21
PMTCT Guidelines: Conflicting Recommendations Kathleen E. Squires, M.D. Thomas Jefferson University

PMTCT Guidelines: Conflicting Recommendations
Kathleen E. Squires, M.D. Thomas Jefferson University

Program Overview
• Rationale for PMTCT • Differences in antiretroviral therapy • Differences in obstetric management • Differences in post-natal management of the infant
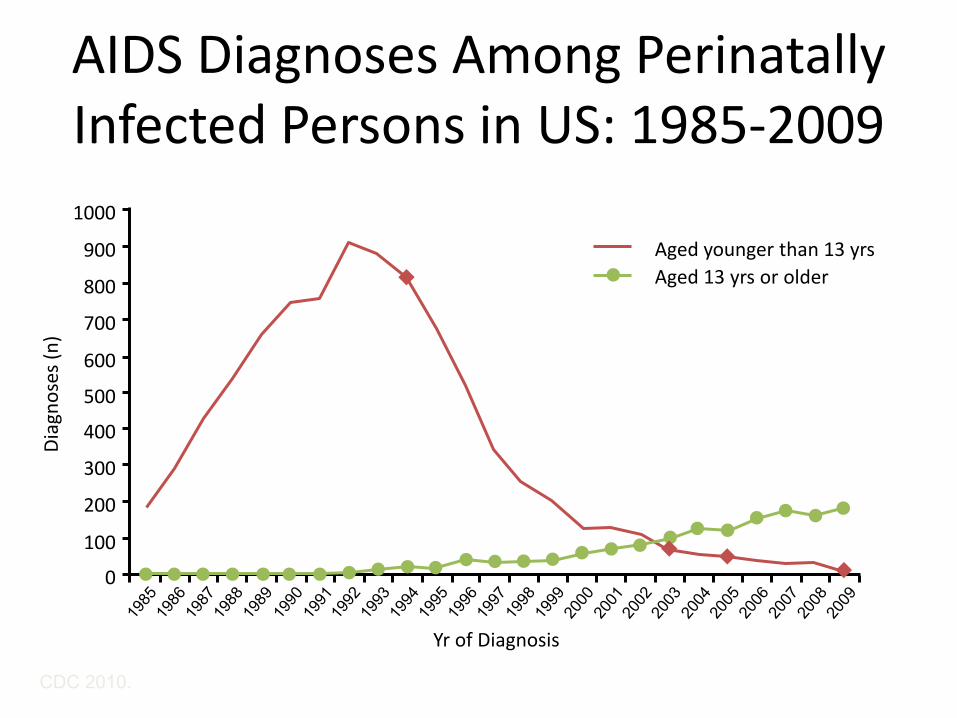
AIDS Diagnoses Among Perinatally Infected Persons in US: 1985-2009
CDC 2010.
Diag
nose
s (n)
1000
900
500
300
0
800
700
600
400
200
100
Yr of Diagnosis
Aged younger than 13 yrs Aged 13 yrs or older

Change in MTCT in Resource-Rich Countries
ZDV Era Combination ARV Era
Tran
smiss
ion
(%)
40
30
20
10
0 1993: WITS
1994: PACTG
076
1997: PACTG
185
1999: WITS
2001: PACTG
247
2002: PACTG
316
2003: WITS
2006: UK
24.5
7.6 5.0
3.3 2.0 1.5 1.2 0.8
Courtesy of Lynne Mofenson.

Basic Principles of Use of Antiretrovirals in Pregnancy
• ARVs should be initiated in all HIV-infected pregnant women regardless of CD4+ cell count or HIV-1 RNA level
• Regimens used should be effective in treatment of nonpregnant adults and should be safe and well tolerated
– Regimen should consist of 2 NRTIs and either an NNRTI or a PI, most often with ritonavir boosting • Include ≥ 1 NRTI with good placental passage
• Earlier initiation more effective in PMTCT • Women entering pregnancy on ART should continue on
regimen, if effective and tolerated
DHHS HIV Perinatal Guidelines. July 31, 2012.
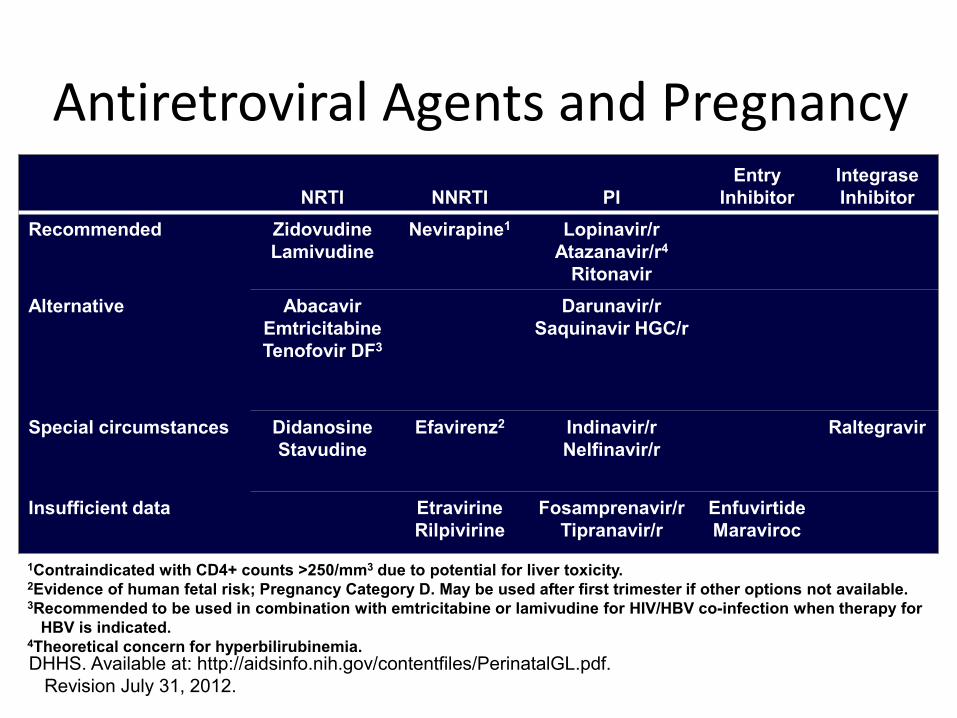
Antiretroviral Agents and Pregnancy
NRTI
NNRTI
PI Entry
Inhibitor Integrase Inhibitor
Recommended Zidovudine Lamivudine
Nevirapine1 Lopinavir/r Atazanavir/r4
Ritonavir Alternative Abacavir
Emtricitabine Tenofovir DF3
Darunavir/r Saquinavir HGC/r
Special circumstances Didanosine Stavudine
Efavirenz2 Indinavir/r Nelfinavir/r
Raltegravir
Insufficient data Etravirine Rilpivirine
Fosamprenavir/r Tipranavir/r
Enfuvirtide Maraviroc
DHHS. Available at: http://aidsinfo.nih.gov/contentfiles/PerinatalGL.pdf. Revision July 31, 2012.
1Contraindicated with CD4+ counts >250/mm3 due to potential for liver toxicity. 2Evidence of human fetal risk; Pregnancy Category D. May be used after first trimester if other options not available. 3Recommended to be used in combination with emtricitabine or lamivudine for HIV/HBV co-infection when therapy for HBV is indicated. 4Theoretical concern for hyperbilirubinemia.
Program Overview
• Rationale for PMTCT
• Differences in antiretroviral therapy • Differences in obstetric management • Differences in post-natal management of the infant
Efavirenz in Pregnancy • Preclinical primate data and retrospective reports in humans raise
concerns about increased risk of neural tube defects[1]
• ART registry reports have not indicated increased risk of birth defects in infants exposed to EFV during the first trimester [2]
• A recent meta-analysis of 1437 women in 19 studies [ with first trimester EFV exposure found NO increased risk of birth defects and only 1 neural tube defect (incidence: 0.07%)[3]
• However, 2 reports of high rates of birth defects in infants exposed to EFV in utero [15.6% [4] and 12.8% [5]]
• Treatment change in pregnancy associated with increased risk of incomplete viral suppression at end of pregnancy[3
1. DHHS HIV Perinatal Guidelines. July 31, 2012. 2. Antiretroviral Treatment Registry, http://www.APRegistry.org 3. Ford N, et al. AIDS. 2011;25:2301-2304. 3. Floridia M, et al. HIV Clin Trials. 2010;11:303-311. 4. Brogly SB et al. Pediatr Inf Dis J 2010;29:721-727. 5. Knapp KM et al. Pediatr Inf Dis J 2012;31:164-70.

EFV Differences
• DHHS Guidelines – Not recommended first
trimester but if a woman is on it don’t switch if this likely to compromise virologic control
BHIVA Guidelines – No evidence for
teratogenicity
– No restrictions for use

Pharmacokinetics
• Considerations for protease inhibitor use during pregnancy – PIs highly protein bound with little placental transfer – Increased free drug levels in third trimester due to
reduction in protein binding
• Clinical significance unknown – No reports of increased virological failure or HIV
transmission associated with use of standard doses
Napravnik S, et al. JAIDS. 2002;31:11-19.

Differences in PI Dosing in Pregnancy
• DHHS Guidelines – LPV/r
• Increase dose in 2nd and 3rd trimesters, especially if treatment-experienced
– ATV/r • Increase dose if treatment-
experienced, receiving TDF, H2 antagonist
– DRV/r • Administer BID
BHIVA Guidelines – LPV/r
– No specific recommendations
– ATV/r
– ? TDM 3rd trimester if TDF
– DRV/r
– Administer BID

Program Overview
• Rationale for PMTCT • Differences in antiretroviral therapy
• Differences in obstetric management • Differences in post-natal management of the infant
Intrapartum Zidovudine
• PACTG 076 – Efficacy of three part zidovudine regimen [1]
– Subsequent reports demonstrating efficacy of this approach
• No evidence that intrapartum use of zidovudine decreased risk of transmission in women on ART with viral loads <10,000 copies/mL [2]
1. DHHS HIV Perinatal Guidelines. July 31, 2012. 2. Warszawaski J et al. AIDS.
Differences in Use of Intrapartum Zidovudine
• DHHS Guidelines – Use intrapartum in
women with VL in 3rd trimester >400 copies/mL
BHIVA Guidelines – Use intrapartum in
women with VL >10,000 copies/mL

Vaginal Delivery vs Elective Caesarean Section
• WITS study – No transmissions in 0/57 women with plasma VL <1000
copies/mL [1]
• Over the past decade the lower limit of detection of commercially available viral load assays has decreased significantly. Studies utilizing these assays have not been repeated so we can only make inferences in terms of recommendations based of VL thresholds.
1. Garcia PM et al. NEJM 1999;341:394-402
Differences in Mode of Delivery
• DHHS Guidelines – Vaginal birth if VL in 3rd
trimester <1000 copies/mL
BHIVA Guidelines – Vaginal birth if VL in 3rd
trimester <50 copies/mL

Program Overview
• Rationale for PMTCT • Differences in antiretroviral therapy • Differences in obstetric management
• Differences in post-natal management of the infant

Neonatal Postexposure Prophylaxis
• PACT 076 • Transmission rate of 1.1% in 916 infants whose mothers
received ART during pregnancy [1]
1. Ferguson W et al. Pediatr Inf Dis J 2011;30:408-412.
Differences in Prophylaxis: Exposed Infant
• DHHS Guidelines – Administer meds for 6
weeks
BHIVA Guidelines – Administer meds for 4
weeks

Differences in ART: Mother with Detectable VL
• DHHS Guidelines – Administer 2 drugs
BHIVA Guidelines – Administer 3 drugs

PMTCT Guidelines: Summary
• Overall goals for guideline panels are consistent • HIV-infected woman who is pregnant
• Suppress HIV RNA to BLOD of assay (<1000 copies/mL [preferably <50 copies/mL]) to minimize risk of transmission of HIV to the fetus and newborn
• Selection of an antiretroviral combination – Take into account known safety, efficacy, and pharmacokinetic data of each
agent during pregnancy
• There are differences between the guidelines documents that clinicians who manage this patient population should be aware of
DHHS. Available at: http://aidsinfo.nih.gov/contentfiles/PerinatalGL.pdf. Revision September 14, 2011.

















