Point-of-Care Ultrasonography for Primary Care Physicians and General Internists Anjali Bhagra, MBBS; David M. Tierney, MD; Hiroshi Sekiguchi, MD; and Nilam J. Soni, MD, MSc Abstract Point-of-care ultrasonography (POCUS) is a safe and rapidly evolving diagnostic modality that is now utilized by health care professionals from nearly all specialties. Technological advances have improved the portability of equipment, enabling ultrasound imaging to be executed at the bedside and thereby allowing internists to make timely diagnoses and perform ultrasound-guided procedures. We reviewed the liter- ature on the POCUS applications most relevant to the practice of internal medicine. The use of POCUS can immediately narrow differential diagnoses by building on the clinical information revealed by the tradi- tional physical examination and refining clinical decision making for further management. We describe 2 common patient scenarios (heart failure and sepsis) to highlight the impact of POCUS performed by internists on efficiency, diagnostic accuracy, resource utilization, and radiation exposure. Using POCUS to guide procedures has been found to reduce procedure-related complications, along with costs and lengths of stay associated with these complications. Despite several undisputed advantages of POCUS, barriers to implementation must be considered. Most importantly, the utility of POCUS depends on the experience and skills of the operator, which are affected by the availability of training and the cost of ultrasound devices. Additional system barriers include availability of templates for documentation, electronic storage for image archiving, and policies and procedures for quality assurance and billing. Integration of POCUS into the practice of internal medicine is an inevitable change that will empower internists to improve the care of their patients at the bedside. ª 2016 Mayo Foundation for Medical Education and Research n Mayo Clin Proc. 2016;91(12):1811-1827 P oint-of-care ultrasonography (POCUS) is a safe and rapidly evolving diagnostic modality. Traditionally, ultrasonogra- phy has been used by imaging specialists, such as radiologists and cardiologists; however, it is now utilized by health care professionals from nearly all specialties. Technological ad- vances have improved portability and minia- turization of equipment, allowing ultrasound imaging at the bedside to make timely diagno- ses and guide procedures. Over the past several years, there has been emerging interest in the routine use of POCUS to potentially expedite and provide cost-efficient, high-value care. 1 This technology has been touted as the “vi- sual stethoscope” of the 21st century. 2,3 The stethoscope, developed 200 years ago, is the classic icon for the traditional diagnostic phys- ical examination and is still the most widely used tool to examine patients at the bedside. It is interesting to note, however, that the stethoscope is truly a “stethophone” because it allows only listening to the human body (steth ¼ chest, phone ¼ sound), rather than truly looking inside the body (scope ¼ to look in). However, as true “scopes,” portable ultrasound devices can generate high-quality images revealing the structure and function of organs. 4 The traditional bedside physical examination has been on the decline within internal medicine for several years for various reasons. 5-9 This increase in ambiguity in diag- nosis is potentially unsettling to internal med- icine physicians who see a variety of complex presentations and want to “do no harm.” Globally, medical education still emphasizes teaching traditional physical examination; however, no patient outcomes data justify application of physical examination tech- niques learned for commonly encountered clinical conditions. As an example, little data exist regarding an evaluation of central venous pressure using jugular venous distention in a morbidly obese patient. Moreover, many From the Division of General Internal Medicine (A.B.) and Division of Pul- monary and Critical Care Medicine (H.S.), Depart- ment of Medicine, Mayo Clinic, Rochester, MN; Abbott Northwestern Hospital, Medical Educa- tion Department, Minne- apolis, MN (D.M.T.); and Section of Hospital Medi- cine, South Texas Veter- ans Health Care System and Division of Pulmonary Diseases and Critical Care Medicine, University of Texas Health Science Center, San Antonio, TX (N.J.S.). REVIEW Mayo Clin Proc. n December 2016;91(12):1811-1827 n http://dx.doi.org/10.1016/j.mayocp.2016.08.023 www.mayoclinicproceedings.org n ª 2016 Mayo Foundation for Medical Education and Research 1811
Transcript
REVIEW
Point-of-Care Ultrasonography for Primary CarePhysicians and General Internists
Anjali Bhagra, MBBS; David M. Tierney, MD; Hiroshi Sekiguchi, MD;and Nilam J. Soni, MD, MSc
Abstract
Point-of-care ultrasonography (POCUS) is a safe and rapidly evolving diagnostic modality that is nowutilized by health care professionals from nearly all specialties. Technological advances have improved theportability of equipment, enabling ultrasound imaging to be executed at the bedside and thereby allowinginternists to make timely diagnoses and perform ultrasound-guided procedures. We reviewed the liter-ature on the POCUS applications most relevant to the practice of internal medicine. The use of POCUS canimmediately narrow differential diagnoses by building on the clinical information revealed by the tradi-tional physical examination and refining clinical decision making for further management. We describe 2common patient scenarios (heart failure and sepsis) to highlight the impact of POCUS performed byinternists on efficiency, diagnostic accuracy, resource utilization, and radiation exposure. Using POCUS toguide procedures has been found to reduce procedure-related complications, along with costs and lengthsof stay associated with these complications. Despite several undisputed advantages of POCUS, barriers toimplementation must be considered. Most importantly, the utility of POCUS depends on the experienceand skills of the operator, which are affected by the availability of training and the cost of ultrasounddevices. Additional system barriers include availability of templates for documentation, electronic storagefor image archiving, and policies and procedures for quality assurance and billing. Integration of POCUSinto the practice of internal medicine is an inevitable change that will empower internists to improve thecare of their patients at the bedside.
ª 2016 Mayo Foundation for Medical Education and Research n Mayo Clin Proc. 2016;91(12):1811-1827
From the Division ofGeneral Internal Medicine(A.B.) and Division of Pul-monary and Critical CareMedicine (H.S.), Depart-ment of Medicine, MayoClinic, Rochester, MN;Abbott NorthwesternHospital, Medical Educa-tion Department, Minne-apolis, MN (D.M.T.); andSection of Hospital Medi-cine, South Texas Veter-ans Health Care Systemand Division of PulmonaryDiseases and Critical CareMedicine, University ofTexas Health ScienceCenter, San Antonio, TX(N.J.S.).
P oint-of-care ultrasonography (POCUS)is a safe and rapidly evolving diagnosticmodality. Traditionally, ultrasonogra-
phy has been used by imaging specialists,such as radiologists and cardiologists; however,it is now utilized by health care professionalsfrom nearly all specialties. Technological ad-vances have improved portability and minia-turization of equipment, allowing ultrasoundimaging at the bedside to make timely diagno-ses and guide procedures. Over the past severalyears, there has been emerging interest in theroutine use of POCUS to potentially expediteand provide cost-efficient, high-value care.1
This technology has been touted as the “vi-sual stethoscope” of the 21st century.2,3 Thestethoscope, developed 200 years ago, is theclassic icon for the traditional diagnostic phys-ical examination and is still the most widelyused tool to examine patients at the bedside.It is interesting to note, however, that thestethoscope is truly a “stethophone” because
Mayo Clin Proc. n December 2016;91(12):1811-1827 n http://dx.dowww.mayoclinicproceedings.org n ª 2016 Mayo Foundation for M
it allows only listening to the human body(steth ¼ chest, phone ¼ sound), rather thantruly looking inside the body (scope ¼ tolook in). However, as true “scopes,” portableultrasound devices can generate high-qualityimages revealing the structure and functionof organs.4 The traditional bedside physicalexamination has been on the decline withininternal medicine for several years for variousreasons.5-9 This increase in ambiguity in diag-nosis is potentially unsettling to internal med-icine physicians who see a variety of complexpresentations and want to “do no harm.”Globally, medical education still emphasizesteaching traditional physical examination;however, no patient outcomes data justifyapplication of physical examination tech-niques learned for commonly encounteredclinical conditions. As an example, little dataexist regarding an evaluation of central venouspressure using jugular venous distention in amorbidly obese patient. Moreover, many
i.org/10.1016/j.mayocp.2016.08.023edical Education and Research
important cardiopulmonary abnormalities thatare easily and rapidly detected by POCUS,such as pericardial fluid, left ventricular (LV)systolic dysfunction, and pleural effusion, areoften missed by traditional physical examina-tion. It is conceivable that patients’ increas-ingly complex medical conditions,physicians’ declining physical examinationskills, and society’s expectation for higherstandards of medical care are all leading toincreased utilization of POCUS for more accu-rate bedside assessments of patients.
POCUS can immediately narrow thedifferential diagnosis by building on clinicalinformation revealed by the history and phys-ical examination10,11 and refine clinical deci-sion making for further work-up andtreatment.12 Recent studies have found thatclinical management involving the early useof POCUS accurately guides diagnosis, signifi-cantly reduces physicians’ diagnostic uncer-tainty, and also changes management andresource utilization.13 From a patient perspec-tive, “very low” discomfort was reportedduring POCUS of the heart, lungs, and deepveins, and most patients agreed to be evalu-ated with POCUS in an emergency depart-ment.14 Additionally, use of POCUS in theemergency department has been reported toimprove patient satisfaction and short-termhealth care resource utilization.15-17
LITERATURE REVIEW AND CLINICALAPPLICATIONSPOCUS can be helpful in a variety of commonclinical conditions by quickly identifyingabnormalities that may not be revealed by atraditional physical examination.2 For instance,consider the evaluation of a patient presentingwith unexplained dyspnea. In these patients,POCUS of the lungs can rapidly detect pleuraleffusions, pulmonary edema (B lines, a typeof comet tail artifact),18 pneumonia (consolida-tion with dynamic air bronchograms),19 orpneumothorax (absence of pleural sliding andpresence of a lung point sign).20
Other conditions readily detected withPOCUS include abdominal aortic aneu-rysms,21 deep venous thromboses,22 and peri-toneal free fluid.23 Central venous pressurecan be estimated by assessing the inferiorvena cava (IVC) or internal jugular vein sizeand collapsibility.24 Focused cardiac
Mayo Clin Proc. n December 2016;91(
ultrasonography can expeditiously assessglobal LV and right ventricular function anddetect the presence of a pericardial effusion.25
Other common POCUS applications includevascular, musculoskeletal, sinus, ocular, nerve,thyroid, gallbladder, liver, spleen, renal, testic-ular, and bladder imaging (Figure 1).
Several medical and surgical subspecialtieshave adopted POCUS protocols to rule in orrule out certain conditions using an algo-rithmic approach. Common protocols includeBLUE (Bedside Lung Ultrasound in Emer-gency) for acute respiratory failure,26 FAST(Focused Assessment with Sonography inTrauma) for peritoneal free fluid,27 RUSH(Rapid Ultrasound for Shock and Hypoten-sion) for shock,28,29 and CLUE (Cardiovascu-lar Limited Ultrasound Examination) for heartfailure.30 These protocols offer a logicalPOCUS workflow for specific clinical sce-narios and provide a foundation to integratePOCUS findings into clinical decision making.
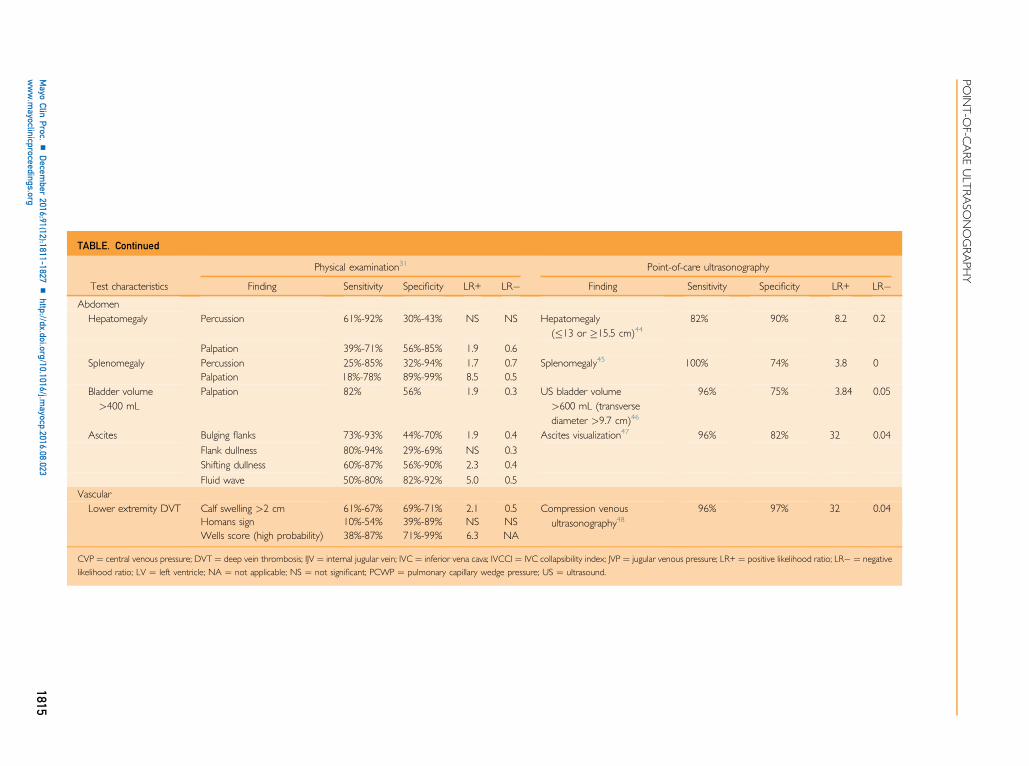
POCUS is not simply a diagnostic algorithmbut rather a tool used by a skilled clinician at thebedside to guide clinical decisionmaking in realtime. Although almost any diagnostic evalua-tion can be aided by POCUS (Figure 1, Table),we will describe 2 common patient scenariosto highlight the impact of POCUS on efficiency,diagnostic accuracy, resource utilization, radia-tion exposure, and patient satisfaction.
CASE 1A 41-year-old man with hypertension, type 2diabetes mellitus, and asthma presented to theoutpatient clinic with worsening shortness ofbreath. The shortness of breath had begunabruptly while the patient was at work in a cab-inet woodworking shop. He had been evaluatedin an urgent care clinic 1 week before presenta-tion and treated with a short course of cortico-steroids and inhaled albuterol. His symptomsimproved initially but subsequently worsened.He reported frequent ankle swelling that hadrecently increased. A review of systems revealedloud snoring at night but no angina, orthopnea,paroxysmal nocturnal dyspnea, recent travel/immobilization, or infectious symptoms.
Traditional Physical ExaminationTraditional physical examination revealed thefollowing:
12):1811-1827 n http://dx.doi.org/10.1016/j.mayocp.2016.08.023www.mayoclinicproceedings.org
d Vital signs: Temperature, 36.2�C; pulse rate,90 beats/min; blood pressure, 128/85 mmHg; respiratory rate, 15 breaths/min; oxygensaturation, 95%; body mass index (calcu-lated as weight in kilograms divided byheight in meters squared), 31 kg/m2
d Head, ears, eyes, nose, and throat: Mildbilateral tenderness on percussion overmaxillary sinuses
d Pulmonary: Distant lung sounds, occasionalexpiratory wheezing bilaterally
Mayo Clin Proc. n December 2016;91(12):1811-1827 n http://dx.dowww.mayoclinicproceedings.org
d Cardiovascular: Distant heart sounds, nomurmur, neck veins not visible, mild bilat-eral edema of the ankles
d Abdomen: Protuberant, no palpable hepa-tosplenomegaly, no shifting dullness or fluidwave
d Skin: No abnormalities
Differential Diagnosis. On physical examina-tion, the differential diagnosis includes asthmaexacerbation, congestive heart failure, allergic
pneumonitis secondary to wood dust, pneu-monia, and pulmonary hypertension due toobstructive sleep apnea.
Plan With Traditional Physical ExaminationAlone. For patients with the aforementionedfindings on traditional physical examination,the following steps would be taken:
d Outpatient chest radiographyd Addition of inhaled glucocorticoid andcontinuation of albuterol for asthma
d Follow-up in 3 to 5 days if no improvementnoted
POCUS-Assisted Physical ExaminationPOCUS-assisted physical examinationrevealed the following:
d Head, ears, eyes, nose, and throat: No fluidlevel present in either maxillary sinus(Figure 2, A)
FIGURE 2. Case 1. Point-of-care ultrasonographcompared with abnormal, fluid-filled maxillary sinus ((right) and abnormal lung with pulmonary edright diaphragm with pleural effusion and dilated inview of the heart showing thickened left ventricuaorta (Ao).
Mayo Clin Proc. n December 2016;91(
d Pulmonary: Lung sliding bilaterallythroughout (Supplemental Video 1, availableonline at http://www.mayoclinicproceedings.org), multiple bilateral B lines (�3 per inter-space) in upper and lower lung fields(Figure 2, B; Supplemental Video 1), smallbilateral pleural effusions with associatedatelectasis (Figure 2, C; SupplementalVideo 2, available online at http://www.mayoclinicproceedings.org)
d Cardiovascular: Measurement of IVC was2.8 cm with less than 50% collapse on inspi-ration (Figure 2, C; Supplemental Video 2),no pericardial effusion, LV wall thickness of2 cm septal and 1.9 cm posterior, LV sys-tolic function severely reduced (Figure 2,D; Supplemental Video 3, available onlineat http://www.mayoclinicproceedings.org),no major mitral or tricuspid regurgitation,right ventricle difficult to view but doesnot appear substantially enlarged
ic images. A, Normal maxillary sinus (left)right). B, Pulmonary images showing normal lungema (left). C, View at the level of theferior vena cava (IVC). D, Parasternal long-axislar (LV) walls, left atrium (LA), and ascending
12):1811-1827 n http://dx.doi.org/10.1016/j.mayocp.2016.08.023www.mayoclinicproceedings.org
d Abdomen: Liver span and spleen sizenormal, no ascites visible
Differential Diagnosis. Based on POCUSexamination findings of a plethoric IVC, bilat-eral B lines, pleural effusions, and severelyreduced LV systolic function, the primary diag-nosis in the differential is acute decompensatedsystolic heart failure with pulmonary edema andelevated central venous pressure. Asthma exac-erbation, allergic pneumonitis, pneumonia,and pulmonary hypertension with obstructivesleep apnea are highly unlikely based on thePOCUS examination findings.
Plan With POCUS-Assisted Physical Exam-ination. For patients with the aforementionedfindings on POCUS-assisted physical exami-nation, the following steps would be taken:
d Admit to hospital from clinicd Comprehensive transthoracic echocardiog-raphy to evaluate LV function and pericar-dial effusion the next morning
d Cardiac ischemic work-upd Intravenous diuresis
DiscussionThe identification of elevated central venouspressure (IVC dilation with minimalcollapse),38,49-53 pulmonary edema (bilateralinterstitial syndrome B lines),54-56 and pleuraleffusions combined with an unanticipatedreduction in LV systolic function25,41,57-64
dramatically changed this patient’s evaluationand management. During his inpatient work-up, isolated LV noncompaction was diagnosedafter cardiac magnetic resonance imaging andcoronary angiography.
Shortness of breath entails a broad differen-tial, and the addition of POCUS in real time atthe bedside can tremendously help mitigatedelay in appropriate testing and diag-nosis.26,33,34,65-74 The presence of B lines onthe initial pulmonary ultrasonography in thispatient focuses the differential on heart failure,pneumonia, interstitial lung disease, and poten-tially pulmonary embolism.26,55,56,74-76 Thedistribution of B lines is helpful in further nar-rowing the differential diagnosis.26 The presenceof bilateral diffuse B lines makes cardiogenicpulmonary edema, viral pneumonia, and other
Mayo Clin Proc. n December 2016;91(12):1811-1827 n http://dx.dowww.mayoclinicproceedings.org
causes of diffuse interstitial lung abnormalitiesmost likely. The differential diagnosis is furthernarrowed by focused cardiac ultrasonographyto assess LV systolic function57,58,60,77 and anIVC examination to estimate the central venouspressure.78 In the absence of cardiac findingssuggestive of cardiogenic pulmonary edema, afocused work-up or empirical treatment ofpneumonia would have ensued.
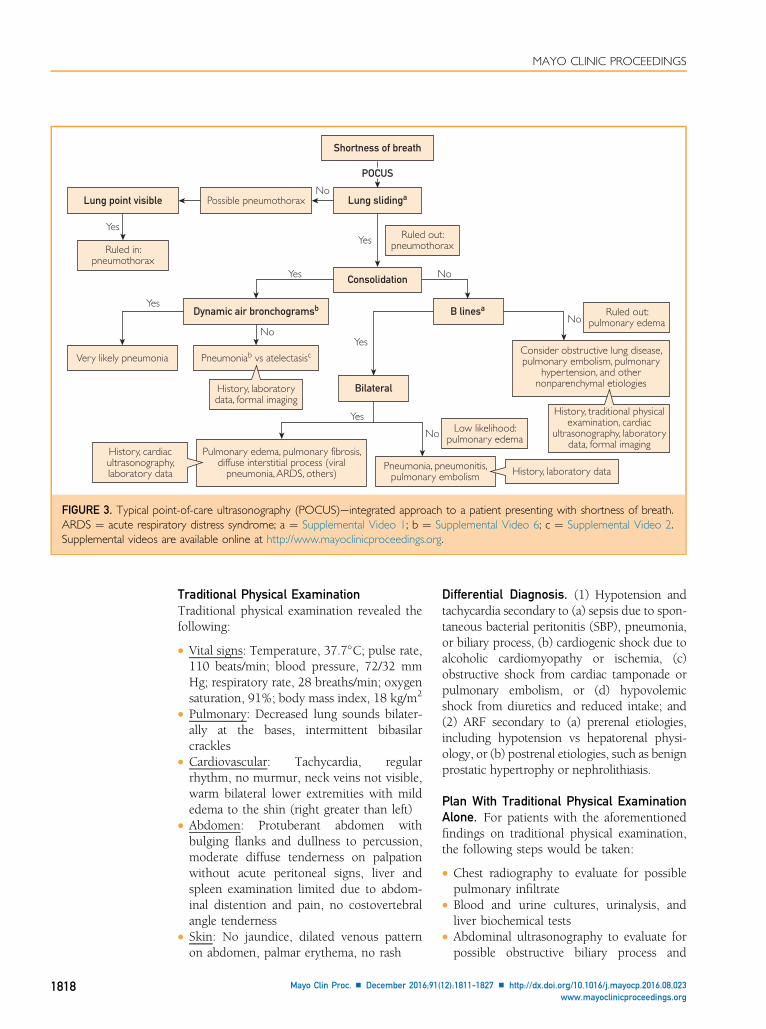
The following workflow may be employed.(1) The lack of B lines on pulmonary ultraso-nography rules out dyspnea from hydrostaticcardiogenic pulmonary edema.26,54 (2) Thelack of consolidation or B lines reduces thelikelihood of pneumonia considerably; in apatient with a low pretest probability of pneu-monia, the diagnosis can be ruled out (notethat although the sensitivity of POCUS forpneumonia is high in critically ill patients,central pneumonia can be missed, especiallyin less severe cases frequently seen in out-patient presentations).19,26,34,66,70,71,74,79-81
(3) The differential diagnosis now includesobstructive lung disease and pulmonaryvascular disease that can be difficult to distin-guish with basic POCUS applica-tions.19,26,34,66,70,71,74,79-81 (4) Auscultationat this point may be valuable if findings ofobstructive lung disease, such as decreasedbreath sounds and wheezing, are present.(5) If findings of obstructive lung disease arenot present, a combination of venous andfocused cardiac ultrasonography can furthernarrow the differential diagnosis to improveefficiency of further work-up (Figure 3).
CASE 2A 69-year-old man with cirrhosis secondary toalcohol abuse, benign prostatic hypertrophy,type 2 diabetes mellitus, and nephrolithiasiswas admitted to the hospital with lethargy,confusion, increased abdominal distention,and a subjective fever over the preceding 24hours. He reported minimal oral intake anda mild productive cough for the past 2 weeks.A syncopal episode while getting out of bedprompted transport to the emergency depart-ment. Initial laboratory tests in the emergencydepartment revealed acute renal failure (ARF),leukocytosis, thrombocytopenia, and elevatedtroponin T level. Electrocardiography revealedsinus tachycardia with 1- to 2-mm lateralST-segment depression.
History, cardiacultrasonography,laboratory data History, laboratory data
History, traditional physicalexamination, cardiac
ultrasonography, laboratorydata, formal imaging
FIGURE 3. Typical point-of-care ultrasonography (POCUS)eintegrated approach to a patient presenting with shortness of breath.ARDS ¼ acute respiratory distress syndrome; a ¼ Supplemental Video 1; b ¼ Supplemental Video 6; c ¼ Supplemental Video 2.Supplemental videos are available online at http://www.mayoclinicproceedings.org.
MAYO CLINIC PROCEEDINGS
1818
Traditional Physical ExaminationTraditional physical examination revealed thefollowing:
d Vital signs: Temperature, 37.7�C; pulse rate,110 beats/min; blood pressure, 72/32 mmHg; respiratory rate, 28 breaths/min; oxygensaturation, 91%; body mass index, 18 kg/m2
d Pulmonary: Decreased lung sounds bilater-ally at the bases, intermittent bibasilarcrackles
d Cardiovascular: Tachycardia, regularrhythm, no murmur, neck veins not visible,warm bilateral lower extremities with mildedema to the shin (right greater than left)
d Abdomen: Protuberant abdomen withbulging flanks and dullness to percussion,moderate diffuse tenderness on palpationwithout acute peritoneal signs, liver andspleen examination limited due to abdom-inal distention and pain, no costovertebralangle tenderness
d Skin: No jaundice, dilated venous patternon abdomen, palmar erythema, no rash
Mayo Clin Proc. n December 2016;91(
Differential Diagnosis. (1) Hypotension andtachycardia secondary to (a) sepsis due to spon-taneous bacterial peritonitis (SBP), pneumonia,or biliary process, (b) cardiogenic shock due toalcoholic cardiomyopathy or ischemia, (c)obstructive shock from cardiac tamponade orpulmonary embolism, or (d) hypovolemicshock from diuretics and reduced intake; and(2) ARF secondary to (a) prerenal etiologies,including hypotension vs hepatorenal physi-ology, or (b) postrenal etiologies, such as benignprostatic hypertrophy or nephrolithiasis.
Plan With Traditional Physical ExaminationAlone. For patients with the aforementionedfindings on traditional physical examination,the following steps would be taken:
d Chest radiography to evaluate for possiblepulmonary infiltrate
d Blood and urine cultures, urinalysis, andliver biochemical tests
d Abdominal ultrasonography to evaluate forpossible obstructive biliary process and
12):1811-1827 n http://dx.doi.org/10.1016/j.mayocp.2016.08.023www.mayoclinicproceedings.org
ascites, followed by diagnostic paracentesisperformed in the radiology department
d Central venous catheter (CVC) placementfor central venous pressure monitoring,fluid resuscitation, and possible vasopressorsupport
d Initiation of empirical broad-spectrum anti-biotics to cover potential pulmonary andabdominal sources of sepsis
d Comprehensive transthoracic echocardiog-raphy to evaluate LV function and pericar-dial effusion the next morning
d Renal ultrasonography in the radiologydepartment to evaluate for hydronephrosis
d Bladder scan or empirical urinary catheterplacement to measure postvoid residualurine volume
d Serial laboratory measurements of lactateand troponin levels with fluid resuscitation
POCUS-Assisted Physical ExaminationPOCUS-assisted physical examinationrevealed the following:
d Pulmonary: Bilateral lung sliding notedthroughout, bilateral elevated hemidia-phragm to tip of scapula with small bilateralpleural effusions and few B lines in bothdependent lung fields associated with mildbilateral atelectasis
d Cardiovascular: Focused cardiac ultrasonogra-phy revealed trace pericardial effusion, normalright ventricle size with increased contractility,hyperdynamic LVwith “kissing” endocardium(Supplemental Video 3, available online athttp://www.mayoclinicproceedings.org), IVCless than 1 cm in diameter with 100% collapseexcept during expiration (SupplementalVideo 4, available online at http://www.mayoclinicproceedings.org). Lower extremityvascular assessment revealed completecompression of saphenous veins, common/deep/superficial femoral veins, and poplitealveins bilaterally
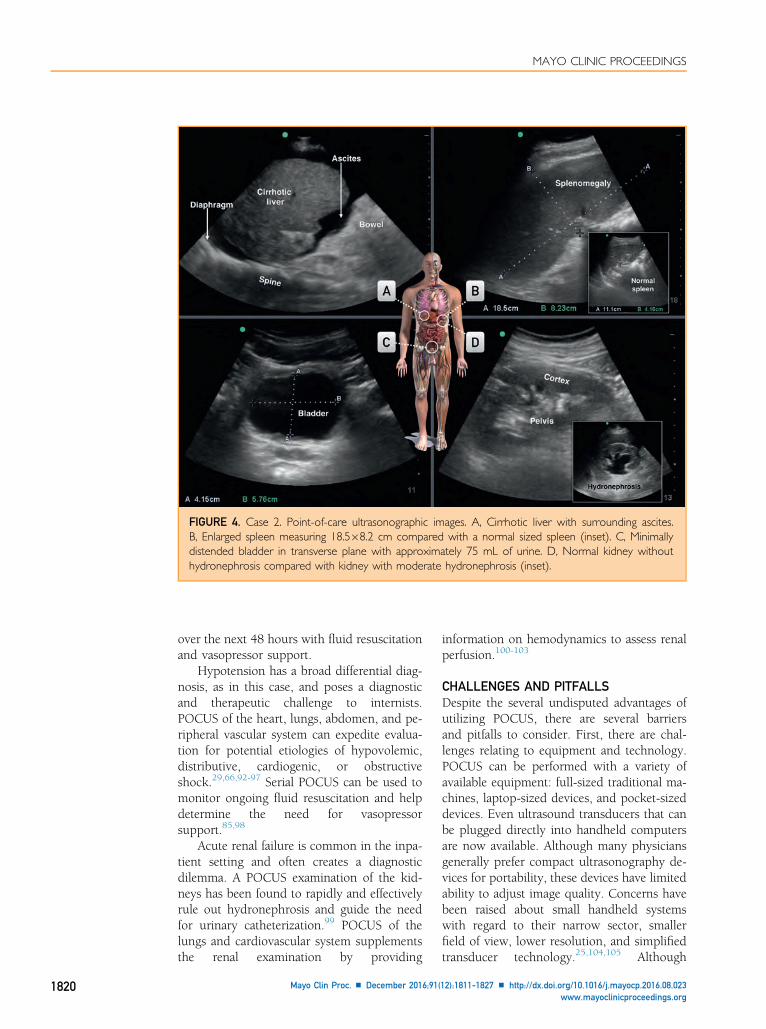
d Abdomen: Moderate ascites throughout(Figure 4, A; Supplemental Video 5,available online at http://www.mayoclinicproceedings.org), small liver (8-cm midcla-vicular span) with scalloped cortex, enlargedspleen (19 cm in long axis and 8 cm in shortaxis) (Figure 4, B), minimally distendedbladder (Figure 4, C), and no hydronephro-sis (Figure 4, D). Gallbladder was noted to
Mayo Clin Proc. n December 2016;91(12):1811-1827 n http://dx.dowww.mayoclinicproceedings.org
be normal with no sonographic Murphysign
Differential Diagnosis. Based on the POCUSfindings of a collapsed IVC, hyperdynamicLV, ascites, splenomegaly, and cirrhotic liver,the differential diagnosis was narrowed tohypovolemia secondary to sepsis syndromedue to SBP or possible biliary process andARF due to a prerenal/renal etiology.
Plan With POCUS-Assisted Physical Exam-ination. For patients with the aforementionedfindings on POCUS-assisted physical exami-nation, the following steps would be taken:
d Bedside paracentesis with ultrasound guid-ance to evaluate for SBP (SupplementalVideo 5)
d Immediate volume resuscitationd Serial bedside POCUS of LV, IVC, and lungsduring fluid resuscitation to monitor forearly signs of pulmonary edema with lowthreshold for transfer to critical care unitfor vasopressor and fluid support
d Empirical broad-spectrum antibiotics tocover possible SBP and biliary source ofsepsis
d Blood and urine cultures, urinalysis, andliver biochemical tests
d Consider right upper quadrant ultrasonog-raphy for possible obstructive biliary process
d Serial laboratory testing including lactateand troponin levels with fluidresuscitation
d Comprehensive transthoracic echocardio-graphy to evaluate LV function and pericar-dial effusion the next morning
DiscussionBedside ultrasound-guided paracentesis hasbeen reported to be safe and effective whenperformed by nonradiologists82-84 and canquickly identify the source of sepsis. Volumeresuscitation guided by POCUS includesdiscontinuation of intravenous fluids whenthe POCUS examination reveals early signsof pulmonary edema74,85 or when minimalchange in stroke volume occurs with a passiveleg raise.86-91 This patient was transitioned tothe intensive care unit for initiation of earlyvasopressor support. The ARF normalized
FIGURE 4. Case 2. Point-of-care ultrasonographic images. A, Cirrhotic liver with surrounding ascites.B, Enlarged spleen measuring 18.5�8.2 cm compared with a normal sized spleen (inset). C, Minimallydistended bladder in transverse plane with approximately 75 mL of urine. D, Normal kidney withouthydronephrosis compared with kidney with moderate hydronephrosis (inset).
MAYO CLINIC PROCEEDINGS
1820
over the next 48 hours with fluid resuscitationand vasopressor support.
Hypotension has a broad differential diag-nosis, as in this case, and poses a diagnosticand therapeutic challenge to internists.POCUS of the heart, lungs, abdomen, and pe-ripheral vascular system can expedite evalua-tion for potential etiologies of hypovolemic,distributive, cardiogenic, or obstructiveshock.29,66,92-97 Serial POCUS can be used tomonitor ongoing fluid resuscitation and helpdetermine the need for vasopressorsupport.85,98
Acute renal failure is common in the inpa-tient setting and often creates a diagnosticdilemma. A POCUS examination of the kid-neys has been found to rapidly and effectivelyrule out hydronephrosis and guide the needfor urinary catheterization.99 POCUS of thelungs and cardiovascular system supplementsthe renal examination by providing
Mayo Clin Proc. n December 2016;91(
information on hemodynamics to assess renalperfusion.100-103
CHALLENGES AND PITFALLSDespite the several undisputed advantages ofutilizing POCUS, there are several barriersand pitfalls to consider. First, there are chal-lenges relating to equipment and technology.POCUS can be performed with a variety ofavailable equipment: full-sized traditional ma-chines, laptop-sized devices, and pocket-sizeddevices. Even ultrasound transducers that canbe plugged directly into handheld computersare now available. Although many physiciansgenerally prefer compact ultrasonography de-vices for portability, these devices have limitedability to adjust image quality. Concerns havebeen raised about small handheld systemswith regard to their narrow sector, smallerfield of view, lower resolution, and simplifiedtransducer technology.25,104,105 Although
12):1811-1827 n http://dx.doi.org/10.1016/j.mayocp.2016.08.023www.mayoclinicproceedings.org
studies have documented that small ultraso-nography devices can be used to answerfocused questions,18,61,106-115 operators mustbe aware of their limitations.
From an operator and training perspective,studies have found that the utility of a POCUSexamination depends on the experience andskills of the operator.42,48,116-120 Operatortraining is crucial for POCUS to be utilizedcorrectly in patient care, and studies haverevealed that barriers to POCUS adoptioninclude insufficient faculty training, high costof ultrasonography machines, and timerequired to train physicians.45,121 The relativelyhigh level of operator dependency comparedwith other diagnostic testing is reasonably ex-pected, given the multiple skills required toperform a POCUS examination. First, a POCUSexamination begins with formulation of a spe-cific clinical question and a decision to utilizePOCUS to answer this question.122 Next, acqui-sition of images requires knowledge of sono-graphic windows, ultrasound physics, andhand-eye-brain coordination to manipulatethe transducer to optimize image quality.122
Interpretation of POCUS images requires skillsthat are independent from physical examinationskills, and operators must recognize artifactsthat are encountered during image acquisitionand interpretation.122 Most importantly,POCUS findings must be interpreted and inte-grated with other clinical data to effectivelyguide clinical decision making.122 Failureduring any step of this multistep process mayundermine the true value of using POCUS.
The skills needed to perform POCUS ex-aminations have not been uniformly taughtin undergraduate or graduate medical educa-tion. Although a movement to integratePOCUS education into medical schools orinternal medicine residency programs hasbeen gaining momentum over the pastdecade,43,121,123-129 there is no consensus onthe training required to reach adequatePOCUS competency levels in general internalmedicine.25,104,110,111,130-133 It is generallyagreed that training must include basic knowl-edge of ultrasound physics and supervisedimage acquisition and interpretation prac-tice.25,104,110,111,130-133
Other potential challenges include theavailability of templates for documentation,electronic storage for image archiving, and
Mayo Clin Proc. n December 2016;91(12):1811-1827 n http://dx.dowww.mayoclinicproceedings.org
policies and procedures for quality assuranceand billing. Emergency medicine societieshave addressed these issues and assistedphysicians in understanding correct andcompliant coding for the past 2 de-cades.37,39,40 In terms of billing, POCUS canpotentially influence the evaluation and man-agement code by affecting the complexity ofmedical decision making (Current ProceduralTerminology).112-115 Some believe that reim-bursement is essential to cover the substantialcost of POCUS education and equipment pur-chasing and maintenance.112-115 Conversely,others view POCUS as an extension of thephysical examination, which raises concernsthat a heavy focus on billing may block theroutine use of POCUS.116-118 Future reim-bursement systems that capture an “episodeof care,” also known as “bundling,” will likelychange the perspectives on POCUS billing,documentation, and image archiving.112,117
As the workflow for POCUS in internal medi-cine matures, medical practices will berequired to provide the administrative infra-structure needed to meet these evolving stan-dards of care for use of POCUS.25,104,116
For effective integration of POCUS into clin-ical care, quality assurance is an importantconsideration. Although quality assurance hasbeen emphasized to avoid misinterpretation ofimages, most malpractice cases related toPOCUS in emergency medicine have been dueto failure to perform a POCUS examination ina timely manner, rather than misinterpretationor misdiagnosis with the use of POCUS.76 Theextent to which quality assurance will be neededin internal medicine and other specialties is yetto be determined because increased legal risksmay occur with either failure to use POCUS ormisinterpretation of POCUS images.
FUTURE RESEARCHEarly POCUS research focused on diagnosticaccuracy to establish that health care profes-sionals with focused training in ultrasonogra-phy can acquire and interpret imagesaccurately. The diagnostic accuracy of front-line physicians performing POCUS examina-tions has been compared with imagingacquired by full-time sonographers and inter-preted by imaging specialists, primarily radiol-ogists or cardiologists. Several publishedstudies have proven that POCUS has
diagnostic accuracy similar to that of criterionstandard imaging studies for specific findings,such as pneumothorax,67,119 pericardial effu-sion,42,120 or lower extremity deep venousthrombosis.48 However, few studies havecompared the diagnostic accuracy of POCUSvs the traditional diagnostic approach usinghistory and physical examination. Interest-ingly, these studies have clearly confirmedthe superiority of POCUS. For instance, halfas many major cardiac findings were missedwhen a cardiac physical examination per-formed by experienced cardiologists wassupplemented with a focused cardiac ultraso-nographic examination.121 Although a fairercomparison may be to compare the diagnosticaccuracy of POCUS to that of physical exami-nation, rather than criterion standard imagingstudies, few comparative studies of internist-performed physical examinations, with orwithout the addition of POCUS, have beenpublished.45
During the past 15 years, POCUS researchhas shifted focus from diagnostic accuracy todemonstration of improved health outcomes.Use of POCUS to guide bedside procedureshas been reported to reduce procedure-related complications, including arterial punc-tures during central venous catheterization,134
postthoracentsis pneumothorax, and postpar-acentesis bleeding complications, along withthe costs and lengths of stay associated withthese complications.123,124 However, few ran-domized trials have been published, and apaucity of data exists supporting the routineuse of POCUS for diagnostic evalua-tions.15,69,77,125-127 Only one randomized trialwith internal medicineetrained physicians hasbeen published comparing routine focusedcardiac ultrasonography vs standard care inhospitalized general medicine patients. Thisstudy found a potential reduction in lengthof stay with the use of POCUS in the cohortof patients with heart failure.43 Thus, compar-ative studies evaluating the clinical and healthservices outcomes of usual care with andwithout the routine use of POCUS by inter-nists for different conditions are needed.
Another interesting facet of POCUSresearch is whether the higher-priority focusis physician training or clinical outcomes. Afundamental question has yet to be answered:How do we effectively train health care
Mayo Clin Proc. n December 2016;91(
professionals, ranging from medical studentsto senior attending physicians, to utilizePOCUS? Experts generally agree that the useof POCUS requires basic knowledge of ultraso-nography, image acquisition and interpretationskills, and an understanding of integration ofPOCUS findings into clinical decision making.If we believe that the focus should be outcomesresearch rather than training, then we are rele-gated to performing studies with a few expertsperforming all POCUS examinations, whichmay be biased toward benefit because theexperts’ skill level is beyond what may beachievable by a physician with average POCUSskills. On the contrary, if we believe trainingshould be the focus, then medical institutions,including medical schools, hospitals, andhealth care systems, will have to invest intraining physicians in basic POCUS applica-tions before large effectiveness trials can beundertaken to evaluate the impact of POCUSon clinical outcomes. As this debate hascontinued, medical schools have begun toinvest heavily in integrating POCUS traininginto clinical skills education, and positive stu-dent reviews and publicity continue to drivethis integration in medical school curricula.Meanwhile, practicing internists are feelinggrowing pressures to acquire basic POCUSskills because their trainees may have moreadvanced POCUS skills than they do.
From a health care system perspective, thefield of POCUS is ripe for health servicesresearch because an increasing number ofPOCUS applications are recommended byevidence-based guidelines. For example,consider the use of ultrasound guidance toplace CVCs. Since the early 2000s, ultrasoundguidance for placement of CVCs has beenrecommended by national patient safetyand quality organizations on the basis of severalrandomized trials and meta-analyses128,129,135;however, the use of ultrasound guidance toinsert CVCs has not been universally adoptedin clinical practice. Investigations usingmethods from implementation science mayreveal barriers to adoption of POCUS use forCVC insertion. Lessons learned from studyingthis implementation gap may guide futureimplementation of POCUS use within the prac-tice of internal medicine.
Certain POCUS applications with well-proven benefits, such as use of ultrasound
12):1811-1827 n http://dx.doi.org/10.1016/j.mayocp.2016.08.023www.mayoclinicproceedings.org
guidance for insertion of CVCs, are primed forsystem-wide implementation. However, adiversified approach to POCUS research isneeded in view of the varying levels of evi-dence supporting different POCUS applica-tions. For known POCUS applications thatare not yet the standard of care, such as eval-uation of acute dyspnea with POCUS, addi-tional clinical outcomes and health servicesresearch will likely be needed to confirmbenefit and assess the effect on health carecosts, length of stay, and patient experience.For other newer, novel POCUS applications,such as elastography and 3-dimensional ultra-sound imaging, diagnostic accuracy studiesare needed to establish their role in clinicalmedicine. Underlying this broad spectrum ofclinical research needs is the need for educa-tional research to help us understand how toeffectively train physicians to use POCUS.Educational research will help us define thescope of training, identify resources needed(equipment, faculty/staff time), and set realisticgoals for training programs.
CONCLUSIONEmpowering internists to assess patients usingPOCUS is an inevitable change in the practiceof internal medicine that has already begun todisseminate. The ability to visualize patho-physiologic features in real time using POCUScan provide expedited, high-quality, safe, andcost-conscious patient care. As new clinicaland educational research emerges, our under-standing of how to integrate POCUS into clin-ical practice will improve, and routine use ofPOCUS in clinical practice will establish newstandards of care.
SUPPLEMENTAL ONLINE MATERIALSupplemental material can be found online athttp://www.mayoclinicproceedings.org. Sup-plemental material attached to journal articleshas not been edited, and the authors takeresponsibility for the accuracy of all data.
Abbreviations and Acronyms: ARF = acute renal failure;CVC = central venous catheter; IVC = inferior vena cava;LV = left ventricular; POCUS = point-of-care ultrasonog-raphy; SBP = spontaneous bacterial peritonitis
Correspondence: Address to Anjali Bhagra, MBBS, Divisionof General Internal Medicine, Mayo Clinic, 200 First St SW,Rochester, MN 55905 ([email protected]).
Mayo Clin Proc. n December 2016;91(12):1811-1827 n http://dx.dowww.mayoclinicproceedings.org
REFERENCES1. Greaves K, Jeetley P, Hickman M, et al. The use of hand-
carried ultrasound in the hospital settingda cost-effectiveanalysis. J Am Soc Echocardiogr. 2005;18(6):620-625.
2. Sekiguchi H. Tools of the trade: point-of-care ultrasonographyas a stethoscope. Semin Respir Crit Care Med. 2016;37(1):68-87.
3. Mulvagh SL, Bhagra A, Nelson BP, Narula J. Handheld ultra-sound devices and the training conundrum: how to get to“seeing is believing” [editorial]. J Am Soc Echocardiogr. 2014;27(3):310-313.
4. Liebo MJ, Israel RL, Lillie EO, Smith MR, Rubenson DS,Topol EJ. Is pocket mobile echocardiography the next-generation stethoscope? a cross-sectional comparison ofrapidly acquired images with standard transthoracic echocardi-ography. Ann Intern Med. 2011;155(1):33-38.
5. Mangione S, Nieman LZ. Cardiac auscultatory skills of internalmedicine and family practice trainees: a comparison of diag-nostic proficiency [published correction appears in JAMA.1998;279(18):1444]. JAMA. 1997;278(9):717-722.
6. Conn RD, O’Keefe JH. Cardiac physical diagnosis in the digitalage: an important but increasingly neglected skill (from stetho-scopes to microchips). Am J Cardiol. 2009;104(4):590-595.
7. Jauhar S. The demise of the physical exam. N Engl J Med. 2006;354(6):548-551.
8. Kugler J, Verghese A. The physical exam and other forms offiction [editorial]. J Gen Intern Med. 2010;25(8):756-757.
9. Verghese A, Brady E, Kapur CC, Horwitz RI. The bedside eval-uation: ritual and reason. Ann Intern Med. 2011;155(8):550-553.
10. Cardim N, Fernandez Golfin C, Ferreira D, et al. Usefulness ofa new miniaturized echocardiographic system in outpatientcardiology consultations as an extension of physical examina-tion. J Am Soc Echocardiogr. 2011;24(2):117-124.
11. Beaton A, Aliku T, Okello E, et al. The utility of handheldechocardiography for early diagnosis of rheumatic heart dis-ease. J Am Soc Echocardiogr. 2014;27(1):42-49.
12. Gorcsan J III, Pandey P, Sade LE. Influence of hand-carriedultrasound on bedside patient treatment decisions for consul-tative cardiology. J Am Soc Echocardiogr. 2004;17(1):50-55.
13. Shokoohi H, Boniface KS, Pourmand A, et al. Bedside ultra-sound reduces diagnostic uncertainty and guides resuscitationin patients with undifferentiated hypotension. Crit Care Med.2015;43(12):2562-2569.
14. Laursen CB, Sloth E, Lassen AT, et al. Does point-of-careultrasonography cause discomfort in patients admitted withrespiratory symptoms? Scand J Trauma Resusc Emerg Med.2015;23:46.
15. Lindelius A, Törngren S, Nilsson L, Pettersson H, Adami J.Randomized clinical trial of bedside ultrasound among patientswith abdominal pain in the emergency department: impact onpatient satisfaction and health care consumption. Scand JTrauma Resusc Emerg Med. 2009;17:60.
16. Howard ZD, Noble VE, Marill KA, et al. Bedside ultrasoundmaximizes patient satisfaction. J Emerg Med. 2014;46(1):46-53.
17. Durston W, Carl ML, Guerra W. Patient satisfaction and diag-nostic accuracy with ultrasound by emergency physicians. Am JEmerg Med. 1999;17(7):642-646.
18. Bedetti G, Gargani L, Corbisiero A, Frassi F, Poggianti E,Mottola G. Evaluation of ultrasound lung comets by hand-held echocardiography. Cardiovasc Ultrasound. 2006;4:34.
19. Lichtenstein D, Mezière G, Seitz J. The dynamic air broncho-gram: a lung ultrasound sign of alveolar consolidation rulingout atelectasis. Chest. 2009;135(6):1421-1425.
20. Lichtenstein DA, Menu Y. A bedside ultrasound sign ruling outpneumothorax in the critically ill: lung sliding. Chest. 1995;108(5):1345-1348.
21. Lin PH, Bush RL, McCoy SA, et al. A prospective study of ahand-held ultrasound device in abdominal aortic aneurysmevaluation. Am J Surg. 2003;186(5):455-459.
22. Frazee BW, Snoey ER, Levitt A. Emergency Departmentcompression ultrasound to diagnose proximal deep veinthrombosis. J Emerg Med. 2001;20(2):107-112.
23. Kirkpatrick AW, Simons RK, Brown R, Nicolaou S,Dulchavsky S. The hand-held FAST: experience with hand-held trauma sonography in a level-I urban trauma center.Injury. 2002;33(4):303-308.
24. Zengin S, Al B, Genc S, et al. Role of inferior vena cava andright ventricular diameter in assessment of volume status: acomparative study; ultrasound and hypovolemia. Am J EmergMed. 2013;31(5):763-767.
25. Spencer KT, Kimura BJ, Korcarz CE, Pellikka PA, Rahko PS,Siegel RJ. Focused cardiac ultrasound: recommendationsfrom the American Society of Echocardiography. J Am SocEchocardiogr. 2013;26(6):567-581.
26. Lichtenstein DA, Mezière GA. Relevance of lung ultrasound inthe diagnosis of acute respiratory failure: the BLUE protocol[published correction appears in Chest. 2013;144(2):721].Chest. 2008;134(1):117-125.
27. Scalea TM, Rodriguez A, Chiu WC, et al. Focused Assess-ment with Sonography for Trauma (FAST): results from aninternational consensus conference. J Trauma. 1999;46(3):466-472.
28. Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam:Rapid Ultrasound in SHock in the evaluation of the criticallylll. Emerg Med Clin North Am. 2010;28(1):29-56, vii.
29. Weingart SD, Duque D, Nelson B. The RUSH exam: RapidUltrasound for Shock and Hypotension. EMCrit website.http://emcrit.org/rush-exam/original-rush-article/. AccessedJune 2, 2016.
30. Kimura BJ, Shaw DJ, Agan DL, Amundson SA, Ping AC,DeMaria AN. Value of a cardiovascular limited ultrasound ex-amination using a hand-carried ultrasound device on clinicalmanagement in an outpatient medical clinic. Am J Cardiol.2007;100(2):321-325.
31. McGee S. Evidence-Based Physical Diagnosis. 3rd ed. Philadel-phia, PA: Elsevier Health Sciences; 2012.
32. Grimberg A, Shigueoka DC, Atallah AN, Ajzen S,Iared W. Diagnostic accuracy of sonography for pleuraleffusion: systematic review. Sao Paulo Med J. 2010;128(2):90-95.
33. Al Deeb M, Barbic S, Featherstone R, Dankoff J, Barbic D.Point-of-care ultrasonography for the diagnosis of acutecardiogenic pulmonary edema in patients presenting withacute dyspnea: a systematic review and meta-analysis. AcadEmerg Med. 2014;21(8):843-852.
34. Chavez MA, Shams N, Ellington LE, et al. Lung ultrasound forthe diagnosis of pneumonia in adults: a systematic review andmeta-analysis. Respir Res. 2014;15:50.
35. Ye X, Xiao H, Chen B, Zhang S. Accuracy of lung ultrasonog-raphy versus chest radiography for the diagnosis of adultcommunity-acquired pneumonia: review of the literatureand meta-analysis. PLoS One. 2015;10(6):e0130066.
36. Blair JE, Brennan JM, Goonewardena SN, Shah D, Vasaiwala S,Spencer KT. Usefulness of hand-carried ultrasound to predictelevated left ventricular filling pressure. Am J Cardiol. 2009;103(2):246-247.
37. Brennan JM, Blair JE, Goonewardena S, et al. Reappraisal of theuse of inferior vena cava for estimating right atrial pressure.J Am Soc Echocardiogr. 2007;20(7):857-861.
38. Kircher BJ, Himelman RB, Schiller NB. Noninvasive estimationof right atrial pressure from the inspiratory collapse of theinferior vena cava. Am J Cardiol. 1990;66(4):493-496.
39. Prekker ME, Scott NL, Hart D, Sprenkle MD, Leatherman JW.Point-of-care ultrasound to estimate central venous pressure:a comparison of three techniques. Crit Care Med. 2013;41(3):833-841.
40. Keller AS, Melamed R, Malinchoc M, John R, Tierney DM,Gajic O. Diagnostic accuracy of a simple ultrasound mea-surement to estimate central venous pressure in
41. Johnson BK, Tierney DM, Rosborough TK, Harris KM,Newell MC. Internal medicine point-of-care ultrasound assess-ment of left ventricular function correlates with formal echo-cardiography. J Clin Ultrasound. 2016;44(2):92-99.
42. Lucas BP, Candotti C, Margeta B, et al. Diagnostic accuracy ofhospitalist-performed hand-carried ultrasound echocardiogra-phy after a brief training program. J Hosp Med. 2009;4(6):340-349.
43. Lucas BP, Candotti C, Margeta B, et al. Hand-carried echocar-diography by hospitalists: a randomized trial. Am J Med. 2011;124(8):766-774.
45. Olson AP, Trappey B, Wagner M, Newman M, Nixon LJ,Schnobrich D. Point-of-care ultrasonography improves thediagnosis of splenomegaly in hospitalized patients. Crit Ultra-sound J. 2015;7(1):13.
46. Daurat A, Choquet O, Bringuier S, Charbit J, Egan M,Capdevila X. Diagnosis of postoperative urinary retention us-ing a simplified ultrasound bladder measurement. AnesthAnalg. 2015;120(5):1033-1038.
47. Keil-Ríos D, Terrazas-Solís H, González-Garay A, Sánchez-Ávila JF, García-Juárez I. Pocket ultrasound device as acomplement to physical examination for ascites evaluationand guided paracentesis. Intern Emerg Med. 2016;11(3):461-466.
48. Pomero F, Dentali F, Borretta V, et al. Accuracy of emergencyphysician-performed ultrasonography in the diagnosis ofdeep-vein thrombosis: a systematic review and meta-analysis.Thromb Haemost. 2013;109(1):137-145.
49. Nagueh SF, Kopelen HA, Zoghbi WA. Relation of mean rightatrial pressure to echocardiographic and Doppler parametersof right atrial and right ventricular function. Circulation. 1996;93(6):1160-1169.
50. Rudski LG, Lai WW, Afilalo J, et al. Guidelines for the echo-cardiographic assessment of the right heart in adults: a reportfrom the American Society of Echocardiography; endorsed bythe European Association of Echocardiography, a registeredbranch of the European Society of Cardiology, and the Cana-dian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23(7):685-713.
51. Simonson JS, Schiller NB. Sonospirometry: a new method fornoninvasive estimation of mean right atrial pressure based ontwo-dimensional echographic measurements of the inferiorvena cava during measured inspiration. J Am Coll Cardiol.1988;11(3):557-564.
52. Yildirimturk O, Tayyareci Y, Erdim R, et al. Assessment of rightatrial pressure using echocardiography and correlation withcatheterization. J Clin Ultrasound. 2011;39(6):337-343.
53. Brennan JM, Blair JE, Goonewardena S, et al. A comparison bymedicine residents of physical examination versus hand-carried ultrasound for estimation of right atrial pressure. AmJ Cardiol. 2007;99(11):1614-1616.
54. Lichtenstein D, Mezière G. A lung ultrasound sign allowingbedside distinction between pulmonary edema and COPD:the comet-tail artifact. Intensive Care Med. 1998;24(12):1331-1334.
55. Lichtenstein DA, Mezière GA, Lagoueyte JF, Biderman P,Goldstein I, Gepner A. A-lines and B-lines: lung ultrasoundas a bedside tool for predicting pulmonary artery occlusionpressure in the critically ill. Chest. 2009;136(4):1014-1020.
57. Alexander JH, Peterson ED, Chen AY, Harding TM,Adams DB, Kisslo JA Jr. Feasibility of point-of-care echocardi-ography by internal medicine house staff. Am Heart J. 2004;147(3):476-481.
12):1811-1827 n http://dx.doi.org/10.1016/j.mayocp.2016.08.023www.mayoclinicproceedings.org
58. Croft LB, Duvall WL, Goldman ME. A pilot study of the clin-ical impact of hand-carried cardiac ultrasound in the medicalclinic. Echocardiography. 2006;23(6):439-446.
59. Kimura BJ, Gilcrease GW III, Showalter BK, Phan JN,Wolfson T. Diagnostic performance of a pocket-sized ultra-sound device for quick-look cardiac imaging. Am J EmergMed. 2012;30(1):32-36.
60. Kobal SL, Trento L, Baharami S, et al. Comparison ofeffectiveness of hand-carried ultrasound to bedside cardio-vascular physical examination. Am J Cardiol. 2005;96(7):1002-1006.
61. Melamed R, Sprenkle MD, Ulstad VK, Herzog CA,Leatherman JW. Assessment of left ventricular function byintensivists using hand-held echocardiography. Chest. 2009;135(6):1416-1420.
62. Mjølstad OC, Andersen GN, Dalen H, et al. Feasibility andreliability of point-of-care pocket-size echocardiography per-formed by medical residents. Eur Heart J Cardiovasc Imaging.2013;14(12):1195-1202.
63. Razi R, Estrada JR, Doll J, Spencer KT. Bedside hand-carriedultrasound by internal medicine residents versus traditionalclinical assessment for the identification of systolic dysfunctionin patients admitted with decompensated heart failure. J AmSoc Echocardiogr. 2011;24(12):1319-1324.
64. Vignon P, Dugard A, Abraham J, et al. Focused training forgoal-oriented hand-held echocardiography performed bynoncardiologist residents in the intensive care unit. IntensiveCare Med. 2007;33(10):1795-1799.
65. Blaivas M, Lyon M, Duggal S. A prospective comparison of su-pine chest radiography and bedside ultrasound for the diag-nosis of traumatic pneumothorax. Acad Emerg Med. 2005;12(9):844-849.
66. Cortellaro F, Colombo S, Coen D, Duca PG. Lung ultrasoundis an accurate diagnostic tool for the diagnosis of pneumoniain the emergency department. Emerg Med J. 2012;29(1):19-23.
67. Ding W, Shen Y, Yang J, He X, Zhang M. Diagnosis of pneu-mothorax by radiography and ultrasonography: a meta-analysis. Chest. 2011;140(4):859-866.
68. Gallard E, Redonnet JP, Bourcier JE, et al. Diagnostic perfor-mance of cardiopulmonary ultrasound performed by theemergency physician in the management of acute dyspnea.Am J Emerg Med. 2015;33(3):352-358.
69. Laursen CB, Sloth E, Lassen AT, et al. Point-of-care ultraso-nography in patients admitted with respiratory symptoms: asingle-blind, randomised controlled trial. Lancet Respir Med.2014;2(8):638-646.
70. Liu XL, Lian R, Tao YK, Gu CD, Zhang GQ. Lung ultrasonog-raphy: an effective way to diagnose community-acquiredpneumonia. Emerg Med J. 2015;32(6):433-438.
71. Nazerian P, Volpicelli G, Vanni S, et al. Accuracy of lung ultra-sound for the diagnosis of consolidations when compared tochest computed tomography. Am J Emerg Med. 2015;33(5):620-625.
72. Volpicelli G, Elbarbary M, Blaivas M, et al; InternationalLiaison Committee on Lung Ultrasound (ILC-LUS) for Inter-national Consensus Conference on Lung Ultrasound (ICC-LUS). International evidence-based recommendations forpoint-of-care lung ultrasound. Intensive Care Med. 2012;38(4):577-591.
73. Özkan B, Ünlüer EE, Akyol PY, et al. Stethoscope versuspoint-of-care ultrasound in the differential diagnosis of dys-pnea: a randomized trial. Eur J Emerg Med. 2015;22(6):440-443.
74. Lichtenstein D. Lung ultrasound in the critically ill. Curr OpinCrit Care. 2014;20(3):315-322.
75. Lichtenstein D, Karakitsos D. Integrating lung ultrasound in thehemodynamic evaluation of acute circulatory failure (the fluidadministration limited by lung sonography protocol). J CritCare. 2012;27(5):533.e11-533.e19.
Mayo Clin Proc. n December 2016;91(12):1811-1827 n http://dx.dowww.mayoclinicproceedings.org
76. Volpicelli G, Mussa A, Garofalo G, et al. Bedside lung ultra-sound in the assessment of alveolar-interstitial syndrome.Am J Emerg Med. 2006;24(6):689-696.
77. Andersen GN, Graven T, Skjetne K, et al. Diagnostic influenceof routine point-of-care pocket-size ultrasound examinationsperformed by medical residents. J Ultrasound Med. 2015;34(4):627-636.
78. Sekiguchi H, Schenck LA, Horie R, et al. Critical care ultraso-nography differentiates ARDS, pulmonary edema, and othercauses in the early course of acute hypoxemic respiratory fail-ure. Chest. 2015;148(4):912-918.
79. Blaivas M. Lung ultrasound in evaluation of pneumonia.J Ultrasound Med. 2012;31(6):823-826.
80. Mongodi S, Via G, Girard M, et al. Lung ultrasound for earlydiagnosis of ventilator-associated pneumonia. Chest. 2016;149(4):969-980.
81. Volpicelli G, Silva F, Radeos M. Real-time lung ultrasound forthe diagnosis of alveolar consolidation and interstitial syn-drome in the emergency department. Eur J Emerg Med.2010;17(2):63-72.
82. Ennis J, Schultz G, Perera P, Williams S, Gharahbaghian L,Mandavia D. Ultrasound for detection of ascites and for guid-ance of the paracentesis procedure: technique and review ofthe literature. Int J Clin Med. 2014;5(20):1277-1293.
83. Nazeer SR, Dewbre H, Miller AH. Ultrasound-assisted para-centesis performed by emergency physicians vs the traditionaltechnique: a prospective, randomized study. Am J Emerg Med.2005;23(3):363-367.
84. Sekiguchi H, Suzuki J, Daniels CE. Making paracentesis safer: aproposal for the use of bedside abdominal and vascular ultra-sonography to prevent a fatal complication. Chest. 2013;143(4):1136-1139.
85. Lichtenstein D. Fluid administration limited by lung sonogra-phy: the place of lung ultrasound in assessment of acute circu-latory failure (the FALLS-protocol). Expert Rev Respir Med.2012;6(2):155-162.
86. Broch O, Renner J, Gruenewald M, et al. Variation of leftventricular outflow tract velocity and global end-diastolicvolume index reliably predict fluid responsiveness in car-diac surgery patients. J Crit Care. 2012;27(3):325.e7-325.e13.
87. Charron C, Caille V, Jardin F, Vieillard-Baron A. Echocardio-graphic measurement of fluid responsiveness. Curr Opin CritCare. 2006;12(3):249-254.
88. Dinh VA, Ko HS, Rao R, et al. Measuring cardiac index with afocused cardiac ultrasound examination in the ED. Am J EmergMed. 2012;30(9):1845-1851.
89. Marik PE, Levitov A, Young A, Andrews L. The use of bio-reactance and carotid Doppler to determine volume respon-siveness and blood flow redistribution following passive legraising in hemodynamically unstable patients. Chest. 2013;143(2):364-370.
90. Monnet X, Rienzo M, Osman D, et al. Passive leg raisingpredicts fluid responsiveness in the critically ill. Crit CareMed. 2006;34(5):1402-1407.
91. Préau S, Saulnier F, Dewavrin F, Durocher A, Chagnon JL.Passive leg raising is predictive of fluid responsiveness in spon-taneously breathing patients with severe sepsis or acutepancreatitis. Crit Care Med. 2010;38(3):819-825.
95. Kanji HD, McCallum J, Sirounis D, MacRedmond R,Moss R, Boyd JH. Limited echocardiography-guided ther-apy in subacute shock is associated with change in man-agement and improved outcomes. J Crit Care. 2014;29(5):700-705.
96. Niendorff DF, Rassias AJ, Palac R, Beach ML, Costa S,Greenberg M. Rapid cardiac ultrasound of inpatients sufferingPEA arrest performed by nonexpert sonographers. Resuscita-tion. 2005;67(1):81-87.
97. Seif D, Perera P, Mailhot T, Riley D, Mandavia D. Bedside ul-trasound in resuscitation and the rapid ultrasound in shockprotocol. Crit Care Res Pract. 2012;2012:503254.
98. Lee CW, Kory PD, Arntfield RT. Development of a fluidresuscitation protocol using inferior vena cava and lung ultra-sound. J Crit Care. 2016;31(1):96-100.
99. Noble VE, Brown DF. Renal ultrasound. Emerg Med Clin NorthAm. 2004;22(3):641-659.
100. Smith-Bindman R, Aubin C, Bailitz J, et al. Ultrasonographyversus computed tomography for suspected nephrolithiasis.N Engl J Med. 2014;371(12):1100-1110.
102. Huang SW, Lee CT, Chen CH, Chuang CH, Chen JB. Role ofrenal sonography in the intensive care unit. J Clin Ultrasound.2005;33(2):72-75.
103. Laing FC. Renal sonography in the intensive care unit.J Ultrasound Med. 2002;21(5):493-494.
104. Via G, Hussain A, Wells M, et al; International LiaisonCommittee on Focused Cardiac UltraSound (ILC-FoCUS);International Conference on Focused Cardiac UltraSound(IC-FoCUS). International evidence-based recommendationsfor focused cardiac ultrasound. J Am Soc Echocardiogr. 2014;27(7):683.e1-683.e33.
105. Cullen MW, Blauwet LA, Vatury OM, et al. Diagnostic capa-bility of comprehensive handheld vs transthoracic echocardi-ography. Mayo Clin Proc. 2014;89(6):790-798.
106. Dalen H, Gundersen GH, Skjetne K, et al. Feasibility and reli-ability of pocket-size ultrasound examinations of the pleuralcavities and vena cava inferior performed by nurses in anoutpatient heart failure clinic. Eur J Cardiovasc Nurs. 2015;14(4):286-293.
107. Testuz A, Müller H, Keller P-F, et al. Diagnostic accuracy ofpocket-size handheld echocardiographs used by cardiologistsin the acute care setting. Eur Heart J Cardiovasc Imaging.2013;14(1):38-42.
108. Prinz C, Dohrmann J, van Buuren F, et al. Diagnostic perfor-mance of handheld echocardiography for the assessment ofbasic cardiac morphology and function: a validation study inroutine cardiac patients. Echocardiography. 2012;29(8):887-894.
109. Trinquart L, Bruno O, Angeli ML, Belghiti J, Chatellier G,Vilgrain V. A hand-held ultrasound machine vs. conven-tional ultrasound machine in the bedside assessment ofpost-liver transplant patients. Eur Radiol. 2009;19(10):2441-2447.
110. Neskovic AN, Edvardsen T, Galderisi M, et al. Focus cardiacultrasound: the European Association of Cardiovascular Imag-ing viewpoint. Eur Heart J Cardiovasc Imaging. 2014;15(9):956-960.
111. Ayuela Azcárate JM, Clau-Terré F, Vicho Pereira R, et al;Grupo de Trabajo de Cuidados Intensivos Cardiológicos yRCP de la SEMICYUC. Consensus document on ultrasoundtraining in intensive care medicine: care process, use of thetechnique and acquisition of professional skills [in Spanish].Med Intensiva. 2014;38(1):33-40.
112. Moore CL. Credentialing and reimbursement in point-of-careultrasound. Clin Pediatr Emerg Med. 2011;12(1):73-77.
113. Platz E, Solomon SD. Point-of-care echocardiography in theaccountable care organization era. Circ Cardiovasc Imaging.2012;5(5):676-682.
Mayo Clin Proc. n December 2016;91(
114. Kaplan A, Mayo PH. Echocardiography performed by the pul-monary/critical care medicine physician. Chest. 2009;135(2):529-535.
115. Koenig SJ, Narasimhan M, Mayo PH. Thoracic ultrasonogra-phy for the pulmonary specialist. Chest. 2011;140(5):1332-1341.
116. Adrish M. Point-of-care ultrasonography: ready to take off?[letter]. Chest. 2015;147(1):e23.
117. Oks M, Narasimhan M. Point-of-care ultrasonography: readyto take off? [reply]. Chest. 2015;147(1):e23-e24.
118. Moore CL, Gregg S, Lambert M. Performance, training, qualityassurance, and reimbursement of emergency physician-performed ultrasonography at academic medical centers.J Ultrasound Med. 2004;23(4):459-466.
119. Lichtenstein DA, Mezière G, Lascols N, et al. Ultrasound diag-nosis of occult pneumothorax. Crit Care Med. 2005;33(6):1231-1238.
120. Mandavia DP, Hoffner RJ, Mahaney K, Henderson SO. Bedsideechocardiography by emergency physicians. Ann Emerg Med.2001;38(4):377-382.
121. Spencer KT, Anderson AS, Bhargava A, et al. Physician-per-formed point-of-care echocardiography using a laptop plat-form compared with physical examination in thecardiovascular patient. J Am Coll Cardiol. 2001;37(8):2013-2018.
122. Geria RN, Raio CC, Tayal V. Point-of-care ultrasound: not astethoscopeda separate clinical entity [letter]. J UltrasoundMed. 2015;34(1):172-173.
123. Mercaldi CJ, Lanes SF. Ultrasound guidance decreases com-plications and improves the cost of care among patients un-dergoing thoracentesis and paracentesis. Chest. 2013;143(2):532-538.
124. Patel PA, Ernst FR, Gunnarsson CL. Ultrasonography guidancereduces complications and costs associated with thoracentesisprocedures. J Clin Ultrasound. 2012;40(3):135-141.
125. Gundersen GH, Norekval TM, Haug HH, et al. Adding pointof care ultrasound to assess volume status in heart failure pa-tients in a nurse-led outpatient clinic: a randomised study.Heart. 2016;102(1):29-34.
126. Wang XT, Liu DW, Zhang HM, Chai WZ. Integrated cardio-pulmonary sonography: a useful tool for assessment of acutepulmonary edema in the intensive care unit. J Ultrasound Med.2014;33(7):1231-1239.
127. Melniker LA, Leibner E, McKenney MG, Lopez P, Briggs WM,Mancuso CA. Randomized controlled clinical trial of point-of-care, limited ultrasonography for trauma in the emergencydepartment: the first sonography outcomes assessment pro-gram trial. Ann Emerg Med. 2006;48(3):227-235.
128. National Institute for Health and Care Excellence (NICE).Guidance on the use of ultrasound locating devices for placingcentral venous catheters: NICE Technology Appraisal Guid-ance [TA49]. National Institute for Health and Care Excel-lence website. https://www.nice.org.uk/guidance/ta49.Published October 4, 2002. Accessed June 2, 2016.
129. Agency for Healthcare Research and Quality. Making HealthCare Safer: A Critical Analysis of Patient Safety Practices. Rock-ville, MD: Agency for Healthcare Research and Quality;2001. Evidence Report/Technology Assessment 43. AHRQpublication 01eE058.
130. Fagley RE, Haney MF, Beraud A-S, et al. Critical care basic ul-trasound learning goals for American anesthesiology criticalcare trainees: recommendations from an expert group. AnesthAnalg. 2015;120(5):1041-1053.
131. Frankel HL, Kirkpatrick AW, Elbarbary M, et al. Guidelinesfor the appropriate use of bedside general and cardiac ul-trasonography in the evaluation of critically ill patients,Part I: General ultrasonography. Crit Care Med. 2015;43(11):2479-2502.
132. Marin JR, Lewiss RE; American Academy of Pediatrics, Com-mittee on Pediatric Emergency Medicine; Society for
12):1811-1827 n http://dx.doi.org/10.1016/j.mayocp.2016.08.023www.mayoclinicproceedings.org
Academic Emergency Medicine, Academy of Emergency Ul-trasound; American College of Emergency Physicians, Pediat-ric Emergency Medicine Committee; World InteractiveNetwork Focused on Critical Ultrasound. Point-of-care ultra-sonography by pediatric emergency medicine physicians. Pedi-atrics. 2015;135(4):e1113-e1122.
133. American Institute of Ultrasound in Medicine; American Col-lege of Emergency Physicians. AIUM practice guideline for theperformance of the focused assessment with sonography for
Mayo Clin Proc. n December 2016;91(12):1811-1827 n http://dx.dowww.mayoclinicproceedings.org
134. Brass P, Hellmich M, Kolodziej L, Schick G, Smith AF. Ultra-sound guidance versus anatomical landmarks for internal jugu-lar vein catheterization. Cochrane Database Syst Rev. 2015;1:CD006962.
135. O’Grady NP, Alexander M, Burns LA, et al. Guidelines for theprevention of intravascular catheter-related infections. Am JInfect Control. 2011;39(4 Suppl 1):S1-S34.