45
Pivot Shift Posterior lateral instability
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | paula-nash |
| View: | 221 times |
| Download: | 2 times |

Pivot Shift
Posterior lateral instability

The anterior cruciate ligament (ACL) is one of the most commonly injured ligaments of the knee.
• The incidence of ACL injuries is currently estimated at approximately 200,000 annually, with 100,000 ACL reconstructions performed each year.
• In general, the incidence of ACL injury is higher in people who participate in high-risk sports, such as basketball, football, skiing, and soccer.

• Approximately 50 percent of ACL injuries occur in combination with damage to the meniscus, articular cartilage, or other ligaments.
• Additionally, patients may have bruises of the bone beneath the cartilage surface. These may be seen on a magnetic resonance imaging (MRI) scan and may indicate injury to the overlying articular cartilage.

Cause
• It is estimated that 70 percent of ACL injuries occur through non-contact mechanisms while 30 percent result from direct contact with another player or object.
• The mechanism of injury is often associated with
deceleration coupled with cutting, pivoting or sidestepping maneuvers, awkward landings or "out of control" play.

• Several studies have shown that female athletes have a higher incidence of ACL injury than male athletes in certain sports.
• It has been proposed that this is due to differences in physical conditioning, muscular strength, and neuromuscular control.
• Other hypothesized causes of this gender-related difference in ACL injury rates include pelvis and lower extremity (leg) alignment, increased ligamentous laxity, and the effects of estrogen on ligament properties.

The methods of surgical repair may be categorized into 3 groups, primary repair, extra-articular repair, and intra-articular
repair.
• Primary repair is not recommended except for bony avulsions, which are mostly seen in adolescents.
• Because the ACL is intra-articular, the ligamentous ends are subjected to synovial fluid, which does not support ligamentous healing.
• Extra-articular repair generally involves a tenodesis of the iliotibial tract.
• This may prevent a pivot shift but has not been shown to decrease anterior tibial translation.
• Intra-articular reconstruction of the ACL has become the criterion standard for treating ACL tears.

• Bone-patella-bone (BTB) autografts are currently popular because they yield a significantly higher percentage of stable knees with a higher rate of return to preinjury sports.
• The major pitfall of these grafts is their association with postoperative anterior knee pain (10-40%).
• Hamstring tendon (HT) grafts are associated with a faster recovery and less anterior knee pain. Critics believe that these are more susceptible to graft elongation

• Allografts have also been very popular because of their efficiency, their ability to provide bony fixation, and the lack of associated patella morbidity.
• However, they are associated with a risk of viral transmission.
• Allografts are best used in revisions. These have also fallen out of favor by some because several deaths linked to clostridial infections

• Synthetic grafts and ligament augmentation devices have also been used.
• Synthetic grafts are no longer acceptable, because of their high rate of complications, including failure and aseptic effusions.

• Intra-articular reconstruction may be performed through a 2-incision technique or a single-incision endoscopic technique; the latter is currently more popular.
• This procedure requires graft stabilization with some type of fixation hardware for all of the graft options.
• • The stabilization may be performed with metal
interference screws, bioabsorbable screws, endobuttons, and cross pins. Each device has its own benefits.
• Double-tunnel ACL reconstructions attempt to reproduce stability in internal rotation and valgus torque applied to the knee.
• Investigations into the benefits of such surgical treatment versus the increased level of difficulty and operative time are currently ongoing.
• Studies at this time have been limited to animal models.
• The results of a 2-year randomized trial noted that the double-bundle technique resulted in fewer graft failures and significantly lower revision rates than the single-bundle technique in anterior cruciate ligament reconstruction.

• ◦After a 3-year follow up, the data from one study showed that patients with combined lesions of the ACL and MCL who had undergone an arthroscopic double-bundle ACL reconstruction showed a significantly greater mean medial joint opening (1.7 mm) compared with uninjured knees (0.9 mm). However, no significant difference was noted between the anteroposterior laxity and other clinical parameters. Because the data showed that residual valgus laxity did not affect anteroposterior laxity significantly, these results suggest that no additional surgical procedure is necessary for the medial collateral ligament in combined lesions.[17]
• Nonsurgical Treatment
• In nonsurgical treatment, progressive physical therapy and rehabilitation can restore the knee to a condition close to its pre-injury state and educate the patient on how to prevent instability.37,38 This may be supplemented with the use of a hinged knee brace. However, many people who choose not to have surgery may experience secondary injury to the knee due to repetitive instability episodes.
• Surgical treatment is usually advised in dealing with combined injuries (ACL tears in combination with other injuries in the knee). However, deciding against surgery is reasonable for select patients. Nonsurgical management of isolated ACL tears is likely to be successful or may be indicated in patients:
• •With partial tears and no instability symptoms39 • •With complete tears and no symptoms of knee instability during low-demand sports who
are willing to give up high-demand sports• •Who do light manual work or live sedentary lifestyles• •Whose growth plates are still open (children)

• The natural history of an ACL injury without surgical intervention varies from patient to patient and depends on the patient's activity level, degree of injury and instability symptoms.
• The prognosis for a partially torn ACL is often favorable, with the recovery and rehabilitation period usually at least three months. However, some patients with partial ACL tears may still have instability symptoms. Close clinical follow-up and a complete course of physical therapy helps identify those patients with unstable knees due to partial ACL tears.
• Arthroscopic picture of damaged articular cartilage in chronically ACL-deficient knee.

• Complete ACL ruptures have a much less favorable outcome.
• After a complete ACL tear, some patients are unable to participate in cutting or pivoting-type sports, while others have instability during even normal activities, such as walking.
• There are some rare individuals who can participate in sports without any symptoms of instability.
• This variability is related to the severity of the original knee injury, as well as the physical demands of the patient.
• About half of ACL injuries occur in combination with damage to the meniscus, articular cartilage or other ligaments. Secondary damage may occur in patients
•

Physiatric Prescription
• phase 1 protocol for physical therapy following a hamstring autograph ACL reconstruction.
• Goals are to maintain full knee extension, control inflammation, and to minimize effects of immobilization.

• Goals• •Retain Range of Motion• •Reduce Swelling• •Retain Muscle Size and Strength• •Cardiovascular Fitness

Modalities
• . • 1) E-Stim (NMES) to improve quadriceps contraction and increase strength
of quadriceps.• - “The effect sizes for quadriceps strength measures (isometric or
isokinetic torque) from 7 studies ranged from –0.74 to 3.81 at approximately 6 weeks postoperatively; 6 of 11 comparisons were statistically significant, with strength benefits favoring NMES treatment.” 2
• - “NMES combined with exercise may be more effective in improving quadriceps strength than exercise alone.” 2
• - “The use of high-intensity electrical stimulation after ACL reconstruction has been shown to improve quadriceps strength, gait, and patient-reported outcomes.”
•
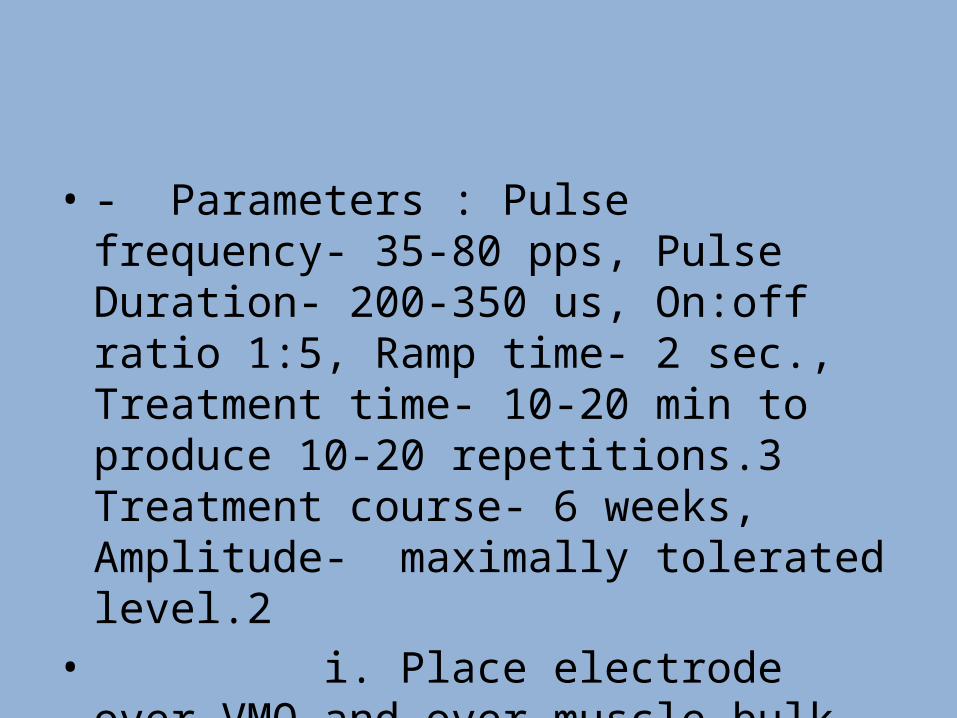
• - Parameters : Pulse frequency- 35-80 pps, Pulse Duration- 200-350 us, On:off ratio 1:5, Ramp time- 2 sec., Treatment time- 10-20 min to produce 10-20 repetitions.3 Treatment course- 6 weeks, Amplitude- maximally tolerated level.2
• i. Place electrode over VMO and over muscle bulk of quadriceps.

2) Cryotherapy • to decrease pain and edema around the knee joint. This will allow for
greater ROM and weight-bearing. • - “• Cold therapy has the ability to reduce local inflammation by producing
local vasoconstriction and reduces nerve conductions.
• These modifications would lead to a reduced level of peripheral and central sensitization in the post-ACL patient.”4
• • - “Control of pain and swelling can be achieved by following the ICE (ice,
compression, and elevation) principle.• • A combination of these techniques results in better outcomes. Cryotherapy
has been found to cause significant decrease in postoperative pain.” 5
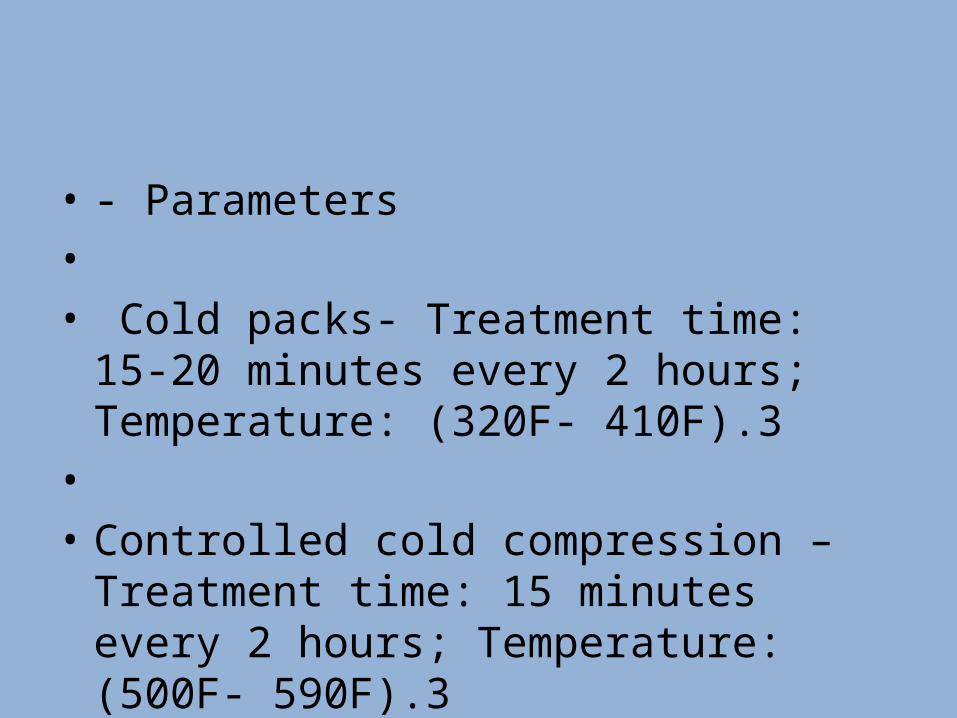
• - Parameters • • Cold packs- Treatment time: 15-20 minutes
every 2 hours; Temperature: (320F- 410F).3• • Controlled cold compression – Treatment
time: 15 minutes every 2 hours; Temperature: (500F- 590F).3

Motion
• Passive• Passive assist• ROM re-education• Active assist• Active• Stretch• ROM limits?

1) Patella mobilization
• to increase ROM in knee extension and flexion. Improving knee ROM will allow patient to return to normal gait and reduce patellofemoral pain.
• -“ Patellar mobilization is used to maintain or increase patellar mobility.
• Inferior mobilization for the patella should be used if the patient has loss of passive flexion and decreased inferior patellar translation during mobility testing.
• Superior glide of the patella is important to ensure full active knee
Maximum anterior translation of the tibia occurs at 15-25 deg of flexion
Limit knee extension

Strengthening
• Isometrics• Multiple angle isometrics• Short arc isotonics• Full arc isotonics• Isokinetrics• Speed• ROM


Open versus closed kinetic chain exercise: issues in rehabilitation after anterior cruciate ligament reconstructive
surgery.
What has been called "closed kinetic chain" (CKC) exercise has become popular in the last 5 to 10 years for use after anterior cruciate ligament (ACL) reconstructive surgery.
• Closed kinetic chain exercises appear to have gained popularity over more traditionally used open kinetic chain (OKC) exercises because many clinicians believe that CKC exercises are safer and more functional.
• When improvement in quadriceps femoris muscle function is an essential treatment goal, therapists may need to combine OKC exercises with CKC exercises to provide optimal training stimuli.

• We conducted a prospective, randomized study of open and closed kinetic chain exercises during accelerated rehabilitation after anterior cruciate ligament recon struction to determine if closed kinetic chain exercises are safe and if they offer any advantages over conven tional rehabilitation.
• The closed kinetic chain group used a length of elastic tubing, the Sport Cord, to per form weightbearing exercises and the open kinetic chain group used conventional physical therapy equip ment.
• Results are reported with a minimum 1-year fol lowup (mean, 19 months).
•

• The closed kinetic chain group had lower mean KT-1 000 arthrometer side- to-side differences, less patellofemoral pain, was gen erally more satisfied with the end result, and more often thought they returned to normal daily activities and sports sooner than expected.
• concluded that closed kinetic chain exercises are safe and effective and offer some important advantages over open kinetic chain ex ercises.
• As a result of this study, they now use the closed kinetic chain protocol exclusively after anterior cruciate ligament reconstruction

• exercisers are told that there should be a certain ratio between the strength of their hamstring and quadriceps muscles.
• Called the H/Q ratio and reported to be anywhere from .50 to .75 with a normative value of .60, the strength ratio of this important agonist/antagonist pairing is considered essential to the stability of the knee joint and to prevent ACL and other injuries.
• The balance of quadriceps to hamstring strength is not 1:1; but closer to 3:2. In general healthy hamstrings can lift 60 - 80% of what healthy quads can do.

• Isokinetic exercises are performed at a dynamic preset fixed speed (ranging from 1 degree per second to approximately 1000 degrees per second) with resistance that is accommodating throughout the range of motion (ROM).
• Accommodating resistance means that Isokinetic exercise is the only way to dynamically load a muscle to its maximum capability throughout every point in the ROM.
• Therefore, the resistance varies to exactly match the force applied by the athlete at every point in the ROM.


• Isokinetics can be performed as an open kinetic chain exercise or a closed kinetic change exercise.
• An open kinetic chain exercise has limited functional carry over.
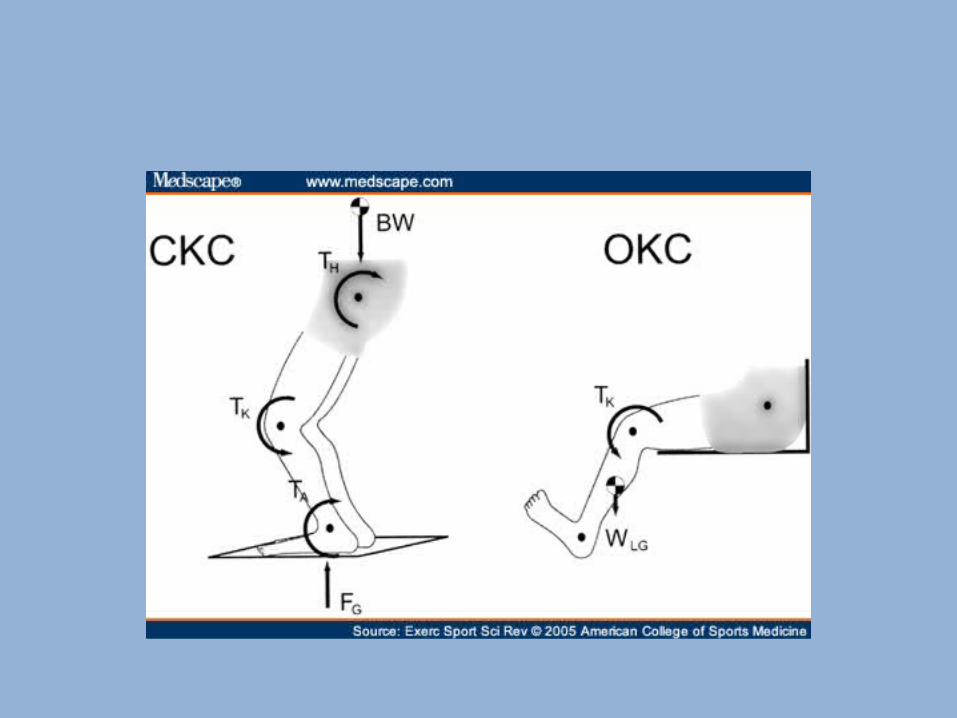
• Open kinetic chain (OKC) exercise is considered to be an activity in which the distal component of the limb (leg) is not fixed or weight bearing but free in space.

• Closed kinetic chain (CKC) exercise is considered to an activity in which the distal fixed end of the limb may be either stationary or moveable.
• For example, a CKC exercise in which the distal end (the foot) is stationary is a squat exercise in which the foot is fixed on the ground, as apposed to moving on a leg press.

Isokinetic machines have the ability to objectively measure muscle strength
The Isokinetic device is attached to a computer, that assesses the torque output of the muscles being testing.
• The torque output is converted to a foot-pound measurement. Isokinetic testing allows for a variety of testing protocols ranging from strength, strength ratios between two muscle groups, power, and endurance.
• Despite the fact that Isokinetic OKC exercise has been labeled as a non-functional exercise























