1 PowerPoint Slides English Spanish Translation Cancer-related Fatigue and Sleep Disorders Video Transcript Fatiga y trastornos del sueño relacionados con el cáncer Transcripción del video Professional Oncology Education Cancer-related Fatigue and Sleep Disorders Time: 29:49 Educación Oncológica Profesional Fatiga y trastornos del sueño relacionados con el cáncer Duración: 29:49 Ellen F. Manzullo, M.D. Professor, General Internal Medicine, Ambulatory Treatment and Emergency Care The University of Texas MD Anderson Cancer Center Dra. Ellen F. Manzullo, Profesora, Medicina Interna General, Tratamiento Ambulatorio y Atención de Emergencia MD Anderson Cancer Center de la Universidad de Texas I’m Dr. Ellen Manzullo and I’m a professor of Medicine here at the University of Texas MD Anderson Cancer Center and I am going to be talking with you regarding cancer-related fatigue and sleep disorders Soy la Dra. Ellen Manzullo, profesora de Medicina en el MD Anderson Cancer Center de la Universidad de Texas, y hablaré sobre la fatiga y los trastornos del sueño relacionados con el cáncer.
Transcript
1
PowerPoint Slides English Spanish Translation
Cancer-related Fatigue and Sleep Disorders Video Transcript
Fatiga y trastornos del sueño relacionados con el cáncer Transcripción del video
Professional Oncology Education Cancer-related Fatigue and Sleep Disorders Time: 29:49
Educación Oncológica Profesional Fatiga y trastornos del sueño relacionados con el cáncer Duración: 29:49
Ellen F. Manzullo, M.D. Professor, General Internal Medicine, Ambulatory Treatment and Emergency Care The University of Texas MD Anderson Cancer Center
Dra. Ellen F. Manzullo, Profesora, Medicina Interna General, Tratamiento Ambulatorio y Atención de Emergencia MD Anderson Cancer Center de la Universidad de Texas
I’m Dr. Ellen Manzullo and I’m a professor of Medicine here at the University of Texas MD Anderson Cancer Center and I am going to be talking with you regarding cancer-related fatigue and sleep disorders
Soy la Dra. Ellen Manzullo, profesora de Medicina en el MD Anderson Cancer Center de la Universidad de Texas, y hablaré sobre la fatiga y los trastornos del sueño relacionados con el cáncer.
2
And a nice place to begin is with the accepted definition of cancer-related fatigue.
Comencemos con la definición de fatiga relacionada con el cáncer.
The definition of cancer-related fatigue is that it’s a distressing, persistent, subjective sense of tiredness or exhaustion related to cancer or cancer treatment that is not proportional to recent activity and it interferes with usual functioning.
Es una sensación de angustia, persistente y subjetiva, de cansancio o agotamiento relacionado con el cáncer o su tratamiento, que no es proporcional a la actividad reciente y que interfiere en el funcionamiento habitual.
3
Now it’s important to keep in mind several characteristics of cancer-related fatigue. Cancer-related fatigue is really a multidimensional symptom and it can encompass not only physical aspects, but also mental, and emotional aspects. And in addition it can really occur anywhere along the spectrum of cancer care. And up to 30% of cancer survivors have been reported to have a loss of energy years after they have completed their treatment.
Es importante tener en cuenta varias características de la fatiga relacionada con el cáncer, que es un síntoma multidimensional y puede abarcar no sólo aspectos físicos, sino también emocionales y mentales. Además, puede aparecer en cualquier momento del tratamiento oncológico. Hasta 30% de los sobrevivientes de cáncer experimentan pérdida de energía aun años después de haber completado su tratamiento.
Now there’s really several barriers to both the assessment and treatment of this symptom, which is really the most common and most distressing symptom in our patient population. The first is that there are naturally time constraints in a busy outpatient practice. Physicians are very busy as well as nurse practitioners in the outpatient setting and that is not really at times conducive regarding asking the patient about this symptom. In addition, many times patients are reluctant to mention fatigue. They don’t want to be perceived as a complainer and also there’s concern that if they mention that they’re having fatigue that this potentially could have an impact on their cancer treatment. Also, another important barrier is that many times physicians feel uncomfortable discussing this symptom simply due to a lack of knowledge in this area. And then finally some patients just think that this is an expected outcome of their cancer and cancer treatment and they just don't mention this during their clinic visit. So, these are all several really important barriers to both the assessment and treatment of cancer-related fatigue.
Existen varios obstáculos para la evaluación y el tratamiento de este síntoma, que en realidad es el más común y angustiante en nuestra población de pacientes. El primero es que hay limitaciones de tiempo en una atareada práctica ambulatoria. En un entorno ambulatorio, los médicos y las enfermeras están muy ocupados y por momentos no es el ambiente más propicio para preguntar al paciente sobre el síntoma. Además, muchas veces los pacientes son reacios a hablar de la fatiga, pues no quieren ser percibidos como quejosos y existe la inquietud de que si mencionan la fatiga, podría tener un impacto en el tratamiento oncológico. Otro obstáculo importante es que muchas veces los médicos se sienten incómodos hablando de este síntoma que desconocen. Por último, algunos pacientes creen que es un resultado esperado del cáncer y su tratamiento, y no lo mencionan durante su visita a la clínica. Todos estos son obstáculos importantes para evaluar y tratar la fatiga relacionada con el cáncer.
4
When we look at the causes of cancer-related fatigue, there are really many important factors. And it’s important to keep in mind that cancer-related fatigue also correlates with decreased daytime activity and also increased nocturnal wakefulness. Some of the important causes of cancer-related fatigue are: the cancer treatment that the patient is undergoing as well as comorbid conditions that the patient has, such as hypothyroidism; and what I will be discussing later, sleep disorders. Also --- we also want to keep in mind patient’s medications can also contribute to the fatigue they’re experiencing. And then some also important causes are poor nutrition as well as symptoms that normally cluster, or can potentially cluster with fatigue, such as pain, anxiety, depression. And so I will be going over all of these potential causes of cancer-related fatigue to begin with.
Al analizar las causas de la fatiga relacionada con el cáncer surgen factores importantes. Debemos tener en cuenta que esta fatiga también se relaciona con la disminución de la actividad diurna y el aumento de la vigilia nocturna. Algunas causas importantes de la fatiga relacionada con el cáncer son: el tratamiento contra el cáncer que el paciente sobrelleva y las condiciones comórbidas que padece, tales como hipotiroidismo; y los trastornos del sueño, de los que hablaré más adelante. También debemos tener en cuenta los medicamentos que toma, que también pueden contribuir a su fatiga. Otras causas importantes son una mala nutrición y los síntomas que normalmente se asocian o pueden asociarse a la fatiga, como dolor, ansiedad y depresión. Ahora hablaremos de todas estas causas de la fatiga relacionada con el cáncer.
Nutritional im --- imbalances is an important one and the patients can experience weight changes as they undergo their cancer treatment. And it’s important to keep in mind that it could be that they gain weight as well as lose weight. Patients commonly think that since they have a cancer diagnosis and they’re undergoing treatment for their cancer, that they will lose weight. But we have found, in certain patient populations, this is not the case at all. And, in fact, patients can also have a significant weight gain and this can also have an impact on their symptom of fatigue. Also, we keep in mind that patients can have motility disorders, particularly in our diabetic patients. And also patients as they are actively undergoing their cancer treatment, they can experience significant nausea, vomiting, diarrhea, all of this which has a negative impact on their nutrition. And then as a result they can also develop fluid and electrolyte imbalances and, for example, have decreases in their potassium and magnesium. So in addition to these nutritional imbalances, another important factor is: patients can experience physical function changes. Many times, as they’re undergoing their chemotherapy or radiotherapy, they will have decreased physical activity and they will subsequently have decreased physical
El desequilibrio nutricional es importante y los pacientes pueden experimentar cambios de peso al comenzar el tratamiento contra el cáncer. Es importante tener en cuenta que pueden subir o bajar de peso. En general, los pacientes creen que, como tienen un diagnóstico de cáncer y reciben tratamiento contra esa enfermedad, van a perder peso, pero hemos determinado que en ciertas poblaciones de pacientes no es el caso. En realidad, los pacientes pueden aumentar considerablemente de peso, lo que también puede afectar sus síntomas de fatiga. Los pacientes pueden tener trastornos de motilidad, en particular los pacientes diabéticos. Quienes reciben un tratamiento contra el cáncer pueden experimentar náuseas, vómitos y diarrea, que tienen un impacto negativo en su nutrición. Como resultado, también pueden desarrollar desequilibrios líquidos y electrolíticos, y tener disminuciones en sus niveles de potasio y magnesio. Además de estos desequilibrios nutricionales, otro factor importante es que los pacientes experimentan cambios en la función física. Muchas veces, mientras reciben quimioterapia o radioterapia, experimentan una disminución de la actividad física y luego de su condición física. Por ello, cuando atendemos pacientes con fatiga relacionada con el cáncer, uno de los primeros temas es el ejercicio y les damos las recomendaciones
5
conditioning. This is why, in many times when we see patients in our cancer-related fatigue, one of the first interventions that we talk to patients about is exercise, telling them the recommendations for all of us is to try to get 30 minutes of exercise on a daily basis, provided that they don’t have any specific limitations as a result of their cancer or their cancer treatment.
universalmente válidas de hacer 30 minutos de ejercicio diariamente si no tienen limitaciones específicas como consecuencia del cáncer o su tratamiento.
Cancer treatments also interfere – or are related to cancer-related fatigue and I have listed here simply all the potential cancer treatments that a patient can be undergoing, such as chemotherapy, radiation therapy, surgery, bone marrow transplantation, biologic response modifiers, as well as hormonal treatments.
Los tratamientos oncológicos también están asociados con la fatiga relacionada con el cáncer. Los tratamientos que puede recibir un paciente son quimioterapia, radioterapia, cirugía, trasplante de médula ósea, modificadores de la respuesta biológica y tratamientos hormonales.
Medications are also a very important factor to keep in mind when evaluating a patient with cancer-related fatigue. And a couple of examples would be, for example, beta-blockers the patients might be on, for the control of hypertension or for some underlying cardiac disease. In addition, patients can be on sedating agents that could contribute to their fatigue. It’s important to keep in mind that there are normally symptoms that cluster with fatigue. And some of the most common symptoms that cluster with fatigue are, for example, pain, anxiety, depression, and what we will be focusing on later on, sleep disorders. And that’s why we always evaluate our patients when we initially see them in our cancer-related fatigue clinic for these symptoms by having them complete questionnaires.
Los medicamentos también son un factor muy importante al evaluar a un paciente con fatiga relacionada con el cáncer. Un ejemplo son los betabloqueantes que los pacientes pueden tomar para controlar la hipertensión o alguna enfermedad cardíaca subyacente. Además, los pacientes pueden tomar sedantes que podrían contribuir a su fatiga. Es importante tener en cuenta que normalmente son síntomas que se asocian con la fatiga. Algunos de los síntomas más comúnmente asociados con ella son dolor, ansiedad, depresión y los trastornos del sueño, de los que nos ocuparemos más adelante. Por eso, en nuestra clínica para pacientes con fatiga relacionada con el cáncer, al examinarlos inicialmente, evaluamos si tienen estos síntomas haciéndolos contestar cuestionarios.
6
Comorbid conditions are also a very important factor to keep in mind when patients are being rel --- evaluated for cancer-related fatigue. For example, anemia: patients when they have a hemoglobin lab --- level usually of 10 or less, they will begin to experience some level of fatigue; also patients with neurologic disorders as well as cardiac dysfunction. It’s important when we evaluate a patient for fatigue to also make certain that they don’t have, for example, an underlying cardiac disorder that could be contributing or could be actually the cause of their fatigue. We also evaluate patients for pulmonary disorders, hepatic disorders, renal dysfunction, rheumatologic disorders. In particular patients with fibromyalgia can experience fatigue, and this is very important to keep in mind. And then of course infectious processes, especially if a patient, for example, is having fever and or requiring --- and is requiring antibiotic therapy this also can impact their fatigue. Finally, endocrine disorders are also very important to keep in mind when evaluating patients for fatigue and, in particular, hypothyroidism, as well as hypogonadism, and adrenal insufficiency. These are three common dis --- endocrine disorders that can have a potential impact on the patient’s fatigue.
Las condiciones médicas comórbidas también son un factor importante al evaluar a un paciente con fatiga relacionada con el cáncer. Por ejemplo, la anemia. Los pacientes con un nivel de hemoglobina de 10 o menos comenzarán a sentir cierta fatiga. También aquellos con trastornos neurológicos o disfunción cardíaca. Al evaluar a un paciente por fatiga, es importante asegurarnos de que no tenga, por ejemplo, un trastorno cardiaco subyacente que pueda contribuir o ser realmente la causa de la fatiga. También evaluamos a los pacientes por trastornos pulmonares y hepáticos, disfunción renal y trastornos reumatológicos. Los pacientes con fibromialgia pueden experimentar fatiga y es muy importante tenerlo en cuenta. Los procesos infecciosos también pueden provocar fatiga, especialmente si un paciente tiene fiebre y requiere un tratamiento con antibióticos. Por último, al evaluar la fatiga también son importantes los trastornos endócrinos, en particular el hipotiroidismo, así como el hipogonadismo y la insuficiencia suprarrenal. Son tres trastornos endócrinos comunes que pueden incidir en la fatiga del paciente.
As far as interventions that are useful for patients with their cancer-related fatigue, a nice way of thinking about it, is that there are non-pharmacologic interventions as well as pharmacologic interventions. Non-pharmacologic interventions would be, for example, psychosocial interventions. As I mentioned previously, exercise is something which is very important and patients many times will sa --- will question how can we ask them to exercise when they are so fatigued? But actually there have been some studies that have been performed in certain patient populations, which have suggested that exercise, with the eventual goal of getting to 30 minutes of exercise a day, can have a very positive impact on the patients’ level of fatigue and decrease the level of their fatigue. Sleep therapy is another very important non-pharmacologic intervention, and this particular relates to sleep hygiene. Patients need to be counseled on the importance of trying to go to bed at the same time every day of the week, getting up at
En cuanto a las intervenciones útiles para los pacientes con fatiga relacionada con el cáncer, podemos clasificarlas como intervenciones farmacológicas y no farmacológicas. Las intervenciones no farmacológicas serían las intervenciones psicosociales. Como ya he mencionado, el ejercicio es muy importante y los pacientes suelen preguntarse cómo podemos pedirles que hagan ejercicio cuando están tan fatigados. Se han realizado estudios en determinadas poblaciones de pacientes que sugieren que un objetivo de 30 minutos de ejercicio diario puede tener un efecto muy positivo en los niveles de fatiga del paciente y reducirlos. La terapia del sueño es otra importante intervención no farmacológica y se relaciona particularmente con la higiene del sueño. Los pacientes necesitan ser asesorados sobre la importancia de acostarse y levantarse a la misma hora todos los días de la semana, así como tratar de restringir su hora de dormir a acostarse y apagar la
7
the same time, trying to restrict their bedtime just to simply going to bed and turning off the TV, so that they don’t have any sort of distractions while they are preparing for bed. And then another important non-pharmacologic intervention is acupuncture. Some pharmacologic interventions that have been --- that are being studied, and as well have been used in the past, are stimulant therapy, such as modafinil. Patients can have some improvement in their fatigue with this intervention. However, we pre --- prior to going ahead and prescribing this, we make sure to do a complete history and physical exam on the patient to make certain that there are not any contraindications to the use of these medications. Also antidepressants at times can be helpful. For example, if a patient really is having significant depression, which could be contributing to their fatigue. And then, in some patient populations, steroid therapy is helpful, but temp --- typically this is more in a palliative care setting and this is really not commonly used for the purpose of just cancer-related fatigue.
TV, a fin de no tener ningún tipo de distracción mientras se preparan para descansar. Otra importante intervención no farmacológica es la acupuntura. Algunas intervenciones farmacológicas que se están estudiando y que ya se han utilizado en el pasado son las terapias estimulantes, como el modafinilo. Con esta intervención, los pacientes pueden experimentar cierta mejoría en la fatiga. Antes de recetarlo, debe hacerse una historia y un examen físico completo para asegurar que no haya contraindicaciones para el uso del medicamento. A veces, los antidepresivos pueden ser útiles. Por ejemplo, si un paciente sufre una depresión importante, podría estar contribuyendo a su fatiga. En algunas poblaciones de pacientes, el tratamiento con esteroides es útil, pero normalmente se utiliza en un entorno de cuidados paliativos y no sólo para tratar la fatiga relacionada con el cáncer.
So it’s important to not only define cancer-related fatigue, which I have already done, but it’s also to be --- it’s important to have a good definition for a sleep disorder. And a simple definition is that a sleep disorder is defined as any disorder that affects, disrupts, or involves sleep
Es importante definir la fatiga relacionada con el cáncer y contar también con una buena definición de qué es un trastorno del sueño. Una definición simple es cualquier trastorno que afecta, perturba o involucra el sueño.
8
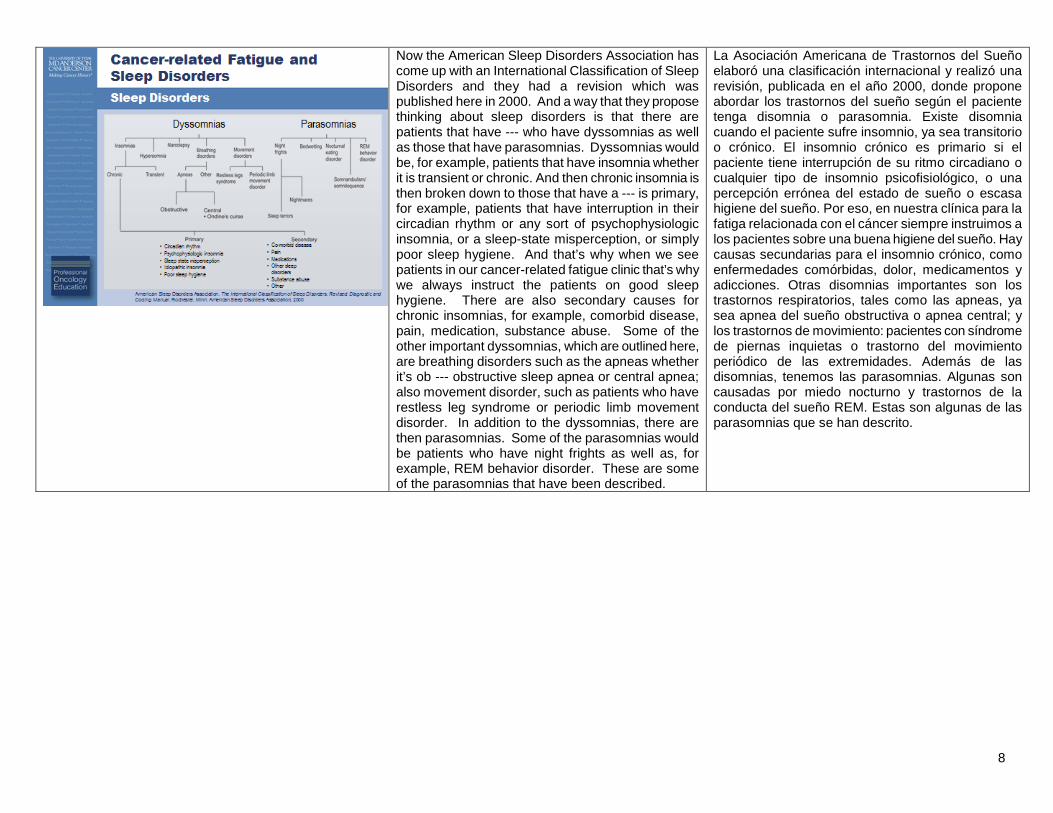
Now the American Sleep Disorders Association has come up with an International Classification of Sleep Disorders and they had a revision which was published here in 2000. And a way that they propose thinking about sleep disorders is that there are patients that have --- who have dyssomnias as well as those that have parasomnias. Dyssomnias would be, for example, patients that have insomnia whether it is transient or chronic. And then chronic insomnia is then broken down to those that have a --- is primary, for example, patients that have interruption in their circadian rhythm or any sort of psychophysiologic insomnia, or a sleep-state misperception, or simply poor sleep hygiene. And that’s why when we see patients in our cancer-related fatigue clinic that’s why we always instruct the patients on good sleep hygiene. There are also secondary causes for chronic insomnias, for example, comorbid disease, pain, medication, substance abuse. Some of the other important dyssomnias, which are outlined here, are breathing disorders such as the apneas whether it’s ob --- obstructive sleep apnea or central apnea; also movement disorder, such as patients who have restless leg syndrome or periodic limb movement disorder. In addition to the dyssomnias, there are then parasomnias. Some of the parasomnias would be patients who have night frights as well as, for example, REM behavior disorder. These are some of the parasomnias that have been described.
La Asociación Americana de Trastornos del Sueño elaboró una clasificación internacional y realizó una revisión, publicada en el año 2000, donde propone abordar los trastornos del sueño según el paciente tenga disomnia o parasomnia. Existe disomnia cuando el paciente sufre insomnio, ya sea transitorio o crónico. El insomnio crónico es primario si el paciente tiene interrupción de su ritmo circadiano o cualquier tipo de insomnio psicofisiológico, o una percepción errónea del estado de sueño o escasa higiene del sueño. Por eso, en nuestra clínica para la fatiga relacionada con el cáncer siempre instruimos a los pacientes sobre una buena higiene del sueño. Hay causas secundarias para el insomnio crónico, como enfermedades comórbidas, dolor, medicamentos y adicciones. Otras disomnias importantes son los trastornos respiratorios, tales como las apneas, ya sea apnea del sueño obstructiva o apnea central; y los trastornos de movimiento: pacientes con síndrome de piernas inquietas o trastorno del movimiento periódico de las extremidades. Además de las disomnias, tenemos las parasomnias. Algunas son causadas por miedo nocturno y trastornos de la conducta del sueño REM. Estas son algunas de las parasomnias que se han descrito.
9
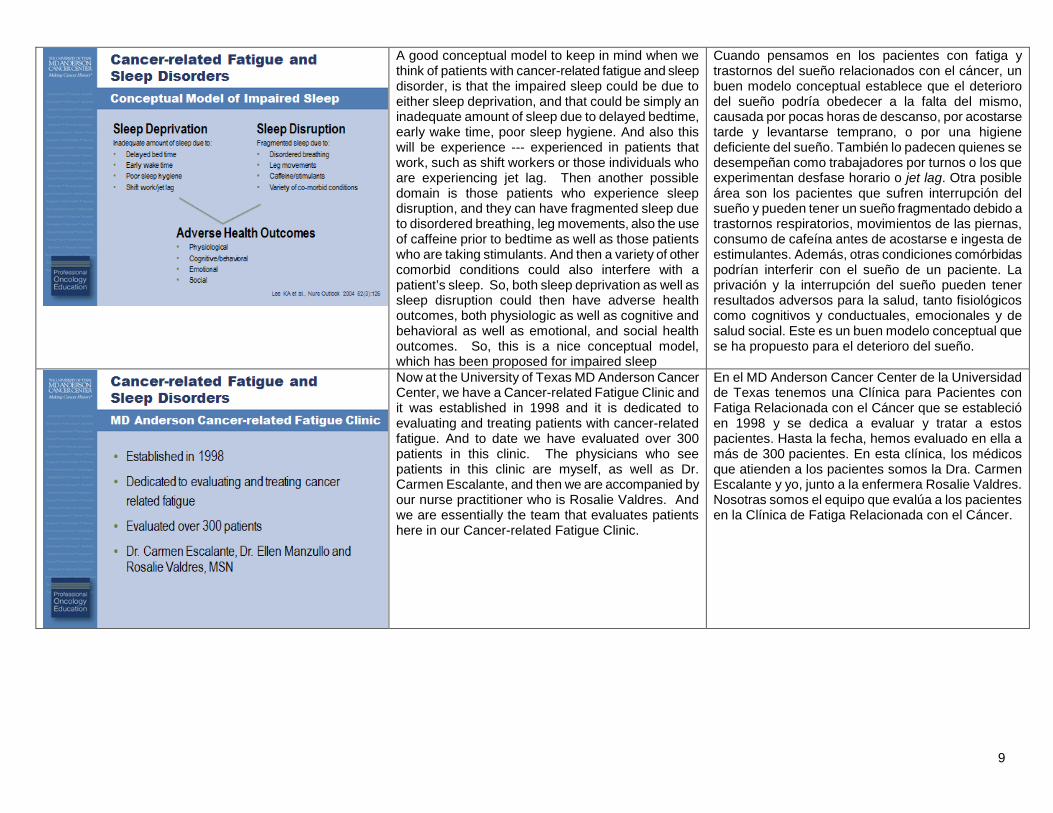
A good conceptual model to keep in mind when we think of patients with cancer-related fatigue and sleep disorder, is that the impaired sleep could be due to either sleep deprivation, and that could be simply an inadequate amount of sleep due to delayed bedtime, early wake time, poor sleep hygiene. And also this will be experience --- experienced in patients that work, such as shift workers or those individuals who are experiencing jet lag. Then another possible domain is those patients who experience sleep disruption, and they can have fragmented sleep due to disordered breathing, leg movements, also the use of caffeine prior to bedtime as well as those patients who are taking stimulants. And then a variety of other comorbid conditions could also interfere with a patient’s sleep. So, both sleep deprivation as well as sleep disruption could then have adverse health outcomes, both physiologic as well as cognitive and behavioral as well as emotional, and social health outcomes. So, this is a nice conceptual model, which has been proposed for impaired sleep
Cuando pensamos en los pacientes con fatiga y trastornos del sueño relacionados con el cáncer, un buen modelo conceptual establece que el deterioro del sueño podría obedecer a la falta del mismo, causada por pocas horas de descanso, por acostarse tarde y levantarse temprano, o por una higiene deficiente del sueño. También lo padecen quienes se desempeñan como trabajadores por turnos o los que experimentan desfase horario o jet lag. Otra posible área son los pacientes que sufren interrupción del sueño y pueden tener un sueño fragmentado debido a trastornos respiratorios, movimientos de las piernas, consumo de cafeína antes de acostarse e ingesta de estimulantes. Además, otras condiciones comórbidas podrían interferir con el sueño de un paciente. La privación y la interrupción del sueño pueden tener resultados adversos para la salud, tanto fisiológicos como cognitivos y conductuales, emocionales y de salud social. Este es un buen modelo conceptual que se ha propuesto para el deterioro del sueño.
Now at the University of Texas MD Anderson Cancer Center, we have a Cancer-related Fatigue Clinic and it was established in 1998 and it is dedicated to evaluating and treating patients with cancer-related fatigue. And to date we have evaluated over 300 patients in this clinic. The physicians who see patients in this clinic are myself, as well as Dr. Carmen Escalante, and then we are accompanied by our nurse practitioner who is Rosalie Valdres. And we are essentially the team that evaluates patients here in our Cancer-related Fatigue Clinic.
En el MD Anderson Cancer Center de la Universidad de Texas tenemos una Clínica para Pacientes con Fatiga Relacionada con el Cáncer que se estableció en 1998 y se dedica a evaluar y tratar a estos pacientes. Hasta la fecha, hemos evaluado en ella a más de 300 pacientes. En esta clínica, los médicos que atienden a los pacientes somos la Dra. Carmen Escalante y yo, junto a la enfermera Rosalie Valdres. Nosotras somos el equipo que evalúa a los pacientes en la Clínica de Fatiga Relacionada con el Cáncer.
10
When the patients show up for their appointment in our clinic, they are asked to complete an assessment packet. And in the assessment packet, there are tools, which are used to assess a variety of symptoms that I’ve previously described that normally cluster and can possibly contribute to fatigue. For example, one of the tool --- tools that we use are the Brief Fatigue Inventory, which assess --- which assesses a patient’s fatigue. There’s also the Brief Pain Inventory, which assesses patients’ level of pain. We also try to get a sense of the patient’s depression level using the Beck Depression Inventory II. Also, we assess the patient for anxiety using the Beck Anxiety Inventory. As far as sleep is concerned, we use the Brief Sleep Disturbance Scale to assess their sleeping habits as well as the Epworth Sleepiness Scale, which also is very helpful in giving us an assessment of the patient’s sleep. All of these tools are very useful to us when we evaluate the patient, and so these patients complete these assessment tools prior to them being seen by both our nurse practitioner as well as one of the physicians.
Cuando los pacientes acuden a su cita, les pedimos que completen un paquete de evaluación que contiene herramientas para evaluar una variedad de síntomas que ya he descrito y que normalmente se asocian a la fatiga y es posible que contribuyan a ella. Una herramienta que utilizamos es el Inventario Breve de la Fatiga, que evalúa la fatiga de cada paciente. También tenemos un Inventario Breve del Dolor, que evalúa el nivel de dolor. Además, tratamos de evaluar el nivel de depresión del paciente con el Inventario de la Depresión de Beck II y medimos su ansiedad mediante el Inventario de la Ansiedad de Beck. Para el sueño, utilizamos la Escala Breve de Alteraciones del Sueño para evaluar los hábitos de sueño, así como la Escala de Somnolencia de Epworth, que es muy útil para cuantificar el sueño de los pacientes. Todas estas herramientas de evaluación son muy útiles, de manera que los pacientes las completan antes de ser revisados por la enfermera profesional y uno de los médicos.
As far as the Brief Fatigue Inventory is concerned, the BFI scores range from 0 to 10. Patients with a BFI score of 0 to 3.9 are considered to have mild fatigue, those with a score of 4 to 6.9 have moderate fatigue, and then those patients with a BFI score of 7 to 10 are considered to have severe fatigue.
El Inventario Breve de la Fatiga utiliza puntuaciones de 0 a 10. Se considera que los pacientes con una puntuación de 0 a 3.9 tienen fatiga leve; los que tienen de 4 a 6.9, fatiga moderada; y los que tienen de 7 a 10, fatiga grave.
11
As mentioned previously, we use the Brief Sleep Disturbance Scale. And this is used to assess the patient’s sleeping habits, and it’s broken down to those patients who score with a mild sleep disturbance, who have a score of 22 to 29; and that ranges to those patients who are considered to have a severe sleep disturbance and those patients will have a score of greater than 35.
Como se mencionó anteriormente, la Escala Breve de Alteraciones del Sueño nos permite evaluar los hábitos de sueño del paciente. Esta escala clasifica a los pacientes desde una alteración del sueño leve, que han obtenido de 22 a 29 puntos, hasta aquellos con una alteración grave del sueño, cuya puntuación es de más de 35.
We also use the Epworth Sleepiness Scale. Now this is used to measure excessive daytime sleepiness; and it’s primarily been evaluated --- it’s primarily validated in patients with obstructive sleep apnea and the average score for the normal population is 0 to 9. And patients that have a score of anywhere usually above 10, a sleep specialist is recommended.
También utilizamos la Escala de Somnolencia de Epworth para medir la somnolencia diurna excesiva y ha sido validada en pacientes con apnea del sueño obstructiva. Una calificación promedio para la población normal es de 0 a 9. Los pacientes que obtienen una puntuación superior a 10 son referidos a un especialista del sueño.
12
We are fortunate here at the University of Texas MD Anderson Cancer Center not only to have our Fa---clinic focused on cancer-related fatigue, but we also have a Sleep Center. Now our Sleep Center was opened in September of 2006 and today greater than 600 sleep studies have been performed. With our Sleep Center, we have three board-certified sleep technologists as well as three board-certified sleep physicians, who are Dr. David Balachandran, Dr. Lara Bashoura, and Dr. Saadia Faiz.
En el MD Anderson Cancer Center de la Universidad de Texas tenemos la fortuna de contar con una clínica que se ocupa de la fatiga relacionada con el cáncer, pero también tenemos un Centro del Sueño. Nuestro Centro del Sueño se inauguró en septiembre de 2006 y ya se han realizado más de 600 estudios sobre el sueño. En nuestro centro tenemos tres técnicos certificados, así como tres médicos del sueño, también certificados: el Dr. David Balachandran y las Dras. Lara Bashoura y Saadia Faiz.
And so, we are in a very unique position here at our institution to be able to evaluate the relationship between cancer-related fatigue and sleep disorders.
Así, en nuestra institución estamos en una posición privilegiada para evaluar la relación entre la fatiga y los trastornos del sueño relacionados con el cáncer.
13
And so, physicians in both the Department[s] of General Internal Medicine, Ambulatory Treatment and Emergency Care as well as physicians in this Sleep Center began to ask the question, “What is the relationship between sleep disorders and fatigue in cancer patients?” And actually this resulted in our initial sleep disorder study.
Los médicos del Departamento de Medicina Interna General, Tratamiento Ambulatorio y Cuidado de Emergencia, así como los médicos en el Centro del Sueño, comenzaron a preguntarse cuál era la relación entre los trastornos del sueño y la fatiga en los pacientes con cáncer, lo que dio como resultado nuestro estudio inicial sobre trastornos del sueño.
And we performed a retrospective study and we looked at the patients who were evaluated in the Cancer-related Fatigue Clinic, and the study period that we used was September 1, 2006, to May 31, 2008. And we identified patients who were referred by the Cancer-related Fatigue Clinic for a sleep consult. We --- reviewed patient demographic information as well as clinical factors. And then we did a review of the symptom status data. And the symptom --- symptom status data came from the results of the assessment tools they completed prior to their initial consult visit in our clinic. And those symptoms, which I prior --- mentioned prior, are, for example, pain, sleep disorders, depression, and anxiety. In this study, we also determined if patients had a sleep study completed and then we reviewed the results of the sleep study.
Realizamos un estudio retrospectivo y analizamos a los pacientes evaluados en la Clínica de Fatiga Relacionada con el Cáncer, que se extendió del 1º de septiembre de 2006 al 31 de mayo de 2008. Identificamos a los pacientes que fueron referidos por la Clínica para una consulta de sueño y analizamos la información demográfica y los factores clínicos de los pacientes. Luego, analizamos los datos de estado de los síntomas, que obtuvimos con las herramientas de evaluación que los pacientes completaron antes de su primera visita a nuestra clínica. Esos síntomas, que ya mencioné, son dolor, trastornos del sueño, depresión y ansiedad. En este estudio determinamos si los pacientes habían realizado un estudio de sueño completo y luego revisamos los resultados.
14
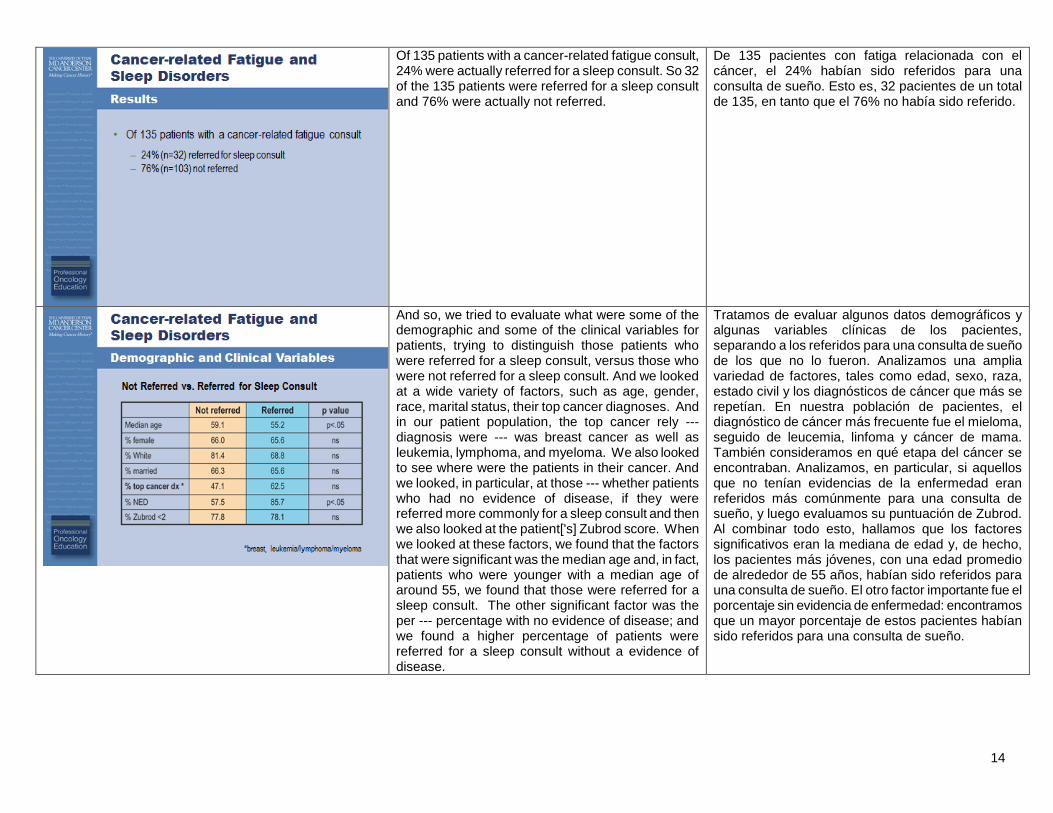
Of 135 patients with a cancer-related fatigue consult, 24% were actually referred for a sleep consult. So 32 of the 135 patients were referred for a sleep consult and 76% were actually not referred.
De 135 pacientes con fatiga relacionada con el cáncer, el 24% habían sido referidos para una consulta de sueño. Esto es, 32 pacientes de un total de 135, en tanto que el 76% no había sido referido.
And so, we tried to evaluate what were some of the demographic and some of the clinical variables for patients, trying to distinguish those patients who were referred for a sleep consult, versus those who were not referred for a sleep consult. And we looked at a wide variety of factors, such as age, gender, race, marital status, their top cancer diagnoses. And in our patient population, the top cancer rely --- diagnosis were --- was breast cancer as well as leukemia, lymphoma, and myeloma. We also looked to see where were the patients in their cancer. And we looked, in particular, at those --- whether patients who had no evidence of disease, if they were referred more commonly for a sleep consult and then we also looked at the patient['s] Zubrod score. When we looked at these factors, we found that the factors that were significant was the median age and, in fact, patients who were younger with a median age of around 55, we found that those were referred for a sleep consult. The other significant factor was the per --- percentage with no evidence of disease; and we found a higher percentage of patients were referred for a sleep consult without a evidence of disease.
Tratamos de evaluar algunos datos demográficos y algunas variables clínicas de los pacientes, separando a los referidos para una consulta de sueño de los que no lo fueron. Analizamos una amplia variedad de factores, tales como edad, sexo, raza, estado civil y los diagnósticos de cáncer que más se repetían. En nuestra población de pacientes, el diagnóstico de cáncer más frecuente fue el mieloma, seguido de leucemia, linfoma y cáncer de mama. También consideramos en qué etapa del cáncer se encontraban. Analizamos, en particular, si aquellos que no tenían evidencias de la enfermedad eran referidos más comúnmente para una consulta de sueño, y luego evaluamos su puntuación de Zubrod. Al combinar todo esto, hallamos que los factores significativos eran la mediana de edad y, de hecho, los pacientes más jóvenes, con una edad promedio de alrededor de 55 años, habían sido referidos para una consulta de sueño. El otro factor importante fue el porcentaje sin evidencia de enfermedad: encontramos que un mayor porcentaje de estos pacientes habían sido referidos para una consulta de sueño.
15
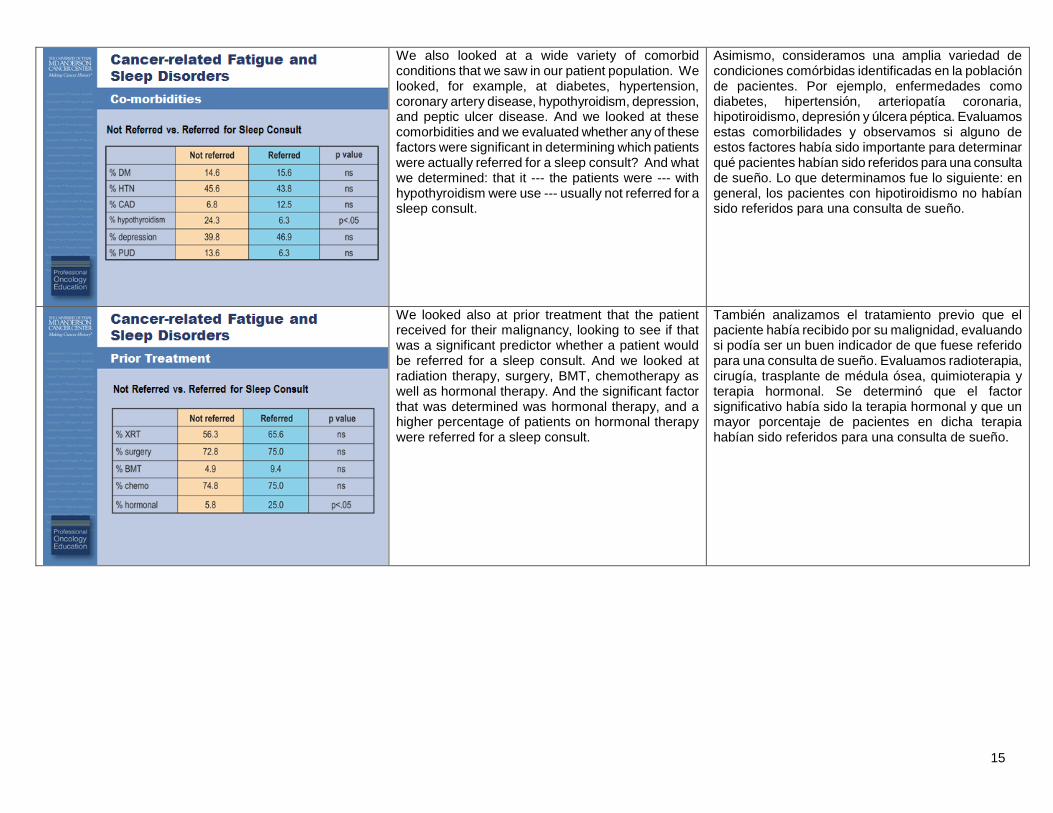
We also looked at a wide variety of comorbid conditions that we saw in our patient population. We looked, for example, at diabetes, hypertension, coronary artery disease, hypothyroidism, depression, and peptic ulcer disease. And we looked at these comorbidities and we evaluated whether any of these factors were significant in determining which patients were actually referred for a sleep consult? And what we determined: that it --- the patients were --- with hypothyroidism were use --- usually not referred for a sleep consult.
Asimismo, consideramos una amplia variedad de condiciones comórbidas identificadas en la población de pacientes. Por ejemplo, enfermedades como diabetes, hipertensión, arteriopatía coronaria, hipotiroidismo, depresión y úlcera péptica. Evaluamos estas comorbilidades y observamos si alguno de estos factores había sido importante para determinar qué pacientes habían sido referidos para una consulta de sueño. Lo que determinamos fue lo siguiente: en general, los pacientes con hipotiroidismo no habían sido referidos para una consulta de sueño.
We looked also at prior treatment that the patient received for their malignancy, looking to see if that was a significant predictor whether a patient would be referred for a sleep consult. And we looked at radiation therapy, surgery, BMT, chemotherapy as well as hormonal therapy. And the significant factor that was determined was hormonal therapy, and a higher percentage of patients on hormonal therapy were referred for a sleep consult.
También analizamos el tratamiento previo que el paciente había recibido por su malignidad, evaluando si podía ser un buen indicador de que fuese referido para una consulta de sueño. Evaluamos radioterapia, cirugía, trasplante de médula ósea, quimioterapia y terapia hormonal. Se determinó que el factor significativo había sido la terapia hormonal y que un mayor porcentaje de pacientes en dicha terapia habían sido referidos para una consulta de sueño.
16
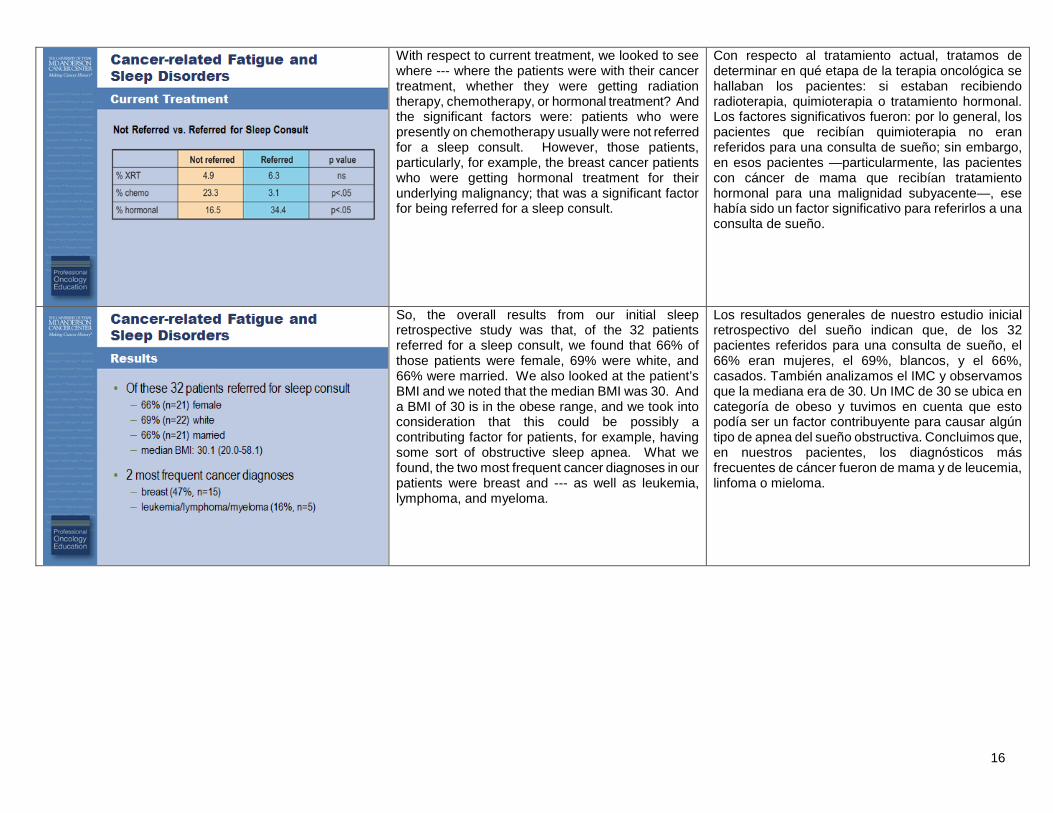
With respect to current treatment, we looked to see where --- where the patients were with their cancer treatment, whether they were getting radiation therapy, chemotherapy, or hormonal treatment? And the significant factors were: patients who were presently on chemotherapy usually were not referred for a sleep consult. However, those patients, particularly, for example, the breast cancer patients who were getting hormonal treatment for their underlying malignancy; that was a significant factor for being referred for a sleep consult.
Con respecto al tratamiento actual, tratamos de determinar en qué etapa de la terapia oncológica se hallaban los pacientes: si estaban recibiendo radioterapia, quimioterapia o tratamiento hormonal. Los factores significativos fueron: por lo general, los pacientes que recibían quimioterapia no eran referidos para una consulta de sueño; sin embargo, en esos pacientes —particularmente, las pacientes con cáncer de mama que recibían tratamiento hormonal para una malignidad subyacente—, ese había sido un factor significativo para referirlos a una consulta de sueño.
So, the overall results from our initial sleep retrospective study was that, of the 32 patients referred for a sleep consult, we found that 66% of those patients were female, 69% were white, and 66% were married. We also looked at the patient’s BMI and we noted that the median BMI was 30. And a BMI of 30 is in the obese range, and we took into consideration that this could be possibly a contributing factor for patients, for example, having some sort of obstructive sleep apnea. What we found, the two most frequent cancer diagnoses in our patients were breast and --- as well as leukemia, lymphoma, and myeloma.
Los resultados generales de nuestro estudio inicial retrospectivo del sueño indican que, de los 32 pacientes referidos para una consulta de sueño, el 66% eran mujeres, el 69%, blancos, y el 66%, casados. También analizamos el IMC y observamos que la mediana era de 30. Un IMC de 30 se ubica en categoría de obeso y tuvimos en cuenta que esto podía ser un factor contribuyente para causar algún tipo de apnea del sueño obstructiva. Concluimos que, en nuestros pacientes, los diagnósticos más frecuentes de cáncer fueron de mama y de leucemia, linfoma o mieloma.
17
As far as the patient reported outcomes were referred, we looked at the results of all of the assessment tools and what was significant, and what we would have anticipated is that those patients with a higher median score on the BSDS, which was one of our sleep tools, those patients with a higher score were referred for a sleep consult.
En cuanto a los resultados informados por el paciente, analizamos los resultados de todas las herramientas de evaluación, qué fue importante y qué podríamos haber anticipado. Los pacientes con una puntuación superior a la media en la Escala Breve de Alteraciones del Sueño —una de nuestras herramientas de evaluación— eran los que habían sido referidos a una consulta de sueño.
Most of the patients referred had good Zubrod scores and a high percentage, 75% of the patients, had no evidence of cancer. As far as the patients' median fatigue score on the BFI scale, the median score was 6.2. However, as you can see, there was really a wide range, ranging from 0.8 to 9.2. And, in our Fatigue Clinic, we see a wide variety of patients with fatigue, and it --- it spans, of course, from very mild to the most severe. Of the patients that were referred for a slip --- sleep consult, 63% of those patients actually went on to have a sleep study in our Sleep Center. And the two most common diagnoses that were discovered were obstructive sleep apnea, and actually 80% had obstructive sleep apnea. And then next was periodic limb movement disorder and actually four patients were diagnosed with this sleep disorder.
La mayoría de ellos tenían una buena puntuación de Zubrod, y un alto porcentaje —el 75%— no presentaba indicios de cáncer. En el Inventario Breve de la Fatiga, la mediana de la puntuación de fatiga fue de 6.2. Como puede verse, el rango fue realmente amplio y varió desde 0.8 hasta 9.2. En nuestra clínica atendemos una amplia variedad de pacientes con fatiga, que abarcan desde casos muy leves hasta los más graves. De los pacientes que fueron referidos para una consulta de sueño, el 63% se hizo un estudio en nuestro Centro del Sueño. Los dos diagnósticos más comunes fueron apnea del sueño obstructiva, en el 80% de los pacientes, y el trastorno del movimiento periódico de extremidades, diagnosticado en 4 pacientes.
18
So, in summary, sleep disorders may be under-recognized in cancer-related fatigue patients. And what we found is that 24% of patients that were evaluated for cancer-related fatigue in our Fatigue Center were found appropriate for sleep consult. So, we --- what this shows is that sleep disorders should be considered when evaluating patients with cancer-related fatigue. This was our initial study. We’re planning to continue the work, evaluating the relationship between cancer-related fatigue and sleep disorders. And, in particular, we want to continue to focus on the impact of sleep dysfunction on cancer-related fatigue, particularly as interventions are made when available. Thank you for very much and I hope this presentation has been helpful.
En resumen, los trastornos del sueño no son debidamente reconocidos en los pacientes con fatiga relacionada con el cáncer. Encontramos que el 24% de los pacientes evaluados por fatiga relacionada con el cáncer en nuestro Centro de la Fatiga eran aptos para una consulta de sueño. Esto demuestra que al evaluar a los pacientes con fatiga relacionada con el cáncer deben considerarse también los trastornos del sueño. Este fue nuestro estudio inicial y planeamos continuar el trabajo evaluando la relación entre la fatiga relacionada con el cáncer y los trastornos del sueño. Queremos concentrarnos particularmente en el impacto que los problemas del sueño tienen sobre la fatiga relacionada con el cáncer, en especial cuando se realizan intervenciones. Muchas gracias y espero que esta presentación les haya sido útil.