7
Post Operative Pain after Cholecystectomy: Conventional Laparoscopy Versus Single Incision Laparoscopic Surgery (SILS)
| Date post: | 07-May-2015 |
| Category: |
Health & Medicine |
| Upload: | apollo-hospitals |
| View: | 2,716 times |
| Download: | 0 times |

Post Operative Pain after Cholecystectomy: Conventional Laparoscopy Versus Single Incision Laparoscopic Surgery (SILS)

Original Article
INTRODUCTION
Laparoscopic cholecystectomy has replaced opencholecystectomy as the gold standard surgical procedurefor majority of patients of gall stone disease [1].Conventional laparoscopic Cholecystectomy is beingperformed using 4 ports. There was a continuous effort tominimize the number of ports, and finally single incisionlaparoscopic surgery (SILS) came into practice [2].
Single incision laparoscopic surgery is a rapidlyevolving method that is complementing traditionallaparoscopy in selected fields and patients [3,4]. It has alsobeen suggested as a bridge between traditionallaparoscopy and natural orifice transluminal endoscopicsurgery [5].
Single incision laparoscopic surgery utilizes three portsthrough the single skin incision at umbilicus [6]. It is beingconsidered as no scar surgery, because the incision isplaced within the umbilical scar that is not visible [7,8].SILS has also decreased post operative pain in somestudies [9]. Many special instruments [6] and ports [10,11]are available now for SILS. Technical modifications like
puppeteering of the gall bladder with a suture have beendone [12]. We however performed SILS cholecystectomyusing only conventional laparoscopic instruments. Thestudy compared SILS and conventional laparoscopiccholecystectomy for post operative pain.
METHODS
Study was done at Indraprastha Apollo Hospital, NewDelhi, India from 1st October 2009 to 31st March 2010.100 patients undergoing cholecystectomy forsymptomatic gall stones who were willing to be part ofthis comparison were included in the study. Patients wererandomized into two groups of 50 each.
Inclusion criteria
Patient with symptomatic cholelithiasis and fit forgeneral anesthesia
Exclusion criteria
Patient unwilling to participate in the study
Acute cholecystitis
Abnormal liver function tests
POST OPERATIVE PAIN AFTER CHOLECYSTECTOMY: CONVENTIONAL LAPAROSCOPY
VERSUS SINGLE INCISION LAPAROSCOPIC SURGERY (SILS)
A Prasad, KA Mukherjee, S Kaul and M Kaur
Department of Minimal Access Surgery, Indraprastha Apollo Hospitals, Sarita Vihar, New Delhi 110 076, India.
Correspondence to: Dr Arun Prasad, Department of Minimal Access Surgery, Indraprastha Apollo Hospitals,Sarita Vihar, New Delhi 110 076, India.
e-mail: [email protected]
Background: This study was done to compare postoperative pain after cholecystectomy done by singleincision laparoscopic surgery (SILS) versus conventional four port laparoscopy. Methods: 100 patientsundergoing cholecystectomy for symptomatic gall stones who were willing to be part of this comparison wereincluded in the study. Patients were randomized into two groups of 50 each. Only conventional instrumentswere used in both groups to keep the cost of surgery same. No special ports, roticulating instruments or flexibletelescopes were used. Pain score was checked after 6 hours of surgery using a visual analogue score.Results: We observed that there was no statistically significant difference in overall post operative pain. But onfurther analysis, we found significant difference in post operative pain score in latter half of our series of SILSwhen compared to conventional laparoscopic cholecystectomy and also the first half of the SILS group. Therewas also significant difference between operative times in earlier and latter half of SILS. Conclusion: Singleincision laparoscopic surgery is a feasible and a promising method for cholecystectomy. It is possible to do thisprocedure with out using special equipment. Although there was no significant difference in overallpostoperative pain, there is a possibility that after the initial learning curve, when the operative time reduces,the postoperative pain may also decrease. More studies are needed.
Keywords: Laparoscopy, Cholecystectomy, Single Incision Laparoscopic Surgery (SILS).
Apollo Medicine, Vol. 7, No. 2, June 2010 124

Original Article
125 Apollo Medicine, Vol. 7, No. 2, June 2010
Fig.1
Contracted gall bladder on ultrasound
Thickened gall bladder wall on ultrasound
Suspicion of gall bladder carcinoma
While the above exclusion criteria are not alwayscontraindications for laparoscopic cholecystectomy, theywere excluded from the study as the focus was on postoperative pain and not feasibility in difficult operativesituations which could be the topic of a future study oncethe benefits are established.
The name of the procedure was kept in a sealedenvelope that was opened after the patient wasanaesthetized. Only conventional instruments were usedin both groups to keep the cost of surgery same. No specialports, roticulating instruments or flexible telescopes wereused.
A standard 4 port cholecystectomy was done for theconventional group.
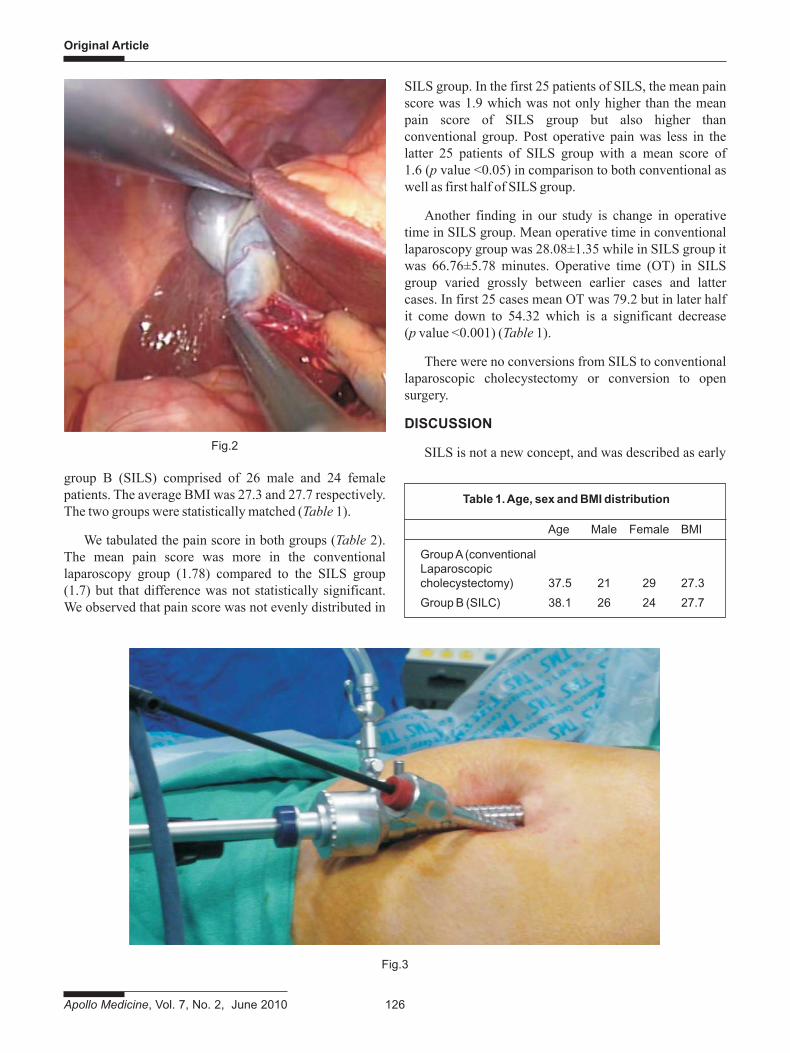
For the SILS group, a 2 cm transverse incision wasmade at the level of umbilicus. Upper skin flap was raisedfor a distance of 1 cm. After initial insufflation with Veressneedle, a 10 mm cannula was inserted at the incision lineand the two 5 mm cannulas half cm inferiorly and laterallyon both sides through the same incision (Fig.1). A grasperintroduced through the right lateral cannula did fundustraction. The left lateral cannula was used for introductionof the dissector to define Calot’s triangle (Fig.2). Theinstrument cannulas and telescope cannula were crossed
by a chop stick method (Fig.3) to avoid sword fighting andclashing of instruments in the abdomen. We started theprocedure with 10 mm laparoscope and later shifted to a 5mm scope from the left lateral cannula to insert the 10 mmclip applicator from the central cannula for clipping of thecystic duct and artery. After dissection from the liver bedand hemostasis, the gall bladder was delivered from thecentral port site. Fascial defects were closed meticulouslyand skin apposed.
Pain score was checked 6 hours after surgery using avisual analogue score. Post operative analgesia was thesame for all patients in the form of injection DiclofenacSodium 75 mg given every12 hours.
Statistical analysis
A member of the team who did not know aboutprocedure performed on the patient did the statisticalanalysis.
RESULTS
100 consecutive patients undergoing cholecystectomywere taken for study and they were divided into twogroups having 50 patients in each group.
Group A – Conventional laparoscopy
Group B – Single incision laparoscopic surgery (SILS)
Patients were in between 19 to 57 years old. We had 21male and 29 female patients in group A (conventional) and
Original Article
Apollo Medicine, Vol. 7, No. 2, June 2010 126
group B (SILS) comprised of 26 male and 24 femalepatients. The average BMI was 27.3 and 27.7 respectively.The two groups were statistically matched (Table 1).
We tabulated the pain score in both groups (Table 2).The mean pain score was more in the conventionallaparoscopy group (1.78) compared to the SILS group(1.7) but that difference was not statistically significant.We observed that pain score was not evenly distributed in
SILS group. In the first 25 patients of SILS, the mean painscore was 1.9 which was not only higher than the meanpain score of SILS group but also higher thanconventional group. Post operative pain was less in thelatter 25 patients of SILS group with a mean score of1.6 (p value <0.05) in comparison to both conventional aswell as first half of SILS group.
Another finding in our study is change in operativetime in SILS group. Mean operative time in conventionallaparoscopy group was 28.08±1.35 while in SILS group itwas 66.76±5.78 minutes. Operative time (OT) in SILSgroup varied grossly between earlier cases and lattercases. In first 25 cases mean OT was 79.2 but in later halfit come down to 54.32 which is a significant decrease(p value <0.001) (Table 1).
There were no conversions from SILS to conventionallaparoscopic cholecystectomy or conversion to opensurgery.
DISCUSSION
SILS is not a new concept, and was described as earlyFig.2
Fig.3
Table 1. Age, sex and BMI distribution
Age Male Female BMI
Group A (conventionalLaparoscopiccholecystectomy) 37.5 21 29 27.3
Group B (SILC) 38.1 26 24 27.7

Original Article
127 Apollo Medicine, Vol. 7, No. 2, June 2010
as 1992 by Pelosi, et al [2] who performed a single-puncture laparoscopic appendectomy. First experienceswith SILS cholecystectomy were reported by Navarra,et al in 1997 [3] and with a different approach by Piskunand Rajpal in 1999 [4].
In recent years, SILS has been focused upon as abridge between Natural orifice transluminal endoscopicsurgery (NOTES) and traditional laparoscopic surgery [5].NOTES is a technically challenging procedure and currentinstruments need to be further improved [13]. SILS, on theother hand, enables the application of a wide range ofalready existing instruments. The main point for reducingthe number of incisions has not only been the cosmeticadvantage but also lowered incision risks, morbidity ofbleeding, incisional hernia, and organ damage. Butbenefits regarding post operative pain in SILS has notbeen confirmed. There were some studies that indicatereduction in post operative pain [9] but those are small andnot sufficient to come to a conclusion.
Most of the available special ports and flexibleinstruments are costly and disposable thereby increasingthe cost of the procedure significantly. In our series weused only traditional laparoscopic instrument andtraditional ports. We did not use any specialized port,rather we adopted different indigenous methods to preventair leak such as applying adhesive dressings, gauze soakedwith ointment etc around the cannulas.
The real challenge of SILS is to avoid conflict betweenthe operative instruments and the camera, to maintain thepneumoperitoneum and reduce operative stress. As aresult of the limited space with using only a singleincision, it is difficult for both the surgeon and theassistant to work in the area [14]. We have developed achop stick method to minimize instrument and telescopeclash during the procedure.
In our study we had 100 patients who were randomlydivided into two groups of 50 patients. Mean postoperative pain was less in SILS group but this was notstatistically significant. Operative time was higher in SILSgroup which is comparable to the recently published series[8,15]. In our early half of SILS series, the operative timewas more than latter half. We found that there wassignificant difference in post operative pain betweenearlier half and latter half of our SILS series. Postoperative pain is also significantly low if we comparelatter half of SILS group with traditional laparoscopicseries. So from these available data it is evident that postoperative pain may have some relation with operativetime. But it is also true that post operative pain was more inpatients of conventional laparoscopy group in compare tolater half of SILS although operative time is more insecond group. So to establish a mathematical relationbetween these two variable (operative time and postoperative pain) a larger study is required. It is likely thatwith increasing experience operative time as well as postoperative pain may decrease.
Table 3. Mean operative time in different groups of patient
Group A Group B Early Later (Conventional SILS Half Half Lap Chole) (Total)
Number of patient 50 50 25 25
Mean operative time 28.08 ± 1.35 66.76 ± 5.78 79.2 54.32
Table 2. Mean post operative pain score in different groups of patient
Number of Mean P value Statisticallypatients pain score ( t test ) significant
Group A (Conventional) 50 2.78 0.16 No
Group B (SILS) 50 2.64
First Half (SILS) 25 2.84 0.02 Yes
Second Half (SILS) 25 2.48
Group A (Conventional) 50 2.78 0.04 Yes
Second Half (SILS) 25 2.48

Original Article
Apollo Medicine, Vol. 7, No. 2, June 2010 128
Single-incision laparoscopic surgery for gall bladderremoval is a feasible and promising method for the treat-ment of symptomatic cholelithiasis [16]. This surgery canbe performed with traditional re-usable laparoscopicinstruments [17]. With experience the operative time isexpected to become comparable with conventionallaparoscopic cholecystectomy. Our study did not showany difference in post operative pain after SILS comparedto standard laparoscopy but we feel that expertise andreduction of operative time may reduce post operativepain. No special telescopes, ports or hand instruments areneeded for this procedure but may have a role in advancedlaparoscopic procedures.
REFERENCES
1. Johnson, CD. ABC of the upper gastrointestinal tractUpper abdominal pain: Gall bladder. Br Med Journal2001; 323:1170-1173.
2. Pelosi MA, Pelosi MA. Laparoscopic appendectomyusing a single umbilical puncture (minilaparoscopy). JReprod Med 1992; 37: 588-594.
3. Navarra G, Pozza E, Occhionorelli S, Carcoforo P, DoniniI. One-wound laparoscopic cholecystectomy. Br J Surg1997; 84: 695.
4. Piskun G, Rajpal S. Transumbilical laparoscopiccholecystectomy utilizes no incisions outside the umbili-cus. J Laparoendosc Adv Surg Tech. 1999; 9: 361-364.
5. Bresadola F, Pasqualucci A, Donini A, et al. Electivetransumbilical compared with standard laparoscopiccholecystectomy. Eur J Surg. 1999; 165(1): 29-34.
6. Tacchino R, Greco F, Matera D. Single-incisionlaparoscopic cholecystectomy: surgery without a visiblescar. Surg Endosc 2009; 23: 896-899.
7. Cuesta MA, Berends F, Veenhof AA. The “invisible cholecystectomy”: A transumbilical laparoscopic operationwithout a scar. Surg Endosc 2008; 22: 1211-1213.
8. Hong TH, You YK, Lee KH. Transumbilical single-portlaparoscopic cholecystectomy: scarless cholecystec-tomy. Surg Endosc 2009; 23: 1393-1397.
9. Kurpiewski W, Pesta W, Kowalczyk M, Glowacki L,Juskiewicz W. SILS cholecystectomy – our firstexperiences. Videosurgery and other miniinvasivetechniques 2009; 4 (3): 91-94.
10. Romanelli JR, Mark L, Omotosho PA. Single portlaparoscopic cholecystectomy with the TriPort system: acase report. Surg Innov 2008; 15: 223-228.
11. Merchant AM, Cook MW, White BC, Davis SS, SweeneyJF, Lin E. Transumbilical Gelport access technique forperforming single incision laparoscopic surgery (SILS). JGastrointest Surg 2009; 13: 159-162.
12. Chow A, Purkayastha S, Aziz O, Paraskeva P.Single-incision laparoscopic surgery forcholecystectomy: an evolving technique. Surg Endosc.2010; 24:709-714.
13. Marescaux J, Dallemagne B, Perretta S, Wattiez A,Mutter D, Coumaros D. Surgery without scars: report oftransluminal cholecystectomy in a human being. ArchSurg 2007; 142: 823-827.
14. Ishikawa N, Arano Y, Shimizu S, et al. Single incisionlaparoscopic surgery (SILS) using cross hand technique.Minim Invasive Ther Allied Technol. 2009;18:322-324.
15. Kuon Lee S, You YK, Park JH, Kim HJ, Lee KK, Kim DG.Single-port transumbilical laparoscopic cholecystec-tomy: a preliminary study in 37 patients withgallbladder disease. J Laparoendosc Adv Surg Tech A2009; 19: 495-499.
16. Ersin S, Firat O, Sozbilen M. Single-incision laparoscopiccholecystectomy: is it more than a challenge? SurgEndosc 2010; 24: 68-71.
17. Cugura JF, Jankoviæ J, Kulis T, Kirac I, Beslin MB. Singleincision laparoscopic surgery (SILS) cholecystectomy:where are we? Acta Clin Croat 2008; 47: 245-248.

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/

















