1 PowerPoint Slides English Text Brazilian Portuguese Translation Hematologic Malignancies: Diagnosing and Staging, Part 2: Lymphoma and Multiple Myeloma VideoTranscript Câncer Hematológico: Diagnóstico e Estadiamento, 2 a Parte: Linfoma e Mieloma Múltiplo Transcrição do video Professional Oncology Education Hematologic Malignancies: Diagnosing and Staging, Part 2: Lymphoma and Mulitple Myeloma Time: 20:19 Educação Profissional em Oncologia Câncer Hematológico: Diagnóstico e Estadiamento, 2 a Parte: Linfoma e Mieloma Múltiplo Duração: 20:19 Jorge Romaguera, M.D. Professor Lymphoma/Myeloma The University of Texas MD Anderson Cancer Center Jorge Romaguera, M.D. Professor Linfoma/Mieloma MD Anderson Cancer Center – Universidade do Texas Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Part II: Lymphoma and Multiple Myeloma Part II: Lymphoma and Multiple Myeloma Part II: Lymphoma and Multiple Myeloma Part II: Lymphoma and Multiple Myeloma Hematologic Malignancies: Hematologic Malignancies: Diagnosis and Staging Diagnosis and Staging Part II: Lymphoma and Part II: Lymphoma and Multiple Myeloma Multiple Myeloma Jorge Romaguera, M.D. Professor Lymphoma/Myeloma Hello. I am Dr. Jorge Romaguera. I am Professor of the Department of Lymphoma and Multiple Myeloma at the University of Texas MD Anderson Cancer Center. I will be speaking to you today about the diagnosis of staging of lymphomas and multiple myeloma. Olá. Eu sou o Dr. Jorge Romaguera. Sou professor do Departamento de Linfoma e Mieloma Múltiplo do MD Anderson Cancer Center da Universidade do Texas. Hoje, falarei sobre diagnóstico e estadiamento de linfomas e mieloma múltiplo.
Transcript
1
PowerPoint Slides English Text Brazilian Portuguese Translation
Hematologic Malignancies: Diagnosing and Staging, Part 2: Lymphoma and Multiple Myeloma VideoTranscript
Câncer Hematológico: Diagnóstico e Estadiamento, 2a Parte: Linfoma e Mieloma Múltiplo Transcrição do video
Professional Oncology Education Hematologic Malignancies: Diagnosing and Staging, Part 2: Lymphoma and Mulitple Myeloma Time: 20:19
Educação Profissional em Oncologia
Câncer Hematológico: Diagnóstico e Estadiamento, 2a Parte: Linfoma e Mieloma Múltiplo Duração: 20:19
Jorge Romaguera, M.D. Professor Lymphoma/Myeloma The University of Texas MD Anderson Cancer Center
Jorge Romaguera, M.D. Professor Linfoma/Mieloma MD Anderson Cancer Center – Universidade do Texas
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Hello. I am Dr. Jorge Romaguera. I am Professor of the Department of Lymphoma and Multiple Myeloma at the University of Texas MD Anderson Cancer Center. I will be speaking to you today about the diagnosis of staging of lymphomas and multiple myeloma.
Olá. Eu sou o Dr. Jorge Romaguera. Sou professor do Departamento de Linfoma e Mieloma Múltiplo do MD Anderson Cancer Center da Universidade do Texas. Hoje, falarei sobre diagnóstico e estadiamento de linfomas e mieloma múltiplo.
2
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Part II: Objectives
Upon completion of this part, participants will
be able to:
• Define lymphoma, including Hodgkin’s and
Non-Hodgkin’s and multiple myeloma
• Discuss the clinical presentation of these diseases
• Discuss the hematologic, radiographic and
pathologic findings for classification and
staging of each
Upon completion of this part of this talk, you will be able to define lymphoma, both Hodgkin’s and non-Hodgkin’s lymphoma as well as multiple myeloma. You will be able to discuss clinical presentation of the cases of these diseases --- [I apologize] --- as well as hematologic, radiographic, and pathologic findings for classification and staging of each.
Após a conclusão desta parte da palestra, vocês deverão ser capazes de definir linfoma, tanto o de Hodgkin quanto o não-Hodgkin, e mieloma múltiplo. Vocês deverão ser capazes de discutir o quadro clínico de casos destas doenças – [desculpem] – bem como achados hematológicos, radiográficos e patológicos para a classificação e o estadiamento de cada uma delas.
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Lymphoma
• Group of malignancies originating in the lymphatic system
• Types of lymphoma
– Hodgkin’s lymphoma
– Non-Hodgkin’s lymphoma (NHL)
• 85% B-cell lymphoma
• 15% T-cell lymphoma
We will start first with lymphoma. This is a group of malignancies that originates in the lymphatic system. It is broadly divided in two categories, the Hodgkin’s lymphoma and the non-Hodgkin’s lymphoma or malignant lymphoma. Here in North America, 85% of the malignant lymphomas are of the B-cell type and 15 are of a T-cell type. We will be discussing in this presentation mainly the B-cell type, which is the most common.
Começaremos com o linfoma. Este é um grupo de neoplasias malignas que se originam no sistema linfático. Dividem-se, grosso modo, em duas categorias: o linfoma de Hodgkin e o linfoma não-Hodgkin ou linfoma maligno. Aqui, na América do Norte, 85% dos linfomas malignos são de células B e 15% são de células T. Nesta apresentação, discutiremos principalmente o tipo de células B, que é o mais comum.
3
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Risk Factors for Lymphoma
• Cause of NHL unknown
• Inherited familial: small percentage
• Environmental
– Chemical suspected (e.g., pesticides/herbicides)
The cause of non-Hodgkin’s lymphoma is not known. It is not accepted to be inherited as other cancers are, although there is a suspicion that there might be some familial inheritance risk. There are environmental factors that have been associated, mainly herbicides. Also the Agent Orange which was used in the Vietnam War, also the creosol that was applied to the telephone posts several --- a decade or two ago. There is a suspicion that high-dose radiation exposure might predispose to non-Hodgkin’s lymphoma. It is known that immune deficiency states such as AIDS, acquired immunodeficiency disease --- syndrome, is a risk factor for developing lymphoma. It is also known that Helicobacter pylori predisposes in a very small population of patients to the development of indolent lymphoma in the stomach. There is also a suspicion of Epstein-Barr virus being behind the lymphomagenesis of several lymphomas. The one that is mostly discussed is the child --- childhood Burkitt’s lymphoma, the African type.
A causa do linfoma não-Hodgkin não é conhecida. Não é aceita a ideia de hereditariedade como acontece com outros cânceres, embora se suspeite haver algum risco de transmissão genética. Existem fatores ambientais associados, principalmente herbicidas. Além disso, o Agente Laranja usado na Guerra do Vietnã e o creosol aplicado nos postes de telefone há várias... há uma década ou duas. Suspeita-se que a exposição a uma elevada dose de irradiação possa predispor [a pessoa] ao linfoma não-Hodgkin. Sabe-se que estados de deficiência imunológica, como o AIDS, a doença... a síndrome da imunodeficiência adquirida, é um fator de risco para linfoma. Sabe-se, também, que a Helicobacter pylori predispõe uma população de pacientes muito pequena ao linfoma indolente no estômago. Além disso, suspeita-se que o vírus de Epstein-Barr esteja implicado na linfomagênese de vários linfomas. O tipo mais discutido é o linfoma de Burkitt na infância, o tipo africano.
4
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Signs and Symptoms
• Enlarged (usually non-tender) lymph nodes that do
not disappear in 2 weeks or respond to antibiotics
• Constitutional symptoms (< 20%)
– Weight loss
– Fever
– Night sweats
You will know or suspect lymphoma if you have a --- an enlarged lymph node that does not disappear after two weeks and is not responding to antibiotics. Usually this lymph node will be non-tender. And it might or not be associated with unexplained weight loss or unexplained fever or drenching night sweats so that you have to change your clothes or your night spread --- sheets.
Sabemos ou suspeitamos que seja linfoma quando da presença de linfonodo aumentado que não desaparece depois de duas semanas e não responde a antibióticos. Geralmente, esse linfonodo não será sensível à palpação. E pode ou não estar associado à perda de peso ou febre inexplicáveis ou sudorese noturna intensa a ponto de ter que trocar a roupa ou os lençóis.
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Lymphoma: Diagnosis
• Biopsy– Fine needle aspiration (FNA)
– Excisional/incisional
– Bone marrow
• Laboratory tests
– CBC and differential
– Serum chemistries
• Imaging studies
– Chest x-ray
– Computed tomography (CT) scan of neck/chest/abdomen/pelvis
– Positron emission tomography (PET) scan in selected cases
To diagnose lymphoma, you will need a biopsy. It could be incisional or excisional. And fine-needle aspiration is also recommended in order to do some of the additional markers and recent studies that have been added to the armamentarium. But you do have a --- you do need a biopsy. This will be able to make --- make you able to subclassify the lymphoma. You will need a bone marrow, both for staging purposes, to see how advanced the disease is. And, in some cases where you present with symptoms but no enlarged lymph nodes, this might be the only place where you have lymphoma. As part of the initial tests, once you have a diagnosis, you will have to evaluate for other prognostic factors, such as elevated levels of lactate dehydrogenase in the serum. You will also want to know how the blood count is to see if there has been an effect of the lymphoma in the platelet count as well as the hemoglobin. You will also want to do imaging studies as part of the workup to find the
Para diagnosticar o linfoma, precisamos de uma biópsia. Pode ser incisional ou excisional. A punção aspirativa com agulha fina também é recomendada para fazer alguns dos outros marcadores e recentes estudos que foram adicionados ao armamentário. Mas, temos que fazer... precisamos de uma biópsia. Com a biópsia poderemos subclassificar o linfoma. Precisamos da medula óssea, para fins de estadiamento e para ver o avanço da doença. E, em alguns casos, em que o paciente apresenta sintomas, mas sem linfonodos aumentados, talvez seja a única localização com linfoma. Como parte dos testes iniciais e em mãos do diagnóstico, temos que avaliar outros fatores prognósticos, como níveis elevados da lactato-desidrogenase no soro. Além disso, devemos conhecer o hemograma e ver se houve um efeito do linfoma na contagem de plaquetas e hemoglobina. Também devemos fazer estudos por imagem como parte do trabalho para descobrir a extensão da doença. Dentre eles, uma
5
extent of disease. This will include a chest x-ray, computed tomographies of the neck, chest, abdomen, and pelvis, and more recently a positron emission tomography in the cases that have large cell non-Hodgkin’s lymphoma or Hodgkin’s lymphoma.
radiografia torácica, tomografias computadorizadas do pescoço, tórax, abdome e pelve e, mais recentemente, uma tomografia por emissão de pósitrons nos casos de linfoma não Hodgkin de grandes células ou linfoma de Hodgkin.
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
World Health Organization (WHO) Classification of B-cell Lymphoma
Jaffe ES. Hematol Am Soc Hematol Educ Program 2009:523
Indolent Aggressive Very Aggressive
• Small lymphocytic lymphoma
• Lymphoplasmacytic/Waldenström’s
macroglobulinemia (WM)
•Marginal zone lymphoma
• Follicle center lymphoma, follicular, grade I-II
• Primary cutaneous follicle center lymphoma
•Multiple myeloma
•Mantle cell lymphoma
• Follicle center lymphoma, follicular, grade III
•Diffuse large B-cell lymphoma (DLBCL)
• Primary mediastinal large B-cell lymphoma
• Lymphomatoid granulomatosis
• Primary cutaneous DLCL- leg type
• Burkitt’s lymphoma
• Intravascular large B-cell lymphoma
There have been many classifications of lymphoma. The most recent one, the World Health Organization Classification from a year or two ago, is mainly a pathologic classification. Although for the clinician it helps to separate them into the slower indolent growth lymphomas, the more aggressive lymphopro --- lymphoproliferative processes, and the very aggressively fast-growing lymphomas. The indolent lymphomas are those mentioned in the table: small lymphocytic lymphoma; Waldenström’s, which is intermediate between lymphoma and a plasmacytic process; the marginal zone lymphomas; the follicle center cell lymphoma follicular grades I and II, which are by far the most common indolent lymphomas; and the follicle center primary cutaneous lymphomas. Other aggressive lymphoproliferative disorders, multiple myeloma is included, but I will discuss this separately. Mantle cell lymphoma is one of the aggressive lymphomas. The follicle center cell follicular grade III is considered aggressive and should be treated as such. The diffuse large B-cell lymphoma is one of the two most common lymphomas along with the follicle center follicular grade I and II, and other more unusual presentations such as primary mediastinal large-cell lymphoma, lymphomatoid granulomatosis, primary cutaneous large-cell lymphoma of the leg type. Under the very aggressive group, the fast growing lymphomas with also a predilection for extranodal presentation are the Burkitt’s and the intervascular large B-cell lymphoma.
Tem havido muitas classificações de linfoma. A mais recente, a Classificação da Organização Mundial de Saúde de um ano a dois atrás, é basicamente uma classificação patológica. Mesmo assim, serve de ajuda ao clínico para separá-los em linfomas indolentes de crescimento mais lento, processos linfoproliferativos mais agressivos e linfomas muito agressivos de rápido crescimento. Os linfomas indolentes são aqueles indicados na tabela: linfoma linfocítico de pequenas células, de Waldenström, que é intermediário entre linfoma e processo plasmocítico, linfomas de zona marginal, linfoma centrofolicular de grau folicular I e II, que são, de longe, os linfomas indolentes mais comuns e linfomas cutâneos primários centrofoliculares. Outros transtornos linfoproliferativos agressivos, o mieloma múltiplo é incluído, mas este será discutido separadamente. O linfoma de células do manto é um dos linfomas agressivos. O de célula centrofolicular de grau III é considerado agressivo e deve ser tratado como tal. O linfoma difuso de grandes células B é um dos dois linfomas mais comuns juntamente com o centrofolicular de graus I e II, e outros quadros clínicos menos comuns, como o linfoma mediastinal primário de grandes células, a granulomatose linfomatoide e o linfoma cutâneo primário de grandes células tipo perna. No grupo dos muito agressivos, os linfomas de rápido crescimento, também com predileção por apresentação extranodal, são os linfomas de Burkitt e o intervascular de grandes células B.
6
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Most Common NHLs
Armitage JO, Weisenburger DD. J Clin Oncol. 1998 16(8):2780
DLBCL
31%BL
2%
FL, 22%
PMLBCL
2%
MALTL
8%
PTCL
7%
SLL/CLL
7%
ALCL
2%
Other, 9%
MCL
6%
MZL, nodal, 2%
T-LL, 2%
This pie chart gives you an idea of the frequency of distribution. Like I said before, the most common lymphoproliferative malignancies, non-Hodgkin’s lymphomas are the large B-cell lymphomas and the follicular lymphomas.
Este gráfico dá uma ideia da frequência de distribuição. Como disse antes, as neoplasias malignas linfoproliferativas mais comuns, os linfomas não Hodgkin são linfomas de grandes células B e linfomas foliculares.
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Follicular Lymphoma
This is an example of how a researcher would evaluate and what he would see under regular electron --- [I’m sorry] --- under regular microscopy on low-power field. This would be a follicular lymphoma, so-called follicular because it respects the follicular active texture of the lymph nodes. The areas that are less dense are the areas that are involved by the lymphoma: and that is the center of the follicle, so-called germinal center of the follicle. The areas in between the follicles are not involved by lymphoma.
Este é um exemplo de como um pesquisador avaliaria e o que veria em um elétron comum – [desculpem] – em um microscópio comum de campo de pequeno aumento. Este poderia ser um linfoma folicular, chamado folicular porque respeita a textura folicular ativa dos linfonodos. As áreas menos densas são aquelas cobertas pelo linfoma e este é o centro do folículo, denominado centro germinal do folículo. As áreas entre os folículos não estão cobertas pelo linfoma.
7
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Diffuse Large B-cell Lymphoma Morphologic Variants
Centroblastic
VariantImmunoblastic
Variant
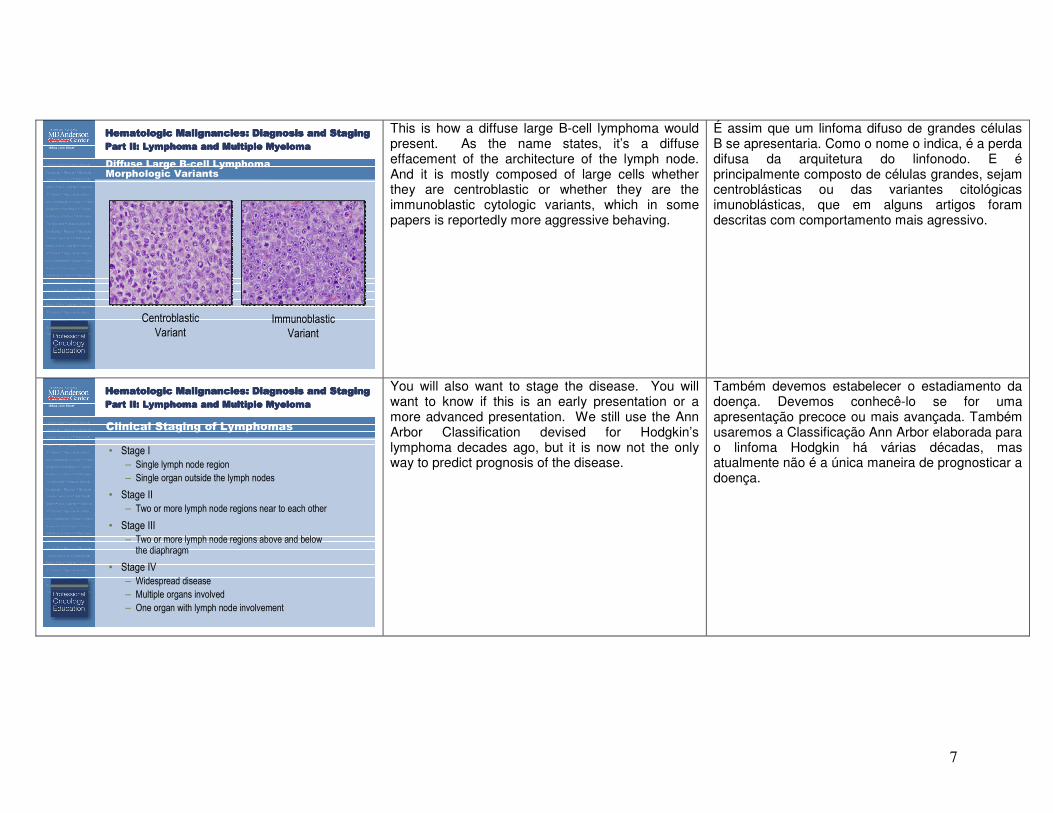
This is how a diffuse large B-cell lymphoma would present. As the name states, it’s a diffuse effacement of the architecture of the lymph node. And it is mostly composed of large cells whether they are centroblastic or whether they are the immunoblastic cytologic variants, which in some papers is reportedly more aggressive behaving.
É assim que um linfoma difuso de grandes células B se apresentaria. Como o nome o indica, é a perda difusa da arquitetura do linfonodo. E é principalmente composto de células grandes, sejam centroblásticas ou das variantes citológicas imunoblásticas, que em alguns artigos foram descritas com comportamento mais agressivo.
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Clinical Staging of Lymphomas
• Stage I
– Single lymph node region
– Single organ outside the lymph nodes
• Stage II
– Two or more lymph node regions near to each other
• Stage III
– Two or more lymph node regions above and below the diaphragm
• Stage IV
– Widespread disease
– Multiple organs involved
– One organ with lymph node involvement
You will also want to stage the disease. You will want to know if this is an early presentation or a more advanced presentation. We still use the Ann Arbor Classification devised for Hodgkin’s lymphoma decades ago, but it is now not the only way to predict prognosis of the disease.
Também devemos estabelecer o estadiamento da doença. Devemos conhecê-lo se for uma apresentação precoce ou mais avançada. Também usaremos a Classificação Ann Arbor elaborada para o linfoma Hodgkin há várias décadas, mas atualmente não é a única maneira de prognosticar a doença.
8
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Clinical Staging of Lymphoma
Stage I Stage II Stage III Stage IV
In this staging system, which I will show in a more illustrative fashion, we have four stages depending upon the areas involved. Stage I is a region of nodes involved either above or below the diaphragm. Stage II are two regional areas both either above or below. Stage III has regions involved below and above the diaphragm. And Stage IV is when there is an extranodal presentation along with a region of lymph nodes or two extranodal presentations. In this illustration, the extranodal sites are the bone marrow and the liver, but there could be other extranodal sites.
Neste sistema de estadiamento, que mostrarei de forma mais ilustrativa, temos quatro estágios, dependendo das áreas acometidas. O estágio I é a região de linfonodos acometidos acima ou abaixo do diafragma. O estágio II são duas áreas regionais, ambas localizadas acima ou abaixo. O estágio III têm regiões acometidas abaixo e acima do diafragma. E o estágio IV ocorre quando há uma apresentação extranodal juntamente com uma região de linfonodos ou duas apresentações extranodais. Nesta ilustração, os sítios extranodais são a medula óssea e o fígado, mas poderia haver outros sítios extranodais.
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
International Prognostic Index (IPI) for Diffuse Large B-cell Lymphoma
Factor Adverse
Age > 60 years
PS ≥ 2
LDH > Normal
Extranodal sites ≥ 2
Stage III-IV
The International Non-Hodgkin's Lymphoma Prognostic Factors Project. N Engl J Med 1993 329(14):987
Factor Adverse
PS ≥ 2
LDH > Normal
Stage III-IV
Age-Adjusted
As I have mentioned before, we have included in the most recent models of prognosis, not only the stage, which you see in the lower part of the graph --- of the table but other factors such as age, performance status, the level of the lactate dehydrogenase in the serum, and the number of extranodal sites. You can see that, according to the number of factors that you have, you will decrease your chances of being alive at five years, going from 73% chance if you have none or one of these five variables in the adverse category, all the way to 26% only if you have four to five of these variables on the adverse area. There is an age-adjusted model that also helps in specific groups of patients by age --- less or equal to 60 versus more than 60.
Como havia mencionado, incluímos nos modelos de prognósticos mais recentes não apenas o estágio, que vocês podem ver na parte inferior do gráfico... da tabela, mas outros fatores, como idade, grau de desempenho, nível da lactato-desidrogenase no soro e o número de sítios extranodais. Podem ver que, de acordo com o número de fatores presentes, haverá menores chances de a pessoa estar viva em cinco anos, passando de 73% de chance, caso não tiver nenhuma destas cinco variáveis na categoria adversa ou tiver uma delas, até 26% somente se tiver de quatro a cinco dessas variáveis na área adversa. Existe um modelo ajustado para a idade que também ajuda grupos específicos de pacientes pela idade... de até 60 [anos] versus mais de 60 [anos].
9
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Factor Adverse
Nodal Sites ≥ 5
LDH > Normal
Age ≥ 60
Stage III-IV
Hemoglobin < 12 g/dL
PrognosisNumber of
Factors Patients (%)
5-year OS
(%)
10-year OS
(%)
Good 0-1 36 90 71
Intermediate 2 37 78 51
Poor ≥3 27 53 36
Solal-Celigny P et al. Blood. 2004 104(5):1258
International Prognostic Index for Follicular Lymphomas (FLIPI)
This previous staging model was for the diffuse large-cell lymphomas. We have since modified it also to be applicable for the follicular lymphomas. This model has five variables also, although two variables have been removed and two new ones have been added, mainly the number of nodal sites and the level of hemoglobin. And, as you can see, this model predicts, for better or worse, 10 year overall survival.
O modelo de estadiamento anterior era para linfomas difusos de grandes células. Desde então o temos modificado para que também seja aplicável a linfomas foliculares. Este modelo tem cinco variáveis também, apesar de que duas foram eliminadas e duas novas foram acrescentadas, basicamente, o número de sítios nodais e o nível de hemoglobina. E, como podem ver, este modelo prevê, para todos os efeitos, 10 anos de sobrevida global.
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Mantle Cell International Prognostic Index (MIPI)
For each prognostic factor, 0 to 3 points were given to each patient and points
were summed up to a maximum of 11. Patients with 0 to 3 points in summary
were classified as low risk, patients with 4 to 5 points as intermediate risk, and
patients with 6 to 11 points as high risk. ECOG performance status was
weighted with 2 points if patients were unable to work or bedridden (ECOG 2-4).
LDH was weighted according to the ratio to the ULN. Thus, for an ULN of 240
U/L, the cutpoints were 180 U/L, 240 U/L, and 360 U/L, for example.
Points Age, y ECOG LDHULN WBC, 109/L
0 < 50 0-1 < 0.67 < 6.700
1 50-59 — 0.67-0.99 6.700-9.999
2 60-69 2-4 1.000 -1.49 1.000-14.999
3 70 — ≥ 1.500 U/dL ≥ 15.000/mm3
Another example where a recently introduced model is being applied is the mantle cell lymphoma. There is a Mantle Cell International Prognostic Index. And these are four variables that have been included in the model. Two of them are familiar because they have been included in the previous models, the age and the serum level of LDH, and the other two are particular to this lymphoma.
Outro exemplo em que o modelo introduzido recentemente está sendo aplicado é o linfoma de células do manto. Existe o Índice Prognóstico Internacional de Células do Manto. E estas são quatro variáveis que foram incluídas no modelo. Duas delas são conhecidas porque foram incluídas nos modelos anteriores, a idade e o nível sérico de LDH, e as outras duas são específicas para este linfoma.
10
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Overall Survival According to MIPI
Hoster E et al. Blood 2008 111(2):558
Numbers of patients at risk
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Probability of overall survival
Months since registration
0 9684726048362412
LR, median not reached
IR, median = 51
HR, median = 29
LR 180 153 131 99 69 39 15 4
IR 145 116 83 57 37 19 9 5
HR 84 58 29 19 8 5 1 0
And based on the number of variables, you will have low, intermediate, and high risk of death from disease.
E tendo por base o número de variáveis, o risco de óbito pela doença será baixo, intermediário ou alto.
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Hodgkin’s Lymphoma: The WHO Classification
• Nodular lymphocyte predominant with or
without diffuse areas
• Classic types:
― Nodular sclerosing
― Mixed cellularity
― Lymphocyte depleted
― Lymphocyte rich, nodular or diffuse
There are other models for T-cell lymphomas, but the T-cell lymphomas are not being discussed in this talk. Going into the Hodgkin’s lymphoma, the World Health Organization Classification divides them into two major types: nodular lymphocyte predominant with or without diffuse areas. This is the least common and the classical types, which are by far the most common: predominantly nodular sclerosing but also mixed cellularity as well, and the lesser common lymphocyte-depleted and lymphocyte-rich subcategories.
Existem outros modelos para os linfomas de células T, mas estes linfomas não fazem parte desta palestra. Com relação ao linfoma de Hodgkin, a Classificação da Organização Mundial de Saúde o divide em dois tipos principais: com predominância linfocítica nodular com ou sem áreas difusas. Estes são os tipos menos comuns e os clássicos, que são, de longe, os mais comuns: com predominância de esclerose nodular, mas também com celularidade mista, e as subcategorias menos comuns com depleção linfocítica e ricas em linfócitos.
11
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Hodgkin’s Lymphoma: Reed-Sternberg Cell
Courtesy of Jeffrey L. Medeiros, M.D.
This is an example of the Reed-Sternberg cell, which is a pathognomonic cell or used to be called pathognomonic for Hodgkin’s. It is still [a] very reliable parameter to diagnosis Hodgkin’s. As you can see in the center of the slide, there is a cell that has two nuclei. And this is a very typical cell that is present in Hodgkin’s lymphomas.
Este é um exemplo de célula de Reed-Sternberg, que é uma célula patognomônica ou antigamente chamada patognomônica para a de Hodgkin. Ainda é um parâmetro bastante confiável para o diagnóstico [do linfoma] de Hodgkin. Como podem ver no centro do slide, há uma célula que tem dois núcleos. E esta célula é bem típica daquelas presentes nos linfomas de Hodgkin.
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Early Stage (Stage I and II) Unfavorable HL
• General risk factors for unfavorable group:
― Large mediastinal mass
― Extranodal disease
― Elevated erythrocyte sedimentation rate (ESR)
― ≥ 3 involved areas
As defined by German Hodgkin Lymphoma Study Group (GHSG)
The classification, as I stated earlier, is the Ann Arbor Classification. And it is still in use. We broadly divide them into the early stages, stage 1 and II. But even among the stage ones and twos, we further divide them into favorable and unfavorable. And any of these factors that you see here will make that person unfavorable and will have implications in terms of treatment: either a large mediastinal mass, or extranodal disease, or three or more involved areas of disease, or an elevated sedimentation rate.
A classificação, como disse antes, é a Classificação Ann Arbor, que ainda está em uso. Grosso modo, os subdividimos em estágios precoces: estágios I e II. Mas, mesmo entre os estágios I e II, os subdividimos posteriormente em favorável e desfavorável. E qualquer um destes fatores que podem ver aqui farão aquela pessoa desfavorável e haverá repercussões em termos de tratamento: uma massa mediastinal grande, uma doença extranodal, três ou mais áreas acometidas pela doença ou uma taxa de sedimentação elevada.
12
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
International Prognostic Score for AdvancedHodgkin’s Lymphoma
• Analysis of 5,141 patients treated
with chemotherapy +/- radiation
• 7 factors emerged:
1. Albumin < 4 g/dL
2. Hemoglobin < 10.5 g/dL
3. Male gender
4. Age > 45
5. Stage IV
6. WBC count ≥ 15,000
7. Lymphocyte count < 600/µL
or 8% of WBC
• Those with 5 or more factor theoretically
would benefit from alternative
treatments, but small group (7% of
population)Hasenclever D, Diehl V. N Engl J Med 1998 339(21):1506
For the Hodgkin’s lymphomas that are advanced stage at presentation, this model has been devised with seven variables. And, as you can see, as the variable number increases, your chance of being alive without recurrence or any events will decrease in this case from 84% to 42%. Again, this is for patients with advanced stage Hodgkin’s lymphoma, stages III and IV.
Para os linfomas de Hodgkin que se apresentam em estado avançado, este modelo foi elaborado com sete variáveis. E, como podem ver, à medida que aumenta o número de variáveis, diminuem de 84% a 42% as chances de estar vivo sem recidivas ou sem qualquer evento. Novamente, isto é para pacientes com linfoma de Hodgkin em estágio avançado, estágios III e IV.
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Multiple Myeloma
• Disseminated malignancy of monoclonal
plasma cells
• Second most common hematologic malignancy
• Findings
– Lytic bone lesions
– Anemia
– Renal failure or azotemia
– Hypercalcemia
– Recurrent infections
The last topic that I want to discuss is multiple myeloma. This is a malignancy of plasma cells which are mature B-cells. It is a very common hematologic malignancy. The main findings are lytic bone lesions, which could cause pain in the patient; anemia, which would give symptoms of fatigue; kidney failure due to precipitation of a protein produced by the myeloma into the kidney; elevated calcium because of destruction of bone and re --- re --- demineralization of the bone; and hypercalcemia would give symptoms of increasing urination; as well as somnolence and could be fatal if not treated soon. You could also present with recurrent infections, mostly urinary.
O último assunto sobre o qual quero discutir é o mieloma múltiplo. Esta é uma neoplasia maligna das células do plasma, que são células B maduras. É um câncer hematológico muito comum. Os principais achados são lesões líticas nos ossos, que podem causar dor no paciente; anemia, que provocaria sintomas de fadiga; insuficiência renal decorrente da precipitação de uma proteína produzida pelo mieloma no rim; elevada concentração de cálcio por causa da destruição e desmineralização do osso; e a hipercalcemia causaria sintomas de aumento da micção, bem como sonolência e poderia ser fatal se não for tratada logo. Também poderia haver infecções recorrentes, a maioria delas urinárias.
13
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Diagnosis of MyelomaDiagnosis of MyelomaDiagnosis of MyelomaDiagnosis of Myeloma
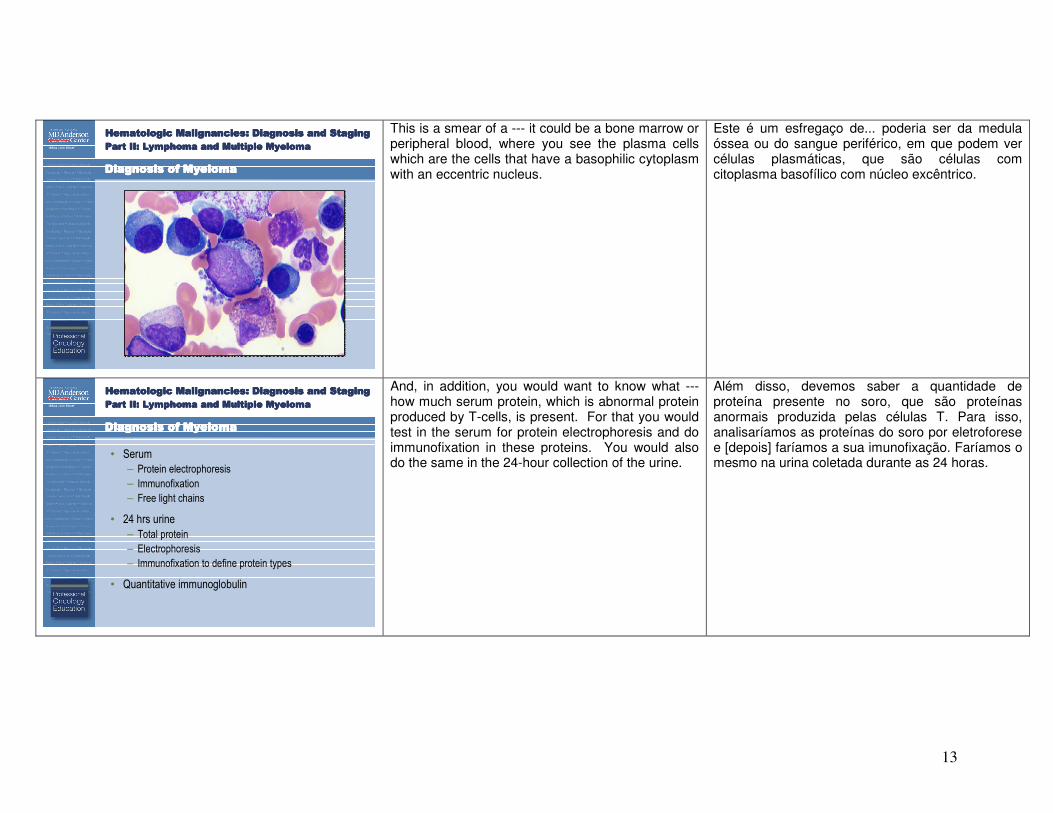
This is a smear of a --- it could be a bone marrow or peripheral blood, where you see the plasma cells which are the cells that have a basophilic cytoplasm with an eccentric nucleus.
Este é um esfregaço de... poderia ser da medula óssea ou do sangue periférico, em que podem ver células plasmáticas, que são células com citoplasma basofílico com núcleo excêntrico.
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
• Serum
– Protein electrophoresis
– Immunofixation
– Free light chains
• 24 hrs urine
– Total protein
– Electrophoresis
– Immunofixation to define protein types
• Quantitative immunoglobulin
Diagnosis of MyelomaDiagnosis of MyelomaDiagnosis of MyelomaDiagnosis of Myeloma
And, in addition, you would want to know what --- how much serum protein, which is abnormal protein produced by T-cells, is present. For that you would test in the serum for protein electrophoresis and do immunofixation in these proteins. You would also do the same in the 24-hour collection of the urine.
Além disso, devemos saber a quantidade de proteína presente no soro, que são proteínas anormais produzida pelas células T. Para isso, analisaríamos as proteínas do soro por eletroforese e [depois] faríamos a sua imunofixação. Faríamos o mesmo na urina coletada durante as 24 horas.
14
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Further Evaluation
If you do an x-ray of your skull, you will see the areas that are lucent. It means that there is less mineralization and these areas are devoid of bone.
Se tirarmos uma radiografia do crânio, poderíamos ver as áreas brilhantes. Significa que há menos mineralização e que essas áreas estão desprovidas de osso.
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
• Routine laboratory studies
– CBC
– Chemistries including calcium,
BUN and creatinine, LDH
• Skeletal survey
• Bone marrow biopsy
• Cytogenetics
• Serum β2M
Further Evaluation
You will do a complete blood count to see if your hemoglobin and platelets are adequate. You will test for the calcium and the kidney function tests in the blood. You will do a skeletal survey to see if you find any other areas in the body that have lytic lesions in your skull --- in your skeleton. You will do the bone narrow biopsy to document involvement by the increased amount of plasma cells. More recently, cytogenetics are becoming important in being able to predict how the patient will respond to therapy as well as survival. And also a blood test for the serum beta-2- microglobulin is becoming important in predicting outcome.
Faremos um hemograma completo para ver se [os níveis de] hemoglobina e plaquetas estão adequados. Faremos análises de sangue para determinar o cálcio e a função hepática. Faremos um exame do esqueleto para ver se encontramos outras áreas no corpo com lesões líticas no crânio... no esqueleto. Faremos uma biópsia da medula óssea para documentar o acometimento com base no aumento das células plasmáticas. Mais recentemente, a citogenética tem assumido um papel importante em poder predizer a resposta do paciente à terapia, bem como a sobrevida. Além do mais, um exame de sangue para a microglobulina beta-2 do soro está se tornando importante para predizer o desfecho.
15
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Durie-Salmon Staging System
Stage Characteristic MM Cell Mass
1 Hgb > 10 g/dL
Ca++ < 12 mg/dL
Bone survey nl or 1 lesion
IgG < 5 g/dL
IgA < 3 g/dL
Urine BJP < 4 g/day
Low
2 Fits neither stage 1 or 3 Int.
3 Hgb < 8.5 g/dL
Ca++ > 12 mg/dL
Advanced bone lesions
IgG > 7 g/dL
IgA > 5 g/dL
Urine BJP > 12 g/day
High
The Durie-Salmon staging system is an old system that is still --- can be applicable to a patient in order to predict how he will do and it is basically a tumor load system. As you can see between cycles --- stages I and III, the difference is that the hemoglobin is lower, the calcium is higher, the bone lesions are more, the amount of protein deposition is more, and this is the high tumoral mass stage.
O sistema de estadiamento de Durie e Salmon é um sistema antigo que ainda pode ser aplicado em pacientes para predizer sua resposta e é basicamente um sistema de massas tumorais. Como podem ver entre os ciclos... os estágios I e III, a diferença é que [os níveis de] hemoglobina diminuíram e os de cálcio aumentaram, as lesões ósseas aumentaram, a quantidade de deposições de proteína aumentaram e este é o estágio de massa tumoral elevada.
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
International Staging System
Stage Characteristic RiskOS
(med. Mos)
1β2M < 3.5 mg/L
Albumin > 3.5 g/dL
Low 62
2β2M 3.5 – 5.4 mg/L
Albumin < 3.5 g/dLInt. 44
3 β2M > 5.5 mg/L High 29
An international system has been devised, which is easy to do. It involves doing two blood tests. It includes a beta-2-microglobulin and a serum albumin. And, as you can see, the survival will range anywhere from 62 to 29% depending upon how many of these two variables are in the poor risk category.
Foi elaborado um sistema internacional, que é fácil de utilizar. Implica fazer dois exames de sangue: o de microglobulina beta-2 e o da albumina sérica. E, como podem ver, a sobrevida variará entre 62% e 29% dependendo da quantidade dessas duas variáveis que se encontrem na categoria de maior risco para óbito.
16
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
MM: Common Cytogenetics
― Deletion 13 (cytogenetics >>>> FISH)
― t(4;14)
― t(14;16)
― Deletion 17q13 (p53 mutation)
― Gain of 1q21
― Non-hyperdiploid
― 22q deletions
• Poor prognosis features
Cytogenetics, as I mentioned before, is important. The lesion 13, the lesion 17 among these that you see are important prognostic features…
A citogenética, como já mencionei, é importante. A lesão 13, a lesão 17 entre estas que vocês podem ver são características prognósticas tão importantes…
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Combining ISS Stage and Chromosomal Abnormalities on Survival Outcomes in Multiple Myeloma
IMWG Analysis
Genetic Abnormalities
4-Year Estimated OS
Minus vs. Plus Abnormality
Log Rank
P Value
Any 73% vs. 57% <.0001
t(4;14)
ISS I
ISS2
ISS3
64% vs. 36%
81% vs. 52%
63% vs. 30%
44% vs. 22%
<.0001
<.0001
<.0001
<.007
Del 17
ISS I
ISS2
ISS3
68% vs. 44%
81% vs. 64%
68% vs. 42%
48% vs. 28%
<.0001
<.020
<.0001
<.020
a. ISS I or ISS2, normal FISH 193/610 deaths (76%)
a vs. b <.0001
a vs. c <.0001
b vs. c <.0001
b. ISS I + abnormal FISH / ISS III +
normal FISH
140/252 deaths (52%)
c. ISS II or ISS III + abnormal FISH 146/196 deaths (32%)
Adapted from: Avet-Loiseau H et al. Blood (ASH Annual Meeting Abstracts) 2009 114: Abstract 743and Avet-Loiseau H. et al. Blood 2007 109:3489
….such that they have been combined with the international staging system. And this is a recent presentation with a combination of these two models that is a better predictor of how the patients will do at four years in terms of survival.
... que foram combinadas com o sistema de estadiamento internacional. E esta é uma apresentação recente com uma combinação desses dois modelos que é um melhor indicador da resposta dos pacientes em quatro anos de sobrevida.
17
Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging Hematologic Malignancies: Diagnosis and Staging
Part II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple MyelomaPart II: Lymphoma and Multiple Myeloma
Summary
• Hematologic malignancies are quite diverse
in their presentation and diagnosis
• Tools are available to assist in diagnosis,
staging and determining prognosis for each
hematologic malignancy
So, in summary, I have described the principle hematologic malignancies. As you see, they are quite diverse in their presentation and diagnosis. We have available ever-increasing tools to assist in diagnosis and staging. And we have developed newer models to try to help determine prognosis and arrange --- and decide what therapy is best according to the different subgroups. I hope this will help you evaluate patients who present in any of these presentations. And this concludes my talk. I hope that you have enjoyed the lecture and we welcome your feedback. Thank you.
Resumindo, descrevi os principais cânceres hematológicos. Como podem ver, são bastante diversos quanto ao quadro clínico e ao diagnóstico. Cada vez mais temos à disposição métodos que auxiliam no diagnóstico e no estadiamento. E desenvolvemos modelos mais novos para procurar determinar o prognóstico e arranjar... decidir a melhor terapia segundo os diferentes subgrupos. Espero que isto sirva de ajuda para avaliar os pacientes que apresentam estes quadros clínicos. Esta é a conclusão da minha palestra. Espero que tenham gostado da apresentação e agradeceríamos suas opiniões e comentários. Obrigado.