114
Pituitary Disease Amy Toscano-Zukor, MD Based upon a presentation prepared by Anne Marie Van Hoven, MD UMDNJ – Robert Wood Johnson Medical School
Pituitary Disease
Amy Toscano-Zukor, MD
Based upon a presentation prepared byAnne Marie Van Hoven, MD
UMDNJ – Robert Wood Johnson Medical School
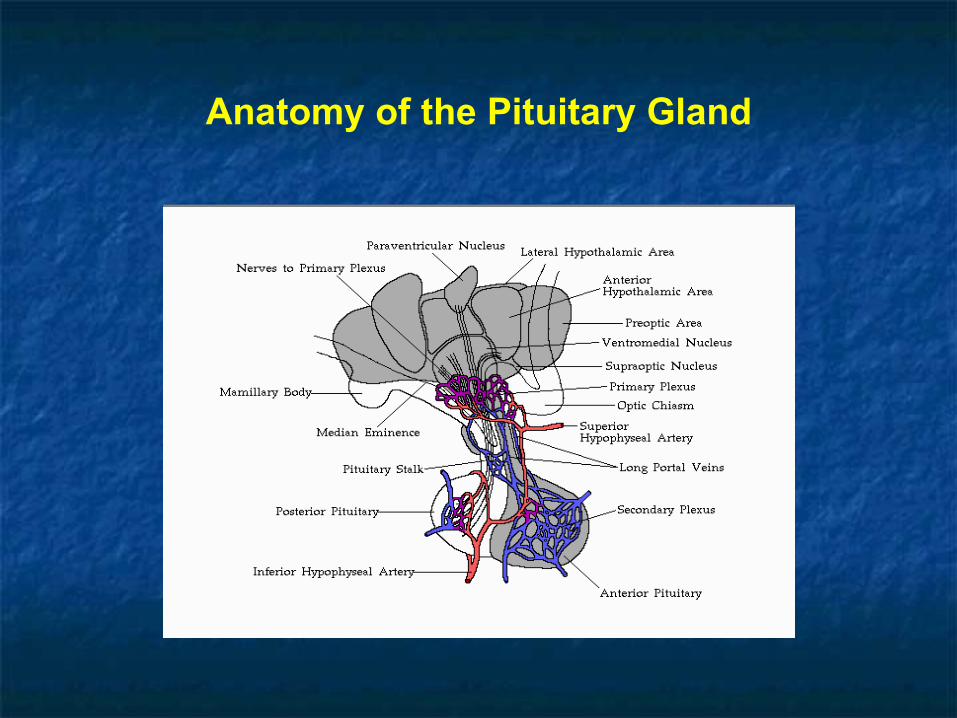
Anatomy of the Pituitary Gland

Pituitary Hormones Anterior Pituitary
Thyroid Stimulating Hormone (TSH) Adrenocorcticotropic Hormone (ACTH) Growth Hormone (GH) Follicle Stimulating Hormone (FSH) Luteinizing Hormone (LH) Prolactin (Prl)
Posterior Pituitary
Arginine Vasopressin (AVP) Oxytocin

Hypothalamic Hormones
Thyrotropin Releasing Hormone (TRH)
Corticotropin Releasing Hormone (CRH)
Growth Hormone-Releasing Hormone (GHRH)
Growth Hormone Release Inhibiting Hormone (Somatostatin)
Gonadotropin Releasing Hormone (GnRH)
Prolactin Release Inhibiting Hormone (Dopamine)

The Hypothalamic- Pituitary Axes

Lesions of Hypothalamic Pituitary Axis
Hypothalamic (hypothalamic or pituitary stalk disease) vs. Primary Pituitary Disease
Acquired Defects: Tumors (inc. Pit. Adenomas), Trauma, Irradiation, Inflammatory/Infiltrative d/s, Vascular d/s (inc. Apoplexy), Empty Sella, Primary Neoplastic d/s, Metastatic d/s, Metabolic d/s and Functional d/s.
Congenital Embryopathic Defects: Kallman’s syndrome, Pituitary Aplasia, Anencephaly, Midline defects.
Genetic Defects: Hypothalamic / Pituitary Hormone Gene Defects and Hormone Receptor Gene Defects.

Clinical Manifestations of Lesions of Hypothalamic Pituitary Axis
Mass effects: Headaches, Visual Field and CN III-VI Defects, Obstructive Hydrocephalus, CSF Rhinorrhea, Hypothalamic Syndromes (DI, SIADH, thirst/ appetite/ satiety/ sleep/ temperature regulation), Frontal/ Temporal Lobe Dysfunction
Endocrine Effects: Hypopituitarism: TSH/ ACTH/ GH/ LH-FSH/ Prolactin Hyperpituitarism: TSH/ ACTH/ GH/ LH-FSH/ Prolactin

Mass Effects of Pituitary Lesions

Organization of visual fibers at the Optic Chiasm
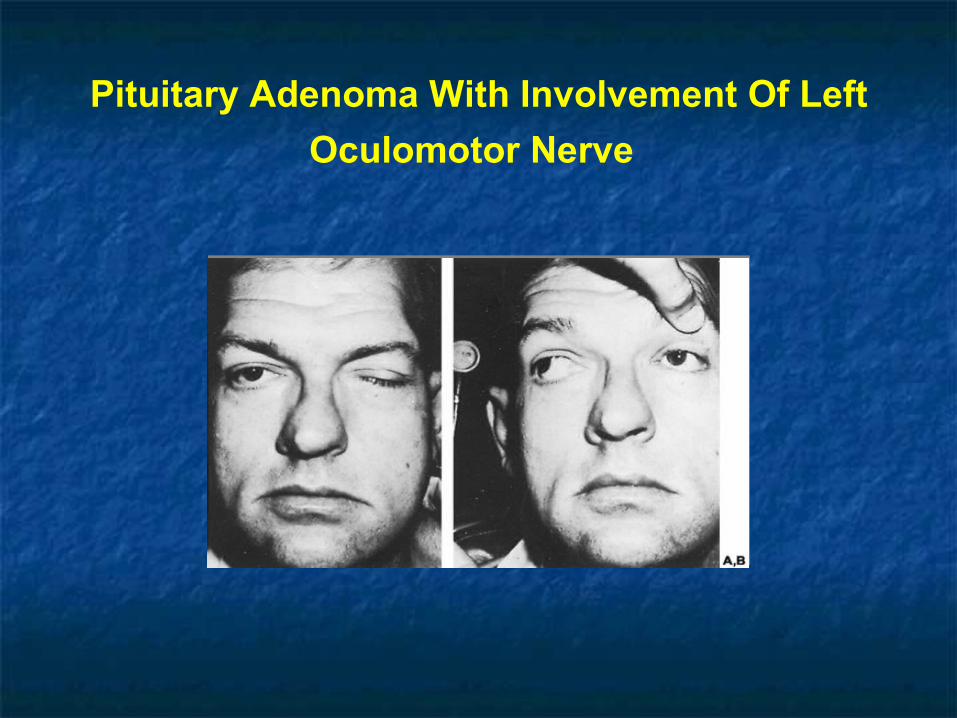
Pituitary Adenoma With Involvement Of Left
Oculomotor Nerve

Pituitary Tumor

Pituitary Apoplexy
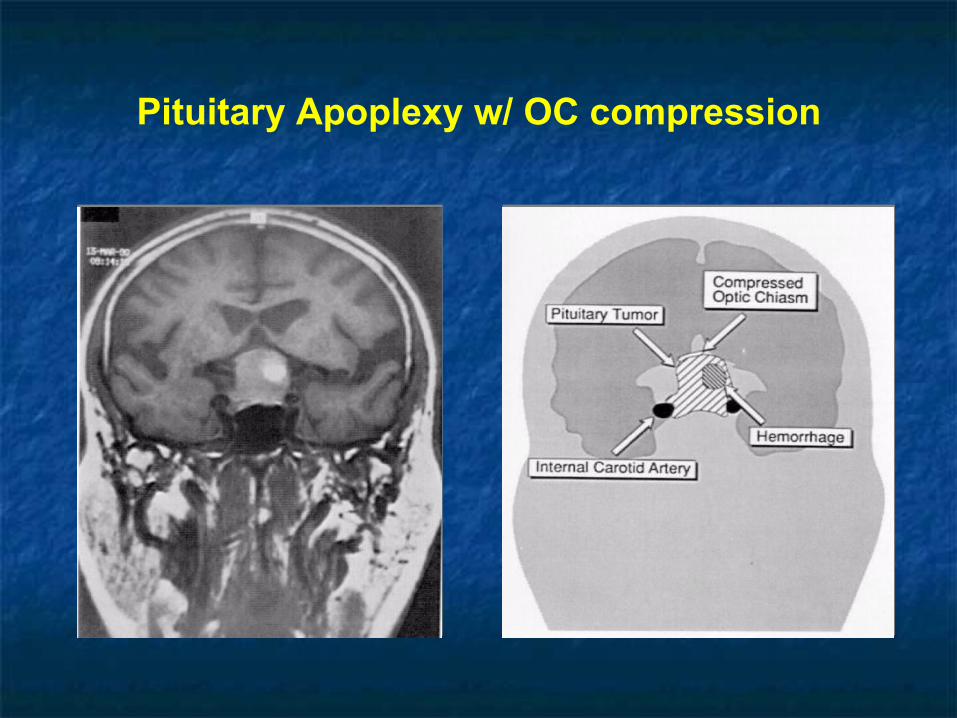
Pituitary Apoplexy w/ OC compression
Clinical Manifestations of Lesions of Hypothalamic Pituitary Axis
Mass effects: Headaches, Visual Field and CN III-VI Defects, Obstructive Hydrocephalus, CSF Rhinorrhea, Hypothalamic Syndromes (DI, SIADH, thirst/ appetite/ satiety/ sleep/ temperature regulation), Frontal/ Temporal Lobe Dysfunction
Endocrine Effects: Hypopituitarism: TSH/ ACTH/ GH/ LH-FSH/ Prolactin Hyperpituitarism: TSH/ ACTH/ GH/ LH-FSH/ Prolactin

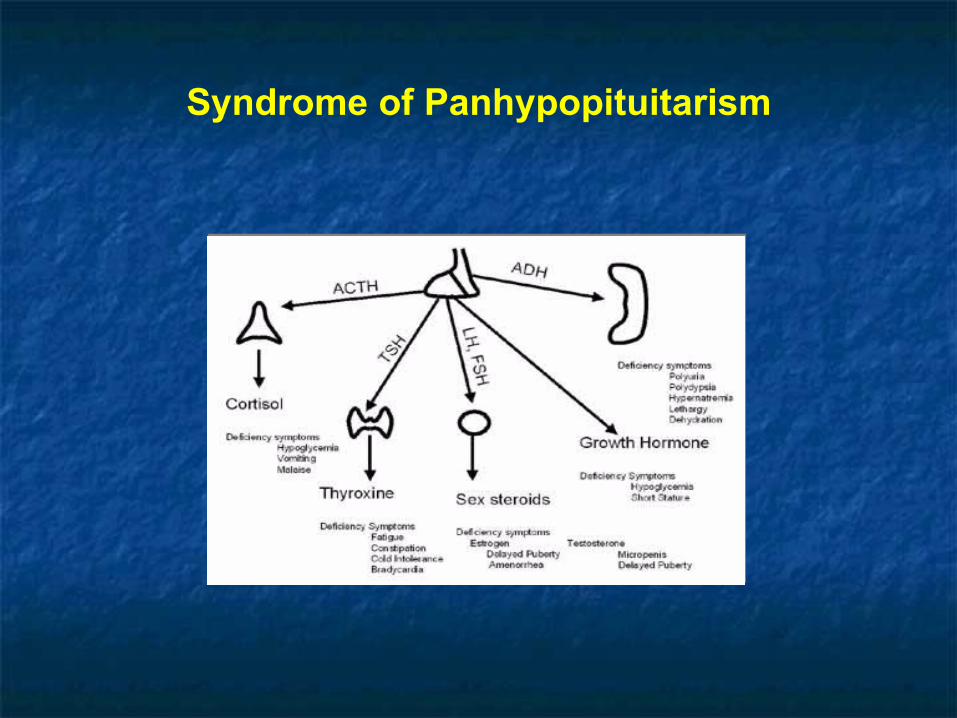
Syndrome of Panhypopituitarism
Progressive loss of Anterior Pituitary function: FSH/LH and GH; TSH; ACTH.
Hypopituitarism with DI is suggestive of Hypothalamic etiology.
Syndrome of Panhypopituitarism
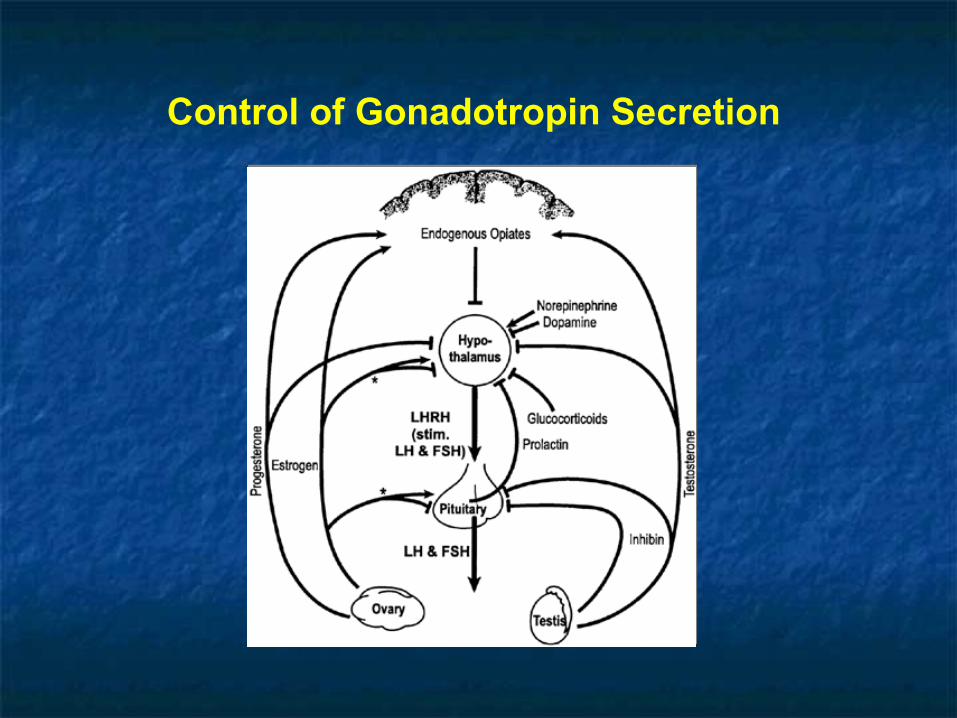
Control of Gonadotropin Secretion

Syndrome of Panhypopituitarism
FSH / LH deficiency:
In women: Oligo-amenorrhea, Infertility, “Post-menopausal” symptomatology, Bone loss.
In Men: Decreased Libido, ED, Gynecomastia with loss of secondary sexual characteristics, Bone loss.
Labs: Gonadotropins inappropriately low for E2 in women and T in men.

Syndrome of Panhypopituitarism
GH deficiency in Adults:
Symptoms: Reduced muscle mass and decreased exercise performance, Increased abdominal adiposity, Decreased psychosocial well being.
Signs: Central adiposity, thin dry skin, Decreased muscle strength.
Labs: Hyperinsulinemia, Dyslipidemia, “Low-normal” IGF-1 with inadequate response on Insulin tolerance test/ L-Dopa test/ L-Arginine test.
Syndrome of Panhypopituitarism
GH deficiency in Children:
GH deficiency (especially prior to onset of puberty) leads to growth retardation/ short stature.
Thyroid and Corticosteroid replacement are necessary for GH action in patients with panhypopituitarism.

Syndrome of Panhypopituitarism
TSH deficiency:
Symptoms: Fatigue, Cold intolerance, Lethargy, Constipation, Diminished appetite, Weight gain, Hoarseness of voice, Menorrhagia.
Signs: Bradycardia, Hypothermia, Pale/ cool/ dry skin, dry hair, “hung up” DTRs, stupor/ coma in severe cases.
Labs: “Low-normal” TSH with low Free T4, Abnormal TRH Stimulation test, Hyponatremia in severe cases.
Syndrome of Panhypopituitarism
ACTH deficiency:
Symptoms: Weakness, Fatigue, Nausea/ Vomiting, Weight loss
Signs: Pale skin with inability to tan, Postural Hypotension.
Labs: Mineralocorticoid function is preserved, Low AM cortisol, +/- ACTH Stimulation test, Poor pituitary ACTH reserve on Insulin tolerance test/ CRH stimulation test/ Metyrapone test.

Maintenance Medications for Hypopituitarism

Empty Sella Syndrome
Defects in diaphragma sella allowing herniation of arachnoid membrane into the hypophyseal fossa thereby leading to transmission of ICP and compressing the pituitary against the walls of the sella.
Primary vs. Acquired (Surgery, Radiation therapy, Infarction)
Pituitary function is usually normal +/- mild elevations of Prolactin.

Empty Sella Syndrome

Clinical Manifestations of Lesions of Hypothalamic Pituitary Axis
Mass effects: Headaches, Visual Field and CN III-VI Defects, Obstructive Hydrocephalus, CSF Rhinorrhea, Hypothalamic Syndromes (DI, SIADH, thirst/ appetite/ satiety/ sleep/ temperature regulation), Frontal/ Temporal Lobe Dysfunction
Endocrine Effects:
Hypopituitarism: TSH/ ACTH/ GH/ LH-FSH/ Prolactin Hyperpituitarism: TSH/ ACTH/ GH/ LH-FSH/ Prolactin

Pituitary Adenoma
Microadenomas are < 10mm.
Macroadenomas are ≥ 10mm.
Majority are monoclonal and not malignant.
May or may not be functional.
Mass effects and hypopituitarism may be present irrespective of functional status.
Functioning (secretes hormones) vs. non-functioning

Prevalence of Pituitary Tumors
TSH tumors<3%
FSH / LH tumors10-15%
ACTH tumors10-15%
GH tumors10-15%
Non-functioning tumors10-25%
Prolactin tumors25-40%
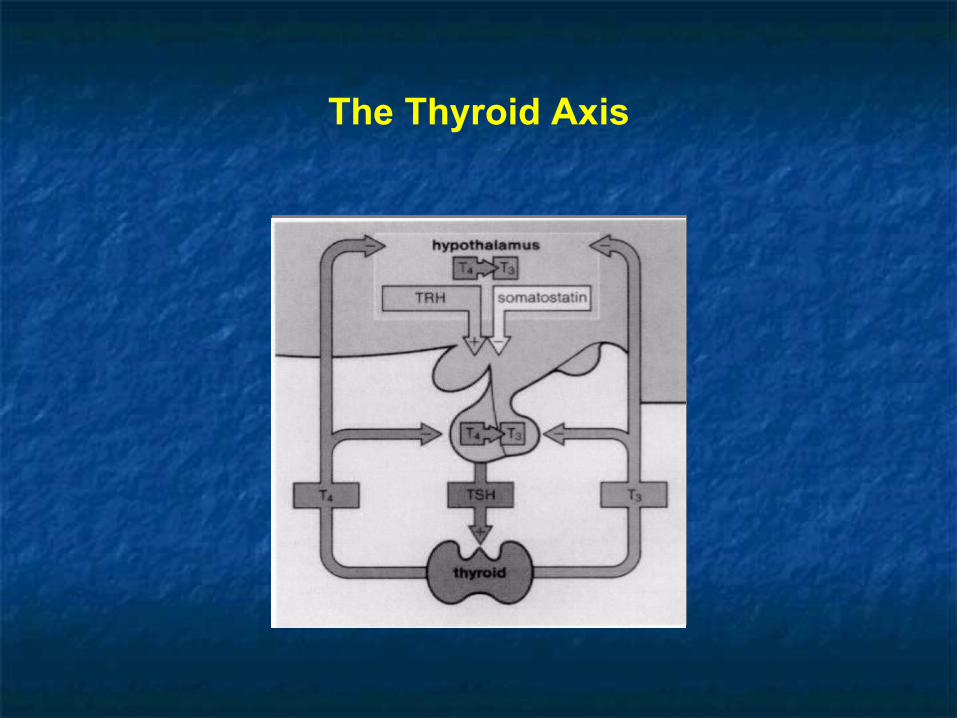
The Thyroid Axis

TSH secreting Pituitary Adenoma TSH molecule may be biologically inactive or may cause
clinical hyperthyroidism resembling Graves’ disease. TSH levels are variable, from normal to as high as 500s. Diagnosis: Inappropriately elevated TSH in presence of
high T3/T4 is highly suggestive. Alpha Subunit levels may be significantly elevated.
Treatment: Pituitary Surgery, Radiation therapy, Octreotide.

FSH/LH secreting Pituitary Adenoma
No characteristic syndrome of hormone excess is seen. Occasionally- In Men: +/- testicular enlargement, hypogonadal
symptoms. In Women: +/- hypogonadal signs and symptoms. Treatment: Pituitary surgery, Radiation therapy.

Neuroendocrine regulation of the HPA axis

ACTH secreting Pituitary Adenoma(Cushing’s Disease)
Accounts for about 60-70% of cases of Cushing’s syndrome.
Symptoms: Fatigue, Weight gain, Easy bruising, Headaches, Irregular menses, Psychiatric symptoms from depression to frank psychosis.
Signs: Plethoric “Moon facies”, ”Buffalo hump”, Central adiposity with thin extremities, Hyperpigmentation, Hypertension, Hirsuitism, Acne, Purple striae, Proximal myopathy.

ACTH secreting Pituitary Adenoma(Cushing’s Disease)
Labs: IFG/IGT, Hypokalemia and Alkalosis, Leukocytosis, Lymphopenia, Bone loss on DXA.
Diagnosis : Elevated 24 hour urinary free cortisol and/or lack of suppression by low dose dexamethasone, Elevated ACTH levels, Ectopic ACTH syndrome ruled out.
Treatment: Pituitary surgery, Medical therapy as temporizing measure, Radiation therapy

GH secreting Pituitary Adenoma(Acromegaly)
“Acral” and “facial” growth in Adults (once the epiphyses of long bones are fused).
40% may co-secrete Prolactin.
Symptoms: Headaches, Arthralgias, Fatigue, Hyperhidrosis, entrapment neuropathies, Sleep Apnea, Deepening of voice, Impotence in men, irregular menses in women.

GH secreting Pituitary Adenoma(Acromegaly and Gigantism)
Signs: “Coarsening” of facial features, enlarged hands and feet secondary to soft tissue hypertrophy, oral malocclusion and increased spacing between teeth, Moist “doughy” skin, increased heel pad thickness, Hypertension, Goiter.
Labs: IFG/IGT, +/- elevated Prolactin, Hypogonadism.
Diagnosis: Elevated IGF-1, Abnormal GTT. In children, gigantism occurs because of accelerated
linear growth (growth plates haven’t fused yet)
Diseases associated with Acromegaly
DM Arthritis and carpal tunnel syndrome
secondary to hypertrophy of joint cartilage Hypogonadism Sleep Apnea HTN, LVH Colon Polyps




Management of Acromegaly

Causes of Hyperprolactinemia

Prolactin secreting Pituitary Adenoma
Most common Pituitary lesion. Majority are microprolactinomas, few are
macroprolactinomas. E2 stimulates lactotroph proliferation. Note: Physiologic elevation of Prolactin is seen
in pregnancy. Idiopathic Prolactinoma: When the etiology is
unclear. A subset of these patients may have macroprolactinemia.
Prolactin secreting Pituitary Adenoma
Prolactin >200ng/ml is consistent with Prolactinoma
Prolactin <50ng/ml is often secondary to physiologic causes.
Prolactin 20-100ng/ml may be secondary to pituitary stalk compression by tumors not actively secreting Prolactin.

Prolactin secreting Pituitary Adenoma
Clinical Presentation: Signs and Symptoms of hypogonadism (especially amenorrhea and infertility in pre-menopausal women) +/- galactorrhea (especially in women) and gynecomastia (in men) +/- tumor mass effects.
Diagnosis: Elevated Prolactin levels in the presence of Pituitary lesion on imaging and other causes of Hyperprolactinemia ruled out.
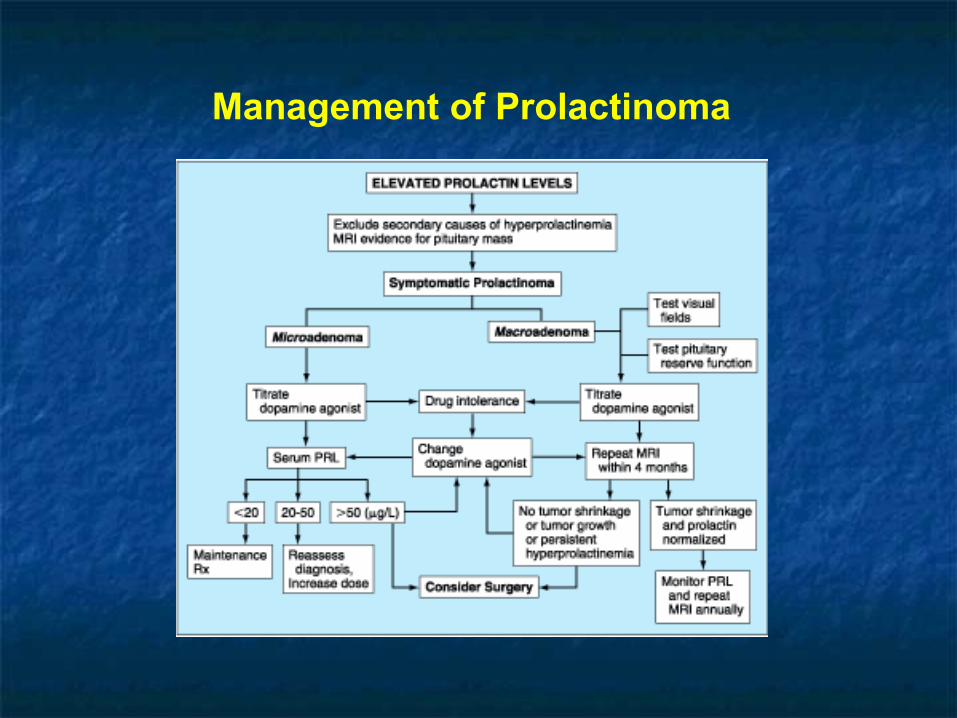
Management of Prolactinoma

Transsphenoidal Surgical Approach

Morbidity and Mortality in Transsphenoidal
Surgery

Posterior Pituitary and AVP Secretion

Variables influencing Plasma AVP
Osmotic: Plasma Osmolality (Water balance)
Hemodynamic: Volume and Pressure sensing
Others: Emesis, Hypoglycemia
Diabetes Insipidus
Excretion of a “large” volume (usually >4 L/d) of hypotonic urine in absence of glycosuria.
Differential Diagnosis: Hypothalamic/ Central DI Nephrogenic DI Primary Polydipsia
Serum Sodium is usually maintained in the normal range. Diagnosis is suggested by inappropriately low Urine Osmolality in relation to the Serum Osmolality.

Causes of Diabetes Insipidus
Diabetes Insipidus
Clinical Features:
Central DI: Relatively abrupt onset of symptoms, Preference for cold liquids, Polyuria and Thirst persisting through the night.
Nephrogenic DI: Lithium, Demeclocycline use, Hypokalemia, Hypercalcemia.
“Psychogenic” Polydipsia: Erratic course, Symptoms exacerbated during stress, Minimal disruption of sleep (lack of nocturia), Underlying psychiatric disease.
Treatment of DI
Adequate water replacement is essential to avoid metabolic complications.
Central DI: DDAVP (Selective action on antidiuretic V2 receptors, minimal on pressor V1 receptors)
Nephrogenic DI: Thiazide leading to greater proximal tubular reabsorption of glomerular filtrate.

SIADH
Hyponatremia with low plasma osm Urine less than maximally dilute Increased urine sodium Euvolemia Normal thyroid and adrenal fxn No drugs that increase ADH
Thyroid Disease
Sheri Gillis Funderburk, MD
Thyroid
Physiology Hypothyroidism Thyroiditis Hyperthyroidism Thyroid Nodules Thyroid Cancer

Thyroid Physiology
Under regulation of the hypothalamus (TRH) and pituitary (TSH)
Thyroid gland synthesizes and releases thyroid hormone
Thyroid consists of thyroid follicles containing colloid material that contains thyroglobulin
Thyroglobulin is a glycoprotein involved in thyroid hormone synthesis

Thyroid Hormone
T4 and to lesser extent T3 is released from thyroid gland Majority T3 is produced peripherally by deiodination of
T4 Majority T4 and T3 is bound to thyroid binding globulin
(TBG) and albumin T4 is bound more tightly than T3 to TBG
Only the free hormone is active
T3 has higher affinity for thyroid receptor T3 is the more active thyroid hormone


Thyroid Hormone
Thyroid
T3 uptake
Indirect measurement of free T4 Constant x T3 resin Uptake x Total T4
Inverse relationship with TBG (in situations whn TBG is high (pregnancy, OCP use), then T3U will be low.
T3U is inversely proportional to the percentage of total T4 that is protein-bound

Thyroid
TBG Increased
Congenital Estrogen
Contraceptive, replacement, pregnancy
Hypothyroidism*
Decreased Congenital Androgens Liver failure Nephrotic syndrome Malnutrition Hyperthyroidism* Sick patients glucocorticoids

Lab values in different scenarios
↑ ↓↓↓Protein binding
↓↓↓Hypothyroidism
↓↑↑↑ Protein binding
↑↑↑Hyperthryoidism
T3RUTotal T3Total T4

Hypothyroidism
Primary Secondary
Pituitary disease follow free T4, TSH unreliable
Tertiary Hypothalamic disease
Sarcoidosis, tumor, radiation Resistance to thyroid hormone
Rare Abnormal binding of thyroid hormone to receptor High TSH and T3/T4 +/- signs hypothyroidism

Hypothyroidism
Symptoms Nonspecific Modest weight gain Cold intolerance Constipation Dry skin Fatigue Constipation Menstrual irregularities Muscle aches
Signs Dry skin/hair Nonpitting edema Thick lips or tongue Slow relaxation phase
of DTR (“hung up reflex”)
Thinning lateral aspect of eyebrows


Primary Hypothyroidism
Hashimoto’s Most common cause hypothyroidism Women>men Incidence increases with age Autoimmune destruction of thyroid gland Associated with positive anti-TPO and/or anti-
thyroglobulin antibody Slowly progressive May coexist with other autoimmune diseases
Hashimoto’s
Labs High TSH, low Total T4, total T3, T3 resin Uptake,
and free T4; positive thyroid peroxidase and/or anti thyroglobulin antibodies
We don’t usually measure free T3 Treatment
Thyroxine replacement T4 vs T3
Subclinical hypothyroidism Modestly elevated TSH with normal T4/T3
Indications for treatment Hypercholesterolemia Symptoms consistent with hypothyroidism

Post Partum Hypothyroidism
Recovery phase
Self limiting
Can reoccur with future pregnancies
Positive Thyroid Peroxidase antibodies associated with increase risk of later developing permanent hypothyroidism

Primary Hypothyroidism (other)
Iatrogenic/Drugs Thyroidectomy Radioablation Anti-thyroid medications Lithium, Amiodarone, Interferon
Frequently underlying autoimmune process Iodine deficiency
Rare in well-developed countries Dyshormonogenesis
Rare Enzymatic defect in biosynthesis
Leads to hypothyroidism and goiter

Myxedema Coma
End stage severe longstanding hypothyroidism
Endocrinology emergency Elderly Hypothermia, bradycardia, hypotension Predisposing condition
Cold, infection, trauma, CNS depressants

Myxedema Coma
Treatment Supportive care
correction hypothermia, treat underlying illness, IV fluids with glucose
IV thyroid replacement
Corticosteroids


Hypothyroidism
Miscellaneous Dosing T4
Elderly vs young Start at 25ug and titrate up 1.5ug/kg body weight
Treat TSH within normal range Exception secondary/tertiary hypothyroidism-free T4 upper
end of normal
Consider R/O adrenal insufficiency Primary vs secondary hypothyroidism

Hypothyroidism in Pregnancy
Thyroid Binding Globulin (TBG) increases with pregnancy
Pregnant women with underlying thyroid disease often unable to increase thyroid hormone production
Patient given instruction as soon as pregnancy confirmed increase dose by 30%
Some evidence hypothyroidism in 1st trimester associated with mental disability in offspring
Goal TSH in pregnancy is less than in non-pregnant patients (< 2)

Differential for thyroiditis: low uptake on scan
Infectious Acute (suppurative)-
fungal, parasite, bacterial, PCP, rare
Subacute: usually viral in origin (granulomatous: de Quervain’s)--tender gland
Painless (non post-partum)
Amiodarone-Induced
Radiation Induced Traumatic
Autoimmune: painless Chronic Lymphocytic
(Hashimotos) Postpartum
Subacute Thyroiditis
Often history viral illness Neck tenderness During recovery phase transient period hypothyroidism
lasting weeks to several months Usually transient Positive antibodies associated with increased risk of
developing primary hypothyroidism

Stages of subacute and postpartum thyroiditis
Hyperthyroid phase occurs first, usually in first 3 months after the viral illness or pregnancy and thyroid pain
Followed by several weeks of a transitory phase when euthyroidism occurs
Followed by a hypothyroid phase for several months
Followed by a Recovery phase when the patient returns to euthyroidism


Subacute Thyroiditis
Labs TSH, Total T4 and T3 resin Uptake or free T4,
total T3, and thyroid antibodies ESR: high Serum thyroglobulin: high in all forms
thyroiditis Imaging
Uptake and Scan: low uptake
Subacute Thyroiditis
Treatment Depending on stage
Beta blockers Anti inflammatory High dose PTU (decrease peripheral conversion
T4 T3) Steroids Thyroid hormone

Hyperthyroidism
Thyrotoxicosis Excess thyroid hormone from any cause
Low TSH +/- elevated T4/T3
Radioactive Iodine uptake and scan helps to differentiate various forms

Hyperthyroidism
Grave’s Disease Subacute Thyroiditis Post-Partum Thyroiditis Lymphocytic thyroiditis Acute Thyroiditis Toxic Adenoma Toxic Multinodular Goiter Iodine induced
IV contrast, iodine containing supplements
Factitious Excess Beta HCG from
molar pregnancy or choriocarcinoma
Struma ovarii TSH producing pituitary
adenoma Medications
Amiodarone, lithium, interferon
Hyperthyroidism
Symptoms Palpitations Anxiety Weight loss/gain Polyphagia Heat intolerance Increased frequency BM Tremulous Difficulty concentrating Menstrual irregularities
Signs Goiter Thyroid bruit* Resting tremor Lid lag Proptosis* Tachycardia/atrial fibrillation Widened pulse pressure Proximal myopathy Neck tenderness Dermopathy* Warm/moist skin

RAIU: most useful test in the differentiatal dx of thyrotoxicosis
High uptake Graves: diffuse pattern Toxic Multinodular
Goiter: irregular patern Solitary Toxic
Adenoma: increased in one area of thyroid
Low Uptake Factitious: low
thyroglobulin levels Iodine-Induced Thyroiditis: have high
thyroglobulin levels; may have high ESR or antibodies, depending on cause

Grave’s Disease
Most common cause hyperthyroidism (60-70%) Autoimmune activation TSH receptor
Thyroid Stimulating Immunoglobulin Familial Women > Men Associated with other autoimmune diseases
Vitiligo, Pernicious Anemia, Myasthenia Gravis, Addison’s disease, TIDM
Anti-TPO and Anti-Thyroglobulin antibodies may also be present
May have positive Thyroid stimulating immunoglobulins and/or positive Thyroid receptor antibodies

Grave’s Disease
Triad Thyroid bruit, dermopathy, proptosis are all
pathognomonic Labs
Suppressed TSH, elevated T4 and/or T3, increased T3 uptake
Imaging Uptake and scan
Increased, diffuse uptake




Grave’s Disease: Treatment
Anti-thyroid medications PTU
Inhibits synthesis thyroid hormone Decreases peripheral conversion T4 T3 Does not block release preformed thyroid hormone Side effects
Agranulocytosis, hepatitis, urticaria 18-24 months treatment to decrease chance of relapse Preferred pretreatment in surgery
Grave’s Disease: Treatment
Anti-thyroid medication Methimazole
Inhibits synthesis only Preferred treatment prior to RAI Same side effects as PTU
Cross reactivity
Beta Blocker Symptomatic relief Decrease peripheral conversion T4T3

Grave’s Disease
Treatment Radioactive iodine
Exacerbation of hyperthyroidism and eye disease Pretreatment drug of choice is methimazole (hold 5-7 days prior to
RAI) Hypothyroidism wanted/potential side effect
Iodine: used in severe thyrotoxicosis or storm Blocks release thyroid hormone Wolf Chaikoff Effect (Escape)
Surgery Rarely used Pretreatment indicated with PTU/Iodine Major complications are hypothyroidism, hypoparathyroidism,
damage to recurrent laryngeal nerve


Toxic Multinodular Goiter
Accounts for 20-30% cases hyperthyroidism Nodular goiter on exam Milder increase in T4/T3 RAI uptake and Scan
Normal to high patchy uptake RAI treatment of choice Large doses of iodine may precipitate
thyrotoxicosis in Non-Toxic MNG
Toxic Adenoma
AKA Plummer’s Disease 3-5% toxic adenoma Caused by solitary hyperfunctioning nodule Nodule may be palpable on exam Low TSH with elevated T4 and/or T3 RAI uptake and scan
Normal to high uptake Solitary hot nodule Remainder glands suppressed
RAI treatment of choice

Hyperthyroidism due to Iodine
Iodine Induced Jod Basedow Underlying thyroid pathology Self limiting History IV contrast obtained within several weeks of
onset or pt is on Amiodarone Low TSH, elevated T4, typically normal T3 Low RAI uptake Pretreatment Symptomatic relief

Hyperthyroidism due to Meds
Medications Lithium Amiodarone
Type I vs Type II Increased thyroid hormone production vs destructive
thyroiditis Often difficult to differentiate Treatment (depending on Type I vs II)
Discontinue amiodarone Anti-thyroid medications (Type 1), steroids (type II), beta-
blocker, surgery

Hyperthyroidism: other causes
Factitious Low TSH Low RAI uptake Decreased thyroglobulin
Elevated in thyroiditis Molar Pregnancy and Choriocarcinoma
Stimulatory effect of hCG, which structurally resembles TSH Struma Ovarii
Ectopic thyroid tissue RAI uptake and scan
Uptake in pelvis and no uptake in neck TSH producing pituitary adenomas
Extremely rare Suspect with elevated T4/T3 and normal/high TSH

Apathetic Hyperthyroidism
Seen in the elderly Thyrotoxicosis without the adrenergic
manifestations Appear depressed, often diagnosed with
mxyedema Weight loss, atrial fibrillation, CHF, muscle
weakness Often Toxic MNG underlying disorder


Hyperthyroidism Emergency
Thyroid Storm Decompensated form of severe thyrotoxicosis Uncommon, life threatening condition Precipitating event
ex. Infection, trauma, surgery, DKA
Fever, tachycardia, neurological abnormalities, hypertension followed by cardiovascular collapse
Treatment Anti-thyroid medications, iodine, steroids, B-blockers, control
hyperthermia


Sick Euthyroid Syndrome
Seen in critically ill patients
Low TSH, free T4, and T3
Elevated Reverse T3*
No treatment


Thyroid Nodule
Extremely common Approximately 50% patients over 65 will
have at least 1 thyroid nodule on US Incidentaloma

Thyroid Nodules
Benign Non toxic Goiter
Not associated with inflammation or neoplastic process Causes
Majority unknown Iodine deficiency Iodine excess Dyshormonogenesis Radiation
Cyst Adenoma Thyroiditis
Thyroid Nodule
Carcinoma Papillary Follicular Anaplastic Medullary Lymphoma Metastatic


Thyroid Cancer
Treatment Surgery Radioactive iodine to ablate any remnant thyroid
tissue Thyroid replacement after surgery and RAI
Suppression of TSH without overt hyperthyroidism
Follow Up Physical Exam TFTs including Thyroglobulin Thyrogen whole body scan Ultrasound

















