Page 1
Dr. M. Manzi
Interventional Radiology UnitFoot & Ankle Clinic
Policlinico Abano TermeRegional Center of Reference for Diabetic Foot
Treatment
Plantar Atch and BTA angioplasty-Who, When and How?
Page 2
DISCLOSURE:
Marco Manzi, MD
•Abbott Vascular: Consultant/Advisory Boarder•Angiodroid: Consultant•BARD: Consultant•BBraun Consultant•CID/ALVIMEDICA Consultant•COOK: Consultant•Boston Scientific: Proctor•Medtronic: Consultant/Proctor•TERUMO: Consultant
Page 3
• Non Healing Surgical Wounds; • TMA;• Foot Ulcers involving more than
one angiosome;• No tibial outflow;• Improving foot outflow in BAD;
When BTA Treatment/Arch Reconstruction/PPL? Our Indications
R.Ferraresi’s Concept of BAD: Big Artery DiseaseSAD: Small Artery Disease
SADBAD
Page 4
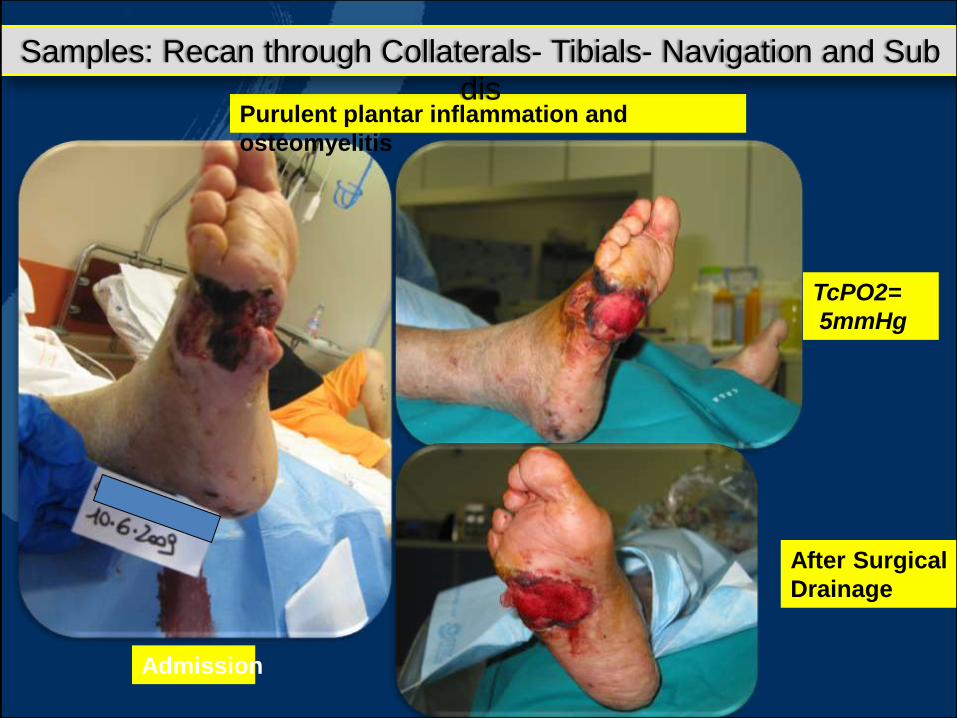
Purulent plantar inflammation and
osteomyelitis
TcPO2=
5mmHg
After Surgical
Drainage
Admission
Samples: Recan through Collaterals- Tibials- Navigation and Sub dis
Page 5
Anatomical Conds and Planning
Page 6
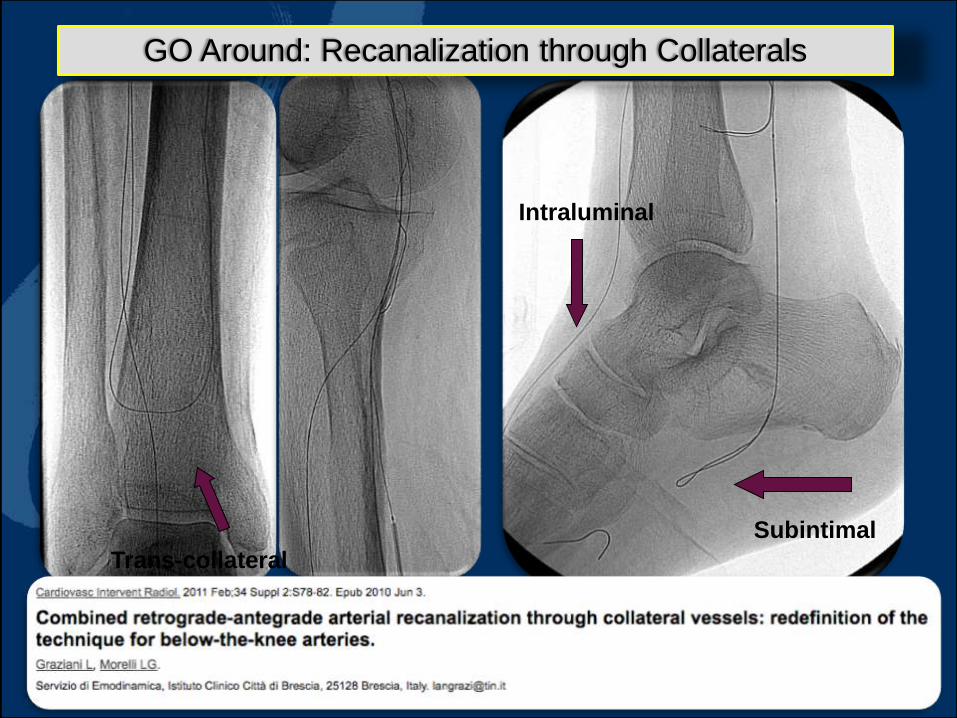
Intraluminal
Subintimal
Trans-collateral
GO Around: Recanalization through Collaterals
Page 7
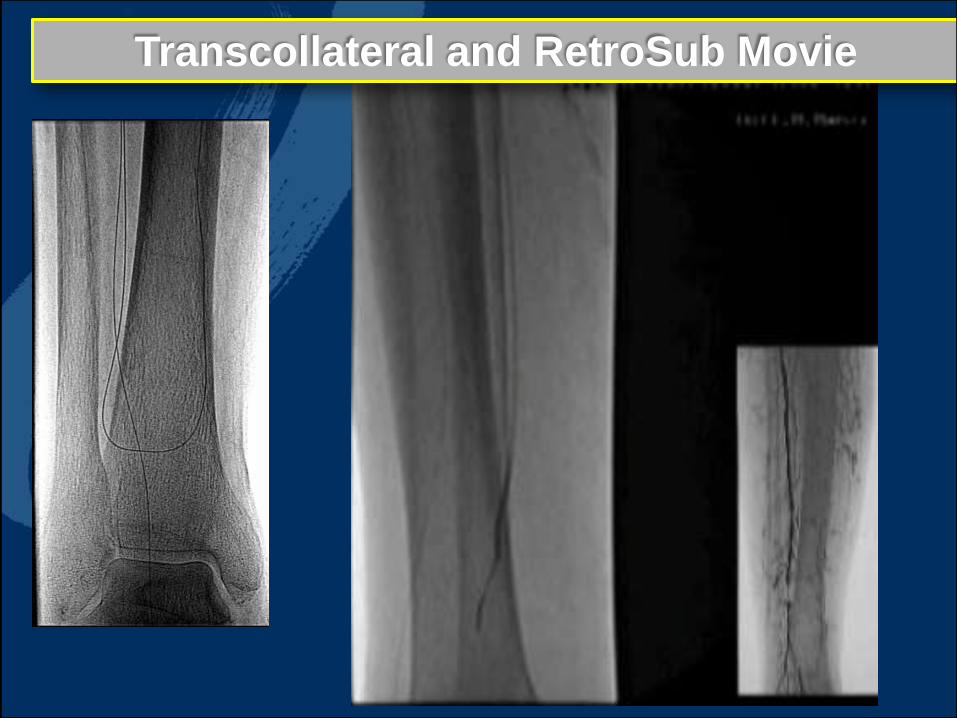
Transcollateral and RetroSub Movie
Page 8
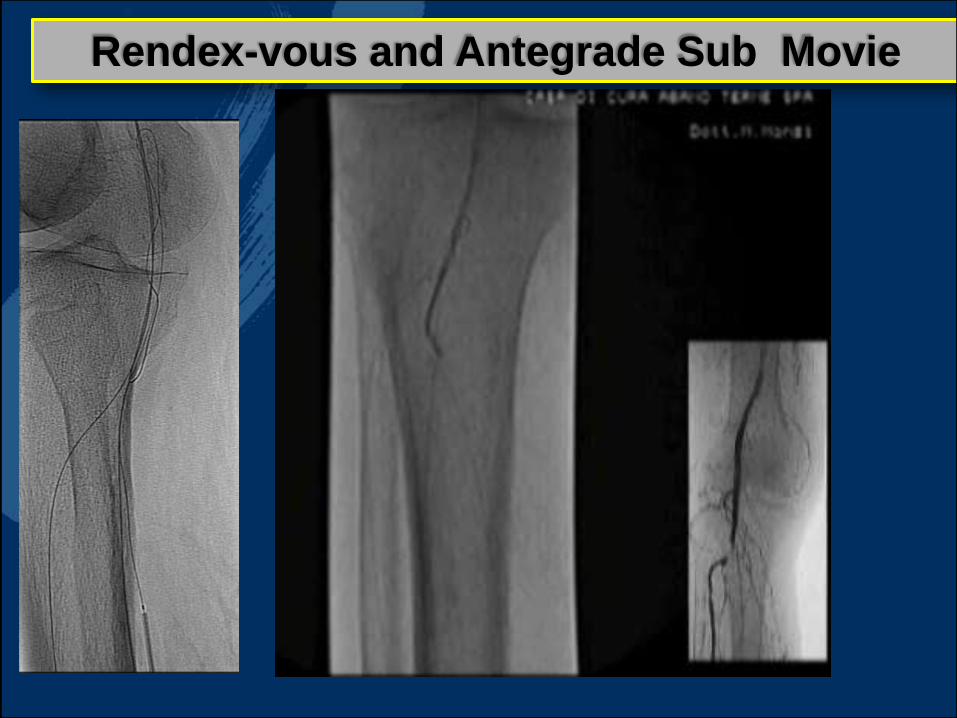
Rendex-vous and Antegrade Sub Movie
Page 9
True Lumen Re-Enter Movie
Page 10
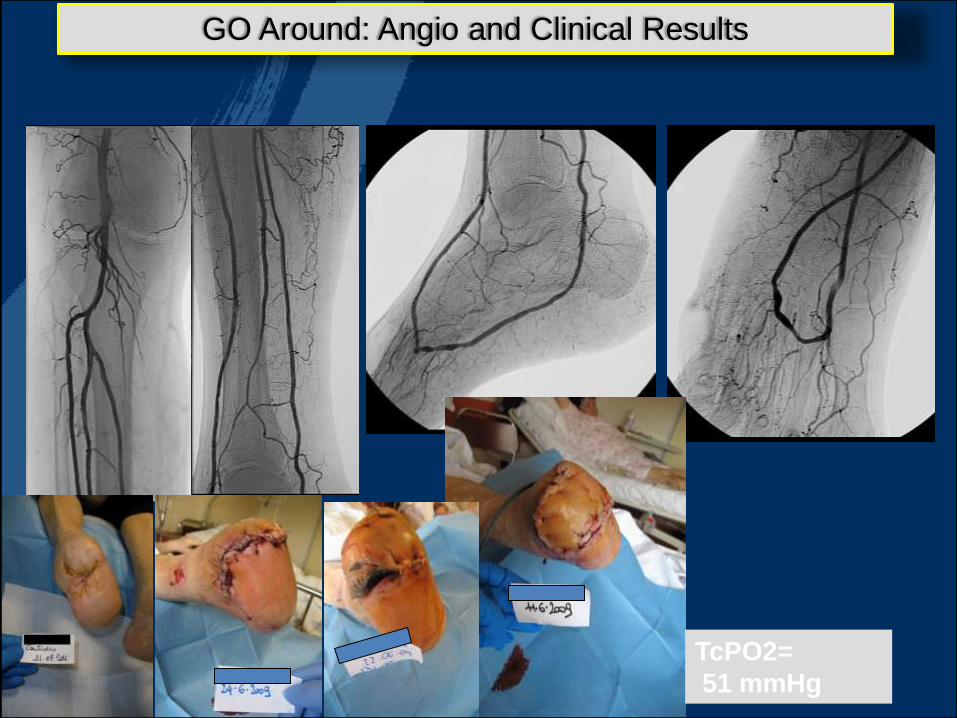
TcPO2=
51 mmHg
GO Around: Angio and Clinical Results
Page 11
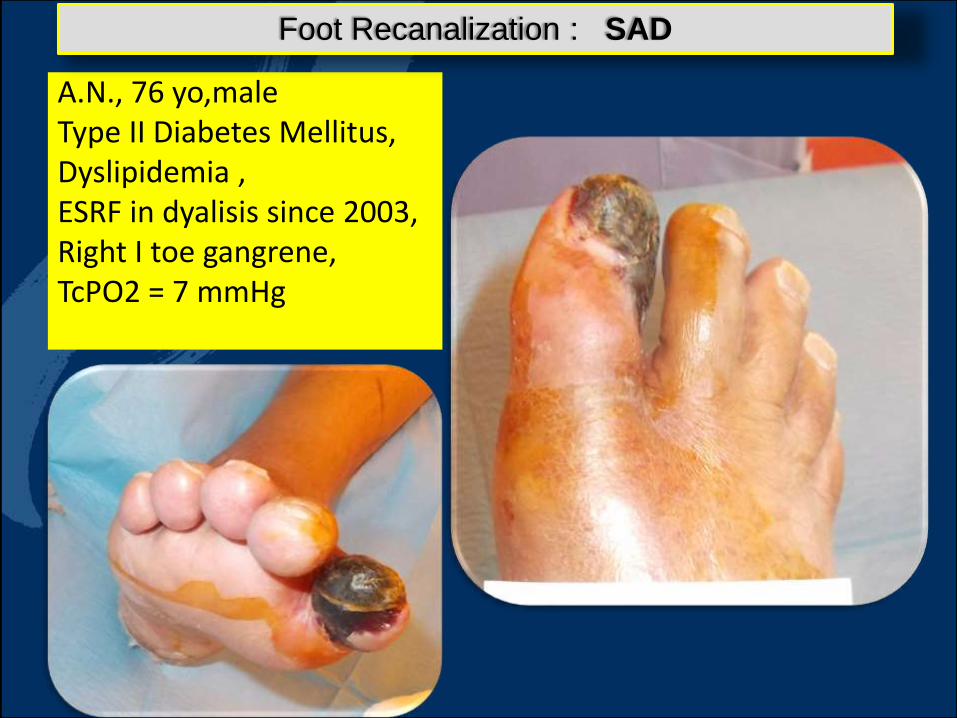
A.N., 76 yo,maleType II Diabetes Mellitus,Dyslipidemia ,ESRF in dyalisis since 2003,Right I toe gangrene,TcPO2 = 7 mmHg
Foot Recanalization : SAD
Page 13
• Long 4F sheathinto PedalArtery
Page 14
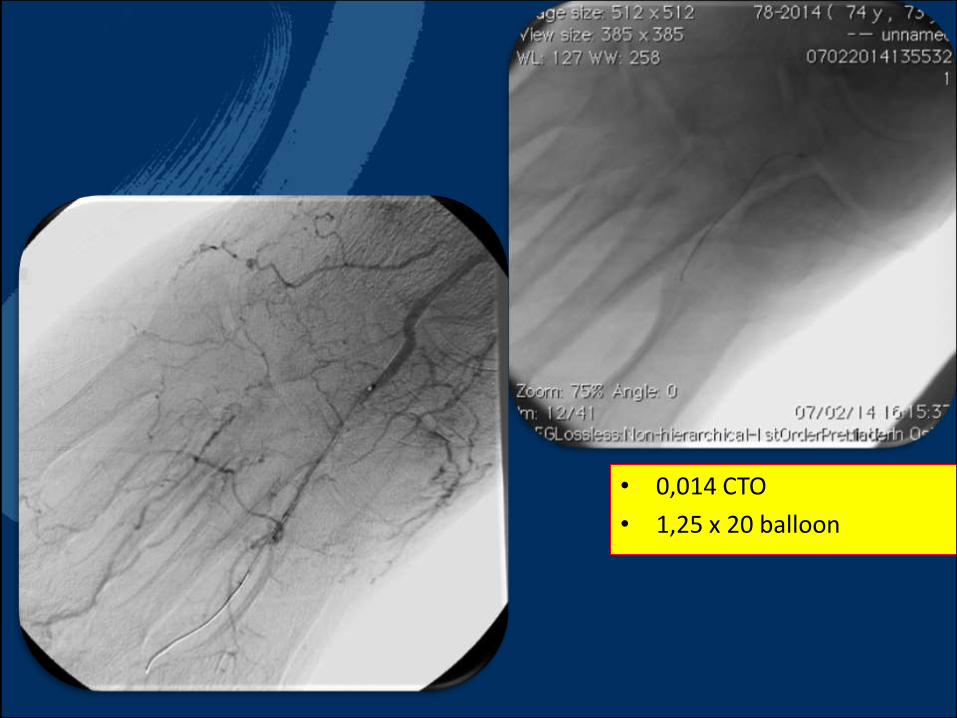
• 0,014 CTO
• 1,25 x 20 balloon
Page 15
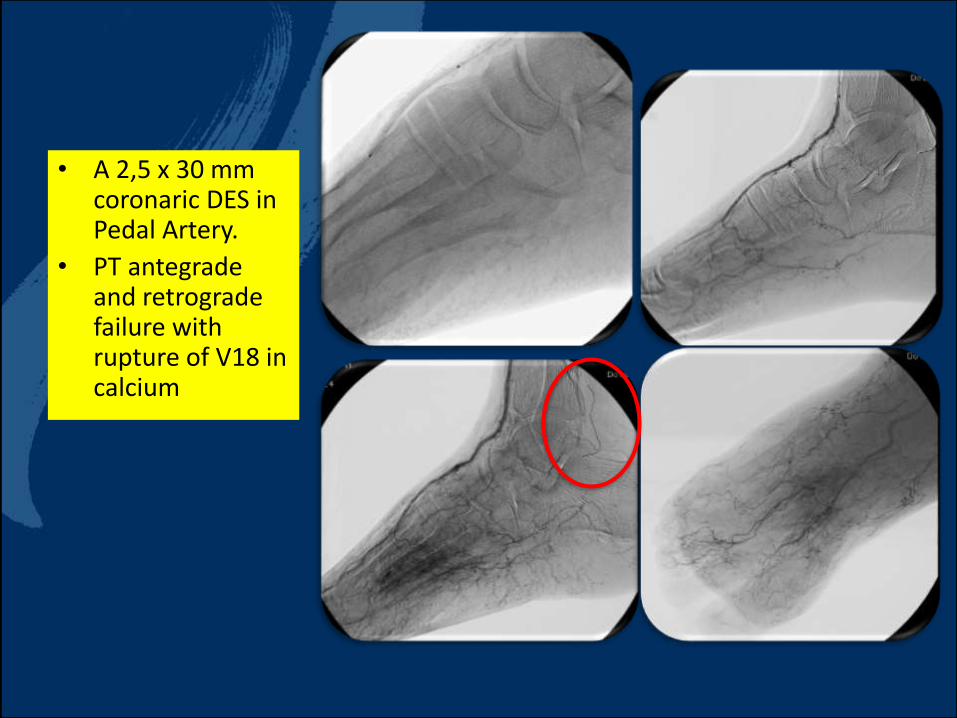
• A 2,5 x 30 mm coronaric DES in Pedal Artery.
• PT antegradeand retrograde failure with rupture of V18 in calcium
Page 16
• An amputation of the I° toe and a hialomatrixskingraft could be performed.
Page 17
• Somethingis goingwrong
Page 19
• BTK Amputation: Frequent “SAD”
STORY
Page 20
Go below-the-ankle or Improving Outflow:
Clear clinical indications: RTF 5-6 patients
Clear pathophysiology: disease of the foot vessels with failure of the foot distribution system
Clear limits: never touch what is, more or less, functioning;
Protect Collaterals with use of Drugs;
Dedicate Wires and Caths ;
Metatarsal Retrograde when failures;
CONCLUSIONS
Page 22
THANKS FOR YOUR ATTENTION
Page 23
Dr. M. Manzi
Interventional Radiology UnitFoot & Ankle Clinic
Policlinico Abano TermeRegional Center of Reference for Diabetic Foot
Treatment
Plantar Atch and BTA angioplasty-Who, When and How?