PORPHYRIA ERYTHROPOIETICA JOHN RAYNE,F.D.S., D.Orth., R.C.S. Department of Oral Surgery, United Oxford Hospitals THEporphyrias are disorders ofporphyrinmetabolism characterised by an excessively high level of circulating uroporphyrin and coproporphyrin. The pigments may be demonstrated in the urine, and deposited in the tissues, including the skin, and the bones. The division into erythropoietic and hepatic porphyrias is of fundamental importance (Schmid et al., 1954). In erythropoietic porphyria, the defect is situated in the bone marrow, where there is a block in the synthesis of haem at the (intermediate) porphyrin stage. The hepatic porphyrias are characterised by the partial inability of the liver to break down porphyrins. The hepatic porphyrias include: acute intermittent, or Swedish, porphyria; porphyria cutanea tarda; mixed, or South African, porphyria; and porphyria cutanea tarda symptomatica (Rimington, I962). There remains haematoporphyrinuria due to intoxication, for example in cases of lead poisoning. Porphyria erythropoietica, or congenital porphyria, or Gunther's disease, is a rare condition of unknown aetiology. Goldberg and Rimington (1962) summarised 5° cases. A further 14 cases have been reported (Varadi, I958; Larizza, I962; Vogulkina & Siniavskaia, 1962; Heilmeyer et al., I963; Pecorella, I963; Chatterjea, 1964; Gross, 1964; Handa, I965). A full report on the general management of this case will appear elsewhere (Kaufman et al., 1966). The standard reference works in the dental literature do not refer to the condition. Gorlin and Pindborg (I964) refer to porphyria erythropoietica in the differential diagnosis of epidermolysis bullosa. Tiecke (1965) is alone in giving a full account and an illustration. It has been suggested that these unfortunate individuals have given rise to the legend of the werwolf (Illis, I964). Their hairy faces, claw-like hands, red teeth, and intermittent mental derangement have, in the primitive mind, imbued them with evil supernatural powers. The red teeth suggest a diet of blood, and photo- sensitivity of the skin leads to nocturnal rather than daytime sorties. The characteristic features of the condition are bullous lesions on the exposed areas producing scarring and deformity, corneal ulceration, ulceration and degenera- tion of cartilage, pigmented teeth, hypertrichosis, hyper-pigmentation of the skin, and haemolytic anaemia with splenic enlargement. The condition is hereditary, being transmitted by an autosomal recessive gene. Photosensitivity is due to deposition of uroporphyrin in the skin. The photo- sensitivity appears early in infancy, in contrast to porphyria cutanea tarda. The sufferers rarely present with abdominal or neurological symptoms, in contrast to acute intermittent porphyria. The normoblasts and some of the erythrocytes fluoresce when exposed to ultraviolet light. This fluorescence is characteristic of porphyrins, and may be demonstrated in the urine, in the teeth, and in the bones post-mortem. 68
Transcript
PORPHYRIA ERYTHROPOIETICA
JOHN RAYNE, F.D.S., D.Orth., R.C.S. Department of Oral Surgery, United Oxford Hospitals
THEporphyrias are disorders ofporphyrinmetabolism characterised by an excessively high level of circulating uroporphyrin and coproporphyrin. The pigments may be demonstrated in the urine, and deposited in the tissues, including the skin, and the bones.
The division into erythropoietic and hepatic porphyrias is of fundamental importance (Schmid et al., 1954). In erythropoietic porphyria, the defect is situated in the bone marrow, where there is a block in the synthesis of haem at the (intermediate) porphyrin stage. The hepatic porphyrias are characterised by the partial inability of the liver to break down porphyrins. The hepatic porphyrias include: acute intermittent, or Swedish, porphyria; porphyria cutanea tarda; mixed, or South African, porphyria; and porphyria cutanea tarda symptomatica (Rimington, I962).
There remains haematoporphyrinuria due to intoxication, for example in cases of lead poisoning.
Porphyria erythropoietica, or congenital porphyria, or Gunther's disease, is a rare condition of unknown aetiology. Goldberg and Rimington (1962) summarised 5 ° cases. A further 14 cases have been reported (Varadi, I958; Larizza, I962; Vogulkina & Siniavskaia, 1962; Heilmeyer et al., I963; Pecorella, I963; Chatterjea, 1964; Gross, 1964; Handa, I965). A full report on the general management of this case will appear elsewhere (Kaufman et al., 1966). The standard reference works in the dental literature do not refer to the condition. Gorlin and Pindborg (I964) refer to porphyria erythropoietica in the differential diagnosis of epidermolysis bullosa. Tiecke (1965) is alone in giving a full account and an illustration.
It has been suggested that these unfortunate individuals have given rise to the legend of the werwolf (Illis, I964). Their hairy faces, claw-like hands, red teeth, and intermittent mental derangement have, in the primitive mind, imbued them with evil supernatural powers. The red teeth suggest a diet of blood, and photo- sensitivity of the skin leads to nocturnal rather than daytime sorties.
The characteristic features of the condition are bullous lesions on the exposed areas producing scarring and deformity, corneal ulceration, ulceration and degenera- tion of cartilage, pigmented teeth, hypertrichosis, hyper-pigmentation of the skin, and haemolytic anaemia with splenic enlargement. The condition is hereditary, being transmitted by an autosomal recessive gene.
Photosensitivity is due to deposition of uroporphyrin in the skin. The photo- sensitivity appears early in infancy, in contrast to porphyria cutanea tarda. The sufferers rarely present with abdominal or neurological symptoms, in contrast to acute intermittent porphyria. The normoblasts and some of the erythrocytes fluoresce when exposed to ultraviolet light. This fluorescence is characteristic of porphyrins, and may be demonstrated in the urine, in the teeth, and in the bones post-mortem.
68
P O R P H Y R I A E R Y T H R O P O I E T I C A 69
CASE R E P O R T
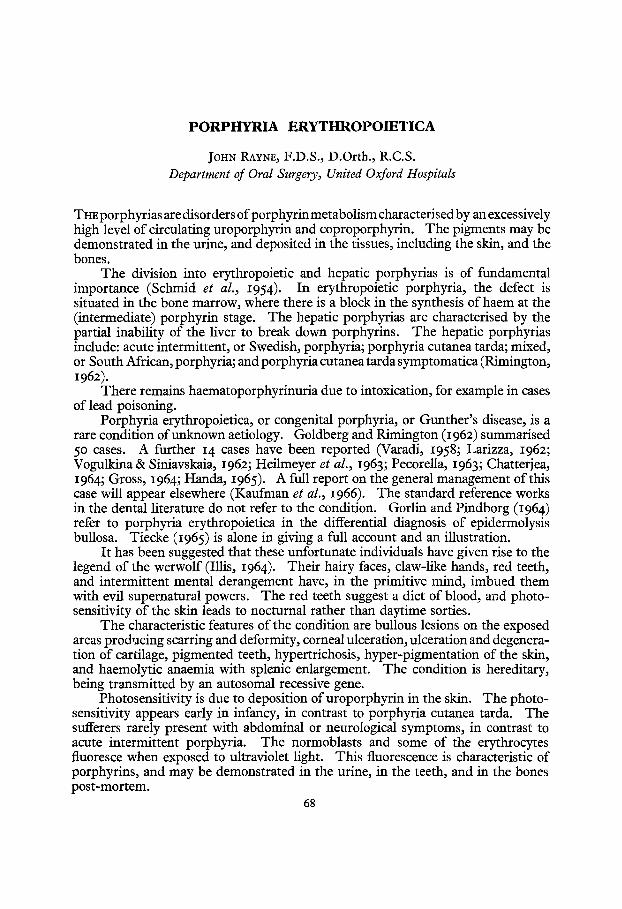
The patient, a I7-year-old girl, has been referred for dental assessment on various occasions since the diagnosis was made at the age of 6 months.
On exposure to direct sunlight, blisters form in the skin which subsequently break down and become infected. The eyelashes are very long, and the face is hairy. The scalp hair is patchy in distribution, and she wears a wig. Ulceration and infection have resulted in loss of the tip of the nose, and the face is disfigured by pitted scars. All the finger-nails have been lost, and the fingers are bent and deformed by scar tissue.
Anaemia has always been present, and does not respond to routine measures. She suffered a severe haemolytic anaemia when she was IO years of age, and an emergency
FIG. I Colour photograph of the patient with white flashlight.
splenectomy was performed. Following the splenectomy, a thrombocytosis developed, and bilateral deep leg vein thrombosis occurred three years later. Corneal ulcers have resulted in her vision being partially obscured by scar tissue.
Mental disturbance has not been a feature of this case, and she was able to attend a village school for several years. In spite of the deformity of her hands she can still use a fork. I t has not been possible to study the genealogy in this case.
Den ta l Condi t ion. The deciduous teeth erupted normally. They were pink in colour. Most of them were exfoliated naturally, but several molars were extracted because of carious exposure, and some deciduous incisors were removed because of delayed eruption of the permanent successors.
The permanent teeth are normal in form. At first they were a dark reddish pink, but the colour has changed to a brownish pink (Fig. i). The incremental lines are easily seen, being accentuated by pigment deposition. The teeth show the characteristic red
7 ° BRITISH JOURNAL OF ORAL SURGERY
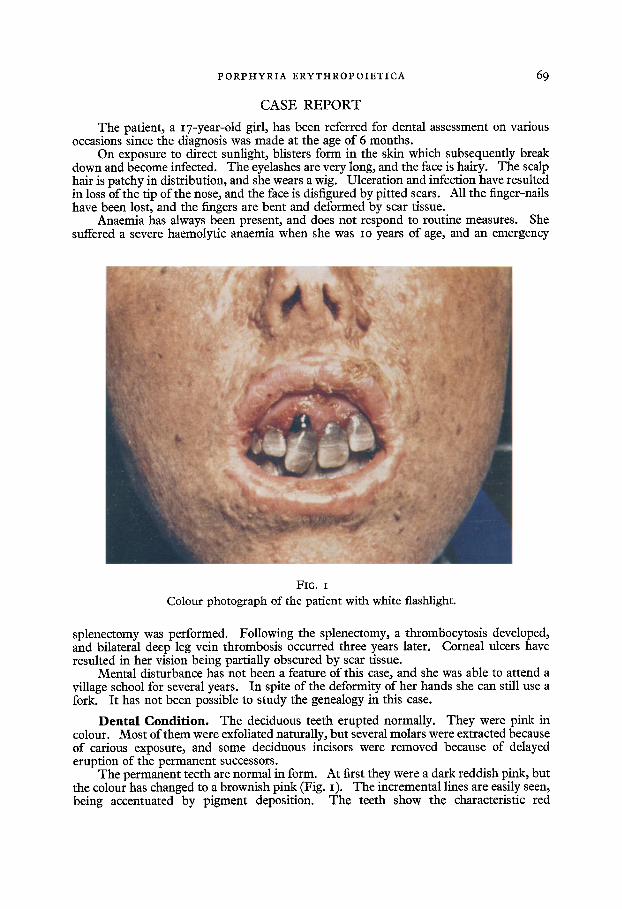
FIG. 2
T h e same subject photographed with ultraviolet light.
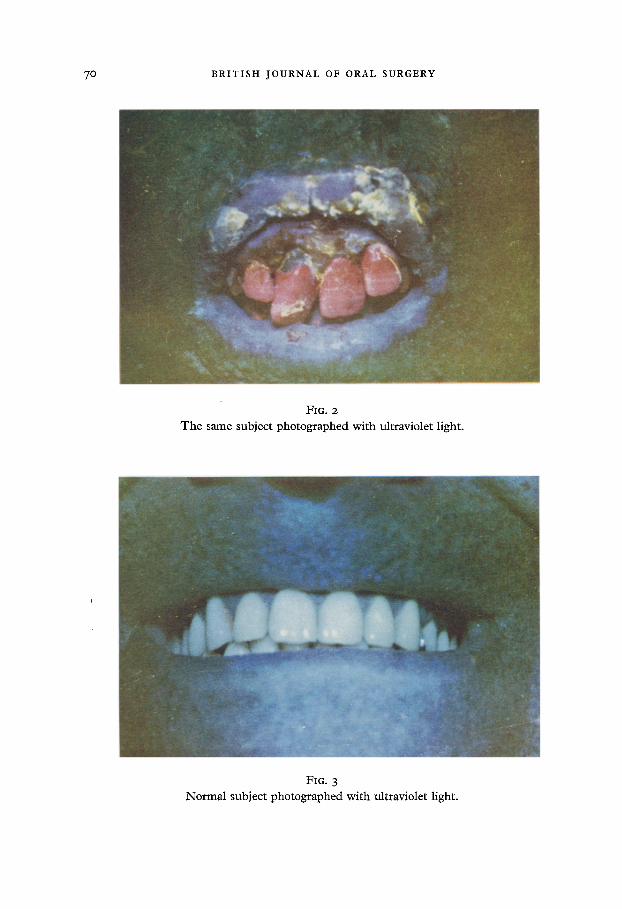
FIG. 3
Norma l subject photographed with ultraviolet light.
P O R P H Y R I A E R Y T H R O P O I E T I C A 7 I
fluorescence of porphyrins (Fig. 2), in contrast to the blue fluorescence of normal teeth (Fig. 3)- The roots of the extracted teeth are a dark indigo colour, and this colour may also be seen at the neck of the right maxillary central incisor tooth, where parodontal recession has occurred.
Irregularity of the incisors is made worse by the form of the upper lip. Scarring of the lip has resulted in the formation of a fight fibrous band which constricts the apices of these teeth. The lack of lip seal has resulted in a failure to restrain mesial drift of the posterior teeth, and crowding is passed on to the incisor region. At the same time the shortness of the upper lip attracts the attention to the deformity of the teeth.
The lips are inextensible and very fragile. In active opening the incisor teeth can be separated by a few millimetres only. The fragility of the rigid lips prevents any con- servative measures on the teeth, even to the extent of brushing them. The only dental treatment that has been carried out is the extraction of painful decayed teeth with endotracheal anaesthesia. The lip has been ruptured by light trauma during extraction of teeth. The lip was sutured and healed normally. Healing of the sockets has been normal.
The induction agent in the anaesthetics was Halothane, as barbiturates are contra- indicated in the porphyrias. It has been shown that an attack may be induced in a subject susceptible to acute intermittent porphyria. I f barbiturates are given to an established case, paralysis may occur (Goldberg & Rimington, I962 ).
Ward (I965) considers complications of pentothal administration in porphyrics to be a rare occurrence. In his retrospective survey of over 6oo,ooo routine anaesthetics, no case of porphyria appeared subsequent to the administration of single doses of sodium pentothal. Thirty-six porphyrics were given pentothal and no complications ensued. Two cases of respiratory paralysis were seen where barbiturates had been administered to porphyrics for long periods.
There have been repeated requests to improve the appearance of the front teeth. Neither orthodontic treatment nor crowns on the upper incisors have been advised because of the poor oral hygiene and lack of lip seal. The stability of dentures is likely to be poor because of the lack of tone in the oral musculature, even if adequate impressions could be taken.
I N V E S T I G A T I O N S OF T H E E X T R A C T E D T E E T H
Histological examination of a decalcified maxillary permanent molar disclosed a coronal abscess in the pulp and deposition of pigment in the dentine.
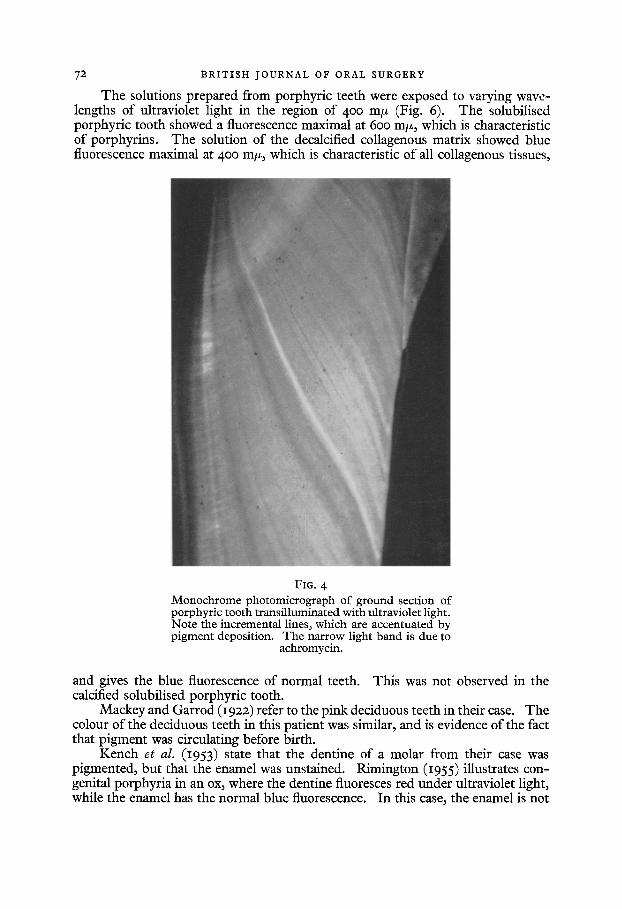
A ground section of a mandibular premolar was examined using ultraviolet light (Fig. 4). Light and dark bands of fluorescence are seen in the dentine, corresponding with varying rates of deposition of inorganic salts. Th e enamel fluoresces deep red. There is a band of yellow fluorescence which results from the administration of achromycin when the patient was Io years of age.
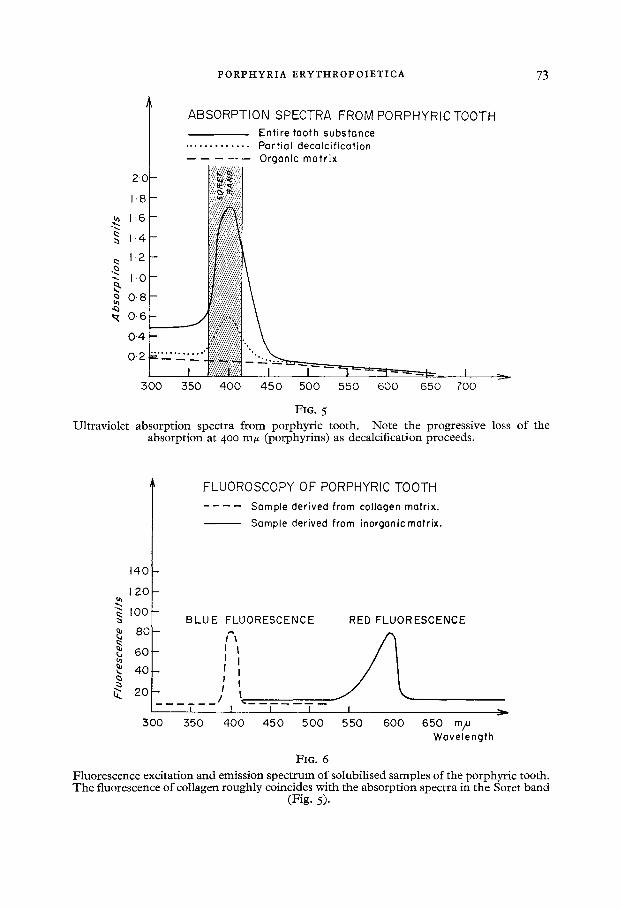
Spectrophotometric investigations of solutions of porphyrins show charac- teristic ultraviolet absorption maxima at about 400 m/z wavelength (the Soret band). No such absorption can be demonstrated in normal teeth. Progressive loss of the absorption at 400 m/z was shown to occur as decalcification proceeds, and this absorbing substance is absent from the organic residue when decalcification is complete (Fig. 5). F rom these observations, it may be inferred that the porphyrins are deposited in the mineral phase, and are not found in the collagenous matrix. No attempt was made to separate enamel from dentine, to establish whether there was a difference in porphyrin distribution. Nor is it possible by this method to differentiate uroporphyrin and coproporphyrin, as they behave in like manner.
72 BRITISH JOURNAL OF ORAL SURGERY
The solutions prepared from porphyric teeth were exposed to varying wave- lengths of ultraviolet light in the region of 400 m/z (Fig. 6). The solubilised porphyric tooth showed a fluorescence maximal at 600 m/z, which is characteristic of porphyrins. The solution of the decalcified collagenous matrix showed blue fluorescence maximal at 4o0 m/z, which is characteristic of all collagenous tissues,
FIG. 4 Monochrome photomicrograph of ground section of porphyric tooth transilluminated with ultraviolet light. Note the incremental lines, which are accentuated by pigment deposition. The narrow light band is due ~o
achromycin.
and gives the blue fluorescence of normal teeth. This was not observed in the calcified solubilised porphyric tooth.
Mackey and Garrod (i922) refer to the pink deciduous teeth in their case. The colour of the deciduous teeth in this patient was similar, and is evidence of the fact that pigment was circulating before birth.
Kench et al. (1953) state that the dentine of a molar from their case was pigmented, but that the enamel was unstained. Rimington (I955) illustrates con- genital porphyria in an ox, where the dentine fluoresces red under ultraviolet light, while the enamel has the normal blue fluorescence. In this case, the enamel is not
PORPHYRIA ERYTHROPOIETICA 73
i ABSORPTION SPECTRA FROM PORPHYRIC TOOTH Entire tooth substance
FIG. 5 Ultraviolet absorption spectra from porphyric tooth. Note the progressive loss of the
absorption at 400 mff (porphyrins) as decalcification proceeds.
140
120 -
IOG-
• 8 0 -
~ 6 0 -
~. 4 0 -
~. 2 o - I
3OO 550
FLUOROSCOPY OF PORPHYRIC TOOTH Sample derived from collagen matrix.
Sample derived from inorganic matrix.
BLUE FLUORESCENCE RED FLUORESCENCE
i I i I I ! ! !
I / t I I I I
400 450 500 550 600 650 mp Wavelength
FIG. 6 Fluorescence excitation and emission spectrum of solubilised samples of the porphyric tooth. The fluorescence of collagen roughly coincides with the absorption spectra in the Soret band
(Fig. 5).
74 BRITISH JOURNAL OF ORAL S U R G E R Y
as deeply pigmented as the dentine, but it fluoresces a more brilliant red. T h e exposed neck of the central incisor does not fluoresce under ultraviolet light. This variability in behaviour of calcified tissues may be due to different concentrations of pigment; it may be due to different wavelengths of ultraviolet light; or it may be due to an interference factor in the structure of the mineralised matrix. T h e precise cause is not understood.
S U M M A R Y
A case of erythropoietic porphyria is presented. T h e characteristic features are infected bullae, leading to pitted scars; ulcera-
tion and loss of extremities of nose and fingers; hypertrichosis, hyperpigmentation, and photosensitivity of the skin; pigmentation of the teeth.
Conservative dental treatment is impossible, because of the fragility of the rigid lips.
Barbiturates are contra-indicated.
ACKNOWLEDGEMENTS
The author is grateful to Dr. H. R. Viekers and Mr. D. S. Hayton-Williams, for their permission to publish this case; to Professor H. J. ft. Blackwood, and Miss H. J. Horsley, of the Royal Dental Hospital, for the investigations of the teeth; to the Department of Human Anatomy, University of Oxford, for the illustrations.
The author also acknowledges a grant made by the United Oxford Hospitals Research Fund to cover the cost of colour illustrations.
REFERENCES
CHATTERJEA, J. B. (1964). Blood, 24, 806. GOLDBERG, A. & RIMINGTON, C. (1962). Diseases of Porphyrin Metabolism. Springfield:
Thomas. GORLIN, R. J. & PINDBORG, J. j. (1964). Syndromes of the Head and Neck. London:
McGraw-Hill. GROSS, S. (1964). Blood, 23, 762. HANDA, F. (1965). Archs Derm., Chicago, 91, 13o. HEILMEYER, L., CLOTTEN, R., KERP, L., MARKER, H., PARRA, C. A. & WETZEL, H. P. (1963).
Dr. reed. Wlschr. 88, 2449. ILLIS, L. (1964). Proc. R. Soc. iVied. 57, 23. KAUFMAN et al. (1966). In press. KENCH, J. E., LANGLEY, F. A. & WILKINSON, J. F. (I953). O. Jl Med. 46, 285. LARIZZA, P. (1962). Panminerva med., 4, 315. MACKEY, L. & GARROD, A. E. (1922). Q. Jl Med. 15, 319. PECORELLA, F. (1963). Pediatria, Napoli, 71, 1227. RIMINGTON, C. (1955). Endeavour, 14, 126. RIMINGTON, C. (1962). Panminerva med. 4, 307. SCHMID, R., SCHWARTZ, S. & WATSON, C. J. (1954)- Archs intern. Med. 93, 167. TIECKE, R. F. (1965). Oral Pathology. New York: McGraw-Hill. VARADI, S. (1958). Br. J. Haemat. 4, 270. VOGULKINA, T. E. & SINIAVSKAIA, O. A. (1962). Pediatriya, 41, 78. WARD, R. J. (1965). Anesthesiology, 26, 213.