32
Poisoning: from paracetamol to legal highs. or “Something old, something new, something borrowed, something blue.” Nick Bateman University of Edinburgh

Poisoning: from paracetamol to legal highs.
or
“Something old, something new, something
borrowed, something blue.”
Nick Bateman
University of Edinburgh

Question 1
Which of the following agents was associated with the greatest number of drug-related deaths in England in 2014?
A. Amfetamines
B. Cocaine
C. Morphine
D. Paracetamol
E. Tricyclic antidepressants
F. Don’t know

Answer Question 1
Which of the following was associated with the greatest number of drug-related deaths in England in 2014?
Deaths
A. Amfetamines 151
B. Cocaine 247
C. Morphine 952
D. Paracetamol 200
E. Tricyclic antidepressants 517
F. Don’t know

2010 2011 2012 2013 2014
All drug poisoning deaths 2,747 2,652 2,597 2,955 3,346
Any opiate 1,527 1,439 1,290 1,592 1,786
Heroin and Morphine 791 596 579 765 952
Methadone 355 486 414 429 394
Cocaine 144 112 139 169 247
Any amphetamine 56 62 97 120 151
Amphetamine 48 46 49 56 85
MDMA/Ecstasy 8 13 31 43 50
PMA / PMMA 0 1 20 29 24
Cannabinoids 11 7 18 13 31
New Psych Sub 22 31 55 63 82
Benzodiazepines 307 293 284 342 372
Diazepam 186 179 207 228 258
Source: Office of National Statistics: Deaths related to Poisoning Sept 2015
Drugs of abuse and with abuse potential

Substance 2010 2011 2012 2013 2014
All drug poisoning deaths
2,747 2,652 2,597 2,955 3,346
Paracetamol 199 207 182 226 200
Antidepressants 381 393 468 466 517
TCAs 194 200 233 235 253
SSRIs 136 127 158 150 159
Others 74 84 104 124 155
Antipsychotics 87 104 102 107 126
Zopiclone / Zolpidem 67 71 83 86 100
Barbiturates 19 37 32 32 50
Prescription drugs

Toxicity with antidepressants
• Cardiovascular- arrhythmias and cardiac failure, hypotension (esp. with amitriptylline)
• CNS- Fits and Coma, late delirium. MECHANISMS: Na+ channel blockade, (some K+ channel blockade), Amine reuptake blockade, increases local catecholamines. Anticholinergic Alpha blockade (amitriptylline) TREATMENT: Bicarbonate for wide QRS, Mg++ for wide QT (measure
manually) Norepinephrine for vasodilatation ? Insulin and glucose for myocardial failure and Intralipid

Question 2
An 18 year old male presents after a paracetamol overdose.
He is deemed to need acetylcysteine as his 4 h paracetamol concentration is 125 mg/L (above nomogram line).
30 min after starting the infusion he develops flushing and complains of chest discomfort
Which of the following is the most appropriate action in addition to stopping the infusion?

Question 2
Which of the following is the most appropriate action in addition to stopping the infusion?
A. Intramuscular adrenaline [0.5 mL of 1:1000 epinephrine (0.5 mg)] B. IV chlorphenamine (10mg) and hydrocortisone
(200mg) C. Nebulised salbutamol (2.5-5mg) D. Hydrocortisone (200mg IV) E. Observe response to stopping infusion F. Don’t know

Answer Question 2 A. Intramuscular adrenaline
[0.5 mL of 1:1000 epinephrine (0.5 mg)]
B. IV chlorphenamine (10mg) and hydrocortisone (200mg)
C. Nebulised salbutamol (2.5-5mg)
D. Hydrocortisone (200mg IV)
E. Observe response to stopping infusion
F. Don’t know
First line treatment chlorphenamine 10mg IV
AND Continue acetylcysteine

WARING, W. S., et al 2006. Clin Tox 44: 441-442. Schmidt L. E. 2013 Clin Tox 51: 467-72
Importance of paracetamol concn. in ADR rate
1 mmol/L =150mg/L
Both studies used case note review to ascertain ADRs

CHM Decision 2012
Adopt the previous ‘high risk’
line for all patients
and/or
use 75 mg/kg ingested dose
AND
Change initial NAC infusion from 15 min to 1 h
Estimated to prevent 1 death about every 2 years in UK. No data to support 1 h infusion (anectodal from N America, inadequate study from Australia)

Paracetamol concn & infusion rate on ADRs: 15 min or 1 hr Odds ratios of adverse events to treatment by presenting blood
paracetamol > or <= 100 mg/L*
All vomiting All anaphylactoid
events / n OR 95% CI p events / n OR 95% CI p
All
patients (n=8351)
>100 78/340 1.09 0.78-1.53 0.618 11/340 0.19 0.10-0.37 <0.001
<=100 102/495 1 - - 73/495 1 - -
15min
infusion (n=321)
>100 27/136 0.77 0.45-1.33 0.354 3/136 0.14 0.04-0.48 <0.001
<=100 46/185 1 - - 26/185 1 - -
1 h
infusion (n=514)
>100 51/204 1.37 0.88-2.12 0.163 8/204 0.21 0.10-0.47 <0.001
<=100 56/310 1 - - 47/310 1 - -
*Controlling for age, sex and infusion rate. 1One patient that had no data on blood paracetamol concentration is excluded.
Bateman et al 2014 BJCP. doi 10.111/bcp12362

First year impact of MHRA guidance
-4,000
-2,000
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
<100 100-149 150-199 >200 >24h Staggered Unknown Total
Inc
rea
se
(e
xtr
ap
ola
ted
to
UK
)
Patient category
Changes comparing year before with year after Extrapolated from data for 3 hospitals
Presentations
Admissions
NAC treatments
Nomogram bands
*MHRA estimate of additional NAC use 4,920-7,200 treatments Data from Bateman et al. Brit J Clin Pharmacol
2014 & Bateman et al. Clin Tox 2014
MHRA Est*
The cost to the NHS is estimated at £17.3 m (95% CI £13.4 to £21.5) to prevent 1 death.

TRIAL TREATMENTS
Acetylcysteine- matching duration of infusions Conventional 20.25 h acetylcysteine regimen 150mg/kg in 200mL, 15 min; 50mg/kg in 0.5L, 4 h ; 100mg/kg in 1 L, 16 h (British National Formulary 2009)
Modified 12 h acetylcysteine regimen 100mg/kg in 200 mL, 2h; 200mg/kg 1L, 10h infusion; followed by 0.5L 5% dextrose to 20.25 h for matching
Ondansetron 4mg IV Pre-treatment with ondansetron v saline placebo
Lancet, 2014. 383; 697-704.

Antiemetic rescue. Kaplan Meier analysis to 12 h
OR at 12 h: Modified v conventional NAC OR 0.37, 97.5% CI 0.18-0.79, P = 0.003 Ondansetron v placebo OR 0.35, 97.5% CI 0.17-0.74, P = 0.002
Patients at risk
Ondanstron/Modified 54 50 46 42 40 40 40
Ondanstron/Conventional 55 41 36 36 36 36 36
Placebo/Modified 55 50 40 37 35 33 33
Placebo/Conventional 54 27 21 21 19 18 18
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 2 4 6 8 10 12
Pro
po
rti
on
of
pa
tie
nts
wit
ho
ut
an
ev
en
t
Time (hours)
Ondansetron / Modified
Ondansetron / Conventional
Placebo / Modified
Placebo / Conventional
Patients at risk
Ondanstron/Modified 54 53 50 50 50 50 50
Ondanstron/Conventional 55 43 40 40 40 40 40
Placebo/Modified 55 55 51 51 50 50 50
Placebo/Conventional 54 41 41 39 38 38 37
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 2 4 6 8 10 12
Pro
po
rtio
n o
f p
atie
nts
w
ith
ou
t a
n e
ve
nt
Time (hours)
Ondansetron / Modified
Ondansetron / Conventional
Placebo / Modified
Placebo / Conventional
OR at 12 h: Modified vs conventional NAC OR 0.23 (0.12 to 0.43, p< 0.0001) Ondansetron vs placebo OR 1.4 (0.78 to 2.53, p= 0.198)
Anaphylactoid rescue. Kaplan Meier to 12 h

Take home message A simpler shorter acetylcysteine regimen, with 12 h
blood samples, and linked to newer approaches of assessing risks of hepatic injury, offers potential for reducing:-
ADRs hospital length of stay medication errors. In addition earlier identification of ‘at risk’ patients on
treatment will allow study of earlier increased NAC treatments.
Studies ongoing to facilitate full licence

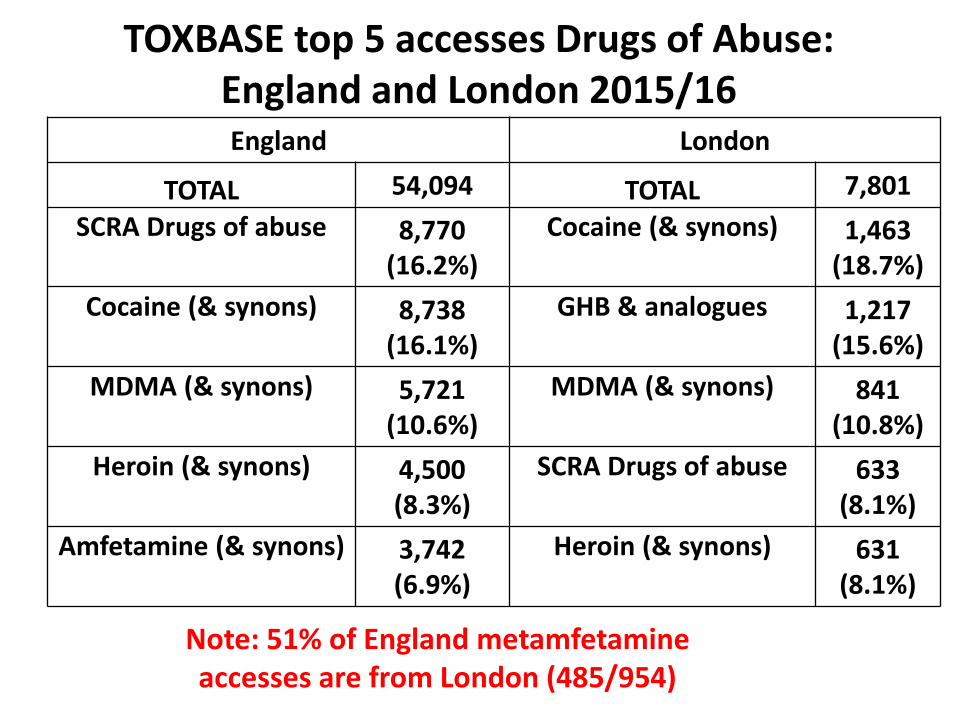
TOXBASE top 5 accesses Drugs of Abuse: England and London 2015/16 England London
TOTAL 54,094 TOTAL 7,801
SCRA Drugs of abuse 8,770 (16.2%)
Cocaine (& synons) 1,463 (18.7%)
Cocaine (& synons) 8,738 (16.1%)
GHB & analogues 1,217 (15.6%)
MDMA (& synons) 5,721 (10.6%)
MDMA (& synons) 841 (10.8%)
Heroin (& synons) 4,500 (8.3%)
SCRA Drugs of abuse 633 (8.1%)
Amfetamine (& synons) 3,742 (6.9%)
Heroin (& synons) 631 (8.1%)
Note: 51% of England metamfetamine accesses are from London (485/954)

Question 3 A 19 year old woman presents after taking an
unknown drug of abuse at a night club. She is confused, has dilated pupils and is noted to have marked ankle clonus. Which of the following drugs is she most likely to have ingested?
A. Cannabis B. Cocaine C. Mephedrone D. Metamfetamine E. MDMA (ecstasy) F. Something else

Question 3 A 19 year old woman presents after taking an
unknown drug of abuse at a night club. She is confused, has dilated pupils and is noted to have marked ankle clonus. Which of the following drugs is she likely to have ingested?
A. Cannabis B. Cocaine C. Mephedrone (cathinone) D. Metamfetamine E. MDMA (ecstasy) (SEROTONIN
SYNDROME) F. Something else

Syndromes
Sedative Stimulant Serotonin Hallucinogenic Dissociative Synthetic Cannabinoid Inhalants Poppers NOTE: Drugs often mixed And not what it says on the label
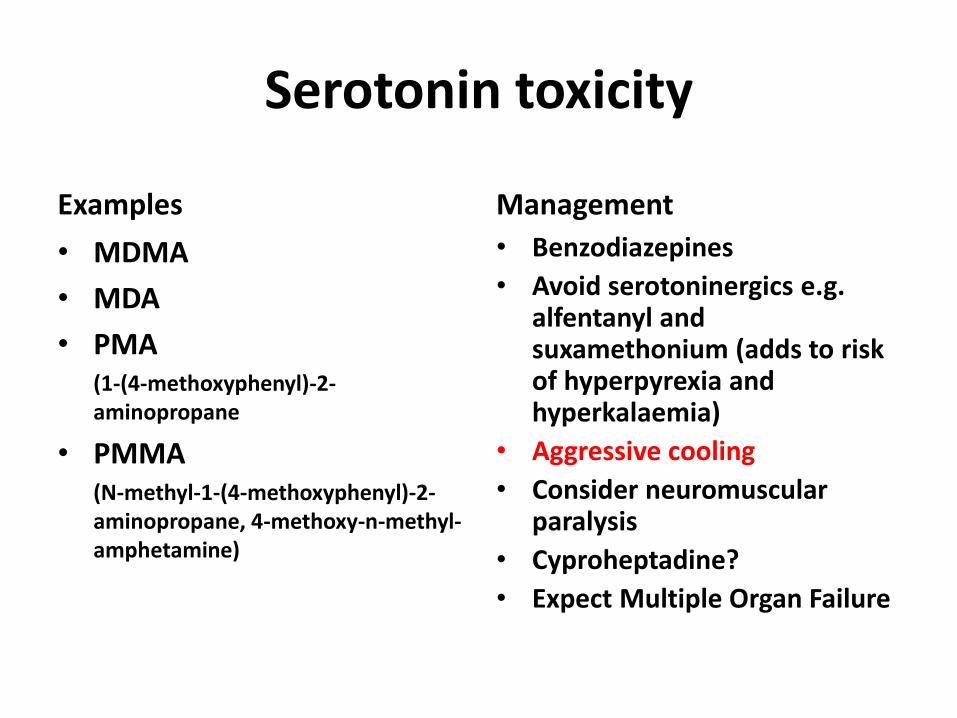
Serotonin toxicity
Examples
• MDMA
• MDA
• PMA (1-(4-methoxyphenyl)-2-
aminopropane
• PMMA (N-methyl-1-(4-methoxyphenyl)-2-
aminopropane, 4-methoxy-n-methyl-amphetamine)
Management
• Benzodiazepines
• Avoid serotoninergics e.g. alfentanyl and suxamethonium (adds to risk of hyperpyrexia and hyperkalaemia)
• Aggressive cooling
• Consider neuromuscular paralysis
• Cyproheptadine?
• Expect Multiple Organ Failure
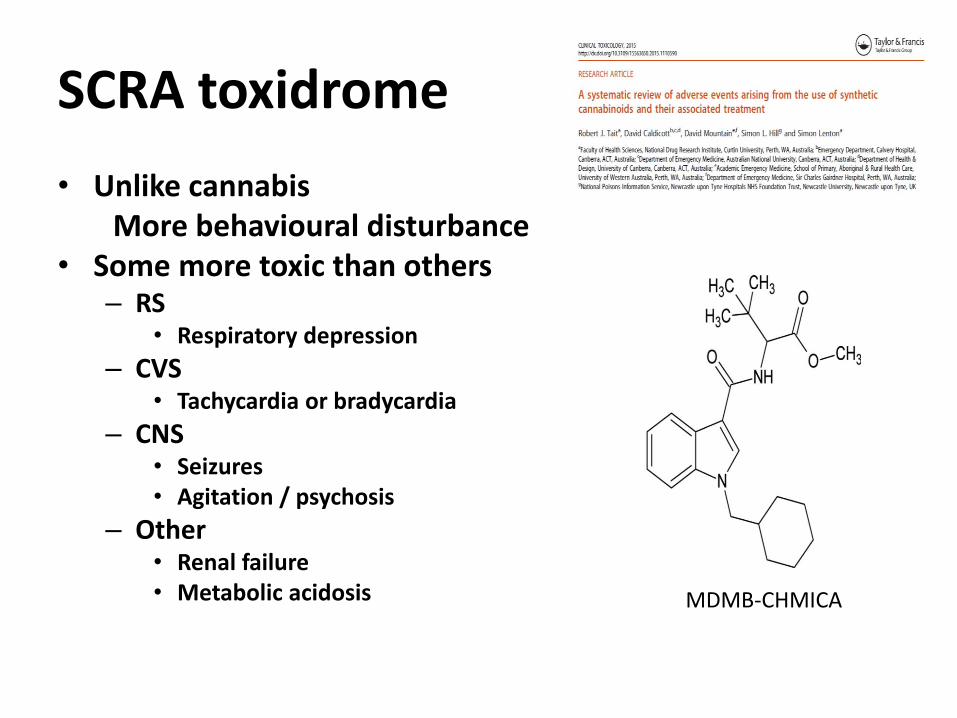
SCRA toxidrome
• Unlike cannabis More behavioural disturbance • Some more toxic than others
– RS • Respiratory depression
– CVS • Tachycardia or bradycardia
– CNS • Seizures • Agitation / psychosis
– Other • Renal failure • Metabolic acidosis MDMB-CHMICA


Question 4
How much longer is the half-life of methadone than that of naloxone?
A. 2x
B. 3x
C. 4x
D. 6x
E. >6x
F. Don’t know

Question 4
How much longer is the half-life of methadone than that of naloxone?
A. 2 x
B. 3 x
C. 4 x
D. 6 x
E. >6 x
F. Don’t know
Methadone half-life 8-50 h; Naloxone 30-80 minutes (Morphine ~ 2-3 h)
ALSO BEWARE MULTIPLE DRUGS AND SLOW RELEASE
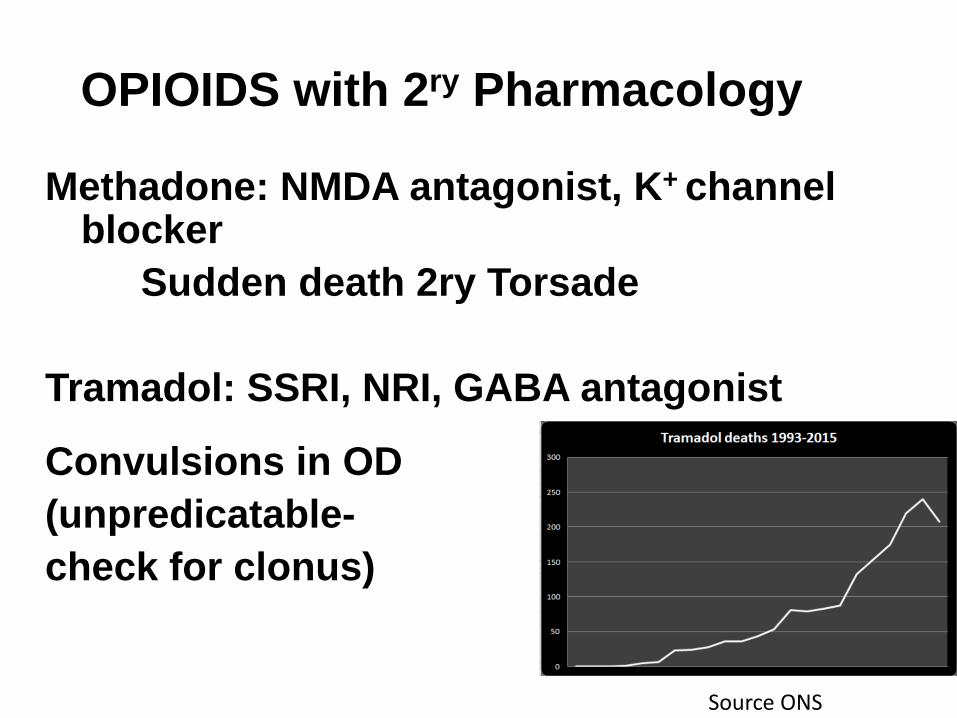
OPIOIDS with 2ry Pharmacology
Methadone: NMDA antagonist, K+ channel blocker
Sudden death 2ry Torsade
Tramadol: SSRI, NRI, GABA antagonist
Convulsions in OD
(unpredicatable-
check for clonus)
h
Source ONS

Question 5 A 45 year old bus driver presented to
hospital complaining his appearance had
changed over his lunch break.
He was otherwise asymptomatic.
What is the likely cause?
A. Beetroot in sandwich
B. Carbon monoxide
C. Hydrogen Cyanide
D. Isobutyl nitrite
E. Undiagnosed cyanotic heart disease
F. Don’t know

Question 5 A 45 year old bus driver presented to
hospital complaining his appearance had
changed over lunch. He was otherwise
asymptomatic. What is the likely cause?
A. Beetroot in sandwich
B. Carbon monoxide
C. Hydrogen Cyanide
D. Isobutyl nitrite (Poppers)
E. Undiagnosed cyanotic heart disease
F. Don’t know
METHAEMOGLOBINAEMIA

Causes of methaemoglobinaemia • Local anaesthetics • Chlorates • Nitrates • Sulphonamides and dapsone • Aniline dyes
All cause massive (1000 fold) increase in methaemoglobin production
Treatment of symptomatic patients (> 30% methaemoglobin) is methylonium chloride (methylene blue) and oxygen.

Cyanosis from HCN and CO
• Very rare in practice • If patient breathing give oxygen treat acidosis
and recovery likely, unless hypoxic brain injury already occurred
• Benefits of hydroxycobalamin (Cyanide) and hyperbaric oxygen (CO) uncertain, so no reason to use either in routine practice (eg smoke inhalation).
• Lactic acidosis is a surrogate for toxicity with cyanide, but very non specific, and will normally recover with resuscitation and fluid.
(remember ethanol as a cause of acidosis too)

TOXBASE App on i-phone and Android
Full access free if you log in with NHS email
Thankyou [email protected]

















