Page 1
LUND UNIVERSITY
PO Box 117221 00 Lund+46 46-222 00 00
Posture, postural ability and mobility in cerebral palsy
Rodby Bousquet, Elisabet
2012
Link to publication
Citation for published version (APA):Rodby Bousquet, E. (2012). Posture, postural ability and mobility in cerebral palsy Department of Orthopaedics,Lund University
General rightsCopyright and moral rights for the publications made accessible in the public portal are retained by the authorsand/or other copyright owners and it is a condition of accessing publications that users recognise and abide by thelegal requirements associated with these rights.
• Users may download and print one copy of any publication from the public portal for the purpose of private studyor research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portalTake down policyIf you believe that this document breaches copyright please contact us providing details, and we will removeaccess to the work immediately and investigate your claim.
Page 2
Posture, postural ability and
mobility in cerebral palsy
Elisabet Rodby Bousquet
Page 3
Copyright © Elisabet Rodby Bousquet
Faculty of Medicine, Department of Orthopaedics
ISBN 978-91-87189-64-7
ISSN 1652-8220
Printed in Sweden by Media-Tryck, Lund University
Lund 2012
Page 4
Contents
Abstract 5
Abbreviations 6
Definitions 7
Original papers 9
Thesis at a glance 10
Introduction 11
Cerebral palsy 11
Definitions 11
Prevalence 12
Classifications 12
Musculoskeletal problems 15
CPUP - Cerebral Palsy follow up program 16
Sitting and standing 17
Mobility 18
Systems theory and motor control 18
Posture and postural ability 19
Assessment tools for posture 20
The Posture and Postural Ability Scale 21
The Functional Mobility Scale 23
Aims 24
Methods 25
Design 25
Participants 25
Data collection 27
Page 5
Statistical analysis 28
Ethical considerations 29
Results 30
Sitting and standing (study I) 30
Wheeled mobility (study II) 31
Walking performance (study III) 32
Postural asymmetries (study IV) 33
Evaluation of the Posture and Postural Ability Scale (study V) 35
Discussion 37
Sitting and standing 37
Wheeled mobility 39
Walking performance 41
Postural asymmetries 43
Evaluation of the Posture and Postural Ability Scale 45
Conclusions 47
Further research 48
Sammanfattning, Summary in Swedish 49
Acknowledgements 51
References 53
Page 6
5
Abstract
Cerebral palsy (CP) is the most common cause of motor disability in children and
adolescents with a prevalence of 2-3/1000. CP is characterized by disorders of
posture and movement with impairments ranging from mild to severe. The ability
to control posture is an important prerequisite for all voluntary movements. A
sustained asymmetric posture predisposes to progressive deformities in people
with CP, such as scoliosis, hip dislocations and contractures.
The aim of this thesis was to enhance knowledge of posture, postural ability and
mobility in people with CP, their use of assistive devices and also to evaluate a
clinical tool for assessment of posture and postural ability.
Study I-III were cross-sectional studies of 562 children with CP, aged 3-18 years,
describing sitting, standing, sit-to-stand and the use of assistive devices, wheeled
mobility, and walking performance according to the Functional Mobility Scale.
The results were analyzed relative to the expanded and revised version of the
Gross Motor Function Classification System (GMFCS), neurological subtype and
age. Study IV was a cross-sectional study describing postural asymmetries and
ability to change position in 102 young adults with CP aged 19-23 years; and the
relation of posture to pain, range of motion, hip dislocation, scoliosis and ability to
change position. Study V evaluated the psychometric properties of the Posture and
Postural Ability Scale for adults with CP at GMFCS I-V.
The GMFCS is a good predictor of sitting and standing performance. Powered
wheelchairs provided independent mobility in most cases while few self-propelled
their manual wheelchairs. To achieve a high level of independent mobility,
powered wheelchairs should be considered at an early age for children with
impaired walking ability. The number of children who walked without aids
increased up to 7 years, but the proportion of children walking independently on
uneven surfaces was incrementally higher in each age group up to 18 years.
Postural asymmetries were associated with scoliosis, hip dislocation, hip and knee
contractures, and inability to change position. The Posture and Postural Ability
scale showed an excellent interrater reliability for experienced raters, a high
internal consistency and construct validity. It can detect postural asymmetries in
adults with CP at all levels of gross motor function.
Page 7
6
Abbreviations
CP Cerebral Palsy
CPUP Cerebral Palsy follow-up Programme and National Quality Register
FMS Functional Mobility Scale
GMFCS Gross Motor Function Classification System
ICF International Classification of Functioning, Disability and Health
PAS Postural Ability Scale
PPAS Posture and Postural Ability Scale
ROM Joint Range of Motion
SCPE Surveillance of Cerebral Palsy in Europe
Page 8
7
Definitions
Assistive devices Any product, instrument, equipment or technology
adapted or specially designed for improving the
functioning of a disabled person.
Cerebral palsy A group of permanent disorders of the development
of movement and posture, causing activity limitation,
that are attributed to non-progressive disturbances
that occurred in the developing fetal or infant brain.
The motor disorders are often accompanied by
disturbances of sensation, perception, cognition,
communication, and behavior, epilepsy, and
secondary musculoskeletal problems.
Environment The physical, social and attitudinal conditions which
are present in an individual’s life.
Hip dislocation Reimers’s migration percentage of 100%1.
Mobility Transferring from one place to another, by walking,
or by using various forms of transportation.
Performance What a person actually “does do” in a daily life
situation, and differs from what a person “can do”.
Posture The shape of the body i.e. the anatomical alignment
of the body segments in relation to each other and
the supporting surface and also the relationship
between the body and the environment.
Postural ability The ability to stabilize the body segments relative to
each other and to the supporting surface; to get into
the most appropriate body configuration for the
performance of the particular task and environment.
This means control of the center of gravity relative to
the base of support during both static and dynamic
conditions.
Page 10
9
Original papers
This thesis is based on the following original papers referred to in the text by their
Roman numerals:
I Rodby-Bousquet E, Hägglund G. Sitting and standing performance
in a total population of children with cerebral palsy: a cross-
sectional study. BMC Musculoskeletal Disorders 2010,11:131
II Rodby-Bousquet E, Hägglund G. Use of manual and powered
wheelchair in children with cerebral palsy: a cross-sectional study.
BMC Pediatrics 2010,10:59
III Rodby-Bousquet E, Hägglund G. Better walking performance in
older children with cerebral palsy. Clinical Orthopaedics and
Related Research 2012, Vol.470(5), pp 1286-1293
IV Rodby-Bousquet E, Hägglund G, Westbom L. Postural asymme-
tries in young adults with cerebral palsy (Submitted)
V Rodby-Bousquet E, Ágústsson A, Jónsdóttir G, Czuba T, Johansson
A-C, Hägglund G. Interrater reliability and construct validity of the
Posture and Postural Ability Scale in adults with cerebral palsy, in
supine, prone, sitting and standing positions. Clinical Rehabilitation
(In press)
Page 11
10
Thesis at a glance
Questions Methods Results Conclusions
I
How do children with CP usually sit, stand, and move between sitting and standing position? What is their use of assistive devices or external support?
Cross sectional study of a total population of 562 children with CP 3-18 years. Use of support or assistive devices to sit, stand, stand up and sit down was analyzed relative to GMFCS, CP subtype and age.
Standard chairs were used by 57%, 62-63% could stand and move between sitting and standing without support. Adaptive seating was used by 42%, support to stand by 31%, and to move from sit-to-stand and back by 18-19%.
Sitting, standing performance and the ability to move between these positions were highly correlated to GMFCS level. The GMFCS is age-related and seems to be a good predictor of sitting and standing performance.
II
What is the use of manual and powered wheelchairs and the degree of independent wheeled mobility in children with CP?
Cross sectional study based on data from the CPUP register of 562 children with CP, 3-18 years. Wheeled mobility was analyzed in relation to GMFCS, subtype and age.
Wheelchairs were used by 165 (29%) indoors, 61 for independent mobility and 104 were pushed by an adult. Wheelchairs were used by 228 child-ren (41%) outdoors; 66 for independent mobility and 162 were pushed.
Powered wheelchairs provided independent mobility in most cases (86%) while manual wheelchairs only did in 14%. To achieve independent mobility powered wheelchairs should be considered at an early age for children with impaired walking ability.
III
How does walking performance differ at different distances and environments, in children with CP?
Cross sectional study of 562 children with CP, 3-18 years. The Functional Mobility Scale (FMS) was used to rate mobility in relation to GMFCS, CP subtype, and age.
FMS correlated to GMFCS and varied between the subtypes. An increased proportion of children walked indepen-dently on all surfaces in each successive age group. 57- 63% walked without and 4-8% with walking aids.
The number of children who walked without walking aids increased up to 7 years, but the proportion of children walking independently on uneven surfaces was higher in each age group up to 18 years.
IV
What is the relationship between posture and the ability to change position, pain, contractures, hip dislocation and scoliosis in adults with CP?
Cross-sectional study of a total population of 102 adults with CP, 19-23 years. Analysis of the relationship between posture and joint range of motion, hip dislocation, scoliosis and pain.
Postural asymmetries were present at all GMFCS levels but more frequent at lower levels of motor function. Hip dislocation and scoliosis increase the odds ratio for an asymmetric posture.
Postural asymmetries were associated with scoliosis, hip dislocation, hip and knee contractures, and inability to change position.
V
How are the psychometric properties of the Posture and Postural Ability Scale for adults with CP?
Posture and postural ability was rated from photos and videos of 30 adults with CP, by three independent raters. Construct validity was evaluated based on known groups, GMFCS I-V.
Excellent interrater reliability (w kappa=0.85-0.99), high internal consistency (alpha=0.96-0.97, item-total correlation=0.60-0.91). Median values differed (p<0.02) between known groups.
The Posture and Postural Ability Scale showed an excellent interrater reliability for experienced raters, a high internal consistency and construct validity. It can detect postural asymmetries in adults with CP at all levels of gross motor function.
Page 12
11
Introduction
Cerebral palsy
Cerebral palsy (CP) is a lifelong heterogeneous disorder affecting posture and
movement. It is the most common cause of motor disability in children and
adolescents with a prevalence of 2-3 children per 10002-8
. The children grow into
adults and the expected survival rate for people with CP is almost the same as for
the general population9. The severity of impairments varies greatly and the
mobility ranges from independent walking to totally dependent wheelchair
mobility4. The motor disorder is often combined with associated impairments such
as learning disability, epilepsy and visual impairment3; 10; 11
. CP was first described
by an orthopaedic surgeon in England, William Little 150 years ago (1862)12; 13
.
He described contractures and deformities resulting from spasticity and paralysis
due to brain damage during infancy, especially in children born pre-term or with
complicated births causing perinatal asphyxia. The condition was sometimes
accompanied by epilepsy and behavioral disorders. Little classified cerebral palsy
in children according to clinical symptoms into hemiplegia (one side more affected
than the other), paraplegia (legs more affected than arms) and generalized
rigidity12
.
Definitions
There have been several attempts to define CP throughout the years. In 1959 Mac
Keith et al14
defined CP as ‘a persisting qualitative motor disorder appearing
before the age of three years, due to a non-progressive interference with
development of the brain.’ Some years later Bax et al (1964)15
proposed the
following definition of CP; ‘a disorder of movement and posture due to a defect or
lesion of the immature brain.’ In 1992 Mutch et al16
defined CP as ‘an umbrella
term covering a group of non-progressive, but often changing, motor impairment
syndromes secondary to lesions or anomalies of the brain arising in the early
stages of development’. The most recent definition and the one used in this thesis
was presented by Rosenbaum et al in 200617
where CP is described as ‘a group of
permanent disorders of the development of movement and posture, causing
Page 13
12
activity limitation, that are attributed to non-progressive disturbances that occurred
in the developing fetal or infant brain. The motor disorders are often accompanied
by disturbances of sensation, perception, cognition, communication, and behavior,
epilepsy, and secondary musculoskeletal problems’.
Prevalence
The prevalence of cerebral palsy in the western world, about 2-3/10002-8
, has not
decreased during the last decades in spite of improvements in maternal health and
neonatal care2; 18
. This could be explained by a decrease in perinatal mortality and
at the same time an increase in survival for children born preterm2; 18
.
The live birth prevalence of CP for the period of 1980 to 1990 was 2.08/1000 in a
study by the Surveillance of Cerebral Palsy in Europe network (SCPE) in 20024.
The prevalence of CP in southern Sweden (Skåne, Blekinge) was 2.4/1000 at 4-7
years of age and 2.8/1000 at 8-11 years of age in children born 1990-1993,
including children born abroad, and the mortality rate was low before 20 years of
age3; 6; 9
. The CP prevalence in adults is less well studied. Young people 17-20
years born 1988-1991 and living in Skåne, Blekinge the 1st
of Jan 2009 had a CP
prevalence of 2.3/1000 and formed the basis of study IV.
Classifications
There have been different classifications of CP since the first was proposed by
Little in 186212; 13
(Table I). Mac Keith et al14
suggested a more detailed
classification based on clinical signs into; spastic CP dived into hemiplegia
(unilateral, upper limb more affected than lower limb), diplegia (bilateral, lower
limbs more affected than upper limbs) and double hemiplegia (bilateral, upper
limbs more affected than lower limbs); dystonic CP (fluctuating tone, disorders of
static and dynamic postural control), choreoathetoid CP (presence of unwanted
movements), mixed forms of CP, ataxic CP (incoordination not due to dystonia,
weakness or choreic movements) and atonic diplegia (bilateral distribution of
weakness and hypotonia).
The Swedish classification of CP subtypes by Hagberg16; 19
has been widely used
and is based on clinical signs into spastic hemiplegia (involving one side of the
body), spastic diplegia (bilateral, lower limbs more affected than upper limbs),
spastic tetraplegia (bilateral involvement of upper more or equal to lower limbs),
ataxic CP (divided into ataxic diplegia and congenital ataxia), dyskinetic CP
(divided into dystonic CP and choreoathetotic CP) and mixed form. In
Page 14
13
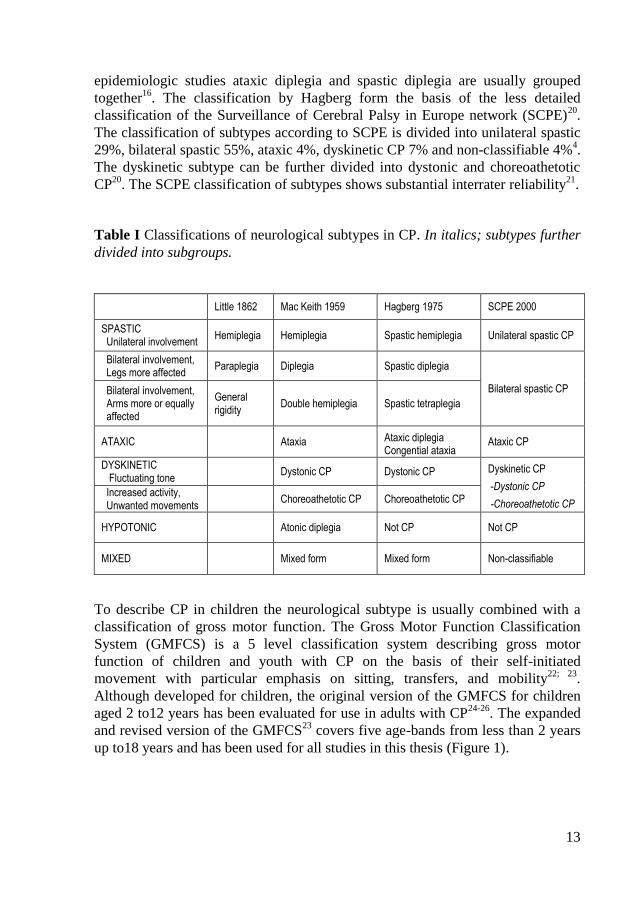
epidemiologic studies ataxic diplegia and spastic diplegia are usually grouped
together16
. The classification by Hagberg form the basis of the less detailed
classification of the Surveillance of Cerebral Palsy in Europe network (SCPE)20
.
The classification of subtypes according to SCPE is divided into unilateral spastic
29%, bilateral spastic 55%, ataxic 4%, dyskinetic CP 7% and non-classifiable 4%4.
The dyskinetic subtype can be further divided into dystonic and choreoathetotic
CP20
. The SCPE classification of subtypes shows substantial interrater reliability21
.
Table I Classifications of neurological subtypes in CP. In italics; subtypes further
divided into subgroups.
Little 1862 Mac Keith 1959 Hagberg 1975 SCPE 2000
SPASTIC Unilateral involvement
Hemiplegia Hemiplegia Spastic hemiplegia Unilateral spastic CP
Bilateral involvement, Legs more affected
Paraplegia Diplegia Spastic diplegia Bilateral spastic CP
Bilateral involvement, Arms more or equally affected
General rigidity
Double hemiplegia Spastic tetraplegia
ATAXIC Ataxia
Ataxic diplegia Congential ataxia
Ataxic CP
DYSKINETIC Fluctuating tone
Dystonic CP Dystonic CP
Dyskinetic CP
-Dystonic CP
-Choreoathetotic CP Increased activity, Unwanted movements
Choreoathetotic CP Choreoathetotic CP
HYPOTONIC Atonic diplegia Not CP Not CP
MIXED Mixed form Mixed form Non-classifiable
To describe CP in children the neurological subtype is usually combined with a
classification of gross motor function. The Gross Motor Function Classification
System (GMFCS) is a 5 level classification system describing gross motor
function of children and youth with CP on the basis of their self-initiated
movement with particular emphasis on sitting, transfers, and mobility22; 23
.
Although developed for children, the original version of the GMFCS for children
aged 2 to12 years has been evaluated for use in adults with CP24-26
. The expanded
and revised version of the GMFCS23
covers five age-bands from less than 2 years
up to18 years and has been used for all studies in this thesis (Figure 1).
Page 15
14
Figure 1 Illustration of the expanded and revised version of the GMFCS, age-band 12-18
years, reprinted with permission from professor Kerr Graham.
Page 16
15
Musculoskeletal problems
Children with CP are not usually born with deformities, and although the lesion of
the brain is non-progressive, many secondarily acquired clinical problems are
progressive, and musculoskeletal abnormalities tend to develop during
childhood27
. In both children with CP28
and typically developing children29
there is
a decline in joint range of motion as they grow older. Several studies24; 30-35
show a
decline in gross motor function in adults with CP such as reduced balance,
walking ability, range of motion together with increasing pain, physical fatigue,
and problems related to spasticity. A crouched standing posture leads to a reduced
hip and knee extension that worsens over time, due to gravity and the altered
position of the body segments in relation to each other36
. Contractures, bone and
joint deformities most commonly affect the spine and the lower extremities
leading to scoliosis, pelvic obliquity, hip dislocation, windswept deformity,
contractures of hips and knees, and foot deformities37; 38
. An asymmetric posture
increases the risk of tissue adaptation leading to these contractures and progressive
deformities39-42
. The time aspect is crucial for the development of contractures
making posture relative to time spent in these positions clinically important41; 43
.
Hip dislocations usually occur at an early age44
. In order to detect lateral migration
and prevent dislocation, children with CP should be followed with radiographs
from an early age45; 46
. Scoliosis is more frequent at lower levels of gross motor
function and the curve magnitude tends to increase with age even after bone
maturity47-49
. Severe scoliosis is associated with pelvic obliquity, windsweeping,
and hip dislocations50-52
affecting the sitting ability, but also to pain, pressure
ulcers, cardiopulmonary and gastrointestinal dysfunction51; 53
. A review of risk
factors for scoliosis by Loethers in 201054
revealed difficulties in interpreting data
since the cut-off for scoliosis on radiographs varied in different studies. In
addition, lateral migration of the hips ranging from 33-60 degrees was sometimes
defined as hip dislocation54
. However, contractures, scoliosis, hip dislocations, and
other fixed deformities can be reduced by early detection and preventive
treatment45; 46; 50; 51; 55; 56
.
The word “Orthopaedics” originates from the Greek words “orthos” (straight) and
“paideia” (children) and was introduced by the pediatrician Nicolas Andry de
Boisregard in 1741. His book “Orthopedia or the art of correcting and preventing
deformities in Children” (Figure 2) was published in English 174357
. Andry
suggested treatment that is still in use today such as early non-surgical treatment
with brace, bandages and shoes. He illustrated this as tying a tree to a pole to
straighten it out (Figure 2).
Page 17
16
Figure 2 Nicolas Andry de Boisregard, Orthopedia, 1743, "http://creativecommons.org/ns#"
During the 19th century in Sweden, physiotherapy was a scientific treatment
called “mechanical medicine”, sanctioned by the Government58
. Physiotherapy
was complementary to the chemical treatment provided by the doctors. Today,
physiotherapy and orthopaedic interventions designed to prevent contractures and
deformities in people with CP are still focused on early detection and prevention.
CPUP - Cerebral Palsy follow up programme
CPUP is a National healthcare programme for people with CP in Sweden45; 55
. It
was initiated in southern Sweden in 1994 as a collaboration by the Orthopaedic
departments and the Habilitation Centres as an attempt to detect and prevent hip
dislocations, scoliosis and contractures in children with CP. The idea was to
improve and standardize the clinical assessment and the radiographic follow up of
the children’s hips and spine from an early age. Since 2005, CPUP is a National
healthcare programme approved by the National Board of Health and Welfare in
Sweden.
The associated registry includes all children with CP born after January 1, 1990,
living in the counties of Skåne and Blekinge, which have a total population of
approximately 1.3 million. The number of children with CP in the area
corresponds to a prevalence of 2.4/10003; 6
. A search is made regularly to identify
all children with cerebral palsy in the area and invite them to participate in CPUP,
and almost all families (98%) have agreed to participate6. The CPUP health care
programme includes a continuing standardized follow up with assessment of gross
and fine motor function, mobility, joint range of motion, clinical findings, and
treatment. The children are examined by their local physiotherapist and
Page 18
17
occupational therapist twice a year until six years of age, then once a year. The
CPUP has been successful in reducing the incidence of hip dislocations in Sweden
to <1% compared to 15% in Norway46
(before Norway implemented the CPUP),
without increasing the number of operations. There has also been a reduction in
the number of severe contractures, scoliosis and windswept deformity45; 46; 50; 51; 55
.
Since 2009 CPUP is a National healthcare programme in Norway and the CPUP
programme is currently expanding to parts of Denmark and Iceland.
In 2009 a project was started to expand CPUP to include adults with cerebral
palsy. All people with CP born 1988-1991 living in the area of Skåne and
Blekinge were invited to participate in CPUP for adults. The place of living on 1st
of January 2009 was ascertained through the Swedish population register
(Statistics Sweden)59
. Adults born 1988-1989 were included in the inventory 2009.
The CP-prevalence was 2.3/1000 at the age of 17-20 years. Adults born 1990-
1991 were previously followed by the CPUP program for children, but before the
hip screening started. In order to assess the adults a form was developed which
included; clinical assessment of joint range of motion, scoliosis, posture, mobility,
gross and fine motor function, tone, and reports about pain, treatment, fractures,
use of orthosis, brace and assistive devices (www.cpup.se).
Sitting and standing
Physical therapy interventions include provision of postural support such as
adaptive seating and standing support to compensate for postural deficits and
increase function60-71
. Almost one third of children with CP are non-ambulant4 and
spend most of their lives in a sitting or lying position. The postural deficits
seriously affect the performance of daily activities in those with severe
impairments64; 72
. Difficulties in controlling voluntary movement and functional
performance can be traced to deficient postural ability73
. Adaptive seating reduces
the need for assistance from a caregiver74-76
and may facilitate daily activities and
functions such as playing77
, eating75-79
, breathing80
and arm and hand function69; 81;
82. A standing position requires more postural ability to keep the centre of gravity
within the base of support, while a sitting position provides a larger base of
support and less joints to stabilise66
. A crouched standing posture leads to a
reduced hip and knee extension that worsens over time, due to gravity and the
altered position of the body segments in relation to each other36
. Even healthy
children standing in a crouched posture show similar postural responses as
children with CP due to biomechanical changes in postural alignment83
.
Page 19
18
Mobility
Mobility in terms of transferring from one place to another, is important for the
cognitive and psychosocial development of children. Children with CP usually
start to walk later than nondisabled children84
, and they walk with a slower speed
and higher energy cost85
. Normal walking is extremely efficient and advances the
body safely from place to place with a minimum of energy86
. In children with CP
there is a strong correlation between the energy cost of walking and the degree of
motor impairment87; 88
. The energy consumption is increased when walking with
assistive devices89-92
. Many children with CP walk in a crouched posture36; 83; 86; 93
.
The crouched gait often worsens over time as a result of increasing muscle
contractures, increasing body weight, and decreasing muscle strength compounded
by gravity94
. Thus, the achieved walking ability is not always maintained through
adolescence and adulthood32; 35; 95
.
Independent mobility is important for activity, participation, and self-sufficiency,
reducing the dependence on caregivers and the environment96-100
. Environmental
and personal factors influence a particular child’s performance in an everyday life
situation101; 102
. Safety and efficiency are important aspects when choosing
mobility methods in different environments100; 103
. Assistive devices for mobility
such as wheelchairs and walking aids can provide independent mobility to children
with disabilities, allowing them to explore their environment96-98; 104
, improving
activity, participation, satisfaction and quality of life105
. Powered wheelchairs
facilitate independent mobility while manual wheelchairs mainly ease the care
load106
. The single most important factor for the experience of participation in
adolescents with disabilities is the possibility to be ‘where it happens’107
, which is
closely related to independent mobility.
Systems theory and motor control
Two motor control theories have been used to describe development of posture
and movement in children with cerebral palsy108-110
. The reflex-hierarchical theory
from the early 1900s, where the nervous system was considered to be organized in
a top down vertical hierarchical structure where higher centres control lower
centres108-110
. Motor development was seen as a maturation of the central nervous
system with increasing corticalization, resulting in emergence of higher levels of
control over the lower levels of reflexes. Any damage to the higher levels of the
brain would result in persistent primitive lower reflexes. The treatment would
focus on techniques to facilitate normal motor patterns and inhibit reflexes and
abnormal motor patterns109
.
Page 20
19
The systems theory which takes musculoskeletal and environmental factors into
account, was first described by Nicolai Bernstein (1967)109; 111
. He viewed the
body as a mechanical system consisting of several joints and muscles with
multiple degrees of freedom. To perform coordinated movements some body
segments need to be stabilized in order to allow mobility in other segments111
. The
specific segments to be stabilized will vary with the task111; 112
. The external forces
applied to the body are gravity and reaction forces from the supporting surface112
.
Internal muscular forces counteract the external forces, providing the stability
necessary to accomplish a task112
. This control of posture includes controlling the
body’s position in space with respect to both stability and orientation ensuring that
the line of gravity falls within the base of support and each body segment is
balanced relative to the segments below109
.
According to the systems theory, movement emerges from interaction between the
individual, the task and the environment, through coordination of many brain
structures and processes109
. This requires motor programmes, perception and
cognition109
. Postural control may also be affected by the attention required when
performing dual tasks113; 114
. The assessment and training of motor function
according to the systems theory focuses on both musculoskeletal and neural
aspects. The therapist should try to identify constraints within the person, the task
or environment that prevent the person from succeeding in functional tasks109; 115
.
Posture and postural ability
There is no universal definition of posture. In this thesis, the term ‘Posture’, relates
to the shape of the body i.e. the anatomical alignment of the body segments in
relation to each other and the supporting surface and also to the relationship
between the body and the environment109; 112; 116
. ‘Postural ability’ refers to the
ability to stabilize the body segments relative to each other and to the supporting
surface; to get into the most appropriate body configuration for the performance of
the particular task and environment. This means control of the centre of gravity
relative to the base of support during both static and dynamic conditions112; 116
.
CP is characterized by disorders of posture and movement4; 64; 66; 72; 83; 117; 118
.
Posture is the base from which movement occur so the ability to control posture is
an important prerequisite for all voluntary movements117; 119
. This requires muscle
tone predominantly in trunk, neck and antigravity muscles of the legs to produce
joint stiffness, in order to counteract the forces imposed by gravity and the ground
reaction forces73; 119
. The antigravity function (stability) provides the mechanical
support necessary for performing movements119
. Even a simple task such as
Page 21
20
raising the arm requires complex control over numerous joints and muscles both to
stabilize posture and to perform the movement120
.
Normally postural responses such as righting, equilibrium and balance reactions
are controlled unconsciously by the brain stem, spinal cord and basal ganglia.
Damage in these areas may cause deficits of postural ability varying from being
unable to move within or change position to having limited ability necessitating
compensatory strategies that lead to asymmetry. Children with CP have difficulties
in fine-tuning postural adjustments64
. Typical characteristics are top-down
recruitment of postural muscles, antagonist co-activation and incomplete
modulation of muscular response64; 83
. These neuromuscular response patterns are
due to both neurological deficits and to biomechanical changes in their postural
alignment83
. Asymmetric postures have long been known to cause progressive
deformities in immobile people with CP due to the effect of gravity39-42
. Whenever
the body deviates from midline, a gravitational moment is produced which
compounds the deviation.
Assessment tools for posture
There are few tools for assessment of posture and postural ability in lying, sitting
and standing position which have been evaluated for people with severe physical
disabilities, and none of them has been evaluated for adults with CP.
For any measurement tool to be scientifically and clinically useful, it must meet
basic psychometric criteria regarding reliability and validity121
. For use in a
clinical setting the instrument should be relatively short and simple to complete
and not require expensive equipment. The Physical Ability Scale122
for assessment
of postural ability in children with severe disabilities was developed by Noreen
Hare during the 1970’s and 80’s. This inspired Pountney and co-workers to
develop the Chailey Levels of Ability61; 123
to describe stages of motor
development in typically developing infants and children with motor impairments.
Its’ validity has been evaluated for children and youth with CP124
. These
instruments form the basis of the Postural Ability Scale (PAS) developed by
Pauline Pope in the early 1990’s116
to assess both posture and postural ability in
people with severe physical disabilities regardless of age and diagnosis. This
assessment tool allows postural ability and posture to be assessed separately. It is
in clinical use for trained professionals but has not been evaluated for its
psychometric properties. During the years of 2009-2011, the PAS was developed
further by Pope and co-workers. The levels of ability were slightly modified and
items added to the quality of posture to allow assessment of posture from a sagittal
as well as a frontal view. This modified and expanded version of the PAS called
Page 22
21
the Posture and Postural Ability Scale (PPAS) has not previously been tested for
reliability or validity.
The Posture and Postural Ability Scale
The Posture and Postural Ability Scale (Table 2) contains a 7-point ordinal scale
for the assessment of postural ability in standing, sitting, supine and prone and six
items for assessment of quality of posture in the frontal plane and another six
items in the sagittal plane. Postural symmetry and alignment gives 1 point for each
item while asymmetry or deviation from midline gives 0 points. The total score of
0-6 points is calculated separately for each position in the frontal and sagittal
plane.
Figure 3 Example of a supine and a standing posture when the person is unable to
maintain an aligned position independently.
The two lower levels of postural ability are in fact a rating of no ability, that is,
they are unable to maintain or change position by themselves (Figure 3). The
difference between those two levels is whether the person can (level 2) or cannot
(level 1) conform to the position when placed by another person, i.e in anatomical
alignment when supported. When a person cannot be placed in prone and standing
due to hip dislocation or severe contractures, especially of the hip flexors, postural
ability is scored as level 1= unplaceable and posture is scored 0.
Page 23
22
Table 2 The Posture and postural ability scale (PPAS) with the 7-point ordinal scale for
assessment of postural ability in standing, sitting, supine and prone position; followed by
assessment of quality of posture. There are six items for assessment of posture in the
frontal plane and another six items in the sagittal plane.
PPAS Levels of postural ability
Level 1 Unplaceable in an aligned posture
Level 2 Placeable in an aligned posture but needs support
Level 3 Able to maintain position when placed but cannot move
Level 4 Able to initiate flexion/extension of trunk
Level 5 Able to transfer weight laterally and regain posture
Level 6 Able to move out of position
Level 7 Able to move into and out of position
Quality of posture , frontal view, (Yes = 1 point, No = 0 points)
Standing Sitting Supine Prone
Head midline Head midline Head midline Head to one side
Trunk symmetrical Trunk symmetrical Trunk symmetrical Trunk symmetrical
Pelvis neutral Pelvis neutral Pelvis neutral Pelvis neutral
Legs separated and straight relative to pelvis
Legs separated and straight relative to pelvis
Legs separated and straight relative to pelvis
Legs separated and straight relative to pelvis
Arms resting by side Arms resting by side Arms resting by side Arms resting (elevated, mid-position)
Weight evenly distributed Weight evenly distributed Weight evenly distributed Weight evenly distributed
Quality of posture , sagittal view, (Yes = 1 point, No = 0 points)
Standing Sitting Supine Prone
Head midline Head midline Head midline Trunk in neutral position
Trunk in neutral position Trunk in neutral position Trunk in neutral position Pelvis neutral
Pelvis neutral Pelvis neutral Pelvis neutral Hips extended
Legs straight, hips/knees extended
Hips mid-position (90°) Legs straight, hips/knees extended
Knees extended
Feet mid-position/flat on floor
Knees mid-position (90°) Feet resting in normal position
Arms resting (elevated, mid-position)
Weight evenly distributed Feet mid-position/flat on floor
Weight evenly distributed Weight evenly distributed
Page 24
23
The Functional Mobility Scale
The Functional Mobility Scale (FMS)125
version 2 can be used for assessment of
the child’s walking performance at three different distances and environments: 5,
50 and 500 m representing the child’s mobility at home, at school, and in the
community, respectively (Table 3). The mobility is rated according to the need of
assistive devices and is assessed by questions put to the child or parent and not by
direct observation. The FMS has been evaluated for reliability, validity, and
sensitivity125
and shows substantial agreement between direct observation and
parental report126
.
Table 3 The Functional Mobility Scale (FMS) Version 2.
____________________________________________________________ Questions
How does your child move around for short distances in the house? (5 m) How does your child move in and between classes at school? (50 m) How does your child move around for long distances such as at the shopping center? (500 m)
Ratings 6. Independent on all surfaces 5. Independent on level surfaces 4. Uses sticks (one or two) 3. Uses crutches 2. Uses a walker or frame 1. Uses wheelchair C. Crawling N. Does not apply, eg, child does not complete the distance
__________________________________________________________________
Page 25
24
Aims
The overall ambition of this thesis was to enhance knowledge of posture, postural
ability and mobility in individuals with CP, the use of assistive devices and also to
evaluate a clinical tool for assessment of posture and postural ability.
Study I: To describe how children with CP usually sit, stand, move between sitting
and standing position, and their use of support/assistive devices, related to age, CP
subtype and level of gross motor function.
Study II: To analyse the use of manual and powered wheelchair indoors and
outdoors, and the degree of independent wheeled mobility, in children with CP.
Study III: To describe walking performance and mobility in children with CP, and
to examine the association between walking performance and level of gross motor
function, CP subtype and age.
Study IV: To describe posture in supine, sitting and standing position, the ability
to change position, and also to analyse the association between posture and pain,
joint range of motion, hip dislocation, scoliosis and ability to change position in
young adults with CP.
Study V: To evaluate reliability, internal consistency and validity of the Posture
and Postural Ability Scale in adults with CP, in supine, prone, sitting and standing
position.
Page 26
25
Methods
Design
Study I-III were cross-sectional studies of a total population of children with CP
describing their sitting and standing performance and the use of assistive devices
(study I), wheeled mobility (study II), and walking performance according to the
Functional Mobility Scale (study III). Study IV was a cross-sectional study
describing postural asymmetries and ability to change position in adults with CP,
and the relation of posture to pain, joint range of motion, hip dislocation, scoliosis
and ability to change position. Study V evaluated the psychometric properties of
the Posture and Postural Ability Scale for adults with CP from photos and videos
of adults at GMFCS level I-V.
Participants
Study I-III included all children with CP followed by the CPUP and living in
southern Sweden during 2008. There was a total of 562 children (326 boys, 236
girls) aged 3 to 18 years (mean age 10.9 years) born 1990-2005 (Table 4).
Study IV included all 102 adults with CP born 1988-1991 (63 males, 39 females)
examined within the CPUP program for adults in southern Sweden, from the start
in October 2009 until the end of 2011. The participants were 19-23 years at
examination (mean age 20.5 years) (Table 4). A total of 172 adults with CP were
identified through medical records. Ten were previously not informed about the
CP diagnosis and were excluded. Invitations to participate in the CPUP health care
programme for adults were sent to 162 persons, of which 26 declined, 20 did not
answer, and 116 accepted. Four of them were recently assessed in the child
rehabilitation services according to their CPUP program, and ten failed to appear.
In total 102 adults were examined before the end of 2011. There were no
statistically significant differences found between the characteristics of
participants and non-participants, except the proportion of unknown GMFCS
levels.
Page 27
26
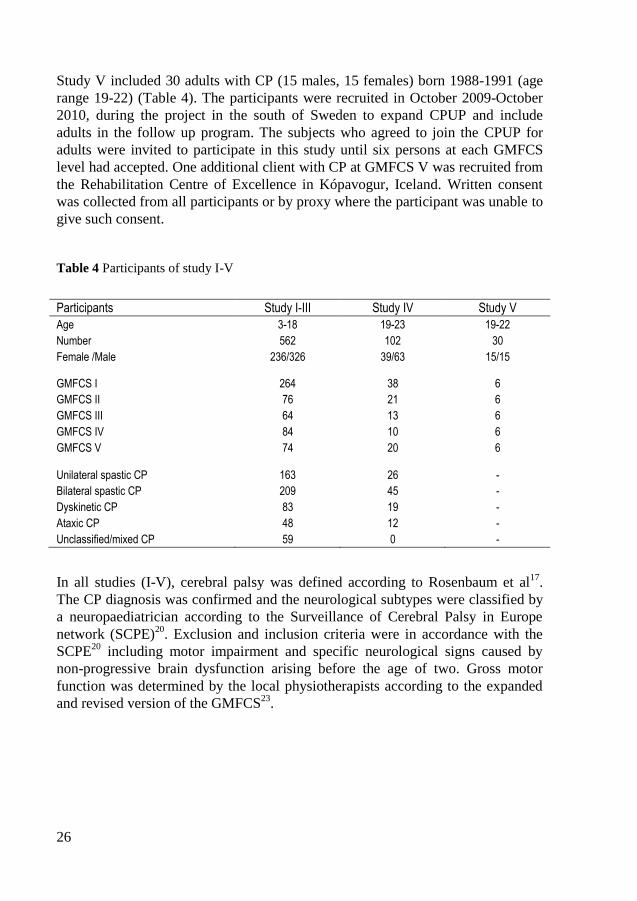
Study V included 30 adults with CP (15 males, 15 females) born 1988-1991 (age
range 19-22) (Table 4). The participants were recruited in October 2009-October
2010, during the project in the south of Sweden to expand CPUP and include
adults in the follow up program. The subjects who agreed to join the CPUP for
adults were invited to participate in this study until six persons at each GMFCS
level had accepted. One additional client with CP at GMFCS V was recruited from
the Rehabilitation Centre of Excellence in Kópavogur, Iceland. Written consent
was collected from all participants or by proxy where the participant was unable to
give such consent.
Table 4 Participants of study I-V
Participants Study I-III Study IV Study V
Age 3-18 19-23 19-22
Number 562 102 30
Female /Male 236/326 39/63 15/15
GMFCS I 264 38 6
GMFCS II 76 21 6
GMFCS III 64 13 6
GMFCS IV 84 10 6
GMFCS V 74 20 6
Unilateral spastic CP 163 26 -
Bilateral spastic CP 209 45 -
Dyskinetic CP 83 19 -
Ataxic CP 48 12 -
Unclassified/mixed CP 59 0 -
In all studies (I-V), cerebral palsy was defined according to Rosenbaum et al17
.
The CP diagnosis was confirmed and the neurological subtypes were classified by
a neuropaediatrician according to the Surveillance of Cerebral Palsy in Europe
network (SCPE)20
. Exclusion and inclusion criteria were in accordance with the
SCPE20
including motor impairment and specific neurological signs caused by
non-progressive brain dysfunction arising before the age of two. Gross motor
function was determined by the local physiotherapists according to the expanded
and revised version of the GMFCS23
.
Page 28
27
Data collection
For study I-III data was extracted from the CPUP register, based on the latest
physiotherapy report for all children with CP born 1990-2005 in the south of
Sweden during 2008. Sitting, standing, wheeled mobility, walking performance
according to the Functional Mobility Scale, the degree of independence and use of
assistive devices were reported by client or by proxy. Data was analyzed in
relation to GMFCS level, CP subtype and age. To analyze data the children were
divided into different age groups according to the Swedish school system: 3 to 6, 7
to 9, 10 to 12, 13 to 15, and 16 to 18 years.
In study I the questions were: A. What kind of chair does the child usually sit in?
The options were: The child uses (1) a standard chair, (2) adaptive seating or (3)
does not sit. Adaptive seating was defined as any special seating, high chair or
seating system provided as an assistive device to those who cannot sit in a
standard chair due to postural deficit or physical disability.
B. How does the child usually maintain a standing position; get into a standing
position from sitting on a chair; sit down on a chair from a standing position? The
options were: The child (1) does it independently without external support; (2)
does it with external support or (3) cannot. External support denotes support from
the environment (wall, furniture, assistive devices) or from another person.
To obtain information on the child’s wheelchair performance (study II), the
children and their caregivers answered the following questions: Does the child
usually use a: (A) Manual wheelchair for mobility indoors? (B) Powered
wheelchair for mobility indoors? (C) Manual wheelchair for mobility outdoors?
(D) Powered wheelchair for mobility outdoors? The options were: (1) No, the
child does not use a wheelchair; (2) Yes, the child self-propels/operates
independently; (3) Yes, the child is pushed by an adult.
The Functional Mobility Scale (FMS)125
was used for assessment of walking
performance, mobility (study III), and need for assistive devices at home (5 m), at
school (50 m), and in the community (500 m) (Table 3).
In study IV data was extracted from the most recent assessment in the CPUP
register for adults born 1988-1991 in the south of Sweden. Posture was assessed
by a physiotherapist using items from the Postural Ability Scale (PAS)116
. Any
deviations from midline in head, trunk, leg, foot position or asymmetries in arm
position or weight bearing gives 0 point each and symmetric, neutral position
gives 1 point each with a total score of 0-6 points where a maximum score of 6
points indicates no postural asymmetry. Passive joint range of motion (ROM) was
assessed by goniometric measurement and classified as limited if extension of
hips, knees or elbows were less than 0 degrees on one or both sides, or inability to
Page 29
28
reach 0 degrees of dorsiflexion of the feet. Scoliosis was defined as either having a
spinal curve at clinical examination by a physiotherapist or had a spinal fusion.
Hip dislocation was determined by an orthopaedic surgeon from radiographs and
defined as Reimers’s migration percentage of 100% in at least one hip1. Presence
of pain, use of assistive devices, ability to maintain and change position and
sleeping positions were reported by client or by proxy.
The psychometric evaluation of the Posture and Postural Ability Scale (study V)
was based on ratings from photos and videos of 30 adults with CP at GMFCS
level I-V. Photos of habitual posture of each individual were taken from a frontal
and sagittal view of the whole body in supine, prone, sitting and standing position.
Habitual refers to the posture customarily adopted by the individual when
instructed to sit, stand or lay down in prone or supine as straight as possible or, the
posture the body assumes when placed as straight as possible in any of these
positions and allowed to settle. The positions were supine lying on a plinth with
arms resting by side; prone lying on a plinth with the head to one side and arms
resting in an elevated position (flexion in elbows and abduction, external rotation
of shoulders); sitting on a plinth with feet on the floor; standing on the floor.
Those who were unable to maintain position independently were provided the
manual support needed to stay in position. Those who required total body support
in standing such as in GMFCS level V, were assessed in a standing brace or on a
tilt table. Videos recorded the participants’ postural ability while instructed to
assume and get out of the four positions. If unable to do this they were placed in
each position. Assessment of ability was then carried out sequentially
corresponding to the points on the Posture and Postural Ability Scale (Table 2) by
three experienced physiotherapists independently.
Statistical analysis
For all statistical analyses P-values less than 0.05 were considered significant. The
statistical analyses were performed using SPSS version17.0 (study I-III), SPSS
version 20.0 and Stata (study IV), and the R software environment (study V).
The chi-squared test for trend (the linear-by-linear association test) was used for
analyzing increasing or decreasing trends in ordinal data such as sitting, standing,
wheeled mobility and walking performance related to GMFCS level and age
(study I-III).
The Kruskal-Wallis test was used to analyze differences between nominal groups
such as CP subtypes (study I-III). Post hoc analyses were performed using the
Mann-Whitney U-test (study I-III). Z-test comparison of proportions with
Bonferroni adjusted p-values was used to analyze differences between participants
Page 30
29
and non-participants (study IV). Pearson’s Chi square and Fishers exact test were
used to analyze differences in ordinal and categorical data.
Spearman’s rank correlation coefficient was used to estimate correlation
coefficients among ordinal variables (study I-IV), and to analyze relationship
between asymmetric postures and categorical variables such as pain, joint range of
motion, hip dislocation and scoliosis (study IV).
Binary logistic regression analysis with adjustment for CP subtype was used to
estimate the relationship between independent walking and age (study III). Ordinal
logistic regression was used to estimate the relationship between asymmetric
posture and joint range of motion, hip dislocation, scoliosis and pain (study IV).
Interrater reliability (study V) was calculated using weighted kappa scores which
takes the degree of disagreement into account127
. The magnitude of weighted
kappa indicates the agreement beyond chance and was interpreted according to
Fleiss 1981128
, where ≤ 0.40 signifies poor agreement, 0.40-0.75 fair to good
agreement and ≥ 0.75 signifies excellent agreement.
Internal consistency (study V) was evaluated using Cronbach’s alpha if item is
deleted and Corrected Item-total correlation based on averaged values for three
raters. Cronbach’s alpha if item is deleted corresponds to the value achieved if a
specific item is removed121
. The Corrected Item-total correlation shows the
correlation between each item and the total score of the measurement and any item
with a value <0.2 should be discarded121
.
For analysis of reliability and consistency all GMFCS levels were combined and
95% nonparametric bootstrap confidence intervals were generated based on a 1000
re samples129; 130
.
Construct validity (study V) was evaluated for known-groups based on GMFCS
I-V with median/range. The Jonckheere-Terpstra test was used when analyzing
arithmetic average values given by the raters.
Ethical considerations
Ethical approval was obtained from the Medical Research Ethics Committee at
Lund University for study I-IV (LU-443-99) and V (2009/361).
Page 31
30
Results
Sitting and standing (study I)
The use of assistive devices and support to sit, stand and move between those
positions correlated to the GMFCS (Table 5), varied between the subtypes
(p<0.001), and was more frequent in pre-school children compared to school-
children (p<0.05).
Table 5 Correlations (p<0.001) between GMFCS levels and independence/use of support
to sit, stand, stand up (move from sit-to-stand) and sit down (move from stand-to-sit).
GMFCS Sit Stand Stand up Sit down
GMFCS 1.00 0.73 0.85 0.88 0.88
Sit 0.73 1.00 0.70 0.72 0.72
Stand 0.85 0.70 1.00 0.91 0.91
Stand up 0.88 0.72 0.91 1.00 0.99
Sit down 0.88 0.72 0.91 0.99 1.00
Of the 562 children 57% used standard chairs, 65% stood independently and 62%
moved between sitting and standing position without support. Adaptive seating
was used by 42%, 31% used support to stand and 18-19% to move between sitting
and standing position. Two children could not sit, 4% (21 children) could not stand
and 18% (102 children) could not move from sit-to-stand.
Adaptive seating was most frequent within the dyskinetic subtype and used by
89%. It was also used by 46% of those with bilateral spastic CP and by 40% of
those with ataxic CP. All children at GMFCS level V used adaptive seating, so did
95% at level IV, 54% at level III and 33% at level II.
Supported standing was used by 48% of the children with spastic bilateral or
dyskinetic CP. At GMFCS IV-V, 84% stood with support. The most frequent
standing device was a standing brace used by 130 children (3 of 4), in some cases
Page 32
31
in combination with a standing frame or a tilt table. Standing frames or tilt tables
were used by 57 children, and standing wheelchairs by 23 children.
Most children who stood independently, also moved into a standing position
without support (Table 5). Of the 172 children who stood with support, half
required support to move from sit-to-stand, and the other half could not move from
sit-to-stand even with support. At GMFCS levels III and IV almost two thirds
(64%) required support to move from sit-to-stand. All children with unilateral
spastic CP could get from sit-to-stand and only 4% required support. Of the
children with ataxic CP 19% used support, as did 29% of those with bilateral
spastic CP while 16% could not move from sit-to-stand. In the dyskinetic subtype
only 17% moved from sit-to-stand independently while 55% could not move from
sit-to-stand even with support.
Wheeled mobility (study II)
Wheelchairs for mobility were used by 165 of the 562 children (29%) indoors, and
by 228 children (41%) outdoors. The use of wheelchairs varied between the
subtypes, and increased with age and GMFCS level. Wheelchairs were most
frequent in children with dyskinetic CP where 69% were pushed in manual
wheelchairs outdoors and 13% operated powered wheelchairs.
Manual wheelchairs were used by 163 children indoors (30% self-propelled and
70% were pushed), and by 219 children outdoors (14% self-propelled and 86%
were pushed). Powered wheelchairs were used by 35 children indoors and by 56
children outdoors. Of those using powered wheelchairs 83% operated
independently indoors and 86% outdoors while the remaining 14-17% required
assistance.
Indoors, wheelchairs were used by 4% at GMFCS level II, 48% at level III and
84% at levels IV-V. Outdoors, 39% at GMFCS level II used a wheelchair, so did
85-90% at levels III-V. Most powered wheelchairs were operated by children at
GMFCS level IV and only one child at level V operated a powered wheelchair
outdoors. All the 25 children at levels III-V who did not use a wheelchair for
outdoor mobility were aged 3-6 years. No child under the age of 4 had
independent wheeled mobility outdoors. In total 5 children under the age of 7
years used powered wheelchairs.
Page 33
32
Walking performance (study III)
Walking performance was reported according to the Functional Mobility Scale
(FMS). Of the 562 children, 63% walked without aids at home, 60% at school,
and 57% in the community setting. Walking aids were used by 4-8% in different
environments. There was a high correlation (rs= -0.91) between the FMS and the
GMFCS at all distances. Most children at GMFCS levels I-II walked all distances
independently but with more difficulties on uneven surfaces and in longer
distances for those at GMFCS II. Walking aids were most frequently used by
children at level III, 33% at home and 52% at school. At GMFCS level IV 10-11%
used walking aids for shorter distances.
Almost all children with spastic unilateral CP walked all three distances without
aids. Walking aids were mostly used by children with ataxic or spastic bilateral CP
in the school environment. In children with ataxic CP 65-81% walked with or
without walking aids in different environments, the corresponding number was 52-
64% for children with bilateral spastic CP, and 16-24% of those with dyskinetic
CP.
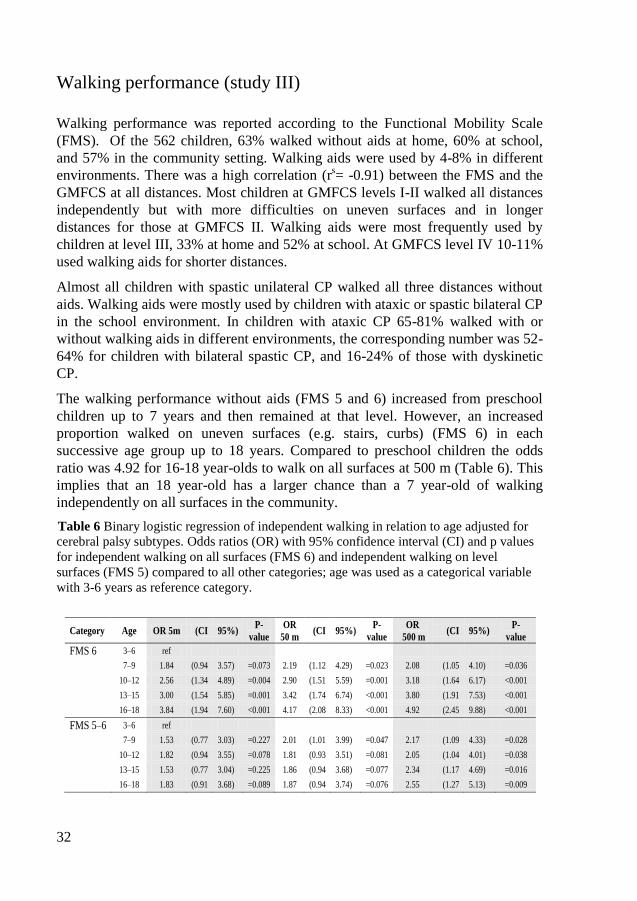
The walking performance without aids (FMS 5 and 6) increased from preschool
children up to 7 years and then remained at that level. However, an increased
proportion walked on uneven surfaces (e.g. stairs, curbs) (FMS 6) in each
successive age group up to 18 years. Compared to preschool children the odds
ratio was 4.92 for 16-18 year-olds to walk on all surfaces at 500 m (Table 6). This
implies that an 18 year-old has a larger chance than a 7 year-old of walking
independently on all surfaces in the community.
Table 6 Binary logistic regression of independent walking in relation to age adjusted for
cerebral palsy subtypes. Odds ratios (OR) with 95% confidence interval (CI) and p values
for independent walking on all surfaces (FMS 6) and independent walking on level
surfaces (FMS 5) compared to all other categories; age was used as a categorical variable
with 3-6 years as reference category.
Category Age OR 5m (CI 95%) P-
value
OR
50 m (CI 95%)
P-
value
OR
500 m (CI 95%)
P-
value
FMS 6 3–6 ref
7–9 1.84 (0.94 3.57) =0.073 2.19 (1.12 4.29) =0.023 2.08 (1.05 4.10) =0.036
10–12 2.56 (1.34 4.89) =0.004 2.90 (1.51 5.59) =0.001 3.18 (1.64 6.17) <0.001
13–15 3.00 (1.54 5.85) =0.001 3.42 (1.74 6.74) <0.001 3.80 (1.91 7.53) <0.001
16–18 3.84 (1.94 7.60) <0.001 4.17 (2.08 8.33) <0.001 4.92 (2.45 9.88) <0.001
FMS 5–6 3–6 ref
7–9 1.53 (0.77 3.03) =0.227 2.01 (1.01 3.99) =0.047 2.17 (1.09 4.33) =0.028
10–12 1.82 (0.94 3.55) =0.078 1.81 (0.93 3.51) =0.081 2.05 (1.04 4.01) =0.038
13–15 1.53 (0.77 3.04) =0.225 1.86 (0.94 3.68) =0.077 2.34 (1.17 4.69) =0.016
16–18 1.83 (0.91 3.68) =0.089 1.87 (0.94 3.74) =0.076 2.55 (1.27 5.13) =0.009
Page 34
33
Postural asymmetries (study IV)
Asymmetric posture, in terms of a low total score on the Postural Ability Scale
(PAS), was present at all GMFCS levels but more frequently at lower levels of
gross motor function. GMFCS correlated significantly (p<0.001) to PAS total
score for posture in supine (rs= -0.78), sitting (r
s= -0.72) and standing (r
s= -0.51).
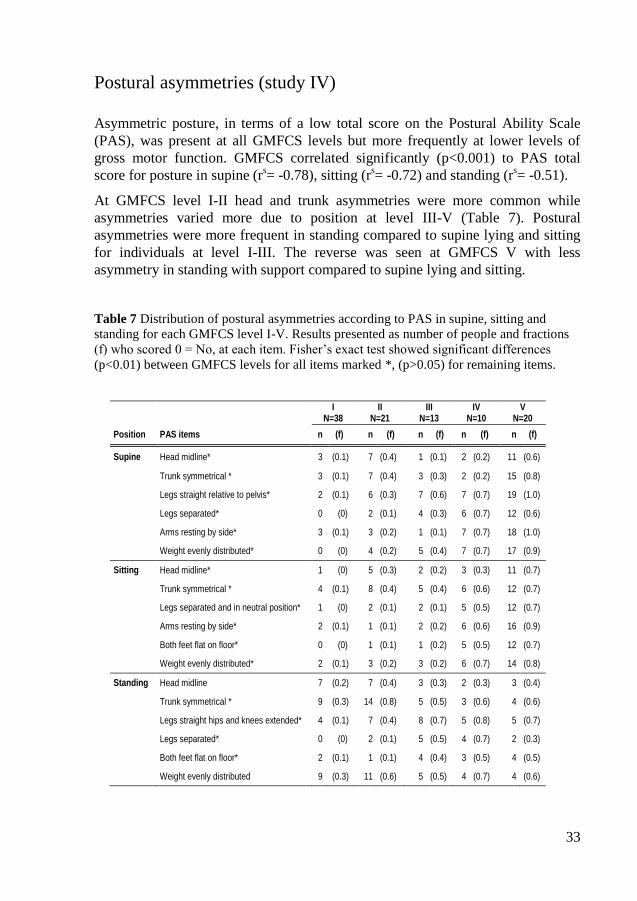
At GMFCS level I-II head and trunk asymmetries were more common while
asymmetries varied more due to position at level III-V (Table 7). Postural
asymmetries were more frequent in standing compared to supine lying and sitting
for individuals at level I-III. The reverse was seen at GMFCS V with less
asymmetry in standing with support compared to supine lying and sitting.
Table 7 Distribution of postural asymmetries according to PAS in supine, sitting and
standing for each GMFCS level I-V. Results presented as number of people and fractions
(f) who scored 0 = No, at each item. Fisher’s exact test showed significant differences
(p<0.01) between GMFCS levels for all items marked *, (p>0.05) for remaining items.
I
N=38 II
N=21 III
N=13 IV
N=10 V
N=20
Position PAS items n (f) n (f) n (f) n (f) n (f)
Supine Head midline* 3 (0.1) 7 (0.4) 1 (0.1) 2 (0.2) 11 (0.6)
Trunk symmetrical * 3 (0.1) 7 (0.4) 3 (0.3) 2 (0.2) 15 (0.8)
Legs straight relative to pelvis* 2 (0.1) 6 (0.3) 7 (0.6) 7 (0.7) 19 (1.0)
Legs separated* 0 (0) 2 (0.1) 4 (0.3) 6 (0.7) 12 (0.6)
Arms resting by side* 3 (0.1) 3 (0.2) 1 (0.1) 7 (0.7) 18 (1.0)
Weight evenly distributed* 0 (0) 4 (0.2) 5 (0.4) 7 (0.7) 17 (0.9)
Sitting Head midline* 1 (0) 5 (0.3) 2 (0.2) 3 (0.3) 11 (0.7)
Trunk symmetrical * 4 (0.1) 8 (0.4) 5 (0.4) 6 (0.6) 12 (0.7)
Legs separated and in neutral position* 1 (0) 2 (0.1) 2 (0.1) 5 (0.5) 12 (0.7)
Arms resting by side* 2 (0.1) 1 (0.1) 2 (0.2) 6 (0.6) 16 (0.9)
Both feet flat on floor* 0 (0) 1 (0.1) 1 (0.2) 5 (0.5) 12 (0.7)
Weight evenly distributed* 2 (0.1) 3 (0.2) 3 (0.2) 6 (0.7) 14 (0.8)
Standing Head midline 7 (0.2) 7 (0.4) 3 (0.3) 2 (0.3) 3 (0.4)
Trunk symmetrical * 9 (0.3) 14 (0.8) 5 (0.5) 3 (0.6) 4 (0.6)
Legs straight hips and knees extended* 4 (0.1) 7 (0.4) 8 (0.7) 5 (0.8) 5 (0.7)
Legs separated* 0 (0) 2 (0.1) 5 (0.5) 4 (0.7) 2 (0.3)
Both feet flat on floor* 2 (0.1) 1 (0.1) 4 (0.4) 3 (0.5) 4 (0.5)
Weight evenly distributed 9 (0.3) 11 (0.6) 5 (0.5) 4 (0.7) 4 (0.6)
Page 35
34
Some limitations of knee, foot and elbow extension were present at all GMFCS
levels while limited hip extension was found at GMFCS level II-V and dislocated
hips at GMFCS III-V (Table 8). Pain was reported by 63 of 102 individuals.
Table 8 Number of people and fractions (f) with hip dislocation, scoliosis, limited ROM,
and pain in relation to GMFCS level.
Asymmetric supine posture correlated (p<0.001) to limited knee extension
(rs=0.42), hip extension (r
s=0.52), hip dislocation (r
s=0.54), and scoliosis (r
s=0.45).
Asymmetric sitting posture correlated to hip dislocation and scoliosis (rs=0.46).
Asymmetric standing posture correlated to limited knee extension (rs=0.52).
Inability to put feet flat on floor in standing had a significant correlation to limited
knee extension (rs=0.40) but not to limited dorsiflexion of the feet. No correlation
was found between posture and pain.
The odds ratio for an asymmetric posture was 8 times higher in supine for those
with limited hip extension and 3 times higher for those with limited knee
extension. The odds ratio for an asymmetric posture was 2.5 times higher in
standing and 4 times higher in supine and sitting for those with scoliosis. It was 7
times higher in sitting and 19 times higher in supine for those with hip dislocation.
All adults at GMFCS levels I-III maintained lying position independently, while
10% of those at GMFCS IV and 60% at GMFCS V needed support to maintain
position. The correlation between GMFCS and ability to change position in lying
was rs=0.67 (p<0.001). Fifty percent of those at GMFCS level IV and V had only
one lying position, the other half used two or three positions. Only eight people, all
at GMFCS I-III, used all four positions; prone, supine, side lying left and right.
The ability to change position correlated to quality of posture in supine (rs= -0.60,
p<0.001). Seven out of nine adults with an asymmetric posture (0 points) could
I
N=38 II
N=21 III
N=13 IV
N=10 V
N=20 Total
N=102
n (f) n (f) n (f) n (f) n (f) n (f)
Hip dislocation 0 (0) 0 (0) 1 (0.1) 1 (0.1) 8 (0.4) 10 (0.1)
Scoliosis 12 (0.4) 7 (0.3) 6 (0.5) 6 (0.6) 17 (0.9) 48 (0.5)
Limited elbow extension 11 (0.3) 6 (0.3) 5 (0.4) 6 (0.6) 10 (0.6) 38 (0.4)
Limited hip extension 0 (0) 3 (0.2) 4 (0.3) 3 (0.3) 11 (0.6) 21 (0.2)
Limited knee extension 18 (0.5) 6 (0.3) 10 (0.8) 8 (0.8) 18 (0.9) 60 (0.6)
Limited foot dorsiflexion 7 (0.2) 8 (0.4) 3 (0.2) 3 (0.3) 4 (0.2) 25 (0.3)
Pain 23 (0.6) 13 (0.6) 7 (0.5) 8 (0.8) 12 (0.6) 63 (0.6)
Page 36
35
not change position and required total assistance; six of them had only one
sleeping position.
All individuals at GMFCS IV and V used postural support to maintain sitting. The
ability to change position from sit-to-stand and stand-to-sit showed a high
correlation to GMFCS levels (rs= 0.88, p<0.001). The ability to move from sit to
stand also correlated with sitting posture (rs= -0.71, p<0.001).
All adults at GMFCS level I-II and 38% at level III stood unsupported, while
supported standing was used by 46% at level III, 90 % at level IV and 74 % at
level V. The remaining 26% at GMFCS V did not stand at all. The correlation of
standing ability to GMFCS was (rs= -0.60, p<0.001). Of the 26 adults using
standing support; seven stood 1-2 hours/day and the remaining 19 stood less than
1 hour/day.
Evaluation of the Posture and Postural Ability Scale (study V)
The Posture and Postural Ability Scale (PPAS) showed excellent interrater
reliability for three independent raters with weighted Kappa values of 0.85-0.99.
There was a high internal consistency for all items. Cronbach’s alpha if item
deleted was 0.96-0.97 with a 95% confidence interval of 0.93-0.98 for all items.
Corrected item-total correlation varied between 0.60-0.91 with the lowest
correlation for sitting posture in the sagittal view.
Table 9 Construct validity of the PPAS. Median values and range for GMFCS I-V and
p-values of averaged values for the three raters.
GMFCS
I II III IV V P
Supine Postural ability 7 (7-7) 7 (7-7) 7 (6-7) 4 (3-7) 1.5 (1-4) <0.001
Posture frontal 6 (2-6) 4 (2-5) 1 (0-6) 0 (0-1) 0 (0-1) <0.001
Posture sagittal 6 (4-6) 4 (1-6) 2.5 (0-6) 0.5 (0-3) 1 (0-3) <0.001
Prone Postural ability 7 (7-7) 7 (7-7) 6 (5-7) 4 (1-6) 1 (1-3) <0.001
Posture frontal 5 (2-6) 4 (2-5) 2 (0-5) 1 (0-3) 0 (0-3) <0.001
Posture sagittal 6 (2-6) 5 (2-6) 3 (0-6) 1 (0-4) 0 (0-4) <0.001
Sitting Postural ability 7 (7-7) 7 (7-7) 7 (2-7) 2 (2-6) 2 (1-2) <0.001
Posture frontal 6 (4-6) 4 (1-6) 3 (0-6) 0 (0-2) 0 (0-4) <0.001
Posture sagittal 3.5 (2-6) 2 (0-5) 3.5 (0-6) 0 (0-4) 1 (0-5) 0.019
Standing Postural ability 7 (7-7) 7 (7-7) 4 (1-7) 1.5 (1-2) 1 (1-2) <0.001
Posture frontal 6 (3-6) 3 (0-5) 0 (0-3) 0 (0-2) 0 (0-2) <0.001
Posture sagittal 5 (4-6) 2 (0-6) 1 (0-4) 0 (0-3) 0 (0-3) <0.001
Page 37
36
The PPAS showed construct validity based on the ability of the assessment tool to
differ between known groups represented by the GMFCS levels I-V. Median
values and range in terms of min and max values are presented together with p-
values (p<0.02) calculated with Jonckheere-Terpstra for averaged values (Table
9). Distribution of scores at each level of gross motor function in all four positions
is provided for all three raters (Figure 4). The PPAS could not identify differences
in postural ability between individuals at levels I-II but was able to detect postural
asymmetries at all GMFCS levels.
Figure 4 Distribution of PPAS scores at GMFCS I-V in all four positions. All observations
are marked with different colours for each rater; red= rater A, blue= rater B, green=rater C.
The squared points connected with a line are means of each gross motor function level.
Page 38
37
Discussion
The overall ambition of this thesis was to enhance knowledge of posture, postural
ability and mobility in people with CP; their use of assistive devices and also to
evaluate a clinical tool for assessment of posture and postural ability.
The samples of study I-IV represent a total population of children or young adults
with CP in the south of Sweden. Therefore the results are likely to give a true
picture of the performance in children and adults of all CP subtypes and all
GMFCS levels. However all participants of study I-III were included in the CPUP
health care programme which may have reduced the number of children who were
unable to sit, stand, walk or move and may also have affected their use of assistive
devices compared to children in areas without prevention programme. The results
show what the children usually do, i.e. their performance, not what they can do,
i.e. their ability. In children with disabilities, ability usually exceeds
performance102
. The discrepancy between ability and performance may relate to
differences in environmental factors102
. The cross-sectional design of study I-IV
can describe differences between groups at a specific moment, not changes over
time.
Sitting and standing
The number of children with CP using adaptive seating decreased with age,
increased with GMFCS levels and was most frequent in dyskinetic CP. Unilateral
spastic CP and ataxic CP were associated with a better sitting and standing
performance than bilateral spastic CP or dyskinetic CP. There was a high
correlation for all outcome measures related to the expanded and revised version
of the GMFCS. The GMFCS is age-related and as most children remain at the
same GMFCS level this classification system seems useful for prediction of the
individual child’s future sitting and standing performance.
Several studies show a significant improvement of sitting posture and postural
control in children with CP using adaptive seating such as seat inserts, external
supports and modular seating systems65; 68; 74; 131
. Adaptive seating also allows
parents to sit facing their child instead of holding them from behind, and this
Page 39
38
facilitates feeding at mealtimes, play, communication and social interaction77
.
Pope et al.63
found improvements in both posture and mobility with the use of
adaptive seating over a three year period in children with CP aged 2.5-9 years who
were unable to sit independently. There is contradictory evidence regarding the
best position for sitting and the optimum inclination of seat surface132; 133
. Due to
the variability in people with CP, the particular task and environment, individual
assessment is required to provide appropriate support. Improvements in sitting
ability can also be achieved through training134; 135
. However it is vital to have
attainable, realistic goals depending on GMFCS level, bearing in mind that
postural ability and attention may be affected when performing dual tasks113; 114
.
The use of support to stand, and to move between sitting and standing position was
more frequent in preschool children than in schoolchildren and adolescents.
However it was not clarified whether this was due to natural development or to
environmental factors. Standing support such as tilt tables, standing frames and
standing braces can provide postural support to maintain upright position.
According to Pin et al.136
static weight bearing has been shown to increase bone
density in children with CP. A study by Kecskemethy et al.137
showed a wide
range of weight bearing loads in people with CP aged 6-21 years, with differences
of up to 29% of body weight between different standers. Gibson et al.138
showed a
significant lengthening of hamstrings in children with CP aged 6-9 years when
using a standing frame for 1 hour/day, 5 days per week.
In this study three of five children moved between sitting and standing position
independently, one of five used external support and one of five could not. Moving
between sitting and standing position requires more postural ability than
maintaining a static position, since the centre of gravity can move out of the base
of support while changing position120; 139
. People with CP have more difficulties in
recovering stability when exposed to balance threats117
. Musculoskeletal
constraints contribute to atypical postural patterns in standing such as a high
degree of antagonist co-activation83
. According to a review by dos Santos et al.140
there are several studies describing sit-to-stand movement in smaller samples of
children with spastic diplegic CP or hemiplegic CP, but our study is the first study
of a total population of children with CP including all subtypes and GMFCS
levels.
In Sweden, assistive devices such as adaptive seating, standing support,
wheelchairs and walking aids are provided free of charge by the Assistive
Technology Centres. This means that the results of these studies reflect the use of
assistive devices without regard to the economic situation of the families. The
opinions of the child and family, the rehabilitation team and the physical
surroundings influence the need for, or use of, assistive devices. Strategies to alter
the environment such as providing assistive devices in order to compensate for
functional impairments and enhance activity and participation have become more
Page 40
39
accepted in paediatric rehabilitation76; 115; 141; 142
. Assistive devices enhance
function in children with CP and reduce the demand on caregivers76; 141
. It is
therefore important that different types of assistive device are carefully considered
for children with CP.
Wheeled mobility
The use of manual wheelchairs increased with GMFCS level, but the use of
manual wheelchairs for self-mobility was more frequent in children at GMFCS III.
The 25 children at GMFCS levels III–V who did not use a wheelchair for outdoor
mobility were all aged 3–6 years and were probably seated in a buggy outdoors.
Powered wheelchairs were most frequent in children at GMFCS IV. Children at
GMFCS levels III–IV achieved a higher degree of independent mobility using
manual and powered wheelchairs. Only one child at GMFCS level V had
independent wheelchair mobility outdoors using a powered wheelchair. This
corresponds to the results seen in the study by Östensjö et al.76
, where the largest
increase in wheeled mobility was seen at GMFCS level IV. Palisano et al.97
analysed the mobility methods in Ontario, Canada. In 360 children at GMFCS
level III–V aged 4–12 years, 67% were pushed in manual wheelchairs outdoors,
7% self-propelled a manual wheelchair and 12% operated a powered wheelchair.
The corresponding numbers for the same age group in the present study were
almost equal: 62% were pushed, 6% self-propelled in manual wheelchairs and
15% operated powered wheelchairs.
Postural instability restricts functional performance and upper extremity function
in children with CP64; 68; 132; 143
. Lacoste et al.143
found that in children with CP who
self-propelled their wheelchairs, 41% had difficulties in driving due to postural
instability. Of children using manual wheelchairs, 89% became unstable when
propelling, as did 61% when operating their powered wheelchairs. Providing a
stable sitting posture is an important prerequisite for improvement in function and
wheeled mobility.
The use of wheelchairs was most frequent in children with dyskinetic CP. Arner et
al.144
also reported difficulties with manual activities in 80% of children with
dyskinetic CP, in 41% of those with ataxic CP and in 39% of those with bilateral
spastic CP. The reduced hand function in combination with postural instability
may contribute to the fact that no child with dyskinetic CP self-propelled a manual
wheelchair outdoors, while 77% of those having a powered wheelchair operated
independently. The results indicate that children with dyskinetic CP need a
powered wheelchair to achieve independent wheeled mobility. However, powered
Page 41
40
wheelchairs require more training and are not as easily transported in cars so
environmental factors must be considered.
Powered wheelchairs were only used by five children (4%) before the age of
seven, even though early self-produced mobility is crucial for the child’s cognitive
and psychosocial development98
. Wheelchairs are often used to symbolize
handicap or disability, so the stereotype of disability is easily reflected by them145
.
This may explain why some parents prefer buggies to wheelchairs hoping to avoid
drawing attention to the disability. However, children with motor impairments
may be at risk of developing learned helplessness if their development of
independence is not supported141
. Experience of self-produced mobility in healthy
infants as young as 8-9 months improves postural compensation to optic flow,
whether it is achieved through walkers, creeping or powered mobility146; 147
.
Powered mobility at an early age is not only a question of learning to drive but
rather a question of driving to learn148
.
Self-produced mobility can be obtained by powered wheelchairs at an early age149
,
but powered mobility still appears to be viewed as the last option for older
children when all other forms of mobility have failed97; 150
. This may be explained
by the traditional view of motor development as hierarchical where children were
expected to walk as much as possible to attain independent walking although it
may not have been the primary or goal of the child or the most functional method
for all environments104
. Fortunately this approach to modify the child rather than
the external factors has changed over the last decades104
. More attention is now
paid to alter the environment in order to facilitate efficient mobility and increase
participation in age-appropriate activities104
.
Bottos et al.149
showed that 21 of 27 children with severe motor disability aged 3–
8 years were able to operate a powered wheelchair with no or minimal adult
assistance. A majority of the parents were opposed to the idea of a power
wheelchair initially, but after provision almost all were positive. The driving skill
was related to the time spent in the powered wheelchair and not to IQ or motor
impairment149
. Butler151
reported improved self-initiated behaviours such as
interaction with objects, communication and changes in location in children aged
2-3 years provided with powered mobility. A randomized controlled study by
Jones et al.152
of 28 children with motor impairments aged 14-30 months, showed
significant improvements in functional mobility and receptive communication in
the children using powered wheelchairs compared to a control group. There was
also a reduction of caregiver assistance with mobility and self-care152
. In a study
by Tefft153
parents reported lower levels of stress, and increased satisfaction with
their child’s ability to move around and to interact, socialize and play with the
family when provided with a powered wheelchair. They also experienced a greater
acceptance by the general public to powered mobility for their children153
.
Powered mobility may also increase alertness and improve sleep/wake pattern148;
Page 42
41
153. Participation and social interaction opportunities in the school environment
improved with the use of assistive devices in children with CP145
.
Östensjö et al76
reported improvements in independent mobility in children with
the use of powered mobility, while manual wheelchairs mainly eased the care
load for parents. Our study supports these results since a majority of children using
powered wheelchairs operated independently while only one child out of seven
attained independent wheeled mobility in a manual wheelchair.
Walking performance
Walking performance in children with CP varies due to personal and
environmental factors. This study shows the most frequent mobility method at
different distances and environments in an unselected total population of children
with CP, 3-18 years. The Functional Mobility Scale (FMS) was used to describe
walking performance at home (5 m), at school (50 m), in the community (500 m),
and its relation to GMFCS level, CP subtype and age.
A limitation to this study is that the ratings of the FMS only provide the child’s
most frequent mobility method. Some children may use several methods such as
both walking with devices and using a wheelchair.
In an analysis from the SCPE database comprising 10,042 children with CP in
Europe, Beckung et al154
reported that in 5-year-old children, 54% had unaided
walking and 16% walked with aids. Rumeau-Rouquette et al155
, in a French study
reported that in children aged 8-14 years, 38- 44% had unaided walking and 13-
28% walked with aids. The number of children with unaided walking in the
present study is similar to Beckung et al. but higher than Rumeau-Rouquette et al.
In the previous studies it is not clear at what distance or in which environment the
walking ability was recorded. The proportion of children using walking aids was
smaller in our study. The use of walking aids was most common in children at
GMFCS level III and in children with ataxic or spastic bilateral CP in the school
environment.
The walking performance increased with GMFCS level. A relationship between
the FMS and the GMFCS would be expected but has, to our knowledge, not
previously been examined. We found a high correlation between the two
classifications, indicating that GMFCS is a good predictor of walking
performance. FMS is developed to measure functional mobility in children
corresponding to GMFCS levels I to IV but does not discriminate between assisted
and independent wheelchair mobility. To overcome this problem a further level,
between FMS 1 and N, could be considered.
Page 43
42
The number of children who walked without aids increased up to 7 years of age.
This is in agreement with the study by Bleck156
, who observed that walking ability
reached a plateau by the age of 7. It is also in agreement with longitudinal analysis
of motor growth curves showing peak motor performance at 6 to 7 years of age157-
159. The present study found, however, that the proportion of children walking
independently on uneven surfaces (FMS 6) was incrementally higher in each age
group up to 18 years. Hanna et al158
reported increased gross motor function (ie
capability) in adolescents at GMFCS I-II. Palisano et al.160
described improved
walking performance outdoors in adolescents at GMFCS II. Ability to walk on
uneven surfaces is important to achieve independent mobility and improve
accessibility in the community, where different surfaces, inclines, curbs, and stairs
are more common100
. This has clinical relevance because older children and
adolescents do more activities outside the home with friends than younger
children99
. Those at GMFCS I do more activities outside than those at levels II-
III99
. This result reflects their unrestricted walking performance.
Hanna et al.158
showed a decline in gross motor function in children at GMFCS
III-V from 8 years of age. Strauss et al.35
showed a decline in walking ability from
20 years and Jahnsen et al.24
reported a reduction in gross motor function in adults
at GMFCS II-III, mostly due to lack of balance, fear of falling, pain and
exhaustion. Several studies have shown increased energy consumption when
walking with assistive devices89-92
. Gibson et al.103
found that children with CP at
GMFCS III-IV consider walking as exercise rather than a functional ability, and
walking interventions were often associated with pain and fear103
. The children
were affected by normative ideas about walking as a moral good that must be
pursued frequently, contributing to negative self-identities in the children and
leading to angst and doubt in parents who feel they didn’t do enough if they let
their children use a wheelchair103
.
Raja et al.88
showed an increasing energy cost with each level of decreasing FMS
score when walking as well as a doubling in energy cost when walking outdoors
on uneven surfaces compared with even surfaces indoors88
. This may explain why
59% of the children at GMFCS level III walked 5 m at home, whereas only 16%
walked 500 m in the community. Franks et al.89
reported that mobility methods
affect school performance; the use of a wheelchair had a less negative impact on
visuomotor accuracy because the children were less tired than when walking with
assistive devices. Jahnsen et al.24
reported an increased experience of freedom,
speed of locomotion, and reduced energy cost in adults with CP at GMFCS III
when starting to use a wheelchair for mobility.
In the present study there was no decline in walking performance in adolescents.
As a result of the CPUP programme, the number of children who develop severe
contractures has been reduced55
. This improvement could result in a diminished or
delayed decrease in walking performance. In general, younger children with CP
Page 44
43
get a more intense treatment and follow up by their physiotherapists than
adolescents and adults. A continuous treatment and training programme in order to
increase oxygen uptake, improve balance and strength, maintain joint range of
motion and reduce pain throughout adolescence may improve walking
performance or prevent a reduction in walking ability in those with a higher level
of gross motor function. The CPUP health care programme continues to monitor
the adolescents with CP as they grow into adults.
Postural asymmetries
Although the brain lesion in CP is non-progressive, many secondarily acquired
clinical problems are progressive, and musculoskeletal abnormalities may develop
continuously during the lifespan27; 37; 48; 49
. Asymmetric postures increase the risk
of tissue adaptation leading to contractures and progressive deformities39-42
which
most commonly affect the spine and the lower extremities37; 38
. Study IV is, to our
knowledge, the first study of postural asymmetries in a total population of adults
with CP.
A limitation of this study is the restricted number of participants when analyzing
the results for each GMFCS level separately. Although the proportion of
participants may seem low (63% of the 162 invited), it is compensated by the total
population approach; non-participants were known and compared to participants,
which is a strength of the study. The study group is a representative part of the
total population in this part of Sweden, with the CP prevalence 2.3/1000 at 17-20
years of age. The distribution of subtypes in the present study almost equals that of
the previous studies. According to the prevalence and distribution of gender,
subtypes and GMFCS levels, the study population is probably representative for
other areas and countries with similar development6.
Postural asymmetries were present at all GMFCS levels, but more frequently at
lower levels of gross motor function and varied in different positions. Normally a
standing position require more postural ability, and those at GMFCS levels I-III
demonstrated more asymmetries in standing compared to sitting and supine lying.
However the reverse was seen at GMFCS level V with a higher proportion of
postural asymmetries in supine and sitting compared to supported standing. This
indicates a lack of postural support in lying and sitting, while supported standing
corrects at least some of the asymmetry. Postural asymmetries can lead to
asymmetric weight bearing which affects the base of support within the center of
gravity can move161
. A crouched posture reduce the ability to recover balance117
.
The time spent in different positions has a great impact on the development of
contractures and deformities. In this study no one who used standing support stood
Page 45
44
more than 1-2 hours/day. This implies that 22-24 out of the 24 hours/day were
spent in a more asymmetric position in sitting or lying for those at GMFCS level
V. In addition they are unable to change their position while lying or sitting. Of
those who were unable to change position in lying half had only one lying
position, indicating that they were not assisted in changing position. Porter42; 52
showed that preferred lying posture influence the direction of deformity with
windsweeping, hip dislocation and spinal curve in children with CP unable to
move out of their preferred posture. A study by Pountney56
on posture
management to prevent hip dislocation supports the importance of maintaining
symmetry without compromising function for those unable to change position.
This highlights the need for a proper assessment of posture, and provision of
postural support when needed, to prevent a sustained asymmetric posture.
Pain was reported by 63 of the 102 participants but no association between posture
and pain was found in this study. There was less reported pain compared to
previous studies by Jahnsen et al.31
(79%) and Andersson & Mattsson34
(82%). It
may be due to the older age of participants in their studies (mean age 34, 36 years
respectively). Limited range of motion was associated with postural asymmetries.
Andersson34
reported contractures in 80% of 221 adults with CP, where knee
contractures were most frequent. This corresponds to our findings where 60% of
all adults with CP had restricted passive knee extension in one or both knees. This
limitation was associated with postural asymmetries in both supine and standing
which requires extended legs. Supine posture was also affected by limited hip
extension, which was present in 22%. Previous studies39-42
indicate that a sustained
asymmetric posture predisposes to progressive deformities in people with CP. This
study has shown an association between posture and limited range of motion but
did not reveal if the contractures were caused by asymmetric posture or if the
limited range of motion caused the postural asymmetries. This illustrates the
importance of continuous monitoring of range of motion and posture in people
with CP.
Hip dislocations and scoliosis were associated with postural asymmetries in all
positions. The prevalence of hip dislocation (10 of 102) in this sample, not
included in the hip prevention programme, corresponds to reports from other
areas46; 162
. Hip dislocation, windswept-deformity and scoliosis are interrelated50
and can be reduced with a hip surveillance programme. Progression of scoliosis
increases with age even after skeletal maturity47-49
. Risk factors for progression are
early onset, large curve magnitude, thoracolumbar curve, total body involvement
and being confined to bed48; 49
. Since 1995 all children in the study area born in
1992 and later are included in a hip surveillance programme, which has reduced
the proportions of hip dislocations, windswept deformities and scoliosis45; 46; 50; 51;
55. The association between these deformities and postural asymmetries shows the
value of hip surveillance programmes. This study illustrates the importance of
Page 46
45
monitoring range of motion and posture not only from an early age in children, but
also ongoing in adults with CP, to allow early identification and preventive
treatment of contractures and postural asymmetries.
Evaluation of the Posture and Postural Ability Scale
The Posture and Postural Ability Scale (PPAS) showed an excellent interrater
reliability, a high internal consistency and construct validity in a standing, sitting,
prone and supine position for adults with CP. Even though an asymmetric posture
is known to cause progressive deformities in people with CP there has been a lack
of clinical assessment tools for posture and postural ability evaluated for adults
with CP. This is, to our knowledge, the first study evaluating an assessment tool
for posture and postural ability in a lying, sitting and standing position for adults.
A limitation of the study is that all three raters participated in the development of
the PPAS; they have long clinical experience and are specialized in posture
management. Further research is needed to examine interrater reliability for
trained practitioners not involved in the modification of the assessment tool. A
further limitation is that the ratings were based on photos and videos. This
removes some variability that arises in clinical practise. Photos provide only a one
point in time reflection of the posture. However, the condition of people with
severe disabilities may alter during the day due to fatigue, pain etc. It may also
change over time making a measurement on different occasions such as test-retest
and intrarater reliability more difficult to interpret. Therefore we chose to evaluate
agreement between different raters and used photos and videos to standardize the
occasion and minimize disagreement due to different performances and
circumstances.
Internal consistency represents the average of the correlations among all items.
The scale demonstrated a high internal consistency for all items where Cronbach’s
alpha if item deleted was 0.96-0.97, which exceeds the 0.8 recommended by
Streiner Norman. Corrected Item-total correlation showed a slightly lower value
for sitting posture in the sagittal view compared to the other items. This is
probably explained by the fact that the height of the plinth was not optimal in
some photos which affected the ratings of hips and knees mid-position. An
adjustable plinth is not always available in clinical practice. If the plinth is not
adjustable or if using a chair it would be desirable to provide additional support for
the feet when needed.
Construct validity was evaluated through the PPAS’s ability to differ between
known groups in terms of the GMFCS levels in CP. According to this
classification, individuals at level I and II can walk and stand unsupported. The
Page 47
46
highest level of the PPAS is to move into and out of position and therefore the
assessment tool was not expected to differ between GMFCS levels I and II in
postural ability. The basic level of postural ability is intact at GMFCS I-III, with
difficulties in fine-tuning muscle contractions to specific tasks and conditions72
.
The distribution of individuals at maximum and minimum score showed an
anticipated ceiling effect for postural ability in all four positions for adults at level
I-II, while the floor effect was higher for posture indicating a better quantity in
terms of ability than quality of posture. This indicates a need for assessing posture
and postural ability separately and as distinct from gross motor function, in order
to detect postural asymmetries and identify need for postural support. A strength
of the PPAS is that it identified postural asymmetries and deviations at all levels of
gross motor function in this study of adults with CP.
The PPAS was sufficiently sensitive to detect small postural asymmetries and
deviations even at GMFCS I and is likely to detect postural asymmetries at an
early stage. The assessment tool has no grading and cannot differ between a mild,
moderate or severe deviation. The rationale is that any deviation will increase by
forces imposed by gravity so it is clinically relevant to detect asymmetric posture
early in order to identify and apply the appropriate intervention to minimize
progressive deformities and contractures.
The PPAS does not require any special equipment and is easy to use in a clinical
setting. It provides important information of the need for postural support and
where it needs to be applied. Although the instrument has been used in clinical
practice for different client groups further research to evaluate its psychometric
properties for people with other diagnoses than cerebral palsy is desirable. All
assessment tools for posture and postural ability currently used in clinical practice
require additional training of the professionals intending to use them.
Page 48
47
Conclusions
About 60% of children with CP, aged 3–18, used standard chairs, stood and
moved between sitting and standing position without external support. Adding
those using adaptive seating and external support, 99% of the children could sit,
96% could stand and 81% could move between sitting and standing position.
Unilateral spastic CP and ataxic CP were associated with a better sitting and
standing performance than the other subtypes. Sitting and standing performance
and the ability to move between these positions were highly correlated to the
expanded and revised version of the GMFCS. The GMFCS is age-related and as
most children remain at the same GMFCS level this classification system seems
useful for prediction of the individual child’s future sitting and standing
performance.
A majority of the children using manual wheelchairs were pushed while powered
wheelchairs provided independent mobility in most cases. Most children with
dyskinetic CP needed a powered wheelchair to achieve independent wheeled
mobility. To achieve as high a level of independent mobility as possible, powered
wheelchairs should be considered at an early age for all children with impaired
walking ability.
We found a variation in walking performance related to CP subtype and a high
correlation between the FMS and the GMFCS. The walking performance without
aids increased from preschool children up to 7 years and then remained at that
level, but the proportion of children walking independently on uneven surfaces
was incrementally higher in each age group up to 18 years. The improved
performance on uneven surfaces is important for achieving independent walking
and improves accessibility in the community. Continuous follow up and treatment
to improve and maintain walking performance is important both in children and
adolescents at higher levels of gross motor function.
Postural asymmetries were found at all GMFCS levels in young adults with CP,
but more frequently at lower levels of gross motor function. Postural asymmetries
were associated with scoliosis, hip dislocation, hip and knee contractures, and
inability to change position. It is important to monitor range of motion, hips, spine
and posture from an early age, but also continuously in adults with CP, to allow
early identification and preventive treatment of contractures and postural
asymmetries.
Page 49
48
The Posture and Postural Ability Scale showed excellent interrater reliability for
experienced raters, high internal consistency and good construct validity. It
showed an anticipated ceiling effect for postural ability at GMFCS I-II while it
identified postural asymmetries at all GMFCS levels indicating a better quantity in
terms of ability than quality of posture in adults with CP. This indicates a need for
assessing posture and postural ability separately and as distinct from gross motor
function in order to detect postural asymmetries and identify need for postural
support. The PPAS was sensitive to detect postural asymmetries and deviations
even at GMFCS I and is likely to detect postural asymmetries at an early stage.
Further research
It is desirable to perform additional studies with longitudinal data based on the
CPUP quality register to enhance further knowledge of functional performance
and posture in a total population of children and adults with CP.
Further studies of postural stability in wheelchair seating are needed to evaluate,
its impact on wheeled mobility and postural asymmetries in people with CP.
Further research is planned to describe how long adults with CP remain in
different positions, their ability to maintain and change position and their use of
assistive devices.
Further research is needed to examine interrater reliability for trained professionals
not involved with the development of the Posture and Postural Ability Scale and
its application to other client groups. An evaluation of its responsiveness is also
desirable.
Page 50
49
Sammanfattning
Summary in Swedish
Cerebral pares (CP) är den vanligaste orsaken till motorisk funktionsnedsättning
hos barn och ungdomar med en prevalens på 2-3/1000. CP innebär en livslång
funktionsnedsättning och den förväntade överlevnaden är nästan densamma som
för befolkningen i stort. CP karaktäriseras av svårigheter med rörelser och postural
förmåga och symtomen varierar från knappt märkbara till kraftigt begränsande.
Förmåga att kunna stabilisera kroppen mot tyngdkraften är en grundförutsättning
för alla viljemässiga rörelser. En asymmetrisk kroppsställning ökar risken för
vävnadsanpassningar som leder till utveckling av kontrakturer och felställningar.
Vid CP är det framför allt rygg och nedre extremiteter som drabbas, vilket kan
leda till skolios, bäckenasymmetri, windswept deformitet, höftluxation, höft- och
knäkontrakturer samt fotdeformiteter. Dessa felställningar kan delvis förhindras
genom tidig upptäckt och preventiv behandling. Eftersom vävnadsanpassningen
ofta sker succesivt över längre tid kan den vara svår att upptäcka utan
standardiserad mätning. Det finns ett fåtal bedömningsinstrument för position och
postural förmåga i liggande, sittande och stående, men inget av dem har
utvärderats för vuxna med CP.
Det övergripande syftet med denna avhandling var att öka kunskaperna kring
position, postural förmåga, förflyttning och hjälpmedelsanvändning hos personer
med CP och att utvärdera ett kliniskt instrument för bedömning av position och
postural förmåga.
Studie I-III var tvärsnittstudier av 562 barn med CP i åldrarna 3-18 år. De
beskriver sitt-, stå-, uppresningsförmåga, hjälpmedelsanvändning (I),
rullstolsanvändning (II) och gångförmåga (III) utifrån grovmotorisk funktionsnivå,
neurologisk subtyp och ålder. Grovmotorisk funktion klassificerades enligt Gross
Motor Function Classification System (GMFCS). Det är en 5-gradig skala där
personer i nivå I går tämligen obehindrat medan personer i nivå V har svårt att
stabilisera kroppen mot tyngdkraften och inte har någon självständig förflyttning.
Studie IV var en tvärsnittsstudie, av unga vuxna med CP i åldrarna 19-23 år, som
beskriver posturala asymmetrier och förmåga att ändra position relaterat till
smärta, rörelseinskränkning, höftluxation och skolios. Studie V var en utvärdering
Page 51
50
av validitet och reliabilitet för bedömningsinstrumentet Posture and Postural
Ability Scale för vuxna med CP.
Omkring 60% av barnen med CP satt och stod utan stöd. Om man lägger till de
som använder hjälpmedel och externt stöd så klarade 99% att sitta, 96% att stå och
81% att resa sig och sätta sig. Det var högst andel barn med unilateral spastisk CP
och ataktisk CP som satt och stod utan stöd. Sitt och ståförmågan var starkt
korrelerad till GMFCS nivå. GMFCS är åldersrelaterad och eftersom de flesta barn
behåller sin GMFCS nivå förefaller denna klassificering användbar för att
prediktera sitt och ståförmåga hos barn med CP (studie I).
Rullstolar användes av 29% inomhus och 41% utomhus. Elrullstol möjliggjorde
självständig förflyttning i de flesta fall medan endast ett av sju barn körde sin
manuella rullstol själv. De flesta barn med dyskinetisk CP behövde elrullstol för
att kunna köra rullstolen själv. För att öka andelen barn med självständig
förflyttning bör elrullstol övervägas redan vid låg ålder för de barn som har nedsatt
gångförmåga (studie II).
Gångförmågan varierade mellan subtyper och korrelerade starkt med GMFCS
nivå. Det totala antalet barn som gick utan hjälpmedel ökade upp till 7 års ålder,
men andelen som gick själv på ojämna underlag var större i varje åldersgrupp ända
upp till 18 år. Att kunna gå på ojämna underlag är viktigt för en självständig gång i
samhället (studie III).
Posturala asymmetrier förekom vid alla GMFCS nivåer men var vanligare vid
lägre funktionsnivå. Asymmetrierna har ett samband med skolios, höftluxation,
höft- och knäkontrakturer samt oförmåga att ändra position. Det är viktigt att
kontinuerligt följa ledrörlighet, höfter, rygg och position från låg ålder men även
upp i vuxen ålder vid CP för att möjliggöra tidig upptäckt och preventiv
behandling av kontrakturer och posturala asymmetrier (studie IV).
Det kliniska bedömningsinstrumentet Posture and Postural Ability Scale visade
mycket hög interbedömarreliabilitet, goda interna mätegenskaper och
begreppsvaliditet. Det identifierade asymmetrier i liggande, sittande och stående
vid samtliga funktionsnivåer hos vuxna med CP och borde därför kunna
möjliggöra tidig upptäckt av posturala asymmetrier (studie V).
Page 52
51
Acknowledgements
I wish to express my sincere gratitude to all people who in one way or another
have supported me and made this thesis possible. I especially want to mention:
Gunnar Hägglund, my main supervisor, for giving me this opportunity and for
believing in me before anyone else did. I am truly grateful for your never failing
support and encouragement from the very start and ongoing during these years.
Your open-minded attitude, strive for new knowledge, enthusiasm and instant
feedback has been vital. You have an extraordinary ability to know exactly what
kind of support I need and how to provide it, in order to step by step increase my
knowledge and independence. It is a true pleasure to work with you.
Lena Westbom, my co-supervisor, for your optimism, support and for sharing your
knowledge of CP, and epidemiology in spite of a busy schedule.
Ann-Christin Johansson, my co-supervisor, for your support and encouragement,
interesting discussions, good advice, and for your patience when introducing me to
statistics.
Jerzy Leppert and Mats Enlund, former and present head of CKF, for your endless
efforts to provide me with the time and resources necessary for my research. I
truly appreciate your support and ability to see possibilities and create
opportunities. Without you, I would not have been able to complete this thesis.
Pauline Pope, my friend and colleague, for introducing me to posture
management. Your passion, wisdom, skills and valuable work for people with
severe neurological disabilities is a great inspiration. I am grateful for your
encouragement, patience and enthusiasm in developing the PPAS and for all your
help in proof-reading my manuscripts and thesis.
Gudny Jónsdóttir and Atli Ágústsson, my friends and co-workers, you
continuously encourage, challenge and inspire me with your skills, open-minded
attitude, enthusiasm and concern for people with severe disabilities.
Page 53
52
Tomasz Czuba, Jonas Ranstam, Rebecca Rylance and Philippe Wagner at RCSyd,
Jonas Björk RSKC, John Öhrvik KI, Kent Nilsson and Andreas Rosenblad CKF
for statistical advice.
All my colleagues and friends at the Centre for Clinical Research Västerås,
Uppsala University and at the Department of Orthopaedics, Lund University for
all your help, encouragement and support. Special thanks to my room-mates Lena
Burström and Magdalena Mattebo for sharing all the ups and downs in research.
All physiotherapists and occupational therapists in Skåne and Blekinge, who
contributed to this research with assessments and reports. With special thanks to
my colleagues Kerstin Arph-Hammargren, Sylvia Marcelius and Anette
Brantmark for all your work with the data collection for adults with CP.
Norbert Grentzelius, Thomas Ehmke and Rolf Hellström for sharing your
knowledge of customized seating and mechanics combined with humor and
concern for each client.
Susanne Hedberg and Henri Aromaa at the Hospital library, Västerås, for quick
and helpful services throughout the years.
My parents Håkan and Ulla-Britt for your unconditional love and never ending
support throughout my entire life. You have taught me that nothing is impossible;
it just takes a strong will, endurance, courage and creativity. Without your
extensive support I would not have been able to complete this thesis. My sister
Christina for being my best friend, supportive and boosting me with energy.
My family Pierre, Eric and Anna for being my greatest joy, and reminding me of
what is most important in life. You have not even once complained about the time
I’ve put into my research, and always encouraged me to continue. I especially
want to thank Anna for always helping me out whenever I’m struggling with
documents, illustrations or any computer problems.
The studies in this thesis were supported by grants from:
The Faculty of Medicine, Lund University,the Centre for Clinical Research
Västerås Uppsala University, Stiftelsen för bistånd åt rörelsehindrade i Skåne,
the Swedish Association of Local Authorities and Regions (SKL), the National
Association for Disabled Children and Youth (RBU), the Linnea and Josef
Carlsson Foundation, the Norrbacka-Eugenia Foundation, Promobilia, Region
Skåne, Landstinget Västmanland.
Page 54
53
References
1 Reimers J. (1980) The stability of the hip in children. A radiological study of the
results of muscle surgery in cerebral palsy. Acta Orthop Scand Suppl 184: 1-100.
2 Hagberg B, Hagberg G, Beckung E, Uvebrant P. (2001) Changing panorama of
cerebral palsy in Sweden. VIII. Prevalence and origin in the birth year period 1991-
94. Acta Paediatr 90: 271-7.
3 Nordmark E, Hägglund G, Lagergren J. (2001) Cerebral palsy in southern Sweden
I. Prevalence and clinical features. Acta Paediatr 90: 1271-6.
4 (2002) Prevalence and characteristics of children with cerebral palsy in Europe. Dev
Med Child Neurol 44: 633-40.
5 Himmelmann K, Hagberg G, Beckung E, Hagberg B, Uvebrant P. (2005) The
changing panorama of cerebral palsy in Sweden. IX. Prevalence and origin in the
birth-year period 1995-1998. Acta Paediatr 94: 287-94.
6 Westbom L, Hägglund G, Nordmark E. (2007) Cerebral palsy in a total population
of 4-11 year olds in southern Sweden. Prevalence and distribution according to
different CP classification systems. BMC Pediatr 7: 41.
7 Yeargin-Allsopp M, Van Naarden Braun K, Doernberg NS, Benedict RE, Kirby
RS, Durkin MS. (2008) Prevalence of cerebral palsy in 8-year-old children in three
areas of the United States in 2002: a multisite collaboration. Pediatrics 121: 547-54.
8 Kirby RS, Wingate MS, Van Naarden Braun K, Doernberg NS, Arneson CL,
Benedict RE, Mulvihill B, Durkin MS, Fitzgerald RT, Maenner MJ, Patz JA,
Yeargin-Allsopp M. (2011) Prevalence and functioning of children with cerebral
palsy in four areas of the United States in 2006: a report from the Autism and
Developmental Disabilities Monitoring Network. Res Dev Disabil 32: 462-9.
9 Westbom L, Bergstrand L, Wagner P, Nordmark E. (2011) Survival at 19 years of
age in a total population of children and young people with cerebral palsy. Dev Med
Child Neurol 53: 808-14.
10 Beckung E, Hagberg G. (2002) Neuroimpairments, activity limitations, and
participation restrictions in children with cerebral palsy. Dev Med Child Neurol 44:
309-16.
11 Himmelmann K, Beckung E, Hagberg G, Uvebrant P. (2006) Gross and fine motor
function and accompanying impairments in cerebral palsy. Dev Med Child Neurol
48: 417-23.
12 Little WJ. (1966) On the influence of abnormal parturition, difficult labours,
premature birth, and asphyxia neonatorum, on the mental and physical condition of
the child, especially in relation to deformities. Clin Orthop Relat Res 46: 7-22.
13 Morris C. (2007) Definition and classification of cerebral palsy: a historical
perspective. Dev Med Child Neurol Suppl 109: 3-7.
Page 55
54
14 Mac Keith RC, Mackenzie ICK, Polani PE. (1959) The Little Club Memorandum
on Terminology and Classification of "Cerebral Palsy". Cerebral Palsy Bullentin 5:
27-35.
15 Bax MC. (1964) Terminology and Classification of Cerebral Palsy. Dev Med Child
Neurol 6: 295-7.
16 Mutch L, Alberman E, Hagberg B, Kodama K, Perat MV. (1992) Cerebral palsy
epidemiology: where are we now and where are we going? Dev Med Child Neurol
34: 547-51.
17 Rosenbaum P, Paneth N, Leviton A, Goldstein M, Bax M, Damiano D, Dan B,
Jacobsson B. (2007) A report: the definition and classification of cerebral palsy
April 2006. Dev Med Child Neurol Suppl 49: 8-14.
18 Rumeau-Rouquette C. (1995) Facteurs de risque des déficiences motrices d'origine
cérébrale chez l'enfant à terme. Journal de Pédiatrie et de Puériculture 7: 394-7.
19 Hagberg B, Hagberg G, Olow I. (1975) The changing panorama of cerebral palsy in
Sweden 1954-1970. I. Analysis of the general changes. Acta Paediatr Scand 64:
187-92.
20 (2000) Surveillance of cerebral palsy in Europe: a collaboration of cerebral palsy
surveys and registers. Surveillance of Cerebral Palsy in Europe (SCPE). Dev Med
Child Neurol 42: 816-24.
21 Sellier E, Horber V, Krageloh-Mann I, J DLC, Cans C. (2012) Interrater reliability
study of cerebral palsy diagnosis, neurological subtype, and gross motor function.
Dev Med Child Neurol 54: 815-21.
22 Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. (1997)
Development and reliability of a system to classify gross motor function in children
with cerebral palsy. Dev Med Child Neurol 39: 214-23.
23 Palisano RJ, Rosenbaum P, Bartlett D, Livingston MH. (2008) Content validity of
the expanded and revised Gross Motor Function Classification System. Dev Med
Child Neurol 50: 744-50.
24 Jahnsen R, Aamodt G, Rosenbaum P. (2006) Gross Motor Function Classification
System used in adults with cerebral palsy: agreement of self-reported versus
professional rating. Dev Med Child Neurol 48: 734-8.
25 Sandström K, Alinder J, Oberg B. (2004) Descriptions of functioning and health
and relations to a gross motor classification in adults with cerebral palsy. Disabil
Rehabil 26: 1023-31.
26 McCormick A, Brien M, Plourde J, Wood E, Rosenbaum P, McLean J. (2007)
Stability of the Gross Motor Function Classification System in adults with cerebral
palsy. Dev Med Child Neurol 49: 265-9.
27 Kerr Graham H, Selber P. (2003) Musculoskeletal aspects of cerebral palsy. J Bone
Joint Surg Br 85: 157-66.
28 Nordmark E, Hägglund G, Lauge-Pedersen H, Wagner P, Westbom L. (2009)
Development of lower limb range of motion from early childhood to adolescence in
cerebral palsy: a population-based study. BMC Med 7: 65.
29 Widhe T. (2001) Spine: posture, mobility and pain. A longitudinal study from
childhood to adolescence. Eur Spine J 10: 118-23.
Page 56
55
30 Opheim A, Jahnsen R, Olsson E, Stanghelle JK. (2009) Walking function, pain, and
fatigue in adults with cerebral palsy: a 7-year follow-up study. Dev Med Child
Neurol 51: 381-8.
31 Jahnsen R, Villien L, Aamodt G, Stanghelle JK, Holm I. (2004) Musculoskeletal
pain in adults with cerebral palsy compared with the general population. J Rehabil
Med 36: 78-84.
32 Jahnsen R, Villien L, Egeland T, Stanghelle JK, Holm I. (2004) Locomotion skills
in adults with cerebral palsy. Clin Rehabil 18: 309-16.
33 Jahnsen R, Villien L, Stanghelle JK, Holm I. (2003) Fatigue in adults with cerebral
palsy in Norway compared with the general population. Dev Med Child Neurol 45:
296-303.
34 Andersson C, Mattsson E. (2001) Adults with cerebral palsy: a survey describing
problems, needs, and resources, with special emphasis on locomotion. Dev Med
Child Neurol 43: 76-82.
35 Strauss D, Ojdana K, Shavelle R, Rosenbloom L. (2004) Decline in function and
life expectancy of older persons with cerebral palsy. NeuroRehabilitation 19: 69-78.
36 Hicks JL, Schwartz MH, Arnold AS, Delp SL. (2008) Crouched postures reduce the
capacity of muscles to extend the hip and knee during the single-limb stance phase
of gait. J Biomech 41: 960-7.
37 Morrell DS, Pearson JM, Sauser DD. (2002) Progressive bone and joint
abnormalities of the spine and lower extremities in cerebral palsy. Radiographics
22: 257-68.
38 Renshaw TS, Green NE, Griffin PP, Root L. (1995) Cerebral Palsy: Ortopaedic
Management. J Bone Joint Surg Am 77: 1590-606
39 Fulford FE, Brown JK. (1976) Position as a cause of deformity in children with
cerebral palsy. Dev Med Child Neurol 18: 305-14.
40 Brown K. (1985) Positional deformity in children with cerebral palsy.
Physiotherapy Theory and Practice 1: 37-41.
41 Scrutton D. (1991) The causes of developmental deformity and their implication for
seating. Prosthet Orthot Int 15: 199-202.
42 Porter D, Michael S, Kirkwood C. (2008) Is there a relationship between preferred
posture and positioning in early life and the direction of subsequent asymmetrical
postural deformity in non ambulant people with cerebral palsy? Child Care Health
Dev 34: 635-41.
43 Tardieu C, Lespargot A, Tabary C, Bret MD. (1988) For how long must the soleus
muscle be stretched each day to prevent contracture? Dev Med Child Neurol 30: 3-
10.
44 Hägglund G, Lauge-Pedersen H, Wagner P. (2007) Characteristics of children with
hip displacement in cerebral palsy. BMC Musculoskelet Disord 8: 101.
45 Hägglund G, Andersson S, Duppe H, Lauge-Pedersen H, Nordmark E, Westbom L.
(2005) Prevention of dislocation of the hip in children with cerebral palsy. The first
ten years of a population-based prevention programme. J Bone Joint Surg Br 87:
95-101.
Page 57
56
46 Elkamil AI, Andersen GL, Hägglund G, Lamvik T, Skranes J, Vik T. (2011)
Prevalence of hip dislocation among children with cerebral palsy in regions with
and without a surveillance programme: a cross sectional study in Sweden and
Norway. BMC Musculoskelet Disord 12: 284.
47 Gu Y, Shelton JE, Ketchum JM, Cifu DX, Palmer D, Sparkman A, Jermer-Gu MK,
Mendigorin M. (2011) Natural history of scoliosis in nonambulatory spastic
tetraplegic cerebral palsy. PM R 3: 27-32.
48 Saito N, Ebara S, Ohotsuka K, Kumeta H, Takaoka K. (1998) Natural history of
scoliosis in spastic cerebral palsy. Lancet 351: 1687-92.
49 Thometz JG, Simon SR. (1988) Progression of scoliosis after skeletal maturity in
institutionalized adults who have cerebral palsy. J Bone Joint Surg Am 70: 1290-6.
50 Persson-Bunke M, Hägglund G, Lauge-Pedersen H. (2006) Windswept hip
deformity in children with cerebral palsy. J Pediatr Orthop B 15: 335-8.
51 Persson-Bunke M, Hägglund G, Lauge-Pedersen H, Wagner P, Westbom L. (2012)
Scoliosis in a total population of children with cerebral palsy. Spine (Phila Pa
1976) 37: E708-13.
52 Porter D, Michael S, Kirkwood C. (2007) Patterns of postural deformity in non-
ambulant people with cerebral palsy: what is the relationship between the direction
of scoliosis, direction of pelvic obliquity, direction of windswept hip deformity and
side of hip dislocation? Clin Rehabil 21: 1087-96.
53 Stewart CP. (1991) Physiological considerations in seating. Prosthet Orthot Int 15:
193-8.
54 Loeters MJ, Maathuis CG, Hadders-Algra M. Risk factors for emergence and
progression of scoliosis in children with severe cerebral palsy: a systematic review.
Dev Med Child Neurol 52: 605-11.
55 Hägglund G, Andersson S, Duppe H, Lauge-Pedersen H, Nordmark E, Westbom L.
(2005) Prevention of severe contractures might replace multilevel surgery in
cerebral palsy: results of a population-based health care programme and new
techniques to reduce spasticity. J Pediatr Orthop B 14: 269-73.
56 Pountney T, Mandy A, Green E, Gard P. (2002) Management of hip dislocation
with postural management. Child Care Health Dev 28: 179-85.
57 Kohler R. (2010) Nicolas Andry de Bois-Regard (Lyon 1658-Paris 1742): the
inventor of the word "orthopaedics" and the father of parasitology. J Child Orthop
4: 349-55.
58 Ottosson A. (2007) Varför ortopeden blev sjukgymnast och varför vi inte kommer
ihåg det. Svensk ortopedi och sjukgymnastik under 1800-talet. Fysioterapi: 38-44.
59 http://www.ssd.scb.se/databaser/makro/start.asp?lang=2. Statistics Sweden,
Statistical database, Population.
60 Green EM, Mulcahy CM, Pountney TE. (1995) An investigation into the
development of early postural control. Dev Med Child Neurol 37: 437-48.
61 Green EM, Nelham RL. (1991) Development of sitting ability, assessment of
children with a motor handicap and prescription of appropriate seating systems.
Prosthet Orthot Int 15: 203-16.
62 Rose J, Wolff DR, Jones VK, Bloch DA, Oehlert JW, Gamble JG. (2002) Postural
balance in children with cerebral palsy. Dev Med Child Neurol 44: 58-63.
Page 58
57
63 Pope PM, Bowes CE, Booth E. (1994) Postural control in sitting the SAM system:
evaluation of use over three years. Dev Med Child Neurol 36: 241-52.
64 Carlberg EB, Hadders-Algra M. (2005) Postural dysfunction in children with
cerebral palsy: some implications for therapeutic guidance. Neural Plast 12: 221-8;
discussion 63-72.
65 Harris SR, Roxborough L. (2005) Efficacy and Effectiveness of Physical Therapy
in Enhancing Postural Control in Children With Cerebral Palsy. Neural Plasticity
12: 229-43.
66 Brogren E, Hadders-Algra M, Forssberg H. (1998) Postural control in sitting
children with cerebral palsy. Neurosci Biobehav Rev 22: 591-6.
67 Liao SF, Yang TF, Hsu TC, Chan RC, Wei TS. (2003) Differences in seated
postural control in children with spastic cerebral palsy and children who are
typically developing. Am J Phys Med Rehabil 82: 622-6.
68 Myhr U, von Wendt L. (1991) Improvement of functional sitting position for
children with cerebral palsy. Dev Med Child Neurol 33: 246-56.
69 Myhr U, von Wendt L, Norrlin S, Radell U. (1995) Five-year follow-up of
functional sitting position in children with cerebral palsy. Dev Med Child Neurol
37: 587-96.
70 Nashner LM, Shumway-Cook A, Marin O. (1983) Stance posture control in select
groups of children with cerebral palsy: deficits in sensory organization and
muscular coordination. Exp Brain Res 49: 393-409.
71 Naslund A, Sundelin G, Hirschfeld H. (2007) Reach performance and postural
adjustments during standing in children with severe spastic diplegia using dynamic
ankle-foot orthoses. J Rehabil Med 39: 715-23.
72 van der Heide JC, Hadders-Algra M. (2005) Postural Muscle Dyscoordination in
Children With Cerebral Palsy. Neural Plasticity 12: 197-203.
73 Gramsbergen A. (2005) Postural Control in Man: The Phylogenetic Perspective.
Neural Plasticity 12: 77-88.
74 Hulme JB, Gallacher K, Walsh J, Niesen S, Waldron D. (1987) Behavioral and
postural changes observed with use of adaptive seating by clients with multiple
handicaps. Phys Ther 67: 1060-7.
75 Redstone F, West JF. (2004) The importance of postural control for feeding.
Pediatr Nurs 30: 97-100.
76 Ostensjo S, Carlberg EB, Vollestad NK. (2005) The use and impact of assistive
devices and other environmental modifications on everyday activities and care in
young children with cerebral palsy. Disabil Rehabil 27: 849-61.
77 Rigby PJ, Ryan SE, Campbell KA. (2009) Effect of adaptive seating devices on the
activity performance of children with cerebral palsy. Arch Phys Med Rehabil 90:
1389-95.
78 Hulme JB, Shaver J, Acher S, Mullette L, Eggert C. (1987) Effects of adaptive
seating devices on the eating and drinking of children with multiple handicaps. Am
J Occup Ther 41: 81-9.
79 Larnert G, Ekberg O. (1995) Positioning improves the oral and pharyngeal
swallowing function in children with cerebral palsy. Acta Paediatr 84: 689-92.
Page 59
58
80 Nwaobi OM. (1986) Effects of body orientation in space on tonic muscle activity of
patients with cerebral palsy. Dev Med Child Neurol 28: 41-4.
81 Stavness C. (2006) The effect of positioning for children with cerebral palsy on
upper-extremity function: a review of the evidence. Phys Occup Ther Pediatr 26:
39-53.
82 Nwaobi OM. (1987) Seating orientations and upper extremity function in children
with cerebral palsy. Phys Ther 67: 1209-12.
83 Woollacott MH, Burtner P, Jensen J, Jasiewicz J, Roncesvalles N, Sveistrup H.
(1998) Development of postural responses during standing in healthy children and
children with spastic diplegia. Neurosci Biobehav Rev 22: 583-9.
84 Liao HF, Jeng SF, Lai JS, Cheng CK, Hu MH. (1997) The relation between
standing balance and walking function in children with spastic diplegic cerebral
palsy. Dev Med Child Neurol 39: 106-12.
85 Furukawa A, Nii E, Iwatsuki H, Nishiyama M, Uchida A. (1998) Factors of
Influence on the Walking Ability of Children with Spastic Cerebral Palsy. Journal
of Physical Therapy Science 10 1-5.
86 Gage JR, Deluca PA, Renshaw TS. (1995) Gait Analysis: Principles and
Applications J Bone Joint Surg Am 77: 1607-23.
87 Johnston TE, Moore SE, Quinn LT, Smith BT. (2004) Energy cost of walking in
children with cerebral palsy: relation to the Gross Motor Function Classification
System. Dev Med Child Neurol 46: 34-8.
88 Raja K, Joseph B, Benjamin S, Minocha V, Rana B. (2007) Physiological cost
index in cerebral palsy: its role in evaluating the efficiency of ambulation. J Pediatr
Orthop 27: 130-6.
89 Franks CA, Palisano RJ, Darbee JC. (1991) The effect of walking with an assistive
device and using a wheelchair on school performance in students with
myelomeningocele. Phys Ther 71: 570-7; discussion 7-9.
90 Mattsson E, Andersson C. (1997) Oxygen cost, walking speed, and perceived
exertion in children with cerebral palsy when walking with anterior and posterior
walkers. Dev Med Child Neurol 39: 671-6.
91 Rose J, Medeiros JM, Parker R. (1985) Energy cost index as an estimate of energy
expenditure of cerebral-palsied children during assisted ambulation. Dev Med Child
Neurol 27: 485-90.
92 Waters RL, Mulroy S. (1999) The energy expenditure of normal and pathologic
gait. Gait Posture 9: 207-31.
93 Wren TA, Rethlefsen S, Kay RM. (2005) Prevalence of specific gait abnormalities
in children with cerebral palsy: influence of cerebral palsy subtype, age, and
previous surgery. J Pediatr Orthop 25: 79-83.
94 Miller F. (2005) Cerebral palsy. New York: Springer Publications
95 Bottos M, Feliciangeli A, Sciuto L, Gericke C, Vianello A. (2001) Functional status
of adults with cerebral palsy and implications for treatment of children. Dev Med
Child Neurol 43: 516-28.
96 Fernandes T. (2006) Independent mobility for children with disabilities.
International Journal of Therapy and Rehabilitation 13: 329-33.
Page 60
59
97 Palisano RJ, Tieman BL, Walter SD, Bartlett DJ, Rosenbaum PL, Russell D, Hanna
SE. (2003) Effect of environmental setting on mobility methods of children with
cerebral palsy. Dev Med Child Neurol 45: 113-20.
98 Tefft D, Guerette P, Furumasu J. (1999) Cognitive predictors of young children's
readiness for powered mobility. Dev Med Child Neurol 41: 665-70.
99 Palisano RJ, Kang LJ, Chiarello LA, Orlin M, Oeffinger D, Maggs J. (2009) Social
and community participation of children and youth with cerebral palsy is associated
with age and gross motor function classification. Phys Ther 89: 1304-14.
100 Palisano RJ, Shimmell LJ, Stewart D, Lawless JJ, Rosenbaum PL, Russell DJ.
(2009) Mobility experiences of adolescents with cerebral palsy. Phys Occup Ther
Pediatr 29: 135-55.
101 Holsbeeke L, Ketelaar M, Schoemaker MM, Gorter JW. (2009) Capacity,
capability, and performance: different constructs or three of a kind? Arch Phys Med
Rehabil 90: 849-55.
102 Young NL, Williams JI, Yoshida KK, Bombardier C, Wright JG. (1996) The
context of measuring disability: does it matter whether capability or performance is
measured? J Clin Epidemiol 49: 1097-101.
103 Gibson BE, Teachman G, Wright V, Fehlings D, Young NL, McKeever P. (2011)
Children's and parents' beliefs regarding the value of walking: rehabilitation
implications for children with cerebral palsy. Child: Care, Health and Development
38: 61-9.
104 Wiart L, Darrah J. (2002) Changing philosophical perspectives on the management
of children with physical disabilities-their effect on the use of powered mobility.
Disabil Rehabil 24: 492-8.
105 Salminen AL, Brandt A, Samuelsson K, Toytari O, Malmivaara A. (2009) Mobility
devices to promote activity and participation: a systematic review. J Rehabil Med
41: 697-706.
106 Østensjø S, Carlberg EB, Vøllestad NK. (2005) The use and impact of assistive
devices and other environmental modifications on everyday activities and care in
young children with cerebral palsy. Disability and Rehabilitation 27: 849-61.
107 Asbjornslett M, Hemmingsson H. (2008) Participation at school as experienced by
teenagers with physical disabilities. Scand J Occup Ther 15: 153-61.
108 Keshner EA. (1981) Reevaluating the theoretical model underlying the
neurodevelopmental theory. A literature review. Phys Ther 61: 1035-40.
109 Shumway-Cook A, Woollacott MH. (2011) Motor control : translating research
into clinical practice. Philadelphia, Pa. ;: Lippincott Williams & Wilkins.
110 Woollacott MH, Shumway-Cook A. (1990) Changes in posture control across the
life span-a systems approach. Phys Ther 70: 799-807.
111 Bernstein NA. (1967) The co-ordination and regulation of movements. Oxford:
Pergamon Press.
112 Bouisset S, Do MC. (2008) Posture, dynamic stability, and voluntary movement.
Neurophysiol Clin 38: 345-62.
113 Reilly DS, Woollacott MH, van Donkelaar P, Saavedra S. (2008) The interaction
between executive attention and postural control in dual-task conditions: children
with cerebral palsy. Arch Phys Med Rehabil 89: 834-42.
Page 61
60
114 Woollacott M, Shumway-Cook A. (2002) Attention and the control of posture and
gait: a review of an emerging area of research. Gait Posture 16: 1-14.
115 Darrah J, Bartlett D. (1995) Dynamic systems theory and management of
children with cerebral palsy: Unresolved issues. Infants and young children 8:
52-5.
116 Pope PM. (2007) Severe and complex neurological disability : management of the
physical condition. Edinburgh: Butterworth-Heinemann/Elsevier.
117 Woollacott MH, Shumway-Cook A. (2005) Postural Dysfunction During Standing
and Walking in Children With Cerebral Palsy: What are the Underlying Problems
and What New Therapies Might Improve Balance?. Neural Plasticity 12: 211-
9.
118 Brogren E, Hadders-Algra M, Forssberg H. (1996) Postural control in children with
spastic diplegia: muscle activity during perturbations in sitting. Dev Med Child
Neurol 38: 379-88.
119 Massion J. (1998) Postural control systems in developmental perspective. Neurosci
Biobehav Rev 22: 465-72.
120 Frank JS, Earl M. (1990) Coordination of posture and movement. Phys Ther 70:
855-63.
121 Streiner DL, Norman GR. (2008) Health measurement scales : a practical guide to
their development and use. Oxford: Oxford University Press.
122 Hallett R, Hare N, Milner A. (1987) Description and evaluation of an assessment
form Physiotherapy 73: 220-5.
123 Pountney TE, Mulcahy C, Green E. (1990) Early Development of Postural Control.
Physiotherapy 76: 799-802.
124 Pountney TE, Cheek L, Green E, Mulcahy C, Nelham R. (1999) Content and
Criterion Validation of the Chailey Levels of Ability. Physiotherapy 85: 410-6.
125 Graham HK, Harvey A, Rodda J, Nattrass GR, Pirpiris M. (2004) The Functional
Mobility Scale (FMS). J Pediatr Orthop 24: 514-20.
126 Harvey A, Baker R, Morris ME, Hough J, Hughes M, Graham HK. (2010) Does
parent report measure performance? A study of the construct validity of the
Functional Mobility Scale. Dev Med Child Neurol 52: 181-5.
127 Conger AJ. (1980) Integration and generalization of kappas for multiple raters.
Psychological Bulletin 88: 322-8.
128 Fleiss J, L. editor. (1981) Statistical Methods for Rates and Proportions.
129 DiCiccio TJ, Efron B. (1996) Bootstrap Confidence Intervals. Statistical Science
11: 189-212.
130 Davison ACaH, D.V. editor. (1997) Bootstrap Methods and Their Application,
Chapter 5. . Cambridge University Press.
131 Chung J, Evans J, Lee C, Lee J, Rabbani Y, Roxborough L, Harris SR. (2008)
Effectiveness of adaptive seating on sitting posture and postural control in children
with cerebral palsy. Pediatr Phys Ther 20: 303-17.
132 McClenaghan BA, Thombs L, Milner M. (1992) Effects of seat-surface inclination
on postural stability and function of the upper extremities of children with cerebral
palsy. Dev Med Child Neurol 34: 40-8.
Page 62
61
133 Michael SM, Porter D, Pountney TE. (2007) Tilted seat position for non-ambulant
individuals with neurological and neuromuscular impairment: a systematic review.
Clin Rehabil 21: 1063-74.
134 Harbourne RT, Willett S, Kyvelidou A, Deffeyes J, Stergiou N. (2010) A
comparison of interventions for children with cerebral palsy to improve sitting
postural control: a clinical trial. Phys Ther 90: 1881-98.
135 Wade W, Porter D. (2012) Sitting playfully: does the use of a centre of gravity
computer game controller influence the sitting ability of young people with cerebral
palsy? Disabil Rehabil Assist Technol 7: 122-9.
136 Pin TW-mM. (2007) Effectiveness of Static Weight-Bearing Exercises in Children
with Cerebral Palsy. Pediatric Physical Therapy Spring 19: 62-73.
137 Kecskemethy HH, Herman D, May R, Paul K, Bachrach SJ, Henderson RC. (2008)
Quantifying weight bearing while in passive standers and a comparison of standers.
Dev Med Child Neurol 50: 520-3.
138 Gibson SKa, Sprod JAb, Maher CAc. (2009) The use of standing frames for
contracture management for nonmobile children with cerebral palsy. International
Journal of Rehabilitation Research 32: 316-23.
139 Buchanan JJ, Horak FB. (2001) Transitions in a postural task: do the recruitment
and suppression of degrees of freedom stabilize posture? Exp Brain Res 139: 482-
94.
140 dos Santos AN, Pavao SL, Rocha NA. (2011) Sit-to-stand movement in children
with cerebral palsy: a critical review. Res Dev Disabil 32: 2243-52.
141 Henderson S, Skelton H, Rosenbaum P. (2008) Assistive devices for children with
functional impairments: impact on child and caregiver function. Dev Med Child
Neurol 50: 89-98.
142 Fauconnier J, Dickinson HO, Beckung E, Marcelli M, McManus V, Michelsen SI,
Parkes J, Parkinson KN, Thyen U, Arnaud C, Colver A. (2009) Participation in life
situations of 8-12 year old children with cerebral palsy: cross sectional European
study. BMJ 338: b1458.
143 Lacoste M, Therrien M, Prince F. (2009) Stability of children with cerebral palsy in
their wheelchair seating: perceptions of parents and therapists. Disabil Rehabil
Assist Technol 4: 143-50.
144 Arner M, Eliasson AC, Nicklasson S, Sommerstein K, Hagglund G. (2008) Hand
function in cerebral palsy. Report of 367 children in a population-based longitudinal
health care program. J Hand Surg Am 33: 1337-47.
145 Huang IC, Sugden D, Beveridge S. (2009) Children's perceptions of their use of
assistive devices in home and school settings. Disabil Rehabil Assist Technol 4: 95-
105.
146 Higgins CI, Campos JJ, Kermoian R. (1996) Effect of Self-Produced Locomotion
on Infant Postural Compensation to Optic Flow. Developmental Psychology
September 32: 836-41.
147 Uchiyama I, Anderson DI, Campos JJ, Witherington D, Frankel CB, Lejeune L,
Barbu-Roth M. (2008) Locomotor experience affects self and emotion. Dev Psychol
44: 1225-31.
Page 63
62
148 Nilsson LM, Nyberg PJ. (2003) Driving to Learn: A New Concept for Training
Children With Profound Cognitive Disabilities in a Powered Wheelchair. American
Journal of Occupational Therapy March/April 57: 229-33.
149 Bottos M, Bolcati C, Sciuto L, Ruggeri C, Feliciangeli A. (2001) Powered
wheelchairs and independence in young children with tetraplegia. Dev Med Child
Neurol 43: 769-77.
150 Wiart L. (2011) Exploring mobility options for children with physical disabilities: a
focus on powered mobility. Phys Occup Ther Pediatr 31: 16-8.
151 Butler C. (1986) Effects of powered mobility on self-initiated behaviors of very
young children with locomotor disability. Dev Med Child Neurol 28: 325-32.
152 Jones MAPTP, McEwen IRPTDPTPF, Neas BRP. (2012) Effects of Power
Wheelchairs on the Development and Function of Young Children With Severe
Motor Impairments. Pediatric Physical Therapy Summer 24: 131-40.
153 Tefft D, Guerette P, Furumasu J. (2011) The Impact of Early Powered Mobility on
Parental Stress, Negative Emotions, and Family Social Interactions. Physical &
Occupational Therapy in Pediatrics 31: 4-15.
154 Beckung E, Hagberg G, Uldall P, Cans C. (2008) Probability of walking in children
with cerebral palsy in Europe. Pediatrics 121: e187-92.
155 Rumeau-Rouquette C, du Mazaubrun C, Mlika A, Dequae L. (1992) Motor
disability in children in three birth cohorts. Int J Epidemiol 21: 359-66.
156 Bleck EE. (1975) Locomotor prognosis in cerebral palsy. Dev Med Child Neurol
17: 18-25.
157 Beckung E, Carlsson G, Carlsdotter S, Uvebrant P. (2007) The natural history of
gross motor development in children with cerebral palsy aged 1 to 15 years. Dev
Med Child Neurol 49: 751-6.
158 Hanna SE, Rosenbaum PL, Bartlett DJ, Palisano RJ, Walter SD, Avery L, Russell
DJ. (2009) Stability and decline in gross motor function among children and youth
with cerebral palsy aged 2 to 21 years. Dev Med Child Neurol 51: 295-302.
159 Rosenbaum PL, Walter SD, Hanna SE, Palisano RJ, Russell DJ, Raina P, Wood E,
Bartlett DJ, Galuppi BE. (2002) Prognosis for gross motor function in cerebral
palsy: creation of motor development curves. JAMA 288: 1357-63.
160 Palisano RJ, Hanna SE, Rosenbaum PL, Tieman B. (2010) Probability of walking,
wheeled mobility, and assisted mobility in children and adolescents with cerebral
palsy. Dev Med Child Neurol 52: 66-71.
161 Aruin AS. (2006) The effect of asymmetry of posture on anticipatory postural
adjustments. Neurosci Lett 401: 150-3.
162 Cooke PH, Cole WG, Carey RP. (1989) Dislocation of the hip in cerebral palsy.
Natural history and predictability. J Bone Joint Surg Br 71: 441-6.