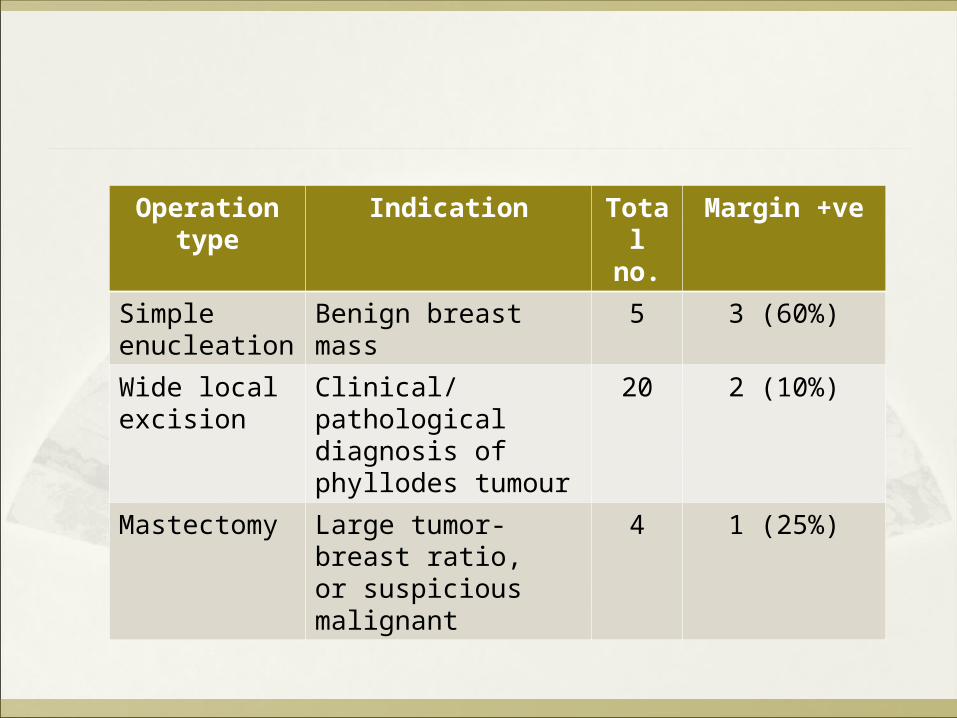
Operation type Indication Total no.
Margin +ve
Simple enucleation
Benign breast mass 5 3 (60%)
Wide local excision
Clinical/ pathological diagnosis of phyllodes tumour
20 2 (10%)
Mastectomy Large tumor-breast ratio, or suspicious malignant
4 1 (25%)

Margin status and histological grade
Involved Touch/ close <1 cm >/= 1 cm
Malignant 2 0 4 2
Borderline 1 2 3 3
Benign 3 3 3 3
Close follow-up

Margin-involved outcomes Age Grade Tumour
size (cm)Primary Operation
FU duration (months)
Lost to FU
Reoperation
Patient A 63 Malignant 3.2 WLE 48 No No
Patient B 48 Malignant 11 Mastectomy 18 No No
Patient C 42 Borderline 6 WLE 14 No Mastectomy for co-existing DCIS
Patient D 50 Benign 7.5 Enucleation 57 No Wide local excision for recurrent phyllodes
Patient E 21 Benign 3.5 Enucleation 35 Yes No
Patient F 40 Benign 2.2 Enucleation 47 No No
Mean FU period: 36 months

POH case series
Results:Local recurrence rate in margin-involved = 16.7%No recurrence was detected in close or clear margin.
Conclusion: Margin status of the primary resection is probably the most important factor in determining risk of recurrence.

Margin-involved phyllodes tumor
Why does it matter? What to do next? How to “prevent”?

Local recurrence
Spitaleri G, Toesca A, Botteri E, et al. Breast phyllodes tumor: a review of literature and a single center retrospective series analysis. Crit Rev Oncol Hematol. 2013 Nov;88(2):427-36.
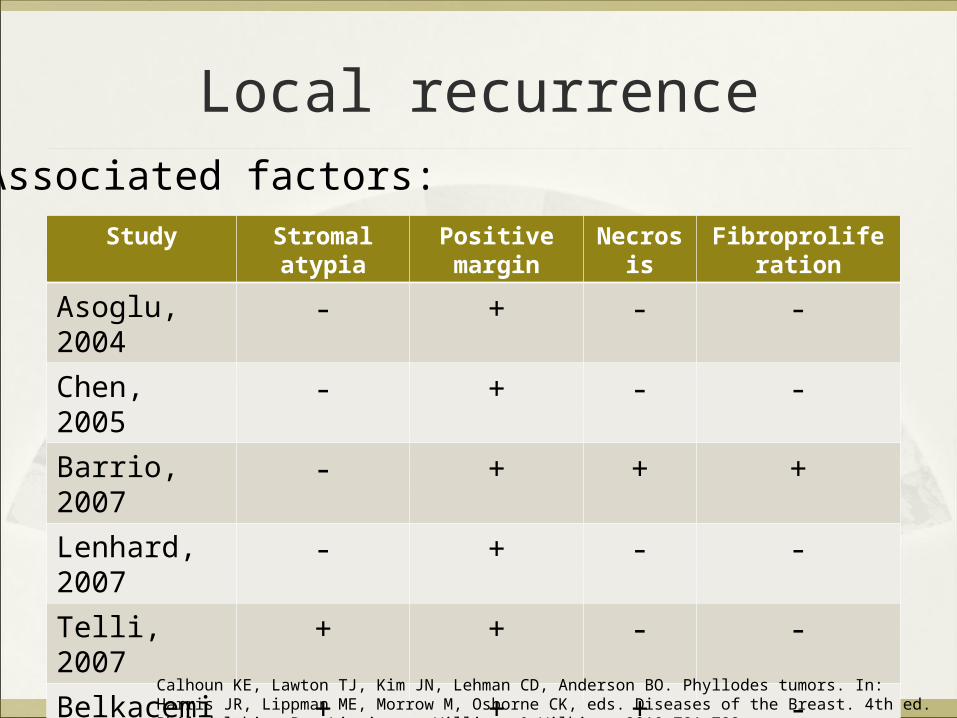
Local recurrence
Study Stromal atypia Positive margin Necrosis Fibroproliferation
Asoglu, 2004 - + - -Chen, 2005 - + - -Barrio, 2007 - + + +Lenhard, 2007 - + - -Telli, 2007 + + - -Belkacemi, 2008
+ + + -
Associated factors:
Calhoun KE, Lawton TJ, Kim JN, Lehman CD, Anderson BO. Phyllodes tumors. In: Harris JR, Lippman ME, Morrow M, Osborne CK, eds. Diseases of the Breast. 4th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2010:781-792.

Disease-free survival curves of 42 patients treated with breast-conservative surgery for phyllodes tumor.
Taira N, Takabatake D, Aogi K, et al. Phyllodes Tumor of the Breast: Stromal Overgrowth and Histological Classification are Useful Prognosis-predictive Factors for Local Recurrence in Patients with a Positive Surgical Margin. Jpn J Clin Oncol 2007;37(10)730–736

Taira N, Takabatake D, Aogi K, et al. Phyllodes Tumor of the Breast: Stromal Overgrowth and Histological Classification are Useful Prognosis-predictive Factors for Local Recurrence in Patients with a Positive Surgical Margin. Jpn J Clin Oncol 2007;37(10)730–736

Margin-involved phyllodes tumor
Why does it matter? Predictor of local recurrence
What to do next? How to “prevent”?
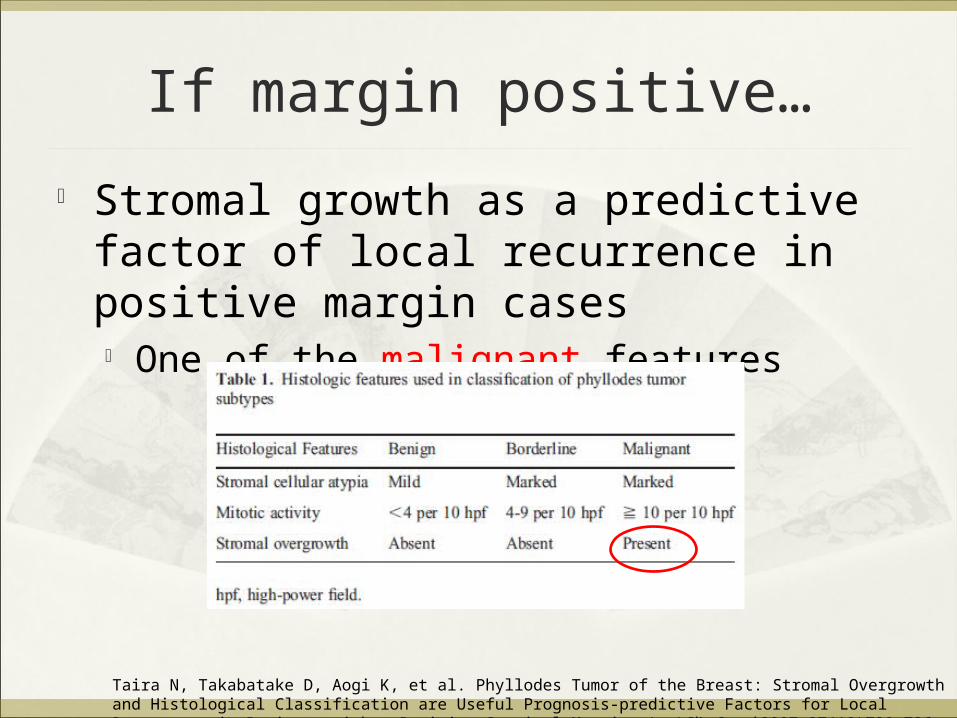
Stromal growth as a predictive factor of local recurrence in positive margin cases One of the malignant features
Taira N, Takabatake D, Aogi K, et al. Phyllodes Tumor of the Breast: Stromal Overgrowth and Histological Classification are Useful Prognosis-predictive Factors for Local Recurrence in Patients with a Positive Surgical Margin. Jpn J Clin Oncol 2007;37(10)730–736
If margin positive…

If margin positive…
Some authors had suggested “wait-and-see” policy for benign phyllodes tumor
Chua, 1989 (106 patients)
Zurrida, 1992 (216 patients): recurrence 8%
Chua CL, Thomas A, Ng BK. Cystosarcoma phyllodes: a review of surgical options. Surgery 1989;105(2 Pt 1):141-147Zurrida S, Bartoli C, Galimberti V, et al. Which therapy for unexpected phyllodes tumour of the breast? Eur J Cancer 1992;28(2-3):654-657

Management strategy ofMargin-involved phyllodes tumor
Benign “wait-and-see” Malignant Re-excision Follow-up every 6 months for initial 2-3 years
(highest chance of recurrence) Then yearly Self breast examination Clinical suspicion on follow-up: triple assessment
Margin-involved phyllodes tumor
Why does it matter? What to do next? How to “prevent”?

Phyllodes tumor
Difficult preoperative diagnosis…..

Phyllodes tumor – Initial workup
Clinical suspicious of phyllodes tumor- Palpable mass- Rapid growth- USG suggestive of fibroadenoma except for size (>2cm) / rapid growth
- History and P/E- USG- MMG for >30yo
Core needle biopsy
Fibroadenoma or indeterminate
Phyllodes tumor (benign, borderline, malignant)
Observe
Fibroadenoma
Excisional biopsy Wide excision (>=1cm) without axillary staging
Patient presentation Triple assessment
M D Anderson Cancer Center 2012

Margin-involved phyllodes tumor
Why does it matter What to do next How to “prevent”
?

Thank you
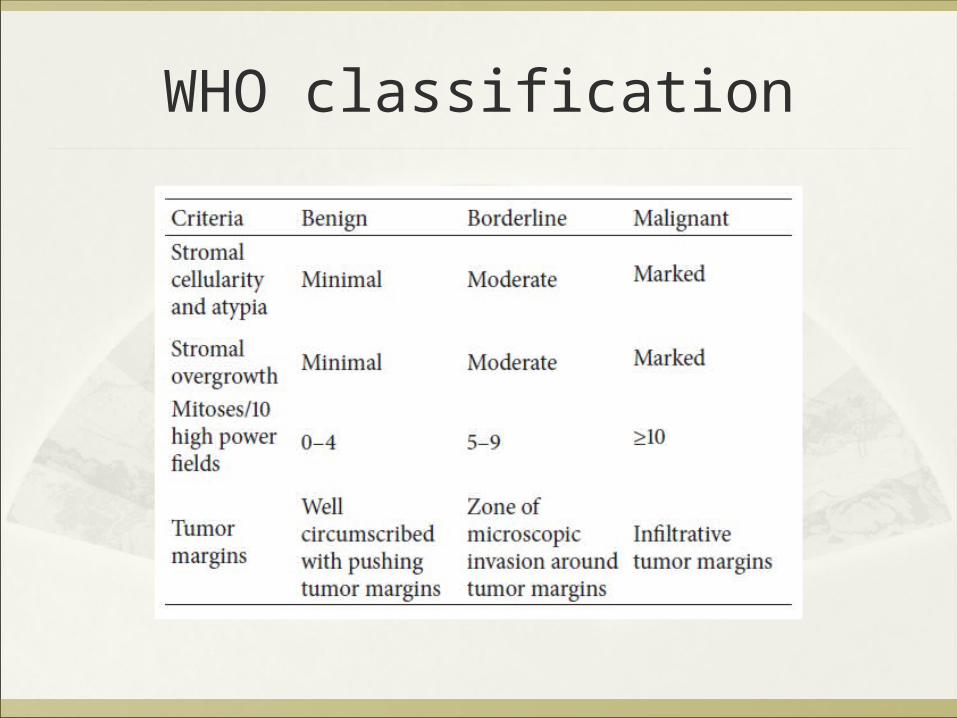
WHO classification


To improve preoperative diagnosisPaddington Clinicopathological Suspicion ScoreClinical findings
Sudden increase in size in a longstanding breast lesion Apparent fibroadenoma >3cm diameter or in patient >35
yearsImaging findings
MMG: Rounded borders/ lobulated appearance USG: Attenuation or cystic areas within a solid mass
FNAC findings Presence of hypercellular stromal fragments Indeterminate features
ANY 2 features mandate core biopsyR K Jacklin, P F Ridgway, P Ziprin, et al. Optimising preoperative diagnosis in phyllodes tumour ofthe breast. J Clin Pathol 2006;59:454–459.
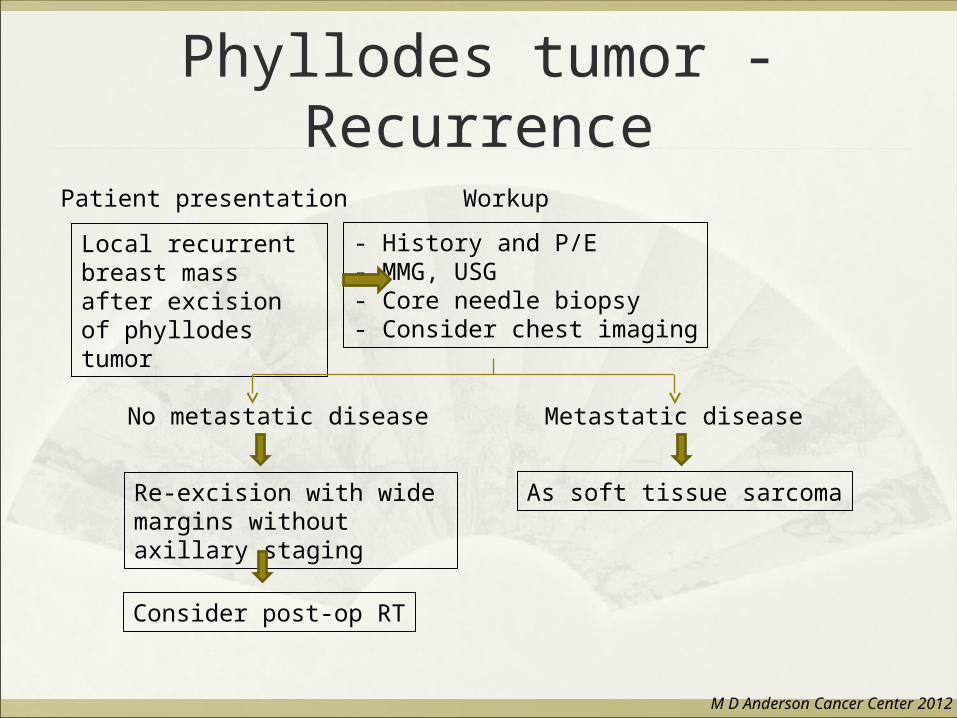
Phyllodes tumor - Recurrence
Local recurrent breast mass after excision of phyllodes tumor
- History and P/E- MMG, USG- Core needle biopsy- Consider chest imaging
No metastatic disease Metastatic disease
Re-excision with wide margins without axillary staging
Consider post-op RT
As soft tissue sarcoma
Patient presentation Workup
M D Anderson Cancer Center 2012

















