Compliance with this Guideline is recommended Page 1 of 18 Policy Directive Women and Babies: Persistent pulmonary hypertension of the newborn (PPHN) Document No: RPAH_GL2014 Functional Sub-Group: Clinical Governance Summary: Babies with persistent pulmonary hypertension will undergo early diagnosis and appropriate management National Standard: Standard 1: Governance for safety and quality in Health service organisations Standard 9: Recognising and responding to clinical deterioration in acute health care Policy Author: Tracey Lutz, Staff Specialist Neonatologist Approved by: General Manager RPA Women and Babies Service Improvement Committee Publication (Issue) Date: March 2017 Next Review Date: March 2020 Replaces Existing Policy: Persistent pulmonary hypertension of the newborn Previous Review Dates: 1998 Note: Sydney Local Health District (LHD) and South Western Sydney LHD were established on 1 July 2011, with the dissolution of the former Sydney South West Area Health Service (SSWAHS) in January 2011. The former SSWAHS was established on 1 January 2005 with the amalgamation of the former Central Sydney Area Health Service (CSAHS) and the former South Western Sydney Area Health Service (SWSAHS). In the interim period between 1 January 2011 and the release of specific LHN policies (dated after 1 January 2011) and SLHD (dated after July 2011), the former SSWAHS, CSAHS and SWSAHS policies are applicable to the LHDs as follows: Where there is a relevant SSWAHS policy, that policy will apply Where there is no relevant SSWAHS policy, relevant CSAHS policies will apply to Sydney LHD; and relevant SWSAHS policies will apply to South Western Sydney LHD.
Transcript
Compliance with this Guideline is recommended Page 1 of 18
Policy Directive
Women and Babies: Persistent pulmonary hypertension of the newborn (PPHN)
Summary: Babies with persistent pulmonary hypertension will
undergo early diagnosis and appropriate management National Standard: Standard 1: Governance for safety and quality in Health service organisations Standard 9: Recognising and responding to clinical deterioration in acute health care Policy Author: Tracey Lutz, Staff Specialist Neonatologist Approved by: General Manager
RPA Women and Babies Service Improvement Committee
Publication (Issue) Date: March 2017 Next Review Date: March 2020 Replaces Existing Policy: Persistent pulmonary hypertension of the newborn Previous Review Dates: 1998
Note: Sydney Local Health District (LHD) and South Western Sydney LHD were established on 1 July 2011,
with the dissolution of the former Sydney South West Area Health Service (SSWAHS) in January 2011. The former SSWAHS was established on 1 January 2005 with the amalgamation of the former Central Sydney Area Health Service (CSAHS) and the former South Western Sydney Area Health Service (SWSAHS).
In the interim period between 1 January 2011 and the release of specific LHN policies (dated after 1 January 2011) and SLHD (dated after July 2011), the former SSWAHS, CSAHS and SWSAHS policies are applicable to the LHDs as follows:
Where there is a relevant SSWAHS policy, that policy will apply
Where there is no relevant SSWAHS policy, relevant CSAHS policies will apply to Sydney LHD; and relevant SWSAHS policies will apply to South Western Sydney LHD.
Compliance with this Guideline is recommended Page 2 of 18
Women and Babies: Persistent pulmonary hypertension of the newborn
CONTENTS
1. Introduction
2. Policy Statement
3. Principles/Guidelines
3.1 Definitions 4
3.2 Incidence 5
3.3 Risk Factors 5
3.4 Pathophysiology 5
3.5 Clinical diagnosis 6
3.6 Echocardiographic diagnosis 6
3.7 Interventions 7
3.8 Outcomes 13
4. Flow Diagram – Management of PPHN 14
5. Key points 15
6. References 15
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 3 of 18
Women and Babies: Persistent pulmonary hypertension of the newborn
1. Introduction
The risks addressed by this policy:
Potential serious morbidity and mortality associated with lack of recognition of PPHN
The aims / expected outcome of this policy
Persistent pulmonary hypertension will be recognised early, diagnosed and appropriately managed
2. Policy Statement
The goal of this policy is to identify babies with pulmonary hypertension and to commence therapy immediately and appropriately. The therapeutic goal should be to avoid hypoxia.
3. Guidelines
3.1 Definition:
During fetal life, the placenta serves as the organ of gas exchange. Blood flow in the pulmonary circulation remains highly restricted by hypoxic pulmonary vasoconstriction of the small pulmonary arteries. This is reversed at birth due to the sudden increase in lung oxygenation when the newborn takes their first breath. The first few breaths induce a rapid decrease in pulmonary vascular resistance and an increase in pulmonary vascular flow with lung expansion1.
Classically, PPHN is defined as the failure of the normal postnatal fall in pulmonary vascular resistance which leads to the persistence of right to left shunts across the fetal channels (ductus arteriosus and foramen ovale) and resultant hypoxia. 2 This is a simplified view of what is a complex condition and in many babies the major shunt is occurring at an intrapulmonary level.2 It is important to think of PPHN as primary or secondary.3
Primary PPHN is the form of PPHN which most closely fits the classical definition, typically presenting soon after birth with hypoxaemia in a baby with clinically and radiologically normal lungs.3 This condition is probably due to a primary dysfunction in the pulmonary endothelial vasodilating mechanisms.2
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 4 of 18
Secondary PPHN is PPHN which is secondary to a disease in the parenchyma of the lungs. This is over- diagnosed and while most babies with lung disease will have pulmonary artery pressures above normal, only the sickest (oxygenation index >25 in term babies 2 or >15 in preterm babies) 4 will consistently have pulmonary pressures close to or above systemic pressures. In these babies the pulmonary vasoconstriction is probably secondary to hypoxia, acidosis and high ventilatory pressures.
3.2 Incidence:
PPHN is an uncommon condition and mainly affects term or post-term babies; however, may be present in the preterm infant. The incidence reported in the UK ranges from 0.4 – 0.68/1000 live births. In a study in 12 major North American Centres, the incidence is reported as 1.9/1000. 5
3.3 Risk Factors:
Primary PPHN is usually idiopathic in origin. It is often associated with a variety of complications of pregnancy including maternal diabetes, maternal hypertension, obesity and post maturity. It has also been described in association with polycythaemia, fetal anaemia and premature ductal closure.
Secondary PPHN o Respiratory: Meconium aspiration, respiratory distress syndrome,
Transient Tachypnea of the Newborn (TTN), pneumonia, bronchopulmonary dysplasia, congenital diaphragmatic hernia, capillary alveolar dysplasia, surfactant deficiency, pulmonary interstitial lymphangiectasia
o Non- Respiratory: Sepsis, Hypoxic Ischaemic Encephalopathy, drugs (Selective Serotonin Reuptake Inhibitors (SSRIs)), Vein of Galen,
3.4 Pathophysiology:
The pathophysiology of PPHN is complex and related to the causes of increased pulmonary vascular resistance in the perinatal period. 5 Some of the factors include
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 5 of 18
3.5 Clinical Diagnosis:
Primary PPHN presents in the early postnatal period as cyanosis where the level of hypoxia is disproportionate to the degree of respiratory distress. The clinical presentation closely mimics that of cyanotic congenital heart disease. There may be differential cyanosis between upper and lower body, clinically and on blood gases. The lung fields are often clear or minimally opacified on X-ray. The degree of hypoxia is variable and the pCO2 is normal or sometimes low.
Secondary PPHN presents primarily as respiratory distress, often with respiratory failure and the need for high ventilator pressures and increasing oxygen requirements. The CXR is mostly abnormal, in keeping with the underlying respiratory condition.
Infants with PPHN may have a prominent precordial impulse, loud second heart sound, a systolic parasternal murmur due to tricuspid incompetence and a large cardiac shadow on chest x-ray.
3.6 Echocardiographic diagnosis: 6
This allows accurate diagnosis of PPHN and should be done as soon as practical in the clinical course. The benefits of echocardiography include the following:
The ability to exclude congenital heart disease. The ability to define the pulmonary artery pressure using tricuspid
incompetence or ductal shunt velocities. Define the presence, degree and direction of shunt through the ductus
arteriosus and foramen ovale. These shunts are often less than is assumed, firstly because pulmonary pressures are subsystemic and secondly because both fetal channels particularly the ductus close early in the course of the disease.4
Define the ventricular outputs. These are commonly very low in the early course.4 Sehgal8 et al demonstrated global myocardial dysfunction in infants with pulmonary hypertension with low right and left ventricular outputs in the majority of babies. Left ventricular output < 100ml/kg/min indicates a high risk of mortality.41
On point of care cardiac ultrasound the following are indicative of pulmonary hypertension
Pulmonary pressures equivalent or greater than systemic pressures measured on the TR jet using continuous wave doppler43
Pulmonary Artery Time to peak velocity to Rv ejection time ratio < 0.2
Reduced LPA velocity – low velocities are predictive of good response to iNO
The direction and velocity of the ductal shunt – a right to left shunt for more than 30% of the cardiac cycle indicates that Pulmonary Artery
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 6 of 18
Pressure (PAP) is higher than systemic pressure. 42
3.7 Interventions:
The aim of treatment is to maintain normal arterial oxygen levels and normal oxygen delivery to the organs of the body. The two most potent natural pulmonary vasodilators are oxygen and lung inflation.
3.7.1. Oxygen
This will help to maintain arterial oxygen levels and will act as a pulmonary vasodilator. However animal data would suggest that optimal pulmonary vasodilation occurs with a paO2 around 100mmHg; however it does depend on whether there is an associated acidosis. 9 No benefit is likely from higher levels of inspired oxygen which may also contribute to secondary lung injury. Therefore maintain saturations in the normal range (95-100%), aiming to maintain paO2 between 60-100 mmHg in term infants.48
3.7.2. Conventional ventilation
This is the mainstay of respiratory support; the principles will be much as described for ventilation of preterm babies but with the following differences.
Muscle relaxants should be reserved for newborns where there is difficulty establishing adequate ventilation despite good sedation.5
To maintain normal blood gases it is sometimes necessary to achieve higher than usual tidal volumes (up to 6mls/kg). Oxygenation is often very sensitive to small reductions in minute volume such as can occur with retained secretions or handling.
Aim to maintain normal pCO2 in the range 35 to 40 mmHg, pCO2 lower than this may cause cerebral vasoconstriction. Hypercarbia leads to pulmonary vasoconstriction and should be avoided.5
3.7.3. High Frequency Oscillatory Ventilation (HFOV):
A review of randomised studies comparing HFOV with conventional ventilation in babies with severe hypoxic respiratory failure has shown no differences in mortality, chronic lung disease or air leak. 10 In a proportion of babies HFOV allowed for better oxygenation by allowing better lung inflation and "alveolar recruitment".11,12 In babies with secondary PPHN and underlying lung parenchymal disease HFOV improves oxygenation and reduces right to left extrapulmonary shunting due to aggressive lung recruitment.1 HFOV should not be started without senior consultation and supervision.
3.7.4. Inotropes:
The role of inotropes in PPHN is poorly substantiated. Low ventricular outputs are common in these babies however it is not clear that this is due to primary pump failure. Observational studies here and elsewhere have suggested that
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 7 of 18
low output may reflect the right ventricle struggling with a high afterload to get blood through the lungs, which in turn causes a low left ventricular output. 7, 13 In animal studies, dopamine has similar vasoconstrictor activity on the pulmonary as on the systemic vasculature, so at an empirical level, dobutamine is the preferred inotrope starting at 10 µ/kg/min. Noradrenalin improves oxygenation in infants with PPHN through a decrease in pulmonary systemic artery pressure ratio and improved cardiac performance. 14
Inotrope Effects Dosage Unwanted Effects
Dobutamine
(first line)
Improves cardiac output
Little peripheral vascular effect
2.5-20µg/kg/min
Noradrenalin
(second line)
Improves cardiac output through inotropic effect
Increases BP (α effect)
Improvement in pulmonary blood flow secondary to the release of endothelial nitric oxide
0.5-1µg/kg/min
Adrenalin
(second line)
Improves cardiac output through inotropic effect
Increases BP (α effect)
0.05-1µg/kg/min
Dopamine
(third line)
Increases mycocardial contractility, BP and cardiac output
Increased systemic vascular resistance
1-20µg/kg/min Increase in systemic and pulmonary pressure at high doses
3.7.5. Vasodilators:
A. Nitric oxide (NO)
o Nitric oxide (NO) is a naturally occurring vasodilator which is present in the vascular endothelium of all the tissues of the body. At a cellular level it works by activating guanylate cyclase leading to an increase in the production of cyclic GMP which in turn relaxes vascular smooth
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 8 of 18
muscle. It is rapidly inactivated in the blood stream with production of methaemoglobin and inorganic nitrates and nitrites. Due to these properties, when it is given by inhalation (iNO) it dilates the pulmonary blood vessels in ventilated lung, reducing pulmonary vascular resistance, increasing pulmonary blood flow and improving ventilation perfusion mismatch without having any significant effect on the systemic vasculature. It is the vasodilator of choice in term babies with persistent pulmonary hypertension.
o It has a rapid onset of action, typically within minutes. The safety and efficacy of iNO for PPHN in term infants has been studied through randomised controlled trials and demonstrates that:
iNO significantly improves oxygenation. 15-21 iNO significantly reduces the need for rescue with
ECMO.16,17 The use of iNO in PPHN does not reduce mortality, length
of hospitalisation, chronic lung disease or alter neurodevelopmental outcomes
o The role of iNO in preterm babies is inconclusive. The Cochrane
review by Barrington & Finer included 9 trials which were categorized into: early rescue, early prophylactic and late therapy groups. iNO used as rescue therapy in the very ill preterm infant was ineffective and if used early for RDS does not improve survival; however was not harmful (no increase in neurodevelopmental disability or IVH). There is some evidence to suggest that later use of iNO to prevent BPD may be useful however, more studies need to be done.34
o Prescribing Nitric Oxide
iNO is registered with the Australian Therapeutic Goods Administration (TGA). It needs to be prescribed on the medication chart. Start and stop times as well as dosage changes must be charted accurately.
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 9 of 18
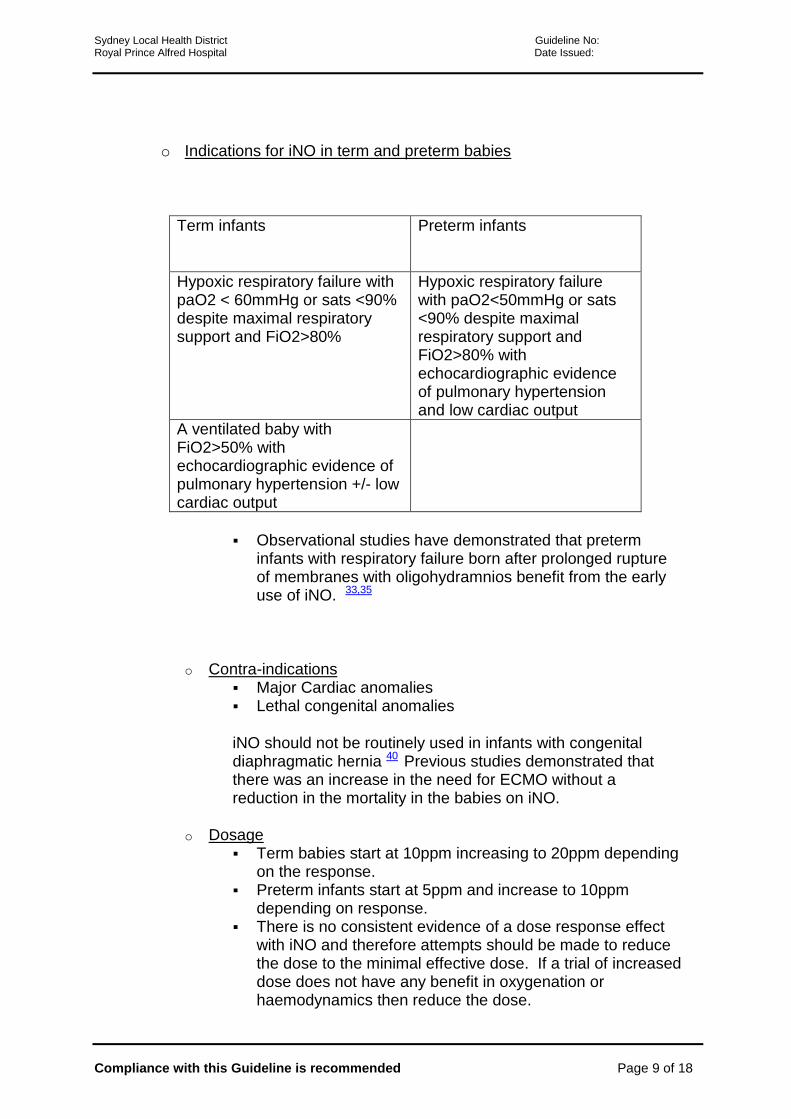
o Indications for iNO in term and preterm babies
Term infants Preterm infants
Hypoxic respiratory failure with paO2 < 60mmHg or sats <90% despite maximal respiratory support and FiO2>80%
Hypoxic respiratory failure with paO2<50mmHg or sats <90% despite maximal respiratory support and FiO2>80% with echocardiographic evidence of pulmonary hypertension and low cardiac output
A ventilated baby with FiO2>50% with echocardiographic evidence of pulmonary hypertension +/- low cardiac output
Observational studies have demonstrated that preterm infants with respiratory failure born after prolonged rupture of membranes with oligohydramnios benefit from the early use of iNO. 33,35
o Contra-indications Major Cardiac anomalies Lethal congenital anomalies
iNO should not be routinely used in infants with congenital diaphragmatic hernia 40 Previous studies demonstrated that there was an increase in the need for ECMO without a reduction in the mortality in the babies on iNO.
o Dosage Term babies start at 10ppm increasing to 20ppm depending
on the response. Preterm infants start at 5ppm and increase to 10ppm
depending on response. There is no consistent evidence of a dose response effect
with iNO and therefore attempts should be made to reduce the dose to the minimal effective dose. If a trial of increased dose does not have any benefit in oxygenation or haemodynamics then reduce the dose.
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 10 of 18
o Complications Methaemoglobinaemia
o iNO can cause methaemoglobinaemia although unlikely at a dose of 20ppm. Preterm infants are more susceptible because of relatively low levels of the enzyme methaemoglobin reductase. Methaemoglobin levels should be checked every 24 hours (≤20ppm); every 12 hours if on higher doses. All infants should be monitored (MetHb monitor). If levels > 5 % iNO should be reduced or stopped.
o Weaning There is little evidence to guide the best method of weaning
iNO. 40 The aim should be to deliver the minimum dose compatible with normal oxygenation and haemodynamics
o In term babies there is an advantage in maintaining a low dose of NO (1-2ppm) while oxygen and ventilator pressures are weaned, especially if there is echocardiographic evidence of raised pulmonary artery pressures.37,40
o FiO2 should be increased prior to discontinuation of iNO therapy 38
o In preterm infants wean as quickly as possible
o iNO delivery system At RPA we use the iNOmax DSIR (Ikaria ) nitric oxide
delivery set up
B. Sildenafil o Sildenafil is a phosphodiesterase 5 inhibitor which results in
vasodilation by selectively reducing pulmonary vascular resistance. Sildenafil is safe and easy to administer; it is available in an IVI and oral preparation and is relatively inexpensive. Enteral administration and gastro-intestinal absorption may be impaired in critically ill patients. A pilot study of intravenous sildenafil demonstrated that it was well tolerated with improved oxygenation in some infants. 22, 39 A randomised control trial evaluating the efficacy of intravenous sildenafil is currently underway.
o There is a lack of evidence to support sildenafil use in persistent pulmonary hypertension in preterm infants.
o Consider Sildenafil in the following circumstances Proven severe PPHN not responding to adequate
ventilation and iNO (limited observational data suggests
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 11 of 18
additional benefit)22 Failed attempt to wean iNO
o Dosage 0.5-2mg/kg/dose 6 hourly
C. Milrinone o Milrinone causes pulmonary vasodilation by inhibiting
phosphodiesterase 3. Milirone is reported to decrease rebound pulmonary hypertension when iNO is ceased. It has inotropic effects and is also effective in reducing the afterload by improving right sided cardiac output. Milrinone led to better oxygenation and improvement in pulmonary and systemic haemodynamics in patients with suboptimal response to iNO23. The safety and efficacy has not been confirmed in a RCT and therefore it is not routinely used at RPAH. 23,24.
D. Magnesium Sulphate o There is insufficient evidence to support its use in PPHN. 25
E. Bosentan o Bosentan is an orally active dual endothelin receptor antagonist
which reduces Peripheral Vascular Resistance (PVR) and pulmonary arterial pressure in pulmonary hypertension in adults. A recent randomised controlled trial demonstrated that bosentan was superior to placebo (p<0.0001) as an adjuvant therapy of PPHN in neonates 26,27. All the trials have been done in low-income settings where iNO and ECMO are not readily available. Bosentan is not used at RPAH.
3.7.6. Extracorporeal membrane oxygenation (ECMO)
Since the introduction of iNO and HFOV, together with surfactant, the need for ECMO in PPHN has declined considerably. However the UK collaborative trial showed a significant reduction in mortality with ECMO treatment in babies with an oxygenation index >40. 28 In babies with an OI >40 despite iNO and HFOV, transfer to a paediatric intensive care for ECMO should be considered. All potential referrals should be discussed with the Paediatric Intensivist at SCH or The Children’s Hospital Westmead. Selection Criteria43
1. Respiratory failure 2. OI > 40 for 4 hours (OI=(MAPX FiO2 x 100)/PaO2
Exclusion Criteria (Absolute)43
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 12 of 18
1. < 2.5kg for V-V ECMO and < 1.8kg for V-A ECMO 2. Major intracranial haemorrhage ( Grade 3 or 4) 3. Severe neurologic injury 4. Lethal malformation
Exclusion Criteria (Relative)43
1. < 34 weeks gestation 2. Mechanical ventilation > 14 days 3. Uncontrolled coagulopathy 4. Grade 1/2 IVH 5. Overwhelming sepsis 6. Syndrome with poor prognosis 7. Congenital diaphragmatic hernia with pre-ductal sats < 90% during
resuscitation or stabilisation 8. Malignancy
Acidosis, prematurity and profound hypoxemia are independently associated with an increased mortality. 29
3.8 Outcomes
Persistent pulmonary hypertension of the newborn has a 10-20% mortality. Survivors have significant morbidities including cognitive delays, hearing loss and risk of rehospitalisation. 30,31 The use of iNO in PPHN did not alter neurodevelopmental and social/emotional/behavioural outcomes compared with infants who were not exposed to iNO 32
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 13 of 18
4. Management of Pulmonary Hypertension of the Newborn
Clinically suspected PPHN
Point of care cardiac ultrasound Confirm PPHN
Exclude congenital cardiac disease
Define SVC, RVO and LVO flows
Adequately oxygenate and ventilate – conventional ventilation/HFOV
Maintain normal saturations
(95-100%); PaO2 60-
100mmHg
PaCO2 normal range
Add inotropes if hypotensive, pulmonary pressures are significantly suprasytemic or low systemic blood flow*
First line – dobutamine
Second line – noradrenalin/adrenalin
Third line – dopamine
Add pulmonary vasodilator if ongoing hypoxic respiratory failure
Inhaled NO
Consider ECMO if OI^ remains > 40 despite HFOV,
iNO and Sildenafil
*RVO and LVO < 150mls/kg/min; SVC< 50mls/kg/min ^Oxygenation Index = (FiO2 x Mean Airway pressure)/ PaO2
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 14 of 18
5. Key points
Optimal alveolar recruitment should be established prior to initiation of iNO therapy
Level of evidence 1b Strength of recommendation A
Nitric oxide (NO) is the vasodilator of choice in term babies 15-21
Level of evidence 1b Strength of recommendation A
Intravenous sildenafil is well tolerated and improves oxygenation in PPHN22
Level of evidence 1b Strength of recommendation A
ECMO should be considered in babies who fail to respond to HFOV and NO 28,29
2. Kinsella JP, Abman SH. Recent developments in the pathophysiology and treatment of persistent pulmonary hypertension of the newborn. J Pediatr 1995; 126:853-64.
3. Fox WW, Duara S. Persistent pulmonary hypertension in the neonate: diagnosis and management. J Pediatr 1983; 103:505-14.
4. Evans N, Kluckow M. Early determinants of right and left ventricular output in ventilated preterm infants. Arch Dis Child 1996; 74:F88-94.
5. Cabral J and Belik J. Persistent pulmonary hypertension of the newborn: recent advances in pathophysiology and treatment. Journal of Pediatrics 2013 89: 226-242
6. Evans N, J. Echocardiographic assessment of the newborn infant with suspected persistent pulmonary hypertension. Seminars in Neonatology 1997; 2:37-48
7. Evans N, Kluckow M, Currie A. Range of echocardiographic findings in term and near term babies with high oxygen requirements. Arch Dis Child 1998; 78: 105-111
8. Sehgal A, Athikarisamy S and Adamopoulos M. Global myocardial function is compromised in infants with pulmonary hypertension. Acta Paediatrica 2012; 101: 410-413
9. Rudolph A, Yuan S. Response of the pulmonary vasculature to hypoxia and H+ ion concentration changes. Journal of Clinical investigation; 1966: volume
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 15 of 18
45: 399-411
10. De Paoli A, Clark R, Bhuta T, Henderson-Smart D. High frequency oscillatory ventilation versus conventional ventilation for infants with severe pulmonary dysfunction born at or near term. The Cochrane Library. 2009
11. Kinsella JP, Truog WE, Walsh WF, Goldberg RN, Bancalari E, Mayock DE, Redding GJ, deLemos RA, Sardesai S, McCurnin DC, et al. Randomized, multicenter trial of inhaled nitric oxide and high-frequency oscillatory ventilation in severe, persistent pulmonary hypertension of the newborn. J Pediatr 1997; 131:55-62.
12. Clark RH, Yoder BA, Sell MS. Prospective, randomized comparison of high-frequency oscillation and conventional ventilation in candidates for extracorporeal membrane oxygenation [see comments]. J Pediatr 1994; 124:447-54.
13. Skinner JR, Hunter S, Hey E. Haemodynamic features at presentation in persistent pulmonary hypertension of the newborn and outcome. Arch Dis Child 1996; 74:F26-32.
14. Tourneux P, Rakza T, Bouissou A et al. Pulmonary circulatory effects of norepinephrine in newborn infants with persistent pulmonary hypertension. Journal of Pediatrics 2008: 153: 345-349
15. Finer N, Barrington K. Nitric oxide for respiratory failure in infants born at or near term. The Cochrane Library. October 2006
16. Roberts J, Fineman J, Morin F et al. Inhaled Nitric Oxide and persistent pulmonary hypertension of the newborn. The New England Journal of Medicine, 1997; 336: 605-610
17. Clark R, Kueser T, Walker M et al. Low-dose nitric oxide for persistent pulmonary hypertension of the newborn. The New England Journal of Medicine, 1997; 342: 469-474.
18. Porta N, Steinhorn R. Pulmonary vasodilatory therapy in the NICU: inhaled nitric oxide, sildenafil and other pulmonary vasodilating agents. Clinics Perinatology 2012 39: 149-154
19. Barr F, Macrae D. Inhaled Nitric oxide and related therapies. Pediatric Crit Care Med, 2010; volume 11 (2): S30-S36
20. Dewhurst C, Ibrahim H, Gothberg S. Use of inhaled nitric oxide in the newborn period: results from the European inhaled nitric oxide registry. Acta Paediatrica. 2010; 99: 854-860
21. Steinhorn R. Pharmacotherapy of pulmonary hypertension. Pediatric Clinics North America. 2012 59 (5): 1129 – 1146
22. Steinhorn R, Kinsella J, Pierce C et al. Intravenous Sildenafil in the
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 16 of 18
treatment of neonates with persistent pulmonary hypertension. The Journal of Pediatrics.2009 155: 841-847
23. McNamara P, Shivananda S, Sahni M et al. Pharmacology of Milrinone in neonates with persistent pulmonary hypertension of the newborn and suboptimal response to inhaled nitric oxide. Paediatric critical care medicine. 2013 14; number 1: 74-83
24. Bassler D, Kreutzer K, McNamara P and Kirpalani H. Milrinone for persistent pulmonary hypertension of the newborn. The Cochrane Libray. November 2010
25. Ho J, Rasa G. Magnesium sulphate for persistent pulmonary hypertension of the newborn. The Cochrane Library. July 2007
26. Mohamed W and Ismail M. A randomized, double-blind, placebo controlled prospective study of bosentan for the treatment of persistent pulmonary hypertension of the newborn. Journal of perinatology 2012 32 (8): 608- 613
27. Nakwan N, Choksuchat D, Saksawad R et al. Successful treatment of persistent pulmonary hypertension of the newborn with bosentan. Acta Pediatrica 2009, 98: 1683-1685
28. UK Collaborative randomised trial of neonatal extracorporeal membrane oxygenation. UK collaborative ECMO Trial Group. Lancet 1996; 348: 75-82
29. Lazar D, Cass D, Darrell L et al. The use of ECMO for persistent pulmonary hypertension of the newborn: a decade of experience. The Journal of Surgical Research, 2012; 177(2): 263-267
30. Rohana N, Boo J, Chandran V et al. Neurodevelopmental outcomes of newborns with persistent pulmonary hypertension. Malaysian journal of Medical Science 2011; 18 (4): 58-62
31. Rosenberg A, Lee N, Vaver K et al. School-age outcomes of newborns treated for persistent pulmonary hypertension. Journal of perinatology 2010: 30 (2): 127-134
32. Lipkin P, Davidson D, Spivak L et al. Neurodevelopmental and medical outcomes of persistent pulmonary hypertension in term newborns treated with nitric oxide. Journal of Pediatrics 2002 140: 306-310
33. Peliowski A, Finer N, Etches et al. Inhaled nitric oxide for premature infants after prolonged rupture of membranes. Journal of paediatrics 1995; 126: 450-453
34. Barrington K, Finer N. Inhaled nitric oxide for respiratory failure in preterm infants. Cochrane Database of Systematic Reviews 2010.
35. Chock V, Van Meurs K. Inhaled nitric oxide for premature prolonged rupture of membranes, oligohydramnios and suspected pulmonary hypoplasia: PiNO
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 17 of 18
Trial Results. American Journal of Perinatology; 2009: 26 (4) 317-322
36. Askie L, Ballard R, Cutter G et al. Inhaled Nitric oxide in preterm infants: an individual-patient data meta-analysis of randomised trials. Pediatrics 2011; 128: 729-739
37. Christenson J, Lavoie A, O Connor M, Bhorade S et al. The incidence and pathogenesis of cardiopulmonary deterioration after abrupt withdrawal of inhaled nitric oxide. Am Journal of Resp Crit Care Med 200: 161 (5): 1443-1449
38. Aly H, Sahni R, Wung J. Weaning strategy with inhaled nitric oxide treatment in persistent pulmonary hypertension of the newborn. Arch Dis Child Fetal Neonatal Ed. 1997; 76 (2): F118-F122
39. Shah P, Ohlsson A. Sildenafil for pulmonary hypertension in neonates. The Cochrane Library; 2011
40. DiBlasi R, Myers T and Hess D. Evidence based clinical practice guideline: Inhaled Nitric Oxide for Neonates with Acute Hypoxic Respiratory Failure. AARC Clinical Practice Guideline. Respiratory Care, December 2010; volume 55 no 12
41. Skinner J, Hunter S, Hery EN. Haemodynamic features at presentation in persistent pulmonary hypertension of the newborn and outcome. Archives Disease in Childhood 1996; 74 F 26-32
42. Skinner J, Alverson D, Hunter S. Echocardiography for the neonatologist. 2000.
43. Extracorporeal Membrane Oxygenation in PICU. Practice Guideline. The Children’s Hospital Westmead.
44. Musewe N, Poppe Delores, Smallhorn J. Doppler Echocardiographic measurement of pulmonary artery pressure from ductal Doppler velocities in the newborn. J Am Coll Cardiology 1990; 15: 446-456
45. Legislative Compliance: Organisation, Management and Staff Obligations – Governing Body and Management manual, Policy Number 2.7.1
46. Code of Conduct – Governing Body and Management Manual, Policy
Number 1.1
47. Governing Body and Management Manual Section 4: Human Resources Management – http://intranet.cs.nsw.gov.au/SSWPolicies/default.htm
48. Lakshminrusimha S, Swartz D, Gugino S et al. Oxygen concentration and pulmonary hemodynamics in newborn lambs with pulmonary hypertension. Pediatric Research 2009; volume 66, no 5.