25
Plaque Morphology in Carotid Disease Tyrone Miller, D.O. Vascular Surgery Fellow Mt. Clemens Regional Medical Center
| Date post: | 04-Jan-2016 |
| Category: |
Documents |
| Upload: | eric-atkins |
| View: | 219 times |
| Download: | 1 times |

Plaque Morphology in Carotid DiseaseTyrone Miller, D.O.Vascular Surgery FellowMt. Clemens Regional Medical Center

Objectives
Background of Carotid Disease
Carotid Plaque Formation
Risk Factors
Plaque Classification
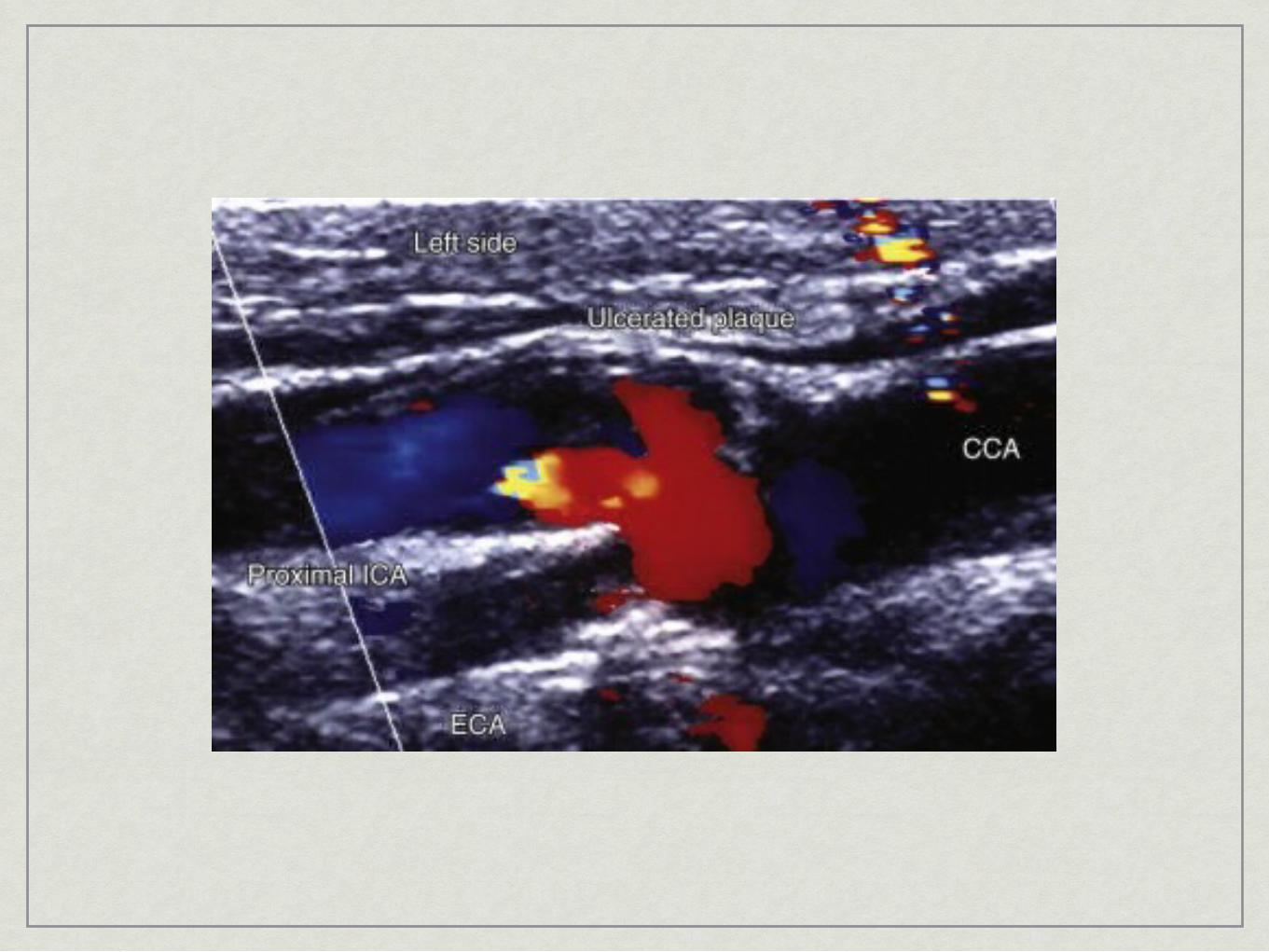
Ulcer classification
Studies

Background
• primary goal = prevention of stroke• 1st successful CEA - DeBakey 1953• Stroke = 3rd leading cause of death in US• 160,000 deaths/yr• 700,000 -> 500,000 new -> 200,000 recurrent• 8.1% 65y/o • 87% of CVA = ischemic 13% = hemorrhagic• extracranial atherosclerotic• intracranial atherosclerotic• lacunar• cardioembolic• misc• cryptogenic• prevalence of cerebrovascular DZ is much greater in pts with PVD
Socioeconomics• decreased life expectancy
• 6-7yrs (60-69)• 5-6yrs (70-79)• 2-3yrs (80+)
• only 50-70% of survivors regain functional independence• 50% some hemiparesis• 30% unable to walk without assistance• 26% dependent in performing ADL’s• 19% aphasic• 35% depressed• 26% nursing home

Risk Factorsagegender (male)race (NA, AA, bi-racial)HTNDMsmokingknown cerebrovascular dzatrial fibrillationlow levels of HDL in elderly mensedentary lifestyleexcessive ETOH useobesityTIA’s
90 day risk of stroke = 3-17.3%greatest risk in the first 30 days1707pts - 10.5% in 90 days --- 5.3% in the first 48hrs10yr risk of CVA, MI, vascular death = 43%

Natural History
• Carotid Atherosclerosis predisposes patients to TIA and stroke, and the risk for these events is proportional to the severity of the carotid disease.
• Chambers and Norris 500 pts with cervical bruit (TIA and CVA, US)• 2.1% (0-29%)• 5.7% (30-74%)• 19.5% (75-100%)
• Calcified plaque is less likely to cause symptoms than soft echolucent plaque
• Roederer et al. • progression from less than 80% stenosis to greater than 80%
stenosis = high risk of CVA/TIA• within 6mths of progression --> 35% risk• within 12mths --> 46%• 1.5% risk in those with stable plaques

Clinical Diagnosis of Carotid Disease
• EMBOLIC SYMPTOMS• Transient monocular blindness• Transient monocular field cuts• Dysarthria • Dysphasia• Aphasia• Monoparesis• Hemiparesis• Hemisensory deficit
• HYPOPERFUSION SYMPTOMS • Bright light amaurosis • Lightheadedness or presyncope associated with any of the
above focal deficits
Indications for Carotid SurgeryAsymptomatic patients:
high grade stenosis if the life expectancy is > 2 years, and the surgeon can perform the procedure with < 3% morbidity and mortality.
Symptomatic Patients:TIA or ischemic stroke within the last 6 mo and ipsilateral 70% - 99% stenosis if a surgeon has perioperative morbidity and mortality of < 6%.TIA or ischemic stroke and ipsilateral moderate (50% -69%) stenosis depending on patient-specific factors such as age, gender, comorbidities, and severity of initial symptoms.
Controversial Area:Asymptomatic stenosis exceeding 80% in a high risk patient. Ulcerated lesions without hemodynamically significant stenosis.

Carotid Plaque Formation
Continued infiltration of lipid into the arterial wall leads to macrophage infiltration, elaboration of growth factors, and chronic inflammation with a slow increase in plaque mass. Macrophage lysis with release of proteolytic enzymes, coupled with further lipid infiltration, results in complex plaque with areas of lipid accumulation, necrotic debris, ongoing chronic inflammation, and calcification.

ClassificationType I: uniformly echolucent
Type II: predominantly echolucent (>50% of the structure of the plaque)
Type III: predominantly echogenic (>50% of the structure of the plaque)
Type IV: uniformly echogenic
Type V: unclassified (heavy calcification causing acoustic shadowing or poor quality images)
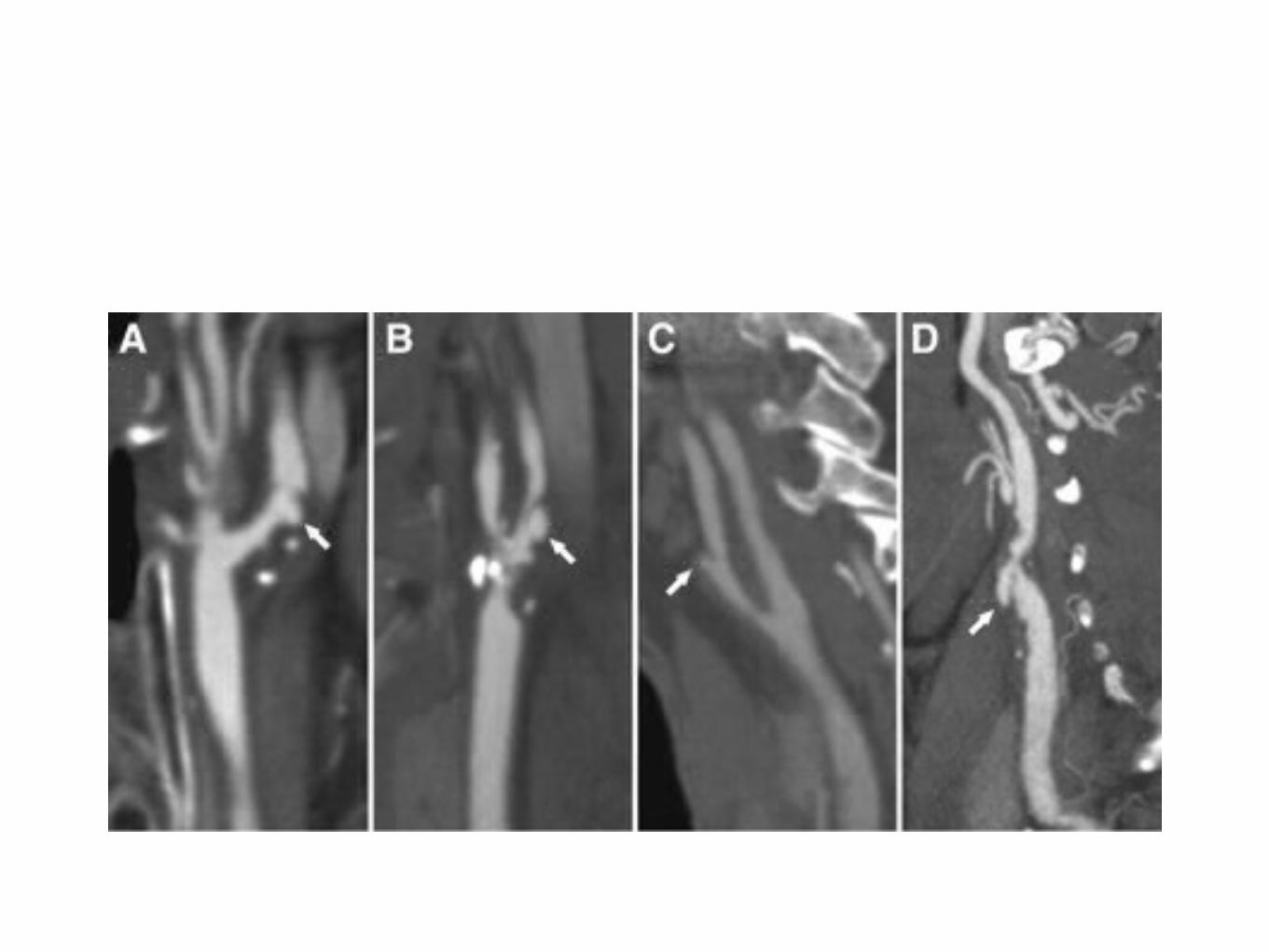
Geroulakos et al.

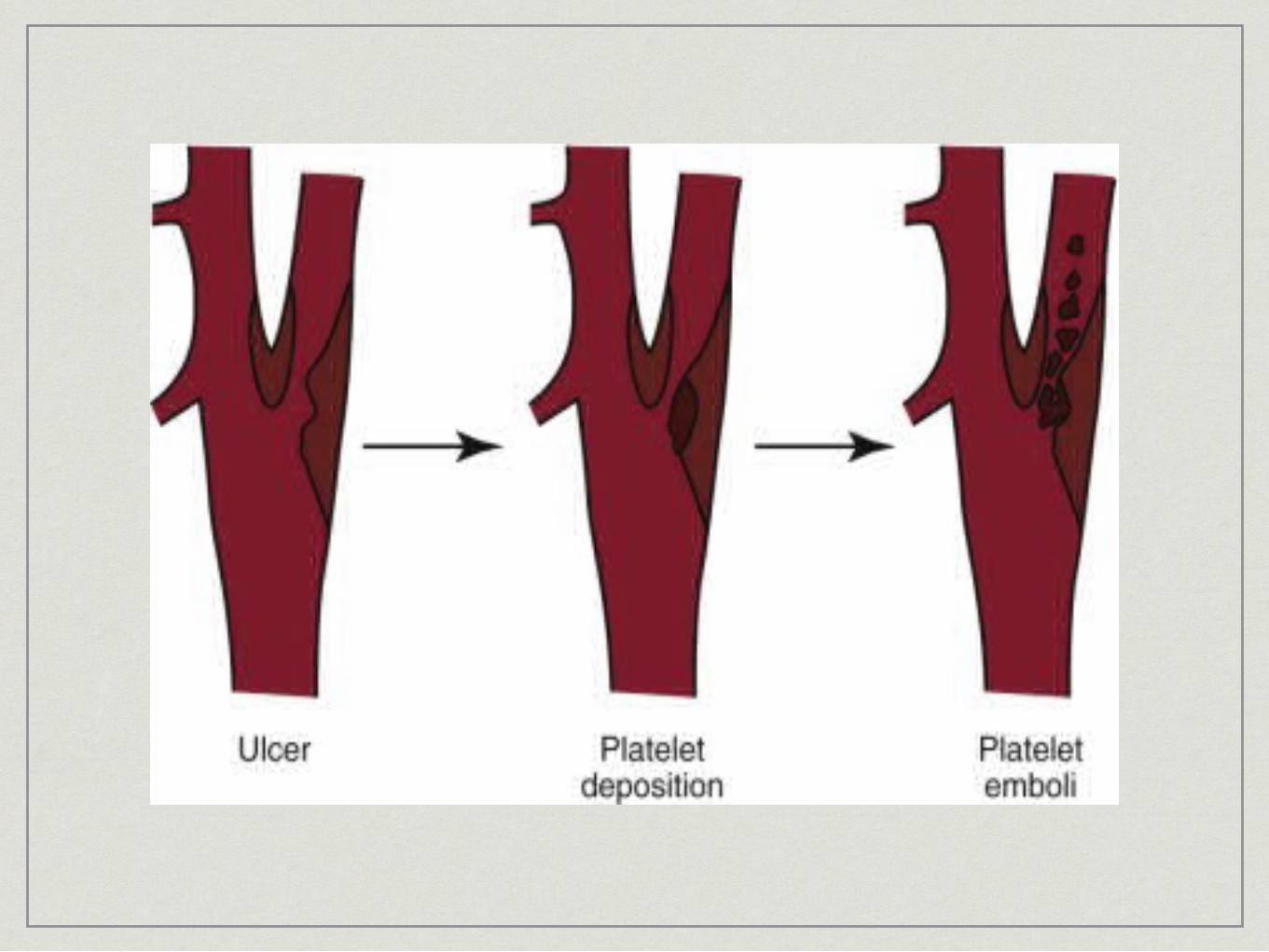

Figure 1. Examples of angiographic carotid plaque surface ulceration (types 1 to 4).
Lovett J et al. Circulation 2004;110:2190-2197
Copyright © American Heart Association

Benefit of Carotid Endarterectomy
Trial Indication Perioperative CVA/Death Risk Reduction P Value
NASCET Sx: ≥70% 5.8% 16.5%/2 yr <.001
Sx: 50%-69% 6.7% 10.1%/5 yr <.05
ECST Sx: 70%-99% 7.5% 9.6%/3 yr <.01
ACAS Asx: ≥60% 2.3% 5.9%/5 yr 0.004
ACST Asx: >60% 3.1% 5.4%/5 yr <.0001
North American Symptomatic CEA TrialEuropean Carotid Surgery TrialAsymptomatic Carotid Athersclerosis StudyAsymptomatic Carotid Surgery Trial

Treatment of Carotid Artery Stenosis: Medical Therapy, Surgery, or Stenting?Giuseppe Lanzino, MD, Alejandro A. Rabinstein, MD, and Robert D. Brown, Jr, MD
• Mayo Clinic Proceedings, 2009• Review of literature• Antiplatelet drug therapy and aggressive correction of risk factors are the
mainstays of medical therapy. • BP control• Lipid lowing (statin)• Aspirin• Exercise >30mins 5 days a week
• Carotid endarterectomy should be strongly considered for symptomatic patients with 70% to 99% stenosis and should also be considered for symptomatic patients with 50% to 69% stenosis if no other etiologic basis for the ischemic symptoms can be found.
• Surgery should be recommended only in selected patients with asymptomatic carotid artery stenosis because of the marginal benefit from revascularization in this patient population.
• The CAS procedure is a valid alternative to CEA for selected patients who have an indication for revascularization and are at high surgical risk.

Carotid Plaque Ultrasonic Heterogeneity and Severity of StenosisAli F. AbuRahma, MD; John T. Wulu Jr, PhD; Brad Crotty
• Background and Purpose:
• Several studies have reported on the correlation of ultrasonic carotid plaque morphology, cerebrovascular symptoms, and intraplaque hemorrhage. This study correlates ultrasonic carotid plaque morphology with the degree of carotid stenosis.

Stenosis Classification/Plaque Morphology/Neurological Events
Stenosis Classification (N)
Homogeneous Plaques, n (%) Heterogeneous Plaques, n (%) P Odds Ratio (95% CI)
Symptomatic* Asymptomatic Symptomatic* Asymptomatic
<50% (794) 127 (16) 529 (84) 94 (68) 44 (32) <0.0001 8.9 (5.8–13.7)
≥50–<60% (564)
78 (21) 295 (79) 145 (76) 46 (24) <0.0001 11.9 (7.7–18.5)
≥60%–<70% (487)
43 (23) 143 (77) 238 (79) 63 (21) <0.0001 12.6 (7.9–20)
≥70%–99% (615)
37 (31) 82 (69) 427 (86) 69 (14) <0.0001 13.7 (8.4–22.4)
Total (2460) 285 1049 904 222 <0.0001 14.9 (12.3–18.3)
P values are for symptomatic homogeneous vs heterogeneous plaques within stenosis classification.
*TIA/stroke.

Plaque Heterogeneity vs Severity of Stenosis
Homogeneous, n (%) Heterogeneous, n (%)
P Odds Ratio (95% CI)
≥50% stenosis (N=1666) 678 (41) 988 (59) <0.001 6.9 (5.6–8.6)
<50% stenosis (N=794) 656 (83) 138 (17)
≥60% stenosis (N=1102) 305 (28) 797 (72) <0.0001 8.2 (6.8–9.8)
<60% stenosis (N=1358) 1029 (76) 329 (24)
≥70% stenosis (N=615) 119 (20) 496 (80) <0.001 8.0 (6.4–10.1)
<70% stenosis (N=1845) 1215 (66) 630 (34)
P values are for heterogeneous values within stenosis groups.

Correlation of Cerebrovascular Symptoms vs Heterogeneity of Plaque and Degree of Stenosis
Symptomatic, n (%) Asymptomatic, n (%) Odds Ratio (95% CI)
All heterogeneous* (N=1126)
904 (80)ठ222 (20)
All ≥50% stenosis† (N=1666)
968 (58) 698 (42) 0.3 (0.3–0.4)
All ≥60% stenosis† (N=1102)
745 (68) 357 (32) 0.5 (0.4–0.6)
All ≥70% stenosis† (N=615)
464 (75) 151 (25) 0.8 (0.6–1.0)
*Includes all stenoses (including <50% stenosis).
†Includes homogeneous and heterogeneous plaques.
‡P<0.0001 vs all ≥50% stenosis and all ≥60% stenosis for symptomatic groups.
§P<0.02 vs all ≥70% stenosis for symptomatic groups.
Ultrasonic plaque echolucency and emboli signals predict stroke in asymptomatic carotid stenosisR. Topakian, MD, A. King, BSc, S.U. Kwon, MD, PhD, A. Schaafsma, MD, M. Shipley, MSc, H.S. Markus, MD and For the ACES Investigators
• Objectives: • Better methods are required to identify patients with
asymptomatic carotid stenosis (ACS) at risk of future stroke. Two potential markers of high risk are echolucent plaque morphology on carotid ultrasound and embolic signals (ES) in the ipsilateral middle cerebral artery on transcranial Doppler ultrasound (TCD). We explored the predictive value of a score based on these 2 measures in the prospective, observational, international multicenter Asymptomatic Carotid Emboli Study.
• Results:• A total of 164 (37.7%) plaques were graded as echolucent. Plaque
echolucency at baseline was associated with an increased risk of ipsilateral stroke alone (hazard ratio [HR] 6.43, 95% confidence interval [CI] 1.36–30.44, p = 0.019). A combined variable of plaque echolucency and ES positivity at baseline was associated with a markedly increased risk of ipsilateral stroke alone (HR 10.61, 95% CI 2.98–37.82, p = 0.0003). This association remained significant after controlling for risk factors, degree of carotid stenosis, and antiplatelet medication.
Carotid Plaque Surface Irregularity Predicts Ischemic StrokeThe Northern Manhattan StudyShyam Prabhakaran, MD; Tatjana Rundek, MD, PhD; Romel Ramas, MD; Mitchell S.V. Elkind, MD, MS; Myunghee Cho Paik, PhD; Bernadette Boden-Albala, MPH, DrPH; Ralph L. Sacco, MD, MS
• Background and Purpose:• There is scant population-based evidence regarding extracranial carotid
plaque surface irregularity and ischemic stroke. Using a prospective cohort design, we evaluated the association of carotid plaque surface irregularity and the risk of ischemic stroke in a multiethnic population.
• Results:• Among 1939 total subjects, carotid plaque was visualized in 56.3% (1
plaque: 21.6%, >1 plaque: 34.7%, irregular plaque: 5.5%). During a mean follow up of 6.2 years after ultrasound examination, 69 ischemic strokes occurred. Unadjusted cumulative 5-year risks of ischemic stroke were: 1.3%, 3.0%, and 8.5% for no plaque, regular plaque, and irregular plaque, respectively. After adjusting for demographics, traditional vascular risk factors, degree of stenosis, and plaque thickness, presence of irregular plaque (vs no plaque) was independently associated with ischemic stroke (Hazard ratio, 3.1; 95% CI, 1.1 to 8.5).
Summary
• Carotid Atherosclerosis predisposes patients to TIA and stroke, and the risk for these events is proportional to the severity of the carotid disease.
• Calcified plaque is less likely to cause symptoms than soft echolucent plaque
• Plaque echolucency is associated with an increased risk of ipsilateral stroke.
• Irregular plaque (vs no plaque) was independently associated with ischemic stroke.

Questions?

















