79
+ Physiology Of Menstruation Dr Anusha Rao P PGY2 (OBG)
| Date post: | 15-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | anusha-rao-p |
| View: | 281 times |
| Download: | 4 times |

+
Physiology Of
Menstruation
Dr Anusha Rao PPGY2 (OBG)

+
Menstruation is a visible manifestation of cyclic, physiologic
uterine bleeding due to shedding of the endometrium following
invisible interplay of hormones mainly through H-P-O axis.
Normal limits:
Frequency: 24-38 days
Regularity: +/- 2-20 days
Duration: 4-8 days
Volume: 5-80 mL

+

+HORMONES FOLLICULAR
PHASE
OVULATION LUTEAL PHASE
DAILY
PRODUCTION
(ug)
OESTRADIOL
PROGESTERONE
50
2 - 3
150-300 100
20 -30
SERUM VALUES
OESTRADIOL
(pg/ml)
PROGESTERONE
(ng/ml)
FSH (mIU/ml)
LH (mIU/ml)
50
<1
10
5
300- 600
15- 20
60
150-200
>5
10
5
DAILY
EXCRETION
TOTAL
OESTROGEN (ug)
PREGNANEDIOL
(mg)
10-25
<1
35- 100 25-75
3-6

+

+ Menstrual cycle can be explained in two cycles which occur
concurrently
• The ovarian cycle and
• The uterine cycle
The Ovarian Cycle consists of
The follicular phase and
The luteal phase
The Uterine Cycle consists of
The proliferative phase and
The secretory phase

+THE OVARIAN
CYCLE

+Follicular
phase

+

+Primordial follicle
Originate in the Endoderm
Migrate to the genital ridge at 5-6weeks
Maximum at 16 – 20 wks : 6 – 7 million
At Birth : 2 million
At Pubery : 0.3 to 0.5 million
Only 400 – 500 follicles ovulate during a woman’s reproductive
years.

+
The primordial follicle is nongrowing and consists of an oocyte,
arrested in the diplotene stage of meiotic prophase, surrounded
by a single layer of spindle-shaped granulosa cells.

+
The initial recruitment and growth of the primordial follicles is gonadotropin
independent and affects a cohort over several months
The total duration of time to achieve pre ovulatory status is approximately 85
days
First visible signs of development are
Increase in the size of oocyte
granulosa cells becoming cuboidal

+
Gap junctions composed of channels formed by arrangement of
proteins known as Connexins –
up regulated and kept open by FSH and
down regulated and closed by LH

+The Pre antral Follicle
Oocyte enlarges and is surrounded by a membrane, the zona
pellucida.
The granulosa cells undergo a multilayer proliferation as the theca
layer continues to organize from the surrounding stroma.

+
The granulosa cells of the preantral follicle synthesizes all 3 classes of
steroids
Estrogens are produced more than androgens or progestins
An aromatase enzyme system converts androgens to estrogens and is a
factor limiting ovarian estrogen production.
Aromatization is induced or activated through the action of FSH.

+
FSH both
initiates steroidogenesis (estrogen production) in granulosa
cells and
stimulates granulosa cell growth and proliferation

+

+
The Antral Follicle Under the influence of estrogen and
FSH, there is an increase in the
production of follicular fluid.
Oocyte and the surrounding granulosa
cells are nurtured in this follicular fluid
The granulosa cells surrounding the
oocyte are now designated the
cumulus oophorus

+
P45OC17
P450arom

+The Two-Cell,
Two-Gonadotropin System
The aromatase activity of the granulosa cells is more than
thecal cells.
In human preantral and antral follicles,
LH receptors are present only on the theca cells and
FSH receptors only on the granulosa
LH stimulates thecal cells to produce androgens that can then
be converted, through FSH-induced aromatization, to
estrogens in the granulosa cells.

+
As the follicle emerges, the theca cells are characterized by their
expression of P450c17, the enzyme step that is rate limiting for the
conversion of 21-carbon substrate to androgens.
Increasing expression of the aromatization system (P450arom) is a
marker of increasing maturity of granulosa cells.
The presence of P450c17 only in theca cells and P450arom only in
granulosa cells is an impressive evidence confirming the two-cell,
two-gonadotropin explanation for estrogen production

+Selection of the Dominant Follicle
The process of conversion of a single follicle to a estrogen
dominant follicle depends on
(1) a local interaction between estrogen and FSH within the follicle,
:-positive feedback
(2) the effect of estrogen on pituitary secretion of FSH:- negative
feedback.
Serves to withdraw gonadotropin support from the other less
developed follicles.

+
The first event in the process of atresia is a reduction in FSH
receptors in the granulosa layer
A wave of atresia among the lesser follicles,
is seen to parallel the rise in estrogen.

+
Lower GnRH pulse frequencies favor FSH secretion, and
higher GnRH pulse frequencies favor LH secretion.
Low levels of estrogen enhance FSH and LH synthesis and
storage, have little effect on LH secretion, and inhibit FSH
secretion.

+
+
High levels of estrogen induce the LH surge at midcycle, and
high steady levels of estrogen lead to sustained elevated LH
secretion.
Low levels of progesterone acting at the level of the pituitary
gland enhance the LH response to GnRH and are responsible
for the FSH surge at midcycle.
High levels of progesterone inhibit pituitary secretion of
gonadotropins by inhibiting GnRH pulses at the level of the
hypothalamus.

+Inhibin, Activin, and Follistatin
This family of peptides is synthesized by granulosa cells in
response to FSH and secreted into the follicular fluid and
ovarian venous effluent.
They are expressed in many tissues through out the body as
autocrine-paracrine regulators.
Inhibin is an important inhibitor of FSH secretion.
Activin stimulates FSH release in the pituitary and augments
FSH action in the ovary.
Follistatin suppresses FSH activity by binding to activin.
+
Inhibin
Blocks the synthesis and secretion of FSH,
Prevent the up-regulation of GnRH receptors by GnRH,
Reduce the number of GnRH receptors present,
At high concentrations, promote the intracellular degradation of
gonadotropins.

+The Preovulatory Follicle
Granulosa cells in the preovulatory follicle
enlarge and acquire lipid inclusions
And theca becomes vacuolated and richly
vascular, giving the preovulatory follicle a
hyperemic appearance.
The oocyte proceeds in meiosis,
approaching completion of its reduction
division.
Approaching maturity, the preovulatory
follicle produces increasing amounts of
estrogen.
Estrogen peaks approximately 24 to 36
hours prior to ovulation.

+
The onset of the LH surge occurs when the peak levels of
estradiol are achieved.
In providing the ovulatory stimulus to the selected follicle, the
LH surge seals the fate of the remaining follicles, with their
lower estrogen and FSH content, by further increasing
androgen superiority.
LH promotes luteinization of the granulosa in the dominant
follicle, resulting in the production of progesterone

+
After adequate estrogen priming, progesterone facilitates the
positive feedback response.
And in the presence of subthreshold levels of estradiol can
induce a characteristic LH surge.
When administered before the estrogen stimulus, or in high
doses (achieving a blood level greater than 2 ng/mL),
progesterone blocks the midcycle LH surge.

+
Progesterone at midcycle is significantly responsible for the
FSH surge.
Thus ensures completion of FSH action on the follicle,
especially making sure that a full complement of LH receptors
is in place in the granulosa layer.
As products of thecal tissue are androgens, the increase in
stromal tissue in the late follicular phase is associated with a
rise in androgen levels.
- for atresia of lesser follicles and for libido
enhancement

+Ovulation

+
A threshold of LH concentration must be maintained for at least
14 to 27 hours in order for full maturation of the oocyte to occur.
Usually the LH surge lasts 48 to 50 hours

+
LH, FSH, Progesterone, growth factors
Plasminogen activator synthesis (granulosa &theca cells)
Plasminogen Plasmin
Collagenase
Disrupts follicular wall

+

+
Estradiol levels plunge as LH reaches its peak. This may be a consequence of LH down-regulation of its own receptors on the follicle.
Due to-
High LH causes supression of steroidogenesis
Low midcycle levels of progesterone exert an inhibitory action on further granulosa cell multiplication, and hence the drop in estrogen
Estrogen can exert an inhibitory effect on P450c17(aromatase enzyme)

+LUTEAL
PHASE

+
Luteinization and the corpus luteum:
granulosa cells increase in size and assume a characteristic
vacuolated appearance associated with the accumulation of a
yellow pigment , lutein.
theca lutein cells may differentiate from the surrounding theca
and stroma to become part of the corpus luteum.

+
Angiopoietin-1 binds to the endothelial Tie-2 receptor & inc.
expr. Of VEGF + LH -> Angiogenesis
Angiopoietin-2, leads to vascular breakdown that accompanies
luteolysis.
Vascularization of the granulosa layer is essential to allow LDL-
cholesterol to reach the luteal cells to provide sufficient
substrate for progesterone.
By day 8 or 9 after ovulation, a peak of vascularization is
reached, associated with peak levels of progesterone and
estradiol in the blood.
+
The leukocytes in the corpus luteum secrete cytolytic
enzymes, prostaglandins, and growth factors involved in
angiogenesis, steroidogenesis, and luteolysis.
Endothelin-1 is a mediator of luteolysis
+
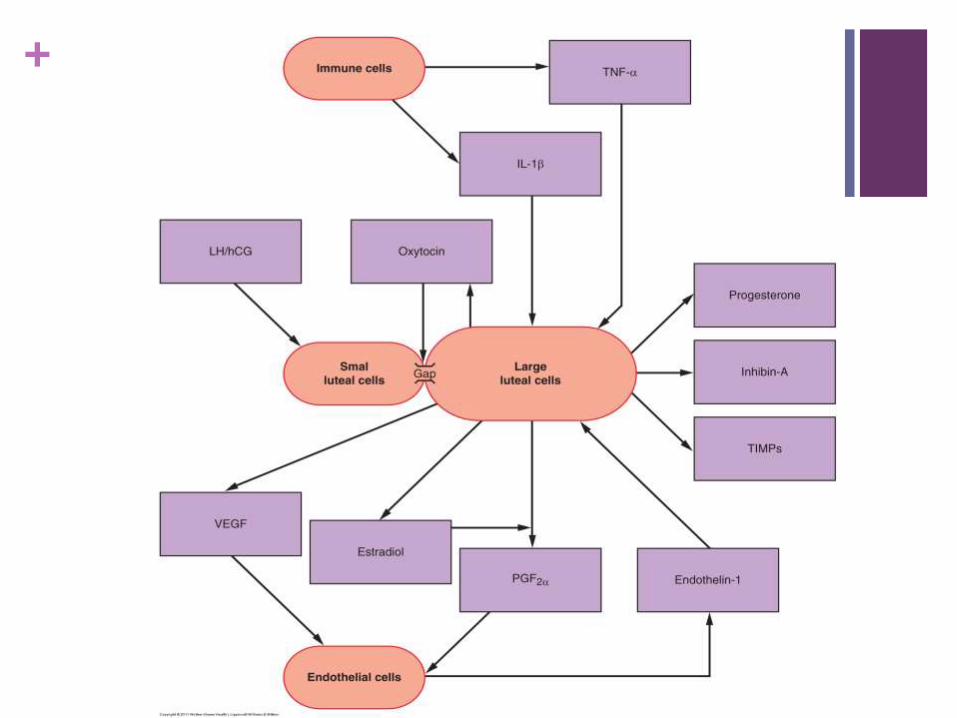
Luteal cell population is composed of two distinct cell types,
large and small cells.
Large cells are derived from granulosa cells and
the small cells from theca cells.
The small cells are the most abundant.
Steroidogenesis takes place in the large cells,
Small cells contain LH and hCG receptors.
LH/hCG receptors are absent on the large cells,

+
The corpus luteum rapidly declines 9 to 11 days after ovulation.
The regression of luteal cells is induced by the estradiol
produced by the corpus luteum.
This action of estrogen is mediated by nitric oxide.
The final signal for luteolysis, however, is prostaglandin F2
alpha, produced within the ovary in response to the locally
synthesized luteal estrogen.

+
Prostaglandin F2Alpha stimulates the synthesis of endothelin
Endothelin-1
inhibits luteal steroidogenesis,
stimulates prostaglandin production in luteal cells.
stimulates the release of TNF Alpha,which induces apoptosis.
+

+
The Luteal-
Follicular
Transition

+
The demise of the corpus luteum results in a nadir in the circulating levels of estradiol, progesterone, and inhibin.
The decrease in inhibin-A removes a suppressing influence on FSH secretion in the pituitary.
The decrease in estradiol and progesterone allows a progressive and rapid increase in the frequency of GnRH pulsatile secretion and a removal of the pituitary from negative feedback suppression.
The removal of inhibin-A and estradiol and increasing GnRH pulses combine to allow greater secretion of FSH compared with LH, with an increase in the frequency of the episodic secretion.
The increase in FSH is instrumental in rescuing approximately a 70-day-old group of ready follicles from atresia, allowing a dominant follicle to begin its emergence.

+

+HORMONES FOLLICULAR
PHASE
OVULATION LUTEAL PHASE
DAILY
PRODUCTION
(ug)
OESTRADIOL
PROGESTERONE
50
2 - 3
150-300 100
20 -30
SERUM VALUES
OESTRADIOL
(pg/ml)
PROGESTERONE
(ng/ml)
FSH (mIU/ml)
LH (mIU/ml)
50
<1
10
5
300- 600
15- 20
60
150-200
>5
10
5
DAILY
EXCRETION
TOTAL
OESTROGEN (ug)
PREGNANEDIOL
(mg)
10-25
<1
35- 100 25-75
3-6

+
From the midluteal peak to menses,
there is a 4.5-fold increase in LH pulse frequency
FSH pulse frequency increases 3.5-fold
The increase in FSH is, as noted, greater than that of LH.

+
UTERINE CYCLE

+
The changes in the endometrium will be discussed in five
phases:
(1) The menstrual endometrium
(2) The proliferative phase
(3) The secretory phase
(4) Preparation for implantation, and finally
(5) The phase of endometrial breakdown.
+

+The Proliferative Phase
The glands :
narrow and tubular, lined by low columnar epithelium cells.
Mitoses
Pseudostratification
A continuous epithelial lining facing the endometrial cavity is
formed.

+ THE
PROLIFERATIVE
PHASE

+
All of the tissue components demonstrate proliferation, which peaks on days
8-10 of the cycle, corresponding to peak estradiol levels in the circulation and
maximal estrogen receptor concentration in the endometrium
Changes are most intense in the functionalis layer in the upper two-thirds of
the uterus, the usual site of blastocyst implantation.

+
The endometrium grows from approximately 0.5 mm to 3.5 to
5.0 mm in height
Restoration of tissue constituents has been achieved by
estrogen-induced new growth as well as incorporation of ions,
water, and amino acids.
An important feature of this estrogen-dominant phase of
endometrial growth is the increase in ciliated and microvillous
cells

+THE
SECRETOR
Y PHASE

+
The endometrium now demonstrates a combined reaction to estrogen and progesterone activity.
Epithelial proliferation ceases 3 days after ovulation.
Total endometrial height is fixed at roughly its preovulatory extent (5-6 mm) despite continued availability of estrogen. This limitation is due to :
Progesterone interference with estrogen receptor expression
stimulation of 17beta-hydroxysteroid dehydrogenase and sulfotransferase, which convert estradiol to estrone sulfate (which is rapidly excreted from the cell)
+
Tissue components continue to display growth, but confinement in a fixed structure leads to progressive tortuosity of glands and intensified coiling of the spiral vessels.
The first histologic sign that ovulation has occurred is the appearance of subnuclear intracytoplasmic glycogen vacuoles in the glandular epithelium on cycle days 17-18.
These structural alterations are soon followed by
- active secretion of glycoproteins and peptides into the
endometrial cavity
-Transudation of plasma
-immunoglobulins obtained from the circulation
The peak secretory level is reached 7 days after the midcycle gonadotropin surge, coinciding with the time of blastocyst implantation

+
IMPLANTATION
PHASE

+
By 13 days postovulation, the endometrium has differentiated into three
distinct zones.
1/4th of the tissue is the unchanged basalis, straight vessels and spindle-
shaped stroma.
The midportion (approx 50% of the total) is the lace like stratum
spongiosum,loose edematous stroma with tightly coiled spiral vessels and
dilated glandular ribbons.
the superficial layer of the endometrium (about 25% of the height) called the
stratum compactum, which has become large and polyhedral stromal cell,
forming a compact, structurally sturdy layer.

+
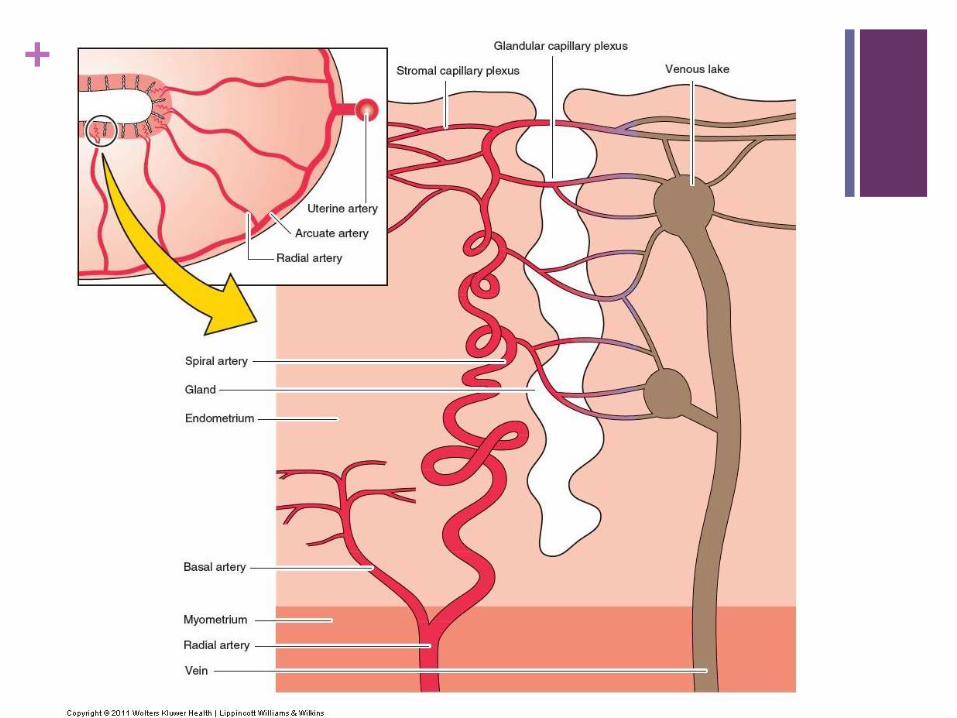
The subepithelial capillaries and spiral vessels are engorged
At the time of implantation, on days 21-22 of the cycle, the predominant
morphologic feature is edema of the endometrial stroma , due to inc in
permeability under the influence of steroids

+
ENDOMETRIAL
BREAKDOWN

+
In the absence of fertilization, implantation, and the consequent
lack of hCG from the trophoblast, the fixed lifespan of the corpus
luteum is completed, and estrogen and progesterone levels
wane.
The most prominent immediate effect of this hormone withdrawal
is a modest shrinking of the tissue height and spiral arteriole
vasomotor responses.

+
The following vascular sequence occurs
With shrinkage of height, blood flow within the spiral vessels
diminishes, venous drainage is decreased, and vasodilation ensues.
Thereafter, the spiral arterioles undergo rhythmic vasoconstriction and
relaxation.
Each successive spasm is more prolonged and profound, leading
eventually to endometrial blanching.
Within the 24 hours immediately preceding menstruation, these
reactions lead to endometrial ischemia and stasis.

+
White cells migrate through capillary walls, extending throughout the
stroma.
During arteriolar vasomotor changes, red blood cells escape into the
interstitial space. Thrombin-platelet plugs also appear in superficial
vessels.
The prostaglandin content (PGF2 alpha and PGE2) in the secretory
endometrium reaches its highest levels at the time of menstruation.
The vasoconstriction and myometrial contractions associated with the
menstrual events are mediated by prostaglandins from perivascular
cells and the potent vasoconstrictor endothelin-1, derived from stromal
decidual cells.

+
In the first half of the secretory phase, acid phosphatase and
potent lytic enzymes are confined to lysosomes, stabilized by
progesterone, which are released with waning of it’s level.
These active enzymes will digest their cellular constraints,
leading to the release of prostaglandins, extravasation of red
blood cells, tissue necrosis, and vascular thrombosis

+

+
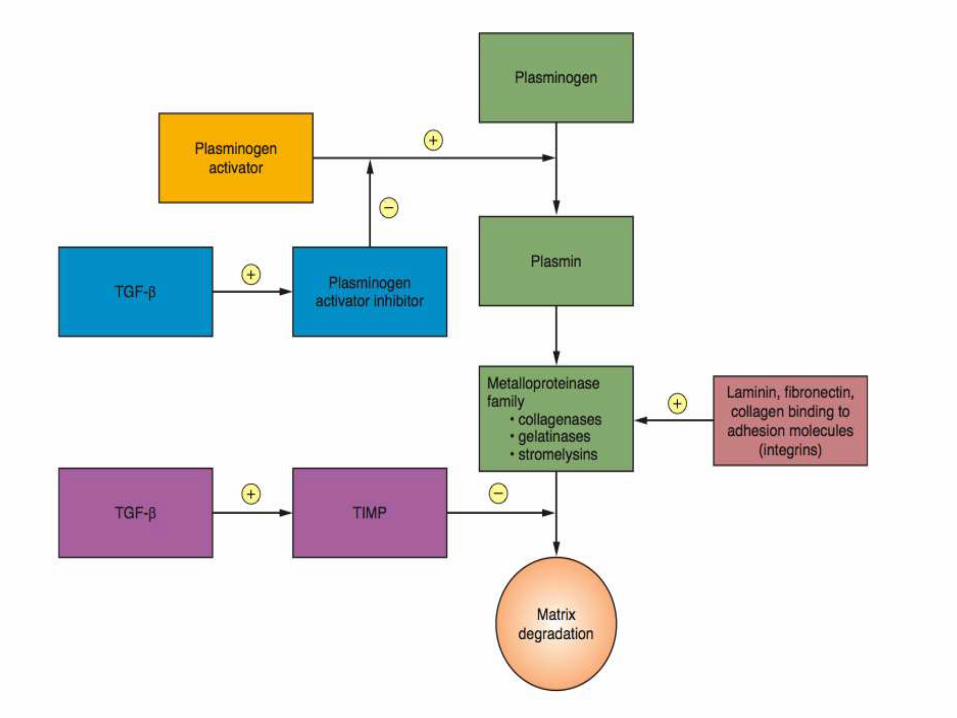
Endometrial tissue breakdown also involves a family of
enzymes, matrix metalloproteinases
The metalloproteinases include
collagenases that degrade interstitial and basement membrane
collagens;
gelatinases that further degrade collagens;
and stromelysins that degrade fibronectin, laminin, and
glycoproteins

+
Progesterone withdrawal from endometrial cells induces matrix
metalloproteinase secretion.
In a nonpregnant cycle, metalloproteinase expression is
suppressed after menses by increasing estrogen levels.
+
+
Progesterone withdrawal is associated with an increase in
VEGF receptor concentrations in the stromal cells.
Although the VEGF system is usually involved with
angiogenesis, in this case these factors are involved in the
preparation for menstrual bleeding, perhaps influencing the
expression of matrix metalloproteinases.

+
Eventually,Leakage occurs as a result of diapedesis, and finally, interstitial hemorrhage occurs due to breaks in superficial arterioles and capillaries.
As ischemia and weakening progress, the continuous binding membrane is fragmented, and intercellular blood is extruded into the endometrial cavity.
New thrombin-platelet plugs form intravascularly upstream at the shedding surface, limiting blood loss.
Increased blood loss is a consequence of reduced platelet numbers and inadequate hemostatic plug formation.
Menstrual bleeding is influenced by activation of clotting and fibrinolysis

+
PAI-1 exerts an important restraining action on fibrinolysis and
proteolytic activity.
Blood loss is also controlled by constriction of the spiral
arteries, mediated by the perivascular cells, myofibroblasts that
surround the spiral arteries.
Myofibroblasts respond to progesterone withdrawal by
expressing prostaglandins and cytokines, causing cycling
vasoconstriction and vasodilation
+
Thrombin generation in the basal endometrium in response to
extravasation of blood is essential for hemostasis.
The basalis endometrium remains during menses, and repair
takes place from this layer.
This endometrium is protected from the lytic enzymes in the
menstrual fluid by a mucinous layer of carbohydrate products
that are discharged from the glandular and stromal cells.

+
A natural cleavage point exists between basalis and
spongiosum, and, once breached, the loose, vascular,
edematous stroma of the spongiosum desquamates and
collapses.
The process is initiated in the fundus and extends throughout
the uterus.
In the end, the typical deflated, shallow, dense, menstrual
endometrium results.

+
Within 13 hours, the endometrial height shrinks from 4 mm to
1.25 mm.
Menstrual flow stops as a result of the combined effects of
Prolonged vasoconstriction of the radial arteries and the spiral
arteries in the basalis,
Tissue collapse,
Vascular stasis,
Estrogen-induced healing
In contrast to postpartum bleeding, myometrial contractions are
not important for control of menstrual bleeding.

+
THANK YOU

















