39
Post-DDW OAG Course - Therapeutic Endoscopy Jeffrey Mosko Division of Gastroenterology St. Michael's Hospital University of Toronto [email protected] June 13, 2015
Post-DDW OAG Course - Therapeutic Endoscopy
Jeffrey Mosko Division of Gastroenterology
St. Michael's Hospital University of Toronto
June 13, 2015
Program Name: Post-DDW OAG course
! Medical Expert (as Medical Experts, physicians integrate all of the CanMEDS Roles, applying medical knowledge, clinical skills, and professional attitudes in their provision of patient-centered care. Medical Expert is the central physician Role in the CanMEDS framework.)
Communicator (as Communicators, physicians effectively facilitate the doctor-patient relationship and the dynamic exchanges that occur before, during, and after the medical encounter.)
Collaborator (as Collaborators, physicians effectively work within a healthcare team to achieve optimal patient care.)
Manager (as Managers, physicians are integral participants in healthcare organizations, organizing sustainable practices, making decisions about allocating resources, and contributing to the effectiveness of the healthcare system.)
Health Advocate (as Health Advocates, physicians responsibly use their expertise and influence to advance the health and well-being of individual patients, communities, and populations.)
Scholar (as Scholars, physicians demonstrate a lifelong commitment to reflective learning, as well as the creation, dissemination, application and translation of medical knowledge.)
Professional (as Professionals, physicians are committed to the health and well-being of individuals and society through ethical practice, profession-led regulation, and high personal standards of behaviour.)
CanMEDS Roles Covered in this Session:�
Financial Interest Disclosure (over the past 24 months)
No relevant financial relationships with any commercial interests
Name: Dr. Jeffrey Mosko�
Outline
1. Barrett’s/EMR – Hot avulsion in BE (Tu1573)
2. Colon/EMR – Water Immersion EMR (725)
– Prophylactic clips after EMR (330)
3. Gastric varices – EUS guided therapy for fundal varices (209)
Outline
1. Barrett’s/EMR – Hot avulsion in BE (Tu1573)
2. Colon/EMR – Water Immersion EMR (725)
– Prophylactic clips after EMR (330)
3. Gastric varices – EUS guided therapy for fundal varices (209)
Hot Avulsion
• Endoscopic Mucosal Resection (EMR) = standard of care for the management of colorectal, laterally spreading tumours (LST)
• Residual rates 1-14% – Higher in larger polyps
• Ablative techniques reserved for portions that are resistant to snaring – APC
– Snare-tip cautery (soft coag) Luigiano et al. Endoscopy 2009�Verrappan et al. GIE 2015�
Hot Avulsion
• Hot avulsion technique (Haber DDW 2014) – Hot biopsy forceps
– Slight tension
– Endocut (tapping)
• Verappan et al. – GIE 2014 – 20 patients undergoing HA for non-lifting areas
• 20/20 successful
• 15% recurrence
• No immediate/long-term AEs
Luigiano et al. Endoscopy 2009�Verrappan et al. GIE 2015�
Hot Avulsion
Tu1573 – Hot Avulsion Provides a Second Chance At Completing Barrett’s Eradication Background • Barrett’s + dysplasia requires complete eradication of
metaplastic columnar mucosa
Objective • Analyze the efficacy and safety of hot avulsion in this
setting Methods • Prospective, single centre, n = 18 • All patients undergoing routine f/u after undergoing
endoscopic Tx of BE-related dysplasia – No raised lesions – Islands/tongues < 1cm – Hot avulsion only Aranda-Hernandez et al. DDW
2015�
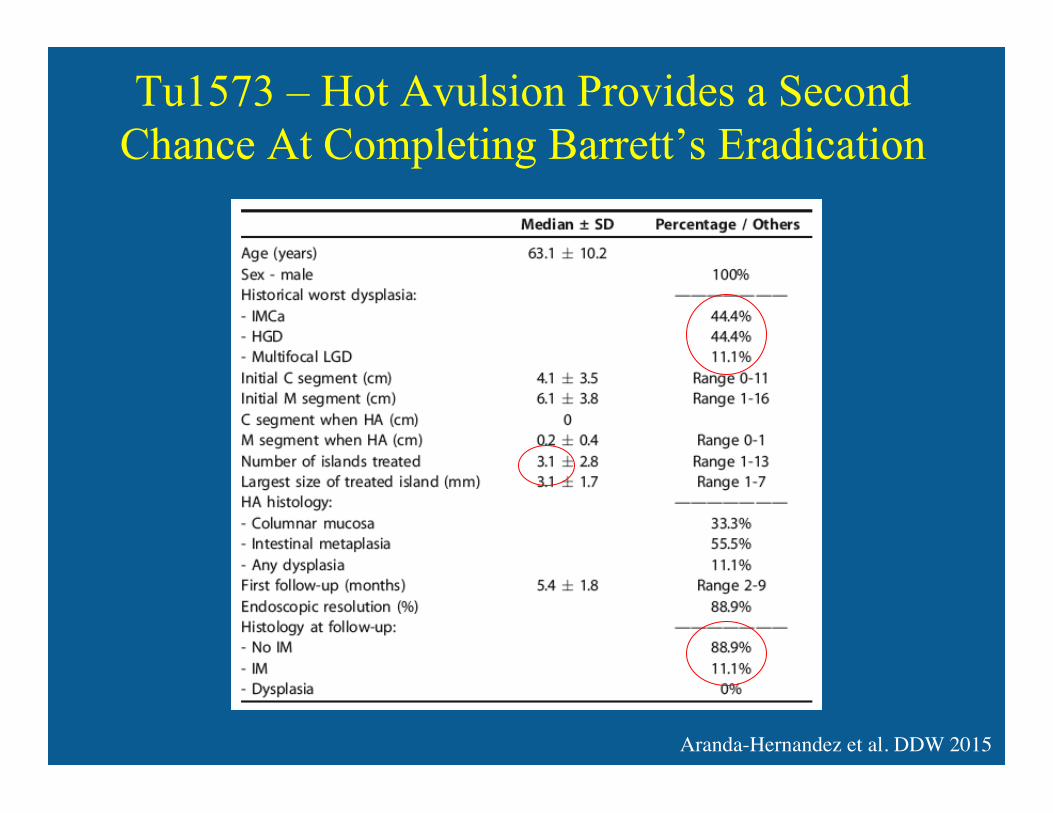
Tu1573 – Hot Avulsion Provides a Second Chance At Completing Barrett’s Eradication
Aranda-Hernandez et al. DDW 2015�
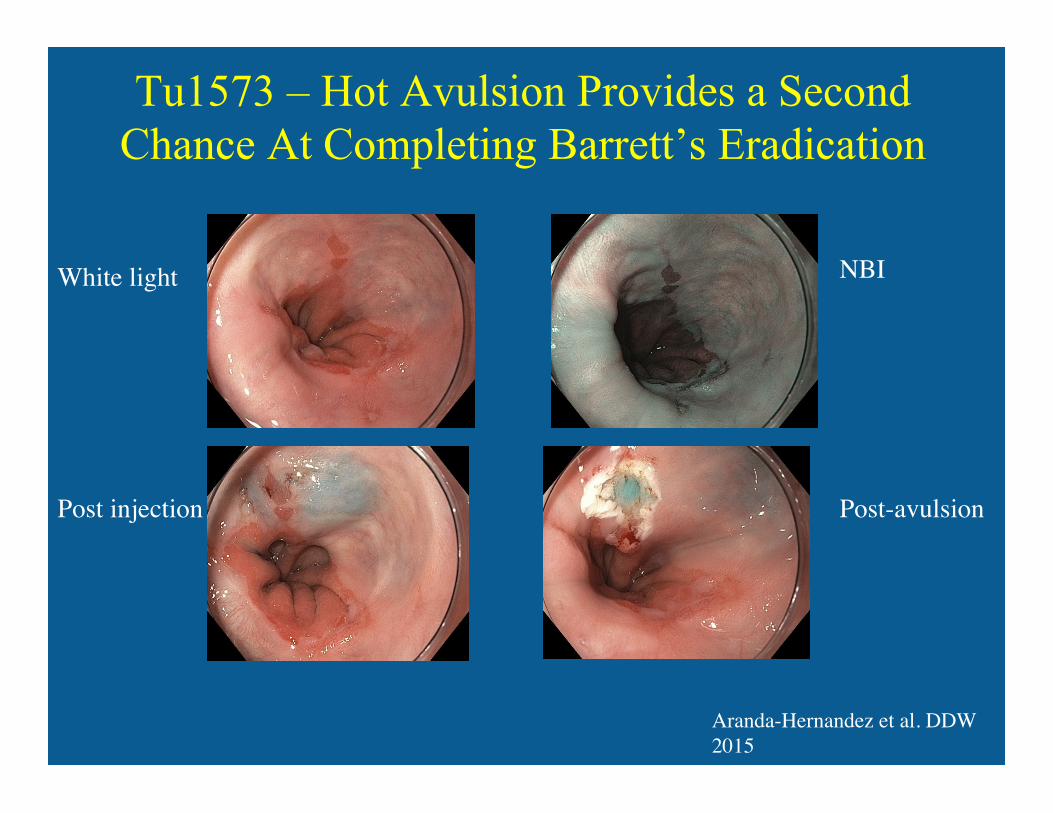
Tu1573 – Hot Avulsion Provides a Second Chance At Completing Barrett’s Eradication
Aranda-Hernandez et al. DDW 2015�
Post injection�
White light �
Post-avulsion�
NBI�
Tu1573 – Hot Avulsion Provides a Second Chance At Completing Barrett’s Eradication
Conclusions:
• Effective, safe and diagnostically useful for eradication of small residual BE areas after first line therapies for BE dysplasia
• Larger controlled studies needed
Aranda-Hernandez et al. DDW 2015�
Outline
1. Barrett’s/EMR – Hot avulsion in BE (Tu1573)
2. Colon/EMR – Water Immersion EMR (725)
– Prophylactic clips after EMR (330)
3. Gastric varices – EUS guided therapy for fundal varices (209)
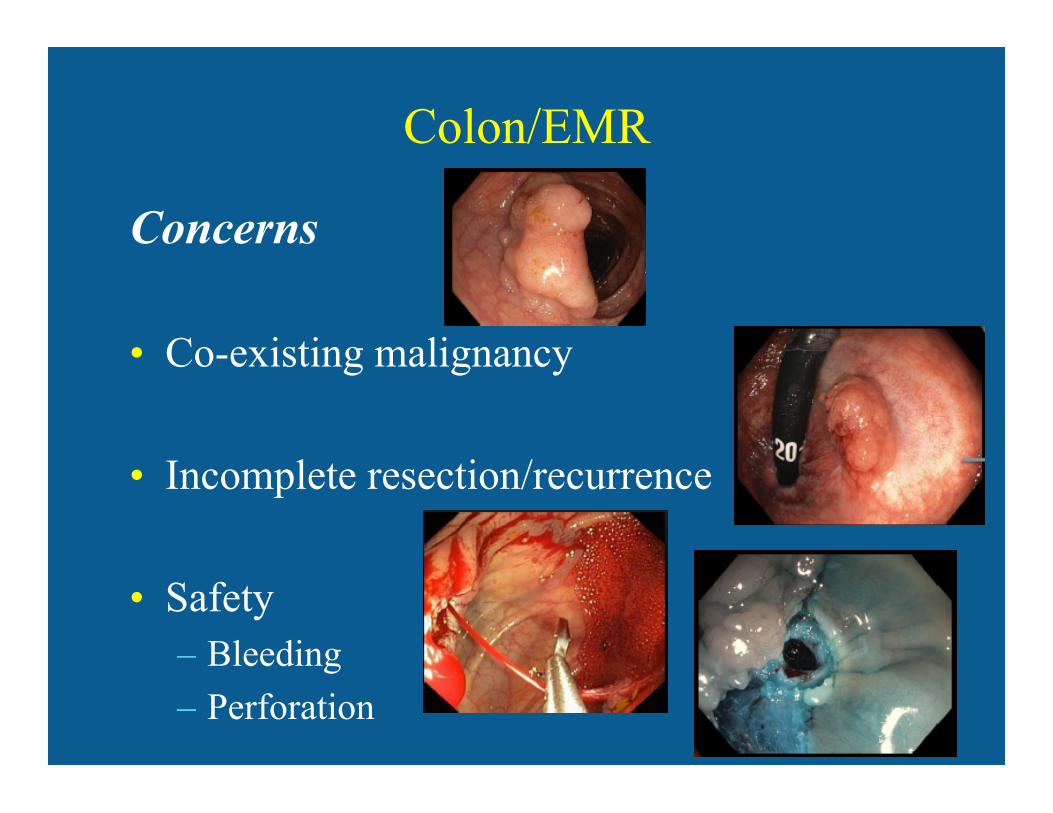
Colon/EMR
Concerns
• Co-existing malignancy
• Incomplete resection/recurrence
• Safety – Bleeding
– Perforation
Colon/EMR
Colon/EMR
Colon/EMR
Incomplete resection/recurrence • Khashab et al. GIE 2009
– 14 studies – Mean recurrence rate = 26%
• Pohl et al. - CARE study Gastro 2013 – Incomplete resection 7-23% – Risk factors:
• Size • Flat • Piecemeal resection • [Prior biopsy - Moss et al., Gastro 2011] • ?submucosal injection
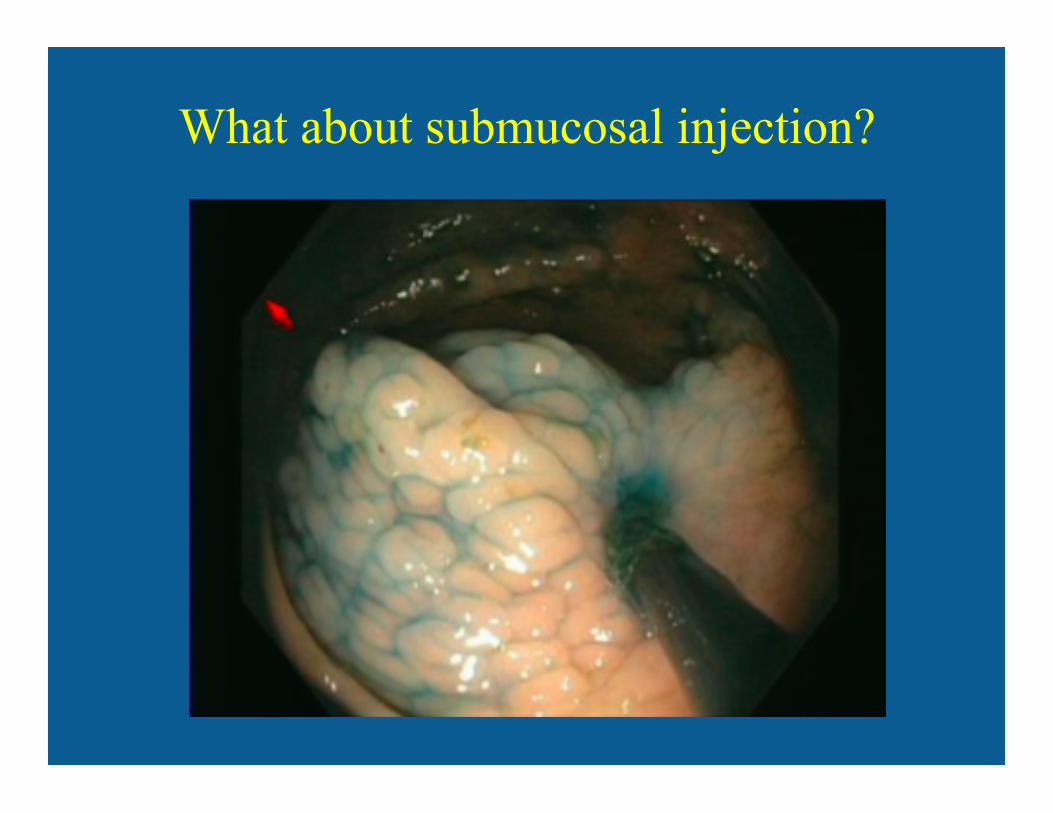
What about submucosal injection?
Underwater EMR
725 – Water Immersion Technique Polypectomy for Large Sessile Colorectal Polyps
• Retrospective, single centre, 2011-2013
• All UEMR
• Outcomes: – Feasibility
– Safety
– Effectiveness
• Results – N = 72 polyps removed via UEMR
Sandhu et al. DDW 2015�
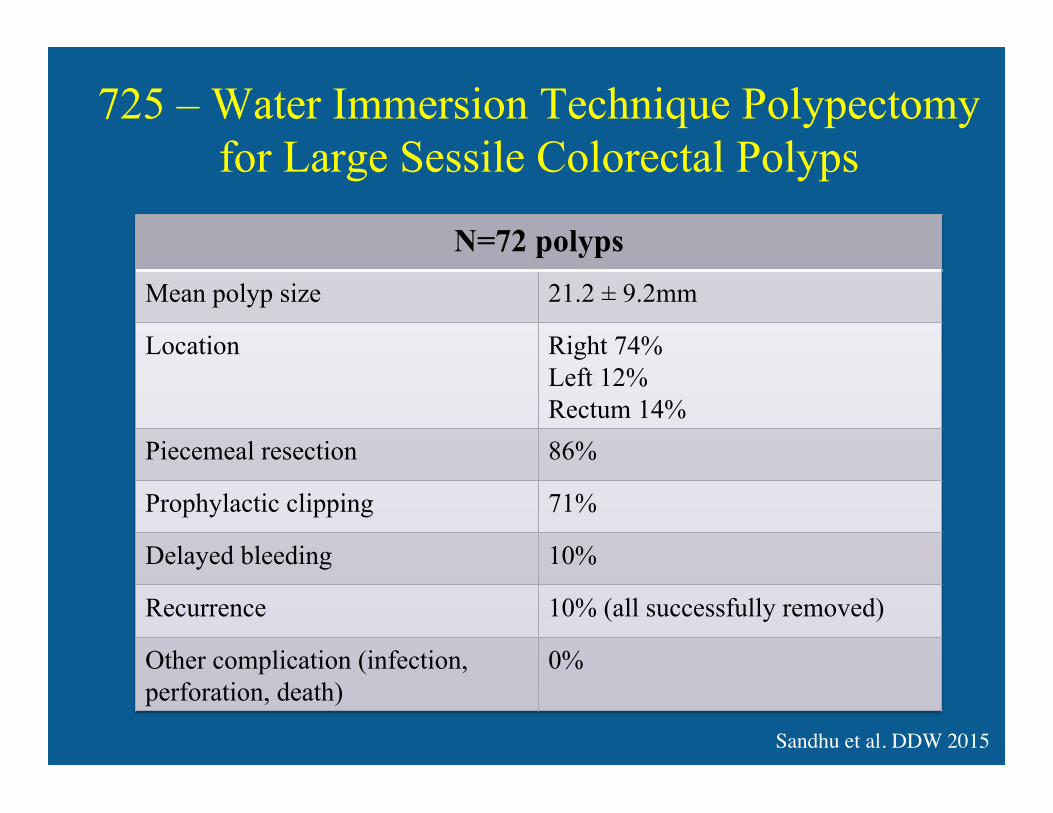
725 – Water Immersion Technique Polypectomy for Large Sessile Colorectal Polyps
N=72 polyps
Mean polyp size 21.2 ± 9.2mm
Location Right 74% Left 12% Rectum 14%
Piecemeal resection 86%
Prophylactic clipping 71%
Delayed bleeding 10%
Recurrence 10% (all successfully removed)
Other complication (infection, perforation, death)
0%
Sandhu et al. DDW 2015�
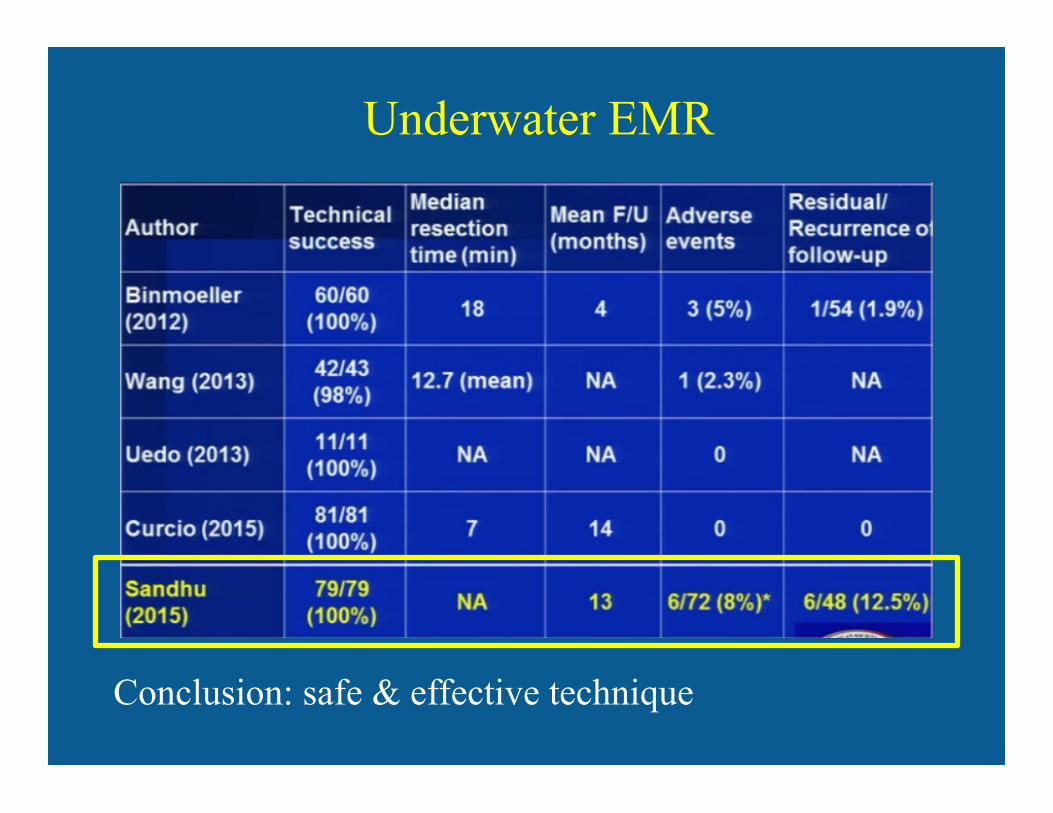
Underwater EMR
Conclusion: safe & effective technique
Colon/EMR
Bourke et al. ACE resection study group
• Now >2500 patients
• Intra-procedural bleeding – 10%
• Post-EMR bleeding 6-7% – 10-12% right colon
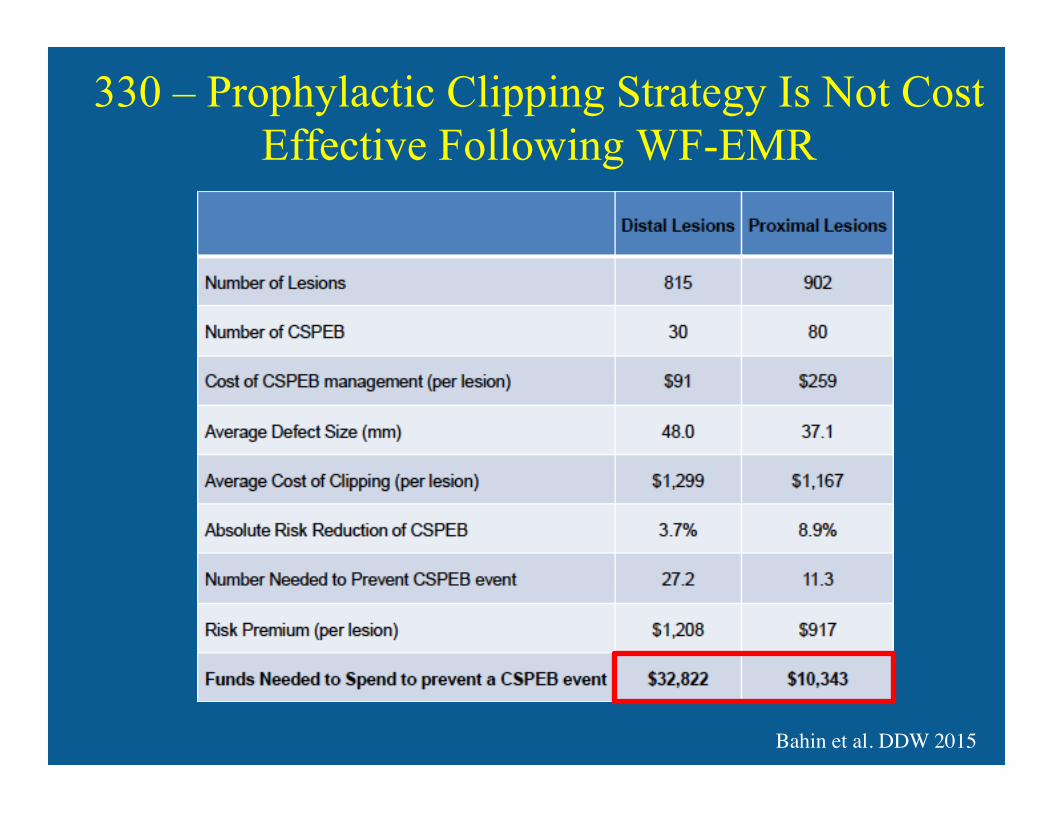
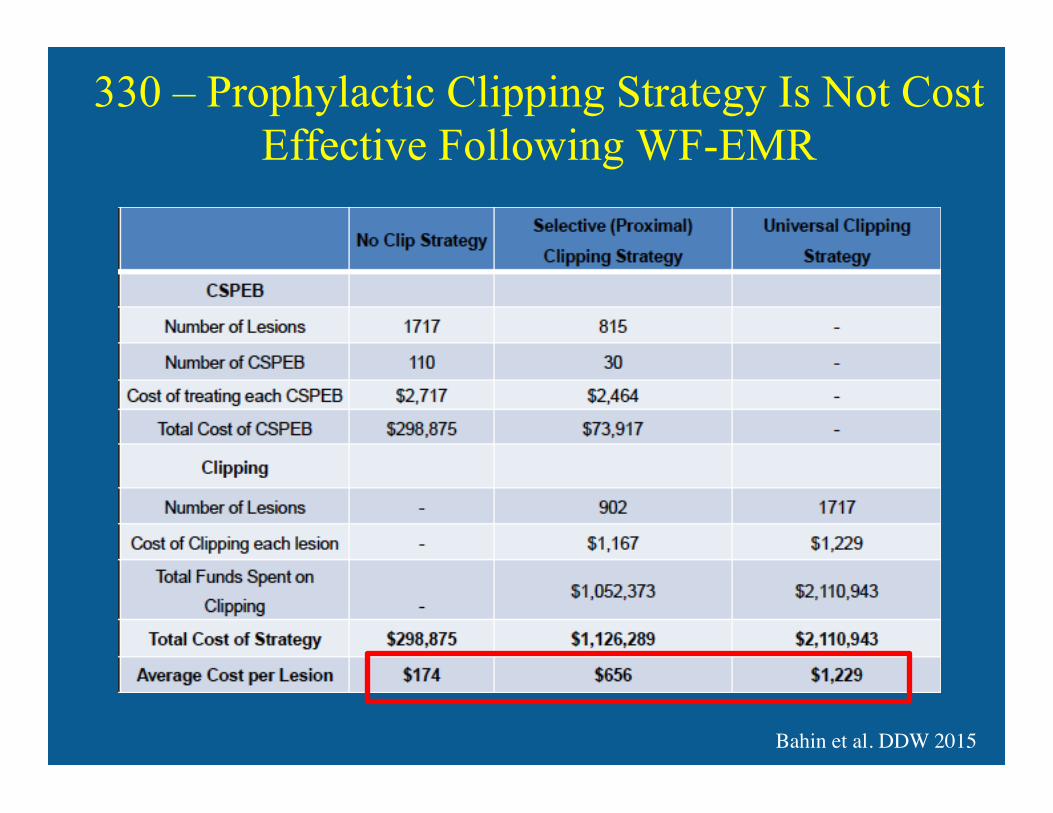
330 – Prophylactic Clipping Strategy Is Not Cost Effective Following WF-EMR
Background • Wide-field endoscopic mucosal resection (WF-
EMR) is an effective strategy for large sessile and laterally spreading colorectal lesions
• Clinically significant post EMR bleeding (CSPEB) = most common adverse event – 6-12% in proximal colon – High morbidity and resource utilization
• No proven therapies to prevent CSPEB
Bahin et al. DDW 2015�
330 – Prophylactic Clipping Strategy Is Not Cost Effective Following WF-EMR
Objective: • Determine cost-effectiveness of a prophylactic
clipping strategy for the prevention of CSPEB
Methods: • Economic modeling study • ACE study
– Prospective, observational – WF-EMR of LSL >20mm – Data @ procedure, 14d (telephone), 4mo - surveillance
colon • CSPEB = bleeding post-procedure requiring ER
visit, admission or repeat intervention Bahin et al. DDW 2015�
330 – Prophylactic Clipping Strategy Is Not Cost Effective Following WF-EMR
Results
• 1717 lesions – mean size 35.8mm
– 52.5% prox colon
• CSPEB rate 6.4% – Proximal 8.9%
– Distal 3.7%
– 45% required endoscopic management
Bahin et al. DDW 2015�
330 – Prophylactic Clipping Strategy Is Not Cost Effective Following WF-EMR
Bahin et al. DDW 2015�
330 – Prophylactic Clipping Strategy Is Not Cost Effective Following WF-EMR
Bahin et al. DDW 2015�
330 – Prophylactic Clipping Strategy Is Not Cost Effective Following WF-EMR
Bahin et al. DDW 2015�
330 – Prophylactic Clipping Strategy Is Not Cost Effective Following WF-EMR
Bahin et al. DDW 2015�
330 – Prophylactic Clipping Strategy Is Not Cost Effective Following WF-EMR
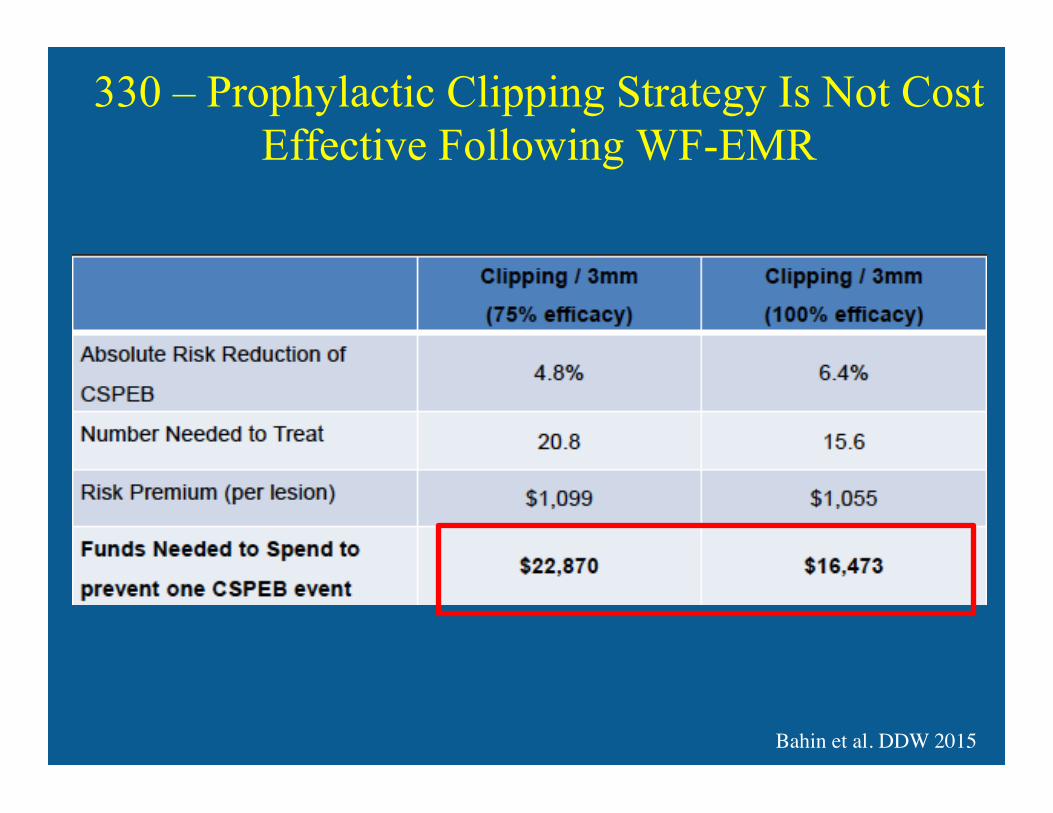
Conclusion:
• Funds needed to spend to prevent 1 CSPEB = $16,000 overall
• $33,000 distal colon
• $10,000 proximal colon
• Selective clipping strategy cheaper but still 4x > not clipping
• Clip price of $11.50 would result in cost-equivalence
Bahin et al. DDW 2015�
Outline
1. Barrett’s/EMR – Hot avulsion in BE (Tu1573)
2. Colon/EMR – Water Immersion EMR (725)
– Prophylactic clips after EMR (330)
3. Gastric varices – EUS guided therapy for fundal varices (209)
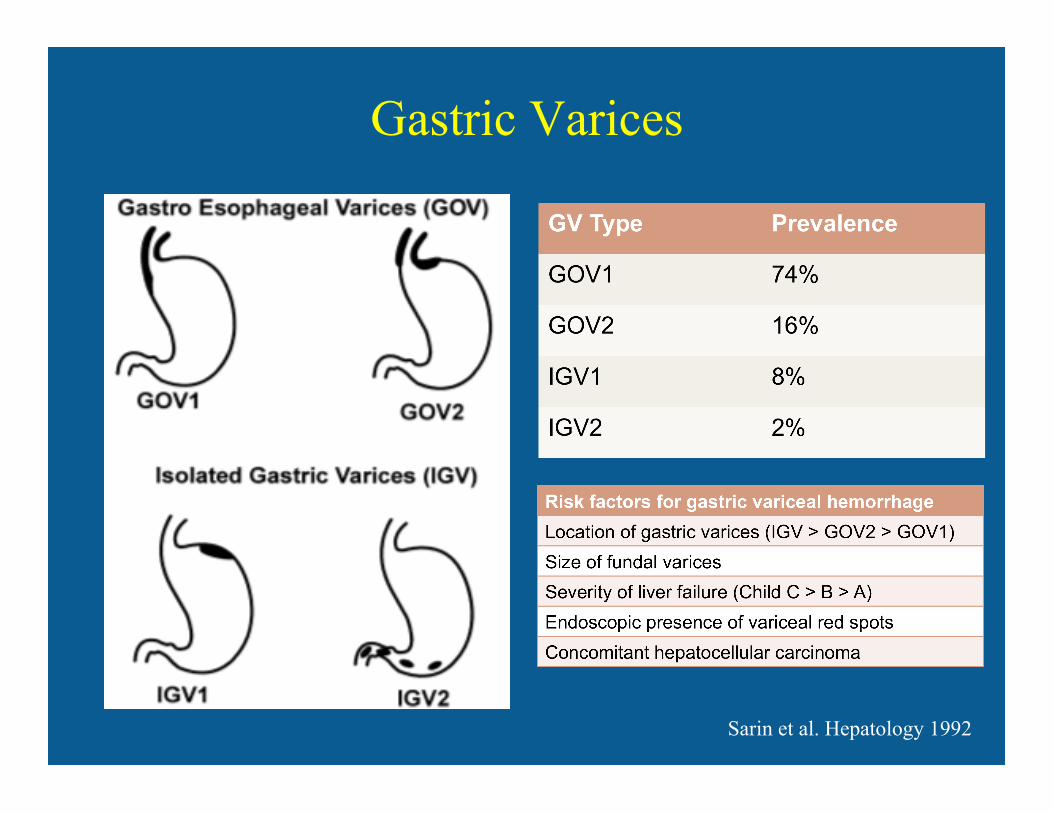
Gastric Varices
Sarin et al. Hepatology 1992
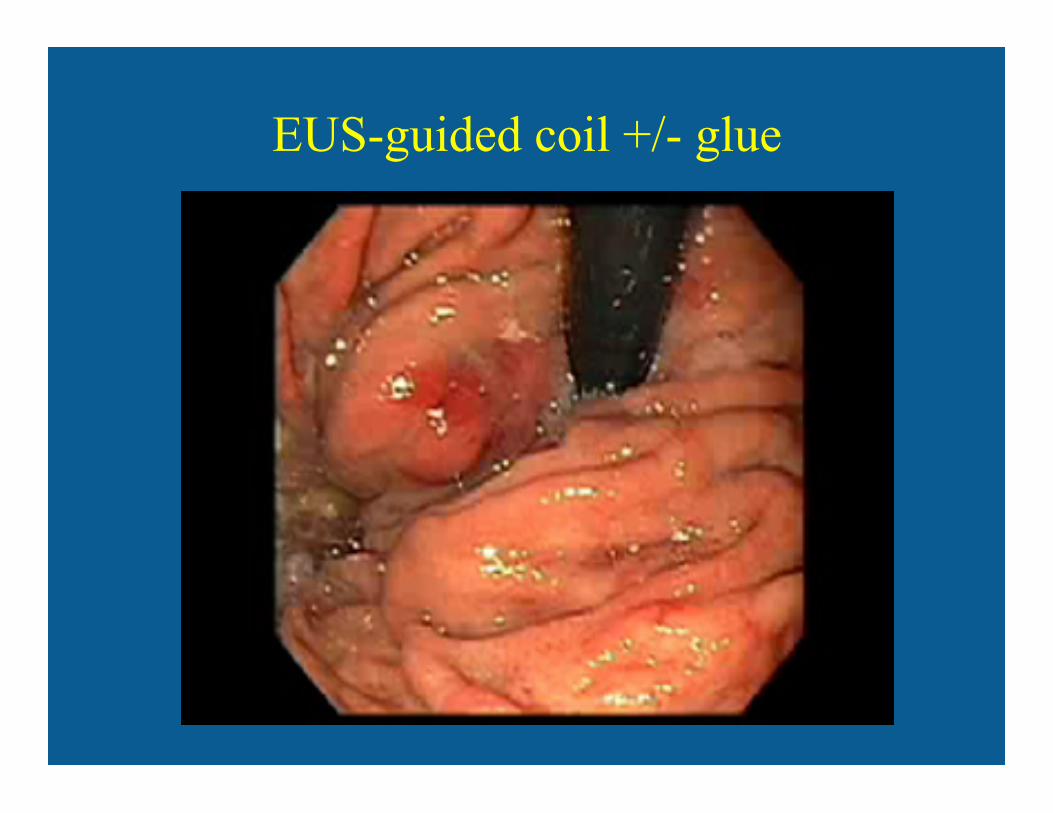
EUS-guided coil +/- glue
209 – EUS-guided treatment of gastric fundal varices with combined injection of coils and glue
Aim: • Evaluate long-term efficacy, safety and outcomes
of EUS guided therapy of GFV with combined coil and CYA injection
Methods • Retrospective, single centre, 2009-2015 • Inclusion:
– Active/recent GV bleed – High risk primary prophylaxis (GV >2cm on EUS)
Bhat et al. DDW 2015�
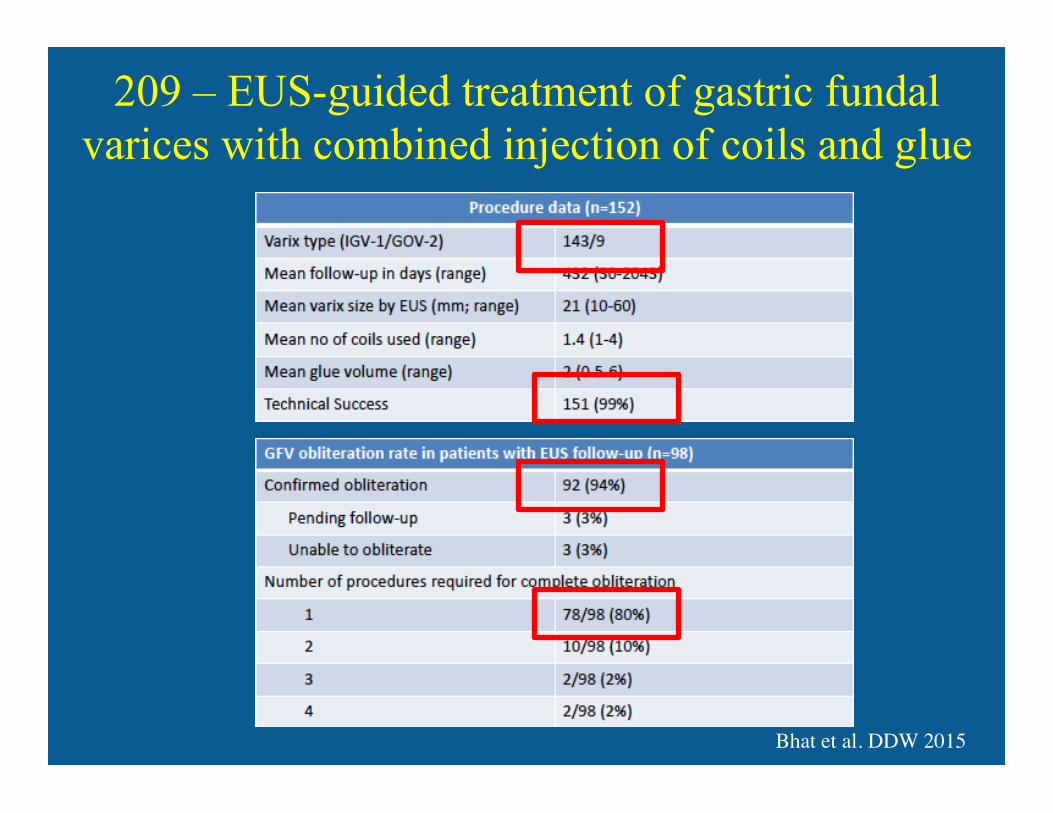
209 – EUS-guided treatment of gastric fundal varices with combined injection of coils and glue
Bhat et al. DDW 2015�
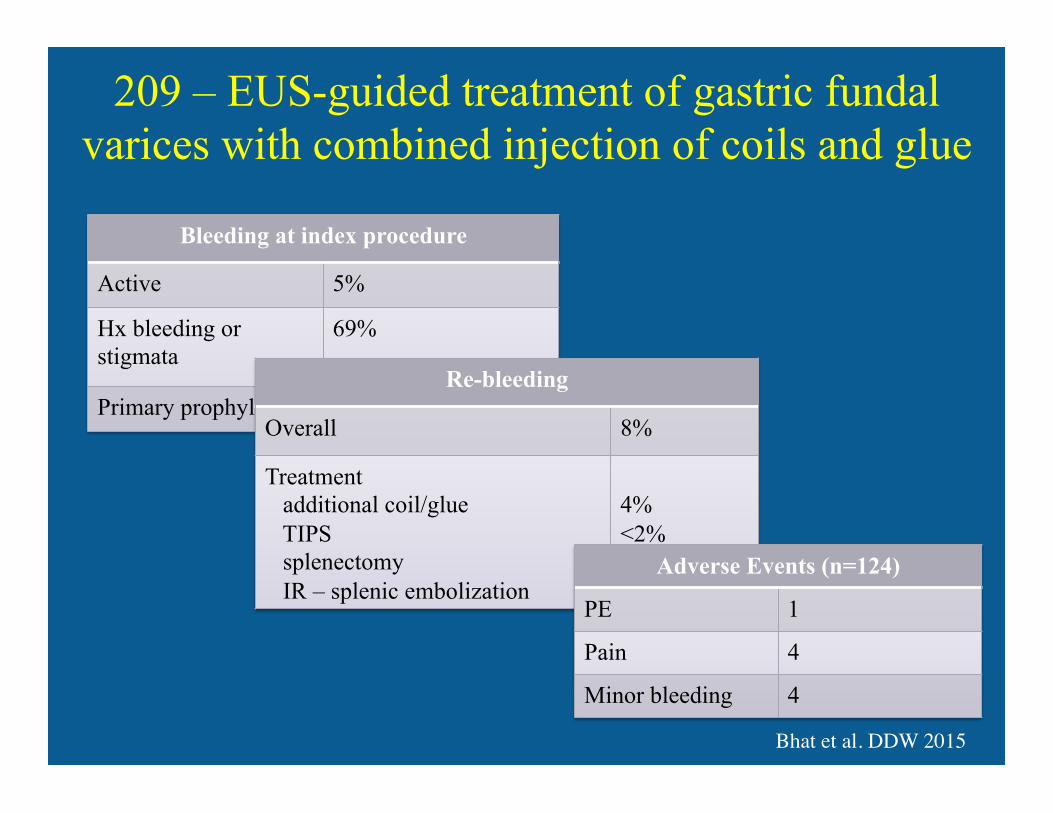
209 – EUS-guided treatment of gastric fundal varices with combined injection of coils and glue
Bhat et al. DDW 2015�
Bleeding at index procedure
Active 5%
Hx bleeding or stigmata
69%
Primary prophylaxis 26% Re-bleeding
Overall 8%
Treatment additional coil/glue TIPS splenectomy IR – splenic embolization
4% <2% <2% <1%
Adverse Events (n=124)
PE 1
Pain 4
Minor bleeding 4
209 – EUS-guided treatment of gastric fundal varices with combined injection of coils and glue
Conclusions: • Highly effective for hemostasis
– Active bleeding – Primary + secondary prophylaxis
• Low risk re-bleeding
• Safe – May reduce/eliminate risk of clinical relevant
CYA embolization
Bhat et al. DDW 2015�
QUESTIONS???

















