26
A Walkthrough of AJRR's PQRS 101 Orthopaedic Quality Resource Center Presented by CECity Jessica Safko Dan Gold

A Walkthrough of AJRR's
PQRS 101
Orthopaedic Quality Resource Center
Presented by CECity
Jessica Safko
Dan Gold

Agenda
PQRS 2015
Defining a Qualified Clinical Data Registry
Measures
Overview of QCDR
Next Steps
Q&A

Physician Quality Reporting System 2015
PQRS Payment Adjustment (Penalty)
•2015 is the first year that there is no longer an incentive payment for
PQRS participation.
•The PQRS program now carries an automatic 2% penalty for non-
participation in reporting PQRS measures by eligible solo providers
and GPRO group practices.
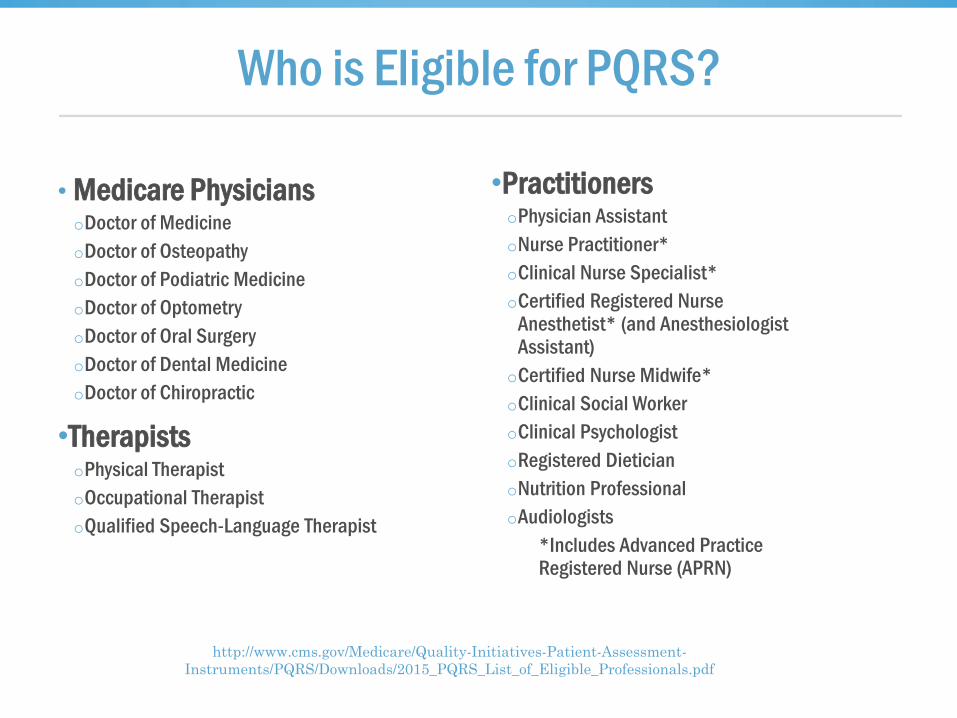
Who is Eligible for PQRS?
• Medicare PhysiciansoDoctor of Medicine
oDoctor of Osteopathy
oDoctor of Podiatric Medicine
oDoctor of Optometry
oDoctor of Oral Surgery
oDoctor of Dental Medicine
oDoctor of Chiropractic
•Therapists oPhysical Therapist
oOccupational Therapist
oQualified Speech-Language Therapist
•Practitioners oPhysician Assistant
oNurse Practitioner*
oClinical Nurse Specialist*
oCertified Registered Nurse Anesthetist* (and Anesthesiologist Assistant)
oCertified Nurse Midwife*
oClinical Social Worker
oClinical Psychologist
oRegistered Dietician
oNutrition Professional
oAudiologists
*Includes Advanced Practice Registered Nurse (APRN)
http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-
Instruments/PQRS/Downloads/2015_PQRS_List_of_Eligible_Professionals.pdf

CMS Quality Agenda
“Transforming Medicare from a passive payer to an active purchaser of high quality, efficient healthcare”
Fee for Service Pay for Value

Value-Based Modifier (VBM)
Value Modifier Payment Adjustment (Penalty) for 2015 PQRS Non-Reporters
•Groups with 2 - 9 EPs and solo practitioners: automatic-2.0% of
MPFS downward adjustment
•Groups with 10+ EPs: Automatic -4.0% of MPFS downward
adjustment
•These adjustments are additive to the 2% PQRS penalty
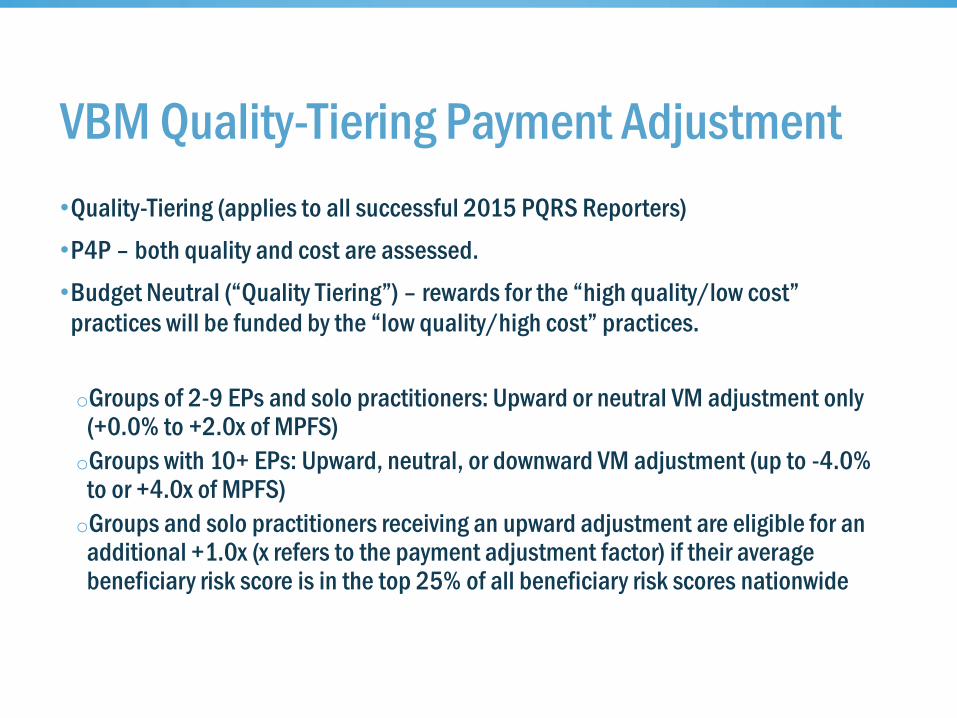
VBM Quality-Tiering Payment Adjustment
•Quality-Tiering (applies to all successful 2015 PQRS Reporters)
•P4P – both quality and cost are assessed.
•Budget Neutral (“Quality Tiering”) – rewards for the “high quality/low cost”
practices will be funded by the “low quality/high cost” practices.
oGroups of 2-9 EPs and solo practitioners: Upward or neutral VM adjustment only (+0.0% to +2.0x of MPFS)
oGroups with 10+ EPs: Upward, neutral, or downward VM adjustment (up to -4.0% to or +4.0x of MPFS)
oGroups and solo practitioners receiving an upward adjustment are eligible for an additional +1.0x (x refers to the payment adjustment factor) if their average beneficiary risk score is in the top 25% of all beneficiary risk scores nationwide

2015 Financial Risk: PQRS & VBM
•VBM penalties are additive to PQRS penalties.
•VBM quality-tiering is phasing in by group size, while PQRS penalties apply regardless of group size.
Physician
Group Size
Reporting Year
Year of
Financial Impact
Providers/Groups
That DON’T
Successfully Report PQRS
Providers/Groups That DO Successfully Report PQRS
PQRS VBM
Quality-Tiering Adjustment
1-9 2015 2017
-4%
(Includes PQRS
and VBM penalties)
No Penalty
Neutral (0%) or Upward (up to 2%)
10+ 2015 2017
-6%
(Includes PQRS
and VBM penalties)
No Penalty
Negative (up to -4%),
Neutral (0%) or
Upward (up to 4%)

Quality-tiering: Methodology
6 quality
Domains yield
a QUALITY
composite score
QUALITY + COST =
Quality-tiering
Value Modifier Amount
Quality of Care Composite Score
Clinical Care
Patient Experience
Population/Community Health
Patient Safety
Care Coordination
Efficiency
Cost Composite Score
Total overall costs
Total costs for beneficiaries with specific conditions

Quality Tiering: Quality Measures
Quality Composite is derived from the following measures:
o PQRS measures
o Outcome measures: • All Cause Readmission
• Composite of Acute Prevention Quality Indicators (bacterial pneumonia, urinary tract infection, dehydration)
• Composite of Chronic Prevention Quality Indicators (COPD, heart failure, diabetes)
o Consumer Assessment of Healthcare Providers and Systems (CAHPS) (reported through PQRS Group Practice Reporting Option - GPRO)
• Optional for GPROs with 2-99 Eps
• Mandatory for GPROs with 100+ EPs

Quality-Tiering: Methodology
QUALITY + COST = Quality-Tiering
2 cost measures
yield a COST
composite score.
Value Modifier Amount
Quality of Care Composite Score
Clinical Care
Patient Experience
Population/Community Health
Patient Safety
Care Coordination
Efficiency
Cost Composite Score
Total overall costs
Total costs for beneficiaries with specific conditions

Quality Tiering - Cost Measures
Cost Composite is derived from the following measures:
oMedicare Spending Per Beneficiary measure (3 days prior and 30 days after an inpatient hospitalization) attributed to the group providing the plurality of Part B services during the hospitalization
oTotal per capita costs measures (Parts A & B) for beneficiaries with 4 chronic conditions:•Chronic Obstructive Pulmonary Disease (COPD)
•Heart Failure
•Coronary Artery Disease
•Diabetes
(All cost measures are payment standardized and risk adjusted, and each group’s cost measures adjusted for specialty mix of the EPs in the group)

2015 PQRS & VBM Takeaways
PQRS:
Avoiding the PQRS penalty now requires more measures, and higher stakes with
up to 2% in PQRS penalties alone
Quality scores of PQRS measures MATTER and will tie into payment under the
VBM
VBM
VBM applies to all physicians and groups of physicians and the penalties are even
higher this year
Penalties for non-PQRS participation, in combination with VBM penalties are in
the 2-6% range depending on practice size
Those that DO report PQRS are automatically included in the VBM Quality-Tiering
process, which penalizes the low-performing providers and rewards the high-
performing providers.

2015 PQRS Reporting Methods

2015 PQRS Program Participation
PQRS Reporting Compliance for Individual Providers and GPRO
Practices
Individual Providers
Measures GroupReport one (1) measure group (per eligible professional) for
a 20 patient sample.
Individual Measures Report on nine (9) individual measures, across at least
three (3) NQS domains for fifty percent (50%) of eligible
Medicare patients. Providers who treat at least 1 Medicare
patient in a face-to-face encounter must report on at least 1
cross-cutting PQRS measure.
Group Practice Reporting Option (GPRO)
Individual Measures Report on nine (9) individual measures, across at least
three (3) NQS domains for fifty percent (50%) of eligible
Medicare patients.1 Practices who treat at least 1
Medicare patient in a face-to-face encounter must report
on at least 1 cross-cutting PQRS measure.
[1] Eligible professionals with a specialty that has less than 9 measures or less than 3 domains would be subject to the Measure-Applicability Validation (MAV) process, but could still avoid the payment adjustment.

2015 PQRS Program Participation & Penalty Avoidance
•Report as an Individual Provider
oQualified PQRS Registry
oElectronic Health Record (EHR)
oMedicare Part B Claims (Claims Based Reporting)
oQualified Clinical Data Registry (QCDR)

What is a Qualified Clinical Data Registry (QCDR)?
• Introduced in 2014, the QCDR method provides a standard to satisfy Physician Quality Reporting System (PQRS) requirements based on satisfactory participation.
•A QCDR is a Centers for Medicare & Medicaid Services (CMS)-approved entity (such as a registry, certification board, collaborative, etc.) that collects medical and/or clinical data for the purpose of patient and disease tracking to foster improvement in the quality of care furnished to patients. The data submitted to CMS via a QCDR covers quality measures across multiple payers and is not limited to Medicare beneficiaries.
•A QCDR is different from a Qualified Registry in that it is not limited to measures within PQRS. A QCDR may submit measures from one or more of the following categories with a maximum of 30 non-PQRS measures allowed:
o Clinician & Group Consumer Assessment of Healthcare Providers and Systems (CGCAHPS)
o National Quality Forum (NQF)-endorsed measures
o Current 2015 PQRS Measures
o Measures used by boards or specialty societies, and
o Measures used in regional quality collaborations

Qualified Clinical Data RegistryWhat Does a Registry Need to Qualify as a QCDR?
•At least 9 measures
•Measures must cross at least 3 national quality strategy domains
o Domains include: Communication and Care Coordination, Community/Population Health, Effective Clinical Care, Efficiency and Cost Reduction, Patient Safety, Person and Caregiver-Centered Experience and Outcomes
•A QCDR must also include at least 2 outcomes measure
o An outcome measure, as defined within the CMS Measures Management System Blueprint v10.0, indicates the result of the performance (or nonperformance) of functions or processes. It is a measure that focuses on achieving a particular state of health.
o If less than 2 outcome measures are available to an Eligible Professional (EP), report on at least 1 outcome measure and also at least one of the following types of measures:
• Patient Safety
• Resource Use
• Patient Experience of Care
• Efficiency/Appropriate Use
•A QCDR is not limited to measures within PQRS, and may include up to 30 non-PQRS measures A QCDR
may include additional measures that are PQRS measures, in addition to the 30non-PQRS measures

AJRR's Orthopaedic Quality Resource Center

AJRR's Orthopaedic Quality Resource Center PQRS Measures
oPQRS Measure #1: Diabetes: Hemoglobin A1c Poor Control
oPQRS Measure #21: Perioperative Care: Selection of Prophylactic Antibiotic – First OR Second Generation Cephalosporin
oPQRS Measure #22: Perioperative Care: Discontinuation of Prophylactic Parenteral Antibiotics
oPQRS Measure #23: Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis
oPQRS Measure #109: Osteoarthritis (OA): Function and Pain Assessment
oPQRS Measure #130: Documentation of Current Medications in the Medical Record
oPQRS Measure #131: Pain Assessment and Follow-Up
oPQRS Measure #217: Functional Deficit: Change in Risk Adjusted Functional Status for Patients with Knee Impairments
oPQRS Measure #226: Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention
oPQRS Measure #350: Total Knee Replacement: Shared Decision-Making: Trial of Conservative (Nonsurgical) Therapy
oPQRS Measure #351: Total Knee Replacement: Venous Thromboembolic and Cardiovascular Risk Evaluation
oPQRS Measure #352: Total Knee Replacement: Preoperative Antibiotic Infusion with Proximal Tourniquet
oPQRS Measure #353: Total Knee Replacement: Identification of Implanted Prosthesis in Operative Report
oPQRS Measure #355: Unplanned Reoperation within the 30 Day Postoperative Period
oPQRS Measure #356: Unplanned Hospital Readmission within 30 Days of Principal Procedure
oPQRS Measure #357: Surgical Site Infection
oPQRS Measure #358: Patient-centered Surgical Risk Assessment and Communication
oPQRS Measure #375: Functional Status Assessment for Knee Replacement: Knee injury and Osteoarthritis
• Knee injury and Osteoarthritis Outcome Score
• Oxford Knee Score
• Knee Society Knee Scoring System
• SF-36
• Veterans RAND 12 Item Health Survey (VR-12)
• Patient Reported Outcomes Measurement Information System (PROMIS)-10
The AJRR‘s Orthopaedic Quality Resource Center includes
22 approved PQRS measures.
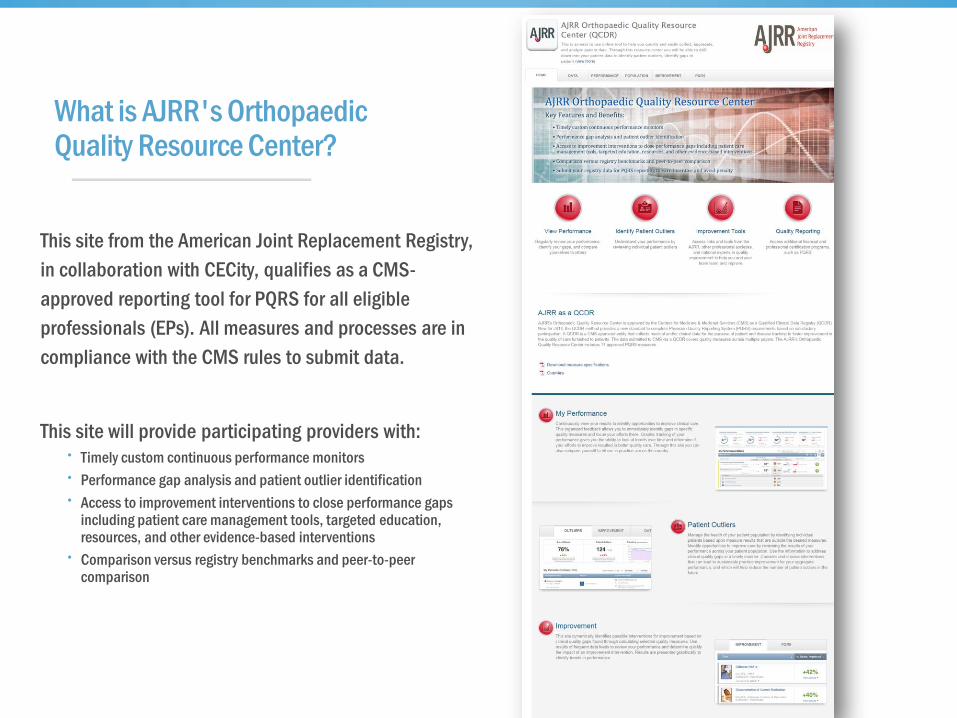
This site from the American Joint Replacement Registry,
in collaboration with CECity, qualifies as a CMS-
approved reporting tool for PQRS for all eligible
professionals (EPs). All measures and processes are in
compliance with the CMS rules to submit data.
This site will provide participating providers with:• Timely custom continuous performance monitors
• Performance gap analysis and patient outlier identification
• Access to improvement interventions to close performance gaps including patient care management tools, targeted education, resources, and other evidence-based interventions
• Comparison versus registry benchmarks and peer-to-peer comparison
What is AJRR's Orthopaedic Quality Resource Center?

AJRR's Orthopaedic Quality Resource Center Data Entry Methods –Manual chart form/Data Upload

The registry will calculate and
display each measure and quality
score in the performance monitor
(as frequently as daily).
Additionally the registry can
generate performance measure
gaps and lists of patient outliers,
and link to interventions and
improvement tools. The registry
can be configured to aggregate
measure scores at the practice,
location, department, and TIN
level, etc.
Measure Performance Scores

Continuous Performance Management
View a Snapshot of your measures
performance and expand to view details
Measure Name
Performance
Trending
Fixed Benchmarks
and Goals
Patient
Outliers

The AJRR Orthopedic Resource Center will be live on August 3, 2015
Pre-Register today at https://www.medconcert.com/ajrr
Registration Fee: $439 per provider
•Includes:
oAccess to Continuous Improvement Registry
oPQRS 2015 CMS Submission
For questions about the registry:
oEmail [email protected]
oCall 847.292.0530

Questions and Answers

















