Chapter 31 Postpartum Headache Alison Macarthur, B.M.Sc., M.D., M.Sc., FRCPC DIFFERENTIAL DIAGNOSIS 677 Primary Headaches 677 Secondary Headaches 679 POST–DURAL PUNCTURE HEADACHE 682 Incidence 682 Symptoms 683 Onset and Duration 683 Imaging 683 Pathophysiology 684 Risk Factors 684 Complications 687 Prevention 687 Treatment 689 Unanswered Questions 695 Postpartum headache is the complaint of cephalic, neck, or shoulder pain occurring during the first 6 weeks after deliv- ery. The overall incidence of postpartum headache has not been determined in a prospective study. However, informa- tion is available from a prospective evaluation of women during the first week postpartum 1 and from a prospectively collected database that recorded symptoms during preg- nancy and the first week after delivery. 2 Among 985 women in the prospective evaluation, the incidence of headache in the first week postpartum was 38.7%. 1 The median time from delivery to onset of symptoms was 2 days, and the median duration of headache was 4 hours. Benhamou et al. 2 examined information collected on preg- nant women who delivered at their institution during a 2-year period; exclusion criteria included recognized dural puncture, preterm delivery, multiple gestation, and/or elec- tive cesarean delivery. Headache was reported by 12% of 1058 patients who had epidural anesthesia without dural puncture and by 15% of 140 patients who delivered without epidural anesthesia. Post–dural puncture headache (PDPH) is one of the most common postpartum complications of neuraxial anes- thesia. However, physicians and nurses should be aware that dural puncture is only one of many causes of postpar- tum headache (Table 31-1). Difficult diagnostic problems may require the opinion of a neurologist. The purpose of this chapter is to discuss the differential diagnosis of post- partum headache and of PDPH in particular. DIFFERENTIAL DIAGNOSIS The classification of headaches follows the International Classification of Headache Disorders (ICHD), created in 1988 by the Headache Classification Committee of the International Headache Society. This classification system, which has been updated (ICHD-II), identifies two broad categories of headaches, primary and secondary (Box 31-1). 3 Primary headaches include migraine, tension-type headache, cluster headache, and other trigeminal auto- nomic cephalgias. Secondary headaches are attributable to specific underlying pathology. Primary headaches are 20 times more common than secondary headaches among women in the first postpartum week. 1 After delivery, women frequently suffer from headache. A retrospective study reviewed 5 years of hospital records to identify women who had postpartum headaches between 24 hours and 6 weeks after delivery. 4 Ninety-five women met these criteria, and although the incidence could not be calculated, the study did identify some important features of postpartum headache. Most women (82%) were still in the hospital at the time of onset of the headache. The demo- graphics of the study population largely reflected the gen- eral population; the mean age was 25 years, 87% of the women had received some type of neuraxial analgesia/ anesthesia, and 29% had a cesarean delivery. Primary Headaches The postpartum patient can present with a recurrence of her known primary disorder or with the first manifestation of a primary condition. Patients with a history of headache disorders typically are diagnosed with one of four major types of primary headaches. The most common postpartum headaches are tension-type and migrainous headaches, which account for almost two thirds of headaches during this period. 1,2 Tension-type headaches are often circum- ferential and constricting, can be associated with scalp ten- derness, and are usually of mild to moderate severity. MIGRAINE Migrainous headaches (or migraines) are defined as recur- ring cranial pain lasting 4 to 72 hours, often with typical features such as pulsating pain in a unilateral location, Chapter 31 Postpartum Headache 677
Postpartum headache is the complaint of cephalic, neck, orshoulder pain occurring during the first 6 weeks after deliv-ery. The overall incidence of postpartum headache has notbeen determined in a prospective study. However, informa-tion is available from a prospective evaluation of womenduring the first week postpartum1 and from a prospectivelycollected database that recorded symptoms during preg-nancy and the first week after delivery.2 Among 985women in the prospective evaluation, the incidence ofheadache in the first week postpartum was 38.7%.1 Themedian time from delivery to onset of symptoms was2 days, and the median duration of headache was 4 hours.Benhamou et al.2 examined information collected on preg-nant women who delivered at their institution during a2-year period; exclusion criteria included recognized duralpuncture, preterm delivery, multiple gestation, and/or elec-tive cesarean delivery. Headache was reported by 12% of1058 patients who had epidural anesthesia without duralpuncture and by 15% of 140 patients who delivered withoutepidural anesthesia.
Post–dural puncture headache (PDPH) is one of themost common postpartum complications of neuraxial anes-thesia. However, physicians and nurses should be awarethat dural puncture is only one of many causes of postpar-tum headache (Table 31-1). Difficult diagnostic problemsmay require the opinion of a neurologist. The purpose ofthis chapter is to discuss the differential diagnosis of post-partum headache and of PDPH in particular.
DIFFERENTIAL DIAGNOSIS
The classification of headaches follows the InternationalClassification of Headache Disorders (ICHD), created in1988 by the Headache Classification Committee of theInternational Headache Society. This classification system,which has been updated (ICHD-II), identifies two broad
categories of headaches, primary and secondary (Box31-1).3 Primary headaches include migraine, tension-typeheadache, cluster headache, and other trigeminal auto-nomic cephalgias. Secondary headaches are attributable tospecific underlying pathology. Primary headaches are20 times more common than secondary headaches amongwomen in the first postpartum week.1
After delivery, women frequently suffer from headache.A retrospective study reviewed 5 years of hospital recordsto identify women who had postpartum headaches between24 hours and 6 weeks after delivery.4 Ninety-five womenmet these criteria, and although the incidence could not becalculated, the study did identify some important features ofpostpartum headache. Most women (82%) were still in thehospital at the time of onset of the headache. The demo-graphics of the study population largely reflected the gen-eral population; the mean age was 25 years, 87% of thewomen had received some type of neuraxial analgesia/anesthesia, and 29% had a cesarean delivery.
Primary Headaches
The postpartum patient can present with a recurrence ofher known primary disorder or with the first manifestationof a primary condition. Patients with a history of headachedisorders typically are diagnosed with one of four majortypes of primary headaches. The most common postpartumheadaches are tension-type and migrainous headaches,which account for almost two thirds of headaches duringthis period.1,2 Tension-type headaches are often circum-ferential and constricting, can be associated with scalp ten-derness, and are usually of mild to moderate severity.
MIGRAINEMigrainous headaches (or migraines) are defined as recur-ring cranial pain lasting 4 to 72 hours, often with typicalfeatures such as pulsating pain in a unilateral location,
Chapter 31 Postpartum Headache 677
TABLE 31-1 Differential Diagnosis of Postpartum Headache
*Estimated from Goldszmidt E, Kern R, Chaput A, Macarthur A. The incidence and etiology of postpartum headaches: A prospective cohort
study. Can J Anaesth 2005;52:971-7; and Stella CL, Jodicke CD, How HY, et al. Postpartum headache: Is your work-up complete? Am J Obstet
Gynecol 2007;196:318.e1-7.
678 Part VIII Anesthetic Complications
nausea, and photophobia.3 Headache with aura is a subtypeof migraine that is characterized by focal neurologic symp-toms preceding the headache. The prevalence of migraine isapproximately 17% in the female population (three timesmore common than the prevalence in the male population)and is more common in patients between 30 and 50 years ofage.5 Pregnancy has an ameliorating effect on migraine fre-quency in the majority of sufferers. However, symptomsmay recur soon after delivery, with reports of 34% recur-rence within the first week postpartum and 55% within thefirst month.6 Generally the symptoms are similar to theirtypical pattern, although often milder and less often
unilateral. It is rare for a migraine to manifest for the firsttime during the postpartum period. There appears to be anassociation between migraine and preeclampsia, which mayreflect an underlying predisposition to cerebral ischemicinjury.7
Secondary Headaches
A common secondary headache in the postpartum period isthe musculoskeletal headache, exacerbated by the maternalphysical exertion of labor and associated sleep deprivation.This headache has accompanying neck and shoulder pain
TABLE 31-1—cont’d Differential Diagnosis of Postpartum Headache
Unknown Progressive nonpulsating headacheAggravated by coughing/strainingAssociated with increased CSF pressure
and normal CSF chemistry
History and physical examinationLumbar puncture
Spontaneous intracranialhypotension
Unknown No history of dural traumaDiffuse, dull headache worsening
within 15 minutes of sitting orstanding
Associated with neck stiffness, nausea,tinnitus, and photophobia
CSF opening pressure < 60 mm H2Oin the sitting position
History and physical examinationLumbar punctureRadioisotope cisternographyCT myelography
Sinusitis Unknown Frontal headache with accompanyingpain in the face
Development of headache coincideswith nasal obstruction
Purulent nasal discharge, anosmia,and fever
History and physical examinationNasal endoscopyCT or MRI
Meningitis Unknown Headache is most frequent symptomOften diffuseIntensity increases with timeAssociated with nausea, photophobia,
phonophobia, general malaise, andfever
History and physical examinationLumbar puncture
Pneumocephalus Unknown Frontal headacheOften an abrupt onset immediately
following dural punctureSymptoms can worsen with upright
posture
History and physical examinationCT
Caffeine withdrawal Unknown Onset of headache within 24 hours ofcessation of regular caffeineconsumptiony
Often bilateral and pulsatingRelieved within 1 hour of ingestion of
caffeine 100 mg
History and physical examination
Lactation headache Unknown Mild to moderate headache associatedtemporally with onset of breast-feeding or with breast engorgement
History and physical examination
yThe ICHD-II criteria state that caffeine-withdrawal headache occurs upon cessation of � 200 mg daily caffeine consumption for more than
2 weeks.3 However, others have suggested that caffeine-withdrawal headache may occur after as little as 3 days’ exposure to 300 mg/day,
or 7 days’ exposure to 100 mg/day.39
Chapter 31 Postpartum Headache 679
without a history of dural puncture. Approximately 11% ofpostpartum headaches are diagnosed as musculoskeletal.1
Other causes of secondary headache are discussed in thefollowing paragraphs.
HYPERTENSIONGestational hypertension is commonly associated withheadache. Eclampsia is a form of hypertensive encephalop-athy characterized by headache, visual disturbances, nausea,vomiting, seizures, stupor, and sometimes coma. Seizuresmay occur in the absence of severe hypertension. Headacheis a serious premonitory sign, being present in over 50% ofwomen in whom eclampsia develops.8 Eclampsia first man-ifests postpartum in 11% to 44% of affected women.8 Otherhypertensive disorders, with or without superimposed pre-eclampsia, may also cause postpartum headache and lead toencephalopathy.
POSTERIOR REVERSIBLE LEUKOENCEPHALOPATHYSYNDROMEPosterior reversible (leuko)encephalopathy syndrome(PRES) was described in 1996 following recognition of aconsistent symptom presentation in a diverse group ofpatients. Conditions associated with PRES include pre-eclampsia, uremia, hemolytic-uremic syndrome, and expo-sure to immunosuppressant drugs.9 Approximately 25% ofcases of PRES occur in pregnant patients. PRES symptomsinclude headache, seizures, altered mental status, visualchanges, and, occasionally, focal neurologic deficits.10
The neuroradiologic features of PRES include symmet-ric areas of cerebral edema, predominantly involvingthe white matter regions of the posterior circulation
(i.e., occipital lobes, posterior parietal, and temporallobes) (Figure 31-1). The pathophysiology of PRES is similarto that of hypertensive encephalopathy, in that altered cere-brovascular regulation causes loss of blood-brain barrierintegrity. The accompanying vasogenic edema can bereversed by prompt recognition and supportive therapy(i.e., cessation of provocative medications, aggressive treat-ment of hypertension, seizure prophylaxis). However, irre-versible cytotoxic edema with permanent neurologicdamage can occur if the initial disorder is not diagnosedearly. This syndrome often manifests in the postpartumperiod, usually in conjunction with preeclampsia.11-15
Diagnosis may be delayed if other potential causes of head-ache are also present (e.g., dural puncture).13,14 Typical fea-tures that distinguish PRES from other postpartumheadaches include seizures and focal neurologic deficits,such as temporary loss of vision.
SUBARACHNOID HEMORRHAGEThe incidence of subarachnoid hemorrhage is increasedduring pregnancy, being estimated at approximately 20per 100,000 deliveries. It usually occurs in patients with acerebral aneurysm, arteriovenous malformation, or hyper-tensive encephalopathy.16 The classic presentation consistsof the sudden onset of a severe headache that is unlike anyprevious headache. Pregnancy may increase the risk ofbleeding because of increased blood volume and hormonalchanges that affect arterial integrity. Other factors associ-ated with subarachnoid hemorrhage during pregnancyinclude cigarette smoking, genetic diseases (e.g., polycystickidney disease), and nulliparity. Suspicion of subarachnoidhemorrhage necessitates urgent investigation by computedtomography (CT), because nonsurgical therapies (e.g., en-dovascular ablation) are available and long-term sequelaecan be minimized.
CORTICAL VEIN THROMBOSISThe incidence of cerebral cortical vein thrombosis isincreased in pregnancy, and is estimated to be 10 to 20per 100,000 deliveries in developed countries.17 The inci-dence appears higher in developing countries (e.g., 450 per100,000 deliveries in India). Often it is difficult to distin-guish cortical vein thrombosis from PDPH, because theheadache of cortical vein thrombosis may have a posturalcomponent. Preceding dural puncture has been reported inseveral cases,18-20 and it has been hypothesized that thereductions in cerebrospinal fluid (CSF) pressure and cere-bral vasodilation that accompany dural puncture predisposeto thrombosis development. Associated features includefocal neurologic signs, seizures, and coma. Cerebral infarc-tion may ensue if diagnosis is delayed. Diagnosis is bestconfirmed by magnetic resonance imaging (MRI), becauseCT appears to identify only a third of cases.21 Treatment ofcortical vein thrombosis largely is symptomatic, with theaim of preventing seizures. Some studies have suggestedthat anticoagulation therapy may improve outcome; how-ever, additional data are needed.22,23
CEREBRAL INFARCTION/ISCHEMIACerebral arterial insufficiency is one cause of stroke in preg-nancy, with an estimated incidence of 19 per 100,000 deliv-eries.24 Approximately half of the events occur in theperipartum period, and the clinical presentation often
BOX 31-1 International Classification of HeadacheDisorders (ICHD-II) Classification
Primary� Migraine� Tension-type headache� Cluster headache and other trigeminal autonomic
cephalgias� Other primary headaches
Secondary� Headache attributed to:� Head and/or neck trauma� Cranial or cervical vascular disorder� Nonvascular intracranial disorder� A substance or its withdrawal� Infection� Disorder of homeostasis� Disorder of the cranial structures (e.g., eyes, ears,
comprises a sudden onset of headache, vomiting, seizures,and focal neurologic deficits. Postpartum cerebral angiopa-thy has been detected with the aid of cerebral angiography,in which a characteristic ‘‘arterial beading’’ indicative ofarterial spasm is evident. Several case reports havedescribed the delayed diagnosis of cerebral infarctionbecause providers assumed a diagnosis of PDPH.25,26 Thekey feature was a nonpostural headache. Initial CT and MRIfindings are often normal, and intracranial Doppler orangiographic investigations may be necessary to diagnoseischemia or infarct.
SUBDURAL HEMATOMAIn rare instances, dural puncture is associated with the sub-sequent development of a subdural hematoma. In severalcase reports, the identification of the subdural hematomawas preceded by symptoms of a PDPH.27-29 Dural punctureresults in leakage of CSF and decreased intracranial pres-sure (ICP). Presumably, the reduction in ICP causes stresson bridging cerebral vessels, thereby precipitating bleeding.Neurologic signs of subdural hematoma are variable butinclude evidence of increased ICP (e.g., headache, somno-lence, vomiting, confusion) and focal abnormalities.
PNEUMOCEPHALUSThe subdural or subarachnoid injection of air used for iden-tification of the epidural space may be associated with thesudden onset of severe headache, sometimes accompaniedby neck pain, back pain, or changes in mental status.30
Headache symptoms can mimic those of PDPH, in thatthey are worse in the sitting position and may be relievedby lying down. Radiologic studies confirm the presence of
intracranial air, and the headache typically resolves over thefirst week.
MENINGITISThe severe headache of meningitis typically manifestswithin the first several postpartum days (see Chapter 32).It is accompanied by fever, nuchal rigidity, and the presenceof Kernig and Brudzinski signs. Lethargy, confusion, vomit-ing, seizures, and a rash may also occur. Usual pathogensinclude streptococci of the viridans type.31 The diagnosis isconfirmed by examination and culture of the CSF.
PSEUDOTUMOR CEREBRI/BENIGN INTRACRANIALHYPERTENSIONParturients with pseudotumor cerebri (i.e., increased ICP inthe absence of a mass lesion) present with headache andvisual disturbances, usually in the antepartum period.The features of the postpartum headache of pseudotumorcerebri mimic the usual chronic headache symptoms expe-rienced by the patient. The diagnosis largely is one of exclu-sion (see Chapter 49). Treatment involves reduction of CSFpressure through the use of glucocorticoids, carbonic-anhy-drase inhibitors, diuretics, or serial lumbar punctures.
BRAIN TUMORIntracranial tumors may manifest as postpartum head-ache.32-34 Headache that is dull rather than throbbing incharacter may be an early symptom of a brain tumor.Nausea, vomiting, seizures, and/or focal neurologic signsmay be present. Neurologic examination may reveal evi-dence of increased ICP. Case reports suggest that atypicalpresentation of headache, either with persisting headache
BA
RL
LR
FIGURE 31-1 Posterior reversible (leuko)encephalopathy syndrome (PRES). A, Areas of hypodensity in the parieto-occipital white matter (blackarrows). B, Abnormal hypodensity is also seen in the cerebellum (white arrows), with the abnormality larger on the left (L) than the right (R).(From Hinchey J, Chaves C, Appignani B, et al. A reversible posterior leukoencephalopathy syndrome. N Engl J Med 1996; 334:494-500.)
Chapter 31 Postpartum Headache 681
symptoms in the supine position or exacerbation followingepidural blood patch, should prompt further neuroradio-logic investigations.32-34
SPONTANEOUS INTRACRANIAL HYPOTENSIONSpontaneous intracranial hypotension develops because ofCSF leakage secondary to dural tears. The tears usuallyoccur at the thoracic spinal level and are not associatedwith prior neuraxial procedures.35 Diagnosis requires radio-isotope cisternography and CT myelography, which mayalso identify the level of the leak. Presentation of this dis-order is identical to that of PDPH, as the pathophysiology isthe same. The only difference is the lack of a prior neuraxialprocedure in spontaneous intracranial hypotension. Onecase report has described the development of a posturalheadache 4 days after a spontaneous vaginal delivery with-out neuraxial anesthesia.36 The patient was found to have acervical-thoracic dural leak.
SINUSITISHeadache caused by inflamed paranasal sinuses is associat-ed with purulent nasal discharge and, occasionally, fever.Pain may be unilateral or bilateral, depending on theextent of the disease, and the skin over the affected sinusmay be tender. Frontal sinus infection causes headache inthe frontal region. Ethmoidal and sphenoidal sinus infec-tions cause periorbital pain, and maxillary sinus infectionmay cause diffuse facial discomfort. The sinuses fill over-night, and pain typically is worse on awakening. Painimproves in the upright position, which assists drainage.37
CAFFEINE WITHDRAWALThe withdrawal of caffeine may lead to headache, increasedfatigue, and anxiety. Caffeine withdrawal headaches havebeen reported in the postoperative period38 and mayoccur after as little as 3 days’ exposure to 300 mg/day or7 days’ exposure to 100 mg/day of caffeine.39 Normal-sizedcaffeinated drinks usually contain 50 to 100 mg of caffeineper serving. Women often decrease their caffeine intake inthe puerperium, and although caffeine withdrawal headachehas not been confirmed as a cause of postpartum headache,the diagnosis should be considered.
LACTATION HEADACHEAskmark and Lundberg40 reported episodes of intense head-ache during periods of breast-feeding in a woman known tosuffer from migraine. Onset of headaches occurred withinthe first few minutes of breast-feeding, and the headachesresolved after cessation of nursing. The headaches wereassociated with an increase in plasma vasopressin concen-tration. Headaches have also been described in women withbreast engorgement who either have elected not to breast-feed or have reduced the frequency of breast-feeding.41
POST–DURAL PUNCTURE HEADACHE
Incidence
Post–dural puncture headache (PDPH) may occur afterintentional dural puncture with a spinal needle or uninten-tional dural puncture with an epidural or other needle.
FIGURE 31-2 Meta-analysis of post–dural puncture headache (PDPH) frequency for epidural needles in the obstetric population. The dots represent thepercentages of patients experiencing the event. The horizontal lines represent the 95% confidence interval (CI). (From Choi PT, Galinski SE, Takeuchi L,et al. PDPH is a common complication of neuraxial blockade in parturients: A meta-analysis of obstetric studies. Can J Anaesth 2003; 50:460-9.)
682 Part VIII Anesthetic Complications
A meta-analysis of studies of PDPH in obstetric patients (n= 328,769) calculated a pooled risk of unintentional duralpuncture with any epidural needle of 1.5% (95% confidenceinterval [CI], 1.5% to 1.5%).42 Following a dural puncturewith an epidural needle, the risk of PDPH was 52.1% (95%CI, 51.4% to 52.8%) (Figure 31-2). The rate of PDPH afterdural puncture with spinal needles ranged between 1.5%and 11.2%, depending on the needle size and type ofneedle (see later) (Table 31-2). Although PDPH is oftenconsidered a ‘‘minor’’ complication of dural puncture, itwas the cause of 14% of obstetric claims in the AmericanSociety of Anesthesiologists (ASA) Closed-Claims Projectdatabase (see Chapter 33).
Symptoms
Patients typically experience headache pain in the frontaland occipital regions. Pain often radiates to the neck, whichmay be ‘‘stiff.’’ Some women have a mild headache thatpermits full ambulation. In others, pain is severe and inca-pacitating. Symptoms are worse in the upright position andare usually relieved in the horizontal position. Abdominalcompression may relieve pain in some patients. The ICHD-II defines PDPH as occurring within 15 minutes of apatient’s moving to an upright position (sitting or standing)and resolving within 15 minutes of the patient’s moving tothe supine position.3
The ICHD-II criteria for PDPH require one of the follow-ing symptoms to be present: neck stiffness, tinnitus, hypa-cusis, photophobia, and nausea. Lybecker et al.43 reportedthe incidence of these symptoms in a prospective study of 75nonobstetric patients with PDPH (Table 31-3). Cranial nervepalsy, thought to be secondary to nerve traction due to low
CSF volume, is occasionally associated with PDPH. The sixthcranial nerve is most susceptible to traction during its longintracranial course. The traction results in failure of theinvolved eye to abduct, and patients may have diplopia.Hearing loss is usually in the low-frequency range and isrelated to reduction of CSF pressure and alteration of haircell position in the inner ear.44 The risk of hearing lossappears to be higher with advanced age (more than 40years) and dural puncture with larger-gauge needles.
Rarer symptoms associated with PDPH include seizures,abdominal pain, and diarrhea. Shearer et al.45 reported post-partum seizures in eight women with severe PDPH withoutconvincing evidence of preexisting hypertension. Cerebralvasospasm was thought to be the etiologic factor.Vercauteren et al.46 described a woman who had receivedepidural analgesia and experienced postpartum seizures witha severe headache. The CSF was blood-stained, but a CTscan showed no source of hemorrhage. This patientimproved dramatically after the performance of a bloodpatch. A 20-year-old man experienced PDPH after adminis-tration of spinal anesthesia with a 25-gauge Quinckeneedle.47 Twelve days after the anesthetic administration,he experienced abdominal pain and diarrhea, which per-sisted despite the lack of evidence of mucosal or organicdisease. One month following spinal anesthesia, an epiduralblood patch procedure was performed, which resulted inprompt resolution of headache and gastrointestinal symp-toms. The investigators speculated that this patient had non-infectious arachnoiditis with lumbosacral root involvement,which resulted in visceral hyperalgesia and dysfunction.
Onset and Duration
Headache typically occurs on the first or second day afterdural puncture; by ICHD-II criteria, it must appear within 5days of dural puncture.3 Ninety-five percent of PDPH head-aches last less than a week. The National Obstetric Anaes-thetic Database project of the Obstetric Anaesthetists’Association of the United Kingdom demonstrated that75% of 975 women with PDPH suffered from headache-associated difficulty in performing the activities of dailyliving.48 Rarely, symptoms may persist for months or evenyears.49
TABLE 31-2 Frequency of Post–Dural Puncture Headachein Obstetric Patients According to Spinal Needle Design
*Ocular symptoms include photophobia, diplopia, and difficulty in
accommodation.
yAuditory symptoms include hearing loss, hypacusis, and tinnitus.
Data from Lybecker H, Djernes M, Schmidt JF. Postdural puncture
headache (PDPH): Onset, duration, severity, and associated
symptoms. An analysis of 75 consecutive patients with PDPH. Acta
Anaesthesiol Scand 1995;39:605-12.
Chapter 31 Postpartum Headache 683
Imaging
Imaging investigations are not routinely recommended forthe postpartum patient with a PDPH unless the symptomssuggest other diagnoses and the diagnosis of PDPH is indoubt. Contrast-enhanced MRI is the method of choice tostudy the meninges and has revealed characteristic findingsof PDPH.50,51 These findings include marked, diffuse con-trast enhancement with thickening of the dura mater, occa-sional extradural fluid collections, and enhancement andexpansion of the superior sagittal sinus. The enlargedvenous sinus may represent compensatory venous expan-sion in response to low CSF pressure.51
Pathophysiology
Debate continues regarding the precise etiology of PDPHsymptoms. The original theory was that pain-sensitivenerve fibers were stimulated by a downward shift of thebrain secondary to a loss of CSF volume. German surgeonAugust Bier52 is credited with the first description of PDPHafter his pioneering work on spinal anesthesia with cocaine.Bier and an assistant performed spinal anesthesia on eachother, using blows to the shin with an iron hammer andapplication of a burning cigar to the skin to demonstratesensory blockade.52 Both experienced severe PDPH. Theassistant forced himself to work the next day, but Bierstayed home for 9 days. Bier suggested that the PDPHmight be caused by CSF loss. Today there is no doubtthat leakage of CSF initiates the syndrome. Kunkle et al.53
consistently produced PDPH by draining 20 mL of CSFfrom volunteers. Symptoms were relieved immediately bysubarachnoid injection of saline to restore initial CSFpressure.
Total CSF volume is estimated to be 150 mL, and theproduction rate is approximately 0.35 mL/min, or a dailyproduction rate of 500 mL. The rate of CSF leakage througha dural hole may exceed the rate of CSF production. If thisoccurs, low CSF pressure results in a loss of the cushioningeffect provided by intracranial fluid.
CSF pressure during labor is normal between contractionsbut increases significantly during painful contractions andexpulsive efforts.54 Effective epidural analgesia attenuatesthis increase in CSF pressure. In a study of postpartum epi-dural space pressures following unintentional dural puncturein five women, epidural space pressures were normal preced-ing the development of headache.55 However, with develop-ment of headache symptoms, the mean epidural pressuremeasurements were found to be decreased significantly.
Not all parturients with PDPH have decreased CSF pres-sure, and not all parturients with a significant CSF leakexperience symptoms.56 The pain of PDPH may becaused, in part, by an increase in cerebral blood flow (andcerebral vasodilation) as a consequence of low CSF pressureor volume. This phenomenon has been observed in ani-mals.57,58 The inverse relationship between intracranialblood volume and CSF volume reflects the body’s effortto maintain a constant intracranial volume.59 The lumbarCSF compartment is a dynamic structure that acts as areservoir for intracranial CSF volume adjustment. Theoccurrence of cerebral vasodilation may explain the reliefof headache symptoms with vasoconstrictors such as caf-feine, theophylline, and sumatriptan.
Risk Factors
In a classic study of 10,098 spinal anesthetic procedurespublished in 1956, Vandam and Dripps60 noted threedemographic factors associated with PDPH: age, gender,and pregnancy. The analysis did not allow determinationas to whether these factors were independent risk factors.Subsequently, other risk factors for development of PDPHhave been identified.
AGEExtensive evidence supports the observation that PDPH isuncommon in patients older than 60 years and is mostcommon in patients younger than 40 years. In the elderly,the dura may be inelastic and less likely to gape after punc-ture. CSF leakage may be impeded by adhesions and calci-fication. The cerebrovascular system also may be lessreactive in older patients. Further, this group is less activephysically, and older patients may be less likely to complain.
GENDERVandam and Dripps60 observed a twofold higher incidence ofPDPH in women than in men (14% versus 7%, respectively).This difference may be related to differences in cerebral vas-cular reactivity, because it is well known that migraine occurspredominantly in females and is influenced by hormonalchanges. Women may have enhanced vascular reactivity, orperhaps changes in cerebral blood flow are more likely toproduce pain in women than in men. A meta-analysis ofrandomized clinical trials identified a twofold higher riskfor PDPH in nonpregnant females than in males.61
VAGINAL DELIVERYVandam and Dripps60 also observed a high incidenceof PDPH (22%) after vaginal delivery. This higher incidencemay be a result of the mechanical consequences of expul-sive efforts during the second stage of labor and/or post-partum hormonal changes in cerebrovascular reactivity.Expulsive efforts during the second stage of labor mayincrease CSF leakage. This possibility has prompted somephysicians to restrict maternal pushing after unintentionaldural puncture and to use forceps to shorten the secondstage of labor. In a 20-year retrospective review of 460 par-turients who experienced unintentional dural punctureduring labor at the Birmingham Maternity Hospital in theUnited Kingdom, Stride and Cooper62 did not identify alower incidence of PDPH in women who underwent pro-phylactic forceps delivery than in those who had spontane-ous vaginal delivery. In contrast, in a retrospective review ofthe records of 33 laboring women who had experiencedunintentional dural puncture, Angle et al.63 found thatwomen who were allowed to push were much more likelyto experience PDPH (relative risk, 7.4; 95% CI, 1.1 to 48.2)and also were more likely to require an epidural blood patch.
MORBID OBESITYSome evidence suggests that morbidly obese patientsare less susceptible to PDPH and are also less likely toreceive an epidural blood patch for treatment of PDPH,64
suggesting either a reduced severity of PDPH or anesthesiaprovider reticence to perform an epidural blood patch inthis patient population. Possible but unproven explanationsfor the lower incidence and severity of PDPH in obese
684 Part VIII Anesthetic Complications
patients include increased abdominal pressure (which mayreduce the extent of CSF leak) and/or reduced physicalactivity of these patients. Other confounding factors, suchas differences in the mode of delivery (higher rate of cesar-ean delivery) and neuraxial opioid administration, may alsoplay a role.
AIR TRAVELPDPH has been reported during air travel after spinal anes-thesia.65 Presumably, the headache is precipitated by achange in the gradient between the subarachnoid space andthe epidural space due to decreased atmospheric pressure.
HISTORY OF PREVIOUS POST–DURAL PUNCTUREHEADACHEA history of PDPH after previous spinal anesthesia isassociated with the development of PDPH with subsequentspinal anesthesia.66 A cohort of nonobstetric women witha history of previous spinal anesthesia were monitored pro-spectively after a second spinal anesthesia procedure. Thosewith a previous history of PDPH were 2.3 times more likely(95% CI, 1.0 to 5.1) to have a second PDPH than womenwithout a history of headache (24.2% versus 10.6%, respec-tively).66 This finding suggests that certain individuals arepredisposed to the development of PDPH.
MULTIPLE DURAL PUNCTURESSeeberger et al.67 found that multiple dural puncturessignificantly increased the risk for PDPH. Surgical patientswho received a second spinal injection owing to failure ofthe initial spinal injection had a 4.2% incidence of PDPH,compared with a 1.6% incidence among patients who had asingle dural puncture.
NEURAXIAL ANESTHETIC TECHNIQUETechnical factors related to the neuraxial technique influ-ence the incidence of PDPH.
Epidural Needle Size/Design
The high rate of PDPH following unintentional dural punc-ture with an epidural needle has led investigators to alterthe epidural needle design or size in an attempt to reduceheadache incidence or severity. Data on the success of thisendeavor are conflicting. In an in vitro study using cadaverdura, no differences were found in fluid leak rate amongpunctures made with Hustead, Tuohy, Crawford, andSprotte epidural needles.68 In contrast, in an in vivo study,Morley-Forster et al.69 observed a lower incidence of PDPHwith use of an 18-gauge Sprotte needle than with use of thestandard 17-gauge Tuohy needle, despite there being nodifference in the unintentional dural puncture rate.A pilot study has examined the utility of a 19-gaugeTuohy needle with a 23-gauge epidural catheter.70
Spinal Needle Design
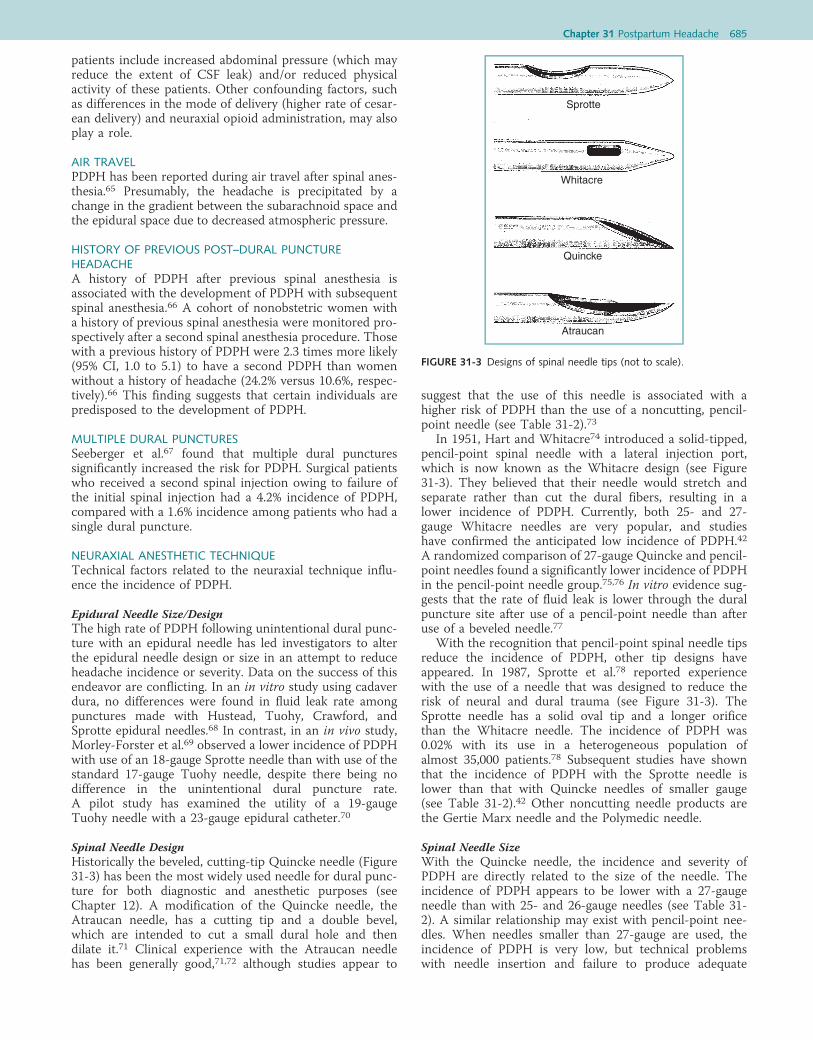
Historically the beveled, cutting-tip Quincke needle (Figure31-3) has been the most widely used needle for dural punc-ture for both diagnostic and anesthetic purposes (seeChapter 12). A modification of the Quincke needle, theAtraucan needle, has a cutting tip and a double bevel,which are intended to cut a small dural hole and thendilate it.71 Clinical experience with the Atraucan needlehas been generally good,71,72 although studies appear to
suggest that the use of this needle is associated with ahigher risk of PDPH than the use of a noncutting, pencil-point needle (see Table 31-2).73
In 1951, Hart and Whitacre74 introduced a solid-tipped,pencil-point spinal needle with a lateral injection port,which is now known as the Whitacre design (see Figure31-3). They believed that their needle would stretch andseparate rather than cut the dural fibers, resulting in alower incidence of PDPH. Currently, both 25- and 27-gauge Whitacre needles are very popular, and studieshave confirmed the anticipated low incidence of PDPH.42
A randomized comparison of 27-gauge Quincke and pencil-point needles found a significantly lower incidence of PDPHin the pencil-point needle group.75,76 In vitro evidence sug-gests that the rate of fluid leak is lower through the duralpuncture site after use of a pencil-point needle than afteruse of a beveled needle.77
With the recognition that pencil-point spinal needle tipsreduce the incidence of PDPH, other tip designs haveappeared. In 1987, Sprotte et al.78 reported experiencewith the use of a needle that was designed to reduce therisk of neural and dural trauma (see Figure 31-3). TheSprotte needle has a solid oval tip and a longer orificethan the Whitacre needle. The incidence of PDPH was0.02% with its use in a heterogeneous population ofalmost 35,000 patients.78 Subsequent studies have shownthat the incidence of PDPH with the Sprotte needle islower than that with Quincke needles of smaller gauge(see Table 31-2).42 Other noncutting needle products arethe Gertie Marx needle and the Polymedic needle.
Spinal Needle Size
With the Quincke needle, the incidence and severity ofPDPH are directly related to the size of the needle. Theincidence of PDPH appears to be lower with a 27-gaugeneedle than with 25- and 26-gauge needles (see Table 31-2). A similar relationship may exist with pencil-point nee-dles. When needles smaller than 27-gauge are used, theincidence of PDPH is very low, but technical problemswith needle insertion and failure to produce adequate
Sprotte
Whitacre
Quincke
Atraucan
FIGURE 31-3 Designs of spinal needle tips (not to scale).
Chapter 31 Postpartum Headache 685
anesthesia are more common.79 Locating the epidural spacebefore insertion of the spinal needle (e.g., using the epiduralneedle as an introducer needle) may improve the rate ofsuccess with fine-gauge needles.
The current popularity of spinal anesthesia in obstetricpatients is largely a result of new needle technology, whichhas led to a reduction in the incidence of PDPH. Because ofthe morbidity associated with PDPH, every effort should bemade to use a needle associated with a low incidence ofPDPH (e.g., a small-gauge, noncutting needle). There aretimes when urgency or body habitus dictates the use of alarger needle, but there is seldom justification for using aQuincke needle larger than 27-gauge.
Direction of Bevel of the Quincke Needle
Studies have confirmed that puncturing the dura materwith the Quincke needle bevel parallel to the long axis ofthe spine is associated with an incidence of PDPH 70%lower than that associated with a perpendicular orienta-tion.80 An early study by Franksson and Gordh81 demon-strated that orientation of the bevel of a Quincke spinalneedle parallel to the long axis of the spine produced lessdural trauma than occurred when the bevel was insertedperpendicularly. These investigators thought that the duralfibers were predominantly longitudinal in direction.Electron microscopy has shown that the dural structure isfar more complex than originally was supposed. Fink andWalker82 noted that the dura consists of multidirectionalinterlacing collagen fibers and both transverse and longitu-dinal elastic fibers. They suggested that the insertion of theneedle with the bevel parallel to the long axis of the spinemost likely results in less tension on the dural hole, andtherefore, a smaller aperture with less CSF leak. In vitrostudies of bevel orientation and fluid leak have providedconflicting results.83,84 However, despite confusing ana-tomic evidence, clinical experience strongly supports inser-tion of the Quincke needle with the bevel parallel to thelong axis of the spine.
Direction of the Bevel of the Tuohy Needle
Norris et al.85 examined two groups of women whoreceived epidural anesthesia with a Tuohy needle. In onegroup the needle was inserted with the bevel perpendicularto the long axis of the spine. In the other group the needleentered the epidural space with the bevel parallel to thelong axis and was rotated 90 degrees before insertion ofthe catheter. The investigators observed a lower incidenceof PDPH in the latter group. However, some anesthesiaproviders argue that rotation of the needle within the epidu-ral space may increase the risk of unintentional dural punc-ture. Richardson and Wissler86 randomly assigned laboringpatients to a cephalad or lateral orientation of the Tuohybevel during epidural needle insertion. The needle wasnot rotated before insertion of the epidural catheter. Therewas no difference in dural puncture rates, but catheter inser-tion was easier with a cephalad orientation of the bevel.86
Midline or Paramedian Approach
There is conflicting evidence as to whether the spinalneedle approach affects the incidence of PDPH. Hatfalvi87
reported no cases of PDPH in a retrospective survey of 4465spinal anesthesia procedures. This investigator used a para-median approach with a 20-gauge Quincke needle, and the
skin was punctured 3 cm from the midline. He suggestedthat tangential dural puncture creates a dural flap and pre-vents PDPH. In contrast, Viitanen et al.,88 prospectivelymonitoring obstetric patients after administration ofsingle-shot spinal analgesia for labor (27-gauge Quinckeneedle), observed PDPH in 3 of 85 (3.5%) patients inwhom the midline approach was used, compared with 15of 127 (11.8%) patients in whom the paramedian approachwas used. Using a rigid paper cylinder model of the dura,Kempen and Mocek89 studied midline and paramedianpunctures with a 22-gauge Quincke needle in differentorientations. With midline punctures, all entry and exitholes were of uniform size regardless of bevel orientation,and no dural flaps were seen. After paramedian punctures,flaps formed when the needle bevel faced the cylinder sur-face with a near-tangential angle of perforation.
Skin Preparation
In a nonrandomized, nonblinded study reported in a letter,Gurmarnik90 found that the removal of dried povidone-iodine from the skin before placement of the spinal needlewas associated with a lower incidence of PDPH (6% versus0%). This investigator recommended removal of the povi-done-iodine before insertion of the spinal needle, and sug-gested that chemical meningismus resulting from povidone-iodine introduced into the intrathecal space by the spinalneedle contributed to PDPH. This finding has not been con-firmed by other investigators. (Editors’ Note: We do not rec-ommend removal of povidone-iodine before initiatingneuraxial analgesia, because povidone-iodine works bydesiccating bacteria, and removing the povidone-iodinereduces its antibacterial effect.)
Air versus Saline Method of Locating the Epidural Space
The method of locating the epidural space may influencethe incidence of PDPH.91 Many anesthesia providers haveadopted the loss-of-resistance-to-saline technique in thebelief that it is associated with a lower incidence of unin-tentional dural puncture and PDPH than the use of air.62,92
However, the data are inconsistent, and not all studies havefound a difference.92-94 In a study of epidural steroid injec-tions (at all spinal levels) in a pain clinic, a single practitionerperformed more than 3700 procedures, alternating weeklybetween use of the loss-of-resistance to air and salinemethods.95 There was no difference between groups in theincidence of unintentional dural puncture. Although the inci-dence of postprocedure headache was lower in the salinegroup, the definition of headache was not rigorous, and itwas not possible to differentiate between headache frompneumocephalus and classic PDPH.95
Choice of Local Anesthetic Drug for Spinal Anesthesia
Naulty et al.96 reported that the use of bupivacaine-glucoseor lidocaine-glucose for spinal anesthesia was associatedwith a higher incidence of PDPH than use of tetracaine-procaine. They postulated that osmotic, cerebral (menin-geal) irritant and/or cerebrovascular effects of the glucosecould be responsible for these findings.
Continuous Spinal Anesthesia
A multicenter trial published in 2008 reexamined the safetyand utility of 28-gauge microcatheters for spinal laboranalgesia.97 There was no difference in the incidence of
686 Part VIII Anesthetic Complications
PDPH (9% versus 4%, respectively) or epidural blood patch(5% versus 2%, respectively), between women randomlyassigned to receive an intrathecal catheter and those whoreceived an epidural catheter; however, the study was insuf-ficiently powered to assess these outcomes. Spinal micro-catheters currently are not commercially available in NorthAmerica.
Combined Spinal-Epidural Anesthesia
Combined spinal-epidural (CSE) analgesia/anesthesia iswidely used for labor analgesia and, to a lesser extent, forcesarean delivery. Intuitively, it seems that the incidence ofPDPH should be identical to that after single-shot spinalanesthesia with the same size and type of needle. Manyanesthesia providers believe that the intentional dural punc-ture with the CSE technique is associated with a higherincidence of PDPH than epidural anesthesia alone.However, the available evidence, primarily from observa-tional studies, suggests that the risk of PDPH is notincreased with the CSE technique.98-100 PDPH rates forthe CSE technique in these three studies were 1.7%,0.43%, and 1.4%, respectively, compared with 1.6%, 0.45%,and 0.8% for the epidural technique.98-100 Initial placementof the epidural needle facilitates precise dural puncture, andthe subsequent increase in epidural space pressure after theepidural injection of local anesthetic may reduce CSF leak-age. If the anesthesia provider is in doubt about correctepidural needle placement, a needle-through-needle duralpuncture might resolve the issue and prevent unintentionaldural puncture with a large-gauge epidural needle.
Complications
The immediate problems associated with PDPH include(1) the inability to perform the activities of daily living,such as providing care for the newborn; (2) an extendedduration (almost one full day) of hospitalization; and (3) ahigher number of emergency room visits, with almost 40%of patients returning for at least one visit.101 Although thesecomplications are very bothersome to the patient, they areshort-lived and do not result in long-term morbidity.However, rare but serious complications may occur afterdural puncture and PDPH.
Zeidan et al.102 reviewed the published reports ofsubdural hematoma after dural puncture. They foundthat subdural hematoma was associated with new neuro-logic symptoms in addition to changing headache charac-teristics. The proposed mechanism of subdural hematomadevelopment is ongoing intracranial hypotension leading tocaudal movement of the brain and rupture of fragile, bridg-ing subdural veins. These cases have been managed withan epidural blood patch as well as with neurosurgicaldecompression.
Dural sinus thrombosis has been documented afterunintentional dural puncture and treatment of PDPHwith an epidural blood patch.18-20 Responsible factors maybe cerebral venous dilation (associated with decreased ICP)and the hypercoagulability that occurs during pregnancy.Therapy may include anticoagulation.
Diplopia or hearing loss after dural puncture, second-ary to cranial nerve dysfunction, may be permanent, evenafter successful treatment of the PDPH with an epiduralblood patch. A review of 95 cases of neurapraxia or
axonotmesis of the ocular cranial nerves concluded thatsymptoms may last from 2 weeks to 8 months but thatalmost 90% of patients recover.103
Two surveys from a single institution have attempted toestimate long-term morbidity arising from unintentionaldural puncture or spinal anesthesia in obstetricpatients.104,105 Women delivering between 1978 and1985,104 and between 1991 and 1996,105 were asked torecall symptoms beginning after their deliveries, includingback pain and headache. The responses of women withunintentional dural puncture or PDPH following spinalanesthesia were compared with those of women who haduneventful procedures. The first study found that 18% ofwomen with unintentional dural puncture had complaintsof frequent headaches or neck ache, compared with only 7%of women experiencing uneventful neuraxial procedures.104
The later study did not confirm a higher risk of headachewith prior unintentional dural puncture but, instead, founda higher rate of backache symptoms.105 These results havenot been confirmed in a prospective study or by otherinvestigators and likely suffer from the limitations of sur-veys that rely on patient recall.
Prevention
A 2005 survey of British obstetric anesthetists identified thefrequency of practices and maneuvers that many believewill reduce the likelihood of a PDPH after unintentionaldural puncture with an epidural needle.106 These includeencouraging postpartum fluid intake (91%) and regularanalgesia administration (83%), and placement of an intra-thecal catheter (15%) at the time of the unintentional duralpuncture. Older practices, such as avoiding pushing duringthe second stage, restricting postpartum mobility, and pro-phylactic epidural administration of saline or autologousblood, appear to be declining in use.
POSTUREIn a Cochrane systematic review, Sudlow and Warlow107
reviewed the evidence for reducing the incidence ofPDPH by use of bed rest rather than early mobilization(usually within 6 hours of dural puncture). The reviewincluded the only randomized trial of obstetric patients,and results were consistent for all patient types; there wasno benefit for bed rest over early mobilization (PDPHincidence 31% versus 27%, respectively). It is important toencourage early ambulation during the puerperium.Pregnant women are hypercoagulable and at higher riskfor deep vein thrombosis and pulmonary embolism, andimmobility increases this risk (see Chapter 38).
HYDRATIONDespite the widespread practice of encouraging womento increase oral fluid intake after unintentional duralpuncture, there is little evidence that greater hydration pre-vents PDPH. The Cochrane review identified only one ran-domized trial of 100 nonobstetric patients.107 There was nodifference in the incidence of PDPH in patients randomlyassigned to receive either 3 L or 1.5 L of fluid per day.
ABDOMINAL BINDERIn a 1975 study, the use of a tight abdominal binder placedimmediately after delivery and continued until discharge
Chapter 31 Postpartum Headache 687
home apparently was successful in reducing the incidenceof PDPH.108 The study included parturients who receivedsingle-shot spinal anesthesia through 22-gauge cuttingneedles, which are more likely to lead to PDPH thanmodern-day spinal needles. However, the applicability ofthis technique to prevent PDPH after unintentional duralpuncture with an epidural needle has not been evaluated.Abdominal binders are seldom used today.
CAFFEINETwo clinical trials in nonobstetric patients have evaluatedthe efficacy of oral caffeine to prevent PDPH, but neitherstudy showed a reduction in the incidence of headache.109
At this time, prophylactic caffeine is not advocated forprevention of PDPH.
INTRASPINAL OPIOIDSEarlier studies suggested that prophylactic neuraxial admin-istration of a hydrophilic or lipophilic opioid does notreduce the incidence of PDPH after spinal anesthesia orunintentional dural puncture.110,111 However, in a ran-domized blinded trial published in 2008, 50 obstetricpatients with unintentional dural puncture and subsequentepidural analgesia received epidural morphine 3 mg orsaline-placebo after delivery and again at 24 hours beforeremoval of the epidural catheter.112 The incidence of PDPHwas 48% in the saline-placebo group and 12% in the mor-phine group. Although no complications were reported, wewould caution against routine administration of epiduralmorphine in these circumstances until this finding is con-firmed and further safety studies are undertaken. Themovement of morphine across the dura is increased bythe presence of a large-gauge needle puncture,113 possiblyincreasing the risk of respiratory depression.
INTRATHECAL CATHETERPlacing a 19- or 20-gauge epidural catheter into theintrathecal space after an unintentional dural punc-ture with an epidural needle has become an increasingly
popular technique.93,106,114-118 The immediate benefits ofan intrathecal catheter are reliable, low-dose labor analgesiaand rapid-onset surgical anesthesia should it be required.Some authorities have speculated that the intrathecal cath-eter may reduce the immediate CSF leak into the epiduralspace by mechanical obstruction and induce an inflamma-tory fibrous reaction in the dura, which facilitates closure ofthe puncture site after removal of the catheter. Currentlyavailable studies are mostly retrospective and observationaland lack rigorous outcome definitions and follow-up. Datafrom these studies are conflicting but suggest that intrathecalcatheters do not significantly reduce the incidence of PDPHunless they are left in place for 24 hours after delivery (Table31-4). The safety of this practice has not been well studied.Randomized clinical trials to assess the effect of intrathecalcatheters on the incidence of PDPH are desirable but wouldlikely require multicenter participation owing to the infre-quent occurrence of unintentional dural puncture.
PROPHYLACTIC EPIDURAL/INTRATHECAL SALINETrivedi et al.119 randomly assigned patients with uninten-tional dural puncture to receive a prophylactic epiduralsaline bolus (40 to 60 mL) or a prophylactic epiduralblood patch (15 mL) given just prior to epidural catheterremoval, or conservative therapy without a saline bolus orblood. The incidence of PDPH was no different between thesaline and control groups (88% versus 67%, respectively).Shah120 studied 17 patients who received an epiduralsaline infusion (at a rate of approximately 40 mL/hr) for24 to 36 hours after unintentional dural puncture. Fourpatients complained of severe interscapular pain, whichresolved when the infusion rate was reduced. SeverePDPH developed in 47% of patients after the infusion wasstopped. Despite these discouraging results, prophylacticepidural saline infusions continue to be popular in somecenters. The saline infusion should not be initiated, how-ever, until residual local anesthetic effects have resolved.
In a nonrandomized, nonblinded study of patients withunintentional dural puncture, Charsley and Abram121
TABLE 31-4 Rate of Post–Dural Puncture Headache after Unintentional Dural Puncture and Prophylactic Intrathecal CatheterPlacement
Study* Study DesignSpinal Catheter,n/N (%)
No Spinal Catheter,n/N (%)
Norris & Leighton114 Retrospective cohort; catheter left in placefor 2 hr
19/35 (54) 11/21 (52)
Cohen et al.115 Retrospective cohort:Catheter discontinued immediately after delivery 8/17 (47)
5/15 (33)
Catheter left in place for 24 hr 0/13 (0)y
Dennehy & Rosaeg116 Case series; catheter left in place for 13-19 hr 0/3 (0) —Paech93 Prospective cohort; catheter discontinued
immediately after delivery21/24 (87) 60/76 (79)
Rutter et al.117 Retrospective cohort; catheter left in place forunknown duration
24/34 (71) 30/37 (81)
Ayad et al.118 Retrospective cohort:Catheter discontinued immediately after delivery 18/35 (51)y
34/37 (92)
Catheter left in place for 24 hr 2/31 (6)y
*Superscript numbers indicate reference citations at the end of the chapter.
yDifferent than no-catheter, P< .05.
688 Part VIII Anesthetic Complications
reported that intrathecal injection of 10 mL of normalsaline immediately before needle or catheter withdrawalresulted in a lower incidence of headache and theneed for blood patch in patients so treated than in a non-randomized control group. The intrathecal injection ofsaline after unintentional dural puncture deserves furtherstudy.
PROPHYLACTIC BLOOD PATCHInterest in the use of prophylactic epidural blood patchprior to removal of the epidural catheter arose after earlyobservational studies suggesting that the incidence ofPDPH was lower with such treatment.119,122,123 A 2001Cochrane review identified two randomized studies involv-ing 65 women, which demonstrated a reduction in the riskof any postpartum headache after unintentional dural punc-ture (odds ratio, 0.06; 95% CI, 0.02 to 0.15).124 However,this review highlighted the difficulty in estimating risk andbenefit with small numbers of patients and PDPH events. In2004 Scavone et al.125 reported a double-blinded trial inwhich 64 parturients with unintentional dural puncturewere randomly assigned to receive 20 mL of autologousblood (prophylactic epidural patch) or a sham prophylacticblood patch. Both groups had a 56% incidence of PDPH;however, the duration of headache was shorter in the pro-phylactic blood patch group.
Because unintentional dural puncture with a 16- or18-gauge epidural needle results in a high incidence ofPDPH, some anesthesia providers believe that a prophylac-tic blood patch is always justified. Others argue that withsuch an approach, a significant number of patients wouldreceive unnecessary treatment and that a blood patch is notdevoid of complications. These latter anesthesia providerscall attention to the potential for epidural catheters tobecome contaminated after prolonged use. The injectionof blood through a contaminated epidural catheter maybe associated with a higher risk of infection than injectionthrough an epidural needle placed de novo for a therapeu-tic blood patch. A case report of a parturient whoreceived a prophylactic epidural blood patch and wassubsequently diagnosed with streptococcal septicemia high-lights the potential risk for maternal infection during thepuerperium.126
If performed, a prophylactic blood patch procedureshould be delayed until residual neuroblockade hasresolved, for several reasons. First, the patient should havefull return of sensation because the occurrence of pain is asignal for the anesthesia provider to stop the injection ofblood. Second, evidence suggests that lidocaine may inhibitcoagulation.127 Third, Leivers128 reported a case of totalspinal anesthesia after the epidural injection of 15 mL ofblood before epidural anesthesia had regressed. This inves-tigator speculated that residual lidocaine in the lumbarCSF was transferred to the brain as a consequence of anincrease in lumbar CSF pressure produced by the patch.(Editors’ Note: One of us [D.H.C.] has observed one caseof transient, total blindness after the rapid, bolus injectionof 30 mL of epidural saline following vaginal delivery in apatient who had experienced unintentional dural punctureduring labor. The blindness resolved after approximately15 to 20 minutes, and subsequent ophthalmologic and neu-rologic findings were normal. The etiology of the transientblindness was unclear. Nonetheless, it seems prudent to
delay administration of prophylactic epidural saline orblood until the nerve block has regressed and toavoid rapid epidural administration of blood or saline atany time.)
It is important to avoid the direct intrathecal injection ofblood. Aldrete and Brown129 reported a case of intrathecalhematoma and arachnoiditis with prolonged neurologicsequelae after prophylactic blood patch. Nineteen millilitersof blood were injected through an epidural catheter that,in retrospect, was positioned in the subarachnoid space.There was considerable resistance to injection of theblood, and severe lower back pain with tinnitus accompa-nied the procedure.
PROPHYLACTIC DEXTRAN PATCHSalvador et al.130 reported the prophylactic epiduralinjection of 20 mL of dextran-40 in 17 patients who hadexperienced unintentional dural puncture with a 17- or18-gauge needle. Three of the patients were parturients,and none of the 17 patients experienced PDPH. This injec-tion was performed before regression of the local anestheticeffect. No additional studies of this technique have beenreported, so its safety and efficacy remain unclear.
Treatment
Early treatment of PDPH is indicated. Not only does it avertthe vicious cycle of immobility, weakness, and depression,but also it may help prevent the rare case of subduralhematoma or cranial nerve palsy in the patient with persis-tent PDPH.
PSYCHOLOGICAL SUPPORTThe patient is aware that PDPH is an iatrogenic problem,and she may be angry and resentful as well as depressed andtearful. Headache makes it more difficult to provide care forthe newborn and to interact with other family members.Severe PDPH may delay discharge from the hospital andmay also have economic consequences.101 Unlike patientswho have PDPH after nonobstetric surgery, postpartumpatients typically are healthy and do not expect to feel ill.Two patients have eloquently described their own misera-ble experiences with postpartum PDPH.131,132 Not surpris-ingly, a retrospective study of 43 obstetric patients withPDPH showed that this complication leads to a negativeattitude toward epidural anesthesia.133
It is essential that anesthesia providers visit the patient atleast once daily to explain symptoms and prognosis,give support, and offer therapeutic options. If feasible, thepatient’s partner should attend these discussions. Nursescan help the patient by ensuring that analgesics are givenon a regular schedule and by teaching alternative breast-feeding techniques, such as the lateral horizontal position.
The anesthesia providers and nurses should writedetailed notes in the patient’s record. After discharge,follow-up telephone conversations should be documented.Headache associated with neuraxial anesthesia was thethird most common reason for litigation among obstet-ric cases in the American Society of AnesthesiologistsClosed-Claims Project database (see Chapter 33), aftermaternal death and newborn brain damage. This factshould dispel any notion that postpartum PDPH is a trivialcomplaint.
Chapter 31 Postpartum Headache 689
POSTUREThe diagnosis of PDPH requires demonstration of a pos-tural component. Significant relief should occur whenthe patient assumes the horizontal position. The proneposition relieves PDPH in some patients, presumablybecause increased intra-abdominal pressure results in anincrease in CSF pressure. Unfortunately, this position isnot comfortable for many patients, especially those whohad a cesarean delivery.
HYDRATIONEnhanced oral hydration remains a popular therapyinitiated by most anesthesia providers for parturients withPDPH,134 but there is no evidence that vigorous hydrationhas any therapeutic benefit in a patient with normal fluidintake. However, no patient with PDPH should be allowedto become dehydrated, because of the fluid requirementsassociated with breast milk and CSF production.
ABDOMINAL BINDERA tight abdominal binder increases intra-abdominal pres-sure, possibly leading to an increase in CSF pressure.This method of treatment has never undergone properassessment.
PHARMACOLOGIC TREATMENTIn the past, a variety of drugs have been used to treat PDPH,including steroids, vasopressin, alcohol, and ergotamine. Asafe and effective oral drug therapy for PDPH would be veryuseful, even if relief is transient. Blood patch therapy is notappropriate or effective in all patients.
Caffeine
Caffeine has been used to treat PDPH for many years,despite lack of clear evidence of its efficacy. A systematicreview of the literature identified a single randomized trialperformed by Camann et al.135 In that trial, 40 postpartumwomen with PDPH received a one-time dose of oral caf-feine 300 mg or placebo. Headache scores (visual analogscale [VAS]) were lower in the caffeine group at 4 hoursthan in the control group (33 ± 6 versus 49 ± 7 mm, respec-tively), but there was no difference at 24 hours. It appearsthat the beneficial effect of caffeine is transient.
The caffeine content of a 150-mL cup of drip coffee isapproximately 150 mg. Caffeine is a cerebral vasoconstric-tor, and one study has demonstrated a reduction of cerebralblood flow after intravenous administration of caffeinesodium benzoate for the treatment of PDPH.136 Caffeineis also a potent central nervous system stimulant. Thereare published case reports of seizures after intravenousadministration of caffeine for the treatment of PDPH inpostpartum patients.137 Bolton et al.138 described a seizureshortly after combined blood patch and intravenous caf-feine therapy. Paech139 reported seizures in a patient whohad received oral caffeine (1000 mg during a 23-hourperiod). Transient atrial fibrillation complicated intrave-nous caffeine therapy for PDPH in a 71-year-old man.140
Caffeine appears in breast milk in very small amounts.141
To our knowledge, there are no reports of adverse effectson the infant after maternal administration of one ortwo doses of caffeine for the treatment of PDPH. Therisk-to-benefit ratio to mother and baby of multiple dosesof caffeine has not been addressed. Until such studies are
available it seems wise to restrict the prescription of oralcaffeine to 600 mg in 24 hours, administered in divideddoses at least 8 hours apart. Long-term caffeine therapycannot be recommended. Another methylxanthine, theo-phylline, is also a cerebral vasoconstrictor and is availablein long-acting preparations. Some physicians have foundthat oral theophylline is more effective than placebo inthe treatment of PDPH, but it has not become a populartherapy.142
Sumatriptan
Sumatriptan is a serotonin receptor agonist that affectspredominantly type 1D receptors. Possessing cerebral vaso-constrictor properties, this agent is used in the treatment ofmigraine. It is given by subcutaneous injection. Side effectsinclude pain at the injection site and, uncommonly, chesttightness. Sumatriptan may cause coronary artery vaso-spasm and should not be used in patients withPrinzmetal’s angina or known coronary artery disease.Carp et al.143 reported that administration of sumatriptan6 mg resulted in complete resolution of PDPH in four of sixpatients. Paech et al.93 reported relief of PDPH in one ofseven patients treated with sumatriptan. Connelly et al.144
studied 10 patients with severe PDPH scheduled forepidural blood patch who were randomly assigned toreceive sumatriptan 6 mg or placebo. After 1 hour, onlyone patient in each group had significant relief, and theinvestigators concluded that sumatriptan was of no value.
Adrenocorticotropic Hormone
The use of adrenocorticotropic hormone (ACTH) for thetreatment of PDPH was first reported in a 1994 letterto the editor.145 Subsequently, anecdotal reports havedescribed different regimens of either intramuscular orintravenously administered ACTH or the synthetic drugscosyntropin and tetracosactrin acetate. Mood elevation,anti-inflammatory effects, increased endorphin levels, andaugmented intravascular volume are postulated as possiblemodes of action in the relief of headache with ACTH.Kshatri and Foster146 described a curative response toACTH in two patients with PDPH. The dose used was1.5 U/kg in 250 mL of normal saline, infused intravenouslyover 30 minutes. Gupta and Agrawal147 assessed the effectof ACTH 60 U intramuscularly in 48 patients with PDPH.Complete and permanent relief was obtained in 40patients, without any side effects. Carter andPasupuleti148 reported the management of a patient withintractable PDPH who had already received three epiduralblood patches; cosyntropin 0.5 mg in 1 L lactated Ringer’ssolution was infused over 8 hours, and the headache wascompletely and permanently relieved.
To date the only randomized clinical trial of ACTHinvolved 18 postpartum women who had PDPH aftereither spinal anesthesia or unintentional dural puncture.149
There was no difference in the severity of headache or therequirement for epidural blood patch between womenwho received tetracosactrin acetate 1 mg intramuscularlyand those who received saline-placebo.
Oliver and White150 described three patients who expe-rienced PDPH after administration of epidural analgesiaduring labor and who subsequently had seizures. All hadreceived two or three doses of tetracosactrin acetate (1 mgintramuscularly), and one had also received sumatriptan.
690 Part VIII Anesthetic Complications
No epidural blood patch procedures were performed. CTscans showed or suggested infarction in two of these sub-jects. The investigators stated that before the occurrence ofthese three cases, ACTH had been used regularly to treatPDPH in their institution but that subsequently they haddiscontinued the administration of ACTH as a therapy forPDPH. No conclusion can be drawn about the possiblecontribution of ACTH therapy to the observed seizureactivity. With the evidence to date, it appears that ACTHtherapy cannot be recommended as first-line treatment ofPDPH but may be considered for cases that are not ame-nable to epidural blood patch therapy.
Miscellaneous Medications
Other agents evaluated for their effectiveness in reducingPDPH symptoms are gabapentin, methylergonovine, andhydrocortisone. Perhaps the most compelling evidence isfor the use of intravenous hydrocortisone (200-mg loadingdose followed by 100 mg three times daily for 2 days).151
Noyan Ashraf et al.151 evaluated 60 parturients who expe-rienced PDPH after spinal anesthesia and were randomlyassigned to receive intravenous hydrocortisone or conven-tional therapy, which consisted of bed rest, hydration, andscheduled acetaminophen with meperidine. Patients whoreceived hydrocortisone had a 50% reduction in headacheseverity as assessed by VAS scores at 6 to 48 hours. A crit-icism of this study is the lack of blinding of the study parti-cipants, which may have influenced their perception ofheadache pain.
Use of gabapentin or methylergonovine has beenreported only in case series. Efficacy and side effects(maternal and neonatal) are unclear.152,153 All three drugsrequire further study before they can be recommended fortherapy of PDPH.
EPIDURAL MORPHINEEldor et al.154 reported six nonobstetric patients whoreceived epidural morphine 3.5 to 4.5 mg to relieve thesymptoms of PDPH. However, this therapy should beused with caution because epidural morphine injected inthe presence of a large dural puncture site may pass readilyinto the CSF and predispose to respiratory depression.
EPIDURAL/INTRATHECAL SALINEThe use of epidural or intrathecal fluids to treat PDPHpreceded epidural blood patch therapy. Intrathecal injectionof fluid was first described by Jacobaeus et al.155 in 1923,and epidural injection of saline was first described by Riceand Dabbs156 in 1950. These first reports were described inconjunction with research attempting to understand thepathophysiology of PDPH, and they demonstrated transientelevation of CSF pressure after fluid injection. Subsequentlythere has been sporadic interest in the injection of fluids(other than blood) into the neuraxial space to treat PDPH.
Usubiaga et al.157 reported the injection of 10 to 30 mL ofsaline through a lumbar epidural catheter in 11 patientswith PDPH after spinal anesthesia in whom 48 hours ofconservative therapy failed. Immediate relief of headachewas observed in 10 patients, and the relief was permanentin 8 patients. However, the investigators did not commentwhether other therapies (e.g., supine posture, abdominalbinder, analgesics) were continued. In a quasi-randomizedtrial, 43 parturients with PDPH after unintentional dural
puncture during an epidural procedure or after spinal anes-thesia with a 25-gauge needle were assigned to receive a 30-mL epidural saline bolus in the lumbar region or a 10-mLlumbar epidural blood patch.158 Forty-two patients had dra-matic relief of their symptoms in the first hour followingthe intervention; however 12 of the 21 (57%) patients whoreceived saline had recurrence of the PDPH in the next24 hours.
Prolonged epidural saline infusion may provide bettertherapy for PDPH symptoms than therapy with a singlebolus.159,160 Two case reports described the use of epiduralsaline infusion for parturients with an unintentional duralpuncture, whose PDPH symptoms returned after epiduralblood patch therapy. The rate of infusion (15 to 25 mL/hr)was limited by the onset of pain in the back, legs, and eyes.A comparative study of epidural saline bolus versus infusionto treat PDPH is needed to determine whether eithermodality continued over 24 hours would provide betterresults than conservative therapy. This option might beconsidered for patients who have a contraindication toepidural blood patch therapy.
EPIDURAL BLOOD PATCHEfficacy
The epidural blood patch procedure, regarded by many asthe gold standard therapy for PDPH, was first described byGormley161 in 1960. He reported relief of PDPH symptomsin seven patients after epidural administration of 2 to 3 mLof blood. However, this report was largely ignored until1970, when DiGiovanni and Dunbar162 described theimmediate and permanent cure of PDPH in 41 of 45patients in whom 10 mL of autologous blood was injectedinto the epidural space. Their success led to the widespreadadoption of this technique for the relief of PDPH. An excel-lent review of the history of PDPH and the development ofthe blood patch was written by Harrington.163
In early case series, the reported success rate of epiduralblood patch therapy for PDPH was between 89% and91%.162,164 Subsequent studies have not confirmed thishigh rate of success. Taivainen et al.165 studied 81 patientswith PDPH after spinal needle puncture. Initially symptomswere relieved in 88% to 96% of patients; however, a perma-nent cure was achieved in only 61%. Safa-Tisseront et al.166
reviewed the experience with blood patch therapy at theirinstitution over a 12-year period (n = 504, including78 obstetric patients). Complete relief of PDPH wasobtained in 75%, partial relief occurred in 18%, and treat-ment failed in 7% of patients. The investigators noted asignificantly higher failure rate of blood patch after large-gauge needle puncture of the dura. The difference in earlyreports and more modern audits of PDPH and epiduralblood patch therapy success may be related to differencesin the duration of follow-up, or perhaps to other differencesin management after blood patch therapy, such as delayedmobilization.
In studies limited to obstetric patients, the publishedsuccess rates of the epidural blood patch have been evenless encouraging. Stride and Cooper62 noted complete andpermanent relief of PDPH in 64% of patients after oneblood patch procedure. Williams et al.94 reported thatonly 33% of their patients obtained complete and perma-nent relief from the first blood patch. Banks et al.167
prospectively monitored 100 patients with unintentional
Chapter 31 Postpartum Headache 691
dural puncture. Fifty-eight patients received a therapeuticblood patch; the treatment completely failed in 3 patients,and 17 patients had recurrence of moderate or severe head-ache requiring further therapy. These observational studiesalso describe the use of repeated epidural blood patch pro-cedures for parturients with a recurrence of PDPH.
A 2002 Cochrane systematic review124 identified onlyone small randomized trial168 evaluating the efficacy of epi-dural blood patch therapy. This trial involved 12 heteroge-neous patients with PDPH who were randomly assigned toundergo epidural blood patch therapy with 10 to 20 mL ofblood or a sham patch procedure. Five of 6 patients receiv-ing a blood patch had complete relief of headache symp-toms at 24 hours, and none of the sham procedure patientsdid. Subsequently two additional randomized trials havebeen reported.169,170 Sandesc et al.169 reported 32 obstetricand nonobstetric patients who had PDPH symptoms for aminimum of 24 hours, who were randomly assigned toreceive either conservative therapy or an epidural bloodpatch. The primary outcome was headache VAS scores at2 and 24 hours. At 2 hours the mean VAS score for theconservative therapy group was 8.2 ± 1.4 cm compared with1.0 ± 0.18 cm for the group receiving a blood patch(P< .001). This difference remained evident at 24 hours.In the largest trial to date, 40 subjects who had PDPH for1 to 7 days were randomly assigned to receive either con-servative therapy or an epidural blood patch using 15 to20 mL of autologous blood.170 The primary outcome washeadache 24 hours after intervention, but patients werefollowed up for 1 week after therapy. The incidence ofheadache at 24 hours was 58% in the blood patch groupcompared with 90% in the conservative therapy group (rela-tive risk, 0.64; 95% CI, 0.43 to 0.96). At 1 week the differencewidened, with 16% incidence of headache in the bloodpatch group versus 86% in the conservative group. In sum-mary, administration of an autologous epidural blood patch,while not perfect, often dramatically relieves this debilitat-ing condition, and at present, it is the therapy with thegreatest likelihood of success.
The optimal volume of injected blood remains contro-versial. Better results have been obtained with injection of20 mL of blood than with the smaller volumes used byGormley and DiGiovanni.161,162 Szeinfeld et al.171 used agamma camera to observe the epidural spread of techne-tium-labeled red blood cells during and after epiduralblood patch. They injected blood until pain occurred inthe back, buttocks, or legs. The mean ± SD volume injectedwas 14.8 ± 1.7 mL of blood, and the mean ± SD spread was9.0 ± 2.0 spinal segments. Blood spread more readily in thecephalad than in the caudad direction. Blood patch relievedheadache in all 10 patients. The investigators concludedthat 12 to 15 mL of blood should be a sufficient patchvolume for most patients. Taivainen et al.165 found thatinjection of a ‘‘height-adjusted’’ volume of blood (minimumof 10 mL to a maximum of 15 mL) conferred no advantageover a standard 10-mL injection. Most anesthesia providersinject 10 to 20 mL of blood.
Beards et al.172 performed MRI studies after the perfor-mance of epidural blood patches (18 to 20 mL) in fivepatients. They noted that the injected blood spread overthree to five segments in a predominantly cephalad direc-tion. All patients had an extensive hematoma in the subcu-taneous fat, and some also had displacement of nerve roots
and/or evidence of intrathecal blood. A thick layer ofmature clot had formed by 7 hours, which had broken upinto smaller clots by 18 hours. These findings may helpexplain the back pain and occasional nerve root pain thatoccur after blood patch.
In another MRI study, Vakharia et al.50 noted compres-sion of the thecal sac and a mean spread over 4.6 segmentsafter the injection of 20 mL of blood (Figure 31-4). Djurhuuset al.173 employed CT epidurography in four patients imme-diately and 24 hours after an 18-mL blood patch. Initialimages showed adherence of clot to the dura in threepatients as well as dural compression in two patients, butthere was no evidence of compression at 24 hours.
Using a goat model, DiGiovanni et al.174 examined themicroscopic appearance of the dura as late as 6 monthsafter dural puncture. Some study animals received a 2-mLblood patch in addition to dural puncture. The investigatorsconcluded that the blood patch acted as a gelatinoustampon that produced no harmful tissue reaction.
The mechanism of epidural blood patch for relief ofPDPH is unclear. Pain relief is often rapid, but CSFvolume is not restored immediately. Thus, there must beanother explanation for the immediate relief of headachebesides ‘‘patching’’ of the dural puncture. Carrie175
hypothesized that epidural injection of blood increaseslumbar CSF pressure, an action that restores intracranialCSF pressure and decreases symptoms. Increased CSF pres-sure also may result in reflex cerebral vasoconstriction.Coombs and Hooper176 demonstrated that epidural bloodpatch therapy resulted in a threefold increase in lumbarCSF pressure. Further, they noted that 15 minutes later,lumbar CSF pressure was sustained at more than 70% ofthe peak pressure observed after the injection of blood.Kroin et al.177 observed that epidural injection of blood inrats caused a sustained increase in CSF pressure throughouta 4-hour study period.
MRI and CT studies have shown that the epidural bloodis largely resorbed or broken up 18 to 24 hours after theprocedure.172,173 It is unlikely that the increase in CSF pres-sure is sustained or that the blood acts as a mechanical plugto block CSF leak for a prolonged duration. The bloodapplied to the hole in the dura may initiate an inflammatoryreaction that facilitates puncture site repair and closure. It ispossible, and even likely, that an epidural blood patchameliorates PDPH by several mechanisms.
Timing
The optimal timing for administration of a blood patch hasnot been studied adequately. Observational studies suggestthat failure is more likely if the blood patch is performedwithin 24 hours of the dural puncture.166,178 It is unclear,however, whether this observation is a result of selectionbias. Early-onset PDPH (often resulting from dural punc-ture with a large-gauge needle) is likely to be more severeand more difficult to treat. Alternatively, a large CSF leakmay displace the clot. Partial healing of the dura may havealready occurred if a blood patch procedure is delayed, apossibility that may explain the better outcome of a delayedpatch procedure.
Technique for Blood Patch
The anesthesia provider should thoroughly explain the risksand benefits of the blood patch procedure to the patient,
692 Part VIII Anesthetic Complications
and the patient should give written informed consent forthe procedure. An epidural blood patch can be accom-plished on an outpatient basis. Contraindications to theadministration of an epidural blood patch are related tocomplications of placing a needle in the central neuraxisor the administration of blood into the epidural space;they include (1) known coagulopathy, (2) local cutaneousinfection or untreated systemic infection, (3) increased ICPdue to a space-occupying lesion, and (4) patient refusal.Transient bradycardia has been observed after administra-tion of an epidural blood patch,179 and some anesthesiaproviders may choose to establish intravenous access andmonitor the electrocardiogram (ECG) in selected patients.
The blood patch procedure should employ sterility mea-sures equivalent to those used in the performance of anyneuraxial procedure. The lateral position is more comfort-able than the sitting position for patients with severe PDPH.If the anesthesia provider is uncertain about the location ofthe dural puncture, the more caudad interspace should bechosen. The epidural space is identified in the usualmanner. Using meticulous sterile technique (includingskin preparation and draping, and donning of a mask andsterile gloves), an assistant withdraws the desired volume ofblood into a syringe, usually 10 to 20 mL. This autologous
blood is injected slowly through the epidural needle, but theinjection is terminated if severe back, leg, or neck pain orpressure occurs. Sometimes slowing the injection rate leadsto resolution of the back pain. Blood patch procedures canbe administered to Jehovah’s Witness patients with a tech-nique designed to keep blood in continuity with thecirculation.180
Occasionally, a few drops of CSF are encountered uponentry of the needle into the epidural space, leading to doubtabout correct needle placement. In this situation a smalltest dose of a local anesthetic agent may be administered,sufficient to cause a rapid onset of spinal anesthesia if theneedle tip is in the intrathecal space. If no neuroblockadeoccurs, a blood patch can be performed.
After the procedure the patient should rest quietly inthe horizontal position for 1 to 2 hours.181 Subsequentlythe patient may resume ambulation, but she should avoidvigorous physical activity for several days. It would bewise for the patient to avoid the Valsalva maneuver andheavy lifting. A stool softener should be prescribed. Mostpatients report almost instantaneous relief of headachesymptoms but may continue to have neck and back full-ness over the next 24 hours. Patients should be counseledto immediately report fever, severe back pain, or radiating
A B
FIGURE 31-4 A, Pre–blood patchmagnetic resonance imaging usingsagittal spin-echo proton density. Thedural puncture has been performedat L2 to L3, which local staticfluid collection (arrows) affirms;‘‘3’’ denotes L3 vertebral body.B, Post–blood patch magneticresonance imaging of cerebrospinalfluid flow in systole shows the longlength of the compression of thethecal sac posteriorly (arrows). (FromVakharia SB, Thomas PS, RosenbaumAE, et al. Magnetic resonance imagingof cerebrospinal fluid leak andtamponade effect of blood patch inpostdural puncture headache. AnesthAnalg 1997;84:585-90.)
Chapter 31 Postpartum Headache 693
lower extremity pain. The anesthesia provider should con-tact the patient daily for several days after the blood patchprocedure.
The blood patch procedure may be repeated if the firstone fails to relieve pain. Often the second procedure issuccessful. The diagnosis should be reconsidered if head-ache persists after two failed blood patch procedures. Aneurology consultation is desirable when a PDPH fails torespond to two blood patch procedures, and should defi-nitely be requested if there is any doubt about the diagnosis.Imaging of the head should be considered to exclude othercauses of headache.
Complications of Blood Patch Procedures
Ong et al.182 reported that the success of neuraxial anesthe-sia/analgesia was impaired in women with a prior history ofunintentional dural puncture with or without epiduralblood patch therapy. However, this conclusion has beenrefuted by follow-up studies in both obstetric183 and non-obstetric patients.184 In both of these retrospective studies,a history of blood patch therapy had no apparent effect onthe quality of subsequent epidural anesthesia. Loughreyet al.185 described a patient who experienced PDPH afterdiagnostic lumbar puncture at term gestation. A bloodpatch was administered and the headache was relieved,but 6 hours later, urgent cesarean delivery was required.Spinal anesthesia was administered via the same interver-tebral space as the blood patch procedure. The anestheticcourse and postoperative period were uneventful, and thepatient had no recurrence of headache.
Although epidural blood patch therapy is the most reli-able method of relieving PDPH symptoms, adverse out-comes are associated with the procedure. These adverseevents can be categorized into two broad groups, infec-tious/hematologic and neurologic.
Infectious/Hematologic Complications Conventional wisdomholds that the patient should be afebrile at the time of ablood patch procedure. Many anesthesia providers believethat it is wise to avoid the epidural injection of blood in thepresence of systemic infection. Meningitis has beenreported after a blood patch.186 After conservative measureshave failed, the optimal treatment of a febrile patient withsevere, persistent PDPH is controversial. Epidural infusionof saline involves the use of an indwelling epidural catheterfor many hours, which may also be undesirable in a febrilepatient. A patch using dextran-40 may be an alternative infebrile patients, but further experience in healthy patients isneeded before this technique can be recommended. Thepresence of high fever or other evidence of sepsis contra-indicates the performance of a blood patch procedure.However, we do not believe that a low-grade fever ofknown etiology is an absolute contraindication to epiduralblood patch therapy, provided that the patient is receivingappropriate antibiotic therapy. Management should be indi-vidualized, and the known benefits of blood patch therapyshould be weighed against the unknown risk of infection.
The risk of epidural blood patch therapy in the presenceof human immunodeficiency virus (HIV) infection has beendebated (see Chapter 44). However, the central nervoussystem is infected with HIV at the time of primary infec-tion; therefore, it seems unlikely that injection of autologous
blood into the epidural space would alter progression of thedisease. There are published reports of the successful use ofepidural blood patch therapy, without sequelae, in patientswho have acquired immunodeficiency syndrome (AIDS) orwho are HIV-positive.187,188
The incidence of cancer during pregnancy is increasingsecondary to advancing maternal age. The development ofPDPH in this population has raised a theoretical concernabout seeding the neuraxial space with neoplastic cells if ablood patch is performed. This concern should be discussedwith the patient and her oncologist before the procedure.Bucklin et al.189 reported the conservative management ofa woman with acute leukemia and PDPH; the investigatorsdiscussed the therapeutic options for this immunocompro-mised patient. The use of epidural fibrin glue was reportedin a nonobstetric patient with metastatic breast cancer andPDPH,190 whereas a blood patch procedure was performedfor PDPH in a young women with rhabdomyosarcoma.191
Neurologic Complications Serious or permanent problemsafter epidural blood patch therapy are rare. Diaz et al.192
wrote an excellent review of case reports of adverse neuro-logic complications after epidural blood patch procedures.These authors identified 26 reports published between 1966and 2004 and stratified the complications into neurologic,neurovascular, or inflammatory events. The events occur-ring in obstetric patients included lumbovertebral symp-toms (defined as low back pain with neurologicimpairment of the lower extremities), subdural hematoma,arachnoiditis, radicular back pain, pneumocephalus, sei-zures, and acute meningeal irritation. Compression compli-cations (i.e., lumbovertebral syndrome, subdural hematoma,cauda equina syndrome) were associated with a larger bloodpatch volume (mean of 35 mL) than the non-compressioncomplications (17 mL). Cranial nerve palsy symptoms thatwere present prior to the blood patch procedure did notuniformly resolve. The delay in administering the bloodpatch may have been a significant factor. Two patientswho were treated within 4 days of the onset of PDPH recov-ered within 6 weeks, whereas three patients treated on days9 to 11 had palsy that persisted for 3 to 4 months. Twoobstetric patients experienced new cranial nerve palsies(involving cranial nerve VII), which manifested as facialweakness after administration of an epidural blood patch.192
Abouleish et al.164 reported the results of the long-termevaluation of 118 patients who had received an epiduralblood patch. Back pain was the most common complica-tion; it occurred during the first 48 hours in 35% of patientsand persisted in 16% of patients, with a mean duration of27 days. These investigators also noted some cases of neckpain, lower extremity radicular pain, and transient temper-ature elevation.
The development of an inflammatory reaction to epidu-ral blood can cause acute arachnoiditis, an entity that canmanifest several days after the successful cure of a PDPHwith a blood patch.193 This phenomenon is believed to besecondary to free radical damage to spinal nerve roots inthe intrathecal space after hemoglobin degradation. Thereare case reports of obstetric patients presenting withthis entity and requiring analgesic therapy for prolongedperiods.194 The diagnosis is made from a presenting his-tory of severe back pain, often with radicular pain, and
694 Part VIII Anesthetic Complications
characteristic MRI findings such as nerve root clumping inthe intrathecal space and adhesions between nerve roots.
The occurrence of new neurologic symptoms after anepidural blood patch procedure should prompt consider-ation of the presence of other intracranial pathology. Suchsymptoms may include (1) mental deterioration due toincreased ICP from an intracranial tumor and (2) seizuresdue to late-onset eclampsia.26,32,195
Diaz196 described a woman in whom permanent parapa-resis and cauda equina syndrome developed after an epidu-ral blood patch with 30 mL of blood injected slowly andwithout symptoms. Low back pain and leg pain developedafter the blood patch procedure, and later the patient alsoexperienced incontinence. Twelve days after the procedure,a subdural hematoma at L2 to L4 was diagnosed and sur-gically treated. Six months later the patient still had signif-icant symptoms. Although a larger volume of blood thanusual was injected, the technique appears to have beenwithin normal practice standards. Other long-term sequelaereported in obstetric patients include a postpartum cerebralischemic event after two epidural blood patch proceduresthat resulted in permanent hemianopsia197 and a calcifiedepidural blood patch leading to chronic back pain.198
Dextran/Gelatin Patch
Dextran-40 and gelatin-based solutions, including Gelfoamand Plasmion, have been substituted for blood in epiduralpatches.130,199,200 These were chosen as alternatives toblood owing to relative contraindications to injection ofblood. The use of alternative solutions appears to bemore common in countries outside North America. In anobservational study of 56 patients, Barrios-Alarcon et al.201
reported that epidural administration of 20 to 30 mL ofdextran-40 was safe and effective for the relief of PDPH;all headaches were relieved permanently. The only sideeffect was a transient discomfort or burning sensation atthe time of injection in 6 patients. Some physicians havetreated intractable PDPH successfully by administering adextran-40 patch followed by epidural infusion of dextranat 3 mL/hr for 5 to 12 hours.202,203
Information on the neurotoxicity of these materials isscant.204 Chanimov et al.204 did not identify neurotoxicityafter infusion of dextran-40 or polygeline (a gelatinpowder) into the rat intrathecal space. However, furtherinformation is needed before these materials can be widelyadopted for epidural patches. From MRI studies of patientswith blood patches, we can anticipate that some dextranwill enter the subarachnoid space. The small but definiterisk of anaphylaxis after the injection of dextran also mustbe considered, although the risk appears minimal withdextran-40.
Fibrin Sealant Patch
Fibrin sealant is composed of fibrinogen and thrombin.Several commercial products are prepared from humanpooled plasma. Products may also contain antifibrinolytics,such as animal aprotinin.205 When injected, these productsform a firm, nonretractable fibrin clot. Epidural injection offibrin glue in rats produces a sustained increase in CSFpressure comparable to the increase that occurs after injec-tion of blood.176 Fibrin sealant has been evaluated for itseffectiveness in preventing dural leaks after spinal surgery.206
Epidural fibrin glue patch procedures have been used
successfully to treat recurrent PDPH,207 spontaneous intra-cranial hypotension,208 and CSF leak after long-term intra-thecal catheterization.209 In the future, fibrin glue may havea role in patients with intractable PDPH, but further study isrequired before it can be recommended for routine use.
Surgery
There are rare reports of curative surgical closure of a duralrent for intractable PDPH. In one case, the interval betweendural puncture and surgery was 5 years.210
SUMMARY OF TREATMENTThe parturient with PDPH should be actively managed withscheduled analgesics, and she should receive psychologicalsupport as she cares for her newborn and manages hersymptoms. If the headache is severe, the physician mayeither try caffeine or proceed directly to epidural bloodpatch. Epidural administration of fluids other than blood,such as saline or dextran, typically is not first-line therapybut may be considered when there are contraindications tothe epidural injection of autologous blood. The accuracy ofPDPH diagnosis must always be considered when atypicalsymptoms are present or when therapy fails.
Unanswered Questions
Important information about PDPH is still lacking. A large,detailed prospective study of PDPH, with and without bloodpatch therapy, with a long follow-up period (e.g., 1 year) isneeded in obstetric patients. What are the long-term effectsof both PDPH and blood patch therapy? How common areresidual back pain, neurologic symptoms, and auditory/visual symptoms, and do they interfere with everyday life?Answers to these questions are needed to enable anesthesiaproviders to give patients reliable information, establish asound basis for informed consent, and administer the bestpossible care. The Obstetric Anaesthetists’ Association andthe Association of Anaesthetists of Great Britain andIreland211 have recommended that each facility providingobstetric anesthesia services have institution-specific proto-cols for the management of PDPH, in order to facilitate theidentification of parturients with this complication and toprovide consistent care.
KEY POINTS
� Dural puncture is only one of many causes ofpostpartum headache, although many are quick toblame postpartum headaches on dural puncture. Adetailed history and physical examination along withindicated neuroimaging in selected cases shouldensure diagnostic accuracy.
� A patient with post–dural puncture headacheexperiences an exacerbation of symptoms when shemoves from the horizontal to the upright position,possibly owing to decreased intracranial pressureand secondary cerebral vasodilation, which affectpain-sensitive intracranial structures.
� Anesthesia providers should use small-gauge (� 24-gauge), noncutting (pencil-point) spinal needleswhenever possible to decrease the risk of post–duralpuncture headache.
Chapter 31 Postpartum Headache 695
REFERENCES
1. Goldszmidt E, Kern R, Chaput A, Macarthur A. The incidence and
etiology of postpartum headaches: A prospective cohort study. Can
J Anaesth 2005; 52:971-7.
2. Benhamou D, Hamza J, Ducot B. Post partum headache after epidural
analgesia without dural puncture. Int J Obstet Anesth 1995; 4:17-20.
3. Headache Classification Committee of the International Headache
Society. The international classification of headache disorders.
Cephalalgia 2004; 24(Suppl 1):1-160.
4. Stella CL, Jodicke CD, How HY, et al. Postpartum headache: Is your
work-up complete? Am J Obstet Gynecol 2007; 196:318. e1-7.
5. Lipton RB, Scher AI, Kolodner K, et al. Migraine in the United
States: Epidemiology and patterns of health care use. Neurology
2002; 58:885-94.
6. Sances G, Granella F, Nappi RE, et al. Course of migraine during
pregnancy and postpartum: A prospective study. Cephalalgia 2003;
23:197-205.
7. Adeney KL, Williams MA. Migraine headaches and preeclampsia: An
epidemiologic review. Headache 2006; 46:794-803.
8. Sibai BM. Diagnosis, prevention, and management of eclampsia.
Obstet Gynecol 2005; 105:402-10.
9. Hinchey J, Chaves C, Appignani B, et al. A reversible posterior leuko-
encephalopathy syndrome. N Engl J Med 1996; 334:494-500.
nial tumor after obstetric anesthesia. Anesthesiology 1979; 51:92-4.
35. Mokri B. Headaches caused by decreased intracranial pressure:
Diagnosis and management. Curr Opin Neurol 2003; 16:319-26.
36. Albayram S, Tuzgen S, Gunduz A, et al. Spontaneous intracranial
hypotension after labor without spinal intervention. Eur J Neurol
2008; 15:91-3.
37. Sobol SE, Frenkiel S, Nachtigal D, et al. Clinical manifestations of
sinonasal pathology during pregnancy. J Otolaryngol 2001; 30:24-8.
38. Weber JG, Klindworth JT, Arnold JJ, et al. Prophylactic intravenous
administration of caffeine and recovery after ambulatory surgical pro-
cedures. Mayo Clin Proc 1997; 72:621-6.
39. Shapiro RE. Caffeine and headaches. Neurol Sci 2007; 28(Suppl
2):S179-83.
40. Askmark H, Lundberg PO. Lactation headache—a new form of head-
ache? Cephalalgia 1989; 9:119-22.
41. Thorley V. Lactational headache: A lactation consultant’s diary. J Hum
Lact 1997; 13:51-3.
42. Choi PT, Galinski SE, Takeuchi L, et al. PDPH is a common compli-
cation of neuraxial blockade in parturients: A meta-analysis of obstet-
rical studies. Can J Anaesth 2003; 50:460-9.
43. Lybecker H, Djernes M, Schmidt JF. Postdural puncture headache
(PDPH): Onset, duration, severity, and associated symptoms: An anal-
ysis of 75 consecutive patients with PDPH. Acta Anaesthesiol Scand
1995; 39:605-12.
44. Ok G, Tok D, Erbuyun K, et al. Hearing loss does not occur in young
patients undergoing spinal anesthesia. Reg Anesth Pain Med 2004;
29:430-3.
� The initial therapy for post–dural punctureheadache consists of psychological support, bed restin the horizontal position, and scheduled oralanalgesics. Although dehydration should be avoided,no evidence supports a role for vigorous hydrationfor prophylaxis or therapy of post–dural punctureheadache.
� The ‘‘gold standard’’ for therapy of post–duralpuncture headache is autologous epidural bloodpatch. A second blood patch procedure may beperformed—and typically is successful—if the firstone fails. If the second procedure fails, alternativediagnoses should be excluded. Other therapies havenot proved as effective and safe as the epiduralblood patch for treatment of post–dural punctureheadache.
696 Part VIII Anesthetic Complications
45. Shearer VE, Jhaveri HS, Cunningham FG. Puerperal seizures after